tigullio cardiologiatigulliocardio.com/2014/ppt/Fumagalli_3_4.pdf · SOD Cardiologia e Medicina...
31
ICD e CRT nel grande anziano: come regolarsi ? S. Fumagalli, Firenze SOD Cardiologia e Medicina Geriatrica, AOU Careggi e Università di Firenze Quando l’evidenza dai trial è insufficiente: il grande anziano tigullio cardiologia 2014 3-4 aprile Santa Margherita Ligure
-
Upload
nguyenxuyen -
Category
Documents
-
view
217 -
download
0
Transcript of tigullio cardiologiatigulliocardio.com/2014/ppt/Fumagalli_3_4.pdf · SOD Cardiologia e Medicina...

ICD e CRT nel grande anziano: come regolarsi ? S. Fumagalli, Firenze
SOD Cardiologia e Medicina Geriatrica, AOU Careggi e Università di Firenze
Quando l’evidenza dai trial è insufficiente: il grande anziano
tigullio cardiologia 2014
3-4 aprile Santa Margherita Ligure
20-39 40-59 60-79 >80
Perc
ent o
f Pop
ulat
ion
Age (years) 65-74 75-84 >85
Per 1
000
Pers
on Y
ears
Age (years)
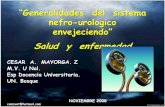
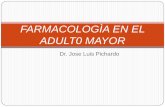
Prevalence of HF National Health and Nutrition
Examination Survey
Incidence of HF Framingham Heart Study
Heart Disease and Stroke Statistics—2012 Update A Report From the American Heart Association
Roger VL, 2012
Men
Speranza di vita alla nascita (2011) Uomini – 79.4 anni Donne – 84.5 anni Speranza di vita a 65 anni (2011) Uomini – 18.4 anni ! 83.4 anni Donne – 21.9 anni ! 86.9 anni http://demo.istat.it/altridati/indicatori/2011/Tab_5.pdf
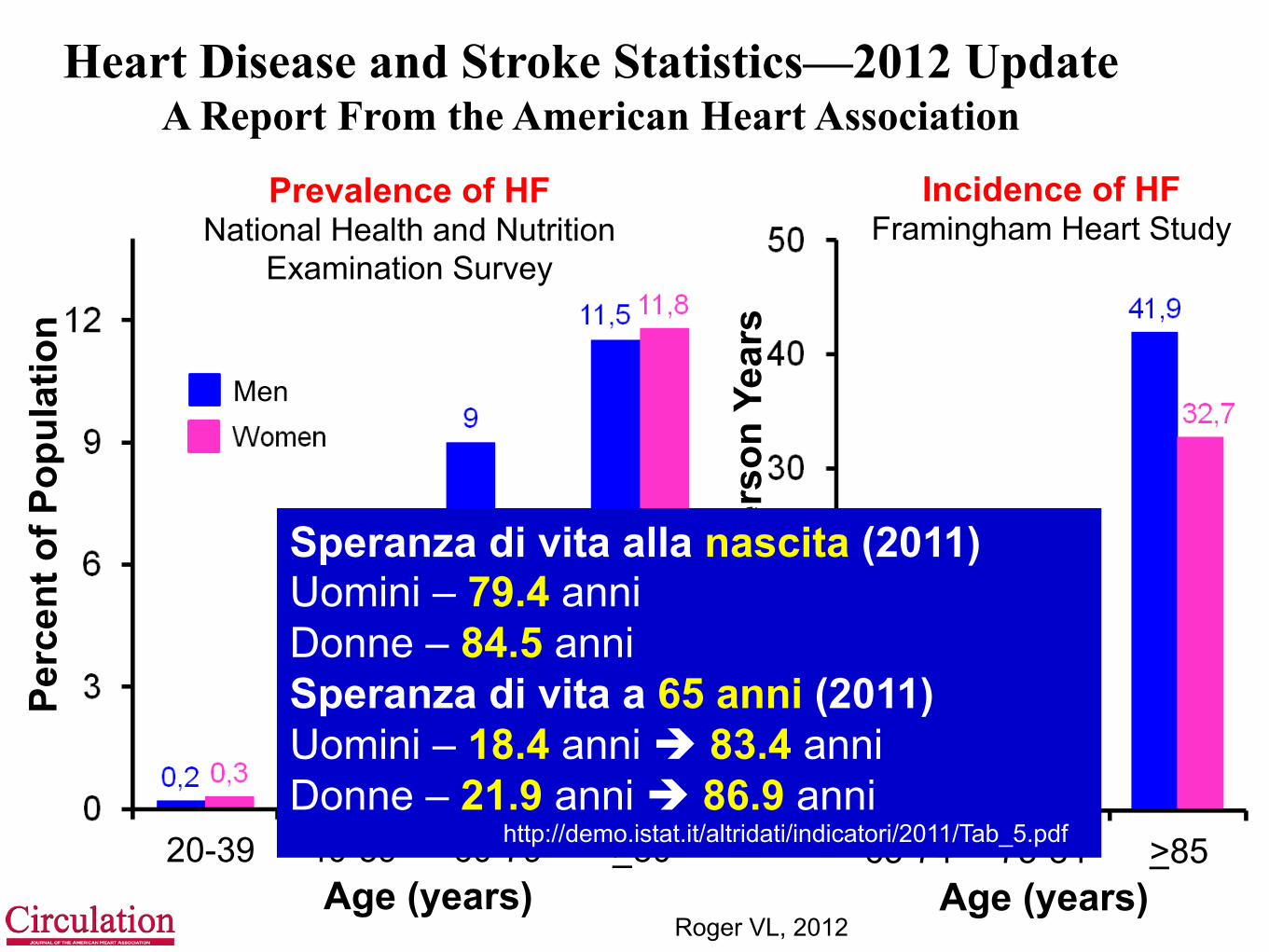
! Despite the compelling findings from several CRT trials, it must be recognized that patients enrolled in these studies were highly selected
! Specifically, few patients >75 were enrolled … ! Thus, RCT evidence for efficacy of CRT in patients
>75 years is lacking and, as previously noted, extrapolation of data from trials in much younger patients to the very elderly may not be justified due to age-related alterations in both the risks (higher) and benefits (potentially lower) in older patients
2011
Età media dei principali trial sugli ICD MADIT (1996) – 63 anni MUSTT (1999) – 66 anni MADIT II (2002) – 64 anni DEFINITE (2004) – 58 anni SCD-HeFT (2005) – 60 anni
