
Thrombolytic therapy of distal upper extremity occlusion · Hypercoagulability Sepsis, DIC,...
23
Thrombolytic therapy of distal upper extremity occlusion (hypothenar hammer syndrome) A therapeutic option of a rare disease Franz Hafner Medical University of Graz Division of Angiology
Transcript of Thrombolytic therapy of distal upper extremity occlusion · Hypercoagulability Sepsis, DIC,...
Thrombolytic therapy of distal upper extremity occlusion(hypothenar hammer syndrome)
A therapeutic option of a rare disease
Franz Hafner
Medical University of Graz
Division of Angiology
Disclosure
Speaker name:
Franz Hafner
I do not have any potential conflict of interest
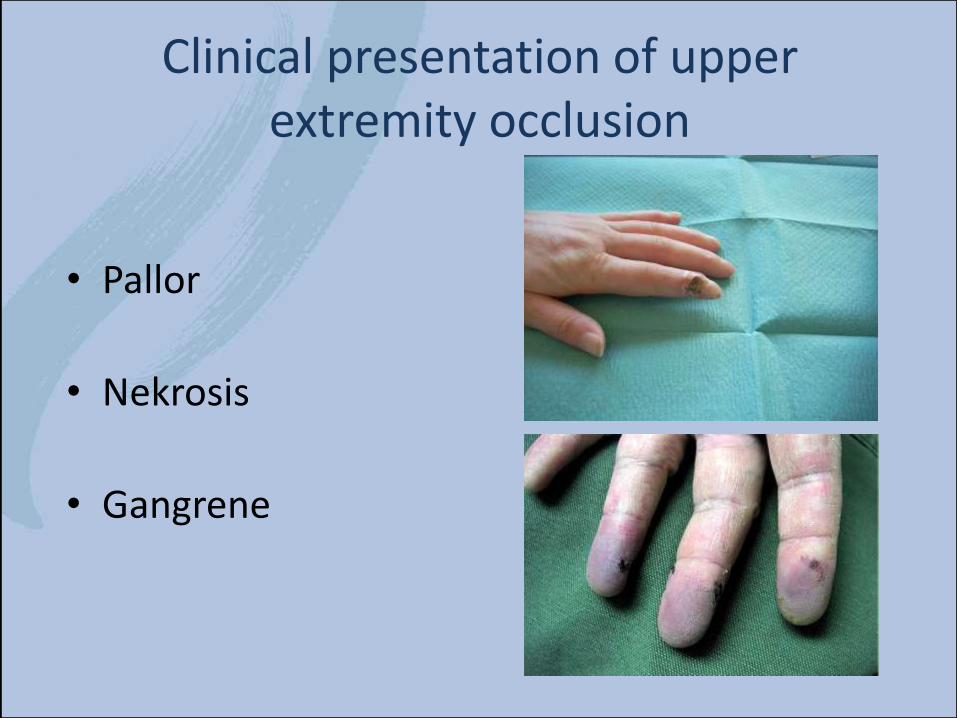
Clinical presentation of upperextremity occlusion
• Pallor
• Nekrosis
• Gangrene
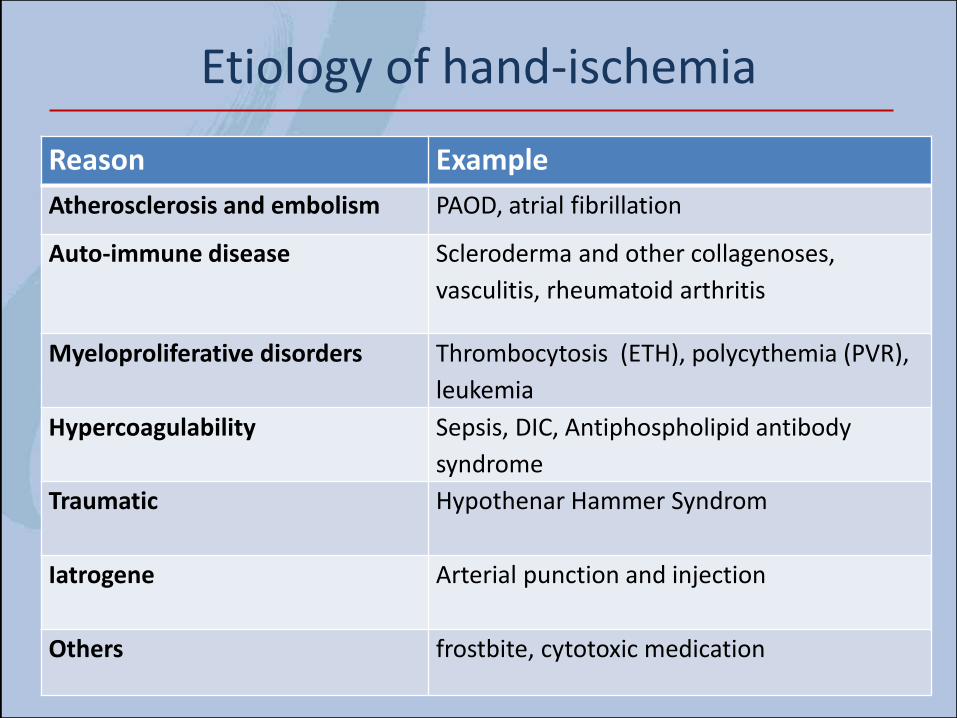
Reason Example
Atherosclerosis and embolism PAOD, atrial fibrillation
Auto-immune disease Scleroderma and other collagenoses,
vasculitis, rheumatoid arthritis
Myeloproliferative disorders Thrombocytosis (ETH), polycythemia (PVR),
