CONTENT · together the cardiovascular system and haemodynamics, move on the pulmonary function and...
41
CONTENT 1. Introduction 2. Structure of the training programme Rotations Acute care Surgery Unit C5 Trauma Cutting Colorectal unit Hepato-biliary unit Endocrine Oncology unit Vascular surgery unit Red Cross Children’s Hospital New Somerset hospital Mitchellsplain District Hospital ICU 3. Formative assessment and examination 4. FCS Intermediate examination syllabus, structure and tutorials 5. FCS Final examination syllabus, structure and tutorials 6. Other courses and requirements 7. Research 8. Leave and relief policy 9. SASSIT
Transcript of CONTENT · together the cardiovascular system and haemodynamics, move on the pulmonary function and...
CONTENT
1. Introduction
2. Structure of the training programme
Rotations
Acute care Surgery Unit
C5 Trauma Cutting
Colorectal unit
Hepato-biliary unit
Endocrine Oncology unit
Vascular surgery unit
Red Cross Children’s Hospital
New Somerset hospital
Mitchellsplain District Hospital
ICU
3. Formative assessment and examination
4. FCS Intermediate examination syllabus, structure and tutorials
5. FCS Final examination syllabus, structure and tutorials
6. Other courses and requirements
7. Research
8. Leave and relief policy
9. SASSIT
1. INTRODUCTION
Welcome to the Department of General Surgery at Groote Schuur Hospital.
The philosophy of our department in terms of training is both supportive and enabling with a strong
emphasis on personal development and responsibility. We aim to train general surgeons who are
not only competent but also independent, innovative, progressive and globally marketable.
One of the biggest challenges you will face as a registrar is to balance the 4 main responsibilities
that will rest on your shoulders for the next 4-5 years:
1. Surgical clinical and operative training to successfully obtain your FCS degree
2. Clinical research to successfully obtain your Mmed (Surgery) degree
3. Teaching undergraduate students and interns
4. Service delivery and optimal patient care in an efficient and innovative way in a resource
challenged environment
Although this might seem like a daunting task, the intention of this department is to provide and
equip you with:
1. Theoretical knowledge and practical ability as well as the interpersonal skills to become an
independent specialist general surgeon of international standard
2. The attitude and ability necessary to become an independent learner and to accept
responsibility for lifelong continuing professional development
3. The ability to plan, conduct, interpret and publish independent research in general surgery
and related fields
4. The work ethic needed and moral and social responsibility to act in the best interest of your
patient, improve the health care system of South Africa and meet our country’s current
health care challenges with a can-do attitude.
The generic outcomes of this training programme can be summarized as follows:
1. The trainee should possess a broad knowledge of :
- Current developments in medicine in general
- Ethical principles applicable to surgery and the practice of medicine in general
- An interdisciplinary approach to patient care
- Epidemiological and statistical principles and their application in analysis scientific data
- Humanitarian and social issues governing the overall practice of surgery and medicine in
general.
2. The trainee should possess the skill to:
- Identify and solve clinical as well as organisational problems with clear, critical and
creative thinking and act in a decisive manner
- Interact with patients and colleagues in a manner that displays exemplary professional
conduct
- Co-operate with all other members of the health care team and step-up as a leader of
the team when necessary
- Collect, analyse, organise and critically evaluate information and apply it appropriately
- Communicate effectively in the clinical as well as academic arenas and be comfortable to
use technological aids as an effective communication tool for teaching purposes as
appropriate.
2. STRUCTURE OF THE TRAINING PROGRAMME
During your surgical training you will rotate through a number of specialist and sub-specialist units.
Each unit has a unique function in your training. Detailed information about the daily
responsibilities and academic expectations of each unit will be discussed.
Outcomes for all rotations include:
1. Thorough knowledge and understanding of anatomy, physiology and general pathology as
applicable to general surgery and all its subspecialties
2. Detailed knowledge and understanding of general surgical principles and intensive care as
well as a broad knowledge and understanding of basic patient care of all surgical disciplines.
3. Thorough knowledge and understanding of up-to-date diagnostic approaches, pre-and post-
operative care and operative technique in recent reputable surgical publications as
applicable to the various units in general surgery.
JUNIOR ROTATIONS:
C14 Groote Schuur Trauma Front Room 3 months
Red Cross Children’s Hospital Trauma Front Room 3 months
Cardiothoracic Surgery 3 months
New Somerset Hospital 3 months
Mitchells Plain District Hospital 3 months
ICU 3 months
Acute Care Surgery 3 months
Relief 3 months
Depending on the number of registrars in the rotation, individual prior experience and service
demands, all registrars might not rotate through all the junior rotations while others might be
required to do a rotation more than once. C14, Acute care surgery, ICU, relief and a secondary level
rotation is non-negotiable.
After completion of your Intermediate exam, you will be eligible to move on to the senior rotations,
SENIOR ROTATIONS:
Acute Care Surgery 3 months
Paediatric and Burns surgery 3 months
Vascular Surgery 6 months
C5 Trauma Cutting 6 months
Colorectal Unit 3 months
Hepato-Biliary unit 3 months
Endocrine and oncology unit 3 months
Upper GIT Unit 3 months
Transplant unit 3 months
Although it will not be possible for all registrars, it is highly advisable to spend 6 months in
- Acute care surgery
- Trauma cutting
- Vascular surgery
The rotation roster will be available 1 month prior to change-over and will be worked out for 6
months at a time. If service delivery demands it, this roster is subject to last minute changes. We
recognise that this often leads to some distress on the part of the registrars but this ensures that
service demands are met. Please be accommodating in this regard – we work as a team with our
patient’s best interests at heart.
ACUTE CARE SURGERY UNIT
The Acute Care Surgery Unit manages all the acute general surgical referrals for Groote Schuur
Hospital and surrounds, excluding trauma. A number of elective general surgical procedures are
performed as well; making this an exciting rotation with plenty of useful learning opportunities.
Weekly Schedule
Ward round every day at 07:30
Afternoon ward round between 14:30 – 16:00
Monday: 12:00 6th year tut (F25 seminar room) (Second call registrar)
13:00 Abscess slate (C6 Trauma theatre)
Tuesday: 8:00 C6 theatre list (until 12:00) (Post call registrar)
09:00 Surgical outpatients (G-floor OPD building)
13:00 Firm Academic meeting (J-floor Main old building or F25 seminar room)
Wednesday: Elective full day theatre (D16 Theatre 7)
Emergency G-scope list (E23 GIT Unit)
12:00 6th year tut (F25 seminar room)(Second call registrar)
13:00 Abscess slate (C6 Trauma theatre)
17:00 Department Academic meeting (J-floor Main old building)
Thursday: OG10 Day theatre – full day (G-floor OPD building)
Elective full day theatre (D17 Theatre 1)
12:00 6th year tut (F25 seminar room)(Second call registrar)
17:00 Departmental Meeting (Alternate: M&M, Research and Journal club)
(J-floor Main old building)
Friday: 10:00 Microbiology Ward round (Led by on-call registrar)
11:00 Pre-clerk round (Interns & Registrars to clerk patients before round)
13:00 Abscess slate (D16 Theatre)
Ward F25
Registrars are expected to see all the patients before 07:30 every day. This also includes ICU
patients and outliers in other wards. Prescription-, antibiotics- and fluid charts must be filled in and
updated everyday. Wounds scheduled for inspection must be exposed before the round. Each
patient should be allocated to a specific registrar, with his/her name and date of admission written
on the cover page. This registrar will be responsible for all aspects of care and all documentation for
this specific patient during their time in the firm. Allocation must be according to admitting doctor
or operating surgeon.
