Thomas Repas DO FACP FACOI FNLA FACE CDE Male Hypogonadism and Testosterone Replacement Therapy...
89
Thomas Repas DO FACP FACOI FNLA FACE CDE Male Hypogonadism and Testosterone Replacement Therapy Board Certified: • Endocrinology, Diabetes and Metabolism • Clinical Lipidology • Nutrition • Internal Medicine Regional Medical Clinic Aspen Centre- Endocrinology 640 Flormann Street Rapid City, South Dakota Clinical Assistant Professor, Dept. of Medicine, University of South Dakota, Sanford School of Medicine
-
Upload
johnathan-thomas -
Category
Documents
-
view
219 -
download
2
Transcript of Thomas Repas DO FACP FACOI FNLA FACE CDE Male Hypogonadism and Testosterone Replacement Therapy...

Thomas Repas DO FACP FACOI FNLA FACE CDE
Male Hypogonadism and Testosterone Replacement
Therapy
Board Certified:• Endocrinology, Diabetes and Metabolism• Clinical Lipidology• Nutrition• Internal Medicine
Regional Medical ClinicAspen Centre- Endocrinology640 Flormann StreetRapid City, South Dakota
Clinical Assistant Professor, Dept. of Medicine, University of South Dakota, Sanford School of Medicine

Objectives
• Testosterone Deficiency in Men– Testosterone Physiology– Clinical presentation of male hypogonadism– Age-related decline of testosterone– Diagnosis and initial evaluation of male hypogonadism
• Testosterone Replacement Therapy– Benefits/Potential Risks– Treatment options– Monitoring and follow-up
I will not be reviewing testosterone therapy in women today- that is the subject of another discussion.
Testosterone Physiologyin Men
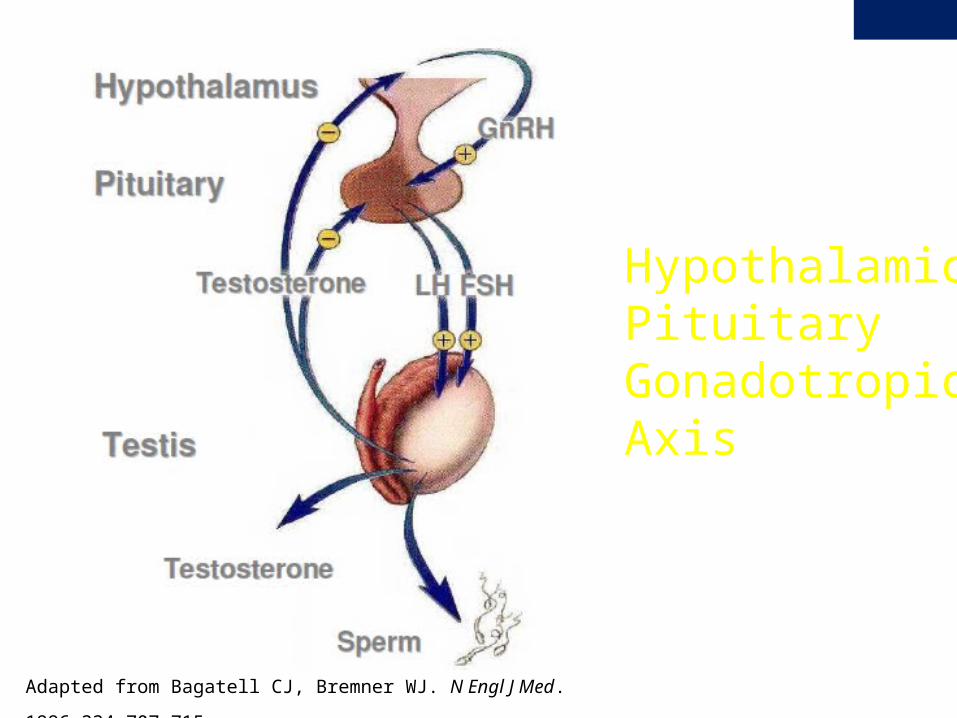
Hypothalamic Pituitary Gonadotropic Axis
Adapted from Bagatell CJ, Bremner WJ. N Engl J Med. 1996;334:707-715.
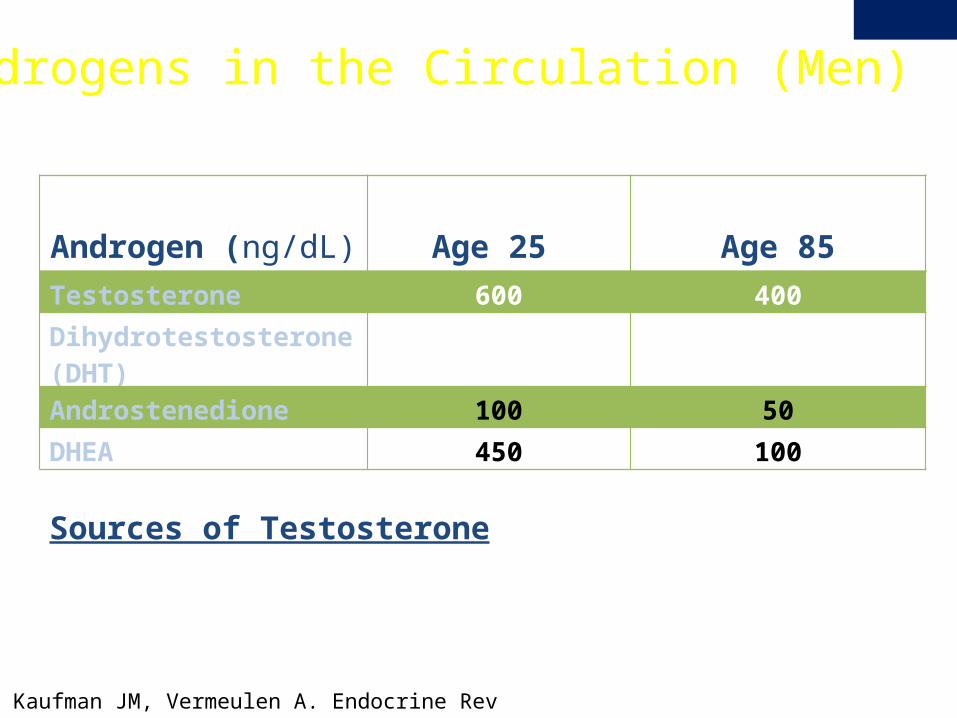
Androgens in the Circulation (Men)
Kaufman JM, Vermeulen A. Endocrine Rev 2005;26(6):883
Sources of Testosterone• Testis >95.0 %• Androstenedione 1.0 %• DHEA 0.6 %
Androgen (ng/dL) Age 25 Age 85
Testosterone 600 400
Dihydrotestosterone (DHT)
20-70 20-70
Androstenedione 100 50
DHEA 450 100
Dunn JF. et al, JCEM 1981
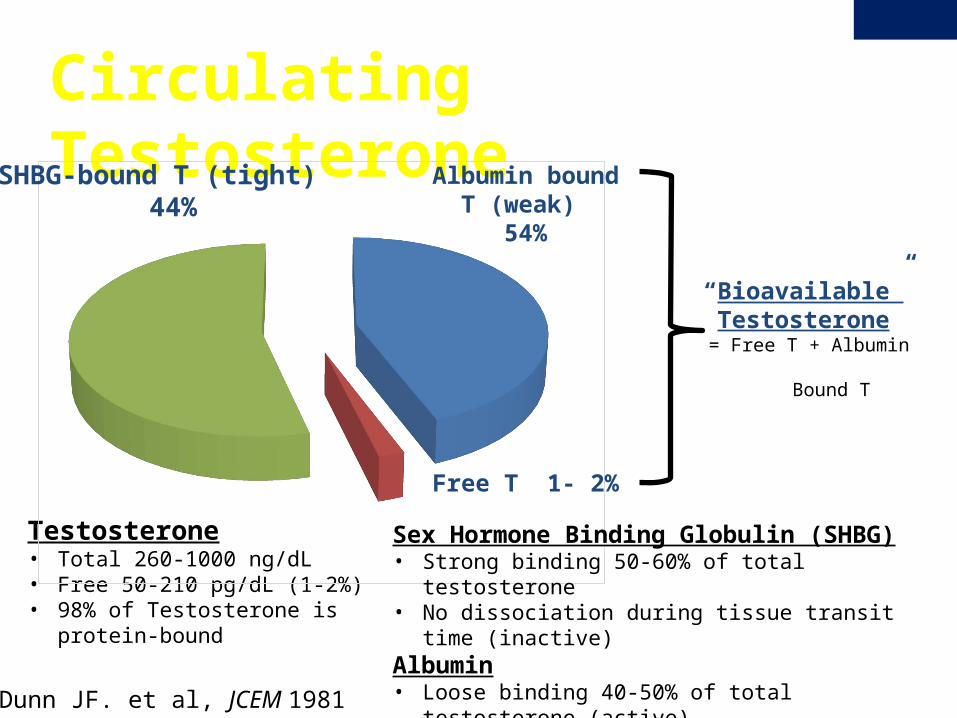
Circulating Testosterone
Testosterone• Total 260-1000 ng/dL • Free 50-210 pg/dL (1-2%) • 98% of Testosterone is protein-bound
SHBG-bound T (tight) 44%
Albumin bound T (weak)
54%
Free T 1- 2%
“Bioavailable” Testosterone
= Free T + Albumin Bound T
Sex Hormone Binding Globulin (SHBG)• Strong binding 50-60% of total testosterone• No dissociation during tissue transit time (inactive)Albumin• Loose binding 40-50% of total testosterone (active)
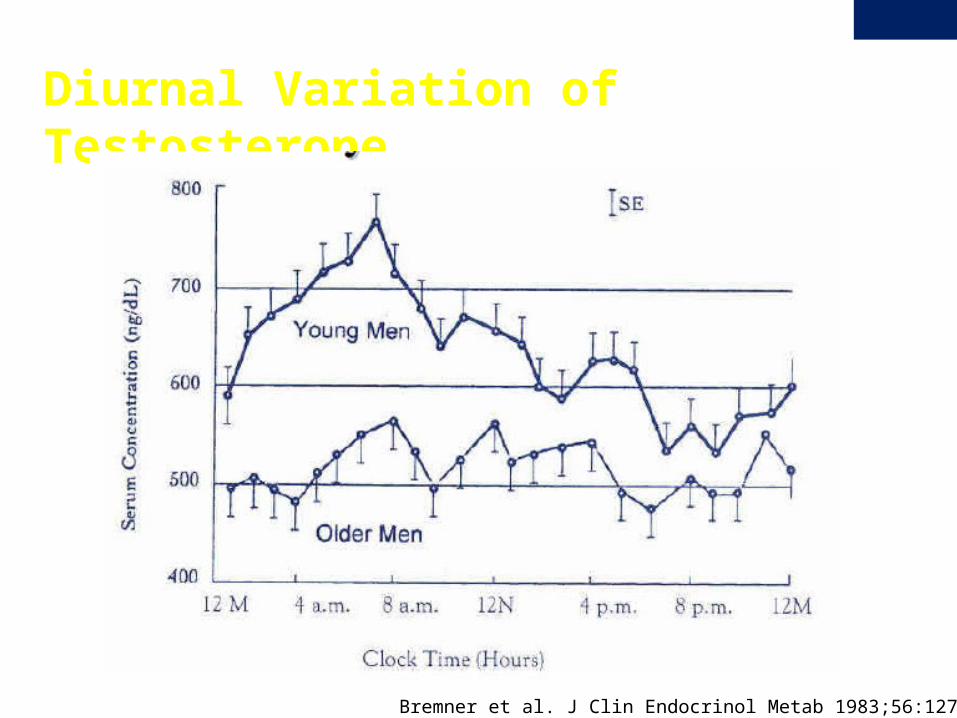
Diurnal Variation of Testosterone
Bremner et al. J Clin Endocrinol Metab 1983;56:1278-81.