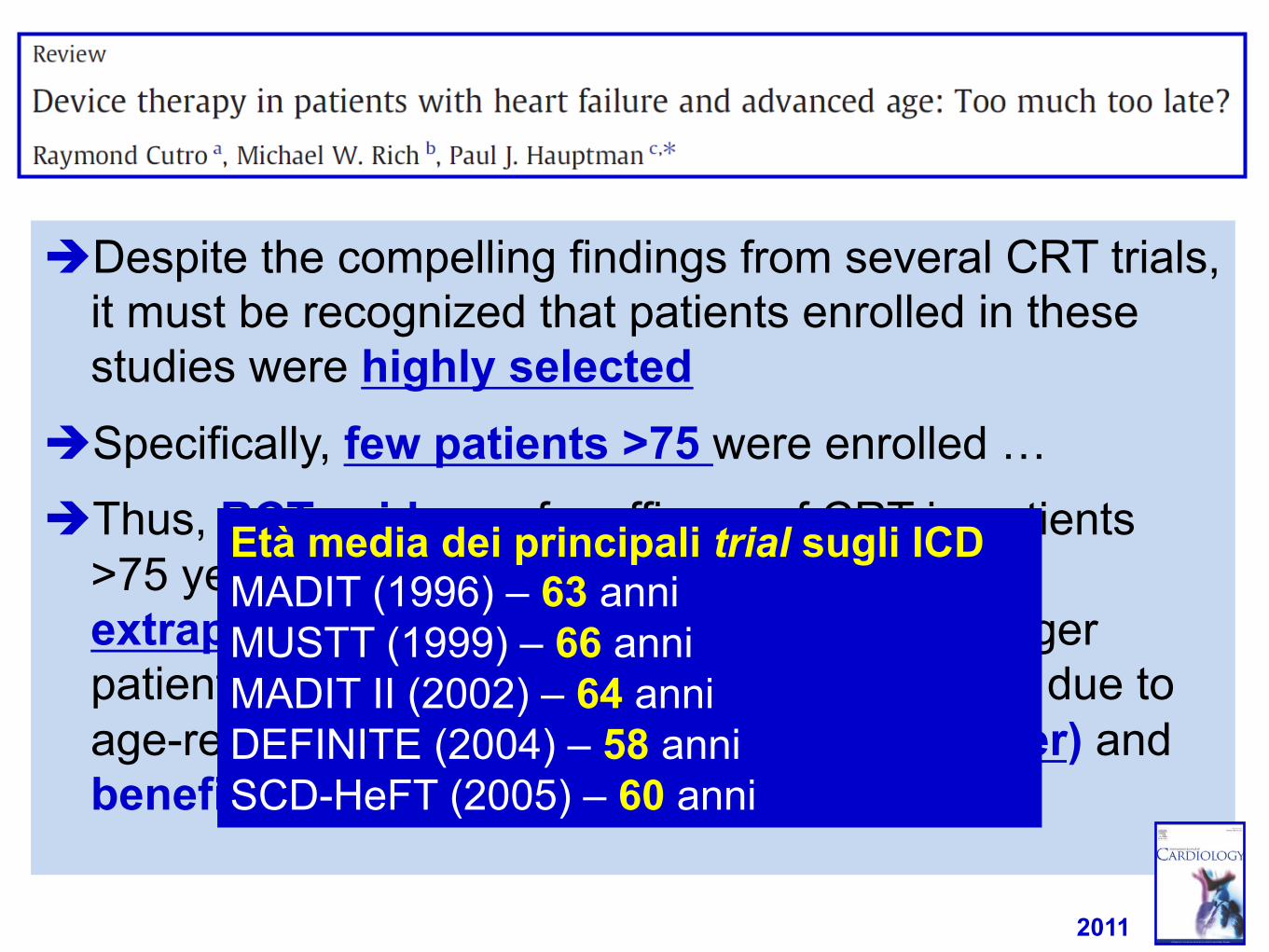
Al-Khatib SM, 2013
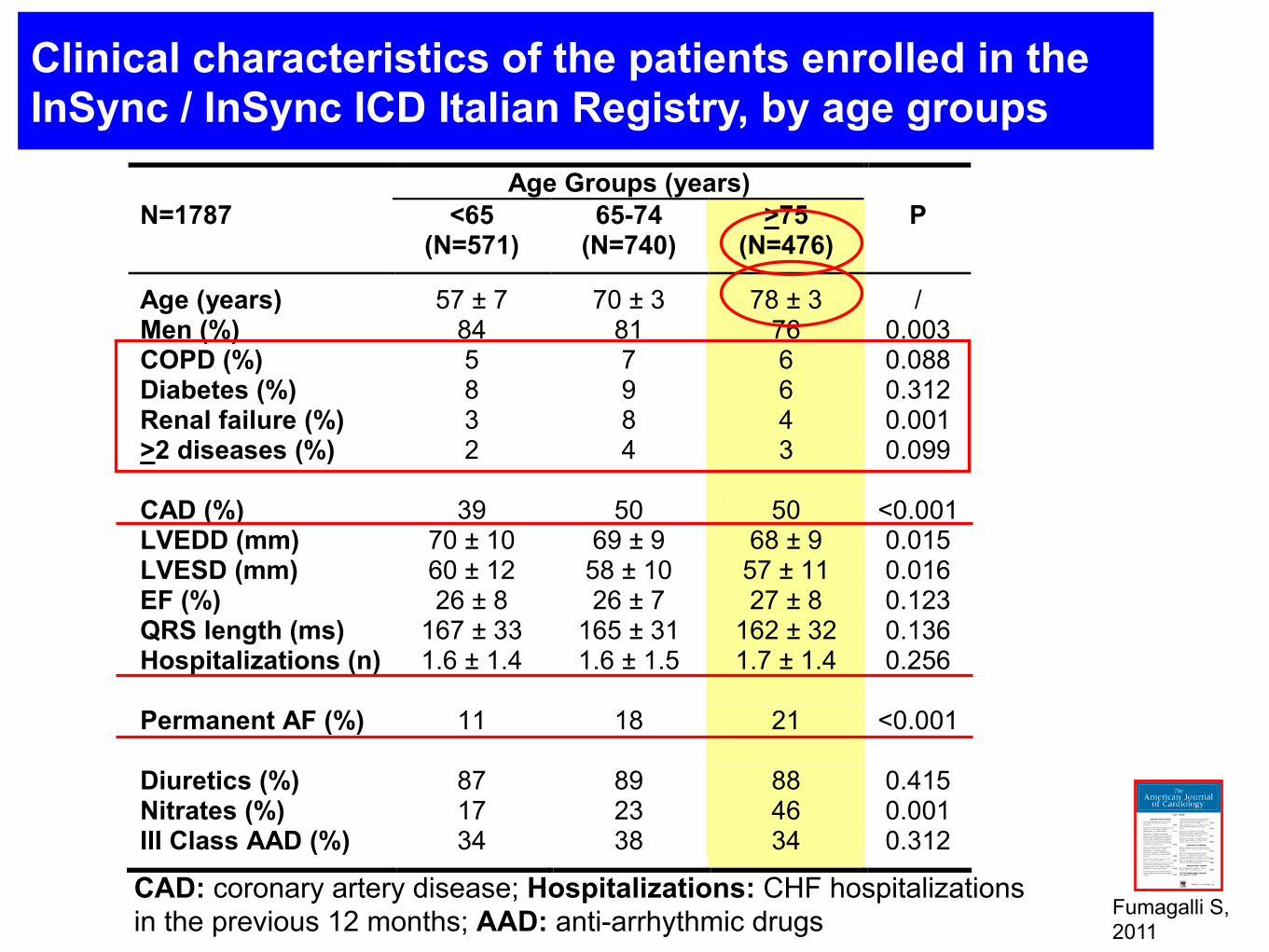
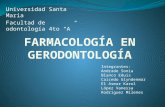
Clinical characteristics of the patients enrolled in the InSync / InSync ICD Italian Registry, by age groups
Age Groups (years) N=1787 <65
(N=571) 65-74
(N=740) >75
(N=476) P
Age (years) 57 ± 7 70 ± 3 78 ± 3 / Men (%) 84 81 76 0.003 COPD (%) 5 7 6 0.088 Diabetes (%) 8 9 6 0.312 Renal failure (%) 3 8 4 0.001 >2 diseases (%) 2 4 3 0.099 CAD (%) 39 50 50 <0.001 LVEDD (mm) 70 ± 10 69 ± 9 68 ± 9 0.015 LVESD (mm) 60 ± 12 58 ± 10 57 ± 11 0.016 EF (%) 26 ± 8 26 ± 7 27 ± 8 0.123 QRS length (ms) 167 ± 33 165 ± 31 162 ± 32 0.136 Hospitalizations (n) 1.6 ± 1.4 1.6 ± 1.5 1.7 ± 1.4 0.256 Permanent AF (%) 11 18 21 <0.001 Diuretics (%) 87 89 88 0.415 Nitrates (%) 17 23 46 0.001 III Class AAD (%) 34 38 34 0.312 CAD: coronary artery disease; Hospitalizations: CHF hospitalizations in the previous 12 months; AAD: anti-arrhythmic drugs Fumagalli S,
2011
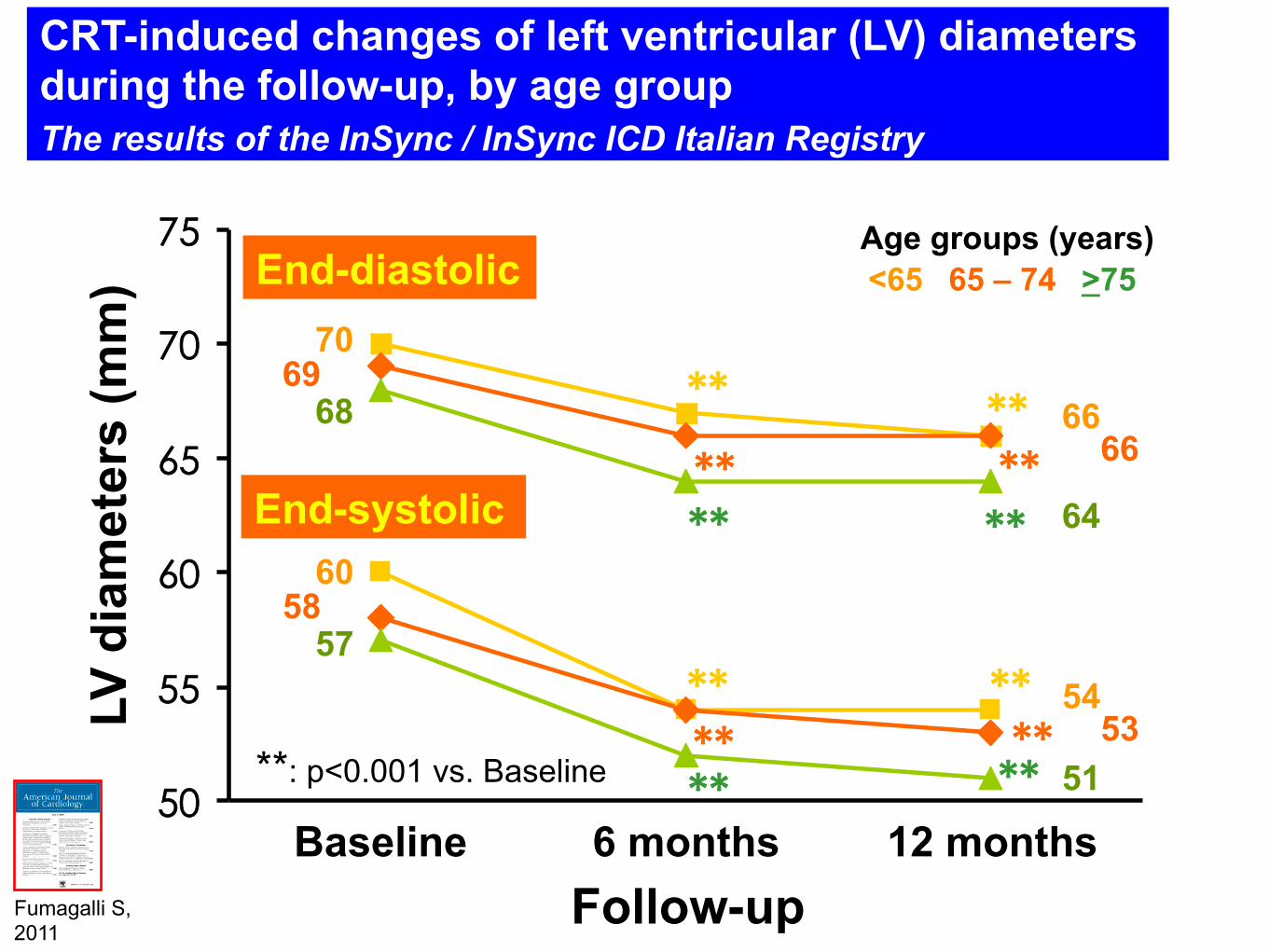
CRT-induced changes of left ventricular (LV) diameters during the follow-up, by age group The results of the InSync / InSync ICD Italian Registry
50
55
60
65
70
75
Baseline 6 months 12 months Follow-up
LV d
iam
eter
s (m
m) End-diastolic
End-systolic
** ** **
** **
**
** ** **
** ** ** **: p<0.001 vs. Baseline
<65 65 – 74 >75 Age groups (years)
66 66
64
69 70
68
53 54
51
58 60
57
Fumagalli S, 2011
15
25
35
45
Baseline 6 months 12 months Follow-up
(%)
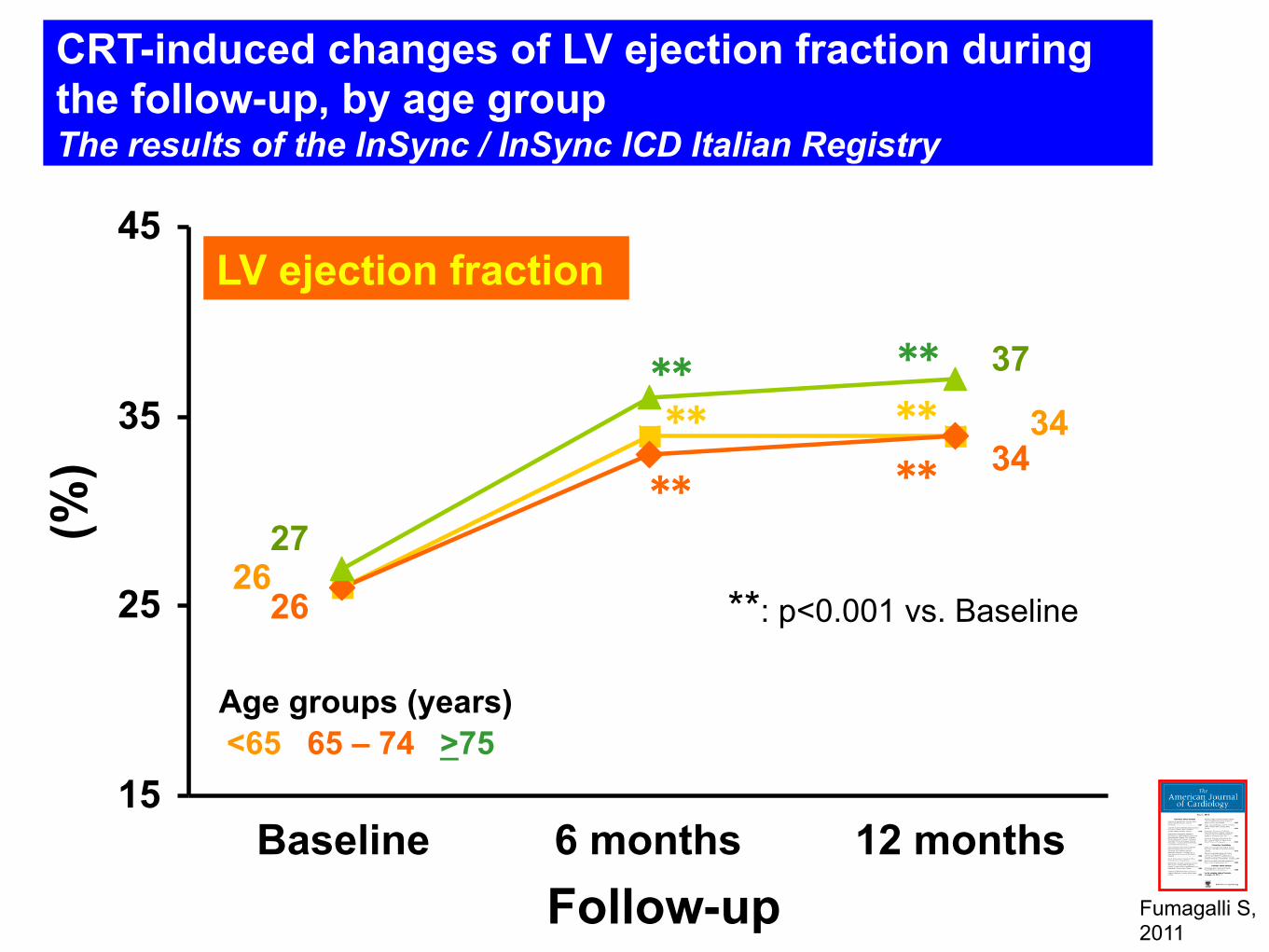
LV ejection fraction
** **
**
** ** **
**: p<0.001 vs. Baseline
CRT-induced changes of LV ejection fraction during the follow-up, by age group The results of the InSync / InSync ICD Italian Registry
26 27
26
34
37
34
<65 65 – 74 >75 Age groups (years)
Fumagalli S, 2011
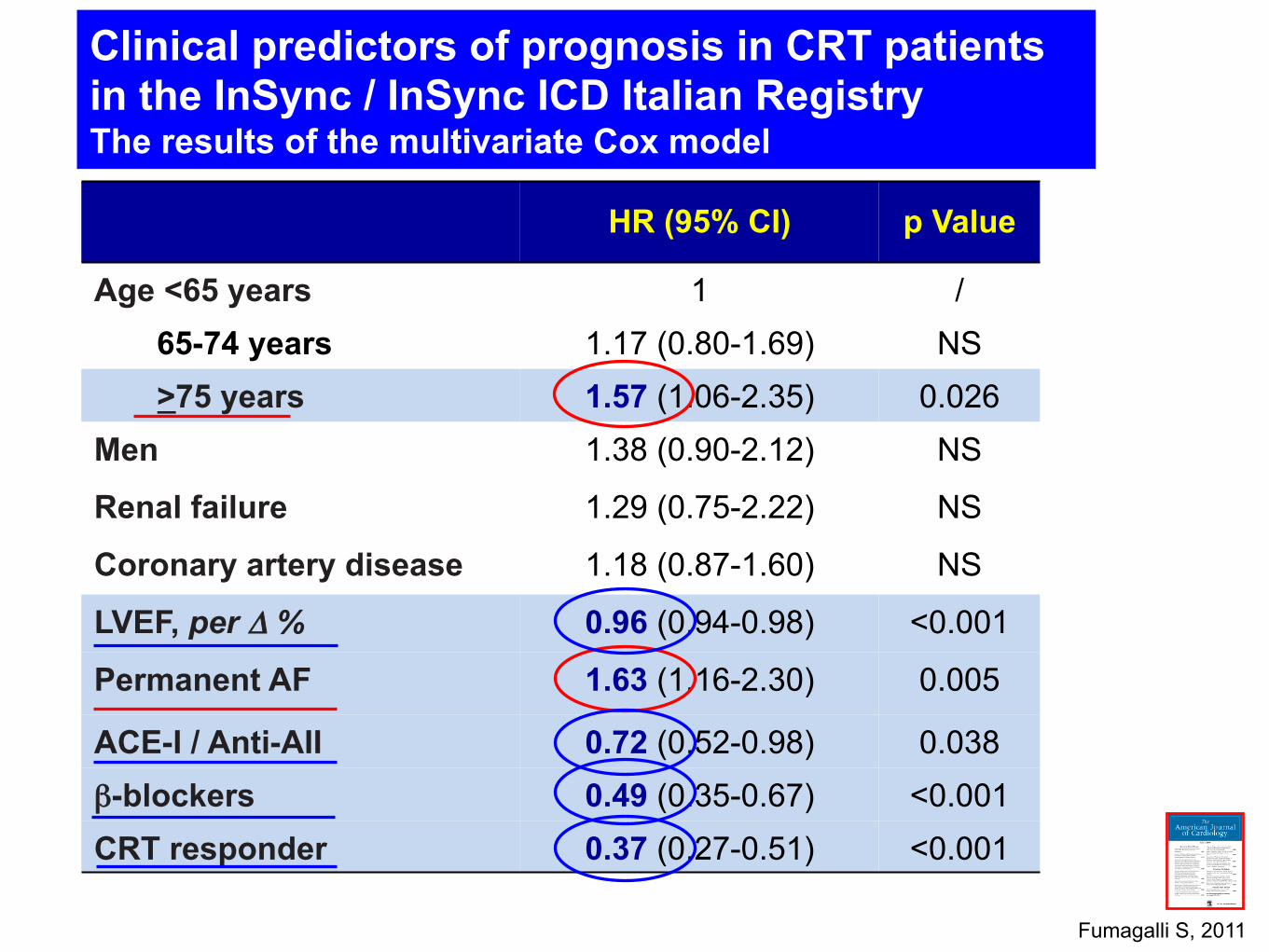
HR (95% CI)
p Value
Age <65 years 1 / 65-74 years 1.17 (0.80-1.69) NS >75 years 1.57 (1.06-2.35) 0.026 Men 1.38 (0.90-2.12) NS
Renal failure 1.29 (0.75-2.22) NS
Coronary artery disease 1.18 (0.87-1.60) NS
LVEF, per Δ % 0.96 (0.94-0.98) <0.001
Permanent AF 1.63 (1.16-2.30) 0.005
