These slides were released by the speaker for internal use by Novartis

Inhaled Nitric Oxide in Congenital Diaphragmatic Hernia
Neil Patel Neonatologist
Royal Hospital for Sick Children, Glasgow
iNO 26th March 2015

iNO 26th March 2015

• Pathophysiology of PH in CDH
• PH therapies in CDH – iNO and friends
• Rationalising neonatal management in CDH
iNO 26th March 2015

CDH babies everywhere in world
iNO 26th March 2015

Congenital Diaphragmatic Hernia
• 3.5 per 10,000 pregnancies
• Defect in developing diaphragm – 85% left sided
• Herniation of abdominal contents into fetal chest
iNO 26th March 2015

iNO 26th March 2015

iNO 26th March 2015

Pulmonary artery pressure and outcome in CDH
A second group consisted of 8 patients (17%) that
showed persistent systemic or suprasystemic pulmonary
artery pressure ratios (ratios 1.0) despite all attempts at
clinical management including nitrous oxide, ECMO,
and surgery (group 2). Even with veno-arterial ECMO,
the estimated pressures remained grossly abnormal over
time. In this group there were no survivors.
The third group was made up of 16 infants (34%) with
moderately elevated pressure ratios ranging from 0.5 to
0.9. In this group, 12 survived (75%), and 4 died. Seven
of the 12 survivors required ECMO support. The median
length of time to reach pulmonary artery pressure ratios
less than 0.5 in this group was 49 days.
Examining the survivors as a group, 46% had pulmo-
nary artery pressure ratios less than 0.5 within the first
week of life, and 66% reached this level within the first
3 weeks. One third of the survivors had elevated pulmo-
nary to systemic artery pressure ratios beyond 3 weeks of
therapy (Fig 3). By 2 and Fisher’s Exact test methods,
systemic ratios were associated with decreased survival
at all time-points when compared with normal-pressure
survivors. Within the first week of life, 60% of the
infants with systemic pulmonary artery pressure ratios
survived (P .003). By the third week, only 38% of
infants with systemic pulmonary artery pressures sur-
vived (P .007), and by the sixth week, there were no
survivors with systemic pulmonary artery pressure ratios
(P .02; Table 1).
ECMO support was required in 23 infants (49%). In
group I, 5 of 23 infants (22%) were placed on ECMO,
and all survived. In group III patients with intermediate
ratios, 11 of 16 (69%) required ECMO, and 7 survived
(64%). In group II patients with persistent systemic or
suprasystemic ratio estimates, all of the infants qualified
for ECMO support, and none survived (Table 2).
DISCUSSION
The clinical course of pulmonary hypertension and its
relationship to outcome in patients with congenital dia-
phragmatic hernia has never been documented in a large
study. The importance of pulmonary hypertension in
ultimately determining survival rates has always been
recognized, but establishing the boundary between re-
versible pulmonary hypertension and irreversible pulmo-
nary hypoplasia has been impossible clinically. To this
end, the acceptance and utilization of current clinical
treatments—delayed surgical repair, permissive hyper-
carbia, extracorporeal membrane oxygenation, and nitric
oxide—are strategies aimed at manipulating pulmonary
artery pressure and the pathophysiology associated with
its abnormal elevation.
The data presented in this report show that in the
context of current treatment strategies, CDH outcomes
can be divided into 3 clinical groups based on serial
echocardiographic analyses of pulmonary artery pressure
estimates. Almost half of all CDH patients will resolve
their pulmonary hypertension within the first 3 weeks of
life without a significant need for ECMO, and survival
rate in this group can be expected to approach 100%. A
smaller group of patients will show persistent systemic
or suprasystemic pulmonary pressures despite every at-
tempt to manage such pressures including nitric oxide,
high-frequency oscillation, ECMO, and delayed surgical
repair—or any combination of these interventions. Such
pressure profiles over time have been unresponsive to
Fig 2. Pulmonary artery pressure ratio and survival.
Fig 3. Time course of resolution of pulmonary hypertension in all
survivors
Table 1. Survival Rate with Pulmonary Artery Pressure Ratio > 1.0
(Systemic or Supra-Systemic)
Week % P value
1 60 .003
3 38 .007
6 0 .02
Table 2. Relationship of PAP:SAP Ratios to ECMO Use and Survival
Group No. of Patients (%) Survival (%)
I (PAP:SAP 0.5) 5 (22) 100
III (PAP:SAP 0.5-0.9) 11 (69) 64
II (PAP:SAP 1.0) 7 (100) 0
Total 23 (49)
309PULMONARY ARTERY PRESSURE AND SURVIVAL IN CDH
Dillon et al, J Ped Surg 39 (3), 2004: 307-312
iNO 26th March 2015

Pulmonary vasculature in CDH
CDH Control
iNO 26th March 2015
Yamataka and Puri, J Ped Surg 32 (3), 1997, 387-390

iNO 26th March 2015

Pathophysiology of pulmonary hypertension
PULMONARY HYPERTENSION
RIGHT TO LEFT SHUNTING
• Within lungs • atrial septum • patent ductus
iNO 26th March 2015

Pathophysiology of pulmonary hypertension
PULMONARY HYPERTENSION
REDUCED LV FILLING RIGHT TO LEFT SHUNTING
• Within lungs • atrial septum • patent ductus
REDUCED LV OUTPUT
iNO 26th March 2015

Pathophysiology of pulmonary hypertension
PULMONARY HYPERTENSION
REDUCED LV FILLING RIGHT TO LEFT SHUNTING
• Within lungs • atrial septum • patent ductus
REDUCED LV OUTPUT “CARDIAC FAILURE”
INCREASED RV
AFTERLOAD
iNO 26th March 2015

