
Thrombus Aspiration in ST Elevation Myocardial...
32
10.1161/CIRCULATIONAHA.116.025371 1 Thrombus Aspiration in ST Elevation Myocardial Infarction: An Individual Patient Meta-analysis Running Title: Jolly et al.;Thrombus Aspiration in STEMI Sanjit S. Jolly, MD, MSc 1 ; Stefan James MD, PhD 2 ; Vladimír Džavík, MD 3 ; John A. Cairns, MD 4 ; Karim D. Mahmoud, MD, PhD 5 ; Felix Zijlstra, MD, PhD 5 ; Salim Yusuf, MBBS, DPhil 1 ; Göran K. Olivecrona, MD, PhD 6 ; Henrik Renlund, PhD 2 ; Peggy Gao, MSc 1 ; Bo Lagerqvist, MD, PhD 2 ; Ashraf Alazzoni, MD 1 ; Sasko Kedev, MD, PhD 7 ; Goran Stankovic, MD 8 , Brandi Meeks, MEng 1 , Ole Frøbert, MD, PhD 9 1 McMaster University and the Population Health Research Institute, Hamilton Health Sciences, Hamilton, ON, Canada; 2 Department of Medical Science, Uppsala University and Uppsala Clinical Research Centre, Uppsala, Sweden; 3 Peter Munk Cardiac Centre, University Health Network, Toronto, ON, Canada; 4 University of British Columbia, Vancouver, Canada; 5 Department of Cardiology, Thorax Center, Erasmus Medical Centre, Rotterdam, The Netherlands; 6 Skåne University Hospital Lund, Lund University, Lund, Sweden; 7 University Clinic of Cardiology, St. Cyril and Methodius University, Skopje, Macedonia; 8 Clinical Center of Serbia and Department of Cardiology, Medical Faculty, University of Belgrade, Belgrade, Serbia; 9 Örebro University, Faculty of Health, Department of Cardiology, Södra Grev Rosengatan, Örebro, Sweden Address for Correspondence: Sanjit S. Jolly, MD, MSc Hamilton General Hospital Rm. C3 118 CVSRI Building 237 Barton St. East, Hamilton, ON, Canada Tel: 905-524-2712 Fax: 905-297-3785 Email: [email protected] Journal Subject Terms: Percutaneous Coronary Intervention; Catheter-Based Coronary and Valvular Interventions 1 McMaster U r niversity an d t he Population H ealth R esearch Institute, H amilton H ea ea ealt lt l h S S S ci cien en ence ce ces, s Hamilton, O N , Canada; 2 Department of M edical Science, Uppsala Universit y a nd Uppsala Clinic ic i al al l R R R esearc c ch h h C entre , Uppsala, Sweden; 3 Pe ete t t r M unk Cardiac C C en e tre , University H ealth Netw tw wor k , To ro o o nt nt nt o, , O O ON N N , C C an an anad a a a a ; ; ; 4 Un Un Univer rsi si ty of Br Br B it is sh h C h ol ol lum um umbi bi bia, V Van an anco couv ver e , Ca a ana na n da da da ; 5 De e epa pa art rt r me me ment n n of Ca a ard d diology, Thora ax C en en n ter n n , Er Er Erasmus Me Me M d di cal C l en ntre, e, R R t ot te terd rdam am am, Th he e Neth ther r la la lands; 6 Sk k kå ån å e e U Un U iver r s sity Ho Ho Hosp sp spital L L L u u u L L L n n nd, u u u u L Lund nd Uni i ve ve vers r r ity d , Lu Lu L nd nd nd, , , S we e ede de d n; 7 Un Un niv iv iv ersi ty ty ty C C y l in nic c c of Ca C rd d dio io iolo gy , , , St St St . Cy Cy ril a nd d a a Metho dius Univer sity , Skopje, Macedonia; 8 Clinical C enter o r f Serbia a a nd a a D d epar tment of C f ardiol ogy, by guest on December 9, 2016 http://circ.ahajournals.org/ Downloaded from by guest on December 9, 2016 http://circ.ahajournals.org/ Downloaded from by guest on December 9, 2016 http://circ.ahajournals.org/ Downloaded from by guest on December 9, 2016 http://circ.ahajournals.org/ Downloaded from by guest on December 9, 2016 http://circ.ahajournals.org/ Downloaded from by guest on December 9, 2016 http://circ.ahajournals.org/ Downloaded from by guest on December 9, 2016 http://circ.ahajournals.org/ Downloaded from by guest on December 9, 2016 http://circ.ahajournals.org/ Downloaded from by guest on December 9, 2016 http://circ.ahajournals.org/ Downloaded from by guest on December 9, 2016 http://circ.ahajournals.org/ Downloaded from by guest on December 9, 2016 http://circ.ahajournals.org/ Downloaded from
Transcript of Thrombus Aspiration in ST Elevation Myocardial...

10.1161/CIRCULATIONAHA.116.025371
1
Thrombus Aspiration in ST Elevation Myocardial Infarction:
An Individual Patient Meta-analysis
Running Title: Jolly et al.;Thrombus Aspiration in STEMI
Sanjit S. Jolly, MD, MSc1; Stefan James MD, PhD2; Vladimír Džavík, MD3;
John A. Cairns, MD4; Karim D. Mahmoud, MD, PhD5; Felix Zijlstra, MD, PhD5;
Salim Yusuf, MBBS, DPhil1; Göran K. Olivecrona, MD, PhD6 ; Henrik Renlund, PhD2;
Peggy Gao, MSc1; Bo Lagerqvist, MD, PhD2 ; Ashraf Alazzoni, MD1;
Sasko Kedev, MD, PhD7; Goran Stankovic, MD8, Brandi Meeks, MEng1,
Ole Frøbert, MD, PhD9
1McMaster University and the Population Health Research Institute, Hamilton Health Sciences,
Hamilton, ON, Canada; 2Department of Medical Science, Uppsala University and Uppsala
Clinical Research Centre, Uppsala, Sweden; 3Peter Munk Cardiac Centre, University Health
Network, Toronto, ON, Canada; 4University of British Columbia, Vancouver, Canada; 5Department of
Cardiology, Thorax Center, Erasmus Medical Centre, Rotterdam, The Netherlands; 6Skåne University
Hospital Lund, Lund University, Lund, Sweden; 7University Clinic of Cardiology, St. Cyril and
Methodius University, Skopje, Macedonia; 8Clinical Center of Serbia and Department of Cardiology,
Medical Faculty, University of Belgrade, Belgrade, Serbia; 9Örebro University, Faculty of Health,
Department of Cardiology, Södra Grev Rosengatan, Örebro, Sweden
Address for Correspondence:Sanjit S. Jolly, MD, MSc Hamilton General HospitalRm. C3 118 CVSRI Building 237 Barton St. East,Hamilton, ON, Canada Tel: 905-524-2712 Fax: 905-297-3785 Email: [email protected]
Journal Subject Terms: Percutaneous Coronary Intervention; Catheter-Based Coronary andValvular Interventions
1McMaster Ur niversity and the Population Health Research Institute, Hamilton Heaeaealtltl h SSScicienenencececes,s
Hamilton, ON, Canada; 2Department of Medical Science, Uppsala University and Uppsala
Clinicici alall RRResearccchhh Centre, Uppsala, Sweden; 3Peetett r Munk Cardiac CCene tre, University Health
Netwtwwork, Torooontntnto,, OOONNN, CCanananada aaa;;; 4UnUnUniverrsisity of BrBrB itisshh Ch olollumumumbibibia, VVananancocouvvere , Caaananan dadada;;; 5Deeepapaartrtr memementnn of
Caaardddiology, Thoraxax Cenennternn , ErErErasmus MeMeM ddical Cl enntre,e, RR totteterdrdamamam,RRR Thhee Neththerrrlalalands; 6Skkkåånå ee UUnU iverrssity
HoHoHospspspital LLLuuuLLLL nnnd,uuuu LLundnd Uniiveveversrr ityyyd ,,, LuLuL ndndnd,,, Sweeededed n; 7UnUnniviviversitytyty CCy linniccc of CaC rdddioioiologyyy,, , StStSt. CyCyril anddaa
Methodius University, Skopje, Macedonia; 8Clinical Center or f Serbia aa ndaa Dd epartment of Cf ardiology,
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from