ACE-I / Anti-AII 0.72 (0.52-0.98) 0.038 β-blockers 0.49 (0.35-0.67) <0.001 CRT responder 0.37 (0.27-0.51) <0.001
Clinical predictors of prognosis in CRT patients in the InSync / InSync ICD Italian Registry The results of the multivariate Cox model
Fumagalli S, 2011
Prob
abili
ty o
f HF/
deat
h
Follow-up (years)
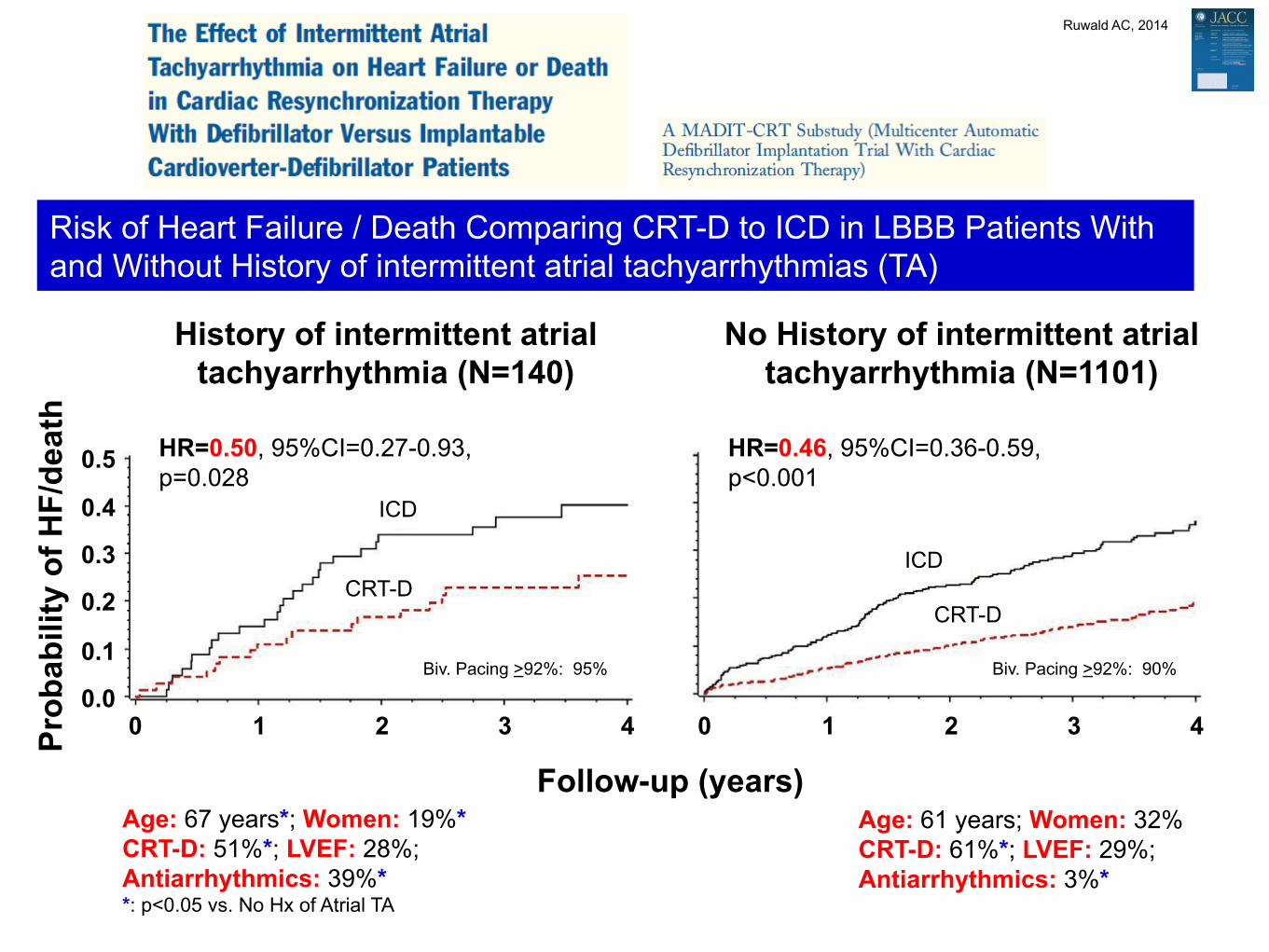
History of intermittent atrial tachyarrhythmia (N=140)
Age: 67 years*; Women: 19%* CRT-D: 51%*; LVEF: 28%; Antiarrhythmics: 39%* *: p<0.05 vs. No Hx of Atrial TA
Risk of Heart Failure / Death Comparing CRT-D to ICD in LBBB Patients With and Without History of intermittent atrial tachyarrhythmias (TA)
ICD
HR=0.50, 95%CI=0.27-0.93, p=0.028
Ruwald AC, 2014
No History of intermittent atrial tachyarrhythmia (N=1101)
0 1 2 3
0.1
0.2
0.3
0.4
0.5
0.0 4 0 1 2 3 4
CRT-D ICD
CRT-D
HR=0.46, 95%CI=0.36-0.59, p<0.001
Age: 61 years; Women: 32% CRT-D: 61%*; LVEF: 29%; Antiarrhythmics: 3%*
Biv. Pacing >92%: 95% Biv. Pacing >92%: 90%
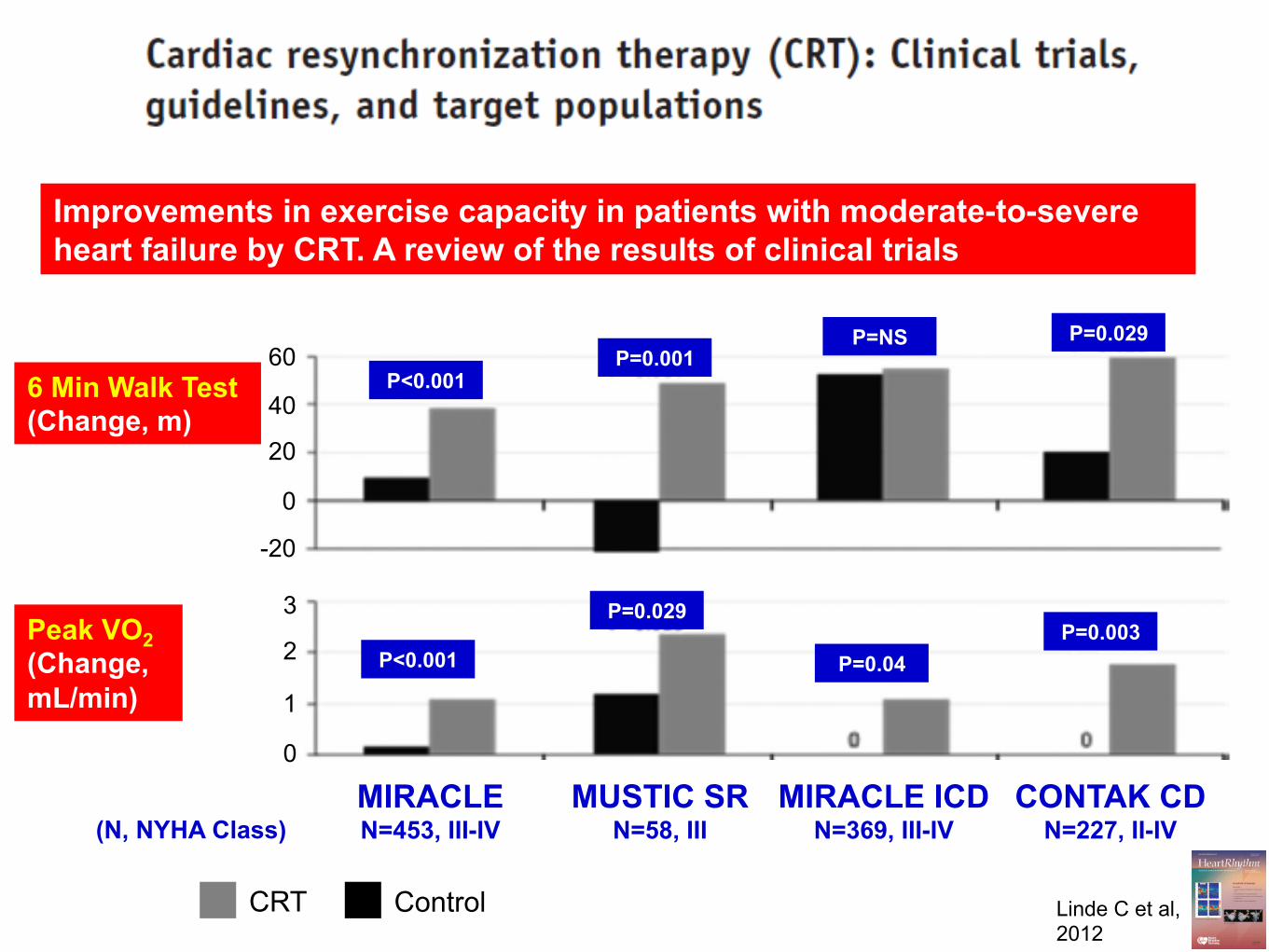
6 Min Walk Test (Change, m)
Peak VO2 (Change, mL/min)
MIRACLE N=453, III-IV
MUSTIC SR N=58, III
MIRACLE ICD N=369, III-IV
CONTAK CD N=227, II-IV
60
40
20
0
-20
3
2
1
0
(N, NYHA Class)
Improvements in exercise capacity in patients with moderate-to-severe heart failure by CRT. A review of the results of clinical trials
Linde C et al, 2012
CRT Control
P<0.001 P=0.001
P=NS P=0.029
P<0.001
P=0.029
P=0.04 P=0.003
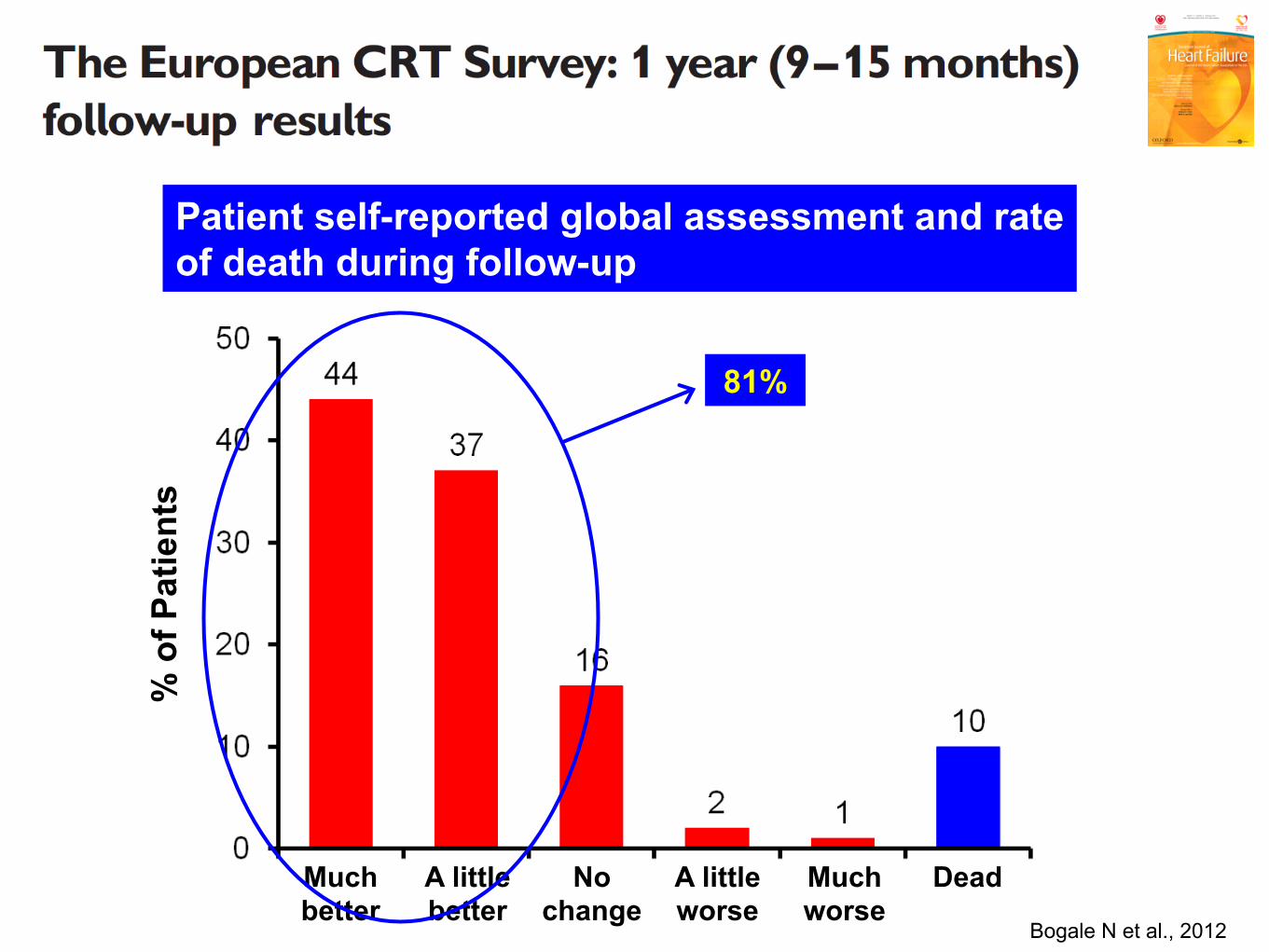
Bogale N et al., 2012
% o
f Pat
ient
s
Much better
A little better
No change
A little worse
Much worse
Dead
Patient self-reported global assessment and rate of death during follow-up
81%
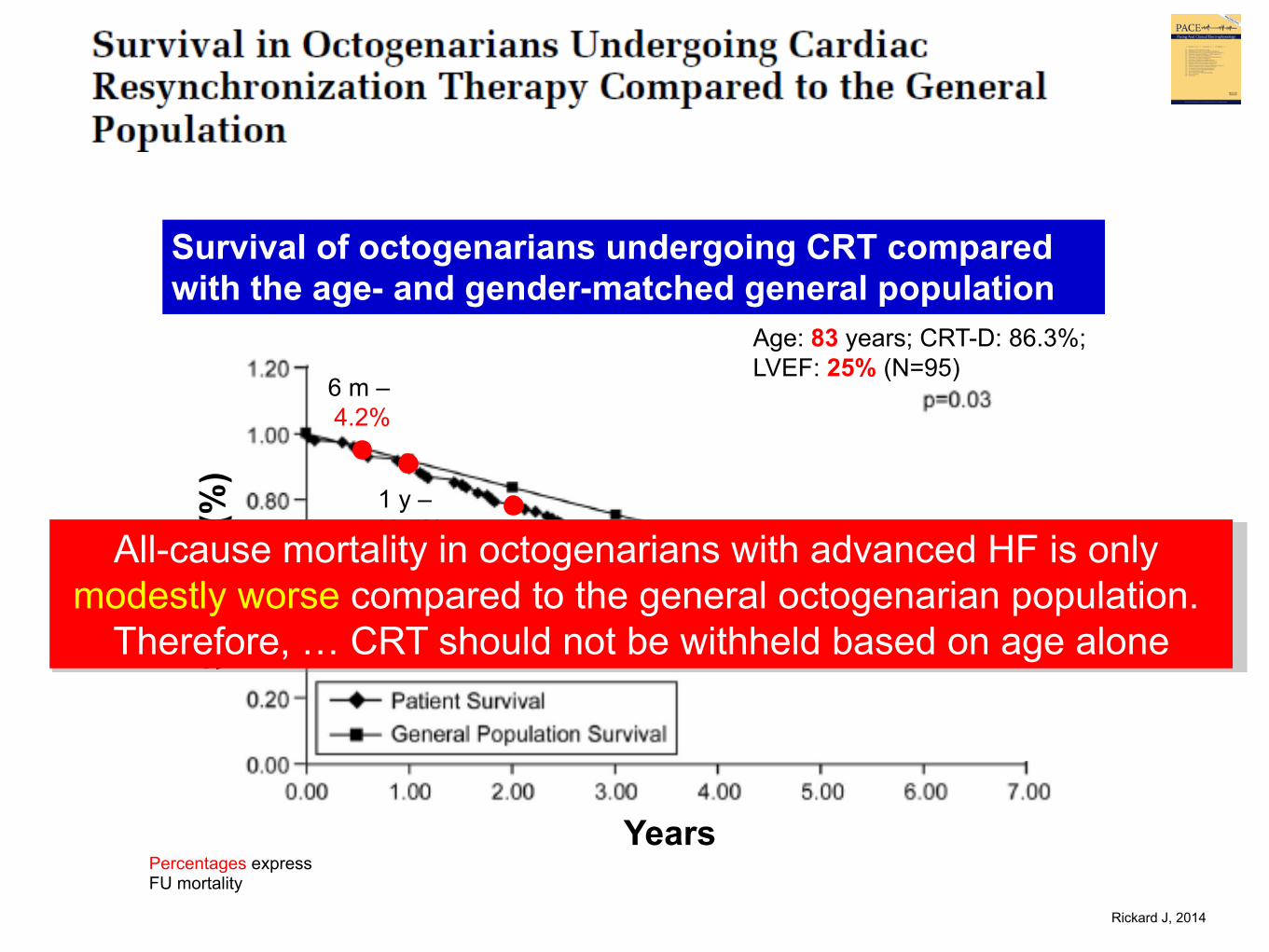
Years
Surv
ival
(%)
Survival of octogenarians undergoing CRT compared with the age- and gender-matched general population
6 m – 4.2%
1 y – 10.5% 2 y –
21.1% 3.6 y – 49.4%
Percentages express FU mortality
Age: 83 years; CRT-D: 86.3%; LVEF: 25% (N=95)
All-cause mortality in octogenarians with advanced HF is only modestly worse compared to the general octogenarian population.
Therefore, … CRT should not be withheld based on age alone
Rickard J, 2014 !