Normal RV structure and function
iNO 26th March 2015

iNO 26th March 2015

RV hypertrophy and effect on LV
iNO 26th March 2015

RV function
iNO 26th March 2015

Tissue Doppler imaging (TDI)
• Uses pulse wave Doppler to measure myocardial velocities as assessment of myocardial function
• Allows separate assessment of systolic (contractile) and diastolic (lusitropic) function
iNO 26th March 2015

Normal pulse wave TDI (PWTDI)
iNO 26th March 2015
IVV: Isovolumic contraction velocity
S: Systolic ejection velocity
E’: Early diastolic veloctiy (active relaxation)
A’: Late diastolic velocity (atrial contraction)

Pulse wave tissue Doppler in CDH
iNO 26th March 2015
Control infant CDH with PH
• Reduced systolic velocities (IVV and S)
• Loss of diastolic E’ velocity
• Abnormal “post-systolic contraction” *
* * *

iNO 26th March 2015
Pulse wave tissue Doppler in CDH

RV function in CDH
• Impaired early diastolic relaxation
• Impaired systolic contraction
iNO 26th March 2015

iNO 26th March 2015

Cardiac failure in CDH
• RV early diastolic and systolic dysfunction • RV dilatation and hypertrophy
– secondary myocardial ischaemia • LV compression and secondary dysfunction • Variable response to elevated PA pressure
iNO 26th March 2015

iNO 26th March 2015

Pathophysiology of PH in CDH
PULMONARY HYPERTENSION
REDUCED LV FILLING RIGHT TO LEFT SHUNTING
Intrapulmonary atrial septum patent ductus
REDUCED LV OUTPUT BIVENTRICULAR FAILURE
INCREASED AFTERLOAD
RV DIASTOLIC DYSFUNCTION AND DILATATION
HYPOXAEMIA HYPOTENSION HYPOPERFUSION ACIDOSIS
iNO 26th March 2015

Pathophysiology of PH in CDH
PULMONARY HYPERTENSION
REDUCED LV FILLING RIGHT TO LEFT SHUNTING
atrial septum and
patent ductus REDUCED LV OUTPUT BIVENTRICULAR
FAILURE
INCREASED AFTERLOAD
RV DIASTOLIC DYSFUNCTION AND DILATATION
HYPOXAEMIA HYPOTENSION HYPOPERFUSION ACIDOSIS
CLINICAL OUTCOMES iNO 26th March 2015