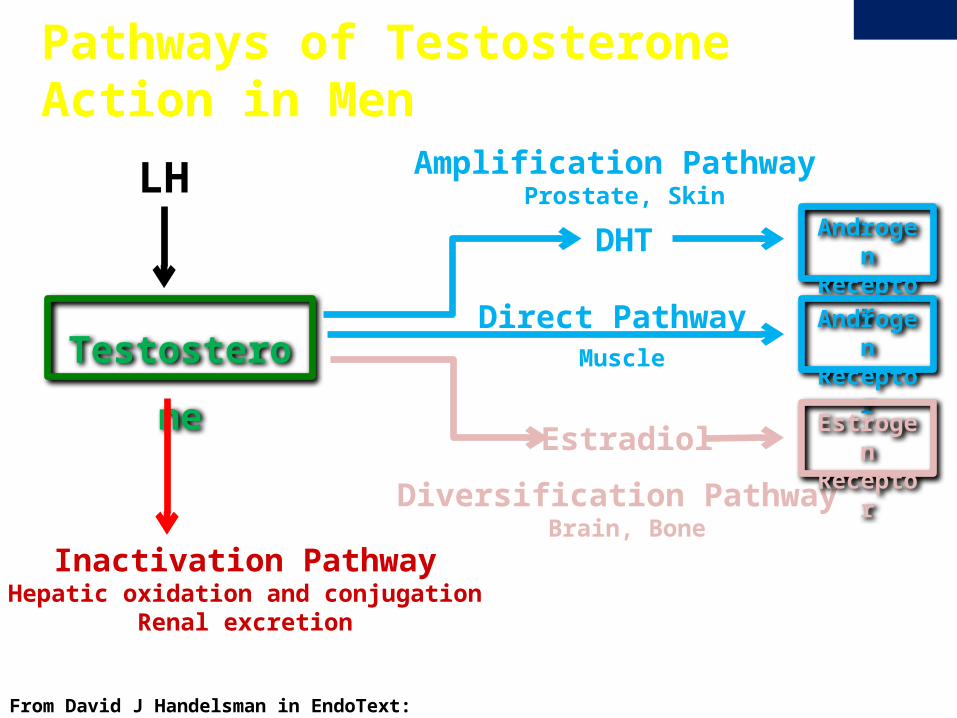
From David J Handelsman in EndoText: http://www.endotext.org/male/male2/maleframe2.htm
Pathways of Testosterone Action in Men
Testosterone
LH
Inactivation PathwayHepatic oxidation and conjugation
Renal excretion
Amplification Pathway Prostate, Skin
Direct Pathway Muscle
DHT
Estradiol
Diversification Pathway Brain, Bone
Androgen
Receptor
Androgen
Receptor
EstrogenReceptor
Actions of Testosterone in Males
Androgenic Activity of Testosterone
• Mediated through binding to the androgen receptor (AR)• AR has high binding affinity for testosterone & DHT• AR does not bind androstenedione, DHEA, DHEAs
Non-Androgenic Activity of Testosterone
• Mediated through aromatization to estradiol which binds to the estrogen receptor
• Estrogen functions in feed back regulation of LH, spermatogenesis, bone homeostasis, lipid metabolism, cardiovascular physiology
• Male estrogen ~20-30 pg/mL, 80% from aromatization, 20% from testis
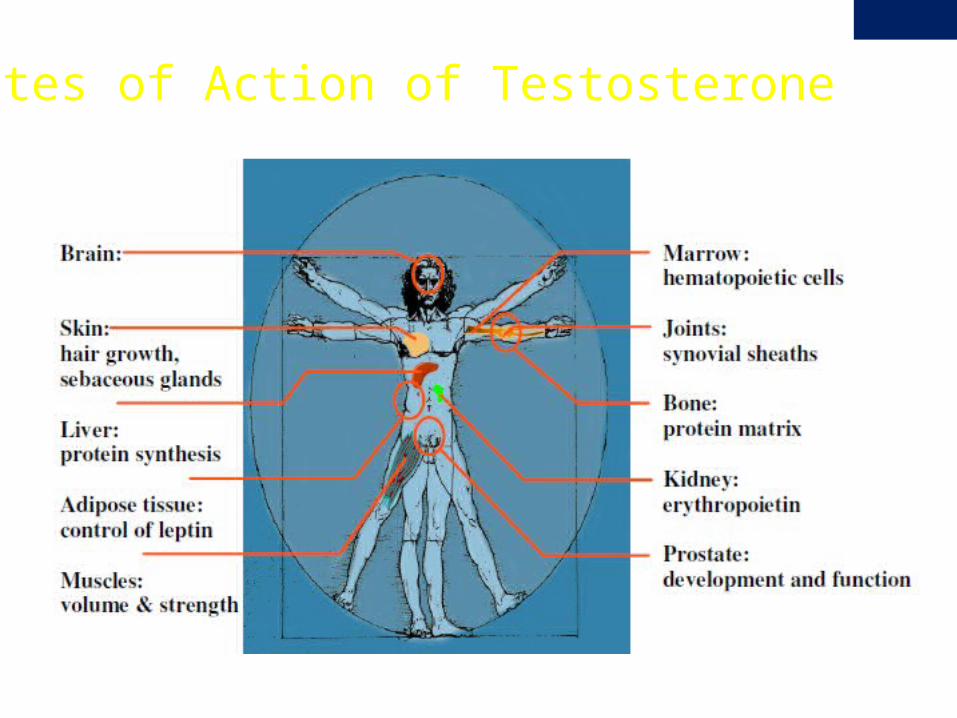
Sites of Action of Testosterone
Male Hypogonadism
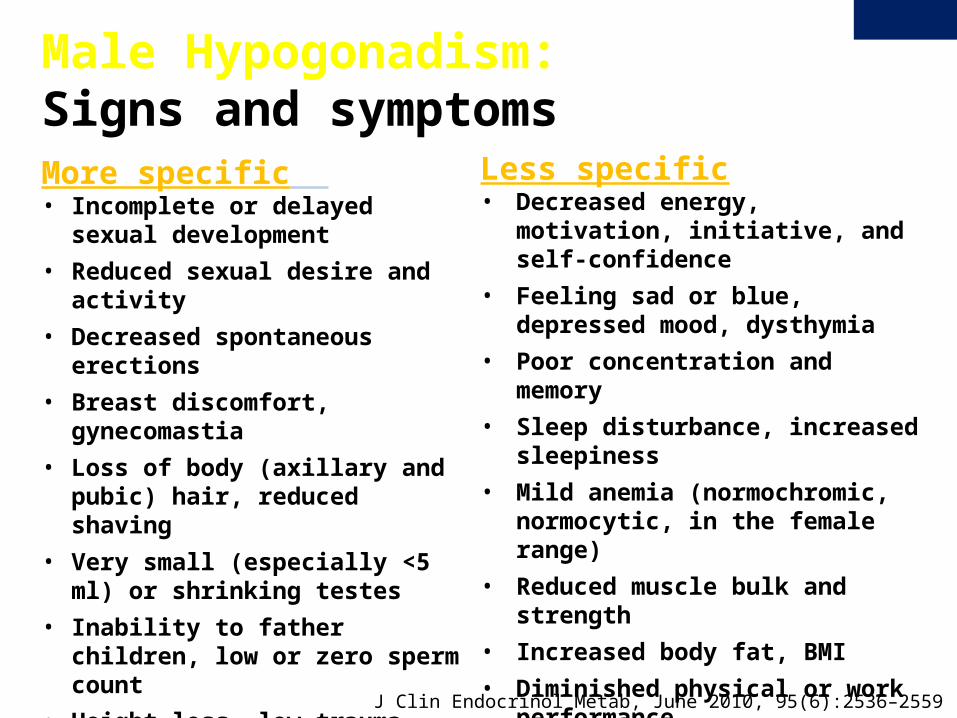
More specific • Incomplete or delayed sexual
development• Reduced sexual desire and activity• Decreased spontaneous erections• Breast discomfort, gynecomastia• Loss of body (axillary and pubic) hair,
reduced shaving• Very small (especially <5 ml) or
shrinking testes• Inability to father children, low or zero
sperm count• Height loss, low trauma fracture, low
BMD• Hot flushes, sweats
Male Hypogonadism: Signs and symptoms
Less specific• Decreased energy, motivation, initiative,
and self-confidence• Feeling sad or blue, depressed mood,
dysthymia• Poor concentration and memory• Sleep disturbance, increased sleepiness• Mild anemia (normochromic, normocytic,
in the female range)• Reduced muscle bulk and strength• Increased body fat, BMI• Diminished physical or work performance
J Clin Endocrinol Metab, June 2010, 95(6):2536–2559
Primary hypogonadism • Klinefelter syndrome• Testicular failure
Secondary hypogonadism• Kallmann’s syndrome • Pituitary disease: pituitary adenomas, hypopituitarism, infiltrative
disorders• Hemochromatosis• Hyperprolactinemia• Drugs: anabolic and corticosteroids, opioids, others• Chronic Liver Disease• Acute illness • Other
Male Hypogonadism: Causes
Congenital• Klinefelter syndrome• Cryptorchidism and defects of
testis development• Testicular biosynthetic defects• Sertoli-cell-only syndrome• LH resistance
Primary Hypogonadism: Causes
Acquired• Orchitis• Orchidectomy• Chemotherapy and other
toxins• Radiation therapy• Trauma/torsion
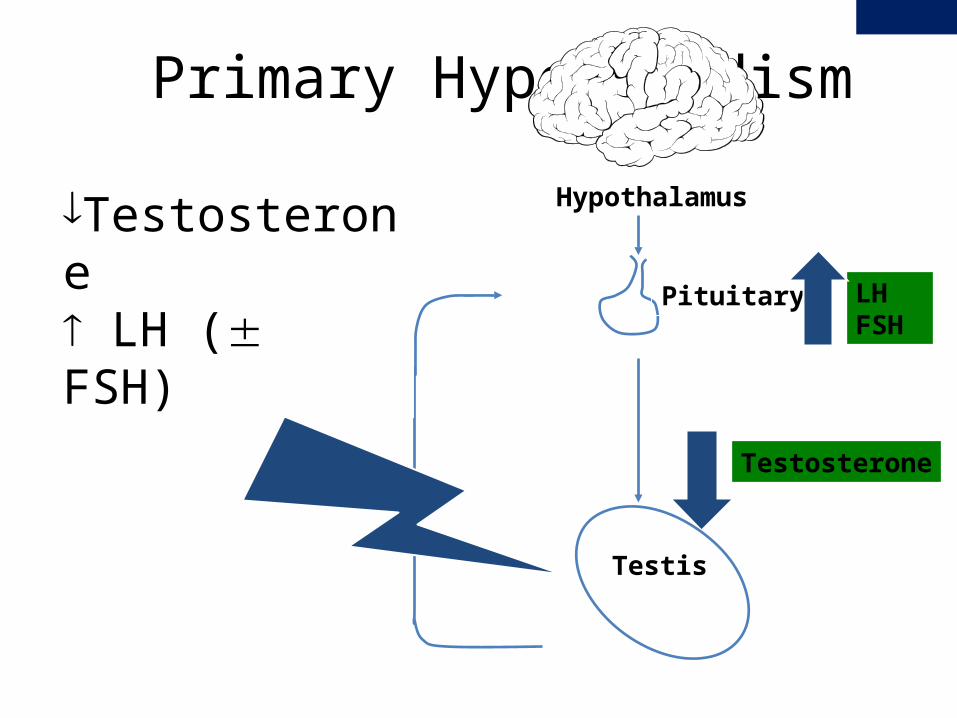
Primary Hypogonadism
Hypothalamus
Pituitary LHFSH
Testosterone
Testis
¯Testosterone LH ( FSH)
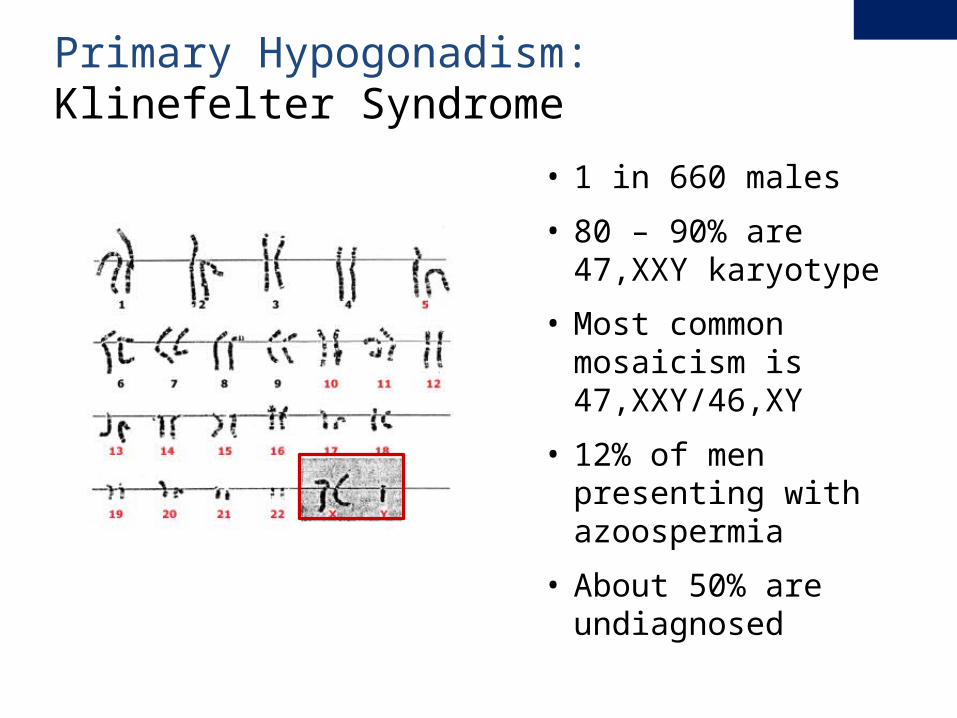
• 1 in 660 males
• 80 – 90% are 47,XXY karyotype
• Most common mosaicism is 47,XXY/46,XY
• 12% of men presenting with azoospermia
• About 50% are undiagnosed
Primary Hypogonadism: Klinefelter Syndrome
• Elevated FSH, LH and low testosterone• Reduced libido, erectile dysfunction, infertility, low
sperm count• Reduced facial and body hair• Gynecomastia• Small testes• Taller than average height• Low bone mass/osteoporosis
Primary Hypogonadism: Klinefelter Syndrome: Signs and Symptoms