10.1161/CIRCULATIONAHA.116.025371
2
Abstract
Background—Thrombus aspiration during percutaneous coronary intervention (PCI) for the treatment of ST elevation myocardial infarction (STEMI) has been widely used; however, recent trials have questioned its value and safety. In this meta-analysis, we, the trial investigators, aimed to pool the individual patient data from these trials to determine the benefits and risks of thrombus aspiration during PCI in patients with STEMI. Methods—Included were large (Nthrombectomy vs. PCI alone in patients with STEMI. Individual patient data was provided by the leadership of each trial. The pre-specified primary efficacy outcome was cardiovascular (CV) mortality within 30 days and the primary safety outcome was stroke or transient ischemic attack (TIA) within 30 days. Results—The 3 eligible randomized trials (TAPAS, TASTE and TOTAL) enrolled 19,047 patients, of whom 18,306 underwent PCI and were included in the primary analysis. CV death at 30 days occurred in 221 (2.4%) of 9155 patients randomized to thrombus aspiration and 262 (2.9%) of 9151 randomized to PCI alone (hazard ratio (HR) 0.84; 95% CI 0.70-1.01, p=0.06). Stroke or TIA occurred in 66 (0.8%) randomized to thrombus aspiration and 46 (0.5%) randomized to PCI alone (odds ratio [OR] 1.43 95% CI 0.98-2.1, p=0.06). There were no significant differences in recurrent myocardial infarction, stent thrombosis, heart failure or target vessel revascularization. In the subgroup with high thrombus burden (TIMI thrombus grade 3) thrombus aspiration was associated with less CV death (170 [2.5%] vs. 205 [3.1%] HR 0.80; 95% CI 0.65-0.98, p =0.03), and with more stroke or TIA (55 [0.9%] vs. 34 [0.5%] OR 1.56;95% CI 1.02-2.42, p=0.04). However, the interaction p-values were 0.32 and 0.34, respectively. Conclusions—Routine thrombus aspiration during STEMI PCI did not improve clinical outcomes. In the high thrombus burden subgroup the trends toward reduced CV death and increased stroke or TIA provide a rationale for future trials of improved thrombus aspiration technologies in this high-risk subgroup.
Clinical Trial Registration—ClinicalTrials.gov identifier NCT02552407, PROSPERO CRD42015025936
Key words: meta-analysis; myocardial infarction; thrombectomy
( [ ] , p )ignificant differences in recurrent myocardial infarction, stent thrombosis, heart fafaailililururu e e e ororr tttararargegg t
vessel revascularization. In the subgroup with high thrombus burden (TIMI thrombmbmbususu gggrararadedede 3)3)3 hrombus aspiration was associated with less CV death (170 [2.5%] vs. 205 [3.1%] HR 0.80;
95% CI 0.65-0.98, p =0.03), and with more stroke or TIA (55 [0.9%] vs. 34 [0.5%] OR 1.56R ;95% CI 1.02-2.42, p=0.04). However, the interaction p-values were 0.32 and 0.34, respectively. Conccclululusisis onnonsss——Roouutine thrombus aspiration duringg STEMI PCI ddidid notot improve clinicaloutccooomes. In tthehehe hhhigiggh thththrororombmbmbususus bbburururden n subgroooupu thhe ttrererendndndsss tott wawaarddd rer duduced d d CVCVCV dddeae thhh aaandndnd ncrreeased stroke or TIIAAA proovivividdde a ratatatioonnale forr futtuure trrtrials ooof ff imprproveded thrhrhroombus s aasa ppirrration echhhnnon logies inn n thtt isis higigh-risksksk subgroupp.
CClili inicall lCCC Triall Re igiistra ition—CClinici lalTriiai ls.gov iidded ntififier NCNCCT00T 2255522404007, PRROSSSPE ORORO C 4201 02 936
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from

10.1161/CIRCULATIONAHA.116.025371
3
Clinical Perspective
What is new?
This is an individual patient meta-analysis of more than 18,000 patients with STEMI
randomized to thrombus aspiration vs. PCI alone.
As a routine strategy, thrombus aspiration did not reduce in cardiovascular mortality for
STEMI patients undergoing primary PCI.
An exploratory analysis of patients with high thrombus burden suggests that thrombus
aspiration may improve CV mortality but at the price of an increased risk of stroke or
TIA.
What are the clinical implications?
Thrombus aspiration should not be used as a routine strategy in patients with STEMI.
Further larger randomized trials are needed to determine if improved forms of thrombus
aspiration can reduce CV mortality and to determine its safety with regards to stroke.
Thrombus aspiration should not be used as a routine strategy in patients wwitith h h STSTSTEMEMEMI.I.I
Further larger randomized trials are needed to determine if improved forms of thrombus
aspiration can reduce CV mortality and to determine its safety with regards to stroke.
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from

10.1161/CIRCULATIONAHA.116.025371
4
Introduction
The optimal treatment for ST elevation myocardial infarction (STEMI) is rapid reperfusion with
timely primary percutaneous coronary intervention (PCI) if available.1 However, one of the
limitations of primary PCI is embolization of thrombus distally and microvascular occlusion,
associated with markedly increased mortality.2 Thrombus aspiration was thought to be a simple
method to remove thrombus prior to stent deployment, thereby reducing distal embolization and
improving outcomes.
Thrombus aspiration became part of routine practice based on the promising results of an
early trial.3, 4 However, the results of more recent, larger, multicenter trials have created
uncertainty about the benefit of thrombus aspiration and suggested possible harm from increased
stroke risk.5-9 None of the individual trials were powered to detect a modest reduction in
mortality (e.g. 20%) or of low frequency events such as stroke. Accordingly, we undertook an
individual patient level meta-analysis to determine the effect of thrombus aspiration on 30-day
cardiovascular mortality and stroke or transient ischemic attack (TIA).
Methods
The meta-analysis was performed in accordance with the PRISMA (Preferred Reporting Items
for Systematic Review and Meta-Analyses) guidelines for individual patient data
meta-analyses.10 The protocol was finalized and registered at PROSPERO (international register
of systematic reviews, CRD42015025936) and clinicaltrials.gov (NCT02552407) prior to
unblinding or any data analysis. Large randomized trials (recruiting 1000 patients or more) that
compared manual thrombus aspiration plus PCI and PCI alone in patients with STEMI were
eligible. Large randomized trials were only included as small trials are more susceptible to
uncertainty about the benefit of thrombus aspiration and suggested possible harmm frfrromomom ininncrcrcreaeaeasses d
troke risk.5-9 None of the individual trials were powered to detect a modest reduction in
mortality ((e.g. 20%) or of low frequency events such as stroke. Accordingly, we undertook an
ndiivivividual patieieienntn llevee elelel mmmetete a-anananalalalysysysis tto o determmminee the e efefeffefefectctct of f ththhroror mbmbusu aspspspiriri atatatioioion onono 3330-0-0 dadaday yy
cardddioioi vascularr mmmororttaliity andndd stroke or trtransiennnt ischchemmmicicic aaatttttacack (TTIA)..
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from

10.1161/CIRCULATIONAHA.116.025371
5
publication bias and tend to be lower quality. A comprehensive search strategy was used for
Medline, EMBASE and Cochrane Central Register of Controlled Trials on September 2, 2016
with no language restriction (online appendix).
Authors of eligible trials collaboratively shared individual patient level data. The
databases from the individual trials were merged into a dedicated SAS file set up for the present
study. Data-sets were rigorously reviewed for completeness and consistency to ensure that no
errors had occurred in reformatting of the data, and to ensure agreement with the original
publications. Any differences were resolved by queries within the collaborative group.
Variables were not defined according to identical criteria in the studies but common definitions
were defined by consensus within the author group, whenever possible. Please refer to online
supplement for details regarding outcomes variables. The TAPAS trial did not prospectively
collect stroke or TIA data and was not included for this outcome. Outcomes were not adjudicated
in TASTE and were from discharge diagnoses in administrative databases and death registry.
The risk of bias was assessed as per the Cochrane Collaboration tool (figure S1).
The three individual trials (TASTE, TAPAS and TOTAL) were each approved by an
institutional review committee and participants provided informed consent.
Study Organization
All data were merged at the Uppsala Clinical Research Center (UCR), Sweden and analyses
were performed using R version 3.2 (R Foundation for Statistical Computing, Vienna, Austria).
Kaplan Meier curves and forest plot figures were created at the Population Health Research
Institute (PHRI), Canada using S-PLUS (TIBCO Software Inc, Palo Alto, Ca).
Statistical Analysis
were defined by consensus within the author group, whenever possible. Please reffererr ttto oo onono lililinenene
upplement for details regarding outcomes variables. The TAPAS trial did not prospectively
collect stroke or TIA data and was not included for this outcome. Outcomes were not adjudicated
n TTAASA TE anddd wwwererereee frfrromomm dddischchchararargegege diagagnoses s s inii aaddmininnisisistrtrtratatativii e e dadadatatababases s ananand d d dededeataa h rerer gigigistststryryry.
Thee e rrir sk of biaasas wwass aasssesseeedd d as per thee Cochrrranne CoCollllllabababorooratatioon totool (fifiguguureere S1).
ThT e thht ree iindidi iviiddu lal t irials (T( ASASTET , TAAAPAAASS and TOOO ATAT )L) were ea hch approvedd bby an
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from

10.1161/CIRCULATIONAHA.116.025371
6
For baseline characteristics, the Wilcoxon rank sum test was used for continuous variables and
Pearson chi square test for categorical variables. The pre-specified primary efficacy outcome was
cardiovascular death at 30 days. The pre-specified primary safety outcome was stroke or TIA at
30 days. The pre-specified primary analysis was a modified intention to treat analysis that
included all randomized patients who had undergone emergency PCI for STEMI with all
analyses conducted according to the originally allocated study group. Patients who did not
undergo PCI for STEMI (i.e. normal coronary arteries) were not included in the primary analysis.
A fixed effect model was used and study level was used as a covariate in analyses and study
level interaction p values were reported.
A p-value of less than 0.05 was considered statistically significant. Hazard ratios and
their 95% confidence intervals (CI) were estimated using a Cox proportional hazards regression
model with treatment group as the predictor variable and p values were used from cox regression.
For outcome of stroke or TIA, the exact time of event was not available during initial
hospitalization in the TASTE trial so logistic regression was used for significance testing and to
calculate odds ratios and 95% CI with treatment group as the predictor variable.
Subgroup Analyses
We hypothesized that thrombus aspiration might be more effective in patients with higher
thrombus burden. Accordingly, pre-specified subgroup analyses were performed comparing
Thrombolysis In Myocardial Infarction (TIMI) thrombus grade <3 vs. and <4 vs. .
Additional pre-specified subgroup analyses were based on time from symptom onset (<6 vs.
6-12 hours vs. >12 hours), initial TIMI flow (0-1 vs. 2-3), lesion location (proximal vs.
non-proximal vessel), tertiles of site primary PCI volume and use of a glycoprotein IIb/IIIa
A p-value of less than 0.05 was considered statistically significant. Hazard d rararatitioos s s ananand d d
heir 95% confidence intervals (CI) were estimated using a Cox proportional hazards regression
model with treatment group as the predictor variable and p values were used from cox regression
For r oooutcome ofofof strrrokoo eee ororr TTTIAIAA, thththe e e exexe acctt time ofofof evevent wwwasasas nnnotoo aavvavailili aba lele duririringngng iiinininitial
hospspspitii alizationnn ininin tthhe TTASTETETE trial so looggistic rrreegreesssioioion nn wawaw s uusedd ffor ssiggnnin ffif cance teet sttinng andd tto d
callc lulatte odddsdd ratiios andd 995%% CI wiithh treatment group as thhe pr dedici tor va iri babble.
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from