iNO 26th March 2015 PCCM October 2013

iNO 26th March 2015 PCCM October 2013
Copyright © 2013 by the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies.Unauthorized reproduction of this article is prohibited
Neonatal Intensive Care
Pediatric Critical Care Medicine w w w .p c c m jo u rn a l.o rg 5
correlated with functional class and a reduced RV E′ predicted
adverse long-term outcome (10). The potential importance of
RV function as a predictor of outcome in CDH specifically is
supported by a recent study by Egan et al (14), who observed
that TDI RV E′ and S′ are impaired in long-term survivors up
to 6 years after CDH repair in the newborn period.
Insufficient antenatal data were available in this study to
allow comparison of TDI RV E′ to existing prenatal predictors
of outcome (observed to expected lung-head ratio and MR
fetal lung volumes) (15–17). Further studies are required to
compare TDI RV E′ with these and other postnatal measures,
including pulmonary artery diameter (e.g., McGoon Index)
and physiologic indices, which have previously been reported
to predict mortality in CDH (18, 19). The small cohort size
and incomplete data in the nonsurvivor group also prevented
meaningful investigation of the relationship between TDI
measures (including RV E′d1–2
) and survival. This will be an
interesting area for further study. However, with increasing
survival in CDH, as in our cohort, future interest is likely to
be in prediction of not only survival but also clinical severity,
early and long-term outcomes.
Does measuring RV function confer any benefit to measuring
PAP alone in CDH? Preoperative PSR has been demonstrated to
predict survival in CDH (20). We now additionally observed that
preoperative PSR also correlates with early outcome in survivors.
However, PSR unlike RV TDI was not measureable in 43% of
infants, due to the absence of TR. Furthermore, in the first 48
hours of life, only RV E′ correlated with outcome but PSR did
not. Nor did PSR as a measure of PAH correlate with RV func-
tion. This highlights the variable response of the RV to PAH but
also points to a key central role of RV function rather than abso-
lute PAP in determining illness severity and outcome in CDH.
This critical relationship between RV function and clinical
status was supported by our observation that RV E′ was lower
in those infants with more severe disease (requiring longer
respiratory therapy). This supports a potential critical role of
the RV in CDH pathophysiology in determining pulmonary
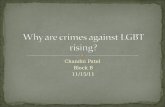
Figure 2. Correlation between averaged right ventricular early diastolic myocardial velocity on days 1 and 2 of lif e (RV E′
d1–2) and duration of
respiratory support (DRS). Receiver-operating characteristics curve for the prediction of DRS more than 21 days using RV E′
d1–2 Filled circle =
individual subject data point (RV E′d1-2
and DRS for each of 16 subjects).
Figure 3. Receiver-operating characteristics curve for the prediction of DRS more than 21 days using right ventricular early diastolic myocardial velocity on days 1 and 2 of lif e (RV E′
d1–2). An averaged RV E′
d1–2 less
than 4.6 cm/ s predicted duration of respiratory support more than 21 days with 100% sensitivity and 8 8% specificity (area under the curve = 0.9 6; SE = 0.04; 95% CI, 0.88–1.05; p = 0.002).
TABLE 2. Correlation Between Echocardiographic and Outcome Measures
Variable
Correlation
RV E′ Length of Stay Duration of Respiratory Support
r p r p r p
RV E′d1–2
–0.75 0.002 –0.84 0.0001
RV S′d1–2
–0.04 0.89 –0.19 0.50
PSRd1–2
a 0.17 0.68 0.28 0.46 0.49 0.19
RV E′preoperative
–0.39 0.19 –0.36 0.22
RV S′preoperative
0.22 0.47 0.14 0.65
PSRpreoperative
a 0.25 0.52 0.75 0.03 0.76 0.02
′ ′ = right ventricular systolic myocardial velocity, PSR = pulmonary:systemic peak pressure ratio.aPSR data obtained in n = 9 infants only, not measurable in remaining infants.
Copyright © 2013 by the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies.Unauthorized reproduction of this article is prohibited
Neonatal Intensive Care
Pediatric Critical Care Medicine w w w .p c c m jo u rn a l.o rg 5
correlated with functional class and a reduced RV E′ predicted
adverse long-term outcome (10). The potential importance of
RV function as a predictor of outcome in CDH specifically is
supported by a recent study by Egan et al (14), who observed
that TDI RV E′ and S′ are impaired in long-term survivors up
to 6 years after CDH repair in the newborn period.
Insufficient antenatal data were available in this study to
allow comparison of TDI RV E′ to existing prenatal predictors
of outcome (observed to expected lung-head ratio and MR
fetal lung volumes) (15–17). Further studies are required to
compare TDI RV E′ with these and other postnatal measures,
including pulmonary artery diameter (e.g., McGoon Index)
and physiologic indices, which have previously been reported
to predict mortality in CDH (18, 19). The small cohort size
and incomplete data in the nonsurvivor group also prevented
meaningful investigation of the relationship between TDI
measures (including RV E′d1–2
) and survival. This will be an
interesting area for further study. However, with increasing
survival in CDH, as in our cohort, future interest is likely to
be in prediction of not only survival but also clinical severity,
early and long-term outcomes.
Does measuring RV function confer any benefit to measuring
PAP alone in CDH? Preoperative PSR has been demonstrated to
predict survival in CDH (20). We now additionally observed that
preoperative PSR also correlates with early outcome in survivors.
However, PSR unlike RV TDI was not measureable in 43% of
infants, due to the absence of TR. Furthermore, in the first 48
hours of life, only RV E′ correlated with outcome but PSR did
not. Nor did PSR as a measure of PAH correlate with RV func-
tion. This highlights the variable response of the RV to PAH but
also points to a key central role of RV function rather than abso-
lute PAP in determining illness severity and outcome in CDH.
This critical relationship between RV function and clinical
status was supported by our observation that RV E′ was lower
in those infants with more severe disease (requiring longer
respiratory therapy). This supports a potential critical role of
the RV in CDH pathophysiology in determining pulmonary
Figure 2. Correlation between averaged right ventricular early diastolic myocardial velocity on days 1 and 2 of lif e (RV E′
d1–2) and duration of
respiratory support (DRS). Receiver-operating characteristics curve for the prediction of DRS more than 21 days using RV E′
d1–2 Filled circle =
individual subject data point (RV E′d1-2
and DRS for each of 16 subjects).
Figure 3. Receiver-operating characteristics curve for the prediction of DRS more than 21 days using right ventricular early diastolic myocardial velocity on days 1 and 2 of lif e (RV E′
d1–2). An averaged RV E′
d1–2 less
than 4.6 cm/ s predicted duration of respiratory support more than 21 days with 100% sensitivity and 8 8% specificity (area under the curve = 0.9 6; SE = 0.04; 95% CI, 0.88–1.05; p = 0.002).
TABLE 2. Correlation Between Echocardiographic and Outcome Measures
Variable
Correlation
RV E′ Length of Stay Duration of Respiratory Support
r p r p r p
RV E′d1–2
–0.75 0.002 –0.84 0.0001
RV S′d1–2
–0.04 0.89 –0.19 0.50
PSRd1–2
a 0.17 0.68 0.28 0.46 0.49 0.19
RV E′preoperative
–0.39 0.19 –0.36 0.22
RV S′preoperative
0.22 0.47 0.14 0.65
PSRpreoperative
a 0.25 0.52 0.75 0.03 0.76 0.02
′ ′ = right ventricular systolic myocardial velocity, PSR = pulmonary:systemic peak pressure ratio.aPSR data obtained in n = 9 infants only, not measurable in remaining infants.

iNO 26th March 2015

RV diastolic function is associated with adverse outcome in CDH
Early RV function appears to be a better predictor of outcome than PAP
RV function, rather than absolute PAp may determine outcome in CDH
iNO 26th March 2015

Patterns of PH and RV function in CDH
0
2
4
6
8
10
12
Age 2 3 4 6 7 8 9 10 14 16 18 19 20 21 22 23 24 26 28 33 35 36 37 37.5 39 43 44 47 51 60
RV S
RV E
ECMO weaning iNO + cardiotropes off
iNO + cardiotropes
extubation
repair
weaning sedation
Sepsis
0
1
2
3
4
Age 2 3 4 6 7 8 9 10 14 16 18 19 20 21 22 23 24 26 28 33 35 36 37 37.5 39 43 44 47 51 60
PDA flow ratio Rl:Lr
R->L
L->R
iNO 26th March 2015

RV function in the first week of life in CDH
• RV diastolic velocities can stratify illness severity • RV early diastolic velocities increase from day 1-2 to day 3-4
iNO 26th March 2015
Moenkemeyer & Patel, PCCM October 2013

RV function after CDH repair
• In more severely affected infants RV early diastolic velocities are
lower at day 3-4 post op
iNO 26th March 2015
Moenkemeyer & Patel, PCCM October 2013

TREATMENT OF PH in CDH
iNO 26th March 2015

TREATMENT OF PH IN CDH
INCREASED PVR
REDUCED LV FILLING RIGHT TO LEFT SHUNTING
atrial septum and
patent ductus REDUCED LV OUTPUT BIVENTRICULAR
FAILURE
RV DIASTOLIC DYSFUNCTION AND DILATATION
HYPOXAEMIA HYPOTENSION HYPOPERFUSION ACIDOSIS
CLINICAL OUTCOMES iNO 26th March 2015