Interns are responsible for the day-to-day running of the ward. Once the ward work is done, interns
are encouraged to join registrars in the various theatres and SOPD. The ward remains the priority
for interns and during office hours there must always be one present to attend to problems, family
etc. All referrals to other departments (including radiology and microbiology) should be registrar-to-
registrar referrals. Interns are expected to lead the afternoon ward rounds. They must know all the
patients and their current issues, as well as the results of the investigations that were requested on
the morning round. These results must be in the folder and appropriately acted upon. We are not
using a jimmy book in F25, as this is non-reliable record keeping. During the ward rounds interns
should make an entry into each patient’s clinical notes on the plan and management decisions. The
quality of the folder directly reflects on our practice. Each patient must have a neat surgical booklet
with clinical notes on the right and all special investigations (blood result sheet on top) filed on the
left. All theatre notes, G-scope reports, afterhours ultrasound reports, ECG’s, Lung function tests,
etc. must be filed and not just loosely put into the folder.
During office hours, patients known to the firm will often represent with problems directly to the
ward. They will normally be seated in the waiting area between F25 and F26 and should be
attended to by the registrar to whom they are known or by an intern as appropriate. Ignoring them
will not make the problem go away. Folders from the legal department for J88’s and medical reports
(mostly from your time in C14) will follow you to the ward. Please check regularly with the ward
clerk, complete these and send them back.
The intern’s office in F25 is mostly the meeting place for the firm. It is everybody’s duty to clean up
after themselves and not to leave the place in a mess.
Patient presentation
Registrars are advised to present patients in a manner befitting their training. They are to note that
they are no longer students and a patient presentation filled with unrequired frivolity should be
refrained from, as this reflects poorly on the individual’s professional abilities. A patient
presentation should be done in a manner of collegial discourse. State clearly the patient’s problem
list. This includes confirmed diagnosis and their current status and management, as well as
undiagnosed problem, usually presented as clinical signs and symptoms.
As mentioned elsewhere in this document, ward rounds commence with the most ill patients in the
Unit, namely in the ICU. To this end, your presentation must clearly reflect your full comprehension
of the pathophysiology of the acutely ill. You are strongly advised to have a systems-based

approach. This can be of your choice, but it should be advised that starting with cerebral function
and then moving down from head-to-toe minimizes the changes of neglecting something. Group
together the cardiovascular system and haemodynamics, move on the pulmonary function and
ventilation, followed by renal function and acid-base status. Then present the functions of the
endocrine system, metabolic system, and immunological system inclusive of microbial infestation.
Conclude with the status of the surgical problem, wounds, etc.
Discharges
A discharge summary must be typed and two copies should be printed for every patient. These
should be saved on the computer in the intern’s office. One copy must accompany the patient and
one copy filed on the left side in patient’s surgical booklet. In addition every patient should have a
TTO, sick letter and a clear follow-up plan. This must be done by the intern in liaison with the
registrar whom would take ultimate responsibility.
Data/Stats Collection and online forms
In order to facilitate the growing need for research publication to be completed by this Unit, there
will be a continued drive towards electronic record keeping. To this end, plans will be made to have
an e-mail in your inbox every morning. This is for simple recording of all admissions and discharges
and must be completed by 06H30 in the morning following a call or 17H00 for discharges. There is
also a form for both morbidity and mortality which must be completed for your patient when
appropriate.
To emphasize the importance of this matter, failure to comply with the research aims of this Unit
will result in the disciplinary action as mentioned elsewhere.
Calls
Interns do calls as per their surgical roster. The hot call intern is responsible for F25 and acute
surgical referrals in conjunction with the registrar on call. Post-call is normally possible after the bulk
of the ward work is done. It is thus a good idea to arrange calls that only one of the Unit’s interns
are on call at a time.
One of the Unit’s own interns must also be available for weekend ward rounds, normally at 08:00.
Registrars are responsible for their own roster and timeously handing it in. During weekdays there
must be a registrar on second call who will be available till 16:00 if the first caller is busy or will take
over the call in the case of absence. The second call registrar also does the abscess slate. Post call is
seen as a privilege and can only be taken when your own patients are completely sorted out.
Tuesday’s SOPD + academic meeting and Friday’s pre-clerk round must also be attended first before
post-call can be taken. All call related queries and complaints must be directed towards the Chief
Resident. Consultant cover is provided by the in-house consultants everyday till 16:00 and
thereafter as per call roster. Weekend rounds are attended by both registrars coming on and going
off.
Leave
Interns’ leave is as per their roster.
Registrars must apply for leave via the registrar leave co-ordinator, currently Dr Liana Roodt. This
includes all types of leave (annual, study, congresses, etc) and can only be granted if on her
timetable. Only one registrar of the firm can have leave at a time. If a relief registrar is provided
he/she will temporary look after the patients of the registrar on leave.
Theatre
Although we are the acute care surgical unit we still have the most elective theatre time of all firms.
All main theatre bookings are done by the junior consultant on an on-line calendar. OG10 is a day
theatre for cases done under local anaesthetic by a registrar on a rotational basis and interns are
encouraged to assist or do some of the cases. Non-urgent referrals can be seen at our SOPD before
booking and urgent in-patient referrals must be seen by registrar on-call to be booked appropriately.
All OG10 booking will be done and managed by the MO, currently Dr Angela Dell. The length of the
list varies, but could be quite full, so it is advisable to start directly after the morning round at about
08:30 –09:00.
Abscess slates are three times a week. The patients are booked directly by C15 doctors, so it is
important to evaluate the patients before anaesthesia. A registrar must be present, but this is a vital
basic surgical skill for all interns to acquire.
C6 theatre is a morning list on a Tuesday that must be booked on the main emergency list the
previous day. The point of this list is to decant less urgent or green cases from the main emergency
list and prevents patients from being unnecessarily starved for prolonged periods. The list needs to
be handed into the C6 theatre before 15:00 on Monday. This must be done by the registrar on call
for Monday as he/she will also do the list on Tuesday morning.
Elective theatre is twice a week. The bulk of our work is hernia’s and lap chole’s which is the two
most common general surgery operations in most practices, but there tend to be a good variety of
cases. The registrars must allocate themselves to lists on a rational basis. This person then takes full
responsibility for the list which includes: seeing patients pre- and post-op; booking PAHCU/ICU beds
when needed; liaising with anaesthetic team for special needs and arriving in theatre no later than
07:40 to facilitate an 08:00 cutting time and set up equipment. An electronic operative report must
also be completed.
All elective cases for the following week should be seen at the pre-clerk round on a Friday, which
make it important to give patients this date when booking them for an operation. The whole team
attends this round where patients are presented, examined and informed consent signed. It also
provides the opportunity to do all the anaesthetic work-up (bloods, CXR, Lung fx and ECG’s) as per
Groote Schuur protocol and write a blue board for when patients come in. Please see addendum at
the end of this document for further guidelines. Interns are welcome to attend elective theatre and
will have the opportunity to assist.
SOPD
Clinic is only once a week and takes priority over most things. We aim to all be there by 09:00 and
interns join when the ward work is done.