10.1161/CIRCULATIONAHA.116.025371
7
inhibitor. Statistical interactions were evaluated at a significance level of 0.05 with no
adjustment made for multiple comparisons.
Results
Of the 19,047 patients enrolled in the three randomized trials, 18,306 underwent PCI and were
included in the primary analysis (figure 1). The individual trials (table S1, figures S2 and S3)
included were the The Thrombus Aspiration during Percutaneous Coronary Intervention in
Acute Myocardial Infarction Study (TAPAS, N=1,071)4, Thrombus Aspiration in ST-Elevation
Myocardial Infarction in Scandinavia (TASTE, N=7,244)11 and routine aspiration
ThrOmbecTomy with PCI versus PCI ALone in Patients with STEMI (TOTAL, N=10,732)7.
These three large trials accounted for 19,047 patients out of 22,057 patients enrolled in manual
thrombus aspiration trials.
Baseline characteristics were well balanced except that the proportion of smokers was
less in the thrombus aspiration group (39.9% vs. 42.4%; p<0.001; Table 1) and the interval from
symptom onset to hospital arrival was longer in the thrombus aspiration group (190 vs. 185.5
min; p=0.025; Table 1). The majority of patients had TIMI 0 or 1 flow in the infarct artery at
baseline.
In the thrombus aspiration group, direct stenting was more frequent (39.5% vs. 21.1%,
p<0.001) and GP IIb/IIa use was slightly lower (32.3% vs. 35.1%, p<0.001). The rate of
cross-over from assigned thrombus aspiration to PCI alone was 5.5% and from PCI alone to
thrombus aspiration was 6.8%. Fluoroscopy time was slightly longer with thrombus aspiration
(13.2 min vs. 12.3 min, p<0.001, Table 1). Stent length, stent diameter and number of stents
were not different between the groups.
ThrOmbecTomy with PCI versus PCI ALone in Patients with STEMI (TOTAL, N=N==10101 ,7,77323232)))777.
These three large trials accounted for 19,047 patients out of 22,057 patients enrolled in manual r
hrombus aspiration trials.
Baselinenene chahaharaaactc erererisissticscscs wwwererere e wewell balanana ced d excececeptptpt thththata ththhe prpropporo tiononon ooof f f smsmsmokkkererrss s wawawas ss
essss inini the thromomombuuss aasppiratitiioono grouppp (3939.9% vsvsv . 4242.44%;%;%; ppp<0<0<0.0001; Tablee 11)1 and theee iinteterval frorom
ymptom onset to hhhos ipitall ar irival was llonger iiin hthhe hthrombbbus aspiiratiion group (1119090 vs. 11885.5
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from

10.1161/CIRCULATIONAHA.116.025371
8
Efficacy and Safety
The primary efficacy outcome of cardiovascular death within 30 days in patients who had
undergone PCI for STEMI was 2.4% in the thrombus aspiration group, compared with 2.9% in
the PCI alone group (hazard ratio 0.84; 95% CI 0.70-1.01, p=0.06 study level interaction p=0.05,
Figure 2, Table 2). The primary safety outcome of stroke or TIA at 30 days was 0.8% in the
thrombus aspiration group compared with 0.5% in the PCI alone group (odds ratio ratio 1.43;
95% CI 0.98-2.1, p=0.06), but with significant study level interaction p=0.02. There were no
statistically significant differences in recurrent myocardial infarction, stent thrombosis or target
vessel revascularization (Table 2). At 1 year, the rate of cardiovascular death was 3.7% in the
thrombus aspiration group compared with 4.2% in the PCI alone group (hazard ratio 0.90; 95%
CI 0.78-1.04, p=0.15, Figure 2).
Subgroup Findings
In those with thrombus aspiration was
associated with reduced cardiovascular death (2.5% vs. 3.1%, hazard ratio 0.80; 95% CI
0.65-0.98, p= 0.03) with no significant heterogeneity across studies (study level interaction
p=0.22). However, this subgroup had an excess in stroke or TIA (0.9% vs. 0.5% odds ratio 1.56;
95% CI 1.02-2.42, p= 0.04, Table 3) with no significant heterogeneity across studies (study level
interaction p=0.09). In the low thrombus burden subgroup (TIMI Thrombus Grade <3), there
were no differences in cardiovascular death (2.2% vs. 2.2%, hazard ratio 1.00; 95% CI
0.68-1.47) or in stroke or TIA (0.5% vs. 0.5%, odds ratio 0.99; 95% CI 0.43-2.26). Interaction
p-values for differences in cardiovascular death and for stroke or TIA, according to the TIMI
thrombus grade 3 cut point were not statistically significant (p = 0.32 and 0.34, respectively,
Table 3).
hrombus aspiration group compared with 4.2% in the PCI alone group (hazard raatitio o o 0.0 909090;;; 959595%%%
CI 0.78-1.04, p=0.15, Figure 2).
Subgroupp Findings
n ththooose with thththroror mbmbusu aaaspspspiririratatatioioi n wawawasss
assoooccic ated withh rrer duduceedd cardrdrdioi vascularr ddeath (2(2( .5% % vsvsvs.. 333.1%1%1%, hazazard rrattiooo 000.80; 95%5%5 CCI
00.665 0-0 9.998, p= 00.0303) withht no isignifici ant hheh terogeneity across studidies ((studdy llevel inii teractiion
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from
10.1161/CIRCULATIONAHA.116.025371
9
When a cut point of TIMI thrombus , there were
similar patterns for cardiovascular death (2.7% vs. 3.2%, hazard ratio 0.82; 95% 0.66-1.02, p
=0.08, subgroup interaction p=0.67, study level interaction p=0.43) and stroke or TIA within 30
days (1.0% vs. 0.6%, odds ratio 1.87; 95% CI 1.18-3.02, P=0.009, subgroup interaction p=0.04,
study level interaction p=0.41, Table 3).
There appeared to be a greater benefit for thrombus aspiration in patients receiving a GP
IIb/IIIa inhibitor for cardiovascular death within 30 days (interaction p=0.048) but there was also
increased risk of stroke or TIA (interaction p=0.04, Figure 3a and 3b). There appeared to be a
potential benefit in patients presenting within 6 hours for CV death but also harm in terms of
stroke (Figure 3a and 3b).
Discussion
In contrast to traditional meta-analyses summarizing group data, the present meta-analysis
used individual patient data which provided considerably greater power to examine important but
low frequency events such as cardiovascular death and stroke and it allowed the evaluation of
specific subgroups such as the one with a high thrombus burden. The protocol was finalized
and registered prior to starting the analysis as per the PRISMA guidelines for individual patient
data meta-analyses.10
At 30 days, there were no statistically significant differences for cardiovascular mortality,
all-cause mortality between a strategy of routine manual thrombus aspiration vs PCI alone
overall.
Although there were no statistically significant subgroup interactions, in the subgroup of
patients with high thrombus burden, there was a nominal reduction in CV mortality and in
troke (Figure 3a and 3b).
Discussion
n ccononontrast to tttrararadiiititiionnnalalal mmmete aaa---anananalalalysysy es s sus mmarara izining grgrgrouououppp dadd taa,, thhhee prrese ent t t memem ta-anananalalalysysysisisis
usededed individuaaall papatiiennt dataaa wwwhich ppprovivided cooonnsidderababablylyly gggrereaater ppowerer tooo eexe aminne e immpportannt bu
ow ffrequency events suchh as cardiiovascular dded athh h andd strokke a dnd it allllowedd the ev lalua ition of
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from