Pulmonary vasodilator therapies in CDH
iNO 26th March 2015

Pulmonary vasodilator therapies in CDH
iNO 26th March 2015

iNO and oxygenation in CDH
iNO 26th March 2015

Haemodynamic effects of iNO in CDH
iNO 26th March 2015

RCTs iNO in CDH
NINOS study (1997) • 53 subjects, > 34 weeks, <14 days
• iNO at 20ppm, increased to max 80ppm
• Used hyperventilation, no standardization of ventilation
Clark et al (2000) • >34 weeks, < 4 days
• Inclusion at OI >25, randomization at OI>40
• iNO weaned to 5ppm after 24 hours, for max 96 hours
iNO 26th March 2015

iNO 26th March 2015
Analysis 1.13. Comparison 1 Inhaled NO versus control, Outcome 13 Bayley PDI more than 2 SD below the
mean.
Review: Nitric oxide for respiratory failure in infantsborn at or near term
Comparison: 1 Inhaled NO versuscontrol
Outcome: 13 Bayley PDI more than 2 SD below the mean
Study or subgroup Treatment Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95%CI M-H,Fixed,95%CI
Davidson 1997 2/35 16/94 34.4 % 0.34 [ 0.08, 1.39 ]
Ninos1996 9/75 17/79 65.6 % 0.56 [ 0.27, 1.17 ]
Total (95% CI) 110 173 100.0 % 0.48 [ 0.25, 0.94 ]
Total events: 11 (Treatment), 33 (Control)
Heterogeneity: Chi2 = 0.40, df = 1 (P= 0.53); I2 =0.0%
Test for overall effect: Z = 2.16 (P= 0.031)
0.1 0.2 0.5 1 2 5 10
Favours treatment Favours control
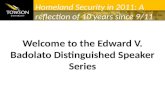
Analysis 2.1. Comparison 2 Inhaled NO versus control in infants with diaphragmatic hernia, Outcome 1
Death or need for ECMO.
Review: Nitric oxide for respiratory failure in infantsborn at or near term
Comparison: 2 Inhaled NO versuscontrol in infantswith diaphragmatic hernia
Outcome: 1 Death or need for ECMO
Study or subgroup iNO Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95%CI M-H,Fixed,95%CI
Ninos1997 24/25 23/28 60.3 % 1.17 [ 0.97, 1.41 ]
Clark 2000 12/13 17/18 39.7 % 0.98 [ 0.81, 1.19 ]
Total (95% CI) 38 46 100.0 % 1.09 [ 0.95, 1.26 ]
Total events: 36 (iNO), 40 (Control)
Heterogeneity: Chi2 = 1.77, df = 1 (P= 0.18); I2 =43%
Test for overall effect: Z = 1.25 (P= 0.21)
0.5 0.7 1 1.5 2
Favors iNO Favors control
35Nitric oxide for respiratory failure in infants born at or near term (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Nitric oxide for respiratory failure in infants born at or near
term (Review)
Finer N, Barrington KJ
Thisisareprint of aCochranereview, prepared and maintained byTheCochraneCollaboration and published in TheCochraneLibrary
2006, Issue4
http://www.thecochranelibrary.com
Nitric oxide for respiratory failure in infants born at or near term (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Nitric oxide for respiratory failure in infants born at or near
term (Review)
Finer N, Barrington KJ
Thisisareprint of aCochranereview, preparedandmaintained byTheCochraneCollaboration andpublished in TheCochraneLibrary
2006, Issue4
http://www.thecochranelibrary.com
Nitric oxide for respiratory failure in infants born at or near term (Review)
Copyright © 2009 The Cochrane Collaboration. Published by JohnWiley & Sons, Ltd.

iNO 26th March 2015
Nitric oxide for respiratory failure in infants born at or near
term (Review)
Finer N, Barrington KJ
Thisisareprint of aCochranereview, prepared and maintained byTheCochraneCollaboration and published in TheCochraneLibrary
2006, Issue4
http://www.thecochranelibrary.com
Nitric oxide for respiratory failure in infants born at or near term (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Nitric oxide for respiratory failure in infants born at or near
term (Review)
Finer N, Barrington KJ
Thisisareprint of aCochranereview, preparedandmaintained byTheCochraneCollaboration andpublished in TheCochraneLibrary
2006, Issue4
http://www.thecochranelibrary.com
Nitric oxide for respiratory failure in infants born at or near term (Review)
Copyright © 2009 The Cochrane Collaboration. Published by JohnWiley & Sons, Ltd.
“Infants with diaphragmatic hernia do not appear to share the benefit of iNO; indeed ……outcomes may be worse in infants with CDH who received inhaled NO compared to controls.”

iNO 26th March 2015
• 57% of infants received iNO
• INO use ranged from 34-92%
• Peak iNO use on day 2 (38%)
• 48% iNO pre op, 40% iNO post op
• Age at iNO: 11%>30days, 3% >60days