G-scopes
Endoscopy at Groote Schuur is a consultant service, but registrars are welcome to join for training if
cleared by Prof Krige or Prof Thomson with a training letter and they have attended the endoscopy
course held by Dr. Chinnery.
Academic Meetings
The firm has its own academic meeting on Tuesdays. There will be a registrar presentation on a
specific relevant topic, interns will present the M&M of the past week and interesting radiology
might be revisited.
After the meeting we will all have “tea” together. There is a tea roster in the intern’s office.
Departmental meetings on Wednesdays and Thursdays are compulsory for registrars. Apologies
must be directed to Prof Kahn’s office. Interns are welcome to attend if they are interested.
End-of-rotation Assessment
Interns will be assessed according to HPSCA recommendations and requirements. Each registrar will
have a formal end of rotation oral assessment for both feedback purposes and academic evaluation
relevant to acute surgery. This is a good opportunity to present your CMSA logbook and evaluation
sheet for the necessary signatures.
The wounded surgeon plies the steel That questions the distempered part; Beneath the bleeding hands we feel
The sharp compassion of the healer's art Resolving the enigma of the fever chart.”
T.S. Eliot
C5 - CUTTING REGISTRAR
Welcome to Ward C5! This ward is your RESPONSIBILITY.
All admissions must be discussed with the C5 registrar on call. He/she is then to inform the ward
sister of the admission.
Patients admitted for abdomen, chest, neck, circulation and vascular observations must be reviewed
regularly when on call.
DO NOT leave patients in the admission area once fully assessed.
Ward Rounds
Ward rounds are held daily at 08H00 and 15H00 religiously.
The patients in ICU are seen once the round in C5 is done.
All patients must be seen prior to the morning ward round. Notes are made in the folders, fluids
written up and the prescription chart revised daily.
The "jimmy work" is the primary responsibility of the registrars. There is an intern allocated to the
unit. Foreign students may assist with the jimmy work but must be supervised at all times.
All special radiological investigations are arranged or booked by registrars with an appropriate
request. These should be discussed with the radiologist-on-call.
The afternoon ward round is a working round and all emergency investigation results and dates for
special investigations must be available. Not all registrars need be present for the p.m. ward round.
However, if the cutting reg-on-call is busy in theatre, there has to be someone available to do the
round.
The incoming and outgoing registrar does weekend ward rounds. Any problems must be discussed
with consultant on call.
Note taking and folders
These must be kept neatly and in the following sequence:
All notes are kept in a Trauma folder.
Referral letter
Front room clerking sheet
Blood and microbiology results
Special investigations; CT reports, ECG, angio reports etc.
Operation notes - electronic
Follow up notes
This is very important as many patients are victims of violent crime and there is always a potential
for litigation and court appearances.
Op notes
Operation notes are made in duplicate. One is inserted into the folder and the other is given to the
department secretary.
Surgery
We are a tertiary institution with all surgical specialities. Make use of them.
We tend to do all of the following emergency operations:
ALL vascular cases except those requiring bypass - i.e. aortic arch injuries, stenting
ALL neck explorations
ALL laparotomies
ALL acute cardiac tamponade
Uncomplicated clotted h/thorax and empyemas
Emergency resuscitative thoracotomies
Diagnostic and therapeutic cavitational endoscopy.
Semi-elective surgery includes:
SSG / debridement
Closure of colostomy
Re-look laparotomy from ICU
Amputations
Clotted haemothorax clearance / decortication
These are done in C6 theatre on a daily basis (Re-looks in D16 usually). Cases must be booked a day
earlier or the morning of surgery and the sister and anaesthetist informed.
We request you realise your limitations. Do not do procedures you are not familiar with.
An assistant to assist with surgery is available daily. These are usually foreign and sixth year
students.
We hope you enjoy your stay with us.
Happy cutting.
PHN
COLORECTAL UNIT
Welcome to the Colorectal Unit!!
Weekly Schedule
Ward round every day at 7:30.
Mondays: Full day theatre
Tuesdays: 8:00 – Academic round Prof Goldberg
9:30 – Meeting in Prof’s office
10:00 – Outpatient clinic E22
Afternoon round after Medical GIT grand ward round
Wednesdays: Morning theatre
13:30 – Combined rectal clinic LE34
Thursdays: 8:00 – Grand Round
9:00 – X-ray meeting
10:00 – Tea
10:30 – Academic round Prof Goldberg
11:00 – Registrar tut with 5th years
12:00 – Weekly summaries of Intestinal Failure patients
Fridays: Interns clerk patients for surgery the following week
Registrars help with pre-clerking
Ward F17
Registrars are expected to see all the patients before 7:30 every day.
Our ward is unique because we have a dedicated unit within a general ward. The Intestinal Failure
Care cubicle has 6 very sick patients. All patients are primarily the responsibility of the registrars.
The patients should be divided between the 2 registrars, so that the one registrar can leave the ward
round early on theatre days to prepare the 1st patient in theatre.
Interns are responsible for the day-to-day running of the ward. Once the ward work is done, interns
should join the registrars in theatre or clinic. All referrals to other departments (including radiology
and microbiology) should be registrar-to-registrar referrals. Interns are responsible to lead the
afternoon ward round. They must know all the patients and their current issues, as well as the
results of the investigations that were requested on the morning round.
If an intern is called after hours to assess a patient in the ward, the registrar MUST be notified of the
patient’s condition. All Intestinal Failure patients must be assessed by a registrar, if the nursing staff
are concerned about his/her condition. These patients have very limited reserve and prompt
appropriate treatment is indicated when necessary.
A temperature spike in any patient with a central line should be communicated to the registrar.
Blood cultures must be done through the CVP and the line removed (tip sent for MCS) if there is a
suspicion of line sepsis.
Discharges
A discharge summary must be typed out for every patient. These should be saved on the computer
in the Intern’s office. The ICD 10 code is mandatory for every patient, and is obtainable from the list
provided in the Intern’s office. If an ICD 10 diagnosis does not appear on that list, please notify Dr
Coetzee, who will supply the code.
We have 2 follow-up clinics:
E22, Tuesdays at 9am – Benign pathology
LE34, Wednesday at 11am – All cancer patients
Both these clinics offer the same services i.e. stomatherapy, removal of sutures, histology results
etc.
Patients should be followed-up only at one clinic. Only the consultant on the ward round can
request for a patient to be seen at 2 occasions for postoperative follow-up.
All cancer patients must be seen within 4 weeks after discharge at the Combined Clinic, LE34.
Appointments are made at extensions 4286/4287. It is VERY important to book these patients as
post-operative follow-up patients for the afternoon clinic. The Colorectal Unit does not have a
waiting list for this clinic, and all our patients must be accommodated at the requested date. If there
is any trouble in getting a follow-up date for a patient, the consultant should be notified.
X-ray Meetings
We have an X-ray meeting with the radiologists every fortnight. Every other Thursday is a teaching X-
ray meeting where the registrars are responsible for presenting the X-rays.
The names of patients whose imaging must be reviewed, will be given to the registrars in the
Tuesday meeting. It is the Intern’s responsibility to prepare a summary of these patients and hand it
to the radiology registrar responsible for that meeting before the end of the day on Tuesday. The
name and speed-dial of the radiology registrar is obtainable from the C10 desk. Attendance of this
meeting is compulsory. Interns are responsible to bring the list of patients, as well as the patient
folders to the meeting.
Weekly summaries
On Thursday afternoons the registrars are responsible to complete the Weekly Summery Sheets on
all Intestinal Failure patients. All microbiology as well as on-going issues should be reviewed.