• Difficulty in social interactions throughout life.
• Impairment of higher level linguistic competence but relative sparing of vocabulary and understanding of language
• Deficit in the ability to sustain attention without impulsivity
• “Characterized by marked lack of insight, poor judgment, and impaired ability to learn from adverse experience”
Primary Hypogonadism: Klinefelter Syndrome: Psychosocial
1. Bender BG, Linden MG, Robinson A.. Am J Med Genet 1993; 48:169.2. Simm PJ, Zacharin MR.. J Pediatr Endocrinol Metab 2006; 19:499.
3. Ross, JL, Roeltgen, JP, Stefanatos, G, et al. Am J Medical Genetics 2008; 146A:708.
• Pulmonary diseases including chronic bronchitis, bronchiectasis, and emphysema
• Certain malignancies: • Germ cell tumors • Breast cancer • Non-Hodgkin lymphoma
• Varicose veins and leg ulcers• Systemic lupus erythematosus• Diabetes mellitus
Primary Hypogonadism: Klinefelter Syndrome: Other Co-morbidities
Bojesen A, Juul S, Birkebaek NH, Gravholt CH. Morbidity in Klinefelter syndrome: a Danish register study based on hospital discharge diagnoses. J Clin Endocrinol Metab 2006; 91:1254.
LHFSH
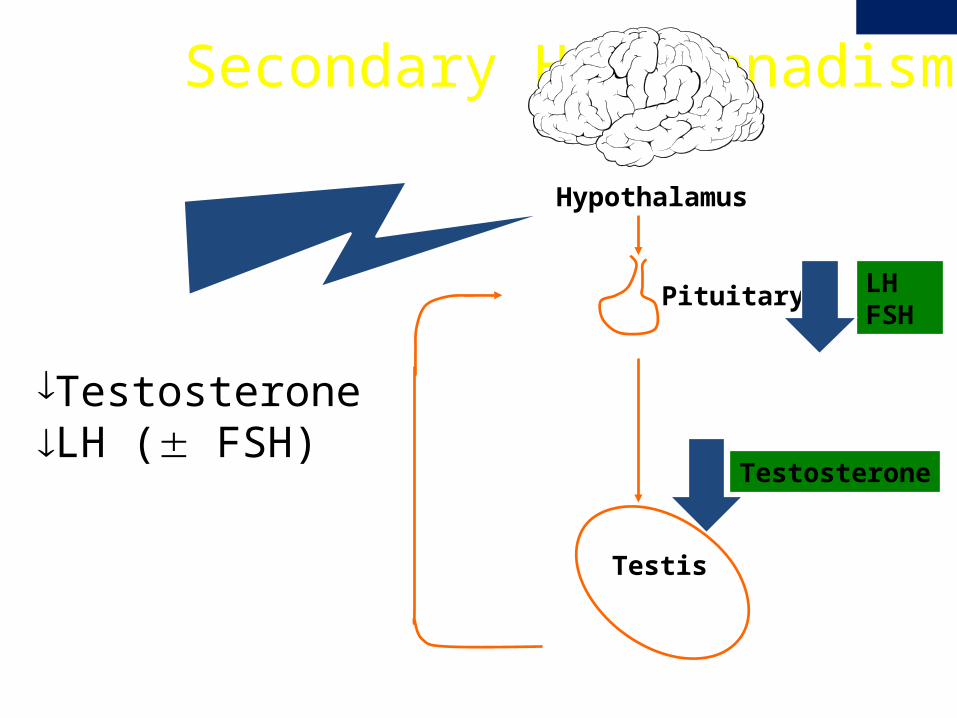
Secondary Hypogonadism
Hypothalamus
Pituitary
Testosterone
Testis
¯TestosteroneLH ( FSH)
Congenital• Kallmann syndrome• Fertile eunuch syndrome• Adrenal Hypoplasia
Congenita• Genetic defects of the
gonadotropin subunits• Prader-Willi syndrome• Laurence- Moon-Biedl
syndrome• Other
Secondary Hypogonadism: Causes
AcquiredStructural:• Tumors: Craniopharyngioma
Pituitary adenomas, glioma, meningioma• Infiltrative disorders: Sarcoidosis,
hemochromatosis, histiocytosis X• Head trauma• Radiation therapy• Hypopituitarism Functional: • Exercise, Anorexia, Anabolic steroids,
Glucocorticoid therapy, Opioids, Critical illness, Other
Secondary Hypogonadism: Kallman’s Syndrome
• Hypogonadism due to deficient hypothalamic secretion of GnRH
• Hypogonadism may be severe, mild, or even transient • One or more non-gonadal congenital abnormalities:
• Anosmia• Red-green color blindness• Midline facial abnormalities such as cleft palate• Urogenital tract abnormalities• Synkinesis (mirror movements)• Neurosensory hearing loss
• Usually sporadic, but familial forms can occur (typically X-linked)
• Mutations in KAL1, fibroblast growth factor receptor , PROK2, and PROKR-2

Secondary Hypogonadism: Acquired due to Severe Illness
Serum testosterone concentration on admission (left panel) and the nadir level in the hospital (right panel) in men with critical illness according to disease severity as measured by the APACHE score. Men with increasingly severe illnesses have lower serum testosterone concentrations. Redrawn from Spratt, DI, Cox, P, Orav, J, et al, J Clin Endocrinol Metab 1993: 76:1548.
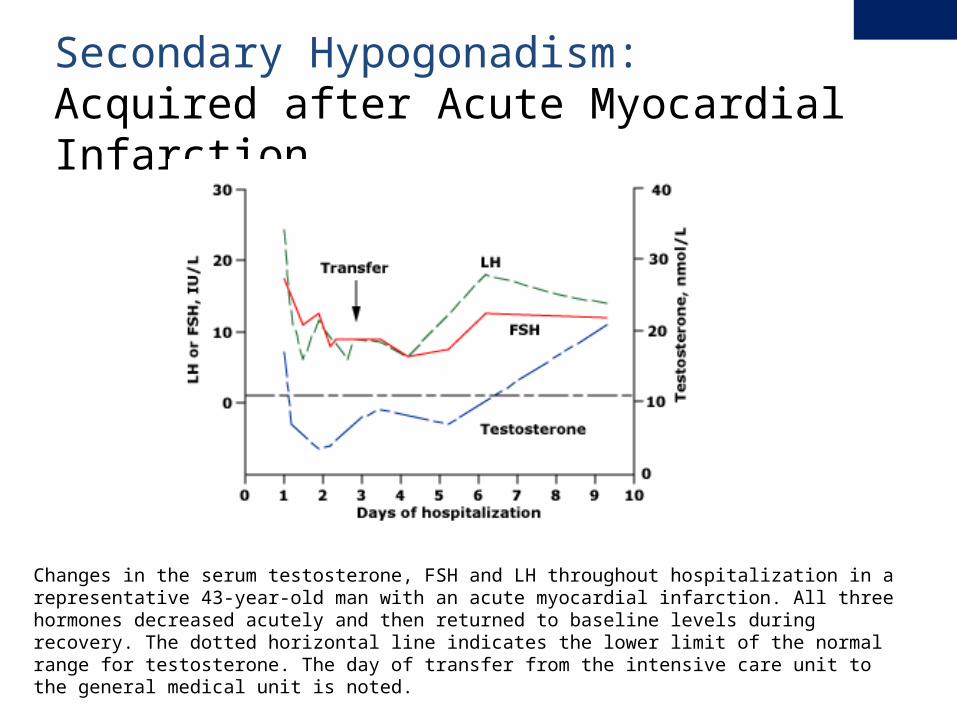
Secondary Hypogonadism: Acquired after Acute Myocardial Infarction
Changes in the serum testosterone, FSH and LH throughout hospitalization in a representative 43-year-old man with an acute myocardial infarction. All three hormones decreased acutely and then returned to baseline levels during recovery. The dotted horizontal line indicates the lower limit of the normal range for testosterone. The day of transfer from the intensive care unit to the general medical unit is noted.