leukemia
Hypercoagulability Sepsis, DIC, Antiphospholipid antibody
syndrome
Traumatic Hypothenar Hammer Syndrom
Iatrogene Arterial punction and injection
Others frostbite, cytotoxic medication
Etiology of hand-ischemia
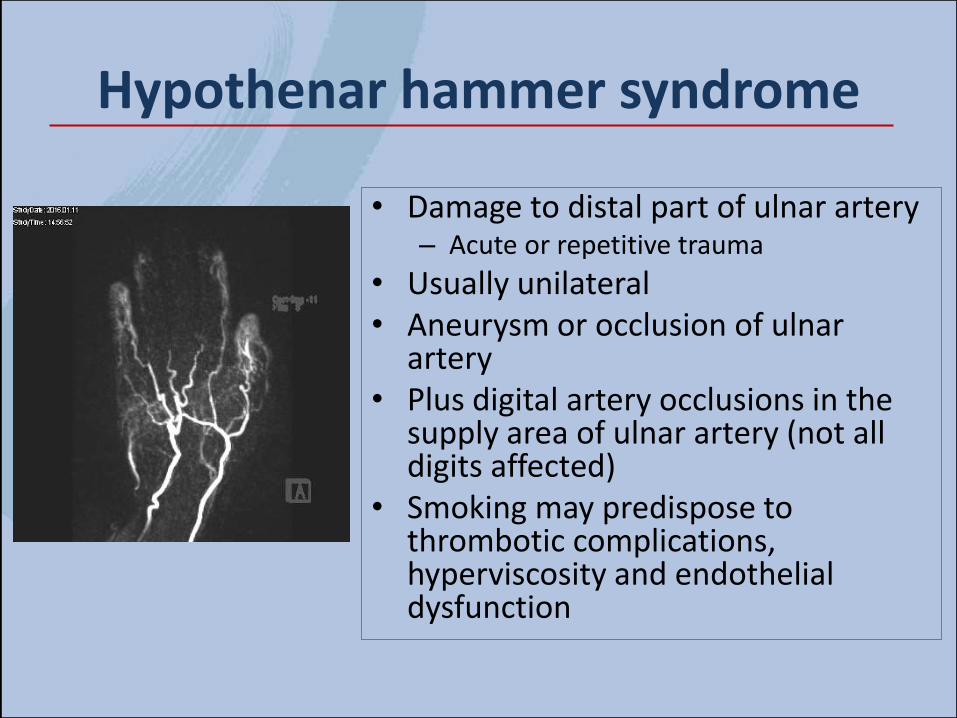
Hypothenar hammer syndrome
• Damage to distal part of ulnar artery– Acute or repetitive trauma
• Usually unilateral• Aneurysm or occlusion of ulnar
artery• Plus digital artery occlusions in the
