Tools and Principles for Optimizing Adherence to HIV Regimens
49
PRINCIPLES FOR OPTIMIZING ADHERENCE TO HIV REGIMENS Edric Paw Cho Sing, Pharm. D. 2015 Candidate University of Toronto Faculty of Pharmacy Advanced Pharmacy Practice Experience Novack’s Rexall Drug Store 1
-
Upload
edric-paw-cho-sing -
Category
Health & Medicine
-
view
123 -
download
6
Transcript of Tools and Principles for Optimizing Adherence to HIV Regimens

1
TOOLS AND PRINCIPLES FOR
OPTIMIZING ADHERENCE TO HIV REGIMENS
Edric Paw Cho Sing, Pharm. D. 2015 CandidateUniversity of Toronto Faculty of PharmacyAdvanced Pharmacy Practice Experience
Novack’s Rexall Drug Store

2
PRESENTATION OVERVIEW• HIV/AIDS Today• HIV Drug Resistance• Mechanism of Drug Resistance• Impact of Adherence• Clinical Tools for Every Day Practice

3
HIV/AIDS TODAY

4
HIV/AIDS TODAY
www.unaids.org

5
1 in 10 ART-naïve patients carried HIV with ≥1 drug resistance mutation.
Rates of drug resistant HIV in ART-naïve patients have been rising, from 3.4% during 1995-1998, to 12.4% by 1999-2000.
North America was found to have the highest prevalence of transmitted resistance (12.9%)
HIV/AIDS TODAY

6
HIV/AIDS TODAY

7
HIV DRUG RESISTANCE

8
HIV resistance can arise in 3 ways:
① Sloppy replication (infidelity)
HIV RESISTANCE

9
HIV RESISTANCEHIV replication is sloppy!
≥1 mutation per genome transcribed ~20 billion mutations/day
HIV replication is high volume!
~10 billion copies/day 107-108 infected cells/day

10
HIV RESISTANCEHIV resistance can arise in 3 ways:
① Sloppy replication (infidelity)
② Through transmission (transmitted resistance)

11
HIV RESISTANCEHow is HIV transmitted?
12
HIV RESISTANCEHIV resistance can arise in 3 ways:
① Sloppy replication (infidelity)
② Through transmission (transmitted resistance)
③ Selective pressures (acquired resistance)

13
WHAT IS DRUG RESISTANCE?Drug Resistance – Ability of disease-causing microorganisms (e.g. bacteria or viruses) to continue multiplying despite the use of otherwise effective drugs.

14
WHAT IS DRUG RESISTANCE?

15
WHAT IS DRUG RESISTANCE?

16
THE MECHANISM OF DRUG RESISTANCE

17
MOR: Viral RT Discrimination M184V, Q151M complex, K65R
MECHANISM OF DRUG RESISTANCE: NRTI
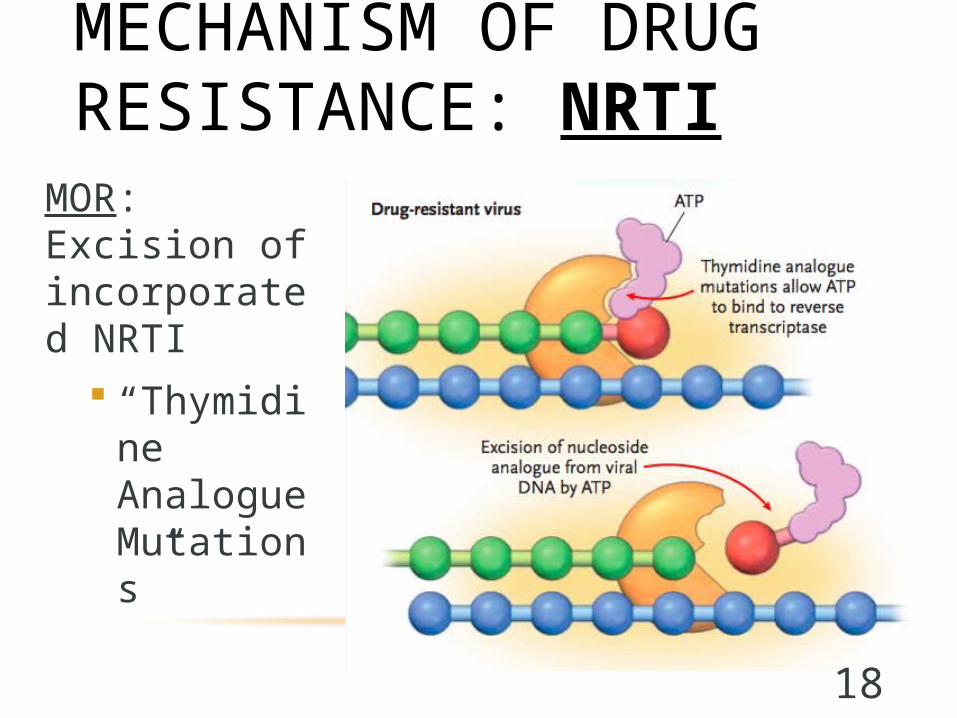
18
MOR: Excision of incorporated NRTI
“Thymidine Analogue Mutations”
MECHANISM OF DRUG RESISTANCE: NRTI