Medication boards should be up-dated and re-written.
Central line sepsis prevention
Because of the significant impact of central line sepsis in intestinal failure patients, we have an active
programme to help prevent this complication. This programme is based on evidence based
interventions proven to reduce line sepsis.
When placing a central line:
ALWAYS wash hands with Chlorhexidine
ALWAYS wear mask, cap, gown and gloves
ALWAYS clean the site with Chlorhexidine
A registered nurse must be present with the Line Placement tick-sheet
CVP sites must be checked daily
We collect data on Central line sepsis and Infection Control audits the ward once a week.
Ward referrals
The registrar on call must see all ward referrals during the day before the afternoon ward round. All
referred patients must be discussed with and reviewed by a consultant.
Always available policy
The consultants of this unit are always available for any queries, any time of day or night. No one in
our team has to make a decision on a problem that he is not comfortable with. Please phone and
ask for advice or help early, to prevent bigger problems later.
Our Numbers:
Adam: 76638
Claire: 76945
We hope that you will enjoy the time in colorectal and that you will gain knowledge and skill to help
many patients in the future.

NEW SOMERSET HOSPITAL
Welcome! New Somerset Hospital (NSH) is a regional general specialist hospital for the metro west
district of the Cape Metropole. A wide variety of surgical problems are seen at NSH providing an
excellent opportunity for mastering your surgical skills.
Weekly Schedule
Duties
There are 4 main areas which need to be covered: Ward, Theatre, Clinic and Scopes. Registrars and
MO’s will rotate on a weekly basis.
Ward round every day at 08:00
Afternoon ward round between 14:00 – 16:00 (On call person and ward person to join)
Theatre Clinic Endoscopy Ward
Monday Starts at 13h00 with urgent cases left from weekend
Starts at 12h00
10 new patients
Starts at 11h00
Urgent cases from weekend
Ward work and referrals
Tuesday Full day theatre Starts at 08h30
45 patients (10 new, 35 follow ups)
Starts after ward round
15 Gastroscopies
3 Colonoscopies
Ward work and referrals
Wednesday Full day theatre Student tutorial at 10h00 after ward round
Starts after ward round
15 Gastroscopies
3 Colonoscopies
Ward work and referrals
Thursday Full day theatre Starts at 08h30
45 patients (10 new, 35 follow ups)
Starts after ward round
15 Gastroscopies
3 Colonoscopies
Ward work and referrals
Friday Full day theatre Starts at 08h30
35 patients (10 new, 25 follow ups)
Starts after ward round
15 Gastroscopies
3 Colonoscopies
Ward work and referrals
Monday: After ward round: Presentation (by registrars or students, M&M).
Wednesday: 17:00 Department Academic meeting (J-floor Main old building)
Thursday: 17:00 Departmental Meeting (Alternate: M&M, Research and Journal club)
(J-floor Main old building)
Ward on 2nd Floor
All registrars are to see patients before the 8:00 ward round. Prescription-, antibiotics- and fluid
charts must be filled in and updated everyday. Wounds scheduled for inspection must be exposed
before the round. The registrar assigned to the ward is responsible for the following:
To ensure that ward work is completed – interns are responsible for taking bloods, removing
chest drains, referrals to social worker, physio, etc.
To discuss all radiology (ultrasound, CT scans etc) with the radiologist present
All referrals to other departments (within NSH and to GSH)
To be on call during the day till the afternoon ward round handover
Discharges: Completed on-line by the interns.
Theatre
Aim to be in theatre by 7:40 to ensure a cutting time of 8:00.
See patients for the slate before you go to theatre and make sure all anaesthetic orders are followed
and blood results available in the folder.
All patients are seen and consented the day before surgery. The 6th year students will present the
patients to the consultant but sometimes he/she will ask you to see patients for next day. This will
occur between your theatre cases.
On Thursday you are responsible for the cases on the Friday slate, you must see them preoperatively
and will do them unsupervised in theatre on Friday. If unsure about a case please ask the consultant
in theatre on Thursday to review the case with you. If you need help on Friday, ask Langa Nqwena
to help with a particular case he should be available after ward round. (Remember to hand in a list at
theatre)
Clinic
There is an outpatient surgical clinic on all weekdays except Wednesday. On Wednesday, the clinic
registrar/MO will take the students for teaching after the ward round. There is a local list after the
clinic on a Friday which takes place in main theatre (Theatre 4).
Scopes
G- and C-scopes are done after the round every day of the week.
Calls
Roster is drawn-up amongst yourselves and must be submitted timeously.
If there is a shortage of registrars / MO’s because of leave, the endoscopy person will cover other
areas.
RED CROSS CHILDREN’S HOSPITAL
Welcome to Red Cross Children’s hospital. I hope you enjoy your time here with us. You will find that the hours required are slightly longer but I guarantee the atmosphere to be friendlier and the enjoyment of the work more than that previously experienced. Should you have any queries or problems feel free to ask. To follow is some information to help you for the next 3 months. Please introduce yourself to Mrs. Vollenhoven ([email protected] - 0216585012), Prof Numanoglu’s secretary on the 6th floor ICH building room 6.15. Give Mrs Adams ([email protected] - 0216585335) on the 6th floor room 6.22 your contact details, e-mail and a photocopy of your ID Card.
THE DEPARTMENT
Head of Department: Prof A Numanoglu
Head of Trauma Unit: Prof AB van As
Head of Clinical Unit: Dr S Cox
Senior Consultant: Dr D van Delft (From Mid-April 2014)
Part time consultant: Prof. H Rode (burns)
Part time consultant: Professor A Millar
Paediatric surgery Trainees: Dr A Theron
Dr Mugambi Matchoki
Dr G Van Niekerk
Dr K Milford
Access
You will need a Red Cross ID tag made by the access control team at the hospital. Please call at one of the departmental secretaries on the 6th floor to get the access form signed by the HOD. Take this with you to the access control office where the card will be made and supplied after being loaded with appropriate access allocations. Use this card to enter all wards, theaters etc.
PACS: please contact the PACS manager via switch board. You need different access user name and password to GSH. Do this on day 1 so that your access is granted within the first week. Without this ordering and viewing of results of all radiology is not possible.
NHLS: the new access system for the NHLS will be coming on line some time in 2014. This is the same as it would be for any of the other hospitals. You would only need to activate this access if Red Cross is the first time you would be using the NHLS system. Contact the local lab for information on how to go about gaining NHLS access.
Bleeps
Bleeps are available from switchboard – but most people prefer to use cell phones. Give Mrs Gio Adams (6th floor ICH) switchboard, Dr Cox and D2 and C2 your cell numbers. Bleep staff via switchboard. Dial 9 and ask for the relevant person.
Wards
D2: General Surgical and Urology C2: Burns D1: Surgical specialties, eyes, ears, plastics, neurosurgery, and orthopedics ICU: On C floor – combined medical and surgical A7: Day Case Surgery TRAUMA WARD: ground floor
Allocation
Two Registrars to D2 One Registrar to C2 Two Registrars to Trauma front Room: Roster via the trauma unit secretary – call her and give your contact details (021 6585 000).
Calls
Trauma registrar to do calls on a shift system as per the trauma unit timetable and need not read further in this document.
Burns registrars will do calls for Paediatric surgery covered by a Paediatric surgery senior registrar or consultant.