10.1161/CIRCULATIONAHA.116.025371
10
all-cause mortality but an increase in stroke or TIA at 30 days. It is biologically plausible that
thrombus aspiration is only beneficial in patients with moderate to high thrombus burden. On
the other hand, if the mechanism of stroke is embolization of thrombus from the coronary artery
to systemic circulation, it is logical that the risk would be higher in patients with high thrombus
burden. Finally, in patients with high thrombus burden, the increase in stroke could
counterbalance an early benefit such that the effect on all-cause mortality at 1 year was neutral.
For stroke or TIA, there was a significant study level interaction. One potential reason
is that the TASTE trial randomized patients after angiography while TOTAL and TAPAS did so
pre-angiography and so it is possible that angiographic anatomy varied between the studies.
Thrombus burden has been linked to stroke risk and one hypothesis is that TOTAL had a higher
stroke risk with thrombus aspiration due to inclusion of patients with a higher thrombus burden.8
To support this hypothesis, in the subgroup of patients with high thrombus burden, we found
consistency at the study level for effect of thrombus aspiration on both CV death and stroke or
TIA. However, these results should be interpreted cautiously, given this is a post hoc analysis.
Furthermore, an important limitation is that TAPAS did not collect stroke or TIA and neurologic
events were not adjudicated in TASTE.
Limitations of current manual thrombus aspiration technology include thrombus
embolization downstream due to wire crossing (prior to aspiration), limited ability to deal with
large organized thrombi, and embolization of thrombus to other vascular territories during
removal of the aspiration catheter. These limitations are consistent with the TOTAL optical
cohence tomography substudy which showed a similar residual thrombus volume after routine
thrombus aspiration and after balloon angioplasty.12
Thrombus burden has been linked to stroke risk and one hypothesis is that TOTAALL hahah d d d a aa hihihighghgheer
troke risk with thrombus aspiration due to inclusion of patients with a higher thrombus burden.8
To support this hypothesis, in the subgroup of patients with high thrombus burden, we found
connsisisistency att tthhhe ssstudydydy llleveve ell fffororo eeeffffffect t ofo thromomo buus assspipipirararatititionoo oonn n bobob thh CCV dededeatatathhh anaa d ststrororokekeke ooor
TIAA.A. Howeveveverr,r tthhese resuulu ttst should bebe interprprp eteded cccauauautitit ououo sls yy, ggivven tthhiss iisi a postt t hohoc analysiis.
Furthhermore, an iimporttant lilimitation iis that TAAPA ASASA ddiid not collllect str koke or TIAAA a dnd neurollogiic
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from
10.1161/CIRCULATIONAHA.116.025371
11
Innovations in device technology should focus on reducing the risk of systemic
embolization of thrombus during thrombus aspiration in addition to improving efficacy. It is
conceivable that improved forms of thrombus aspiration that mitigate stroke risk could reduce
cardiovascular mortality in patients with high thrombus burden. The effects on cardiovascular
mortality and stroke or TIA observed in this meta-analysis in the high thrombus burden subgroup,
should be considered exploratory given that the subgroup interactions were not statistically
significant and that there was no adjustment for multiple testing. These findings could serve as a
basis for much larger trials with new devices that reduce the risk of systemic embolization.
Such trials would need to enroll 26,000 patients with a high thrombus burden to be powered for a
20% reduction in cardiovascular mortality based on the event rates observed in this data-set. The
feasibility of such a trial may be questioned, however, the large fibrinolytic trials enrolled similar
numbers of patients.
The finding that thrombus aspiration may reduce cardiovascular mortality but increase
stroke or TIA in those treated with GP IIb/IIIa inhibitors should be interpreted cautiously. First,
GP IIb/IIIa inhibitors use is likely highly correlated to thrombus burden. Second, these were
open label trials and GP IIb/IIIa use is a post randomization variable that may be impacted by
knowledge of treatment assignment and procedural complications such as no reflow.
This individual patient meta-analysis is novel because it utilized cause-specific mortality
(CV mortality) compared to all-cause mortality presented in the original TASTE and TAPAS
publications.3, 11 This is important as cause-specific mortality is more likely to be responsive to
the intervention than all-cause mortality and thus increases study power. Furthermore, we
pre-specified our primary outcome at 30 days instead of 180 days (primary outcome of TOTAL)
as we hypothesized that the greatest benefit may be early for a one time intervention compared to
20% reduction in cardiovascular mortality based on the event rates observed in thihis s dadad tataa--seseet.t.t ThTT e
feasibility of such a trial may be questioned, however, the large fibrinolytic trials enrolled similar
numbers of patients.
The findndndinng g g thhatata ttthrhrhromommbububus s s asasa piraration mmmaya reeducccee e cacaardrdrdioovavaascscs ulu arar moortrtrtalala ititity y y bub t ininncrcrcreaeaeasesese
troookekek or TIA ininn thohosee ttreatededed with GP IIb/IIIaaa iinhhibbitttorororsss shshshouould bbee inteerrprerereted cautututiioususly. Firrst,
GGP IIb/b/III Ia iinhhibibiitors use iis llikikely hihi hghlly correlated d to thrombbub s bburdden. SSecondd, thhese were
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from

10.1161/CIRCULATIONAHA.116.025371
12
an ongoing therapy. Finally, we had detailed baseline data and were able to examine the effect of
thrombus aspiration on important subgroups based on thrombus burden and time of symptom
onset, both factors which may predict benefit of thrombus aspiration.
Limitations of this analysis are related to limitations of the datasets of the individual trials.
The TAPAS did not prospectively collect the outcome of nonfatal stroke and was not included in
the stroke analyses.3 Direct stenting was recommended in TAPAS but not in the other trials.
TASTE collected the composite outcome of stroke or TIA but not stroke alone, necessitating the
composite of stroke or TIA as safety outcome in our meta-analysis.11 The time of stroke or TIA
during the initial hospitalization was not collected in TASTE so a time to event analysis was not
possible for this outcome. Outcomes in the TASTE trial were from administrative databases,
clinical registries and death certificates and were not adjudicated. Another limitation is that
thrombus grade was assessed prior to wire crossing in both TAPAS and TOTAL and after wire
crossing in TASTE. There was no adjustment for multiple comparisons so all secondary
analyses should be considered hypothesis generating. Another limitation is that no adjustment for
clustering was performed. Finally, despite nearly 20,000 patients randomized, this analysis still
was relatively underpowered to detect a modest but clinically important, 20% relative risk
reduction in cardiovascular mortality within 30 days.
Conclusions
Routine manual thrombus aspiration during STEMI PCI did not improve clinical outcomes
overall. Whether improved methods for thrombus aspiration could reduce the risk of stroke and
enhance overall benefit is not known, and warrants testing in future trials among patients with
high thrombus burden.
possible for this outcome. Outcomes in the TASTE trial were from administrativive e e dadad tatatabababaseseesss,
clinical registries and death certificates and were not adjudicated. Another limitation is that
hrombus ggrade was assessed prior to wire crossing in both TAPAS and TOTAL and after wire
crosssisising in TAAASSSTE.EE ThThTherere e wawawasss nonono adjdjusu tmennnt t foorr muuultltltipipiplelele ccommmpapaparirisoonsn sooo alalall l l sesesecondnddararary y y
analalalyysy es shoulldd d bee connssidererered hypotheesiis generere atining.. AnAnAnotoothehherr limimitationon iiis that no o aadjujustmennt fo
lcluste iring was performedd. Fiinally, ddespite nearlly 2200,000 patients randod imized, thihis an lalysiis s itillll
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from

10.1161/CIRCULATIONAHA.116.025371
13
Disclosures
During the conduct of the TOTAL trial, SSJ received an institutional research grant from
Medtronic. During the conduct of the TASTE trial SJ received institutional research grants
from Medtronic, Vascular Solutions and Terumo Inc. Thereafter he has received institutional
research grants from Boston Scientific, Abbot Vascular, Astra Zeneca and The Medicines
Company. He has received honoraria from Astra Zeneca, The Medicines Company, Bayer and
Boston Scientific.
References
1. Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: A quantitative review of 23 randomised trials. Lancet. 2003;361:13-20.
2. Henriques JP, Zijlstra F, Ottervanger JP, de Boer MJ, van 't Hof AW, Hoorntje JC, Suryapranata H. Incidence and clinical significance of distal embolization during primary angioplasty for acute myocardial infarction. Eur Heart J. 2002;23:1112-1117.
3. Svilaas T, Vlaar PJ, van der Horst IC, Diercks GF, de Smet BJ, van den Heuvel AF, Anthonio RL, Jessurun GA, Tan ES, Suurmeijer AJ, Zijlstra F. Thrombus aspiration during primary percutaneous coronary intervention. N Engl J Med. 2008;358:557-567.
4. Vlaar PJ, Svilaas T, van der Horst IC, Diercks GF, Fokkema ML, de Smet BJ, van den Heuvel AF, Anthonio RL, Jessurun GA, Tan ES, Suurmeijer AJ, Zijlstra F. Cardiac death and reinfarction after 1 year in the thrombus aspiration during percutaneous coronary intervention in acute myocardial infarction study (tapas): A 1-year follow-up study. Lancet. 2008;371:1915-1920.
5. Frobert O, Lagerqvist B, Gudnason T, Thuesen L, Svensson R, Olivecrona GK, James SK. Thrombus aspiration in st-elevation myocardial infarction in scandinavia (taste trial). A multicenter, prospective, randomized, controlled clinical registry trial based on the swedish angiography and angioplasty registry (scaar) platform. Study design and rationale. American heart journal.160:1042-1048.
6. Lagerqvist B, Frobert O, Olivecrona GK, Gudnason T, Maeng M, Alstrom P, Andersson J, Calais F, Carlsson J, Collste O, Gotberg M, Hardhammar P, Ioanes D, Kallryd A, Linder R, Lundin A, Odenstedt J, Omerovic E, Puskar V, Todt T, Zelleroth E, Ostlund O, James SK. Outcomes 1 year after thrombus aspiration for myocardial infarction. N Engl J Med. 2014;371:1111-1120.
7. Jolly SS, Cairns JA, Yusuf S, Meeks B, Pogue J, Rokoss MJ, Kedev S, Thabane L, Stankovic G, Moreno R, Gershlick A, Chowdhary S, Lavi S, Niemela K, Steg PG, Bernat I, Xu Y, Cantor WJ, Overgaard CB, Naber CK, Cheema AN, Welsh RC, Bertrand OF, Avezum A, Bhindi R, Pancholy S, Rao SV, Natarajan MK, Ten Berg JM, Shestakovska
1. Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous s ththhrororombmbmbolololytytyticici therapy for acute myocardial infarction: A quantitative review of 23 randoomimimisesed d d trtrtriaiaialslsls..Lancet. 2003;361:13-20.
2. Henriques JP, Zijlstra F, Ottervanger JP, de Boer MJ, van 't Hof AW, Hoorntje JC, Suryapranata H. Incidence and clinical significance of distal embolization during primaryananangigigiopopoplalal sty y for acute myocardial infarction.n. Eur Heart J. 202 02;2;23:1112-1117. JJ
3. Svilaasss TTT, VlVV aaaar r PJPJPJ,, vavaann n dedederr r Hoorsrst IC, DiDD errccks GFGFGF, , dedede Smmemettt BJB , vav n dededen n n HeHeH uvelele AAAF,F,F, Anthonio RRL, JJeeessurururunn GAA, TaTTan n ES, SuSuurmem ijjeer AJ,, ZZZijlsstrra F. TThrhrroomo bus asasaspiiraaation during ppprirr mam ryy percucuuttat neous coorronaryyy inntererveeentntntioioionnn. N N N Englg J MMededd. 22008;358585 :55557-5677.
4. VVVlaararar PPPJJJ, SSvvilaaaas T, vavavan nn deeerr r HoHoHorsrsrst tt ICCC,, DDiD errcckss s GGFG , ,, FoFoFokkkkememma MLML, dedede SSSmememett t BBBJ,, vvan deen HeH uv lel AAF, AAntthho inio RL, Jessurun GGAA,A TTan ES, Suurm ieijjej r AAJ, iZijljlstra F. CCarddiiac ddeathh
d i f i f i h h b i i d i
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from