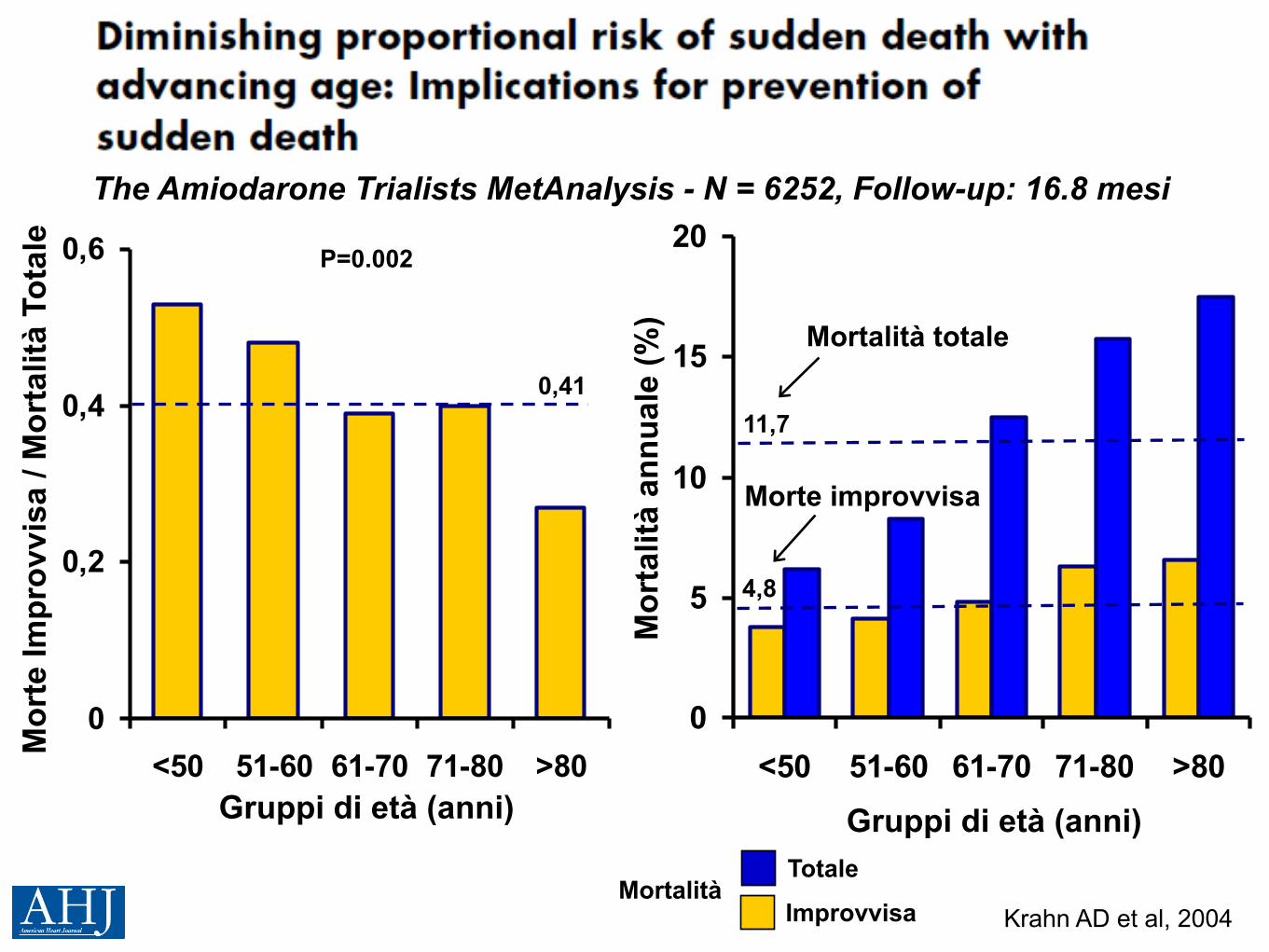
Mor
te Im
prov
visa
/ M
orta
lità
Tota
le
0
0,2
0,4
0,6
<50 51-60 61-70 71-80 >80Gruppi di età (anni)
0,41
P=0.002
Mortalità Totale
Improvvisa
Gruppi di età (anni)
0
5
10
15
20
<50 51-60 61-70 71-80 >80
Mor
talit
à an
nual
e (%
)
11,7
4,8
Mortalità totale
Morte improvvisa
Krahn AD et al, 2004
The Amiodarone Trialists MetAnalysis - N = 6252, Follow-up: 16.8 mesi
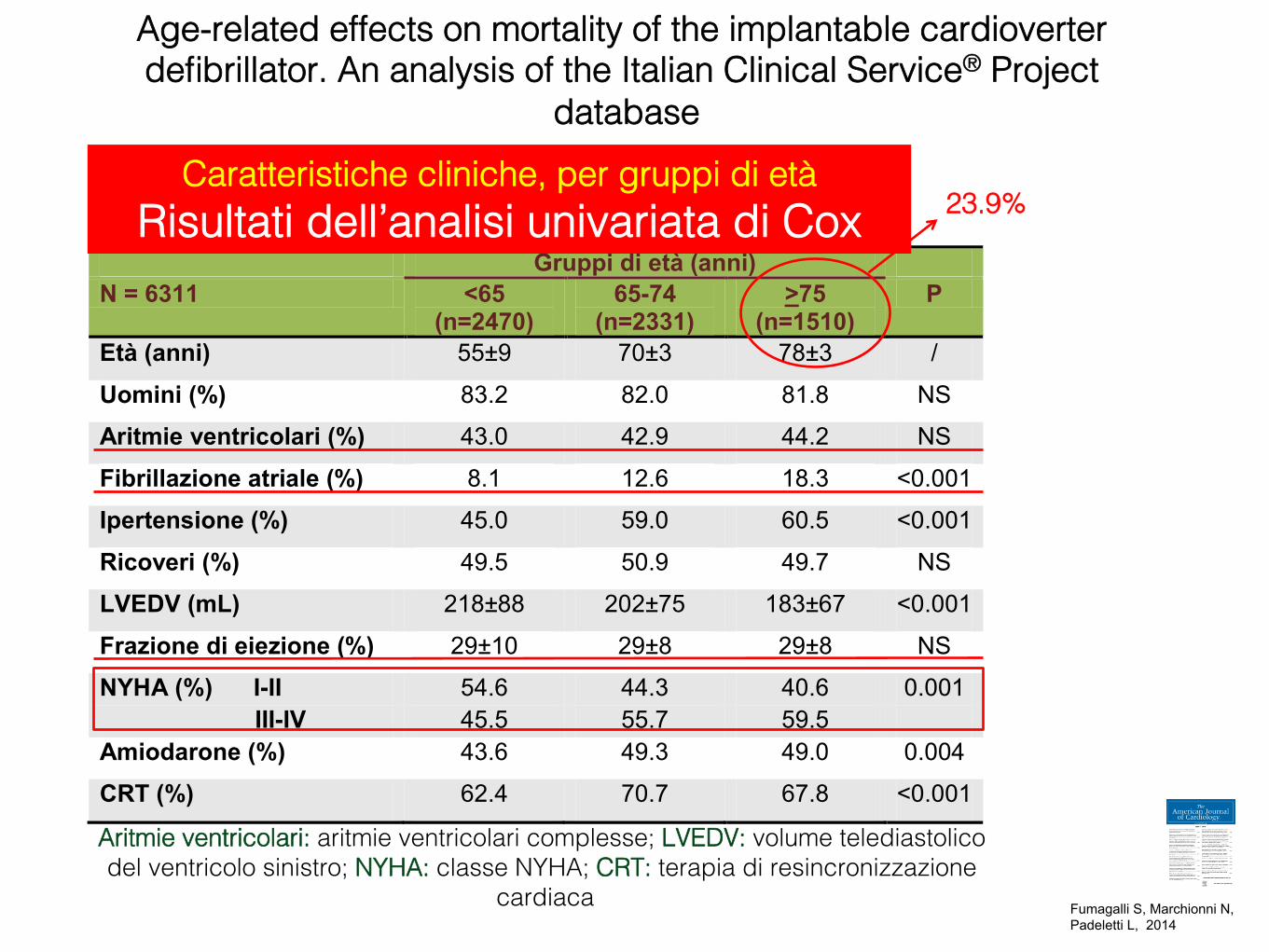
Gruppi di età (anni) N = 6311 <65
(n=2470) 65-74
(n=2331) >75
(n=1510) P
Età (anni) 55±9 70±3 78±3 /
Uomini (%) 83.2 82.0 81.8 NS
Aritmie ventricolari (%) 43.0 42.9 44.2 NS
Fibrillazione atriale (%) 8.1 12.6 18.3 <0.001
Ipertensione (%) 45.0 59.0 60.5 <0.001
Ricoveri (%) 49.5 50.9 49.7 NS
LVEDV (mL) 218±88 202±75 183±67 <0.001
Frazione di eiezione (%) 29±10 29±8 29±8 NS
NYHA (%) I-II 54.6 44.3 40.6 0.001 III-IV 45.5 55.7 59.5 Amiodarone (%) 43.6 49.3 49.0 0.004
CRT (%) 62.4 70.7 67.8 <0.001
Aritmie ventricolari: aritmie ventricolari complesse; LVEDV: volume telediastolico del ventricolo sinistro; NYHA: classe NYHA; CRT: terapia di resincronizzazione
cardiaca!
23.9%!Caratteristiche cliniche, per gruppi di età!
Risultati dell’analisi univariata di Cox!
Age-related effects on mortality of the implantable cardioverter defibrillator. An analysis of the Italian Clinical Service® Project
database!
Fumagalli S, Marchionni N, Padeletti L, 2014 !
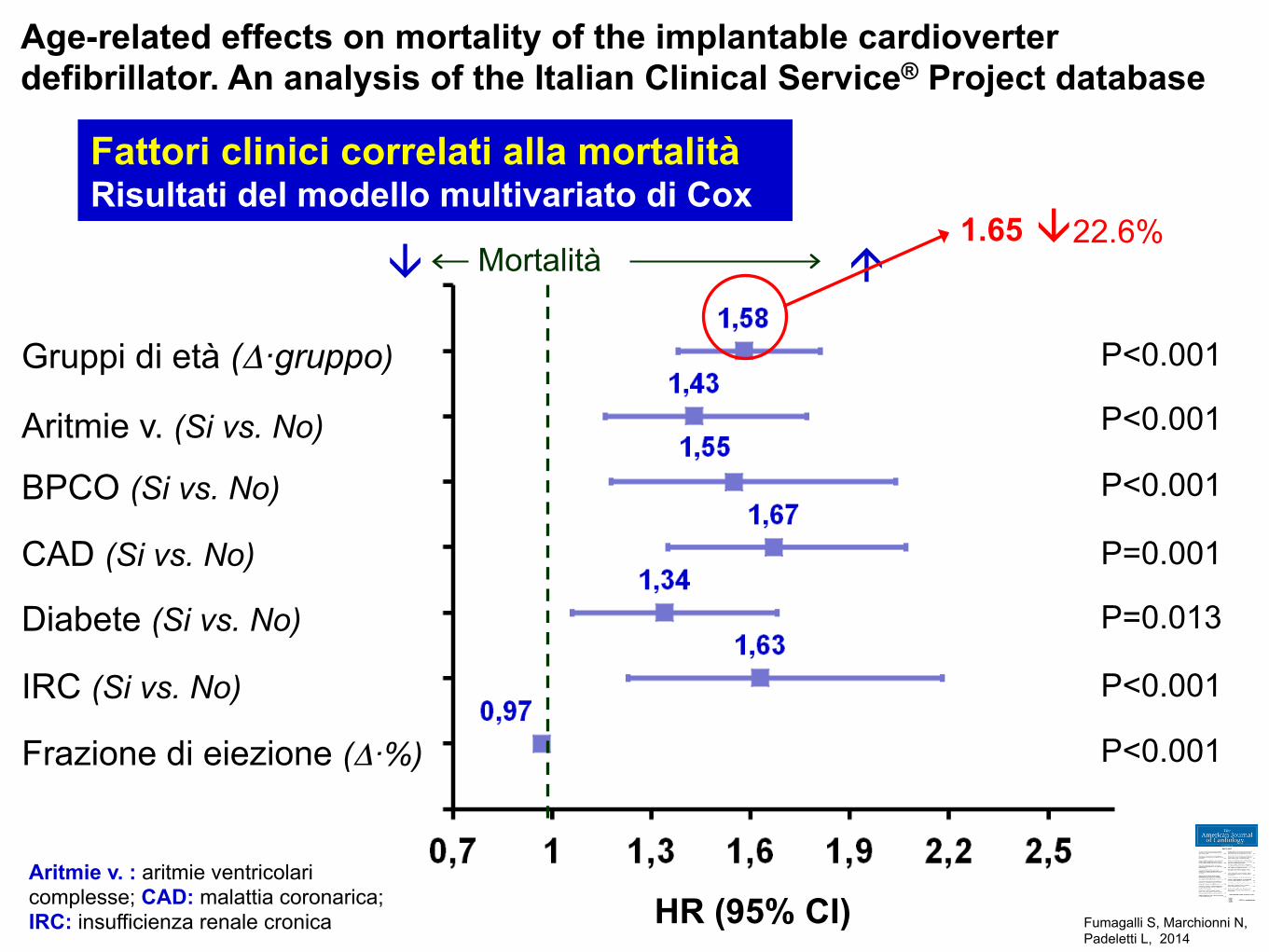
HR (95% CI)
Aritmie v. (Si vs. No)
IRC (Si vs. No)
BPCO (Si vs. No)
CAD (Si vs. No)
Gruppi di età (Δ·gruppo)
P<0.001
P<0.001
P<0.001
P<0.001
P=0.001
P<0.001
Diabete (Si vs. No) P=0.013
Frazione di eiezione (Δ·%)
Fattori clinici correlati alla mortalità Risultati del modello multivariato di Cox
Aritmie v. : aritmie ventricolari complesse; CAD: malattia coronarica; IRC: insufficienza renale cronica
Mortalità "#1.65 #22.6%
Age-related effects on mortality of the implantable cardioverter defibrillator. An analysis of the Italian Clinical Service® Project database
Fumagalli S, Marchionni N, Padeletti L, 2014 !
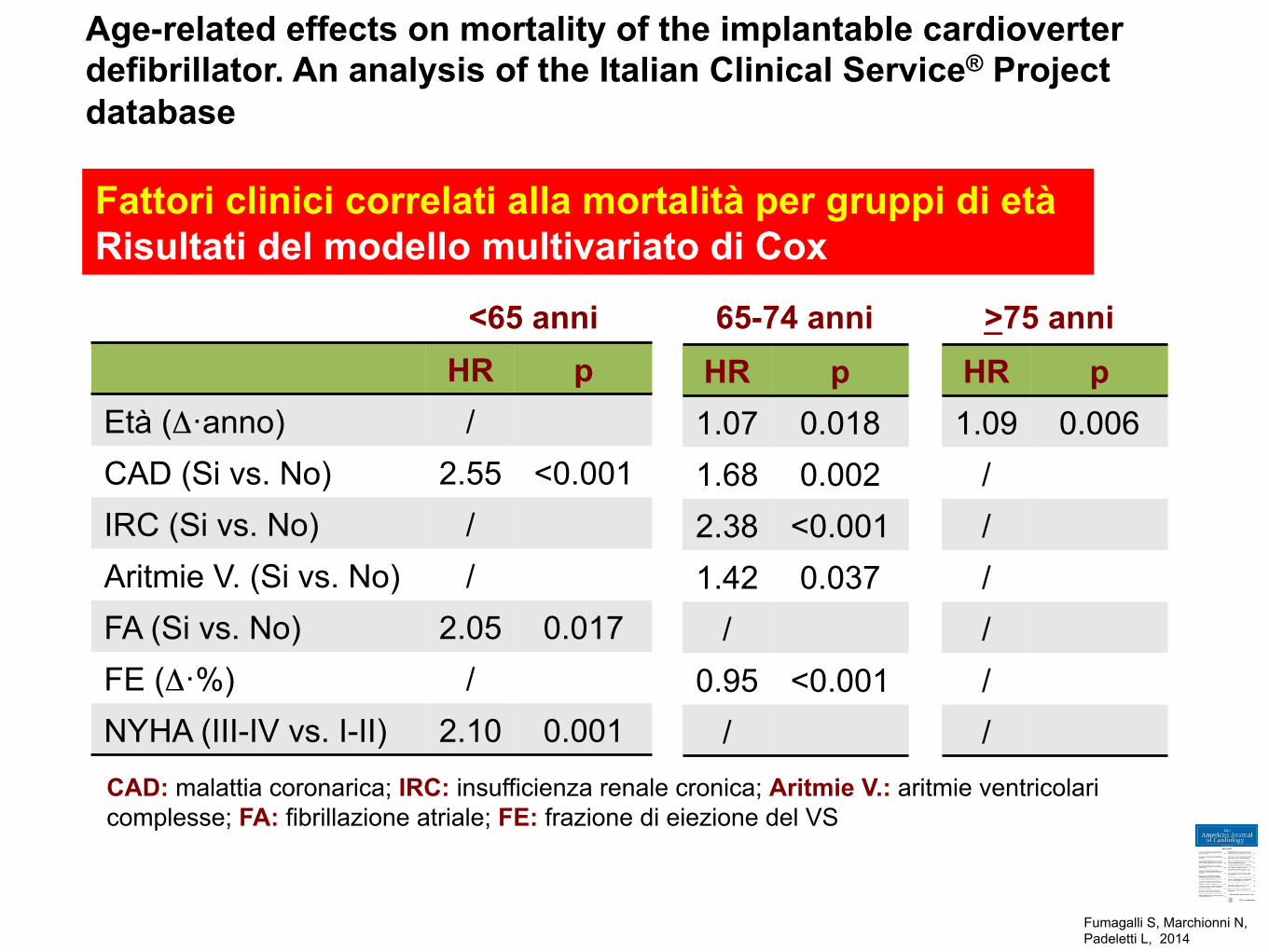
HR p Età (Δ·anno) / CAD (Si vs. No) 2.55 <0.001 IRC (Si vs. No) / Aritmie V. (Si vs. No) / FA (Si vs. No) 2.05 0.017 FE (Δ·%) / NYHA (III-IV vs. I-II) 2.10 0.001
HR p 1.07 0.018 1.68 0.002 2.38 <0.001 1.42 0.037
/ 0.95 <0.001
/
HR p 1.09 0.006
/ / / / / /
<65 anni 65-74 anni >75 anni
Fattori clinici correlati alla mortalità per gruppi di età Risultati del modello multivariato di Cox
CAD: malattia coronarica; IRC: insufficienza renale cronica; Aritmie V.: aritmie ventricolari complesse; FA: fibrillazione atriale; FE: frazione di eiezione del VS
Age-related effects on mortality of the implantable cardioverter defibrillator. An analysis of the Italian Clinical Service® Project database
Fumagalli S, Marchionni N, Padeletti L, 2014 !