Redrawn from Spratt, DI, Cox, P, Orav, J, et al, J Clin Endocrinol Metab 1993; 76:1548.
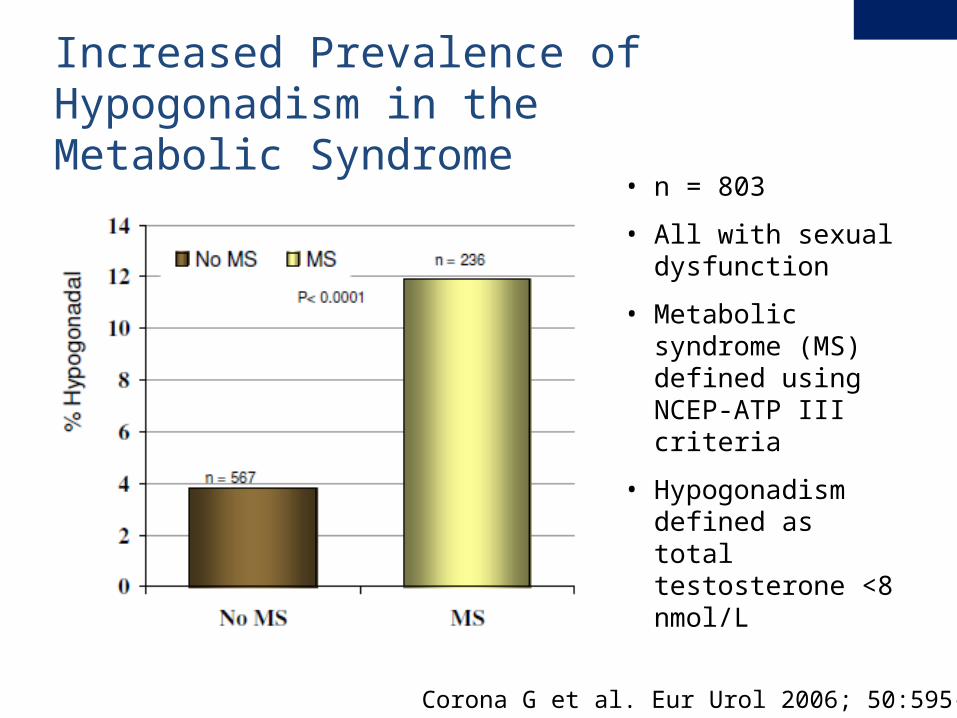
• n = 803
• All with sexual dysfunction
• Metabolic syndrome (MS) defined using NCEP-ATP III criteria
• Hypogonadism defined as total testosterone <8 nmol/L
Increased Prevalence of Hypogonadism in theMetabolic Syndrome
Corona G et al. Eur Urol 2006; 50:595-604
• Prospective study: 794 men, ages 50 – 90 years
• 3.05 fold (CI 1.88 – 4.95) increased prevalence of low testosterone in metabolic syndrome patients
• In men with low testosterone: 1.33 (CI 1.10 – 1.62) risk of death
Hypogonadism in the Metabolic Syndrome: Associated with Increased Mortality
Laughlin G et al. Endocrine Society Annual Meeting 2007;OR55-2.
• Age-related decline begins ~30-40 years of age at approximately 1.2% per year
• Average testosterone age 75 compared to age 25:• Total i35%• Bioavailable i50%
However, many men in the 7th & 8th decade have normal testosterone levels
Effect of Age on Testosterone
1 Harman SM et al. J Clin Endocrinol Metab 2001;86:7242 Feldman HA, et al. J Clin Endocrinol Metab 2002;87:589
3Ferrini RL, Barrett-Connor E. Am J Epidemiol 1998;147:750
Various ill-defined terminologies have been suggested:
• Late Onset Hypogonadism (LOH)1
• Andropause1
• Syndrome of Male Hypogonadism2
• Androgen Deficiency in the Aging Male (ADAM)2
• Middle-Age Crisis3
• Testosterone Deficiency Syndrome (TDS)3
• “MAN”-o-pause
Age-related Decline in Testosterone
1. Bassil, Nazem et al. Therapeutics and Clinical risk Management 2009;5:427-4482. Hernandez et al. Postgraduate Medicine 2008;120(4):733. Delev et al. Folia Medica 2009;51(1):15
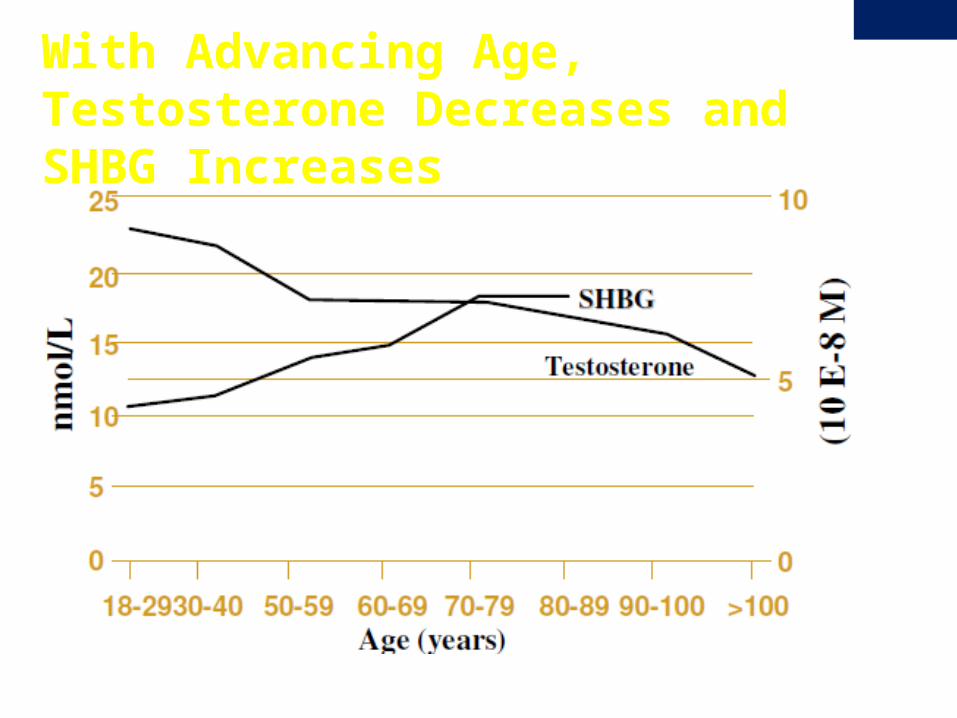
With Advancing Age, Testosterone Decreases and SHBG Increases
Testis1
i Volume 30% Number Leydig cells g
i Testosterone secretion
Neuroendocrine regulation2
Loss of GnRH timing release g i LH signaling to Leydig cells g
i Testosterone secretion
Increased SHBG3
i Nonspecific more tightly bound fraction of testosterone g i Bioavailable testosterone
1Mulligan T, Iranmanesh A, Veldhuis JD. J Clin Endocrinol Metab 2001;86:55472Deslypere JP, et al. J Clin Endocrinol Metab 1987;64:68
3 Mechanism unclear
Mechanism of Decreased Testosterone with Age
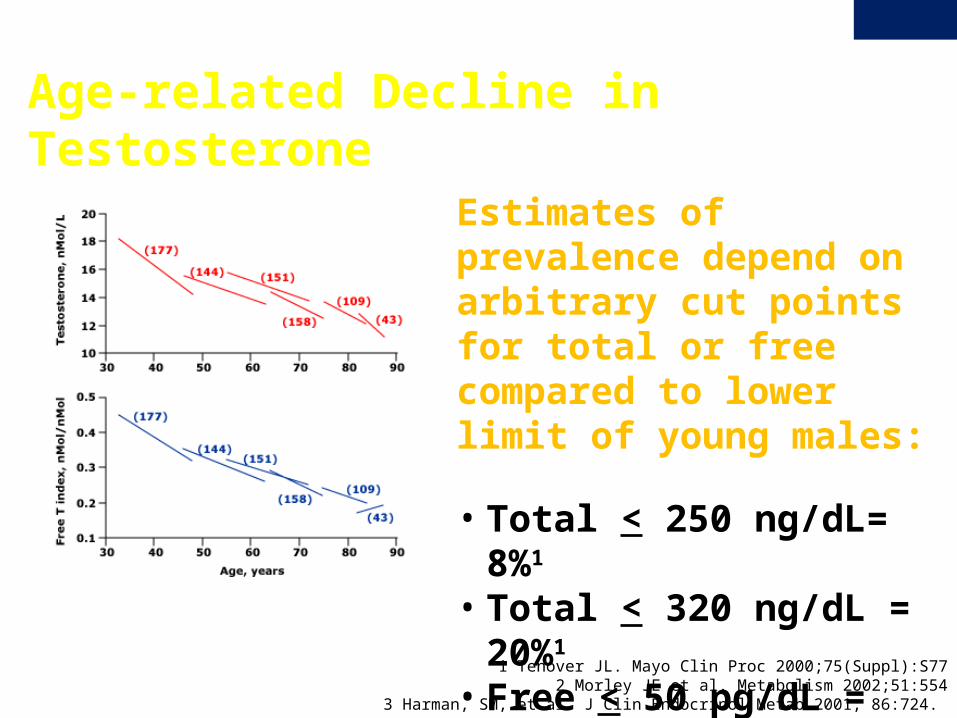
Age-related Decline in Testosterone
Estimates of prevalence depend on arbitrary cut points for total or free compared to lower limit of young males:
• Total < 250 ng/dL= 8%1
• Total < 320 ng/dL = 20%1
• Free < 50 pg/dL = 33%2
1 Tenover JL. Mayo Clin Proc 2000;75(Suppl):S772 Morley JE et al. Metabolism 2002;51:554
3 Harman, SM, et al. J Clin Endocrinol Metab 2001; 86:724.
Diagnosis and Initial Evaluation of Male
Hypogonadism
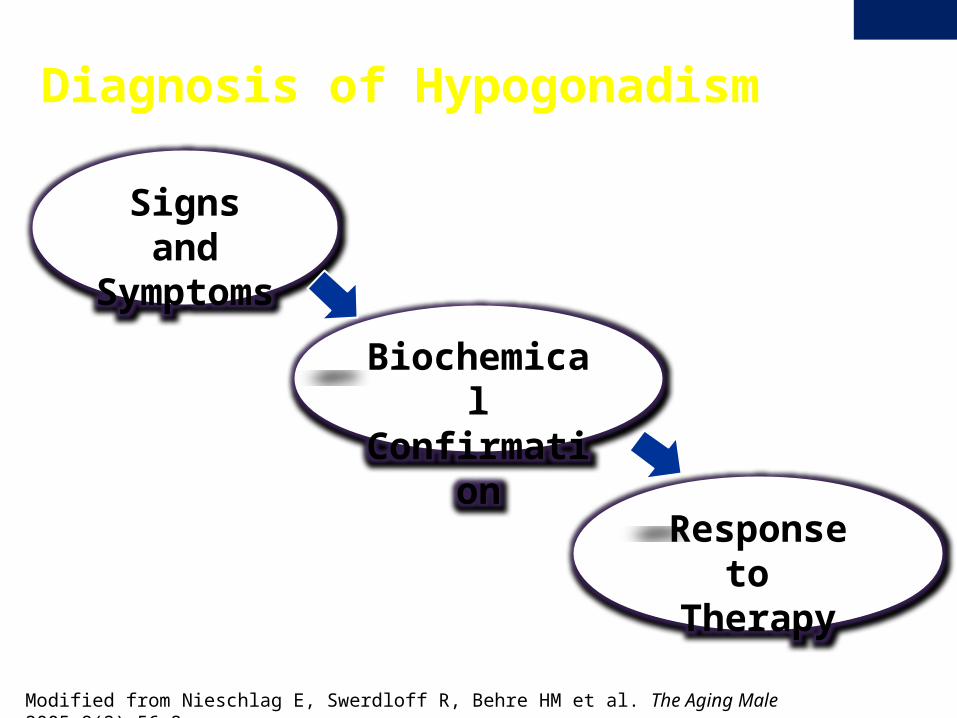
Modified from Nieschlag E, Swerdloff R, Behre HM et al. The Aging Male 2005;8(2):56-8.