10.1161/CIRCULATIONAHA.116.025371
14
O, Gao P, Widimsky P, Dzavik V, Investigators T. Randomized trial of primary pci with or without routine manual thrombectomy. N Engl J Med. 2015;372:1389-1398.
8. Jolly SS, Cairns JA, Yusuf S, Meeks B, Gao P, Hart RG, Kedev S, Stankovic G, Moreno R, Horak D, Kassam S, Rokoss MJ, Leung RC, El-Omar M, Romppanen HO, Alazzoni A, Alak A, Fung A, Alexopoulos D, Schwalm JD, Valettas N, Dzavik V, Investigators T. Stroke in the total trial: A randomized trial of routine thrombectomy vs. Percutaneous coronary intervention alone in st elevation myocardial infarction. Eur Heart J.2015;36:2364-2372.
9. Jolly SS, Cairns JA, Yusuf S, Rokoss MJ, Gao P, Meeks B, Kedev S, Stankovic G, Moreno R, Gershlick A, Chowdhary S, Lavi S, Niemela K, Bernat I, Cantor WJ, Cheema AN, Steg PG, Welsh RC, Sheth T, Bertrand OF, Avezum A, Bhindi R, Natarajan MK, Horak D, Leung RC, Kassam S, Rao SV, El-Omar M, Mehta SR, Velianou JL, Pancholy S, Dzavik V, Investigators T. Outcomes after thrombus aspiration for st elevation myocardial infarction: 1-year follow-up of the prospective randomised total trial. Lancet.2016;387:127-135.
10. Stewart LA, Clarke M, Rovers M, Riley RD, Simmonds M, Stewart G, Tierney JF. Preferred reporting items for systematic review and meta-analyses of individual participant data: The prisma-ipd statement. JAMA. 2015;313:1657-1665.
11. Frobert O, Lagerqvist B, Olivecrona GK, Omerovic E, Gudnason T, Maeng M, Aasa M, Angeras O, Calais F, Danielewicz M, Erlinge D, Hellsten L, Jensen U, Johansson AC, Karegren A, Nilsson J, Robertson L, Sandhall L, Sjogren I, Ostlund O, Harnek J, James SK. Thrombus aspiration during st-segment elevation myocardial infarction. N Engl J Med. 2013;369:1587-1597.
12. Bhindi R, Kajander OA, Jolly SS, Kassam S, Lavi S, Niemela K, Fung A, Cheema AN, Meeks B, Alexopoulos D, Kocka V, Cantor WJ, Kaivosoja TP, Shestakovska O, Gao P, Stankovic G, Dzavik V, Sheth T. Culprit lesion thrombus burden after manual thrombectomy or percutaneous coronary intervention-alone in st-segment elevation myocardial infarction: The optical coherence tomography sub-study of the total (thrombectomy versus pci alone) trial. Eur Heart J. 2015;36:1892-1900.
p p p p ;11. Frobert O, Lagerqvist B, Olivecrona GK, Omerovic E, Gudnason T, Maenng g M,MM AAAasasasa a a M,MM
Angeras O, Calais F, Danielewicz M, Erlinge D, Hellsten L, Jensen U, Johhhananansssononon AAAC,C,C, Karegren A, Nilsson J, Robertson L, Sandhall L, Sjogren I, Ostlund O, Harnek J, JamesSK. Thrombus aspiration during st-segment elevation myocardial infarction. N Engl J Med. 2013;369:1587-1597.
12. BhBhB ininindididi RR, KaK jander OA, Jolly SS, Kassamm SS, Lavi S, Niemmela K,K Fung A, Cheema AN, Meeks BBB, AAAlexoxox popopouluu ososos DDD, , KoKK ckka a V, CCCanantoorr WJJJ, , KaKaKaivivivossojojja aa TPT ,, ShS essstatatakokokovsvsv ka OO,,, GaGaGaooo P,P Stankovic GG, DDzzzavikk k VVV, Sheeeththth TT. Culppriit leessionon thrommmbbbus bburdenen aaaftftfter mannnuuau llthrombbecce toomymy oor peeerccrcutaneous ccoronaara yy innttervrvrvenenentititionon-alonene in stst-sses ggmg ent elele evevaationmymymyocococarararddid aal inffaarction:n:n: TTTheee ooopptp icicicalalal cohohoherre enncce tttomomomogogogrraraphphp y y y susus b-ststudddy y y ofoo thehehe tttotalal (thrombbecttomy versus pci allone))) triall. EuE r HeH art J. 20201511 3;336:181892929 1-19909 0. JJ
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from

10.1161/CIRCULATIONAHA.116.025371
15
Table 1. Baseline Characteristics and Procedural Variables
Thrombus AspirationN= 9155
PCI aloneN= 9151
DemographicsAge, years (mean ±SD) 63.3 (12.0) 63.1 (12.1)Age > 75 yr (%) 1620 (17.7) 1521 (16.6)Male (%) 6930 (75.7) 7002 (76.5)Killip class IV 72 (0.8) 71 (0.8)
HistoryCurrent smoker (%)† 3535 (39.9) 3740 (42.4)Hypertension (%) 4239 (46.6) 4228 (46.5)Diabetes mellitus (%) 1419 (15.5) 1449 (15.9)Prior myocardial infarction (%) 907 (10.0) 940 (10.3)Prior PCI (%) 788 (8.6) 821 (9.0)
Thrombus AspirationN= 9155
PCI aloneN= 9151
Initial PCI procedureTime from symptom onset to PCI start (min) y 190.0 (128–311) 185.5 (125-300)Radial access (%) 5828 (67.4) 5843 (67.6)Bivalirudin (%) 3846 (42) 3735 (40.8)Enoxaparin (%) 572 (6.2) 572 (6.3)Unfractionated intravenous Heparin (%) 7693 (84) 7761 (84.8)Glycoprotein IIb/IIIa inhibitor (%)‡‡ 2957 (32.3) 3209 (35.1)Contrast Volume (mL, SD)* 171 (98) 168 (100.3)Fluoroscopy time (min, SD)** 13.2 (19.2) 12.3 (25.4)TIMI thrombus grade (%) ***
0 - No thrombus present 728 (8.0) 803 (8.8)1 - Possible thrombus present 999 (11.0) 1112 (12.2)2 - Definite thrombus present, <0.5 vessel diameter 497 (5.5) 496 (5.5)3 - Definite thrombus present, 0.5-2.0 vessel diameters 1516 (16.6) 1321 (14.5)4 - Definite thrombus present, >2.0 vessel diameters 1658 (18.2) 1623 (17.8)5 - Total occlusion 3718 (40.8) 3740 (41.1)
Pre-PCI TIMI 0/1 flow (%) 6808 (74.9) 6870 (75.5)Direct Stenting (%) 3594 (39.5) 1916 (21.1)
Bare-metal stent 4783 (52.2) 4806 (52.5)1 drug-eluting stent 4059 (44.3) 4038 (44.1)
Number of stents, mean (SD) 1.4 (0.7) 1.4 (0.7)Total stent length mm, mean (SD) 28 (15.5) 28.1 (15.4)Stent diameter mm, mean (SD) 3.2 (0.5) 3.1 (0.5)Vessel treated at Index PCILeft main coronary artery 79 (0.9) 86 (0.9)Left anterior descending coronary artery 3945 (43.1) 4039 (44.1)Left circumflex coronary artery 1404 (15.3) 1408 (15.4)Right coronary artery 4129 (45.1) 4069 (44.5)Coronary bypass graft 38 (0.4) 36 (0.4)Medications at Hospital Dischargez
Aspirin 8238 (97.4) 8217 (97.3)Ticagrelor 2043 (24) 2040 (24)
Time from symptom onset to PCI start (min) 190.0 (128 311) 185.5 (1( 25 300)Radial access (%) 5828 (67.4) 5843 (6(6(67.7.7 6)6)6)Bivalirudin (%) 3846 (42) 3735 (4(40.0.0 8)8)8)Enoxaparin (%) 572 (6.2) 572 (6.3)Unfractionated intravenous Heparin (%) 7693 (84) 7761 (84.8)Glycoprotein IIb/IIIa inhibitor (%)‡‡ 2957 (32.3) 3209 (35.1)Contrararaststst VVVolololumumume ee (mmLL,L SD)* 171 (98) 168 (100.3)Fluoorororoscopy timememe (mimimin, SSD)D)D)** 13.222 (((19199.2.2.2) 12.3.33 (((252525.4.. )TIMIMIM thrombus grraade (%(%(%) *******
0 - NoN thrombububus prpresenent 7222888 (8.00) 808003 (88.8)1 - PoPoPossible ttthrhrhrommbbus ppresennnt 999999 (11.00)0 111111121 (1122.2)22 - DeDeDefifiniiiteee ttthrhhromommbubub ss prprp esesenentt, <<<0.00 5 5 vevesssselelel dddiiamemmeteeerr 49499777 (55 5.55))) 4949666 (5(5.55))3 - Definite thrombus present 0 5-2 0 vessel diameters 1516 (16 6) 1321 (14 5)
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from