supply area of ulnar artery (not all digits affected)
• Smoking may predispose tothrombotic complications, hyperviscosity and endothelialdysfunction
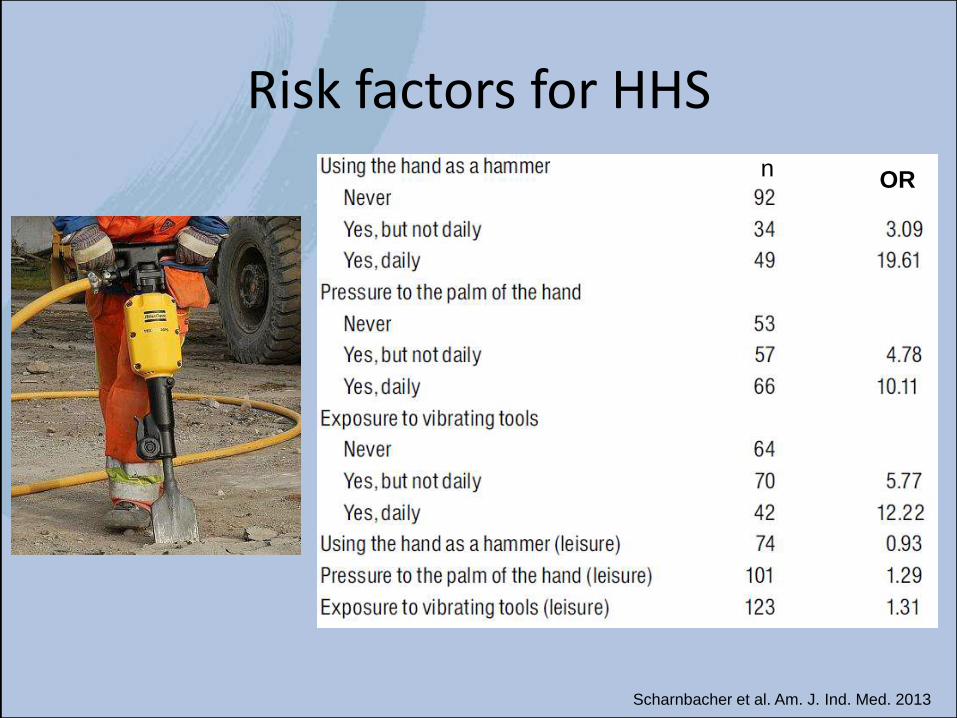
Risk factors for HHSn
OR
Scharnbacher et al. Am. J. Ind. Med. 2013
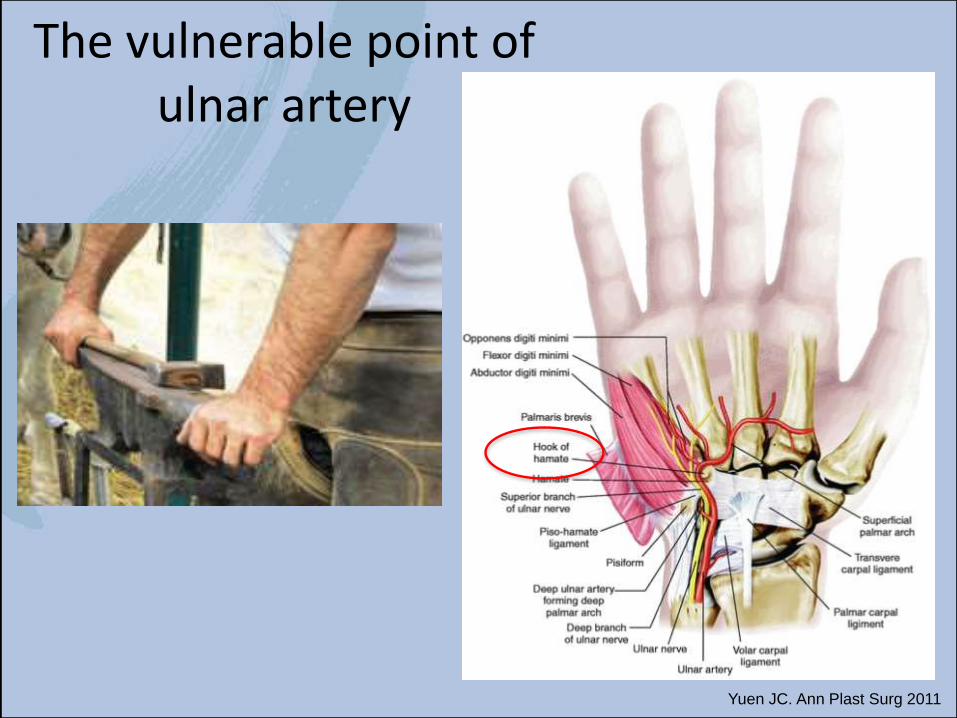
Yuen JC. Ann Plast Surg 2011
The vulnerable point of ulnar artery
Natural course of HHS
• Raynaud phenomenon 35-100%
• Digital ischemia 45-68%
• Digital necrosis 37-43%
• Dominant hand 92%
• Recurrence rate >30%
Marie I. et al. Medicine 2007;86;6