Why are we using (more!) iNO in CDH?
• Limitations of existing RCTs – conducted in older treatment eras
– Small populations
– Short durations of treatment
– Didn’t account for variable patterns / timing of PH in CDH
• INO may improve oxygenation and haemodynamics and buy time e.g. for ECMO or for repair of CDH
• iNO may be more effective in combination with new therapies
iNO 26th March 2015

iNO 26th March 2015

Sildenafil
• PDE-5 inhibitor
• Oral preparations introduced first to allow weaning of iNO
• IV preparation now available
iNO 26th March 2015

iNO 26th March 2015

iNO 26th March 2015
• 2005-2012, single centre experience
• 112 CDH infants • 19 (17%) discharged on oral
sildenafil
Pediatric Cardiology 2013

iNO 26th March 2015

iNO 26th March 2015

Milrinone: “inodilator”
iNO 26th March 2015
Lakshminrusimha and Steinhorn, PCCM 2013
• Pulmonary vasodilator
• Improved diastolic function (lusitropy)
• Improved systolic function (inotropy)
• (systemic vasodilatation)

iNO 26th March 2015
Fax +41 61 306 12 34E-Mail [email protected]
Original Paper
Neonatology 2012;102:130–136
DOI: 10.1159/000339108
Use of Milrinone to Treat Cardiac Dysfunction in Infants with Pulmonary Hypertension Secondary to Congenital Diaphragmatic Hernia:A Review of Six Patients
Neil Patel
Royal Children’s Hospital, Melbourne, Vic. , Australia
there was a significant increase in early diastolic myocardial
velocities in the RV, accompanied by increasing systolic ve-
locities in the RV and IVS. Oxygenation index was significant-
ly reduced, blood pressure unchanged, and ductal shunt ve-
locity minimally altered over the same time period. Conclu-
sions: Milrinone use was associated with an improvement in
systolic and diastolic function in the RV, corresponding to an
improvement in clinical status.
Copyright © 2012 S. Karger AG, Basel
Introduction
In infants with pulmonary hypertension (PHT), in-cluding those with congenital diaphragmatic hernia (CDH), elevated pulmonary vascular resistance increases afterload on the right ventricle (RV) leading to systolic and diastolic ventricular dysfunction [1, 2] . Milrinone is a phosphodiesterase-3 inhibitor which has been proposed to be of benefit in this setting. The rationale for the use of milrinone is threefold: as a direct pulmonary vasodilator, as an inotrope to improve systolic function, and as a lu-sitropic agent to improve diastolic function [3] . In infants with persistent PHT of the newborn, milrinone has been demonstrated to improve oxygenation index (OI) [4] .
Key Words
Pulmonary hypertension Congenital diaphragmatic
hernia Milrinone Phosphodiesterase 3 inhibitor
Newborn infants Tissue Doppler imaging
Abstract
Background: Pulmonary hypertension and secondary car-
diac dysfunction are important contributors of morbidity
and mortality in infants with congenital diaphragmatic her-
nia (CDH). Milrinone, a phosphodiesterase-3 inhibitor, may
be useful in this setting for its combined actions as a pulmo-
nary vasodilator and to improve systolic and diastolic func-
tion. Objectives: This study aimed to assess the effects of
milrinone on cardiac function and pulmonary artery pres-
sure in infants with CDH. Methods: A retrospective review of
echocardiograms performed on infants with CDH who re-
ceived milrinone was performed. Tissue Doppler imaging
velocities were used to assess systolic and diastolic function.
Pulmonary artery pressure was assessed from the pattern
and velocity of ductal shunting. Results: Six infants with
CDH and severe pulmonary hypertension were identified.
Systolic and diastolic myocardial velocities were reduced in
the right ventricle (RV) and interventricular septum (IVS) at
baseline. In the 72 h after commencement of milrinone,
Received: February 7, 2012
Accepted after revision: April 10, 2012
Published online: June 16, 2012
Dr. Neil Patel, BA, MB ChB, MRCPCH, MD Royal Children’s Hospital Flemington Road Melbourne, VIC 3052 (Australia) Tel. +61 3 9345 5008 or +61 413 417 011, E-Mail nei l.patel @ rch.org.au
© 2012 S. Karger AG, Basel1661–7800/12/1022–0130$38.00/0
Accessible online at:www.karger.com/neo
Fax +41 61 306 12 34E-Mail [email protected]
Original Paper
Neonatology 2012;102:130–136
DOI: 10.1159/000339108
Use of Milrinone to Treat Cardiac Dysfunction in Infants with Pulmonary Hypertension Secondary to Congenital Diaphragmatic Hernia:A Review of Six Patients
Neil Patel
Royal Children’s Hospital, Melbourne, Vic. , Australia
there was a significant increase in early diastolic myocardial
velocities in the RV, accompanied by increasing systolic ve-
locities in the RV and IVS. Oxygenation index was significant-
ly reduced, blood pressure unchanged, and ductal shunt ve-
locity minimally altered over the same time period. Conclu-
sions: Milrinone use was associated with an improvement in
systolic and diastolic function in the RV, corresponding to an
improvement in clinical status.
Copyright © 2012 S. Karger AG, Basel
Introduction