10.1161/CIRCULATIONAHA.116.025371
16
Prasugrel 966 (11.4) 961 (11.3)Clopidogrel 5124 (60.3) 5085 (59.9)Statin 8097 (95.3) 8086 (95.3)Angiotensin Converting Enzyme inhibitor or receptor blocker
6188 (72.8) 6251 (73.7)
Beta Blocker 7161 (84.3) 7198 (84.9)Oral anticoagulant 493 (5.8) 497 (5.9)† Current smoker P<0.001, y time from symptom onset to PCI P=0.025 ‡‡GP IIb/IIIa inhibitor P<0.001, *Contrast volume P<0.001, **Fluoroscopy time P<0.001 (TASTE and TOTAL only),*** TIMI thrombus grade P<0.001, z Medications at discharge only available from TASTE and TOTAL.
Table 2: Outcomes
Outcome Thrombus Aspiration N= 9155
PCI Alone N= 9151
HR 95% CI P value
Primary OutcomeCardiovascular death at 30 days 221 (2.4) 262 (2.9) 0.84 0.70-1.01 0.06Key Safety Outcome Stroke or TIA at 30 days* 66/8518 (0.8) 46/8476 (0.5) 1.43 0.98-2.1 0.06Other Outcomes at 30 daysAll Cause death 232 (2.5) 273 (3.0) 0.85 0.71-1.01 0.06Myocardial infarction 96 (1.0) 104 (1.1) 0.92 0.70-1.21 0.55Congestive heart failure** 141/ 8653(1.6) 128/8648 (1.5) 1.10 0.87-1.40 0.44Target vessel revascularization 215 (2.3) 239 (2.6) 0.90 0.74-1.08 0.24Cardiovascular death, MI, cardiogenic shock, congestive heart failure, stent thrombosis or target vessel revascularization**
604/8653(7.0) 654/8648 (7.6) 0.92 0.82-1.03 0.14
Outcomes at 1 yearCardiovascular death 343 (3.7) 380 (4.2) 0.90 0.78-1.04 0.15All cause death 426 (4.7) 464 (5.1) 0.91 0.80-1.04 0.18Myocardial infarction 233 (2.5) 239 (2.6) 0.97 0.81-1.16 0.73Congestive heart failure** 268/8653 (3.1) 258/8648 (3.0) 1.04 0.87-1.23 0.68Target vessel revascularisation 495 (5.4) 504 (5.5) 0.97 0.86-1.10 0.68Stroke or TIA* 128/8055 (1.6) 103/7990 (1.3) 1.24 0.95-1.61 0.11
*Data only available from TASTE and TOTAL trials and OR reported not HR. ** Data only available from TASTE and TOTAL trials
0.1414
N= 9155Primary OutcomeCardiovascular death at 30 days 221 (2.4) 262 (2.9) 0.84 0.70700--1.11.01011 0.00 060606Key Safety Outcome Stroke or TIA at 30 days* 66/8518 (0.8) 46/8476 (0.5) 1.43 0.98-2.1 0.06Other Outcomes at 30 daysAll CaCaCausususee dededeatatathhh 232 (2.5) 273 (3.0) 00.885 0.71-1.01 0.06Myyyooco ardial infafafarcrr titit onoo 9696 (1.0) 1010044 4 (1(11.1.11) 0.0.929 00.0 7077 -1.21212 00.0 5555Cooonngestive heart ffaiailurereea ****** 1441/ 86533((1.66)) 122128/864644888 (1.5.5) 11.110 0.878787--1.40400 0.444444Taaargrgrget vessel rrrevevevasscculaarrizationon 2215 (2.3))) 2323239 99 (2(2(2.66.6)) 00.990 0.7444-1.0808 0.2424Cardrdrdioioiovasculararar dded atth, MMI,, cardddioioiogegeg nicshshocockk,k cccongeeestststivivee hhehearara tt fafafaililururee, sstetetent thrombosis or target vessel
6060604/44 86535353(77.00) 66654/864646488 (7.6.66) 00.992 0.828282---1.0303
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from

10.1161/CIRCULATIONAHA.116.025371
17
Table 3: Outcomes by High and Low Thrombus Burden
Outcome Thrombus Aspiration
PCI Alone HR 95% CI P value Interaction P
Cardiovascular Death at 30 daysTIMI Thrombu 170 (2.5) 205 (3.1) 0.80 0.65-0.98 0.03 0.32TIMI Thrombus Grade <3 49 (2.2) 53 (2.2) 1.00 0.68-1.47 0.99
144 (2.7) 174 (3.2) 0.82 0.66-1.02 0.08 0.67TIMI Thrombus Grade <4 75 (2.0) 84 (2.3) 0.89 0.65-1.22 0.48Stroke or TIA at 30 days*
55 (0.9) 34 (0.5) 1.56 1.02-2.42 0.04 0.34TIMI Thrombus Grade <3 11 (0.5) 12 (0.5) 0.99 0.43-2.26 0.98
51 (1.0) 27 (0.6) 1.87 1.18-3.02 0.009 0.04TIMI Thrombus Grade <4 15 (0.4) 19 (0.5) 0.80 0.40-1.57 0.512Other Outcomes at 30 daysAll Cause Death
176 (2.6) 210 (3.1) 0.81 0.66-0.99 0.04 0.31TIMI Thrombus Grade <3 54 (2.4) 58 (2.4) 1.00 0.69-1.45 0.99
150 (2.8) 179 (3.3) 0.83 0.67-1.03 0.10 0.68TIMI Thrombus Grade <4 80 (2.1) 89 (2.4) 0.90 0.66-1.22 0.49Myocardial Infarction
78 (1.1) 84 (1.3) 0.90 0.66-1.23 0.52 0.95TIMI Thrombus Grade <3 17 (0.76) 20 (0.83) 0.93 0.49-1.77 0.82TIMI Thrombus Grade 65 (1.2) 68 (1.3) 0.96 0.68-1.35 0.80 0.61TIMI Thrombus Grade <4 30 (0.8) 36 (0.96) 0.82 0.51-1.33 0.43Outcomes at 1 yearCardiovascular Death
261 (3.8) 298 (4.5) 0.84 0.72-1.0 0.05 0.17TIMI Thrombus Grade <3 78 (3.5) 78 (3.2) 1.08 0.79-1.47 0.64
219 (4.1) 249 (4.6) 0.87 0.73-1.04 0.14 0.61TIMI Thrombus Grade <4 120 (3.2) 127 (3.4) 0.94 0.73-1.21 0.64All Cause Death
318 (4.6) 353 (5.3) 0.87 0.75-1.01 0.07 0.20TIMI Thrombus Grade <3 104 (4.7) 106 (4.4) 1.06 0.81-1.39 0.69
262 (4.9) 289 (5.4) 0.90 0.76-1.06 0.20 0.74TIMI Thrombus Grade <4 160 (4.3) 170 (4.6) 0.94 0.76-1.16 0.56Stroke or TIA*
98 (1.6) 76 (1.3) 1.24 0.92-1.68 0.17 0.94TIMI Thrombus Grade <3 30 (1.6) 27 (1.3) 1.20 0.71-2.05 0.49
81 (1.7) 54 (1.2) 1.48 1.05-2.10 0.03 0.11TIMI Thrombus Grade <4 47 (1.4) 49 (1.5) 0.96 0.64-1.44 0.85*Stroke or TIA outcomes have odds ratio reported instead of hazard ratio
TIMI Thrombus Grade <3 54 (2.4) 58 (2.4) 1.00 0.69 1.45 0.99150 (2.8) 179 (3.3) 0.83 0.67-1.03 0..10100 0.0.0.686868
TIMI Thrombus Grade <4 80 (2.1) 89 (2.4) 0.90 0.66-1.22 0.494949Myocardial Infarction
78 (1.1) 84 (1.3) 0.90 0.66-1.23 0.52 0.95TIMI Thrombus Grade <3 17 (0.76) 20 (0.83) 0.93 0.49-1.77 0.82TIMI TTThrhrhrommombububusss Grradade 65 (1.2) 68 (11.3) 0.96 0.68-1.35 0.80 0.61TIMMIMI TTThrombuusss GrGrGradadade <4<< 303 (0.0.8)8 363 (00.96)) 0.0 822 0.515 -1.333333 0.0.0.43Ouutctctcomes at 1 yearCardrdrdiovascularrr DDDeaeath
262626111 (3(3(3.8.. ) 22988 (44.555) 0..84 0.722-11.1 000 0..050505 0.17TITIMIMI TTThrhh ombububuss GrGrradadadee <3<3< 787878 ((33.5)55 78787 (333.22))) 1.11 08080 00.7999-11.474747 0.00 64664
219 (4 1) 249 (4 6) 0 87 0 73-1 04 0 14 0 61
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from

10.1161/CIRCULATIONAHA.116.025371
18
Figure Legends
Figure 1. PRISMA flowchart
Figure 2. Kaplan Meier Curves for cardiovascular mortality
Figure 3. A. Subgroup analysis for cardiovascular mortality at 30 days. B. Subgroup analysis for
stroke or TIA within 30 days
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from

by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from

Time to CV death
Months of Follow-up
Cum
ulat
ive
Haz
ard
Rat
es
0.0
0.2
0.4
0.6
0.8
1.0
0 2 4 6 8 10 12
No. at Risk
Thrombectomy
PCI Alone
9155 8853 8810 8778 8536 8509 8437
9151 8807 8759 8729 8488 8458 8383
0.0
0.01
0.02
0.03
0.04
0.05
0.06
0 2 4 6 8 10 12
PCI alone
Thrombectomy
Hazard ratio, 0.90 (95%CI, 0.78-1.04); P=0.15
Cu
Cu
Cum
um
um
ulalala
tititiveveve H
azar
d R
ates
0.222
0.444
0.6
0.00 0
0.01
0.02
0.03
0 20 2 4 64 64 6 8 100
Thrombectomy
Hazard ratio, 0.90 (95%CI, 0.78-1.04); P=0.15
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from