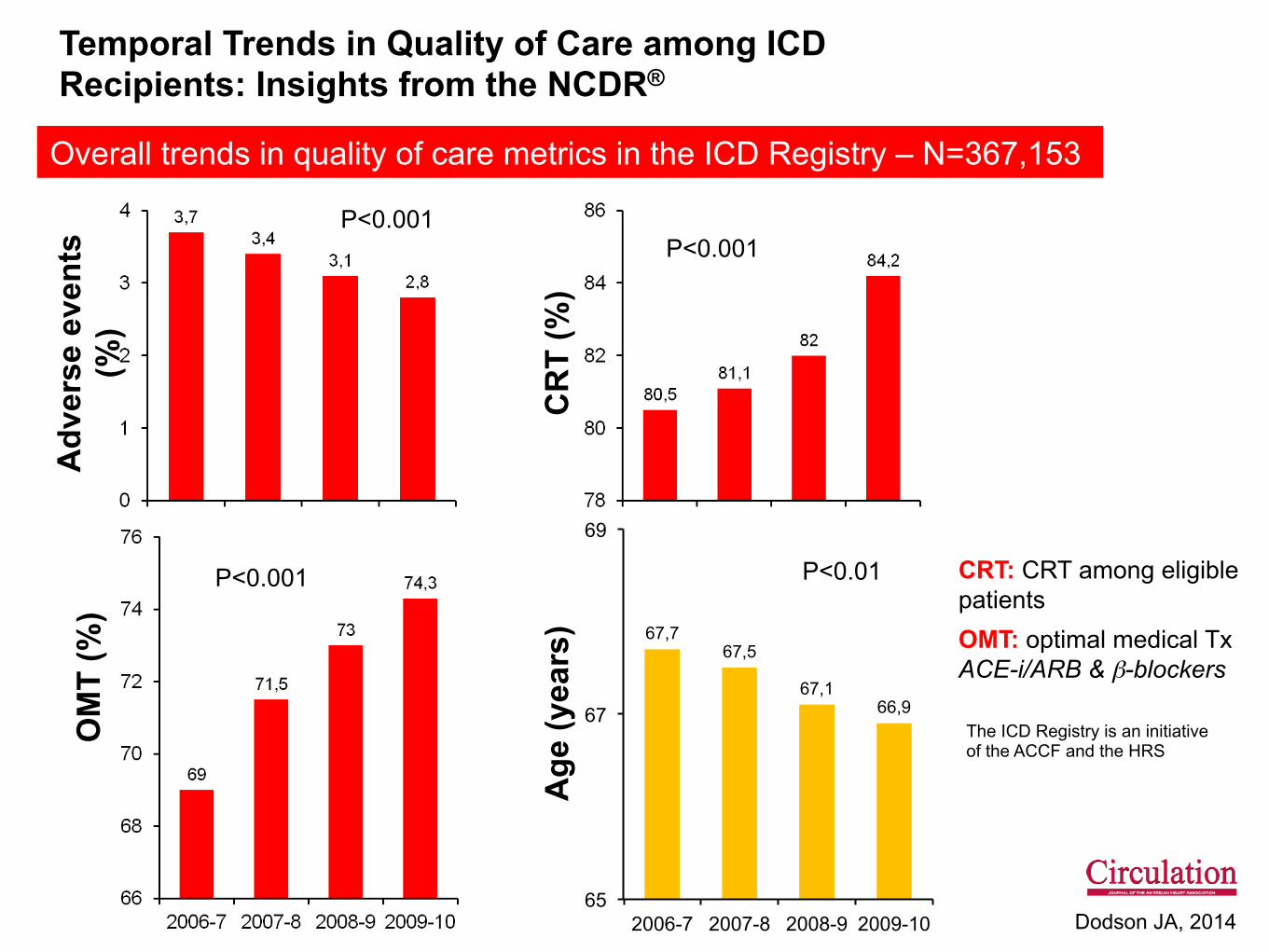
67,7 67,5
67,1 66,9
65
67
69
2006-7 2007-8 2008-9 2009-10
Adv
erse
eve
nts
(%)
OM
T (%
)
CR
T (%
) A
ge (y
ears
) CRT: CRT among eligible patients OMT: optimal medical Tx ACE-i/ARB & β-blockers
Overall trends in quality of care metrics in the ICD Registry – N=367,153
P<0.001
P<0.001
P<0.001
P<0.01
Temporal Trends in Quality of Care among ICD Recipients: Insights from the NCDR®
Dodson JA, 2014
The ICD Registry is an initiative of the ACCF and the HRS
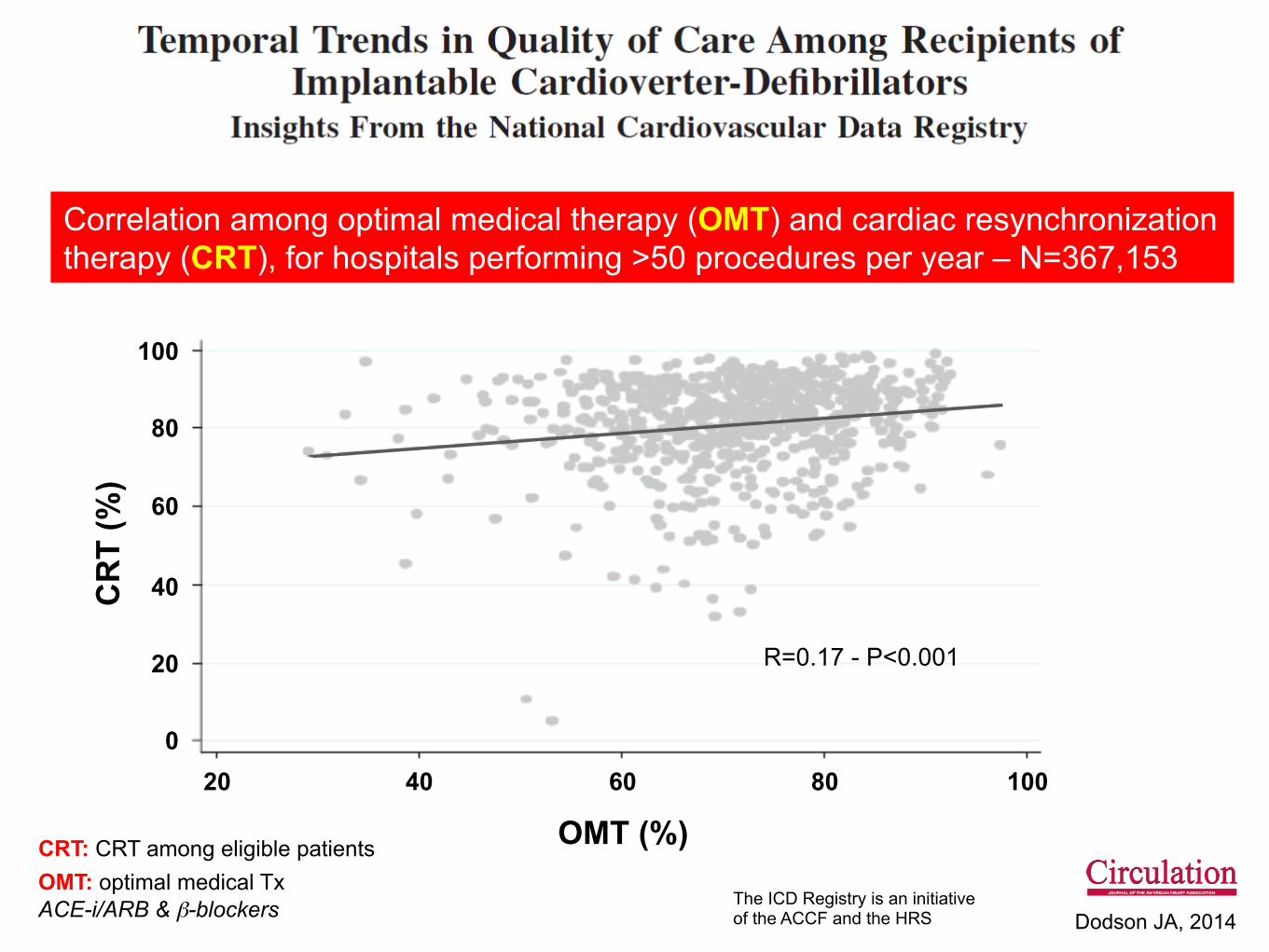
OMT (%)
CR
T (%
)
CRT: CRT among eligible patients OMT: optimal medical Tx ACE-i/ARB & β-blockers
Correlation among optimal medical therapy (OMT) and cardiac resynchronization therapy (CRT), for hospitals performing >50 procedures per year – N=367,153
R=0.17 - P<0.001
20
Dodson JA, 2014
40 60 80 100 0
20
40
60
80
100
The ICD Registry is an initiative of the ACCF and the HRS
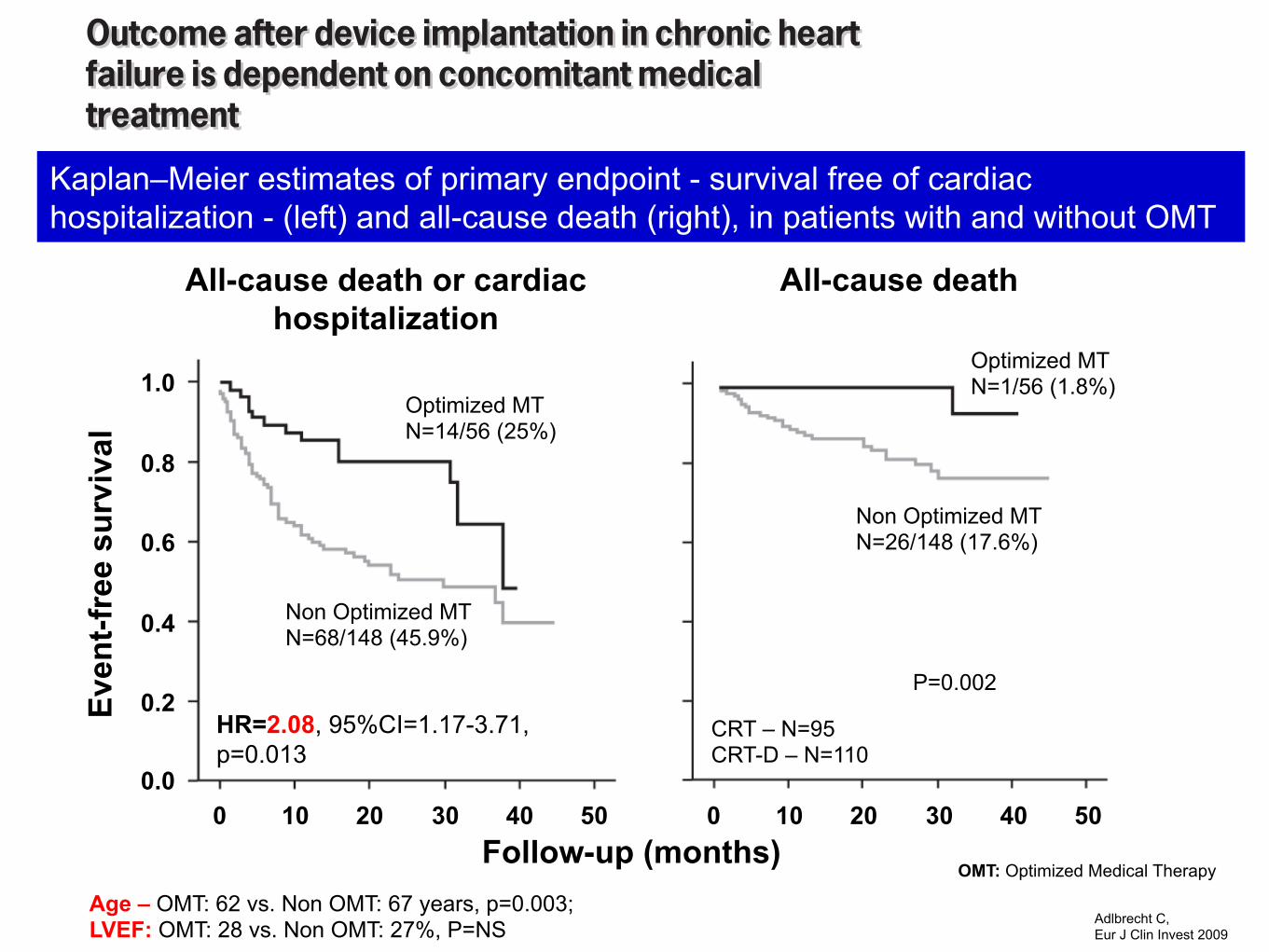
Even
t-fre
e su
rviv
al
Follow-up (months)
All-cause death or cardiac hospitalization
Age – OMT: 62 vs. Non OMT: 67 years, p=0.003; LVEF: OMT: 28 vs. Non OMT: 27%, P=NS
Kaplan–Meier estimates of primary endpoint - survival free of cardiac hospitalization - (left) and all-cause death (right), in patients with and without OMT
Optimized MT N=14/56 (25%)
HR=2.08, 95%CI=1.17-3.71, p=0.013
Adlbrecht C, Eur J Clin Invest 2009
All-cause death
0 10 20
0.2
0.4
0.6
0.8
1.0
0.0 30 40 50
Non Optimized MT N=68/148 (45.9%)
P=0.002
0 10 20 30 40 50
Optimized MT N=1/56 (1.8%)
Non Optimized MT N=26/148 (17.6%)
CRT – N=95 CRT-D – N=110
OMT: Optimized Medical Therapy
Outcome after device implantation in chronic heartfailure is dependent on concomitant medicaltreatmentC. Adlbrecht*, M. Hulsmann*, M. Gwechenberger*, G. Strunk†, C. Khazen*, F. Wiesbauer*, M. Elhenicky*,S. Neuhold*, T. Binder*, G. Maurer*, I. M. Lang* and R. Pacher*
*Medical University of Vienna, Vienna, Austria, †Vienna University of Economics and Business, Vienna, Austria
ABSTRACT
Background Device implantation in chronic heart failure (CHF) for cardiac resynchronization therapy (CRT) withor without implantable cardioverter ⁄ defibrillator (ICD) is an established treatment option for symptomaticpatients under medical baseline therapy. Although recommended, the need for optimization of medical therapywas never proven. As in ‘the real world’, medical therapy is not always up-titrated to the desirable dosages; thisprovides the opportunity to evaluate the impact of optimizing medical therapy in patients who had received adevice therapy with proven effectiveness.
Materials and methods This observational cohort study retrospectively assessed the ‘real life’-effect of CRTcompared with that of CRT ⁄ ICD therapy and the impact of concomitant pharmacotherapy on outcome. Outcomeof patients with guideline recommended renin–angiotensin system inhibitor and ß-blocker dosages was com-pared with that of patients who failed to reach the desired dosages. Mean follow-up for the 205 CHF (95 CRTand 110 CRT ⁄ ICD) patients was 16Æ8 ± 12Æ4 months.
Results In the total study cohort, 83 (41%) reached the combined primary endpoint of all-cause death or cardiachospitalization [CRT group: 25 (26%), CRT ⁄ ICD group: 58 (52Æ7%), P < 0Æ001]. Multiple cox regression analysisrevealed non-optimized medical therapy at follow-up [HR = 2Æ080 (1Æ166–3Æ710), P = 0Æ013] and CRT ⁄ ICD vs.CRT [HR = 2Æ504 (1Æ550–4Æ045), P < 0Æ001] as significant predictors of the primary endpoint.
Conclusion Our data stress the importance of professional monitoring and titration of pharmacotherapy notonly in medically treated CHF patients but also in patients under device therapy by a heart failure unit or a special-ized cardiologist.