In infants with pulmonary hypertension (PHT), in-cluding those with congenital diaphragmatic hernia (CDH), elevated pulmonary vascular resistance increases afterload on the right ventricle (RV) leading to systolic and diastolic ventricular dysfunction [1, 2] . Milrinone is a phosphodiesterase-3 inhibitor which has been proposed to be of benefit in this setting. The rationale for the use of milrinone is threefold: as a direct pulmonary vasodilator, as an inotrope to improve systolic function, and as a lu-sitropic agent to improve diastolic function [3] . In infants with persistent PHT of the newborn, milrinone has been demonstrated to improve oxygenation index (OI) [4] .
Key Words
Pulmonary hypertension Congenital diaphragmatic
hernia Milrinone Phosphodiesterase 3 inhibitor
Newborn infants Tissue Doppler imaging
Abstract
Background: Pulmonary hypertension and secondary car-
diac dysfunction are important contributors of morbidity
and mortality in infants with congenital diaphragmatic her-
nia (CDH). Milrinone, a phosphodiesterase-3 inhibitor, may
be useful in this setting for its combined actions as a pulmo-
nary vasodilator and to improve systolic and diastolic func-
tion. Objectives: This study aimed to assess the effects of
milrinone on cardiac function and pulmonary artery pres-
sure in infants with CDH. Methods: A retrospective review of
echocardiograms performed on infants with CDH who re-
ceived milrinone was performed. Tissue Doppler imaging
velocities were used to assess systolic and diastolic function.
Pulmonary artery pressure was assessed from the pattern
and velocity of ductal shunting. Results: Six infants with
CDH and severe pulmonary hypertension were identified.
Systolic and diastolic myocardial velocities were reduced in
the right ventricle (RV) and interventricular septum (IVS) at
baseline. In the 72 h after commencement of milrinone,
Received: February 7, 2012
Accepted after revision: April 10, 2012
Published online: June 16, 2012
Dr. Neil Patel, BA, MB ChB, MRCPCH, MD Royal Children’s Hospital Flemington Road Melbourne, VIC 3052 (Australia) Tel. +61 3 9345 5008 or +61 413 417 011, E-Mail neil.patel @ rch.org.au
© 2012 S. Karger AG, Basel1661–7800/12/1022–0130$38.00/0
Accessible online at:www.karger.com/neo
Fax +41 61 306 12 34E-Mail [email protected]
Original Paper
Neonatology 2012;102:130–136
DOI: 10.1159/000339108
Use of Milrinone to Treat Cardiac Dysfunction in Infants with Pulmonary Hypertension Secondary to Congenital Diaphragmatic Hernia:A Review of Six Patients
Neil Patel
Royal Children’s Hospital, Melbourne, Vic. , Australia
there was a significant increase in early diastolic myocardial
velocities in the RV, accompanied by increasing systolic ve-
locities in the RV and IVS. Oxygenation index was significant-
ly reduced, blood pressure unchanged, and ductal shunt ve-
locity minimally altered over the same time period. Conclu-
sions: Milrinone use was associated with an improvement in
systolic and diastolic function in the RV, corresponding to an
improvement in clinical status.
Copyright © 2012 S. Karger AG, Basel
Introduction
In infants with pulmonary hypertension (PHT), in-cluding those with congenital diaphragmatic hernia (CDH), elevated pulmonary vascular resistance increases afterload on the right ventricle (RV) leading to systolic and diastolic ventricular dysfunction [1, 2] . Milrinone is a phosphodiesterase-3 inhibitor which has been proposed to be of benefit in this setting. The rationale for the use of milrinone is threefold: as a direct pulmonary vasodilator, as an inotrope to improve systolic function, and as a lu-sitropic agent to improve diastolic function [3] . In infants with persistent PHT of the newborn, milrinone has been demonstrated to improve oxygenation index (OI) [4] .
Key Words
Pulmonary hypertension Congenital diaphragmatic
hernia Milrinone Phosphodiesterase 3 inhibitor
Newborn infants Tissue Doppler imaging
Abstract
Background: Pulmonary hypertension and secondary car-
diac dysfunction are important contributors of morbidity
and mortality in infants with congenital diaphragmatic her-
nia (CDH). Milrinone, a phosphodiesterase-3 inhibitor, may
be useful in this setting for its combined actions as a pulmo-
nary vasodilator and to improve systolic and diastolic func-
tion. Objectives: This study aimed to assess the effects of
milrinone on cardiac function and pulmonary artery pres-
sure in infants with CDH. Methods: A retrospective review of
echocardiograms performed on infants with CDH who re-
ceived milrinone was performed. Tissue Doppler imaging
velocities were used to assess systolic and diastolic function.
Pulmonary artery pressure was assessed from the pattern
and velocity of ductal shunting. Results: Six infants with
CDH and severe pulmonary hypertension were identified.
Systolic and diastolic myocardial velocities were reduced in
the right ventricle (RV) and interventricular septum (IVS) at
baseline. In the 72 h after commencement of milrinone,
Received: February 7, 2012
Accepted after revision: April 10, 2012
Published online: June 16, 2012
Dr. Neil Patel, BA, MB ChB, MRCPCH, MD Royal Children’s Hospital Flemington Road Melbourne, VIC 3052 (Australia) Tel. +61 3 9345 5008 or +61 413 417 011, E-Mail neil.patel @ rch.org.au
© 2012 S. Karger AG, Basel1661–7800/12/1022–0130$38.00/0
Accessible online at:www.karger.com/neo