Signs and Symptoms
Biochemical Confirmation
Response to Therapy
Diagnosis of Hypogonadism
i libidoi virilityi sexual activityi energyi cognitive functioni bone mineral densityi muscle massh insulin resistance and central adiposityi erectile function h insomnia, nervousness, hot flashesh apathy, depressed mood
Possible signs and symptoms of testosterone deficiency
J Clin Endocrinol Metab, June 2010, 95(6):2536–2559
• Do you have a decrease in sex drive?• Do you have a lack of energy?• Do you have a decrease in strength and/or endurance?• Have you lost height?• Have you noticed a decreased enjoyment of life?• Are you sad and/or grumpy?• Are your erections less strong?• Has it been more difficult to maintain your erection• throughout sexual intercourse?• Are you falling asleep after dinner?• Has your work performance deteriorated recently?
ADAM Questionnaire
Morley, J et al. Metabolism. 2000;49: 1239-1242
• Hypopituitarism, sellar mass, radiation to the sellar region, or other diseases of the sellar region
• Treatment with medications that affect testosterone production or metabolism, such as glucocorticoids and opioids
• HIV-associated weight loss• End-stage renal disease on hemodialysis• Moderate to severe chronic obstructive lung disease• Infertility• Osteoporosis or low trauma fracture, especially in a young
man• Type 2 diabetes mellitus• Other disorders
Conditions with high prevalence of low testosterone in which testing is advised
Endocrine Society Clinical Practice Guideline for Testosterone Therapy in Adult Men with Androgen Deficiency Syndromes. J Clin Endocrinol Metab, June 2010, 95(6):2536–2559
Initial Evaluation and Biochemical Confirmation of Male Hypogonadism
J Clin Endocrinol Metab, June 2010, 95(6):2536–2559
1. ALWAYS rule out other potential causes of symptoms:• Untreated sleep apnea• Uncontrolled diabetes or hypertension • Other chronic disease (liver, renal failure, thyroid, etc)• Anemia, malnutrition, acute illness
2. Order initial laboratory studies:• AM total, free and bioavailable testosterone
3. If low testosterone identified:• Confirm by repeating AM testosterones at least once• Determine if primary vs. secondary: LH, FSH• Evaluate for possible causes: CMP, prolactin, iron studies• If secondary hypogonadism or hprolactin, consider MRI• Confirm there are no contraindications prior to beginning therapy: PSA,
digital rectal exam, CBC
Total Testosterone: • Methods: radioimmunoassay (RIA ), immunometric
assays, or liquid chromatography tandem mass spectrometry
• Affected by abnormal levels of SHBG• Low SHBG may result in low-normal (< 300 ng/ml) or
slightly below normal total testosterone in men who are eugonadal
• High SHBG may result in low normal total testosterone measurements in men with hypogonadism
Laboratory Assays:Total Testosterone
J Clin Endocrinol Metab, June 2010, 95(6):2536–2559
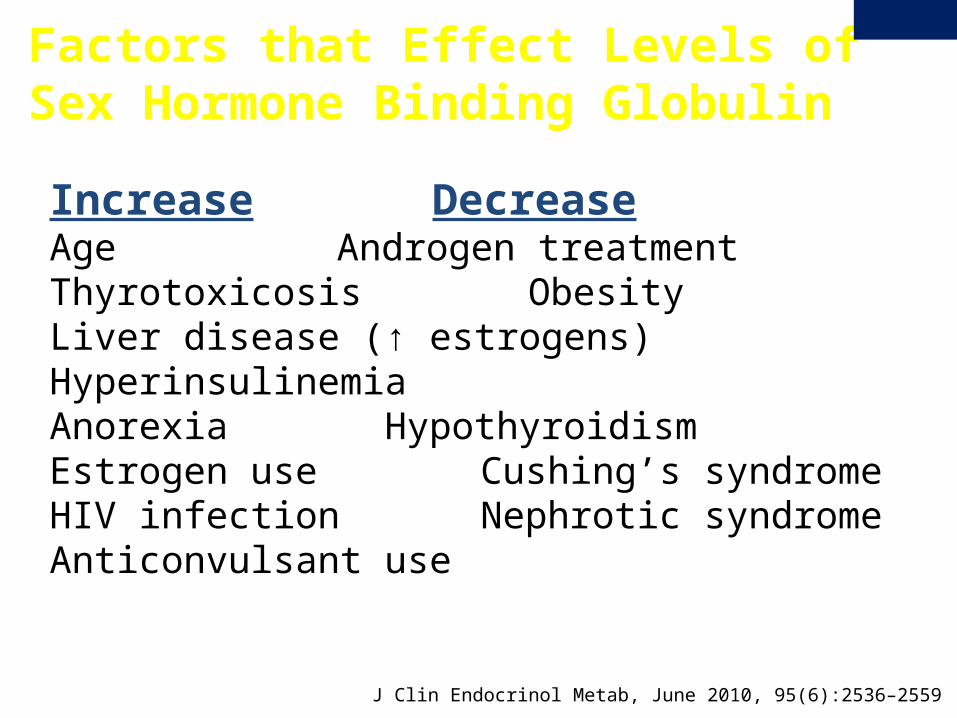
Increase DecreaseAge Androgen treatmentThyrotoxicosis ObesityLiver disease (↑ estrogens) HyperinsulinemiaAnorexia HypothyroidismEstrogen use Cushing’s syndromeHIV infection Nephrotic syndromeAnticonvulsant use
Factors that Effect Levels of Sex Hormone Binding Globulin
J Clin Endocrinol Metab, June 2010, 95(6):2536–2559
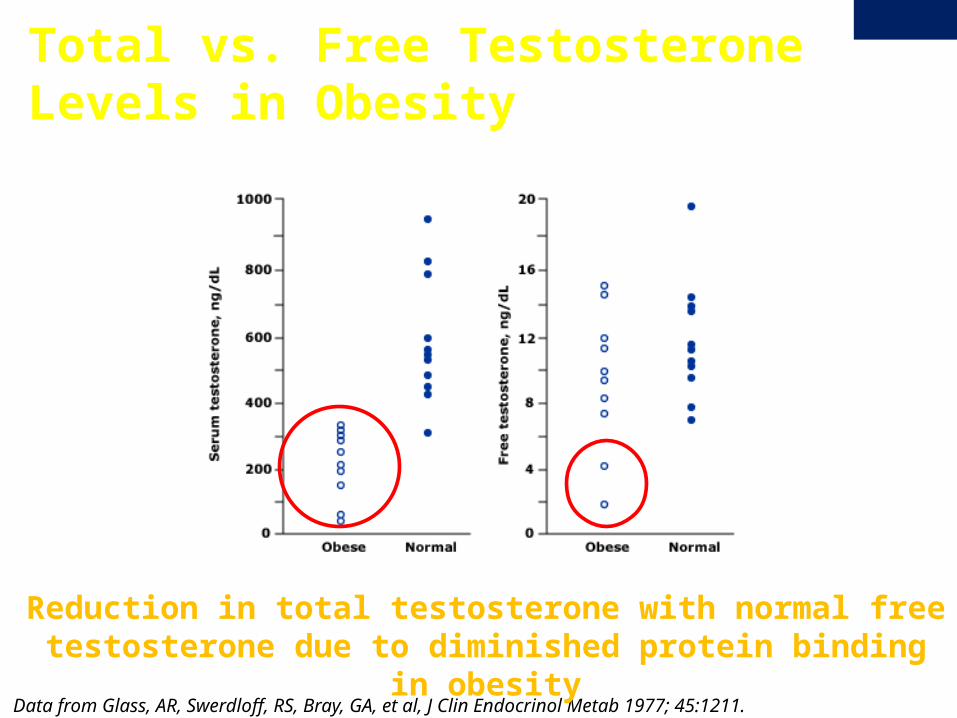
Data from Glass, AR, Swerdloff, RS, Bray, GA, et al, J Clin Endocrinol Metab 1977; 45:1211.
Reduction in total testosterone with normal free testosterone due to diminished protein binding in obesity
Total vs. Free Testosterone Levels in Obesity
‘Direct’ free T • Common analog displacement assay• Flawed methodology- not reliable- should not be used.
Calculated free T • Better than analog assay but affected by accuracy of assays used to
measure total testosterone and serum binding proteins
Free T by equilibrium dialysis• Reliable and gold standard but more expensive• Available only at certain reference labs
Bioavailable Testosterone:• Accurate measure of “free” and albumin-bound (ie biologically
active) testosterone
Laboratory Assays:Free Testosterone
J Clin Endocrinol Metab, June 2010, 95(6):2536–2559
AACE Hypogonadism Guidelines, Endocr Pract. 2002;8(No. 6)
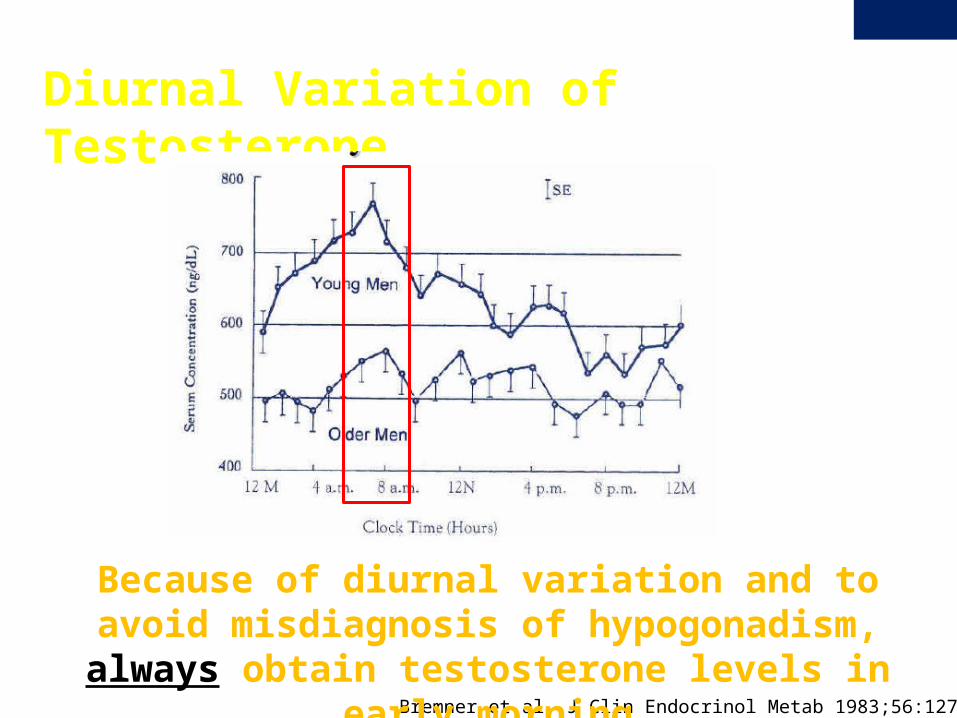
Diurnal Variation of Testosterone
Bremner et al. J Clin Endocrinol Metab 1983;56:1278-81.