Senior in D2 will do seniors registrar calls with pediatric surgical fellows. These calls will cover the paediatric surgical service at Red Cross, burns and affiliated neonatal nurseries. It will be done with an intern and consultant.
Post call early day is not guaranteed only if the workload permits. This especially holds true on Tuesday and Friday.
There is an on-call sleep room in E3. The key will be stored in E1 and needs to be returned there daily so that the cleaners can access the room. Reg room is room number 7.
Burns
See the protocols for clerking, fluids, analgesia, and consent in C2.
This protocol is lengthy and you are advised to familiarize yourself with it. It is available electronically and in hard copy in the unit. Please read it as even if you are doing general surgery as opposed to burns, you will be seeing and assessing burned patients when on call, on the weekends and at the OPD clinics.
General
The Burns registrar: Responsible for the running of the burns ward. This entails ward
management, theatre lists (preparation and performing them), burns out patients and Sarah
Fox. You will be under the supervision of Prof. Rode and Dr Saleigh Adams from Plastic Surgery,
but the patients in that ward are your responsibility. The senior registrars will be happy to
provide assistance and advice where required. Discuss each list with the anaethetist doing the
list. Note blood requirements and size of burn/ graft on the list.
You are also required to attend SOPD on a Tuesday morning, Radiology meeting 12:30 and the 14:00 teaching round on a Tuesday as well as Tuesday and Friday afternoon teaching sessions and meetings.
D2 Registrar: To help in the running of D2 ward under the guidance of the Paediatric Surgery Senior Registrars. See timetable for details. The running of D2 is arduous and requires a team effort so please consult with the senior registrars what is to be done and where over and above the timetable you will be given.
Theatres
ALL Patients booked for theatre (A7, Main theatre) MUST BE DISCUSSED WITH SENIOR REGISTRARS OR CONSULTANT FIRST.
A7 theatre: Only well patients with NO medical history (ASA 1) older than 2 years for minor procedures and abscess patients older than one year
Main theatre: All other patients
Somerset Bookings:
There is a Somerset booking book for children over 3 years of age needing day case surgery. Somerset will do 3 cases a week. Please book all appropriate cases on this list. It is an attempt to reduce our day case surgery waiting list.
Meetings
Ward Rounds
The 07:30 am ward round is a time to discuss problems in the wards and the previous days referrals from other wards and hospitals. Have all the names of ALL the referrals you saw the day before, as well as the X-Rays ready loaded on the passage monitor in D2. ALL out of RXH consultations MUST have their stickers placed in the SURGERY file.
ALL surgical patients must be seen, examined, notes made and fluid charts filled in prior to the 7:30 consultant rounds.

Radiology Meeting
Tuesday at 12.30. All to attend. This is generally an important meeting where difficult decisions are made. The list is created daily on the ward rounds as we add patients for discussion. f you are running the meeting, hand in the list to the radiology department the day before, with brief summaries of all the patients. In addition, load them onto the Public Folders section on PACS under the appropriate meeting and date. Bring all the folders to the meeting and document all the decisions in the patients’ notes. Remember to carry out the decisions after the meeting.
Surgical forum
Tuesday 08.00 to 09.00am. This meeting is compulsory. Various specialties present topics of interest. You may be required to present at a Tuesday morning meeting, but will be informed of this when needed.
M and M
Monthly M and M meetings are held on the last Tuesday of the month at 15:15 to 17.00. All to attend. Please remember to add all M and M details in the M and M file as soon as possible after the event.
WAG
The ‘Week at a Glance” meeting takes place in the ICH 6th floor board room. All of the following weeks operative cases are discussed, radiology reviewed and operative lists planned. Familiarize yourself with the files of the patients whose surgery you will be involved in and know the patient prior to the meeting! The D2 ward clerk will have all the folders ready mid-week. The operative list allocation of surgeons is done way in advance on the registrar time table.
Adobe
Friday 14.00 to 15.00
This is an on-line meeting hosted by our department 2 out of 4 weeks. It discusses various topics of paediatric surgical interest. You will be allocated a turn to present. The topic needs to be confirmed with Prof Numanoglu the week before for on-line advertising. The presentation needs to be 30 to 40 min long. There is opportunity for on-line polls which you can add to your presentation for the audience to vote. Both the presentation and the polls need to be loaded on the system by Prof Numanoglu the day before.
Other Tuesday meetings are taken up with Journal club, teaching and research. You will be allocated days to present at the M and M, Journal club as well as the teaching sessions. This roster is organized on a 3 month basis so there is no excuse not to be prepared. On no account are emergency cases to be booked during this time unless under exceptional circumstances.
Coding and Documentation
ICD 10 All out patients and inpatient cases need an ICD code. You will need to write the ICD 10 code on the yellow form on the front of the folder of every out patient. If the code does not exist on the laminated sheets available in OPD, then at the very least, write the diagnosis
ICD 9 All operations need ICD 9 codes written on the op note. This is not negotiable. There are hard copies of the ICD 9 codes available in the theater write up area as excel versions on the computers in this area
Consent Consents are audited. All details need to be on the consents including 2 witnesses and all sections filled in. All in correct consents are collected and reviewed each month in the theater committee meeting.
WHO Checklist This needs to be filled in for every patient. There are 3 sections, all need surgeon input, and the final one is a surgical signature. Do not forget this. These forms are also collected by management and audited.
Operation Notes All op notes need to be written in duplicate no matter how small the procedure. A carbon copy is added to the general surgical file in theater. All should have the procedure code written on top right corner. Copy left in the theatre folder is entered into the electronic database. Please write legibly!!
CLINICAL/OPERATIVE PHOTOS Please ask Dr Theron to give you access to the paediatric surgery pictures dropbox file. All pictures taken during your rotation here should be uploaded into this folder or relevant sub-folder. There is UCT wi-fi (eduroam) available in theatre and 7th floor ICH building library.
Teaching
Undergraduate:
The registrars from GSH are required to give 3 to 4 tutorials a week. This includes the basic surgical skills course on a Monday 14:00. There are 2 tutorials on a Thursday that are given by paediatric Surgery trainees or GSH registrars. These will be rostered on a tutorial roster in the first week of your time here.
Postgraduate:
Teaching occurs on the teaching ward round on Tuesdays at 14.00, in theater, at all the meetings detailed above, and with Professor Rode’s tutorials on a Thursday afternoon. The paediatric surgery trainees will be able to give you the topics for that week’s tutorials.
HELP!!
Never perform procedures you are unhappy with. There is always help around.
If there is a resus in the hospital and you are first on the scene, call switchboard and tell them there is a RED BOX and the location. Miraculously, people will materialize from all over the hospital to help. Likewise, if you hear the RED BOX call, you go to the relevant ward to help.
There are always at least 2 doctors in ICU, available for advice and help.
There is always a medical registrar or MO on call in the hospital.
Children are different to adults. Their physiology, tissue planes and surgical management is very different so even if you have performed certain procedures on adults there approach in children may differ so please consult your seniors and don’t extrapolate adult management. There is always help and advice around.
Important Points
There is a file present in ward D2. Please place all stickers of Morbidity and Mortality, Radiology meeting cases, Ward consults, Neonatal unit consults on the relevant pages. This file is used as a statistical basis to get the hospitals tertiary care grant, as well as an organizational base for M and M, and meeting organization.