19
MOR: Reduction of NNRTI affinity to allosteric site Drug-dependent mutations (K103N efavirenz,
Y181C nevirapine)
MECHANISM OF DRUG RESISTANCE: NNRTI

20
MOR: Enlargement of catalytic site, reduction of PI affinity to the enzyme
MECHANISM OF DRUG RESISTANCE: PI

21
MUTATIONS AND RESISTANCELow Genetic Barrier – Single mutations which cause complete resistance
Ex. All NNRTI, 3TC
High Genetic Barrier – Multiple step-wise mutations needed to cause resistance
Ex. Protease Inhibitors, most NRTI

22
DISTRIBUTION OF DRUG RESISTANCE

23
DISTRIBUTION OF DRUG RESISTANCEReduced susceptibility more common for NNRTI’s compared to NRTI’s or PI’s

24
THE IMPACT OF ADHERENCE
25
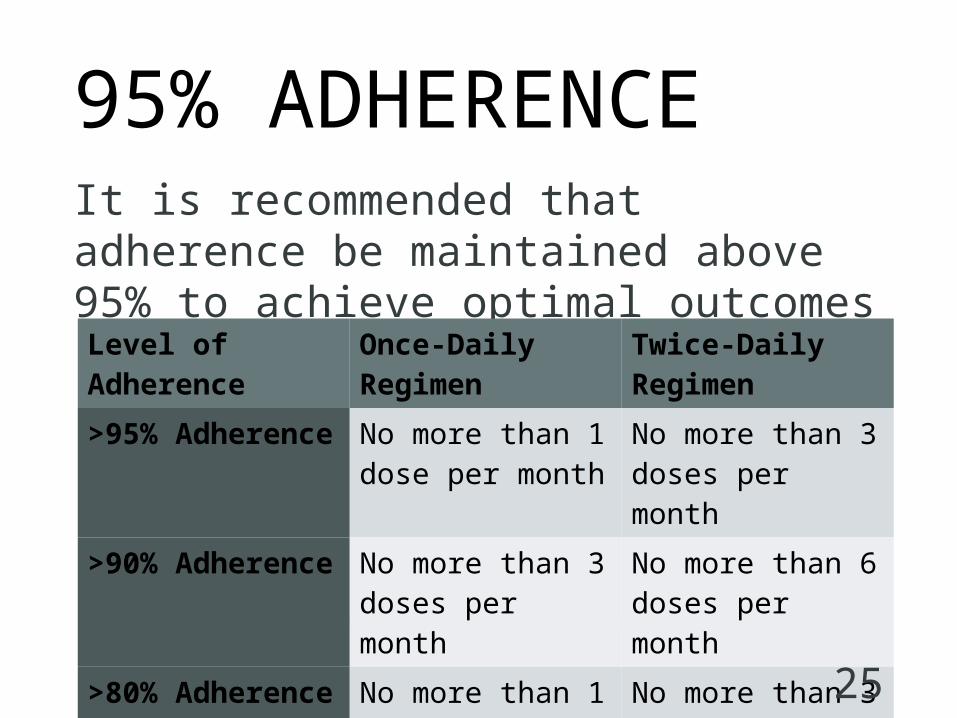
95% ADHERENCEIt is recommended that adherence be maintained above 95% to achieve optimal outcomes
Level of Adherence Once-Daily Regimen Twice-Daily Regimen
>95% Adherence No more than 1 dose per month
No more than 3 doses per month
>90% Adherence No more than 3 doses per month
No more than 6 doses per month
>80% Adherence No more than 1 dose per week
No more than 3 doses per week

26
95% ADHERENCEExample #1: Once-daily regimen
FTC/TDF (Truvada)Raltegravir (Isentress)
FTC/TDF/ELV/c (Stribild)
Example #2: Twice-daily regimen
Miss no more than 1 dose per month
Miss no more than 3 doses per month