Keywords Cardiac resynchronization, device therapy, heart failure, medical therapy, outcome.
Eur J Clin Invest 2009; 39 (12): 1073–1081
Introduction
Device implantation in chronic heart failure (CHF) forcardiac resynchronization therapy (CRT) with or withoutimplantable cardioverter ⁄ defibrillator (ICD) is an establishedtreatment option for symptomatic patients under medicalbaseline therapy [1]. The Comparison of Medical Therapy,Pacing, and Defibrillation in Heart Failure (COMPANION)study demonstrated comparable outcomes for CRT andCRT ⁄ ICD combination devices, with a further reduction ofmortality in the combination therapy group compared withthat in the group undergoing medical therapy alone [2]. Ina large multicentre prospective observational study, lower
rates of sudden cardiac death were reported for CRT ⁄ ICDcompared with that for CRT; however, this did not trans-late into significant improvements of total mortality [3].Patients included in randomized trials were under optimalmedical baseline therapy before implantation andmedications were adjusted as appropriate at the scheduledfollow-up visits; this was suggested to be one plausibleexplanation for the low mortality rates [1].
Recently published data from the Multicenter AutomaticDefibrillator Trail (MADIT) II demonstrated the importance ofconcomitant medical therapy in patients with ICD for primary
European Journal of Clinical Investigation Vol 39 1073
DOI: 10.1111/j.1365-2362.2009.02217.x
ORIGINAL ARTICLE
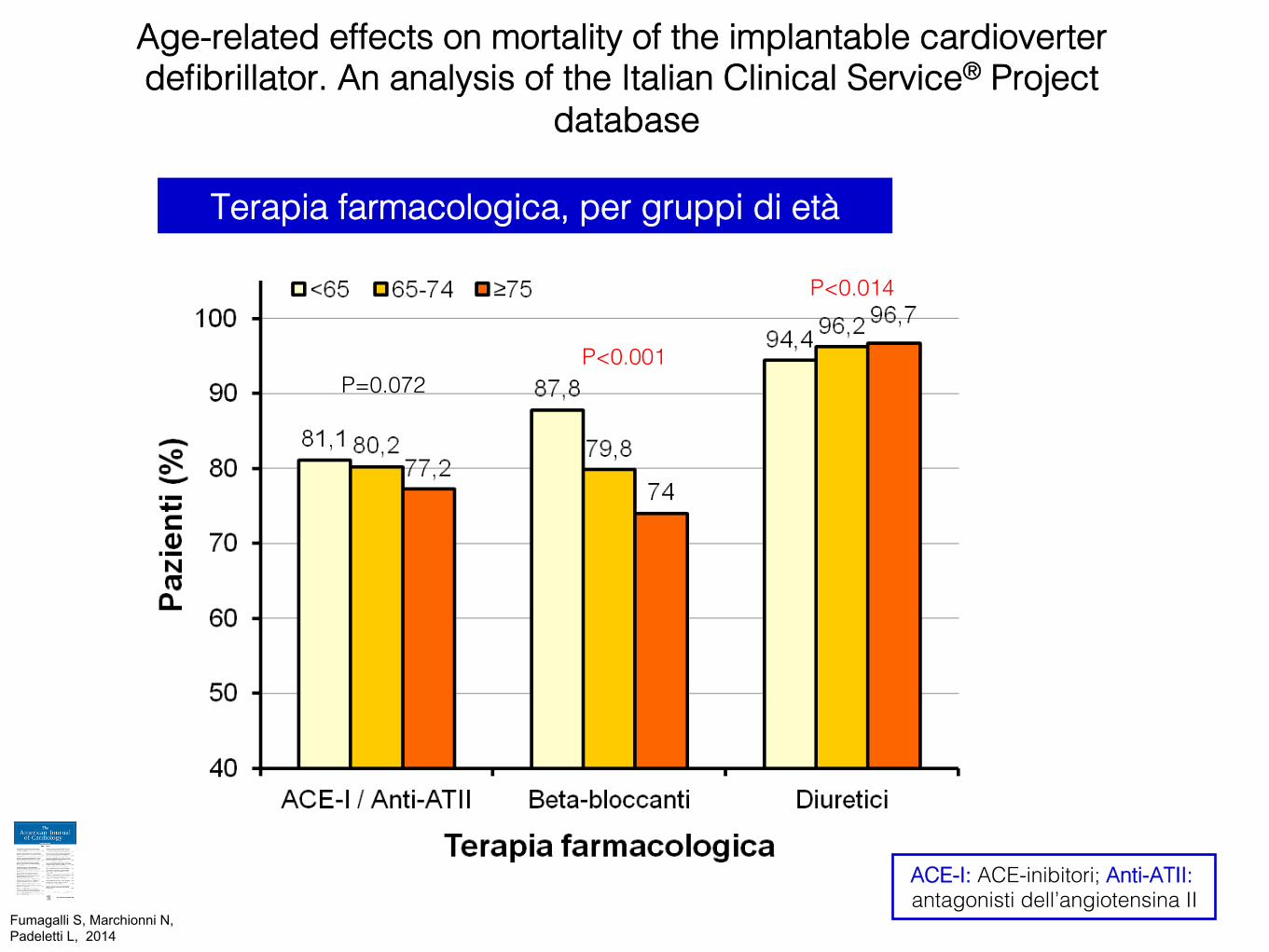
P=0.072!P<0.001!
P<0.014!
Terapia farmacologica, per gruppi di età!
ACE-I: ACE-inibitori; Anti-ATII: antagonisti dell’angiotensina II!
Age-related effects on mortality of the implantable cardioverter defibrillator. An analysis of the Italian Clinical Service® Project
database!
Fumagalli S, Marchionni N, Padeletti L, 2014 !
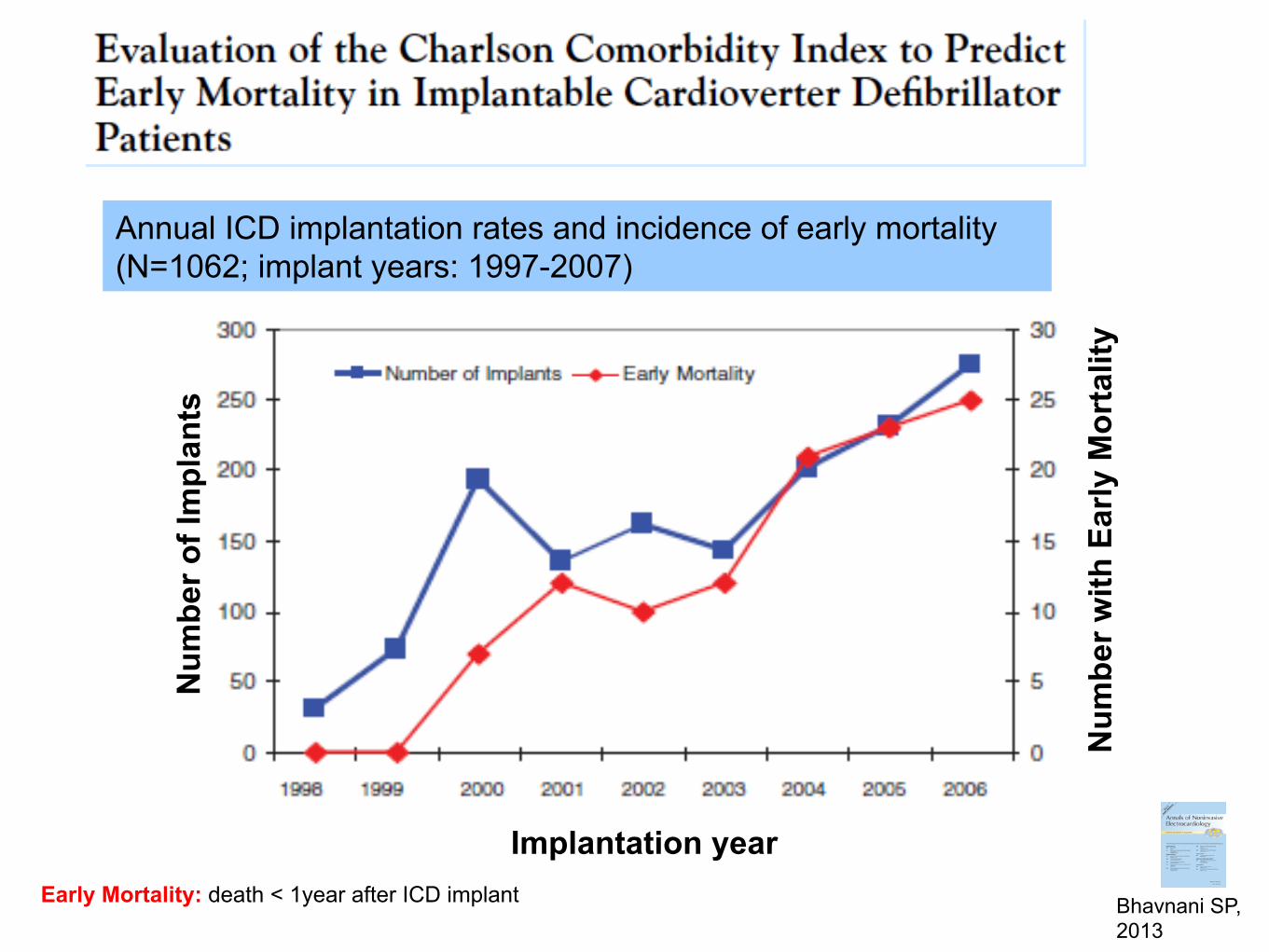
Implantation year
Num
ber o
f Im
plan
ts
Early Mortality: death < 1year after ICD implant
Annual ICD implantation rates and incidence of early mortality (N=1062; implant years: 1997-2007)
Bhavnani SP, 2013
Num
ber w
ith E
arly
Mor
talit
y
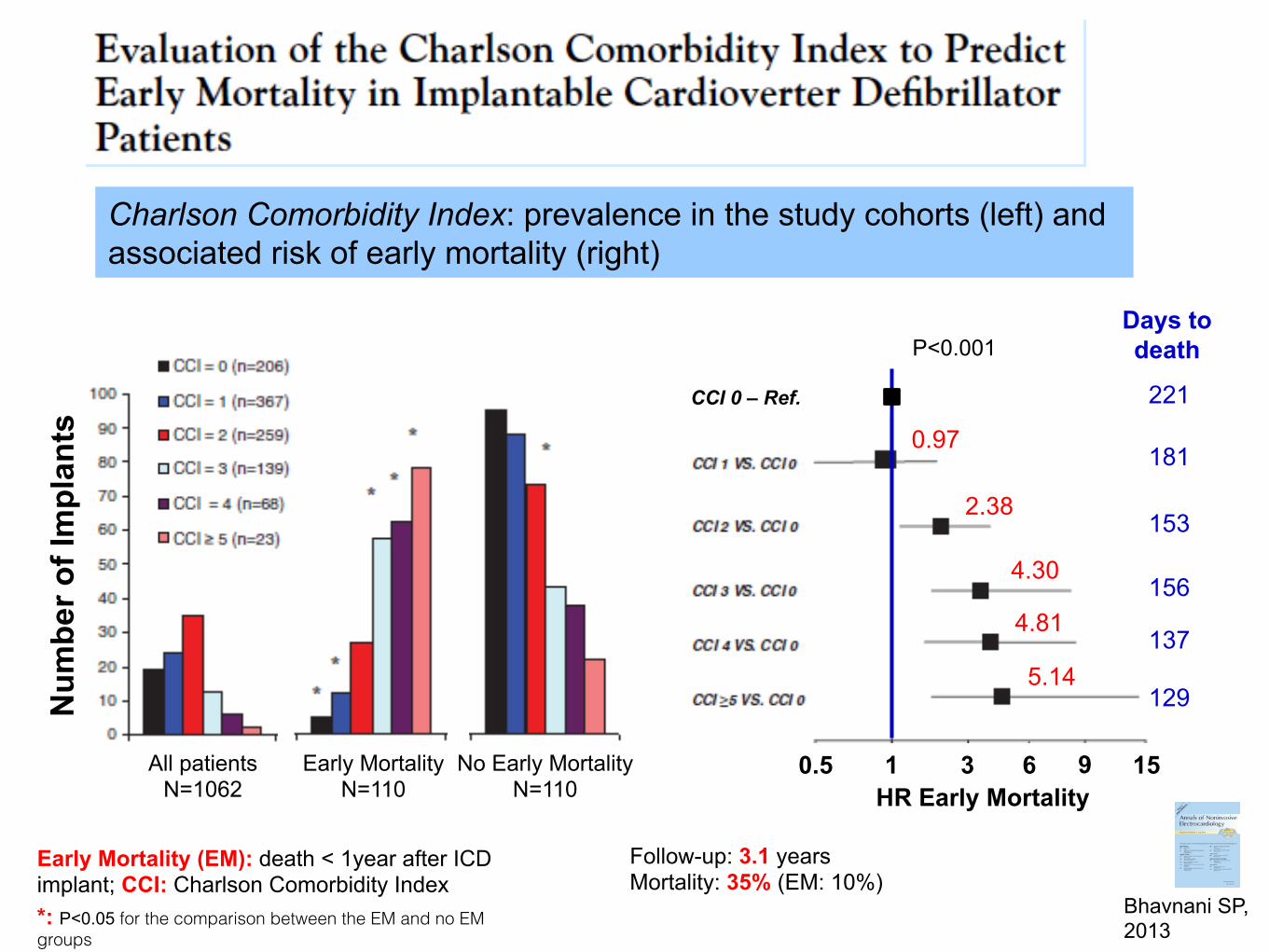
All patients N=1062
Num
ber o
f Im
plan
ts
Early Mortality (EM): death < 1year after ICD implant; CCI: Charlson Comorbidity Index
Charlson Comorbidity Index: prevalence in the study cohorts (left) and associated risk of early mortality (right)
Bhavnani SP, 2013
Early Mortality N=110
No Early Mortality N=110
*: P<0.05 for the comparison between the EM and no EM groups
HR Early Mortality 0.5 1 3 6 15
5.14
4.81
4.30
2.38
0.97
9
P<0.001
129
137
156
153
181
CCI 0 – Ref. 221
Days to death
Follow-up: 3.1 years Mortality: 35% (EM: 10%)
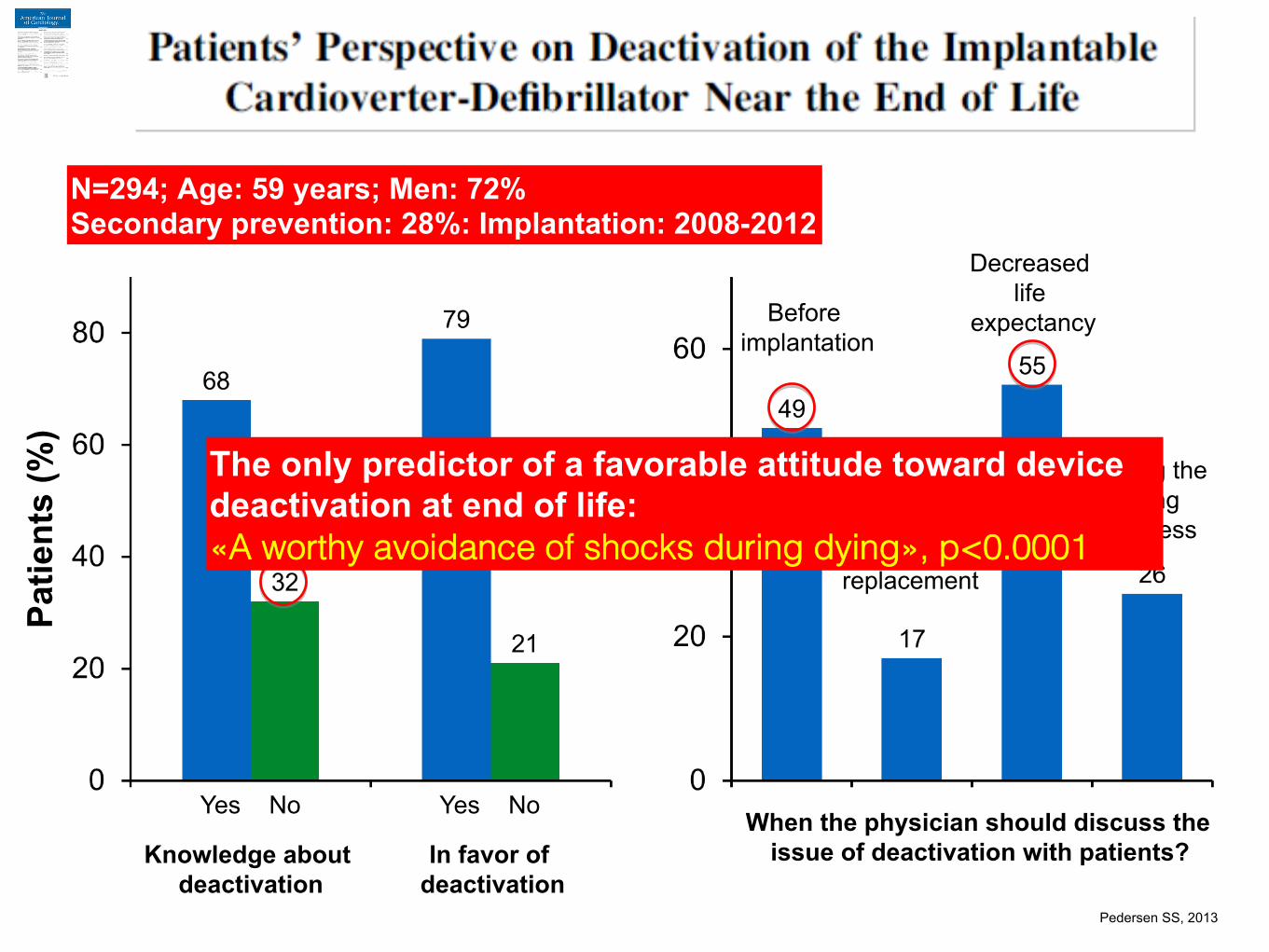
Patie
nts
(%)
Knowledge about deactivation
In favor of deactivation
Yes No Yes No
Before implantation
Battery replacement
Decreased life
expectancy
During the dying
process
When the physician should discuss the issue of deactivation with patients?