0.5 1.0 2.0
OVERALL
TIMI Thrombus Grade:
>=3
<3
TIMI Thrombus Grade:
>=4
<4
Initial TIMI Flow:
0-1
2-3
Symptom onset (h):
<6
6-12
>12
Vessel:
Non-proximal
Proximal
Lesion:
Non LAD lesion
LAD lesion
Site PCI Volume:
Tertile 1
Tertile 2
Tertile 3
Glycoprotein inhib:
No
Yes
18306
13576
4635
10739
7472
13678
4515
14016
2615
629
7234
11072
10856
7407
5879
6861
5514
12137
6166
no. of events/total no. (%)
Thrombectomy
221/9155 (2.4)
170/6892 (2.47)
49/2224 (2.2)
144/5376 (2.68)
75/3740 (2.01)
195/6808 (2.86)
24/2286 (1.05)
142/6958 (2.04)
44/1359 (3.24)
20/317 (6.31)
48/3618 (1.33)
173/5537 (3.12)
95/5455 (1.74)
125/3674 (3.4)
67/2952 (2.27)
81/3417 (2.37)
73/2759 (2.65)
170/6198 (2.74)
51/2957 (1.72)
PCI Alone
262/9151 (2.9)
205/6684 (3.07)
53/2411 (2.2)
174/5363 (3.24)
84/3732 (2.25)
219/6870 (3.19)
42/2229 (1.88)
181/7058 (2.56)
51/1256 (4.06)
10/312 (3.21)
72/3616 (1.99)
190/5535 (3.43)
117/5401 (2.17)
145/3733 (3.88)
85/2927 (2.9)
89/3444 (2.58)
87/2755 (3.16)
174/5939 (2.93)
88/3209 (2.74)
Hazard Ratio(95%CI)
0.84(0.7-1.01)
0.8(0.65-0.98)
1(0.68-1.47)
0.82(0.66-1.02)
0.89(0.65-1.22)
0.9(0.74-1.09)
0.55(0.34-0.92)
0.79(0.64-0.99)
0.79(0.53-1.18)
1.97(0.92-4.21)
0.66(0.46-0.96)
0.91(0.74-1.12)
0.8(0.61-1.05)
0.87(0.69-1.11)
0.78(0.57-1.07)
0.92(0.68-1.24)
0.83(0.61-1.14)
0.94(0.76-1.16)
0.63(0.44-0.88)
P(INTERACTION)
0.321
0.666
0.078
0.06
0.143
0.658
0.755
0.048
Favours Thrombectomy Favours PCI Alone
Flow:
onset (h):
proxxix mmalm
mal
LAD lesion
7472
13678
4515
14016
261555
66296
72344
11101 772
10856
75/3740 (2.01)
195/6808 (2.86)
24/2286 (1.05)
142/6958 (2.04)
44/1359 (3.24)
20/317 (6.31)
48/48/48/3618 (1.33)
173173173/5537 (3..12)1212
95/5455 (1.74)
84/3732 (2.25)
219/6870 (3.19)
42/2229 (1.88)
181/7058 (2.56)
51/12556 (6 (6 (4.06)
10/312 (33.21)
772/33616 (66 (1.99)
19090190/55535 335 (3.3.3.43)43)43)
117/5401 (2.17)
0.89(0.65 1.22)
0.9(0.74-1.09)
0.55(0.34-0.92)
0.79(0.64-0.99)
0.79(0(( .53-1.11.18)11
1.9997(((0.92-4.21)
0.6666(((0.46-00.9996)
0.9991(((0.74-11.112)
0.8(0.61-1.05)
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from

0.5 1.0 2.0
OVERALL
TIMI Thrombus Grade:
>=3
<3
TIMI Thrombus Grade:
>=4
<4
Initial TIMI Flow:
0-1
2-3
Symptom onset (h):
<6
6-12
>12
Vessel:
Non-proximal
Proximal
Lesion:
Non LAD lesion
LAD lesion
Site PCI Volume:
Tertile 1
Tertile 2
Tertile 3
Glycoprotein inhib:
No
Yes
16994
12619
4291
9872
7038
12819
4078
12963
2427
589
6610
10384
10125
6828
5696
6765
4482
11854
5137
no. of events/total no. (%)
Thrombectomy
66/8518 (0.77)
55/6430 (0.86)
11/2055 (0.54)
51/4969 (1.03)
15/3516 (0.43)
57/6408 (0.89)
9/2057 (0.44)
48/6452 (0.74)
10/1258 (0.79)
3/299 (1)
23/3310 (0.69)
43/5208 (0.83)
30/5100 (0.59)
36/3393 (1.06)
25/2875 (0.87)
24/3373 (0.71)
17/2243 (0.76)
45/6072 (0.74)
21/2446 (0.86)
PCI Alone
46/8476 (0.54)
34/6189 (0.55)
12/2236 (0.54)
27/4903 (0.55)
19/3522 (0.54)
41/6411 (0.64)
5/2021 (0.25)
30/6511 (0.46)
10/1169 (0.86)
2/290 (0.69)
13/3300 (0.39)
33/5176 (0.64)
21/5025 (0.42)
25/3435 (0.73)
12/2821 (0.43)
21/3392 (0.62)
13/2239 (0.58)
38/5782 (0.66)
8/2691 (0.3)
0dds Ratio(95%CI)
1.43(0.98-2.1)
1.56(1.02-2.42)
0.99(0.43-2.26)
1.87(1.18-3.02)
0.8(0.4-1.57)
1.39(0.94-2.1)
1.76(0.61-5.74)
1.62(1.03-2.59)
0.92(0.38-2.26)
1.41(0.23-10.8)
1.77(0.91-3.6)
1.3(0.83-2.06)
1.41(0.81-2.5)
1.46(0.88-2.46)
2.05(1.05-4.24)
1.15(0.64-2.09)
1.31(0.64-2.75)
1.13(0.73-1.75)
2.9(1.33-6.98)
P(INTERACTION)
0.342
0.041
0.683
0.549
0.457
0.93
0.432
0.038
Favours Thrombectomy Favours PCI Alone
onset (h):
proxiimalmama
mal
LAD lesesesiononon
eesiosionn
olume:
12819
4078
12963
2427
589
666661000
1038884
111012225
682682888
57/6408 (0.89)
9/2057 (0.44)
48/6452 (0.74)
10/1258 (0.79)
3/299 (1)
23/23/3313313310 (0 (0 (0 60 60.69)99
43/43/43/555208 (0.8883)33)
3030/30/5515100 (0.5559)9)9)
36/36/33333393 (1.00066)6)
41/6411 (0.64)
5/2021 (0.25)
30/6511 (0.46)
10/1169 (0.86)
2/290 (0.69)
13/3/3/33033 0 (0 (0.39)9))
333/555176 (6 (0.64)4)4)
2221/555025 (5 (0.4442)))
252525/34333435 (5 (5 (0 70.73)3)3)
1.39(0.94-2.1)
1.76(0.61-5.74)
1.62(1.03-2.59)
0.92(0.38-2.26)
1.41(0.23-10.8)
1 71 71.77(0(0(0.91.9.9 -3.3.3.6)6)6
1.333(00.83-2.0006)
1.4441((0(0.81-222.55)
1 41.466(6(0.8888 22-2.46)6)6
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from

Sasko Kedev, Goran Stankovic, Brandi Meeks and Ole FrøbertSalim Yusuf, Göran K. Olivecrona, Henrik Renlund, Peggy Gao, Bo Lagerqvist, Ashraf Alazzoni,
Sanjit S. Jolly, Stefan K. James, Vladimír Dzavík, John A. Cairns, Karim D. Mahmoud, Felix Zijlstra,Meta-analysis
Thrombus Aspiration in ST Elevation Myocardial Infarction: An Individual Patient
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2016 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation published online December 9, 2016;Circulation.
http://circ.ahajournals.org/content/early/2016/12/09/CIRCULATIONAHA.116.025371World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org/content/suppl/2016/12/09/CIRCULATIONAHA.116.025371.DC1.htmlData Supplement (unedited) at:
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Circulation Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on Decem
ber 9, 2016http://circ.ahajournals.org/
Dow
nloaded from

1
SUPPLEMENTAL MATERIAL

2
Supplemental Methods: Search Strategy for Ovid MEDLINE and EMBASE as of September 2, 2016
Results using Search Strategy 1 Myocardial Infarction.mp. (440266) 2 Thrombectomy.mp. (23156) 3 Thrombus Aspiration.mp. (3260) 4 Thromboaspiration.mp. (426) 5 2 or 3 or 4 (25178) 6 Randomized.mp. (1465727) 7 1 and 5 and 6 (818) 8 Remove duplicates from 7 (605)

3
Supplemental Table S1: Characteristics of Included Trials
Table S1. Trial overview
TOTAL TASTE TAPAS
n 10,732 7,244 1,071
n screened Not reported 12,005 1,161
% included Not reported 60 92
No. of centers 87 31 1
Included symptom duration, hrs 0-12 0.5-24 0.5-12
Intervention Routine Thrombus Aspiration Routine Thrombus Aspiration Routine Thrombus Aspiration with direct stenting when possible
Manual Aspiration device Export® Export®, Pronto®, Eliminate® Export®
Primary Outcome CV death, new MI, chock, or NYHA IV heart failure within 180 days
30 day all-cause death Myocardial blush grade 0 or 1
CV, cardiovascular; NYHA, New York Heart Association; MI, myocardial infarction.