iNO 26th March 2015

Rationalising therapies in CDH
• Understanding of pathogenesis of PH in CDH
• Multiple pulmonary vasodilators + inodilators
• Some evidence of haemodynamic benefits
• Lack of RCT support
iNO 26th March 2015

A rationale approach…
iNO 26th March 2015

(Early) RV dysfunction / hypertrophy
INCREASED PVR
Severity and survival
iNO 26th March 2015
hypoxia LVO / BP

(Early) RV dysfunction / hypertrophy
INCREASED PVR
Severity and survival
iNO 26th March 2015
hypoxia LVO / BP
REARLY AND REGULAR ASSESSMENT

(Early) RV dysfunction / hypertrophy
INCREASED PVR
iNO 26th March 2015
hypoxia LVO / BP
REARLY AND REGULAR ASSESSMENT
TARGETED, SYSTEMATIC, EARLY
THERAPY
REDUCED SEVERITY IMPROVED SURVIVAL

Clinical assessment of PH and RV function
• Simple
• Quantifiable
• Accurate
iNO 26th March 2015

Echocardiography
iNO 26th March 2015

iNO 26th March 2015
Fax +41 61 306 12 34E-Mail [email protected]
Original Paper
Neonatology 2008;94:22–30
DOI: 10.1159/000112641
N-Terminal-pro-B Type Natriuretic Peptide as a Useful Tool to Evaluate Pulmonary Hypertension and Cardiac Function in CDH Infants
Maria J. Baptistaa, c Gustavo Rocha a Fátima Clementea Luís F. Azevedo b
Dick Tibboel d Adelino F. Leite-Moreira b Hercília Guimarães a José C. Areias a
Jorge Correia-Pinto a, c
a Divisions of Pediatric Cardiology, Neonatology and Pediatric Surgery, Department of Pediatrics,
Hospital S. João, b Serviços de Fisiologia, Bioestatistica e Informática Médica, Faculdade de Medicina da
Universidade do Porto, Porto , and c Life and Health Sciences Research Institute, School of Health Sciences, University
of Minho, Braga , Portugal; d Department of Pediatric Surgery, Erasmus Medical Center,
Sophia Children’s Hospital, Rotterdam , The Netherlands
ly correlated with estimated pulmonary artery pressure,
right ventricular Tei index, and tricuspid E/A ratio. Addition-
ally, we found that CDH infants with NT-proBNP 1 11,500 pg/
ml experienced a worse prognosis. Conclusions: We dem-
onstrated that PH is associated with NT-proBNP elevation
and diastolic impairment in CDH infants. Early elevations in
NT-proBNP levels seem to alert for a subset of CDH infants
with worse prognosis. Copyright © 2007 S. Karger AG, Basel
Introduction
Despite many advances in the management of con-genital diaphragmatic hernia (CDH), the outcome of af-fected infants remains unpredictable and varies from year to year even in experienced teams with predeter-mined treatment protocols. Its morbidity and mortality is largely dependent of pulmonary hypertension (PH) and hypoplasia [1] . Pulmonary hypoplasia installs during prenatal development [2–4] and limited possibilities exist to attenuate it [5, 6] . PH is likely secondary to pulmonary
Key Words
N-terminal-pro-B type natriuretic peptide Congenital
diaphragmatic hernia Pulmonary hypertension
Cardiac function Diastole
Abstract
Objective: In congenital diaphragmatic hernia (CDH) the se-
verity of pulmonary hypertension (PH) is considered, by sev-
eral authors, determinant of clinical outcome. Plasmatic N-
terminal-pro-B type natriuretic peptide (NT-proBNP) might
be useful in diagnosis and management of PH in newborns,
although its interest in CDH infants remains to be defined.
Early NT-proBNP levels were assessed in CDH infants and
correlated with cardiovascular echocardiographic parame-
ters. Patients and Methods: 28 newborns, CDH and age-
matched controls were enrolled in a prospective study. Clin-
ical condition, NT-proBNP plasmatic levels, echo parameters
of PH and biventricular function were assessed at 24 h after
delivery as well as survival outcome. Results: Estimated
mean pulmonary pressure and NT-proBNP were significant-
ly higher in CDH than control infants. NT-proBNP significant-
Received: June 4, 2007
Accepted after revision: September 24, 2007
Published online: December 21, 2007
formerly Biology of the Neonate
Maria João Baptista Escola de Ciências da Saúde, Universidade do Minho Campus de Gualtar, CPII (piso 3) PT–4709-057 Braga (Portugal) Tel. +351 253 604 807, Fax +351 253 604 831, E-Mail [email protected]
© 2007 S. Karger AG, Basel1661–7800/08/0941–0022$24.50/0
Accessible online at:www.karger.com/neo
Fax +41 61 306 12 34E-Mail [email protected]
Original Paper
Neonatology 2008;94:22–30
DOI: 10.1159/000112641
N-Terminal-pro-B Type Natriuretic Peptide as a Useful Tool to Evaluate Pulmonary Hypertension and Cardiac Function in CDH Infants
Maria J. Baptistaa, c Gustavo Rocha a Fátima Clementea Luís F. Azevedo b
Dick Tibboel d Adelino F. Leite-Moreira b Hercília Guimarães a José C. Areias a
Jorge Correia-Pinto a, c
a Divisions of Pediatric Cardiology, Neonatology and Pediatric Surgery, Department of Pediatrics,
Hospital S. João, b Serviços de Fisiologia, Bioestatistica e Informática Médica, Faculdade de Medicina da
Universidade do Porto, Porto , and c Life and Health Sciences Research Institute, School of Health Sciences, University
of Minho, Braga , Portugal; d Department of Pediatric Surgery, Erasmus Medical Center,
Sophia Children’s Hospital, Rotterdam , The Netherlands
ly correlated with estimated pulmonary artery pressure,
right ventricular Tei index, and tricuspid E/A ratio. Addition-
ally, we found that CDH infants with NT-proBNP 1 11,500 pg/
ml experienced a worse prognosis. Conclusions: We dem-
onstrated that PH is associated with NT-proBNP elevation
and diastolic impairment in CDH infants. Early elevations in
NT-proBNP levels seem to alert for a subset of CDH infants
with worse prognosis. Copyright © 2007 S. Karger AG, Basel
Introduction
Despite many advances in the management of con-genital diaphragmatic hernia (CDH), the outcome of af-fected infants remains unpredictable and varies from year to year even in experienced teams with predeter-mined treatment protocols. Its morbidity and mortality is largely dependent of pulmonary hypertension (PH) and hypoplasia [1] . Pulmonary hypoplasia installs during prenatal development [2–4] and limited possibilities exist to attenuate it [5, 6] . PH is likely secondary to pulmonary
Key Words
N-terminal-pro-B type natriuretic peptide Congenital
diaphragmatic hernia Pulmonary hypertension
Cardiac function Diastole
Abstract
Objective: In congenital diaphragmatic hernia (CDH) the se-
verity of pulmonary hypertension (PH) is considered, by sev-
eral authors, determinant of clinical outcome. Plasmatic N-
terminal-pro-B type natriuretic peptide (NT-proBNP) might
be useful in diagnosis and management of PH in newborns,
although its interest in CDH infants remains to be defined.
Early NT-proBNP levels were assessed in CDH infants and
correlated with cardiovascular echocardiographic parame-
ters. Patients and Methods: 28 newborns, CDH and age-
matched controls were enrolled in a prospective study. Clin-
ical condition, NT-proBNP plasmatic levels, echo parameters
of PH and biventricular function were assessed at 24 h after
delivery as well as survival outcome. Results: Estimated
mean pulmonary pressure and NT-proBNP were significant-
ly higher in CDH than control infants. NT-proBNP significant-
Received: June 4, 2007
Accepted after revision: September 24, 2007
Published online: December 21, 2007
formerly Biology of the Neonate
Maria João Baptista Escola de Ciências da Saúde, Universidade do Minho Campus de Gualtar, CPII (piso 3) PT–4709-057 Braga (Portugal) Tel. +351 253 604 807, Fax +351 253 604 831, E-Mail [email protected]
© 2007 S. Karger AG, Basel1661–7800/08/0941–0022$24.50/0
Accessible online at:www.karger.com/neo