At Red Cross, any anaethetist does the premeds, not necessarily the one doing the list. Discuss all cases for theatre with the consultant anaethetist the day before the case. That way there cannot be any surprises, and there is much smoother running of the list
Information Sheet for D2 Ward Rotating Registrars
The working day starts at 7am in D2 Ward. You will be expected to see, examine, write up fluids, orders and notes for the high care and second cubicle patients. The visiting paediatric surgical registrars will see some of these patients too. At 7.30am there is a consultant ward round. At 8am you may be asked to go theatre where the anaesthetists will be waiting for you eagerly so the slate can begin. Tell them you are there and ask them to start. There should be someone in theatre at 07.50 at the beginning of every slate so as to ensure a 08.00 start.
The ward registrar
The ward is very busy with an extremely high turnover. Because of this many tasks get overlooked. The interns need guidance, as most have not done paediatrics before, and it can be a very stressful job for them. All GSH rotating registrars will have a period of being allocated the ward registrar job. It is best to do it the week that you have a weekend call, so you know the patients well before the call, but this will not always be possible as the burns registrars also cover weekend calls. Your week will be allocated on the ‘duty’ roster. The role of the ward registrar is as follows.
Should stay to the end of the morning hand over round
To be first contact for the interns if they have any queries or problems in the ward
To assist the interns in organizing radiological investigations especially contrast investigations, CT and MRI’s
To do dictated discharge summaries on complex patients which will be allocated on discharge
To make sure all the pre-op patients are clerked by the interns before the afternoon ward round and that the appropriate pre operative tests are done and results present
To formulate a preliminary theatre booking list and hand it in to theatre by 14.00
When necessary, refer patients to anaesthetics
To consent the patients before the round. (The interns are not allowed to consent patients, and the senior registrars will take consent of the complex cases.)
To be on the afternoon ward round with the intern on call, the registrar on call and a senior registrar
All ward consultations
Take all day time surgical emergency calls
The compilation of the theatre slate is still the responsibility of the senior Paediatric Surgery Trainee. They are also ultimately responsible in checking that all patients are ready for theatre, and the relevant investigations have been done. Doing the ward registrars job does not preclude you from going to theatre or any teaching. If organized, it may take an hour or two a day. If you have any problems do not hesitate to call any senior for help.
Day Case Surgery
The GSH registrars will run the A7 day case theatre with help from one of the senior registrars or a consultant. This is where you will learn to do the most common paediatric surgical operations. You need to be in A7 at 7.45 to consent the patients and write the list.
Calls
Calls are either alone or with a senior registrar. You will do between a 1 in 4 to 1 in 5 call rota. There is no official post call, but if you have had a rough night, we do not mind if you take off early as long as your duties are covered, and you hand over. You will be the first on call. This means that you will receive all the referrals and see all the patients. These will then be discussed with the senior registrar on call if need be. Please do not hesitate to
call the senior registrar if you are unsure of anything. If patients need theatre, they need to be booked in theatre, consented and discussed with the senior registrar on call and anaesthetic consultant on call for the day. To start with, all operations should be done with a senior registrar present. As a general rule, no operations should be done after 12midnight unless it is a life or limb saving situation. If patients need to wait for theatre, make sure they are well resuscitated, have the appropriate antibiotics if needed and are relatively pain free. Make sure there appropriate fluids are also written up.
D2 Ward Rounds
7:30 Ward Round Every Day will begin with a department ward round at 07.30 The ward round will achieve the following objectives:-
Department notices and communication
Handover of all information on patients referred on the previous nights call
Ward round o Patient diagnosis, condition and concerns o Effective concise written and verbal nursing orders o Updating diagnosis and coding
Diagnostic problems highlighted
Theatre slates discussed
Bed issues discussed Prior to morning ward round Duties
All patients must be seen by a doctor prior to the meeting
Every patient must have notes, feeds and or fluids written up
Nursing orders must be written up on the patients whiteboard o This can be done at the time of seeing the patient or if in doubt after the morning round
Present patients seen
Interns to supervise students
ALL outliers in other wards to be seen prior to the meeting Allocation High Care1: Paediatric surgery senior registrar and Trainees High Care 2: GSH registrars All other cubicles: Interns and GSH registrars Outliers in other wards to be seen by interns – allocate one of you Paediatric surgery senior registrar running D2 will move through the ward seeing new admissions and see all patients briefly.
3. FORMATIVE ASSESSMENT AND EXAMINATION
1. Prior to your appointment you should have obtained your FCS Primary examination from
the Colleges of Medicine of SA (CMSA)
2. You will be eligible to write the FCS Intermediate examination of the CMSA when you have
Passed the Primary
Completed not less than 18 months of approved training in surgery, embracing trauma and intensive care and the surgical specialities. Of the 18 months training called for, not less than 6 months must be spent in general surgery, not less than 3 months must be spent in ICU and not less than 6 months must be spent in one or more of the surgical specialities (orthopaedics, urology, neurosurgery, paediatric surgery, cardiothoracic surgery, plastic and reconstructive surgery)
Obtained the ATLS Certificate
3. In order for you to be eligible to complete your FCS Final examination, you have to meet the
following requirements:
36 months in a numbered registrar training post.
Hard copy and electronic format of the Portfolio must be submitted together with a consolidation sheet.
Proof of submission of research component (Effective from 15 June 2012
applications).
4. At the end of each rotation, all registrars will complete an end-of-block oral examination
and consultant staff will evaluate the progress of each registrar. Satisfactory continuous
evaluation is necessary to allow a registrar to attempt CMSA examination.
5. Mmed evaluation: Please contact you supervisor for details and criteria
I think a surgeon is particularly suited by temperament to the short story form as opposed to the novel, because the short story i s rather like a surgical operation. It has a beginning, middle, and an end--at least my stories all do: you make an incision, you rummage around inside for a little while, then you stitch it up. Writing a short story is like taking out an inflamed appendix.... The act of making an incision is the creation of a wound for the purpose of healing the patient. The earliest forms of writing were exactly that: taking up a sharp rock and gouging out hieroglyphics in a flat stone--making wounds, as it were, to tell a story. The difference, of course, is that the surgical wound must heal, eventually, but the writer's wound does not. Richard Selzer
4. FCS INTERMEDIATE EXAMINATION: SYLLABUS AND TUTORIALS
CONSULTANT IN CHARGE: Dr Juan Klopper
After successful completion of a rotation through the Intensive Care Unit, registrars are allowed to
enter the College of Medicine’s Intermediate Exam in Surgery, which is held twice a year in various
academic centres in South Africa. This examination comprises two written multiple choice papers,
each of three hour duration. Successful candidates are invited for two 20 minute oral exams.
Preparation for the oral part of the examination is deemed very important and the training program
is designed specifically to help registrars in this preparation.
The program requires registrars to attend a two hour session from 18:00 every Thursday evening in
the Department. A set topic list is provided and registrars are urged to read up on the topic
beforehand. The aim of the program is to get the registrar comfortable with his or her own voice
and to learn to verbalize knowledge. The program also teaches answer skills such as construction,
body language, tone of voice, and most importantly, how to handle the difficult question and the
question to which the answer is not known.
From dress code to a deeper insight into the exam, this program now has a great history of success.
Participation will leave you with confidence and a sense of calm as you walk into the exam room.