N=294; Age: 59 years; Men: 72% Secondary prevention: 28%: Implantation: 2008-2012!
The only predictor of a favorable attitude toward device deactivation at end of life: «A worthy avoidance of shocks during dying», p<0.0001!
Pedersen SS, 2013 !
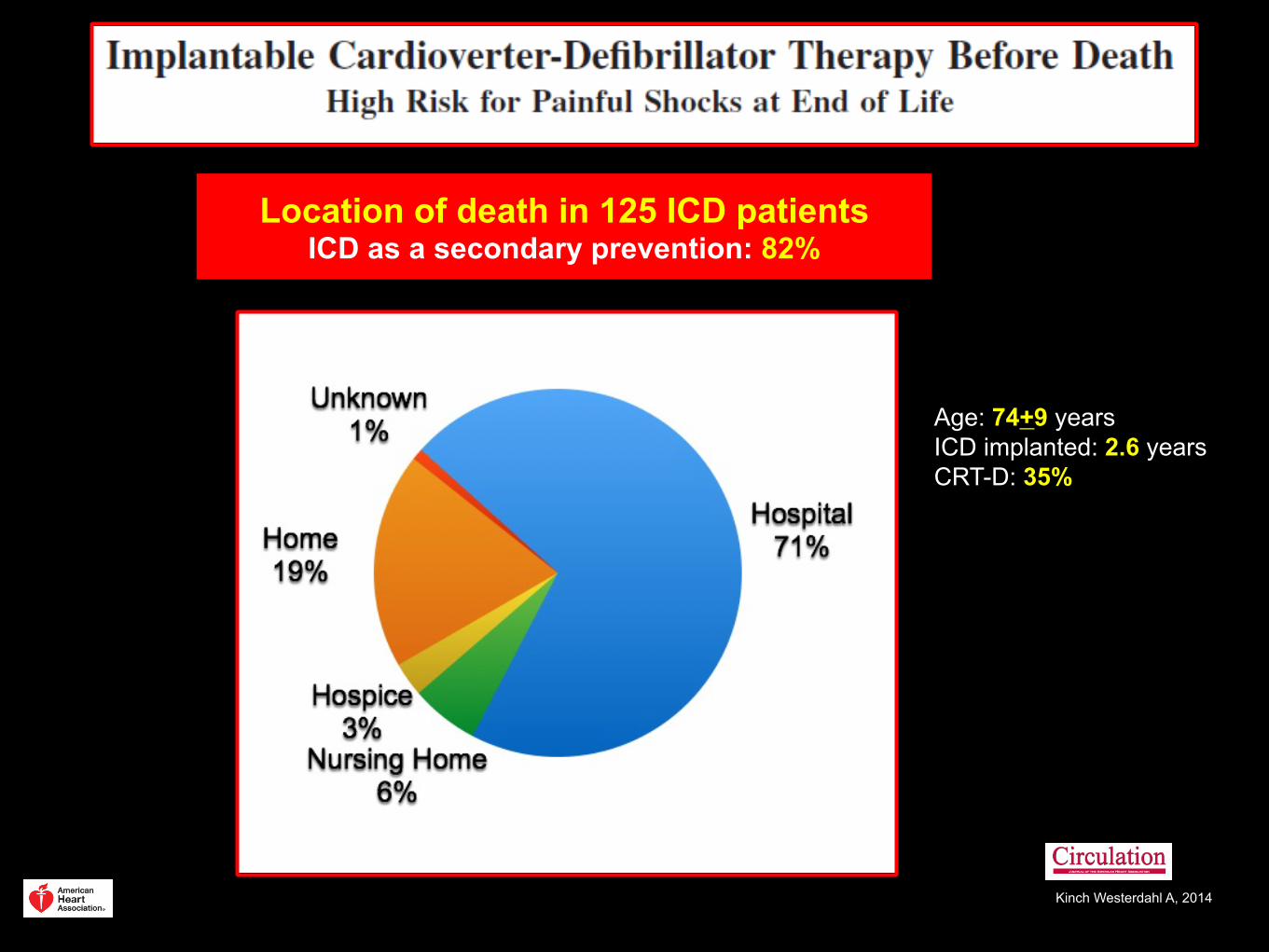
Location of death in 125 ICD patients ICD as a secondary prevention: 82% !
Kinch Westerdahl A, 2014 !
Age: 74+9 years ICD implanted: 2.6 years CRT-D: 35%
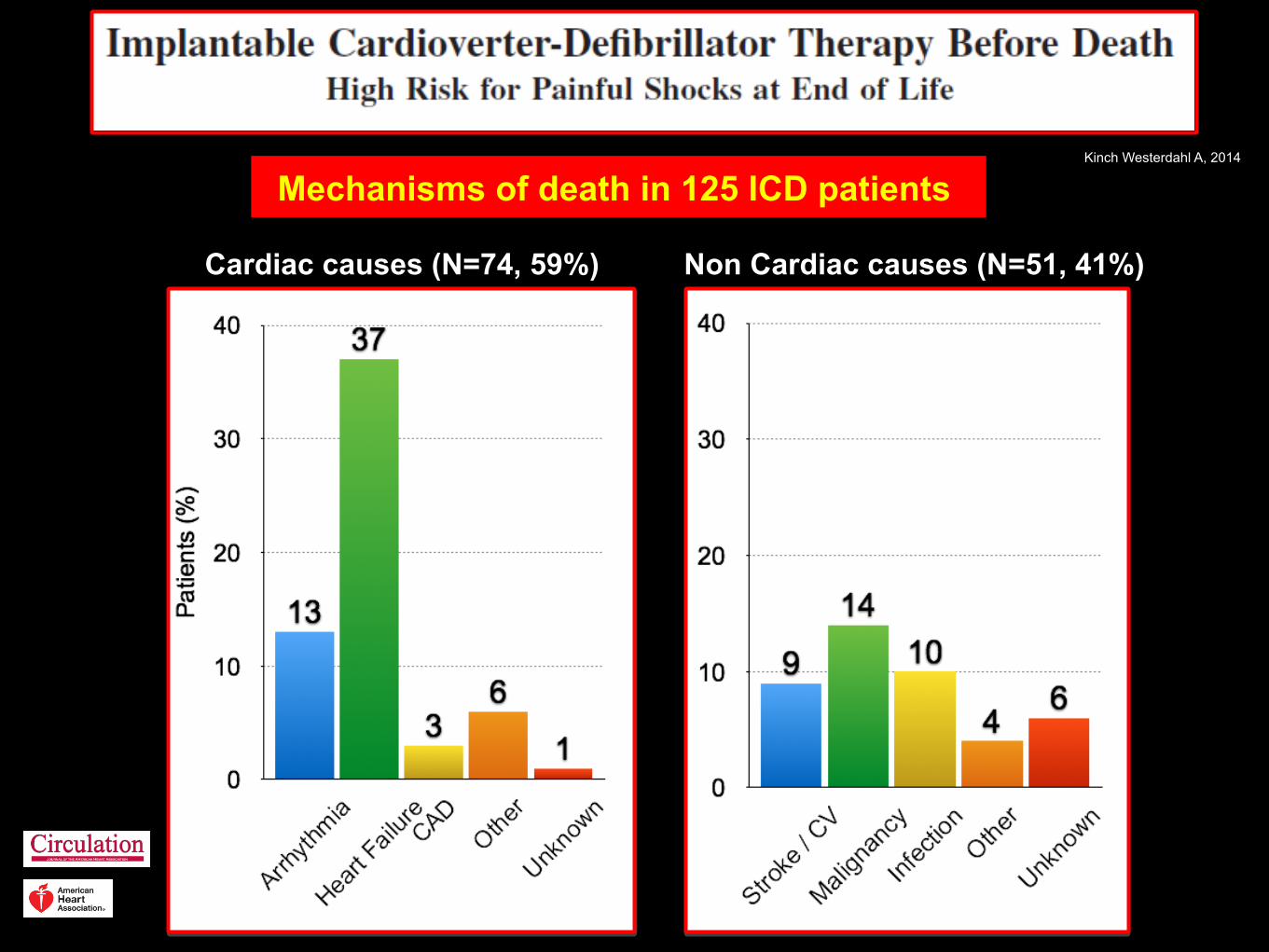
Mechanisms of death in 125 ICD patients ! Kinch Westerdahl A, 2014 !
Cardiac causes (N=74, 59%) Non Cardiac causes (N=51, 41%)
Kinch Westerdahl A, 2014 !
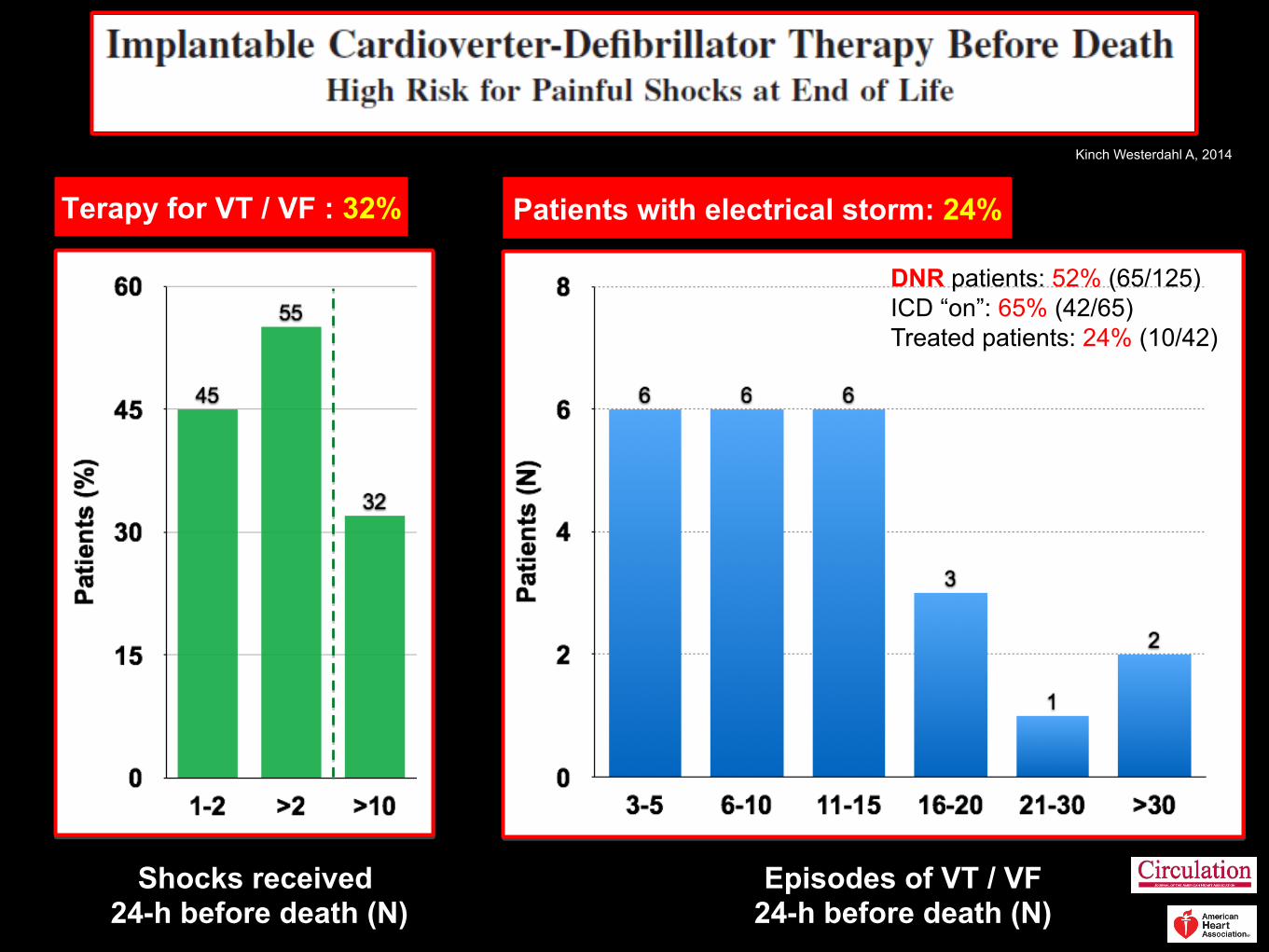
Shocks received 24-h before death (N)
Terapy for VT / VF : 32%
Episodes of VT / VF 24-h before death (N)
Patients with electrical storm: 24% !
DNR patients: 52% (65/125) ICD “on”: 65% (42/65) Treated patients: 24% (10/42)!