4
Supplemental Table S2: Outcome Definitions
Table S2.
Trial CV Death Recurrent MI Heart Failure
TOTAL
All deaths with a clear cardiovascular or unknown cause will be classified as cardiovascular.
Recurrent myocardial infarction (MI) will be subdivided into MI within the first 24 hours of randomization, between 24 hours and 7 days after randomization and more than 7 days after randomization.
New or worsening NYHA Class IV heart failure is defined as a physician decision to treat HF with IV diuretic, inotropic agent or vasodilator plus at least one of the following: 1) presence of pulmonary edema or pulmonary vascular congestion on chest radiograph thought to be due to HF; 2) rales reaching above the lower 1/3 of the lung fields thought to be due to HF; or 3) PCWP or LVEDP ≥ 18 mm Hg.
MI occurring within 24 hours of randomization
Recurrent ischemic symptoms greater than 20 minutes with new ST elevation greater than 0.1 millivolt in at least 2 contiguous leads not due to changes from evolution of the index MI.
MI occurring between 24 hours and 7 days of randomization
Ischemic symptoms greater than 20 minutes and either i) elevation or re-elevation of cardiac biomarkers (CK-MB or troponin) greater than twice the upper limit of normal, and if already elevated then further elevations more than 50% above a previous value that was decreasing or, ii) new ST segment elevation or, new significant Q waves in at least 2 contiguous leads, which are separate from the baseline MI.
MI occurring after 7 days of randomization
Typical rise and fall of biochemical markers of myocardial necrosis to greater than twice the upper limit of normal or if markers were already elevated, further elevation of a marker to greater than 50% of a previous value that was decreasing and > 2X ULN, with at least one of: i) ischemic symptoms, ii) development of new pathological Q waves, iii) ECG changes of new ischemia, or Pathological evidence of MI.

5
Trial CV Death Recurrent MI Heart Failure MI occurring within 24 hours following non-index PCI that is performed more than 24 hours after randomization
Cardiac biomarker (CK-MB or troponin) greater than 3 times the upper limit of normal (ULN) or increased by 50% from the pre-procedural valley level and greater than or equal to 3 times ULN in patients with already elevated enzymes, or new ST segment elevation or development of significant Q waves in 2 or more contiguous leads which are discrete from baseline MI.
Within 24 hours Post-CABG
CK-MB (or Total CK, if CK-MB is unavailable) greater than or equal to 5 times ULN and increased 50% from the pre-procedural valley level AND > 5 X ULN in patients with already elevated enzymes and development new pathological Q waves in 2 or more contiguous leads, or CK-MB value greater or equal to 10 times ULN without new pathological Q waves.
TASTE
All deaths with a clear cardiovascular or unknown cause will be classified as cardiovascular by information from national death registry.
Rehospitalization for myocardial infarction defined as ICD codes I21 and I22 by the treating physician
ICD code I50 as judged by the treating physician.
TAPAS
Death was regarded as cardiac unless an unequivocal non-cardiac cause of death was established
Reinfarction was defined as recurrent symptoms with new ST-segment elevation and elevation of cardiac markers to at least twice the upper limit of normal. +NSTEMI.
Not available
Meta-analysis definition
All deaths with a clear cardiovascular or unknown cause will be classified as cardiovascular.
Recurrent MI as per study definition 30 days, 180 days, 1 year Heart failure (TOTAL and TASTE only)
6
Trial CV Death Recurrent MI Heart Failure 30 days, 180 days, 1 year
Table S2. Continued
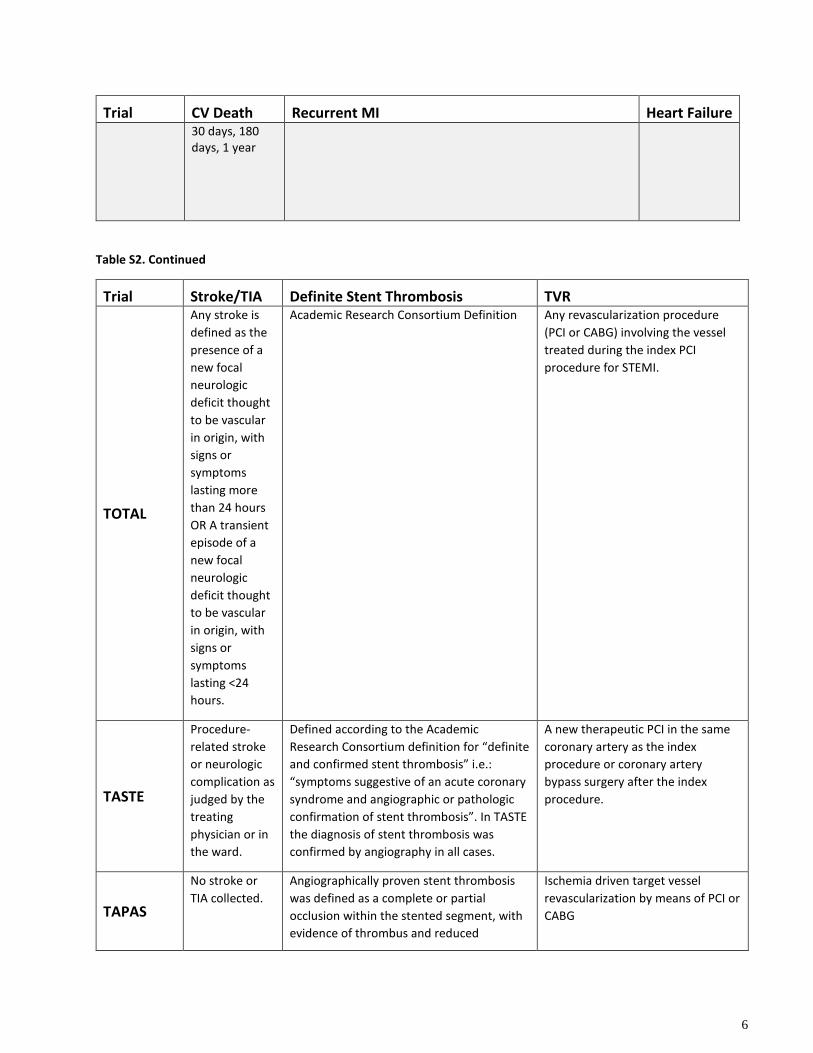
Trial Stroke/TIA Definite Stent Thrombosis TVR
TOTAL
Any stroke is defined as the presence of a new focal neurologic deficit thought to be vascular in origin, with signs or symptoms lasting more than 24 hours OR A transient episode of a new focal neurologic deficit thought to be vascular in origin, with signs or symptoms lasting <24 hours.
Academic Research Consortium Definition Any revascularization procedure (PCI or CABG) involving the vessel treated during the index PCI procedure for STEMI.
TASTE
Procedure-related stroke or neurologic complication as judged by the treating physician or in the ward.
Defined according to the Academic Research Consortium definition for “definite and confirmed stent thrombosis” i.e.: “symptoms suggestive of an acute coronary syndrome and angiographic or pathologic confirmation of stent thrombosis”. In TASTE the diagnosis of stent thrombosis was confirmed by angiography in all cases.
A new therapeutic PCI in the same coronary artery as the index procedure or coronary artery bypass surgery after the index procedure.
TAPAS
No stroke or TIA collected.
Angiographically proven stent thrombosis was defined as a complete or partial occlusion within the stented segment, with evidence of thrombus and reduced
Ischemia driven target vessel revascularization by means of PCI or CABG

7
Trial Stroke/TIA Definite Stent Thrombosis TVR antegrade flow (TIMI flow <3) with a concurrent acute clinical ischaemic event
Meta-analysis definition
Stroke/TIA 30 days, 180 days, 1 year
Definite stent thrombosis 24 hours, 30 days, 180 days, 360 days
TVR 30 days, 180 days, 1 year

8
Supplemental Figure S1: Risk of bias as per the Cochrane Collaboration’s tool
Trial W
as s
eque
nce
gene
ratio
n de
scrib
ed?
Was
the
allo
catio
n se
quen
ce
conc
eale
d?
Wer
e pa
rtici
pant
s b
linde
d?
Was
the
stud
y ou
tcom
e as
sess
men
t bl
inde
d?
Was
ther
e in
com
plet
e ou
tcom
e da
ta?
Was
ther
e se
lect
ive
outc
ome
repo
rting
?
Other sources of bias?
TAPAS Open Label Trial TASTE Open Label Trial TOTAL Open Label Trial = Low risk = Unclear = High risk

9
Supplemental Figure S2: CV Death at 30 days by Study
Supplemental Figure S3: Stroke or TIA at 30 days by Study
0.5 1.0 2.0
OVERALL
TAPAS
TASTE
TOTAL
N
18306
1005
7237
10064
no. of events/total no. (%)
Thrombectomy
221/9155 (2.41)
6/502 (1.2)
99/3618 (2.74)
116/5035 (2.3)
PCI Alone
262/9151 (2.86)
19/503 (3.78)
103/3619 (2.85)
140/5029 (2.78)
Hazard Ratio(95%CI)
0.84(0.7-1.01)
0.42(0.19-0.92)
0.96(0.73-1.27)
0.85(0.68-1.08)
P-value
0.0581
0.0311
0.7753
0.1845
Favours Thrombectomy Favours PCI Alone
P(INTERACTION)
0.05
CV Death at 30 Days
0.5 1.0 2.0
OVERALL
TASTE
TOTAL
N
16994
7237
9757
no. of events/total no. (%)Thrombectomy
66/8518 (0.77)
24/3618 (0.66)
42/4900 (0.86)
PCI Alone
46/8476 (0.54)
27/3619 (0.75)
19/4857 (0.39)
Odds Ratio(95%CI)
1.43(0.98-2.1)
0.89(0.51-1.54)
2.2(1.3-3.87)
P-value
0.0627
0.674
0.0044
Favours Thrombectomy Favours PCI Alone
P(INTERACTION)
0.02
Stroke/TIA at 30 Days


