Thrombolysisa therapeutic option?
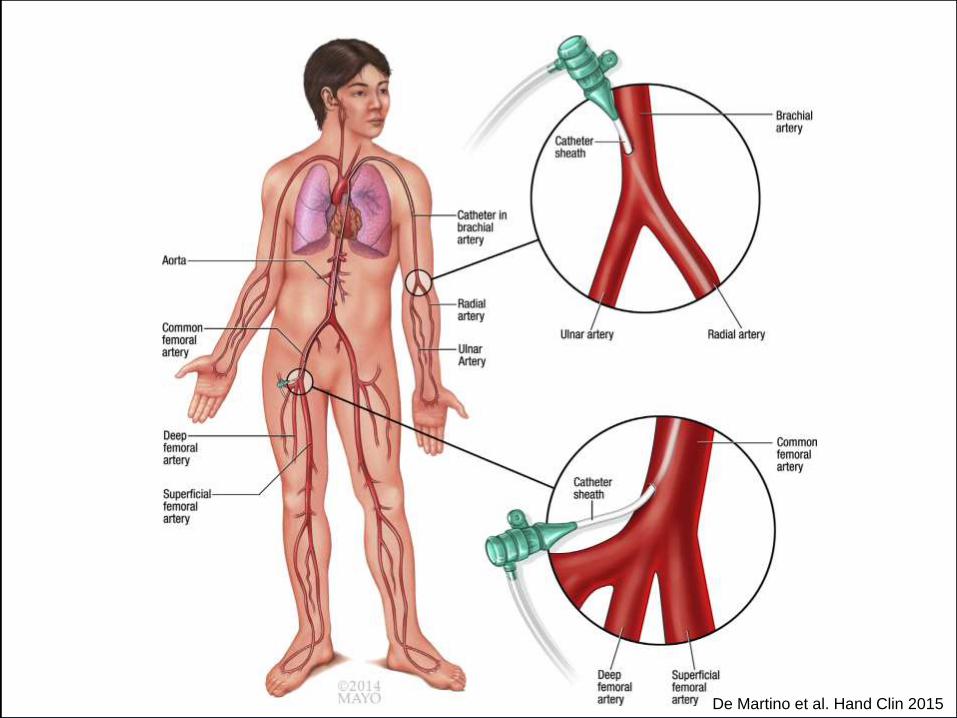
De Martino et al. Hand Clin 2015
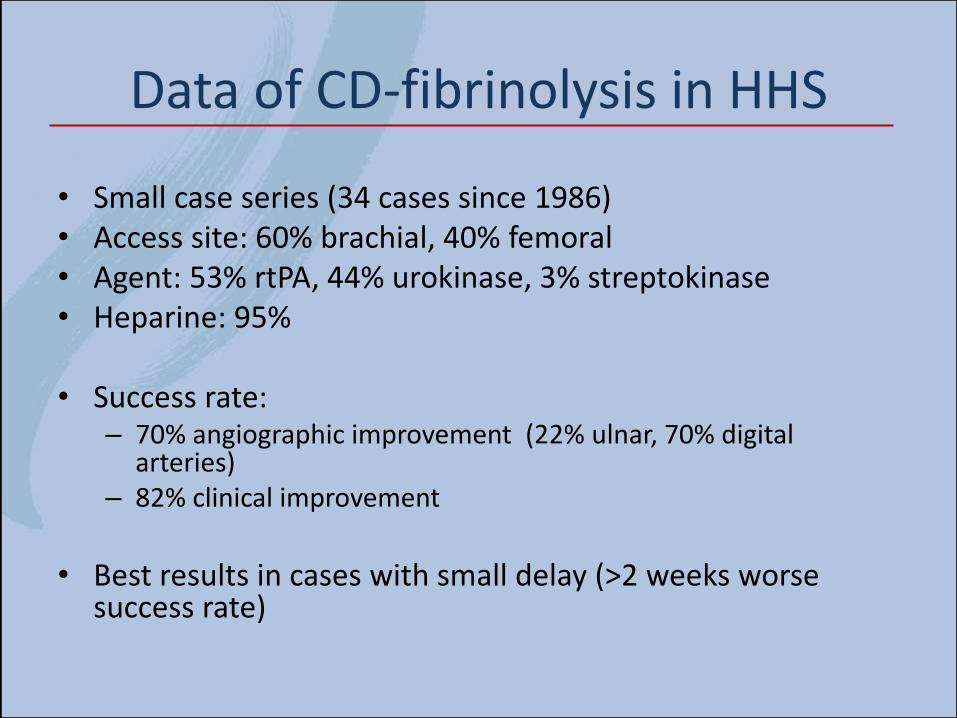
Data of CD-fibrinolysis in HHS
• Small case series (34 cases since 1986)• Access site: 60% brachial, 40% femoral• Agent: 53% rtPA, 44% urokinase, 3% streptokinase• Heparine: 95%
• Success rate:– 70% angiographic improvement (22% ulnar, 70% digital
arteries)– 82% clinical improvement
• Best results in cases with small delay (>2 weeks worsesuccess rate)
