Thrombo embolic Complications in Bladder Cancer
36
Thrombo embolic Complications in Bladder Cancer Jehonathan H Pinthus MD, Ph.D, FRCSC Associate Professor Department of Surgery/Urology McMaster University
Transcript of Thrombo embolic Complications in Bladder Cancer

Thrombo embolic Complications in Bladder Cancer
Jehonathan H Pinthus MD, Ph.D, FRCSC Associate Professor
Department of Surgery/Urology McMaster University

VTE complications in bladder cancer patients
§ Post-radical cystectomy
§ Effect of neo-adjuvant chemotherapy
§ Metastatic bladder cancer

NSQIP- 30 day Incidence of DVT
J Vasc Surg 2012;55:1035-41

NSQIP- 30 day Incidence of PE
J Vasc Surg 2012;55:1035-41

NSQIP- 30 day Incidence of VTE
J Vasc Surg 2012;55:1035-41

Timing of VTE Events in Cystectomy § ACS NSQIP Database queried for 1307 patients who
underwent radical cystectomy for malignancy between 2005 to 2011
§ 6% overall incidence of clinical VTE § Median time to VTE 14 days § 55% diagnosed after discharge § 6.4% 30 day mortality if diagnosed with VTE § Within the limitation of the study, predictive risk factors for
VTE: age, operative time and sepsis
§ J Urol. 191, 943-947, April 2014

Timing of VTE Events in Cystectomy
J Urol. 191, 943-947, April 2014

ENOXACAN II § Pivotal trial addressing the question of VTE risk reduction by
employing extended VTE prophylaxis using LMWH (enoxaparin)
§ Double-blind, randomized multicentre trial in patients undergoing planned curative open surgery for “abdominal and pelvic” cancer (not urology specific)
§ All received enoxaparin (40 mg sc) daily for 6-10 days and then randomly assigned to enoxaparin or placebo for another 21 days
§ Detection of VTE by bilateral venography between days 25 and 31 or sooner if symptomatic
N Engl J Med, Vol. 346, No. 13 · March 28, 2002

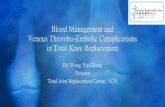
ENOXACAN II- Disease Sites

ENOXACAN II-VTE Reduction
12.0%
1.8%0.6%
4.8%
0.6%0%
0%
2%
4%
6%
8%
10%
12%
14%
VTE ProximalDVT
PE
Incide
nce of Outcome Even
tPlacebon = 167Enoxaparin 40 mg sc qdn = 165
RRR = 60%
p = NS
NNT = 14
p = NS
3-month follow-up VTE rate difference persisted (13.8% placebo vs. 5.5% enoxaparin)

p = NS
p = NS
3.6%
0%
5.1%
0.4%
0%
1%
2%
3%
4%
5%
6%
Any Bleeding
Major Bleeding
Incide
nce of Outcome Even
t Placebo n = 248 Enoxaparin n = 253
ENOXACAN II-Bleeding

§ Presently only study specifically examining the role of “extended VTE prophylaxis” in the radical cystectomy population
§ University of Chicago series § Investigator switched to 28 day extended VTE prophylaxis in
January 2013 § Study examines the period of January 2011 to May 2014 (ie
before and after this change) with primary endpoint of symptomatic VTE
Joseph J. Pariser,* Shane M. Pearce, Blake B. Anderson, Vignesh T. Packiam, Vivek N. Prachand, Norm D. Smith and Gary D. Steinberg Article in Press-J Urol Nov 2016

Extended VTE Prophylaxis in Cystectomy § Total of 402 patients § 234 standard inpatient VTE prophylaxis § 168 extended VTE prophylaxis with enoxaparin § Overall VTE rate decreased from 12% to 5% with extended
regimen (p=0.024) § Principle benefit in the post discharge VTE rate (6% vs 2%,
p=0.039) § 46% of VTE occurred after discharge § Given then non-randomized methodology, a multivariate
analysis confirmed that used of extended prophylaxis was independently associated with reduced VTE (OR 0.33, 95% CI 0.14-0.76)
§ No increased risk of bleeding observed in the latter group

In patients with bladder cancer who undergo radical cystectomy: § VTE occurs with significant frequency § VTE associated with morbidity, cost and mortality § VTE incidence can be favorably modified through
employment of extended LMWH prophylaxis


Main findings: § Analysis of 202 consecutive patients with UC of the bladder
treated with RC § 8.4% developed TEE, including 8/42 (19%) of patients
receiving NCT and RC and 9/160 (5.6%) treated by upfront RC.
§ Pre-operative TEE was a significant independent predictor of progression and CSS (HR=3.91 95% CI: 1.34-11.45)

International project aims
§ Define the incidence of thrombo-embolic events (TEE) in patients with urothelial carcinoma of the bladder undergoing neo-adjuvant chemotherapy (NAC)
§ Characterize TEE § Pre-op vs. post op § Types § Detection methods § Risk factors § Effect on survival § large database, multivariate, multi-institution

Methodology § Patient population: patients with urothelial carcinoma of the
bladder undergoing neo-adjuvant chemotherapy (NAC) § Thrombo-embolic events (TEE) were defined as
§ radiographically confirmed deep vein thrombosis (DVT) § radiographically confirmed pulmonary embolism (PE) § Arterial, venous or port site thrombosis § patients starting on anti-coagulant medication during neo-
adjuvant chemotherapy

