TKI discontinuation in CML
14
TKI Discontinuation in CML Udomsak Bunworasate King Chulalongkorn Memorial Hospital Chulalongkorn University
Transcript of TKI discontinuation in CML

TKI Discontinuation in CML
Udomsak BunworasateKing Chulalongkorn Memorial Hospital
Chulalongkorn University

BCR/ABL Tyrosine Kinase Inhibitors (TKI)
ImatinibGlivec, STI-571 Dasatinib
Sprycel, BMS-354825
NilotinibTasigna, AMN-107
• Survival of CML pts. who respond to treatment is close to the healthy population. • TKI discontinuation in responded pts. has been proposed due to - Economic impact of treating patients during lifetime - Quality of life, long-term tolerability/toxicity (esp. in younger pts.)

Discontinuation Studies in CML-CP • Imatinib N
– STIM 100– STIM2200– ALLG CML8 (TWISTER) 40– A-STIM 80– EUROSKI 200 (planned 700)
• Nilotinib/Dasatinib N– STOP 2G-TKI 50– ENESTfreedom 175– ENESTop 117– ENESTpath 1058– DASFREE ~74 Mahon et al. Ann Hematol 2015,94:S187-93

To stop imatinib, it is necessary to achieve and sustain very low level of residual disease
Michor F et al. Nature 2005, 435:1267-70 Mahon et al. ASH 2013 [abstract 255]


Study Rx before Response for Definition of relapse TFR % discontinuation discontinuation (median f/U)
STIM1 IFN->I* for MR4.5 for ≥2 yrs Loss ofMMR or ≥1-log 40 % (55mos) ≥3 yrs or increase in BCR-ABL
STIM2 I for ≥3 yrs MR4.5 for ≥2 yrs Loss ofMMR or ≥1-log 46 %at 2 yrsor increase in BCR-ABL
ALLG CML8 I for ≥3 yrs MR4.5 for ≥2 yrs Loss of MMR or confirmed 42.7 % (42 mos)(TWISTER) loss of MR4.5
A-STIM I for ≥3 yrs MR4.5 for ≥2 yrs Loss of MMR 64 % (23 mos)
EUROSKI I, N*, D* MR4 for ≥1 yr Loss of MMR 61 % at 6 mos.(in progress)
STOP 2G-TKI N, D CMR for median Loss of MMR 61.1 %29 mos (preliminary)
Discontinuation Studies in CML-CP
I=Imatinib, N=Nilotinib, D=DasatinibMahon et al. Ann Hematol 2015,94:S187-93

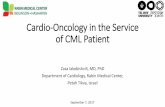
TWISTER
FREQUENT AND SUSTAINED DRUG-FREE REMISSION IN THE AUSTRALASIAN CML8 TRIAL OF
IMATINIB WITHDRAWAL
Median follow-up of 42 months (range 15 – 72)
Ross et al. Blood 2013;122(4):515-22

Sustained CMR for at least 2 yrs is of major importance in TKI discontinuation
78%
15%
p = 0.0002
Takahashi et al. Haematologica 2012; 97(6): 903-6

Study Rx before Response for Definition of relapse TFR % discontinuation discontinuation (median f/U)
STIM1 IFN->I* for MR4.5 for ≥2 yrs Loss ofMMR or ≥1-log 40 % (55mos) ≥3 yrs or increase in BCR-ABL
STIM2 I for ≥3 yrs MR4.5 for ≥2 yrs Loss ofMMR or ≥1-log 46 %at 2 yrsor increase in BCR-ABL
ALLG CML8 I for ≥3 yrs MR4.5 for ≥2 yrs Loss of MMR or confirmed 42.7% (42 mos)(TWISTER) loss of MR4.5
A-STIM I for ≥3 yrs MR4.5 for ≥2 yrs Loss of MMR 64 % (23 mos)
EUROSKI I, N*, D* MR4 for ≥1 yr Loss of MMR 61 % at 6 mos.(in progress)
STOP 2G-TKI N, D CMR for median Loss of MMR 61.1 %29 mos (preliminary)
Discontinuation Studies in CML-CP
I=Imatinib, N=Nilotinib, D=DasatinibMahon et al. Ann Hematol 2015,94:S187-93

“According to STIM” (A-STIM)Loss of MMR As a Trigger for Restarting Imatinib
• Enrolled patients with MR4.5 or UMRD for ≥ 2 years on imatinib • After discontinuation, loss of MMR was used as the criteria for
restarting imatinib • All patients who re-initiated imatinib therapy after a loss of MMR
regained MR4.5 after a median of 7.3 months of treatment
Relapse-free Survival by Relapse Criteria
50
25
0
Perc
ent R
elap
se-fr
ee (%
)
0 6 12 18 24 30 36 42 48
Months
54 60 66 72 78 84 90 96
100
75
P < .0001
Without loss of MMR: 63.7%
STIM criteria*: 38.1%
Without loss of CMR: 26.5%
*Two consecutive increasing values of detectable MRD
Rousselot et al. Haematologica. 2012;97(s1): 77 [abstract 194].Rousselot et al . J Clin Oncol 2014;32:424-430

• In the STIM study, a fluctuation in BCR-ABL transcript was detected in 5 of the 39 without confirmed molecular relapse.
Mahon et al. Lancet Oncol 2010; 11: 1029–35
Fluctuation of BCR-ABL detection after discontinuation

BCR-ABL DNA evidence of residual disease in patients with UMRD
Ross DM et al. Blood 2013;122(4):515-22.


Conclusion
• Around 40% of CML pts. with stable deep molecular response for at least 2 yrs. are likely to remain in prolonged TFR after treatment discontinuation
• The rate is around 60% if the loss of MMR is the criteria of molecular recurrence
• In most cases, TKI discontinuation needs to be done under a clinical trial with close molecular monitoring
• A long-term follow-up of the discontinuation studies will be necessary to affirm cure