A wise doctor does not mutter incantations over a sore that needs the knife. Sophocles Never let the skin stand between you and the diagnosis. The aim is to operate only when necessary but not to delay a necessary operation. -Moshe Schein-

5. FCS FINAL EXAMINATION: SYLLABUS AND TUTORIALS
The only weapon with which the unconscious patient can immediately retaliate upon the
incompetent surgeon is haemorrhage.William Stewart Halstead, 1852-1922
There are four degrees of intra-operative haemorrhage: 1. "Why did I get involved in this operation?"
2. "Why did I become a surgeon?" 3. "Why did I study to become a doctor?" 4. "Why was I born?".
Alexander A. Artemiev
6. OTHER COURSES AND REQUIREMENTS:
1. Laparoscopic lab work, logbook and course
2. Endoscopy course and logbook
3. DSTC Trauma Surgery course
4. Medical statistics
ENDOSCOPY
All new trainees (medical and surgical) planning on joining the endoscopy team for a rotation must please inform Dr Chinnery.
A trainee should ideally be able to commit to a 3 month period during which regular exposure on a weekly basis would be best as continuous training offers maximum benefit. At present there are 3 emergency scope lists run by the senior surgical consultants at GSH (Upper GI, Emergency Surgery, Surgical Oncology), and 2 by the senior medical gastrointestinal consultants. Further opportunity exists at New Somerset, Mitchell’s Plain and Victoria Hospitals, but this must be arranged independently with the consultants involved.
It would be very advisable for prospective trainees to complete the basic endoscopy course (next course 10/01/2014) before planning to start their training. This course will be held three times a year.
Registrars post-intermediates and on the senior rotations will be given preference should there be more than one eligible trainee per list.
The first 5 scopes will be observed and the trainee will learn and assist the GI nursing staff with the scope cleaning and processing in order to familiarise themselves with the equipment. Thereafter the trainee will be allowed to begin scoping under consultant supervision. No interventional endoscopy (excluding biopsies) will be allowed without a consultant in the room. The nursing staff are authorised to call the consultant to come and assist the trainee.
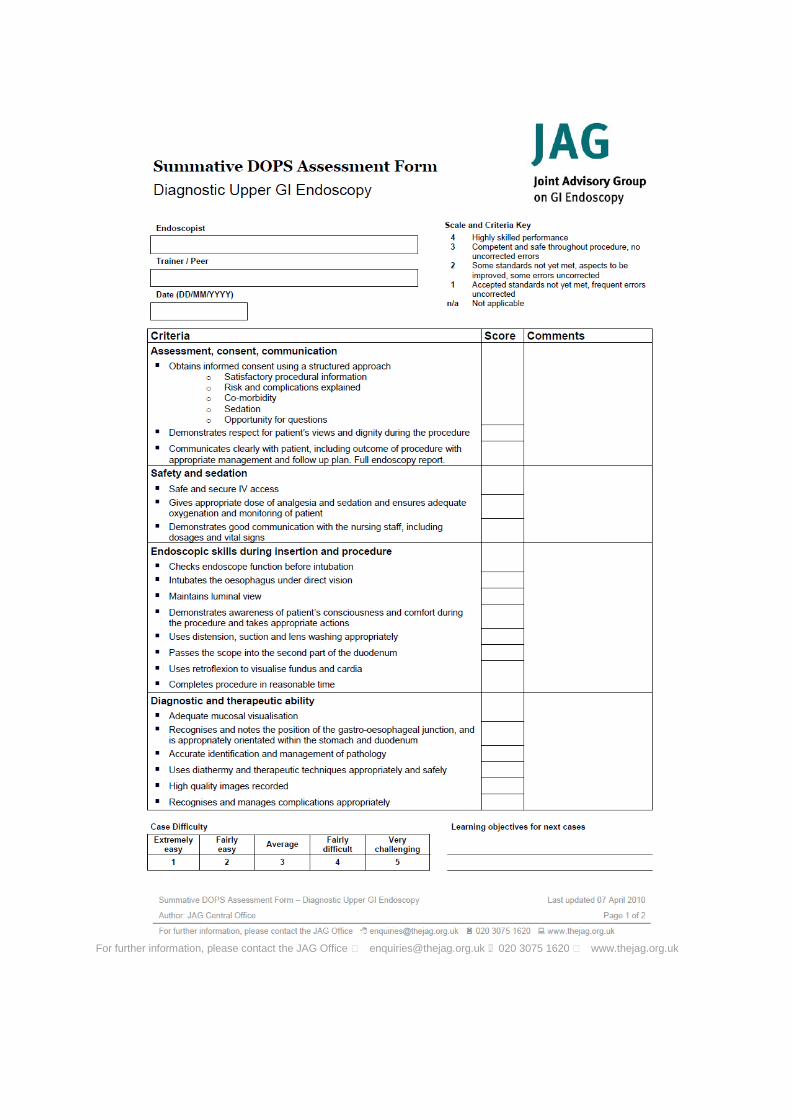
After every endoscopy list the trainee will be required to hand in a logbook, signed by the consultant responsible, to Ms Patton. Once 150 scopes have been performed by the trainee, he/she is to inform Dr Chinnery or Prof Thomson. At this point a formal DOPS assessment will take place, and if successful the trainee may be signed off to proceed with scopes unsupervised. Please take into consideration that training cannot disrupt service delivery.
If trainees have prior exposure to endoscopic training, they are welcome to have the DOPS assessment at the onset to evaluate if they may be excused from the endoscopic training program, and proceed to scoping on the emergency lists in E23. Should the initial DOPS assessment not be successful, a further 20 supervised scopes must be performed before a second DOPS assessment is attempted.
All trainees working in the endoscopy unit will be expected to have a basic understanding of and be familiar with common pathology and protocols used.
Junior consultants that are going to be training registrars will be required themselves to complete a DOPS assessment first. If junior consultants are inexperienced with interventions, they are please to ask for a senior endoscopist to be in the room supervising before they proceed.
Please be aware that due to the recent increase in equipment damage, with considerable expenses, only consultants will be allowed to perform after-hours endoscopy.
We hope that formalising the process will allow better exposure to training, allow all trainees to
rotate for 3 months at least once during their 4 years, allow for a better evaluation and overview of
the training offered by the unit, and ensure less equipment damage and a more pleasant working
environment for all.
Please direct any queries to Dr Chinnery.
Kind regards
Dr Galya Chinnery
Prof Sandie Thomson
Prof Jake Krige
Sr Mare van Wyk
For further information, please contact the JAG Office �[email protected] 020 3075 1620 �www.thejag.org.uk
7. Research and MMed
MEDICAL STATISTICS FOR THE BUSY CLINICIAN
Every registrar is obliged to complete a thesis for a Master’s degree in surgery during their training.
Although most registrars are or become familiar with the various topics in general surgery, it is the
methodology and statistical analysis of a research project that is probably the leading cause of
procrastination when it comes to completing a project. Although help with statistical analysis is
available, it remains important for every registrar to understand their own research and analysis.
Notwithstanding the requirement to complete a research project, medical statistics forms and
integral part of the required knowledge for all healthcare workers. It is impossible to critically
appraise the surgical literature without some understanding of statistics.
The course in medical statistics aims to explain medical statistics without the rigours involved in
mathematical statistics. Instead, the course makes use of over-the-counter software in the form of
Microsoft Excel to give every participant the tools and knowledge to get straight into analysing their
own data. The course runs over two days (Saturday and Sunday) and is organised on an ad hoc
basis.
MMED THESIS
Every registrar is required to complete a thesis for the purposes of obtaining in Master’s degree in
Surgery before completion of their FCS final examination. This requires planning and with the busy
four-year schedule, no time should be lost in getting your thesis completed.