10 Participating Centers Centre Investigators Number of
patients University of British Columbia
Drs. Peter Black and Hamid Abdi 78
University of Turku Drs. Peter Boström 34
University of Helsinki Drs. Peter Boström and Ilmari Koskinen 42
University of Rochester Dr. Janet Kukreja 39
Keck Medicine of USC Dr. Sia Daneshmand 232
McGill University Dr. Wassim Kassouf 37
Fox Chase Cancer Centre Dr. Daniel Canter 144
University of Texas Southwestern
Dr. Yair Lotan 87
Juravinski Cancer Centre Dr. Jehonathan Pinthus 58
Netherlands Cancer Institute
Drs. Bas Van Rhijn and Elies Fransen van de Putte 76
Total 827

Khorana score

Patient characteristics Non-TEE Patients (n=707)
TEE Patients (n=120)
Age at diagnosis, y, median (IQR)
65.0 (57.9 - 71.6)
66.0 (57.8-73.0)
Sex Male Female
527 (75%) 175 (25%)
86 (70%) 37 (30%)
Khorana score 1 2 3 4
290 (41%) 117 (17%) 50 (7.1%) 4 (0.6%)
58 (47%) 21 (17%) 12 (9.8%) 2 (1.6%)
Medication Anti-platelet
75 (11%)
23 (19%)

Patient characteristics - continued Non-TEE Patients (n=707)
TEE Patients (n=120)
Pathological stage Ta-T2 T3-4 TxN+
297 (42%) 201 (29%) 152 (22%)
55 (44%) 32 (26%) 33 (27%)
Duration of NAC (weeks, median IQR)
10.9 (8.9 – 12.4)
9.1 (7.6 – 12.0)
Lymph nodes removed median (IQR)
19 (11 - 38)
23 (14 - 40)
Lymph node density (%, median, IQR)
11.8% (5 - 29)
16.0% (7 - 41)
Progression 155 (19%) 46 (37%)
Progression-free survival (months, median, IQR)
9.0 (3.9 – 16.9)
10.7 (4.2 – 24.5)

Neo-adjuvant Chemotherapy Regimen
Non-TEE Patients (n=707)
TEE Patients (n=120)
MVAC 172 (26.9%) 21 (20.2%)
Gemcitabin/Cisplatin 339 (53.1%) 65 (62.5%)
Gemcitabin/Carboplatin 55 (8.6%) 7 (6.7%)
Cisplatin/Etoposide 25 (3.9%) 4 (3.9%)
Cisplatin 10 (1.6%) 0 (0%)
Other (includes several different NACs)
36 (5.6%) 7 (6.7%)

Development of TEE (any: pre-op, early (<30days) and late (>30 days) post-op)
0%
10%
20%
30%
40%
TEE
inci
denc
e
Mean 14.5%

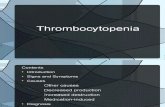
Development of TEE
0%
10%
20%
30%
McM
aste
r
U R
och
UTS
W
Vanc
ouve
r P
C
US
C/N
orris
NK
I-AvL
Hel
sink
i
FCC
C
Turk
u
McG
ill
TEE
inci
denc
e
pre-op
early post-op
late post-op

Development of TEE - pre-op 59 events (7.1%)
0%
10%
20%
JCC URoch UTSW Keck UBC NKI Helsinki FCCC Turku McGill
TEE
inci
denc
e

Post NAC imaging practice (CT of the chest)

Incidental PE § In a prospective analysis of 407
oncology patients who had CT imaging of the chest for indications other than PE detection, PE was found in up to 11% of the patients who had recently received chemotherapy. (Browne et al J Thorac Oncol, 2010)
§ The detection of unsuspected PE on staging CT in cancer patients may have a similar impact on survival and complications compared to symptomatic PE. (Donadin et al Intern Emerg Med, 2014 and den Exter et al J Clin Oncol, 2011)

Development of TEE – post-op early (<30 days): 21 events (2.6%)
0%
10%
20%
JCC URoch UTSW Keck UBC NKI Helsinki FCCC Turku McGill
TEE
inci
denc
e

Development of TEE – post-op late (>30 days): 36 events (4.8%)
0%
10%
20%
JCC URoch UTSW Keck UBC NKI Helsinki FCCC Turku McGill
TEE
inci
denc
e


Type of TEE
DVT 42%
PE 42%
arterial E 7%
stroke 0%
port site thrombosis
6%
DVT & PE 3%

Detection of TEE
clinical 68%
incidental 32%

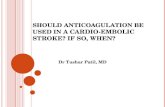
Kaplan-Meier Survival Curve (any: pre-op, early (<30days) and late (>30 days) post-op)
no TEE
TEE p=0.018

Conclusions § TEEs are very common in bladder cancer patients
undergoing neoadjuvant chemotherapy followed by RC § Majority of TEEs occur before RC (58%)
§ TEE is an independent predictor of progression-free survival after adjusting for age, Khorana score and pathologic stage § HR 1.57, 95% CI 1.08-2.29, p=0.02
§ Further investigation with a prospective trial testing thromboprophylaxis during NAC and pre-operative imaging is warranted

Multicenter retrospective, international study from 29 academic institutions. Institutional data of 1762 metastatic UC/VH patients from 2000 to 2013
Non-urotheilal histology (SHR: 2.67; 95% CI: 1.72-4.16, P < 0.001), moderate to severe renal dysfunction (SHR: 2.12; 95% CI: 1.26-3.59, P = 0.005), and cardiovascular disease (CVD) or CVD risk factors (SHR: 2.27; 95% CI: 1.49-3.45, P = 0.001) were associated with increased VTE rates. Different chemotherapy regimens did not alter risk
Overall survival was worse in patients with VTE (median 6.0 m vs. 10.2 m, P < 0.001).