Because of diurnal variation and to avoid misdiagnosis of hypogonadism, always obtain testosterone levels in early
morning
Variability of Testosterone: A Single Low Value DOES NOT Diagnose Hypogonadism
• 30% of men with testosterone in mildly hypogonadal range will be normal on repeat measurements
• 15% of healthy young men may have a testosterone transiently below the normal range in a 24-hour period
• A substantial number of men ages 65 - 80 who have low serum testosterone in the afternoon will have normal testosterone in the morning
Brambilla DJ, O’Donnell AB, Matsumoto AM, McKinlay JB 2007 I ntraindividual variation in levels of serum testosterone and other reproductive and adrenal hormones in men. Clin Endocrinol (Oxf) 67:853-862
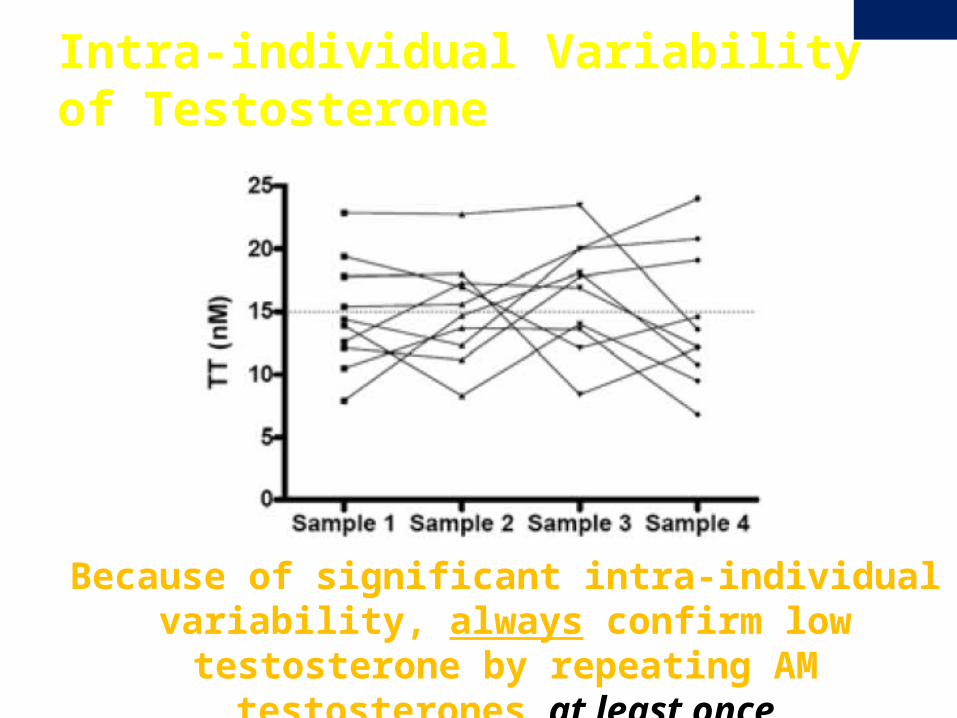
Intra-individual Variability of Testosterone
Because of significant intra-individual variability, always confirm low testosterone by repeating AM testosterones
at least once
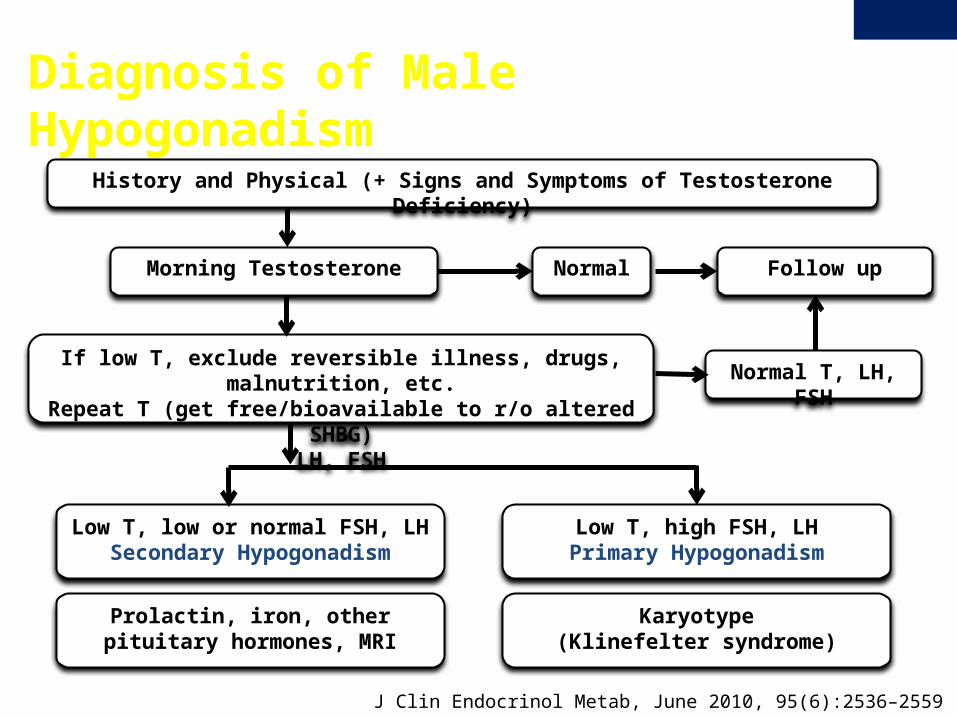
Diagnosis of Male Hypogonadism
J Clin Endocrinol Metab, June 2010, 95(6):2536–2559
History and Physical (+ Signs and Symptoms of Testosterone Deficiency)
Morning Testosterone
If low T, exclude reversible illness, drugs, malnutrition, etc.Repeat T (get free/bioavailable to r/o altered SHBG)
LH, FSH
Follow up
Low T, low or normal FSH, LHSecondary Hypogonadism
Low T, high FSH, LHPrimary Hypogonadism
Prolactin, iron, other pituitary hormones, MRI
Karyotype(Klinefelter syndrome)
Normal T, LH, FSH
Normal
What about a low normal total testosterone (<300 ng/dl)?
J Clin Endocrinol Metab, June 2010, 95(6):2536–2559
1. If testosterone was not drawn in AM- repeat in AM
2. If acute illness or other reasons to have low testosterone- ALWAYS address these causes first (if possible) and repeat AM testosterone again.
3. Get bioavailable (or calculated free) testosterone in AM
• If bioavailable/calculated free testosterone normal, patient is eugonadal and does not need testosterone therapy at this time (even despite having low-normal or even slightly-low total testosterone)
What about a low normal total testosterone (<300 ng/dl)?
J Clin Endocrinol Metab, June 2010, 95(6):2536–2559
4. If still unsure whether patient has hypogonadism or not- repeat again (DO NOT begin testosterone therapy until certain of diagnosis)
5. If patient has consistently below normal or low-normal total AND low bioavailable/calculated free AM testosterones AND ALSO symptoms possibly due to testosterone deficiency- consider trial of therapy:
• If patient responds- continue therapy and monitor as appropriate.
• If no response within 2 or 3 months despite therapeutic testosterone levels- discontinue.

Testosterone Replacement Therapy
• Provide testosterone therapy only in those with confirmed androgen deficiency
• Replicate physiological testosterone levels so they are comparable (ie biologically identical) with eugonadal men.
• Restore benefits of normal androgen status with no more adverse events than eugonadal men of similar age.
Testosterone Replacement Therapy: Goals of Therapy
Endocrine Society Clinical Practice Guideline for Testosterone Therapy in Adult Men with Androgen Deficiency Syndromes. J Clin Endocrinol Metab, June 2010, 95(6):2536–2559
• There is no upper age limit for androgen replacement therapy
• Testosterone therapy unlikely to prolong life, as androgen deficiency does not shorten life expectancy*
• However, there may be other potential benefits of therapy in hypogonadal males, including in elderly men
Testosterone Replacement Therapy: in Older Men
*Liu PY, Death AK, Handelsman DJ Endocr Rev 2003
Testosterone Replacement Therapy: Potential BenefitsLikely • Improved libido• Improved muscle mass
and decreased fat mass• Increased strength • Increased bone density• Improved sense of well
being and mood
Possible? (not confirmed in all studies)• Improved A1c and lipids in
men with type 2DM?• Improvements in cognition
and/or depression ?