27
THE BRITISH COLUMBIA STUDYObjective: To examine long-term effects of adherence on virologic and immunologic response
Primary Outcome: Immunologic response (CD4+): ≥145 cells/uL Virologic response (pVL+): 65% of the time with VL<50 copies/mL
Stratification of Responses: Best response (CD4+/pVL+) Incomplete response (CD4+/pVL- or CD4-/pVL+) Worst response (CD4-/pVL-)
28
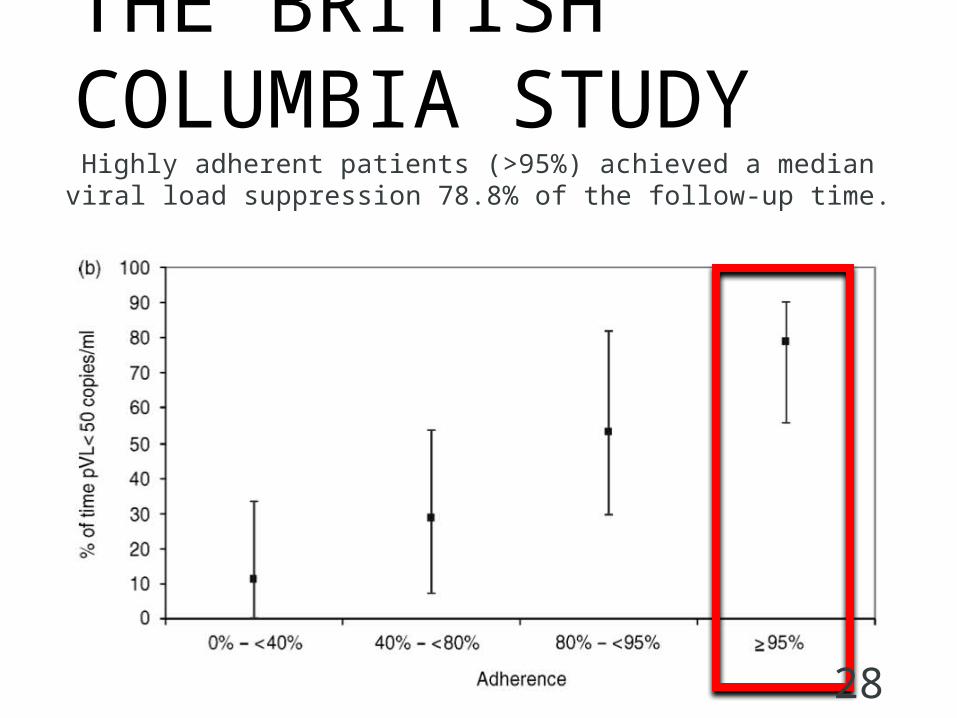
THE BRITISH COLUMBIA STUDYHighly adherent patients (>95%) achieved a median viral
load suppression 78.8% of the follow-up time.

29
THE BRITISH COLUMBIA STUDYAfter adjustment for certain baseline characteristics,
the probability for “best” response was higher for highly adherent patients (>95%)
30
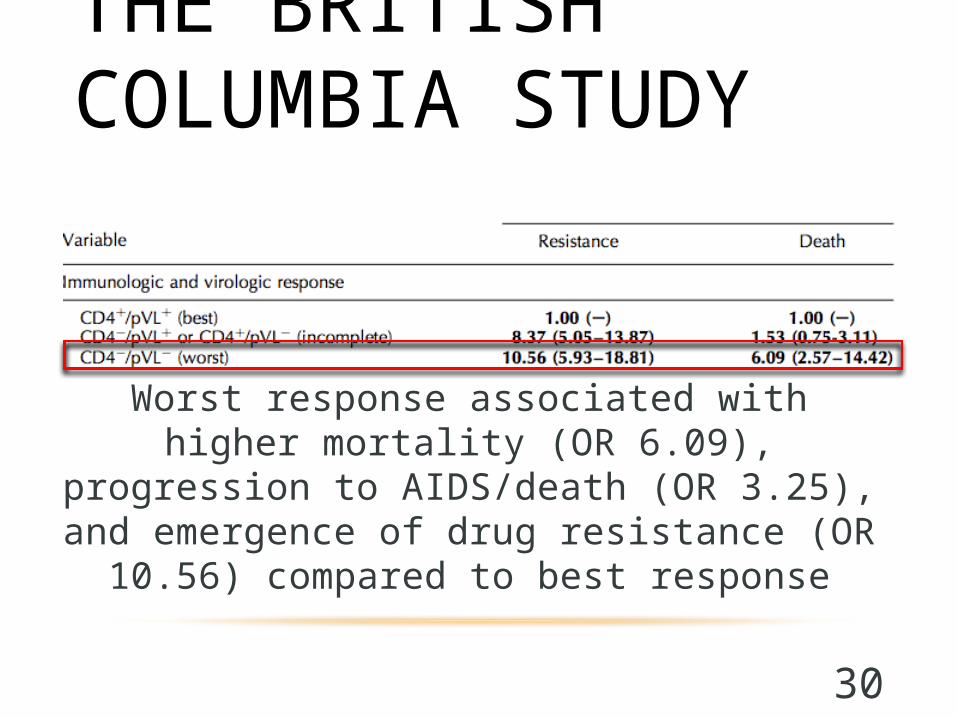
THE BRITISH COLUMBIA STUDY
Worst response associated with higher mortality (OR 6.09), progression to AIDS/death (OR 3.25),
and emergence of drug resistance (OR 10.56) compared to best response