The process involves the completion of various forms and documents, as well as adherence to the
policies and requirements of the University. To aid every registrar in this process a video is available
online, which explain the logistical necessities that you have to comply with. The link to the video is:
http://www.youtube.com/watch?v=dm1tVm06PLM&list=PLsu0TcgLDUiJf72OpNVKHQhbv9fBZaHZq
&index=1
8. Leave and relief policy
Guidelines and rules:
Annual registrar leave within the Department of Surgery 2014 1. Booking leave
• Leave requests are to be submitted, in writing, via email to [email protected] • Please use this email address always when requesting or querying leave: I am likely to
forget things if asked over the phone or in the passage, and can in any case seldom answer questions without consulting the roster, the master of which is on my computer.
• I will not be able to check and process requests on a daily basis – please be aware that I will update the leave and relief roster once a week granted that there is not a sudden crisis.
• Leave forms should be completed and handed in to Melissa van Harte at the beginning of each month. We will go through all the forms once a month and confirm the leave has been allocated on the roster.
• Prof Kahn will not sign forms not countersigned by either Prof Navsaria or myself. • Please be aware that registrars are generally not allowed leave during their ICU or Relief
rotations – although exceptions have been made in the past, this should please be avoided at all cost in the future. Attempts to plan the rotation further in advance will be made to help avoid this recurring problem.
• Book as far in advance as possible • The further in advance you book leave, the more likely you are to get your chosen
slot • Please be considerate to colleagues writing exams: if you are not writing, please try
to avoid requesting leave in the weeks preceding either a written or an oral exam, so that these slots can be used for study leave.
• The leave request form has been designed to encourage people to plan and book their leave in advance. I recognize that this is not always possible but strongly encourage you to do so.
2. How much leave?
• Per person: • 22 days per annum: this applies to supernumerary registrars as well. In order for the
rotations to run smoothly, it is important that we can all count on each other to play by the same rules. That said, I am open to discuss personal dilemmas and special circumstances – life does not always play by the rules. It is important that we know that we are able, as a department, to pull together and make a plan to accommodate each other.
• Please try to use all your allocated leave each year: it becomes progressively more difficult to accommodate carry-over leave
• If there is a query regarding how much leave a registrar has due to him/her, the onus is on the registrar to obtain the relevant documentation from HR.
• In a row: • Registrars should not take more than 11 working days of leave at a time, except in special
circumstances.
• These circumstances need to be discussed with Prof Navsaria. • How many registrars at a time?
• The relief rotation is currently only able to provide relief for 3-4 registrars at a time, HOWEVER:
• There are too many registrars to provide relief to everyone and certain rotations might have to function without relief for certain periods of time.
3. Rotations to which relief is not routinely sent
• These include: • Transplant • Endoscopy/Upper GI • Mitchellsplain (may occasionally require relief) • C14 (may occasionally require relief)
• In times of crisis, registrars in endoscopy and transplant may be called upon to cover calls in
poorly staffed rotations, or to leave their rotation to join one that is short staffed. 4. Study leave
• Registrars writing final exams are permitted study leave: for every day of annual leave put in, they will receive an extra day of study leave, up to a maximum of seven days (ie: 7 days of annual leave gets 7 days of study leave; 10 days of annual leave only gets 7 days of study leave)
• This leave must be taken within three months of the written paper • The application for leave must be accompanied by the letter from the College confirming your
acceptance into the exam • If the leave slots are already full for the requested period, the leave will not be granted. • Registrars are thus encouraged to book study leave as early as possible, to avoid frustration. • Registrars writing intermediate exams only qualify for two days of study leave for the written
and one day for the oral exam. This department has a very flexible leave policy. Please try to respect the above guidelines, and also to be considerate to your colleagues, so that the policy can remain that way. If you are called on to help out in a time of shortage or crises, please try to keep in mind that we have a responsibility – not only to the system we work in but maybe more importantly, to each other – you never know when you might be the one that needs the support of your colleagues. BOOK EARLY, COMMUNICATE CLEARLY, HAVE A LITTLE PATIENCE – and hopefully we will all be able to get the break we need! Warm regards. Liana Roodt (76455)

MEMO : ALL GENERAL SURGICAL REGISTRARS
SUBJECT : LEAVE ALLOCATION FOR 2014
FROM : LIANA ROODT
DATE : 30 October 2014
Please complete the following form as soon as possible and email back to [email protected]
before 30/11/2014
- Please note that exam candidates will get preference.
- If you are not writing exams, please do not request leave during March/
May/August/October.
- For the ease of planning the rotation and leave, please indicate when you aim
to write intermediates or finals ( e.g March 2014/ Aug 2015 etc)
Leave should be in blocks of 2 weeks, preferably starting on the 1st or 16th of the month. Please make
sure that you take 2 weeks between February – July and 2 weeks between August-January 2015. If
you fail to request 2 separate blocks of leave, PLEASE NOTE THAT YOUR LEAVE CANNOT BE
GUARANTEED and that you risk loosing some of your leave days.
Should several people request the same slot, leave will be allocated based on seniority and a first-
come-first-serve basis. For this reason I have included a 1st choice and 2nd choice request on the
form.
Warm regards.
Liana
Name :______________________________________
I am planning to write exams …………………………………………
Period of Leave requested:
1st Choice FEB-JULY ___________________________AUG –JAN………………………………………..
2nd Choice : FEB-JULY __________________________AUG-JAN…………………………………………..
9. SASSiT – SA SOCIETY FOR SURGEONS IN TRAINING
Mission
The society will provide a platform to improve surgical training by:
Providing opportunities for both knowledge and technical skills transfer from the vast number of
South African surgical experts;
Providing a voice for the opinions and concerns of all surgical trainees through our
representation on the College of Surgeons’ council
And at the Association of Surgeons of South Africa (ASSA);
By becoming proactive about the changes affecting surgical training and the practice of surgery
in South Africa.
SASSIT is a society for all surgical trainees run by trainees!
The SASSiT Executive Committee represents YOU at national forums. We are included in policy
making and are part of the evolving landscape of Surgery in South Africa.
Membership Benefits
As a SASSiT member you are an associate member of ASSA. This entitles you to FREE access to
SAJS, BJS and Annals of Surgery. (www.surgeon.co.za)
Registrar symposium – hosted annually
FCS (SA) Intermediate Exam Preparation Course – hosted bi-annually
FCS (SA) Final Exam Preparation Course
SASSiT discounted rates for members to attend congresses
Travel grants:
- 25 x R5000 awarded by ASSA to attend their annual congress
- SASSiT Travel Grant
Updates on national academic events on Facebook & Twitter
Free copy of SAJS posted to you monthly
Spesnet Research Methodology and Advanced Research Courses to assist with your MMed
preparation
ASSA/SASSiT scrubs, manufactured by TANC – delivered at no extra cost to your university.
Becoming a member
Membership fees for 2014: R380
Apply online: www.sassit.co.za










![Shrinking Lung Syndrome: A Pulmonary Manifestation of ... · scan]) and pulmonary function tests (PFTs). Pulmonary function tests were carried out in our pulmonary function laboratory,](https://static.fdocuments.net/doc/165x107/5f03189c7e708231d40783f1/shrinking-lung-syndrome-a-pulmonary-manifestation-of-scan-and-pulmonary-function.jpg)