iNO 26th March 2015
Plasma vascular endothelial growth factor A and placental growth factor: novel biomarkers of pulmonary hypertension in congenital diaphragmatic hernia
Neil Patel , Florian Moenkemeyer , Susie Germano , Michael M. H. Cheung
AJP Lung Feb 2015

iNO 26th March 2015
Regu
lar assessmen
t of p
ulm
on
ary pressu
re & card
iac (RV
) fun
ction
BIRTH
Discharge and beyond

iNO 26th March 2015
Regu
lar assessmen
t of p
ulm
on
ary pressu
re & card
iac (RV
) fun
ction
BIRTH
Discharge and beyond
First line:
Evidence of effects of PH: HYPOXIA / BP / RV dysfunction
Optimise ventilation, sedation, acid-base, Ca/Mg, sepsis

iNO 26th March 2015
Regu
lar assessmen
t of p
ulm
on
ary pressu
re & card
iac (RV
) fun
ction
BIRTH
Discharge and beyond
Second line:
hypoxia RV dysfunction
First line:
Evidence of effects of PH: HYPOXIA / BP / RV dysfunction
Optimise ventilation, sedation, acid-base, Ca/Mg, sepsis

iNO 26th March 2015
Regu
lar assessmen
t of p
ulm
on
ary pressu
re & card
iac (RV
) fun
ction
BIRTH
Discharge and beyond
Second line:
hypoxia RV dysfunction
Worsening hypoxia or RV dysfunction
Third line:
First line:
Evidence of effects of PH: HYPOXIA / BP / RV dysfunction
Optimise ventilation, sedation, acid-base, Ca/Mg, sepsis

iNO 26th March 2015
Regu
lar assessmen
t of p
ulm
on
ary pressu
re & card
iac (RV
) fun
ction
BIRTH
Discharge and beyond
Second line:
hypoxia RV dysfunction
First line:
Evidence of effects of PH: HYPOXIA / BP / RV dysfunction
Optimise ventilation, sedation, acid-base, Ca/Mg, sepsis
PGE1 to maintain PDA if PAP>SBP / PDA closing / RV dilated

iNO 26th March 2015
Regu
lar assessmen
t of p
ulm
on
ary pressu
re & card
iac (RV
) fun
ction
BIRTH
Discharge and beyond
Second line:
hypoxia RV dysfunction
Worsening hypoxia or RV dysfunction
Third line:
First line:
Evidence of effects of PH: HYPOXIA / BP / RV dysfunction
Optimise ventilation, sedation, acid-base, Ca/Mg, sepsis
PGE1 to maintain PDA if PAP>SBP / PDA closing / RV dilated
BP First line: Treat PH
Dopamine (max 10 mcg/kg/min)
-hydrocortisone -low dose Adr (if LV fx) -low dose NA (if SVR)
BP
BP

Targeted timing of procedures inc surgery
0
2
4
6
8
10
12
Age 2 3 4 6 7 8 9 10 14 16 18 19 20 21 22 23 24 26 28 33 35 36 37 37.5 39 43 44 47 51 60
RV S
RV E
ECMO weaning iNO + cardiotropes off
iNO + cardiotropes
extubation
repair
0
1
2
3
4
Age 2 3 4 6 7 8 9 10 14 16 18 19 20 21 22 23 24 26 28 33 35 36 37 37.5 39 43 44 47 51 60
PDA flow ratio Rl:Lr
R->L
L->R
iNO 26th March 2015

A new RCT?
iNO 26th March 2015
Early and regular assessment of PAp and cardiac (RV) function
Targeted: • Systematic pulmonary vasodilator
/ cardiotrope use.
• Timing of procedures: surgery, weaning, extubation
Newborn with CDH
CONTROL (current therapy)
OUTCOMES: DEATH, ECMO, DISABILITY
VS.

iNO 26th March 2015
Morgan, Farah Eaton, Jason R. Dyck, Stephen L. Archer and Bernard ThébaudDon Walker, Kathryn G. Todd, Pierre Gressens, Zamaneh Kassiri, Khurram Nadeem, Beverly Christina Luong, Juliana Rey-Perra, Arul Vadivel, Greg Gilmour, Yves Sauve, Debby Koonen,
Congenital Diaphragmatic HerniaAntenatal Sildenafil Treatment Attenuates Pulmonary Hypertension in Experimental
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2011 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/CIRCULATIONAHA.108.845909
2011;123:2120-2131; originally published online May 2, 2011;Circulation.
http://circ.ahajournals.org/content/123/19/2120
World Wide Web at: The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on April 8, 2014http://circ.ahajournals.org/Downloaded from by guest on April 8, 2014http://circ.ahajournals.org/Downloaded from

Take home message
iNO 26th March 2015

iNO 26th March 2015

iNO 26th March 2015

iNO 26th March 2015
Staff and patients of the : Royal Hospital for Sick Children, Glasgow Royal Children’s Hospital, Melbourne Murdoch Childrens Research Institute Florian Moenkemeyer Michael Cheung Michael Stewart Joanne Behrsin Anja Bialkowski John Mills
Thanks to