Key points
• The incidence of SCD increases with age owing to increasing prevalence of CHD and CHF among elderly individuals
• Elderly patients are more likely to have PEA or asystole at the time of SCD and are less likely to survive a cardiac arrest
• The mortality benefit and cost-effectiveness of primary prevention ICD therapy in elderly patients is dependent on competing mortality risks
• CRT has demonstrated mortality and HRQL benefits across age groups
• A substantial and growing proportion of primary prevention ICD and CRT devices are being implanted in elderly patients, and additional outcomes data in this growing population are needed
In lieu of randomized trial data, long-term outcome data from registries will be required to evaluate both the clinical effectiveness and cost-effectiveness of ICD and CRT in the elderly population
2013
Impl
anta
tion
Rat
e / 1
00.0
00
Year
65-74
>75
55-64
45-54 20-44
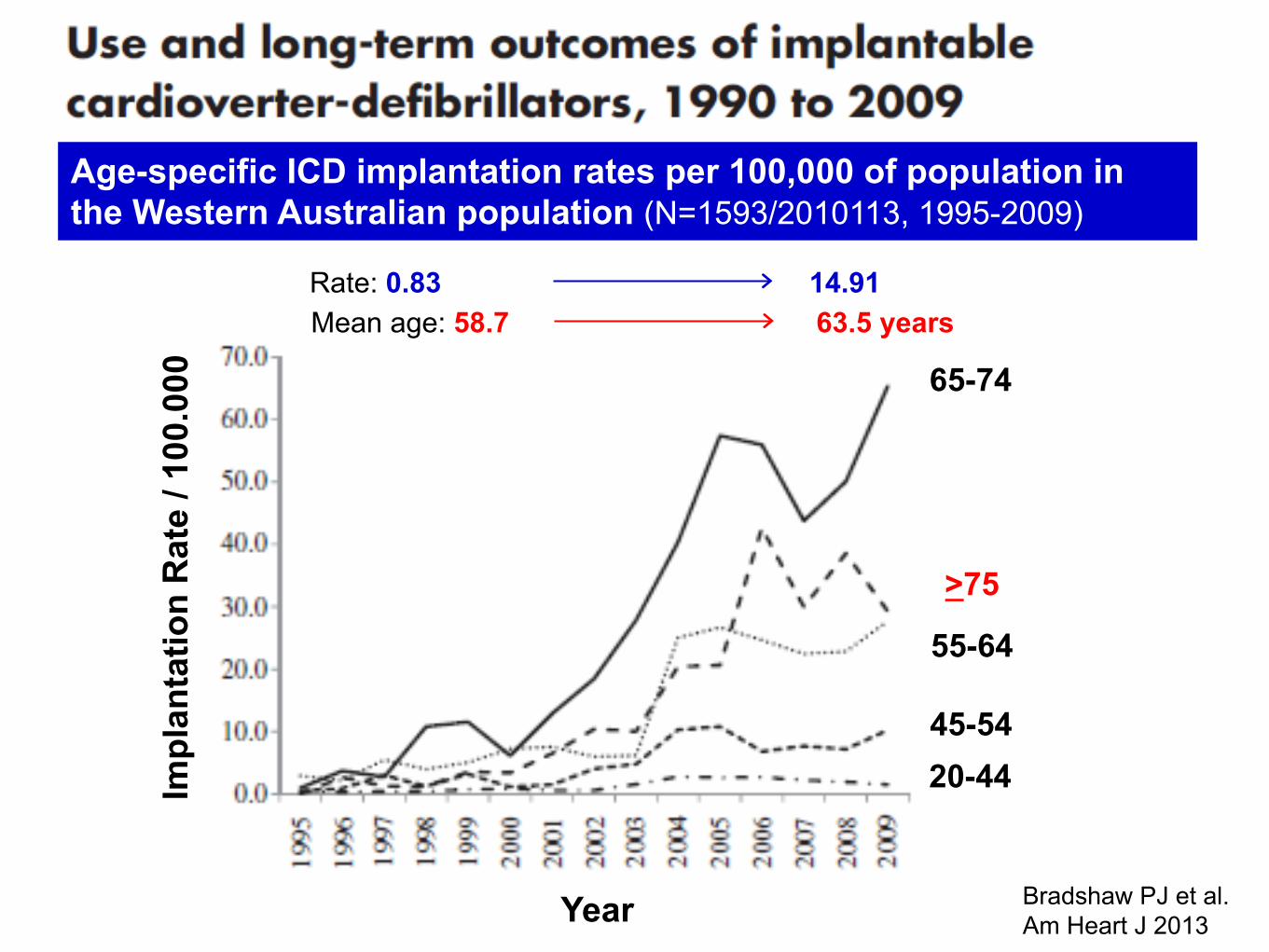
Rate: 0.83 14.91 Mean age: 58.7 63.5 years
Age-specific ICD implantation rates per 100,000 of population in the Western Australian population (N=1593/2010113, 1995-2009)
Bradshaw PJ et al. Am Heart J 2013
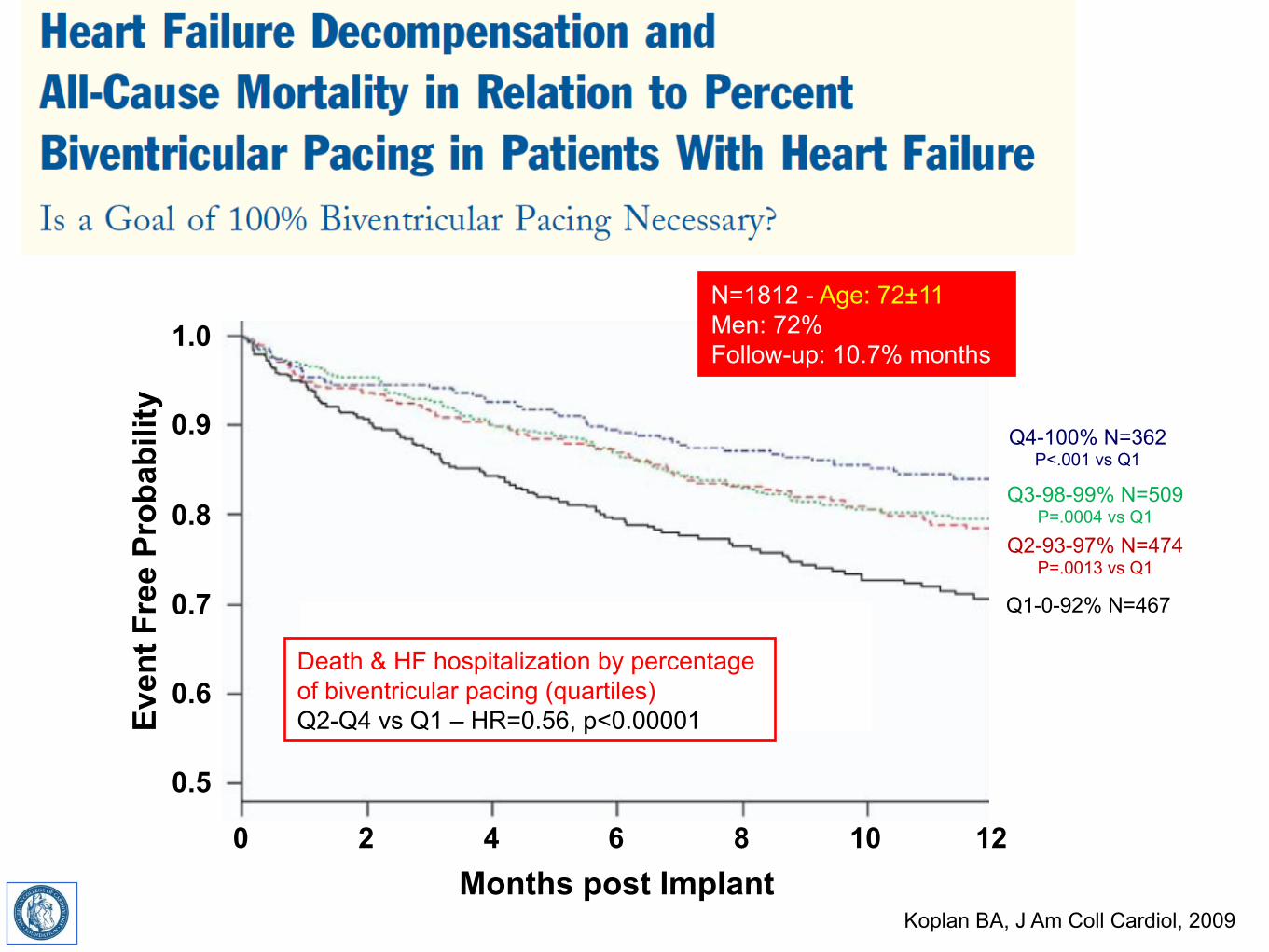
0.5
0.6
0.7
0.8
0.9
0 2
Even
t Fre
e Pr
obab
ility
4 6 8 10
1.0
12 Months post Implant
Q1-0-92% N=467
Q4-100% N=362 P<.001 vs Q1
Q3-98-99% N=509 P=.0004 vs Q1
Q2-93-97% N=474 P=.0013 vs Q1
N=1812 - Age: 72±11 Men: 72% Follow-up: 10.7% months
Death & HF hospitalization by percentage of biventricular pacing (quartiles) Q2-Q4 vs Q1 – HR=0.56, p<0.00001
Koplan BA, J Am Coll Cardiol, 2009
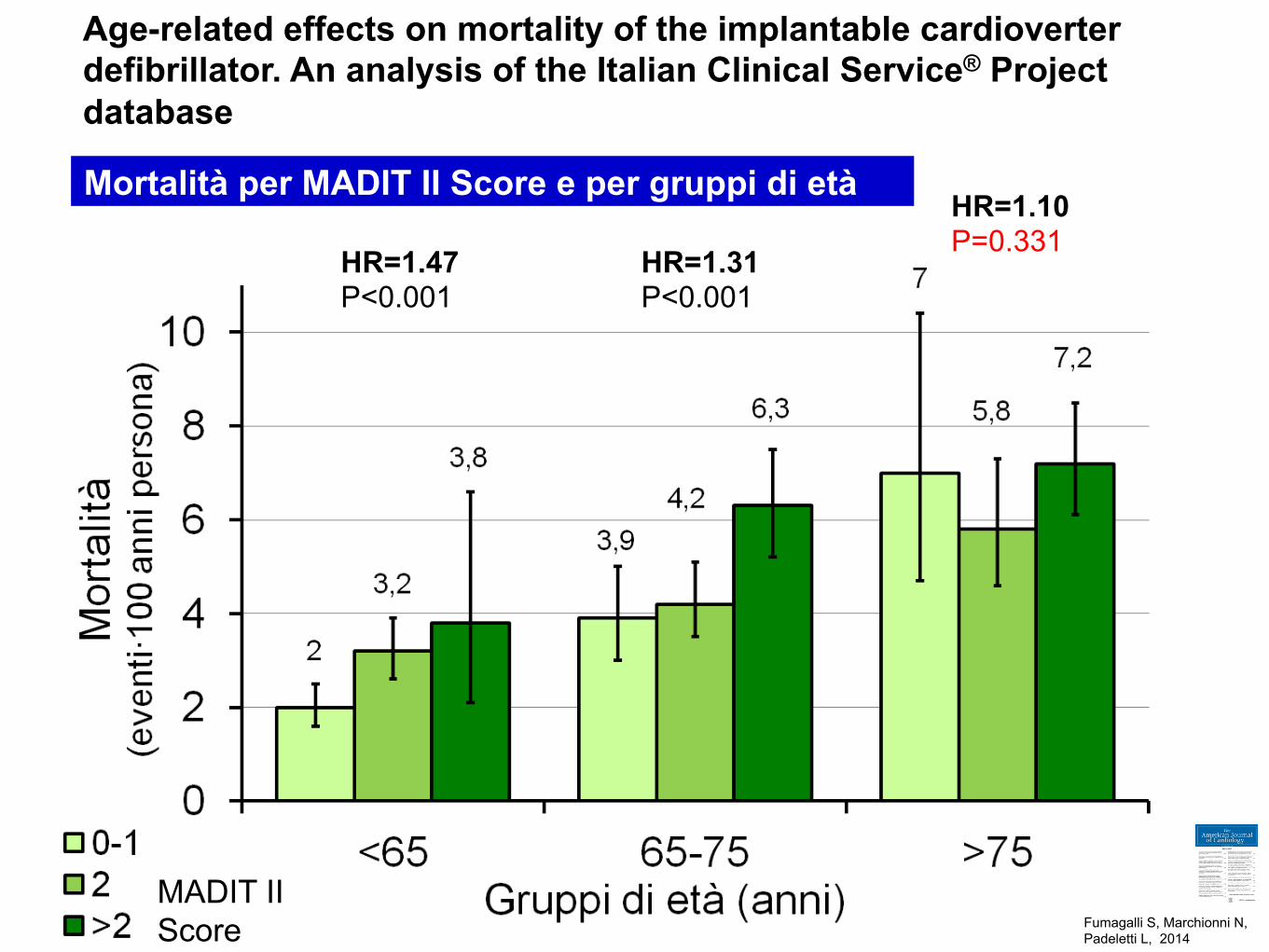
Mortalità per MADIT II Score e per gruppi di età
MADIT II Score
HR=1.47 P<0.001
HR=1.31 P<0.001
HR=1.10 P=0.331
Age-related effects on mortality of the implantable cardioverter defibrillator. An analysis of the Italian Clinical Service® Project database
Fumagalli S, Marchionni N, Padeletti L, 2014 !
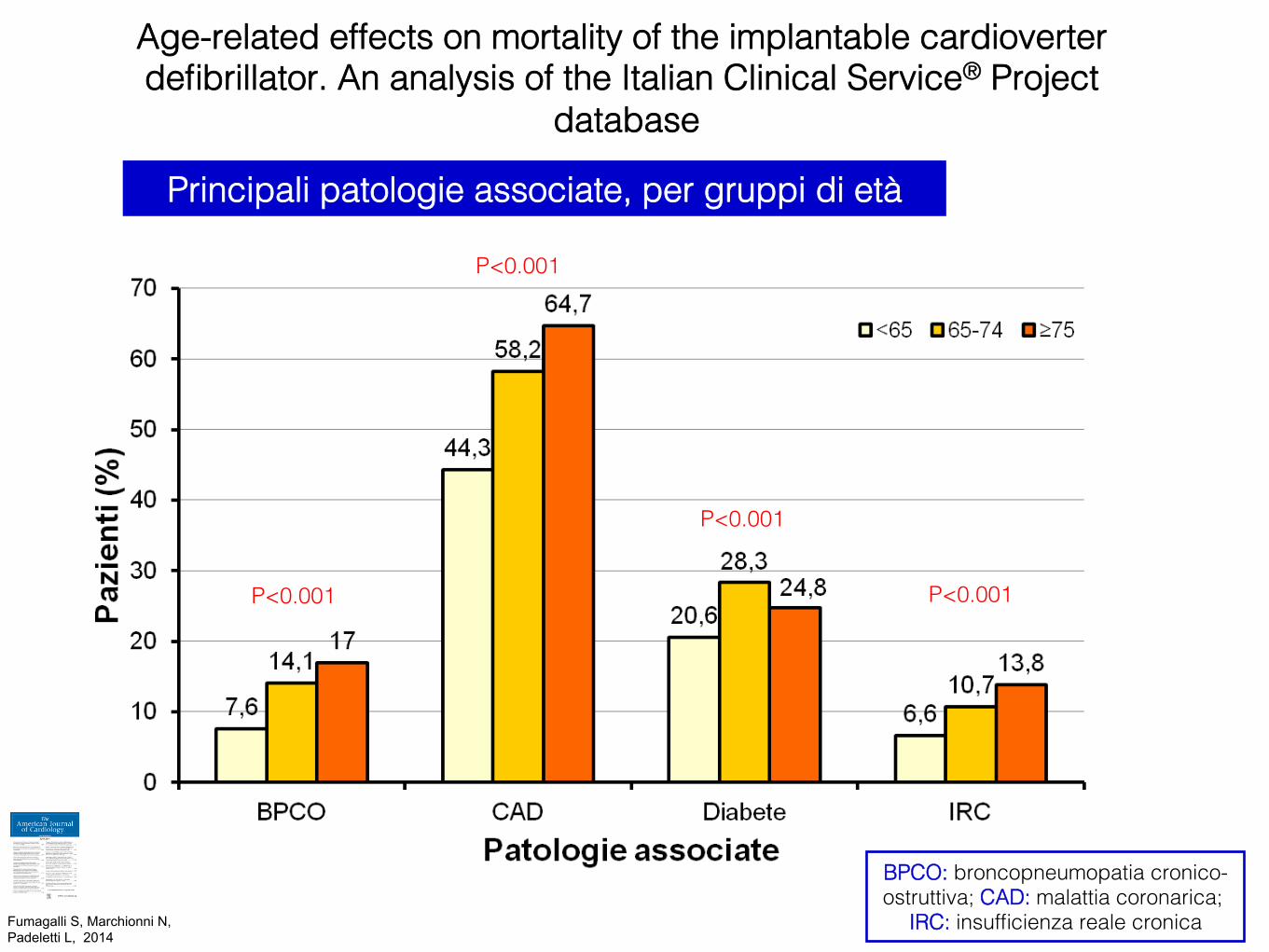
P<0.001!
P<0.001!
P<0.001!
P<0.001!
BPCO: broncopneumopatia cronico-ostruttiva; CAD: malattia coronarica;
IRC: insufficienza reale cronica!
Principali patologie associate, per gruppi di età!
Age-related effects on mortality of the implantable cardioverter defibrillator. An analysis of the Italian Clinical Service® Project
database!
Fumagalli S, Marchionni N, Padeletti L, 2014 !