NOTE: These beneficial effects have only been seen in men with
documented hypogonadism
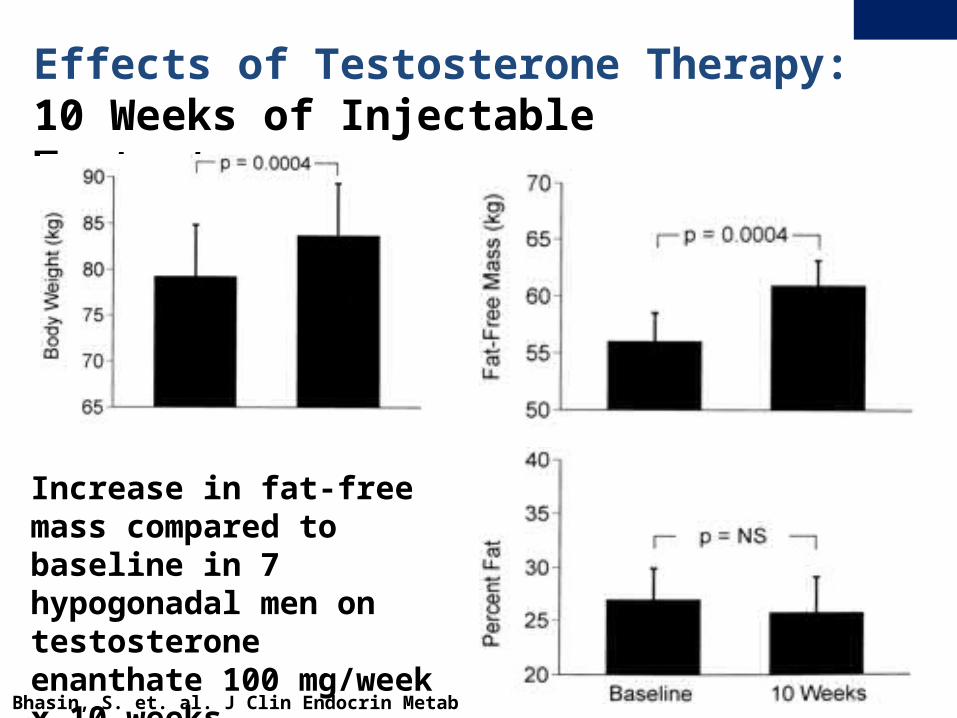
Effects of Testosterone Therapy:10 Weeks of Injectable Testosterone
Increase in fat-free mass compared to baseline in 7 hypogonadal men on testosterone enanthate 100 mg/week x 10 weeks
Bhasin, S. et. al. J Clin Endocrin Metab 1997;82:407
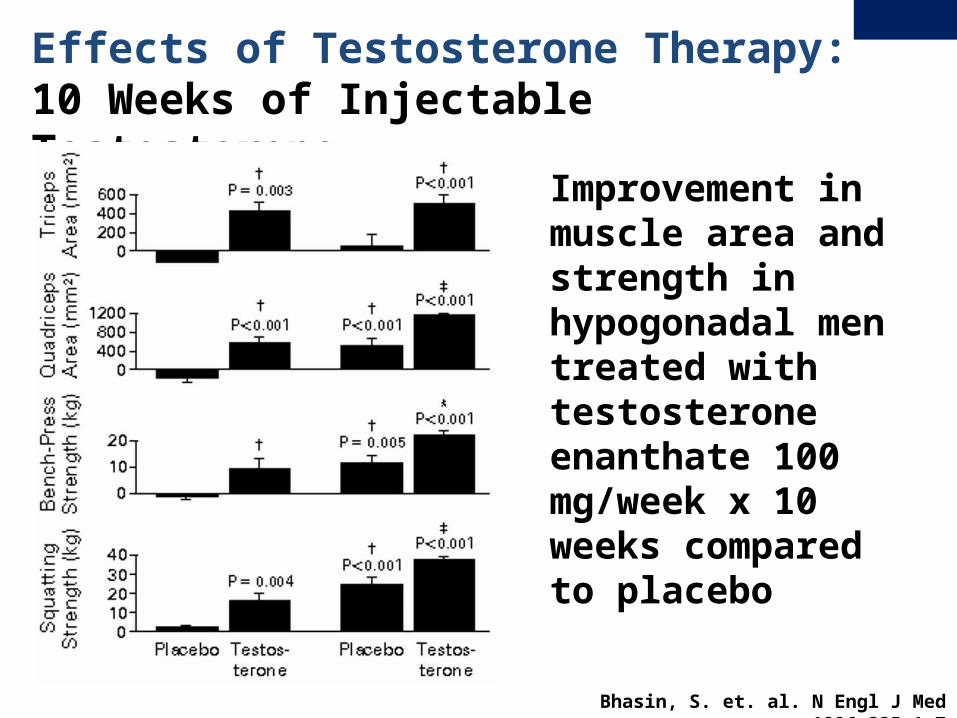
Effects of Testosterone Therapy:10 Weeks of Injectable Testosterone
Improvement in muscle area and strength in hypogonadal men treated with testosterone enanthate 100 mg/week x 10 weeks compared to placebo
Bhasin, S. et. al. N Engl J Med 1996;335:1-7
1. Wang, J Clin Endocrinol Metab. 81:3578, 19962. Snyder,JCEM. 1999;84:26473. Wang, JCEM. 2000;85:2839
• Improved sense of well-being and mood1
• Improved sense of well-being with transdermal T therapy in older men with serum total < 3502
• Similar findings in testosterone gel (study included older men with low-normal serum T)3
Effects of Testosterone Therapy:Sense of Well-Being and Mood
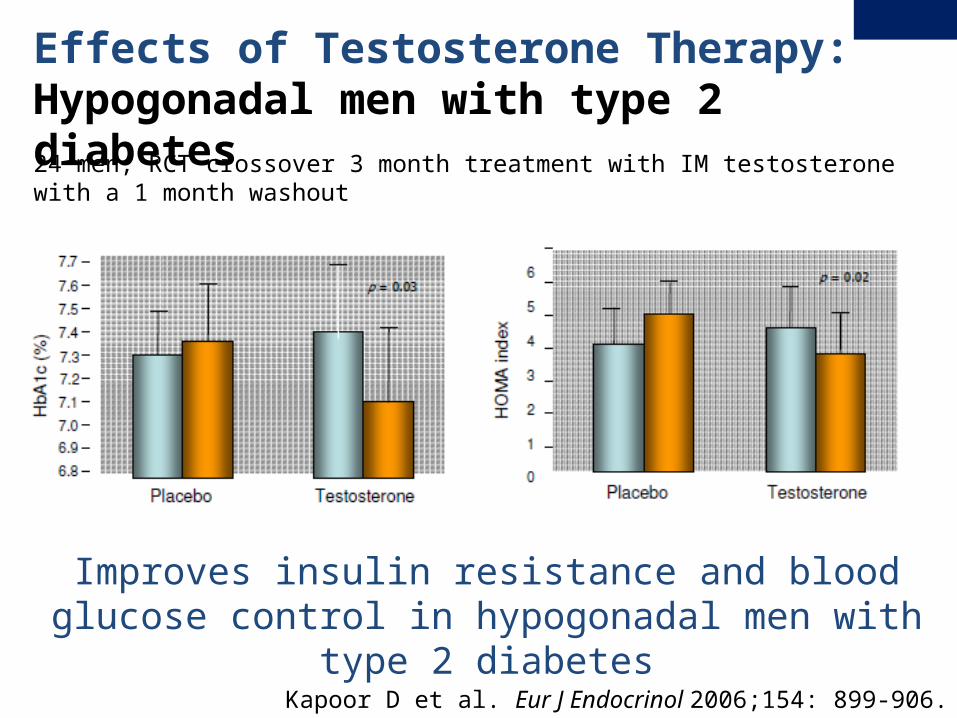
Improves insulin resistance and blood glucose control in hypogonadal men with type 2 diabetes
Effects of Testosterone Therapy: Hypogonadal men with type 2 diabetes
Kapoor D et al. Eur J Endocrinol 2006;154: 899-906.
24 men, RCT crossover 3 month treatment with IM testosterone with a 1 month washout
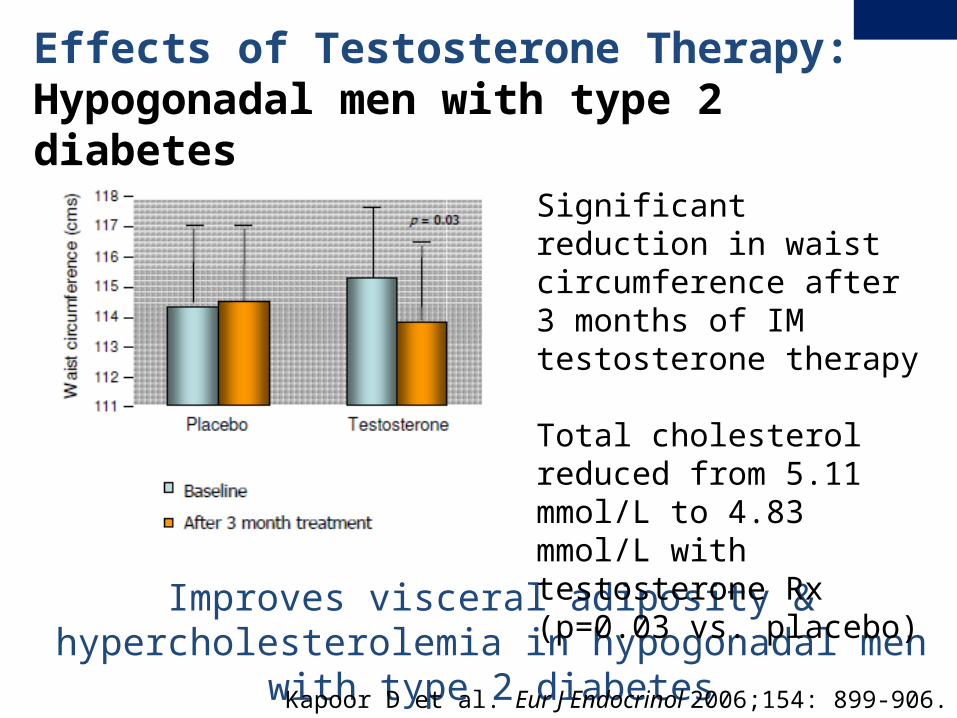
Improves visceral adiposity & hypercholesterolemia in hypogonadal men with type 2 diabetes
Effects of Testosterone Therapy: Hypogonadal men with type 2 diabetes
Significant reduction in waist circumference after 3 months of IM testosterone therapy
Total cholesterol reduced from 5.11 mmol/L to 4.83 mmol/L with testosterone Rx (p=0.03 vs. placebo)
Kapoor D et al. Eur J Endocrinol 2006;154: 899-906.