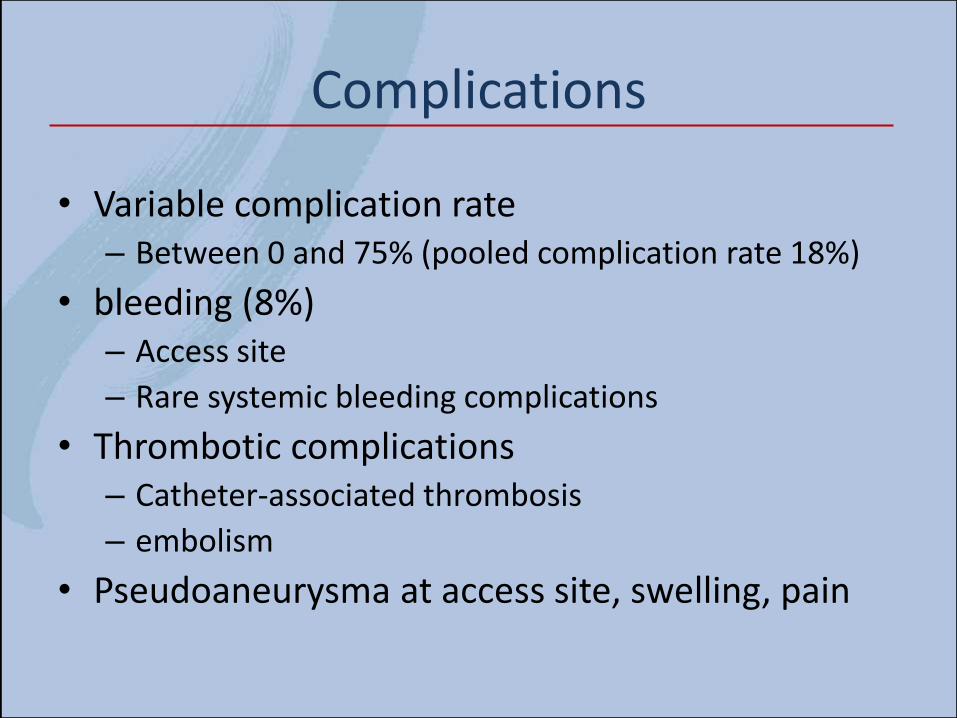
Complications
• Variable complication rate– Between 0 and 75% (pooled complication rate 18%)
• bleeding (8%)– Access site
– Rare systemic bleeding complications
• Thrombotic complications– Catheter-associated thrombosis
– embolism
• Pseudoaneurysma at access site, swelling, pain
Case – Hypothenar Hammer Syndrome
42 year old male construction worker
Pain and pallor digit 2-4 left hand
Smoker (20py)
Delay 14 days

„our regimen of CDT in HHS“
• 4F brachial access, US-guided puncture