31
THE BRITISH COLUMBIA STUDY
Conclusion: Adherence is a key feature influencing both virologic and
immunologic responses. When adherence < 95%, patients were more likely to experience
poor responses to treatment. When adherence > 95%, NNRTI and PI/r –based regimens
provided the highest likelihood of virologic and immunologic response.
Poor virologic and immunologic response led to negative health outcomes.

32
CLINICAL TOOLS FOR EVERY DAY
PRACTICE

33
ASSESSING ADHERENCE
1. Acknowledge the difficulties of adherence
“Taking pills every day is hard. Most people have problems taking their pills at some point during treatment. I am going to ask you about problems that you may have had taking your pills. Please feel comfortable telling me about pills you may have missed or taken late. I am asking because I want to make it easier for you to take them.”

34
ASSESSING ADHERENCE
2. Confirm understanding of the regimen
• “How many of [Drug A] are you taking per day?”
• “How often do you take [Drug A] per day?”
• “Are there any special instructions that you follow?”

35
ASSESSING ADHERENCE
3. Self-Assessment of Adherence
• Over the past 3 days
• Over the past week
• Over the past month
36
ASSESSING ADHERENCE
4. Reasons for Missed Doses
• Forgetful
• Away from home
• Too busy
• Side effects
• Feeling sick or depressed
• Ran out of pills

37
ASSESSING ADHERENCE
5. Ask about side effects or other problems
• “Do you have any difficulty swallowing the medications?”
• “Do the medications upset your stomach?”

38
ASSESSING ADHERENCE
6. Collaborate with the patient to facilitate adherence
• Review the potential risks of poor adherence
• Set goals (≥ 95% adherence)
• Offer specific suggestions

39
PROMOTING ADHERENCE

40
PROMOTING ADHERENCE: MEDISAFE
Visual, easy-to-use pill reminder and medication management app
• Free
• iTunes and Google Play
MediSafe reminds patient to take their pillMed-Friend (family member/care-taker) is notified if patient forgets to take pill.

41
PROMOTING ADHERENCE: MEDISAFE

42
PROMOTING ADHERENCE: HIVPLUS
Comprehensive HIV treatment resource with daily pill and appointment reminders
• Free
• iTunes and Google Play
Additional features: VL/CD4 tracker, pharmacy finder, health articles, treatment guidelines, clinical trials, complementary and alternative medicine information

43
PROMOTING ADHERENCE: HIVPLUS

44
PROMOTING ADHERENCE: GLOWCAP
Gadget fitting over prescription bottle and lights and beeps when dose is due. Sends alert to family members if bottle is not opened.
• $80 + $15/month (AT&T)
• American productAdditional features: Adherence reports, refill request button

45
PROMOTING ADHERENCE: GLOWCAP

46
PROMOTING ADHERENCE: GLOWPACK

47
GENERAL PRINCIPLES Successful adherence is an on-going effort Positive reinforcement Maintain open lines of communication Identify barriers to adherence Individualize strategies Non-judgmental approach

48
SUMMARY• Drug resistance hinders optimal HIV
management
• Transmitted HIV resistance is an on-going issue
• Different ARV drug classes have different genetic barriers to resistance
• ≥95% adherence is optimal
• Pharmacists are in a position to assess adherence and recommend tools to promote adherent behaviours

49
THANK YOU FOR LISTENING.QUESTIONS?