• Microcatheter (Rebar® 27) distal ulnar artery
• Heparine 1000 IE/h via introducer sheath(APTT adjusted, 60-80sec)
• rtPA (Actilyse ®) 1.5mg/h via microcatheter
• Alprostadil 0.4µg/h via introducer sheath
• Duration of CDT: max 24 hours
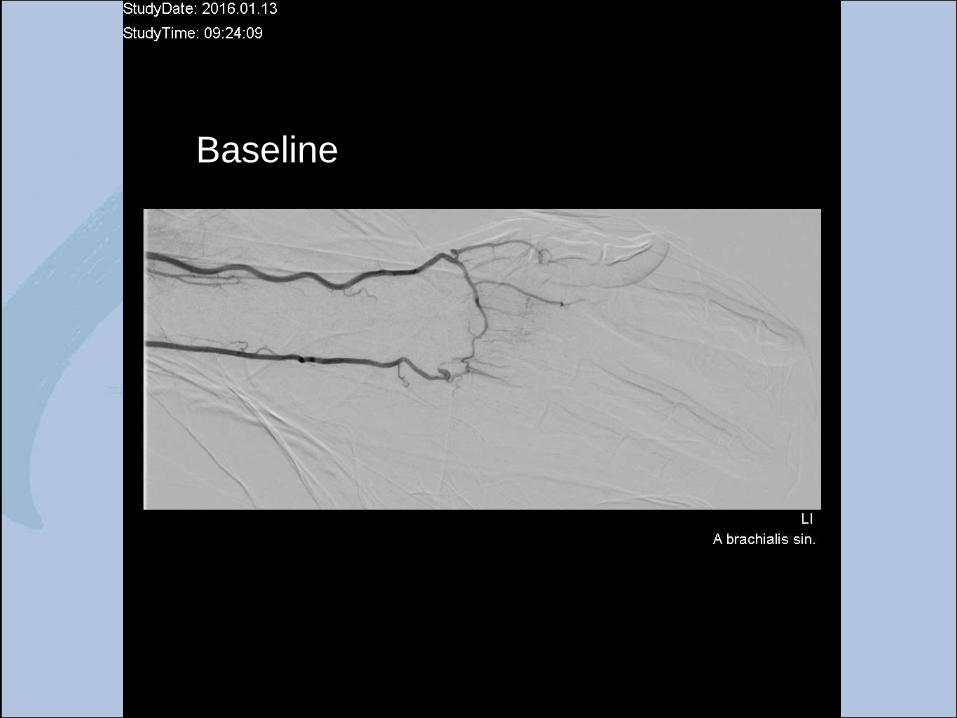
Baseline
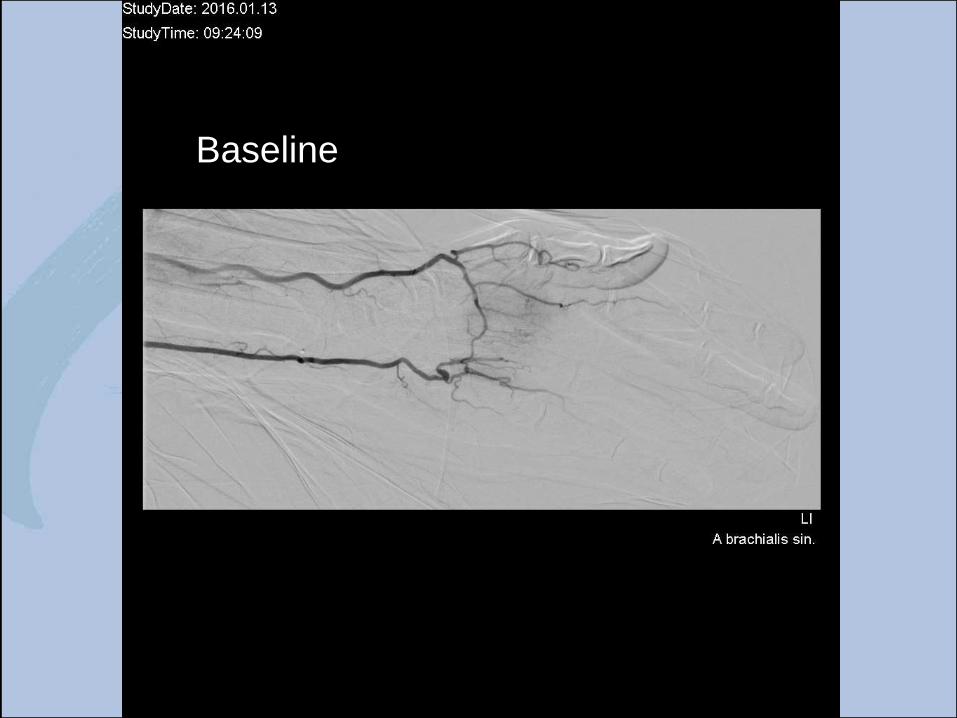
Baseline
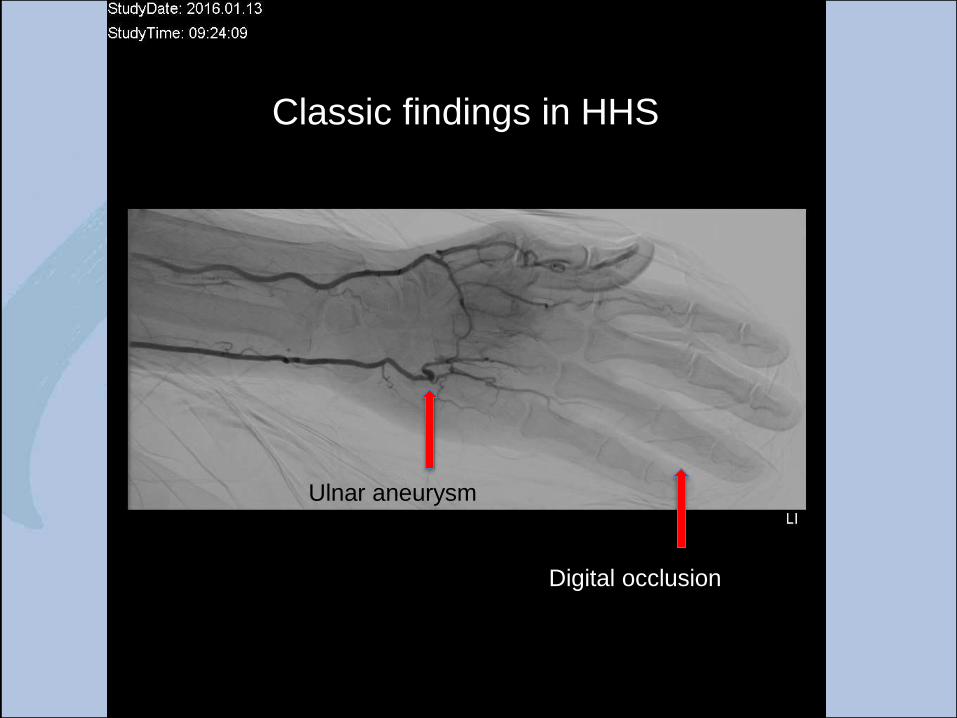
Ulnar aneurysm
Digital occlusion
Classic findings in HHS
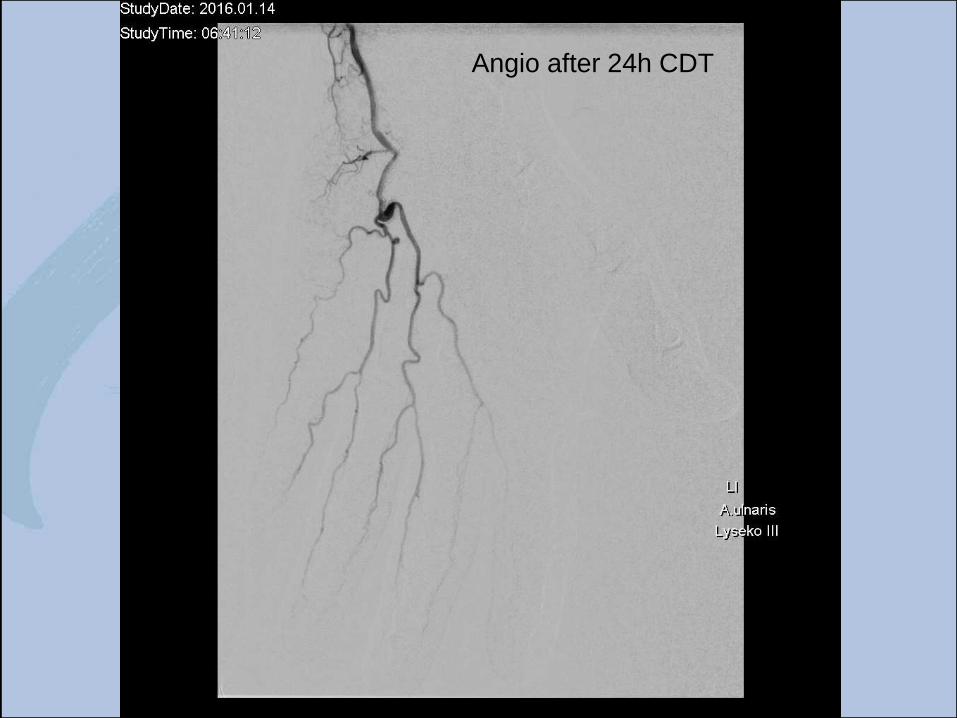
Angio after 24h CDT

Angio after 24h CDT

Angio after 24h CDT
Summary
– Catheter-directed thrombolysis represents a beneficial therapy in hypothenar hammersyndrome
– Best results in cases with small delay of symptoms
– Brachial access preferred
– Improvment of digital perfusion and symptomsdespite frequent persisting ulnar occlusion
Thrombolytic therapy of distal upper extremity occlusion(hypothenar hammer syndrome)
A therapeutic option of a rare disease
Franz Hafner
Medical University of Graz
Division of Angiology


