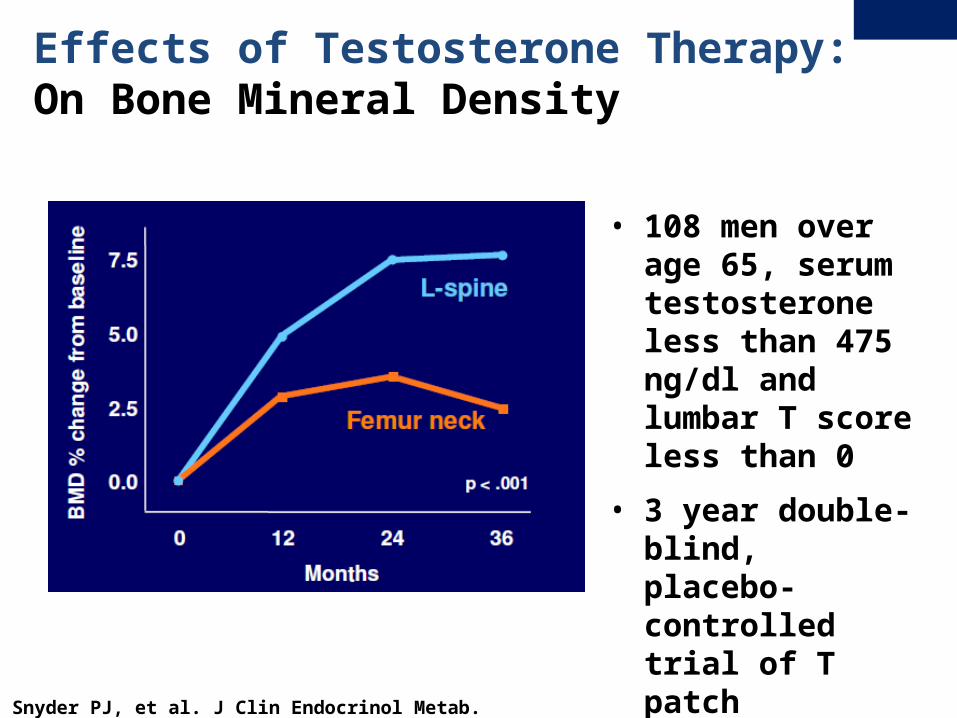
Effects of Testosterone Therapy: On Bone Mineral Density
• 108 men over age 65, serum testosterone less than 475 ng/dl and lumbar T score less than 0
• 3 year double-blind, placebo-controlled trial of T patch
Snyder PJ, et al. J Clin Endocrinol Metab. 1999;84:2647-53

Effects of Testosterone Therapy: On Bone Mineral Density
• Spine BMD response to 3 years of testosterone therapy depended on level of testosterone before treatment
• Baseline testosterone greater than 400 ng/dl = no increase in BMD
Snyder PJ, et al. J Clin Endocrinol Metab. 1999;84:2647-53
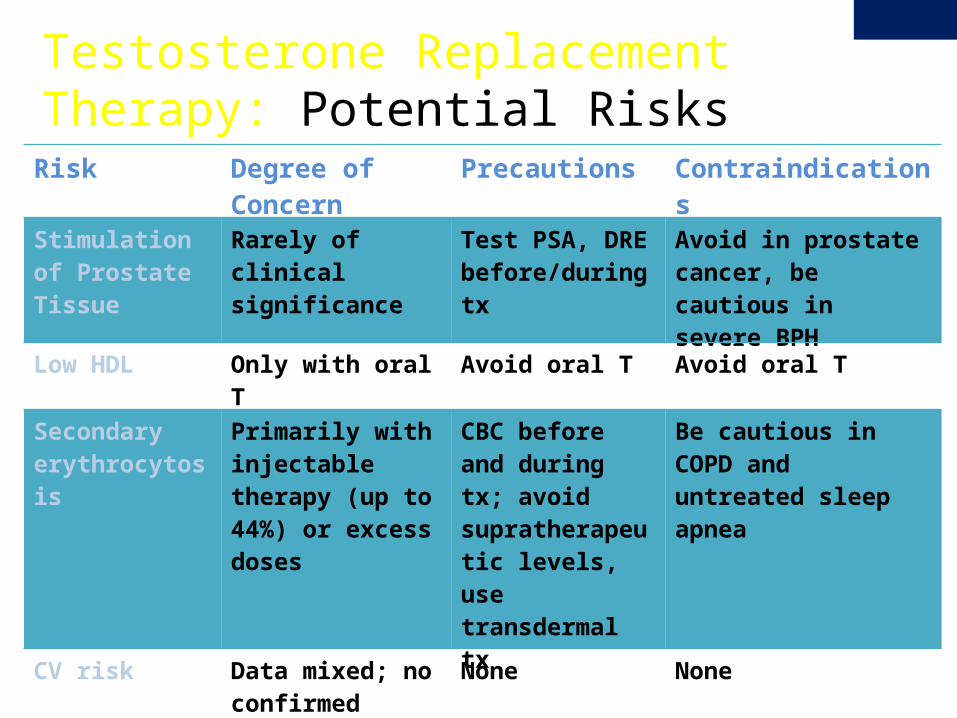
Testosterone Replacement Therapy: Potential Risks
Risk Degree of Concern Precautions Contraindications
Stimulation of Prostate Tissue
Rarely of clinical significance
Test PSA, DRE before/during tx
Avoid in prostate cancer, be cautious in severe BPH
Low HDL Only with oral T Avoid oral T Avoid oral T
Secondary erythrocytosis
Primarily with injectable therapy (up to 44%) or excess doses
CBC before and during tx; avoid supratherapeutic levels, use transdermal tx
Be cautious in COPD and untreated sleep apnea
CV risk Data mixed; no confirmed definitive harm
None None
Venous thrombosis
No clinical evidence None None
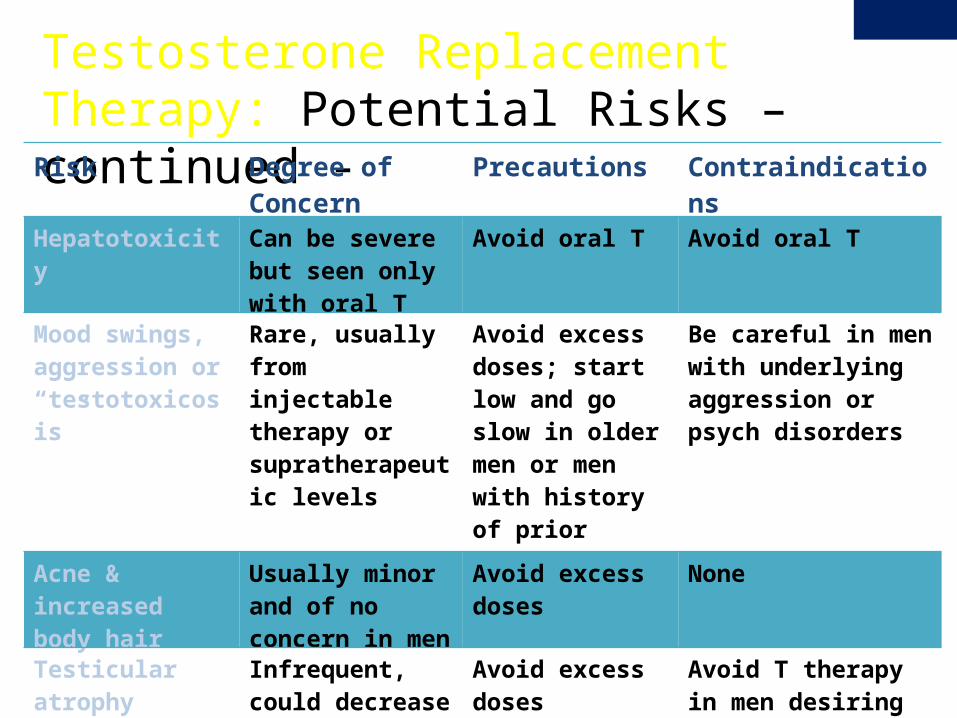
Testosterone Replacement Therapy: Potential Risks – continued -
Risk Degree of Concern
Precautions Contraindications
Hepatotoxicity Can be severe but seen only with oral T
Avoid oral T Avoid oral T
Mood swings, aggression or “testotoxicosis”
Rare, usually from injectable therapy or supratherapeutic levels
Avoid excess doses; start low and go slow in older men or men with history of prior issues
Be careful in men with underlying aggression or psych disorders
Acne & increased body hair
Usually minor and of no concern in men
Avoid excess doses None
Testicular atrophy Infrequent, could decrease fertility
Avoid excess doses Avoid T therapy in men desiring fertility
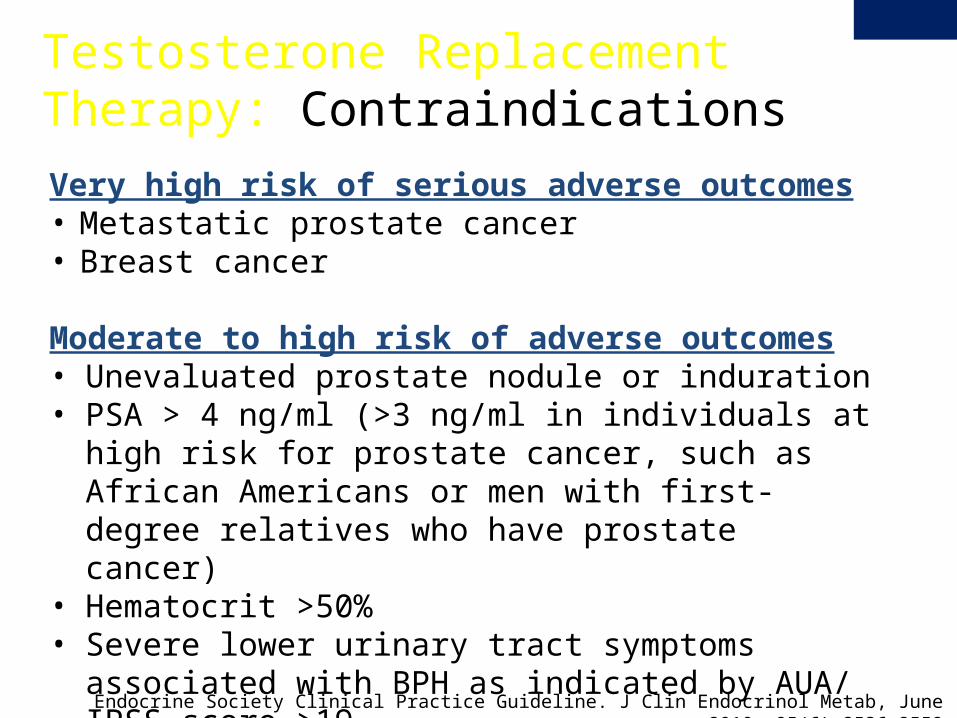
Very high risk of serious adverse outcomes• Metastatic prostate cancer• Breast cancer
Moderate to high risk of adverse outcomes• Unevaluated prostate nodule or induration• PSA > 4 ng/ml (>3 ng/ml in individuals at high risk for
prostate cancer, such as African Americans or men with first-degree relatives who have prostate cancer)
• Hematocrit >50%• Severe lower urinary tract symptoms associated with BPH as
indicated by AUA/ IPSS score >19• Uncontrolled or poorly controlled CHF
Testosterone Replacement Therapy: Contraindications
Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab, June 2010, 95(6):2536–2559
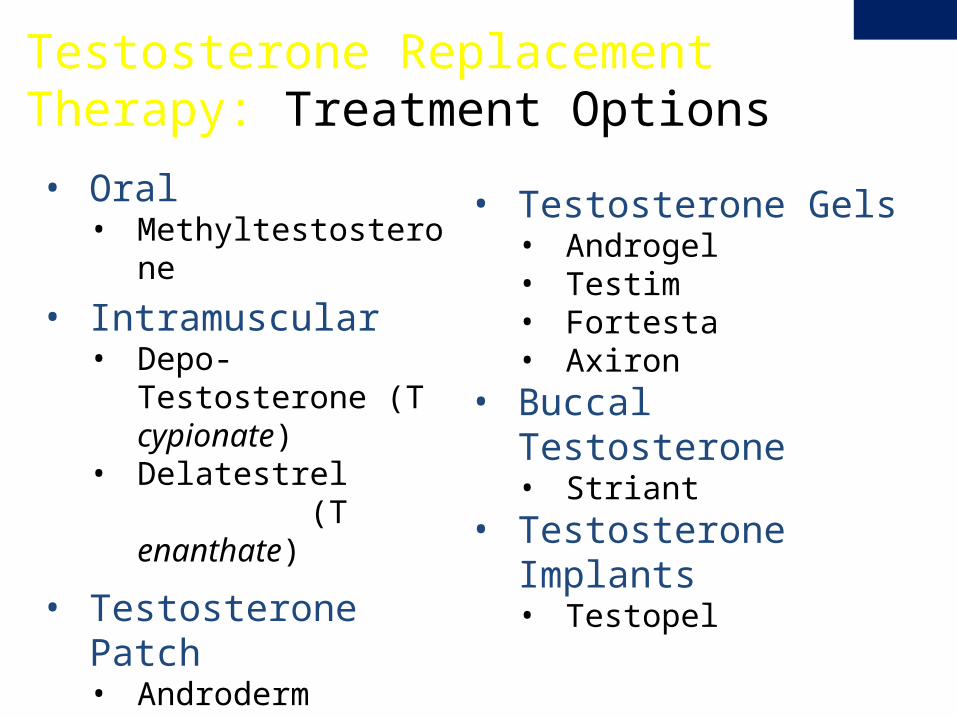
• Oral• Methyltestosterone
• Intramuscular• Depo-Testosterone (T
cypionate)• Delatestrel (T
enanthate)
• Testosterone Patch• Androderm
Testosterone Replacement Therapy: Treatment Options
• Testosterone Gels• Androgel • Testim• Fortesta• Axiron
• Buccal Testosterone• Striant
• Testosterone Implants• Testopel
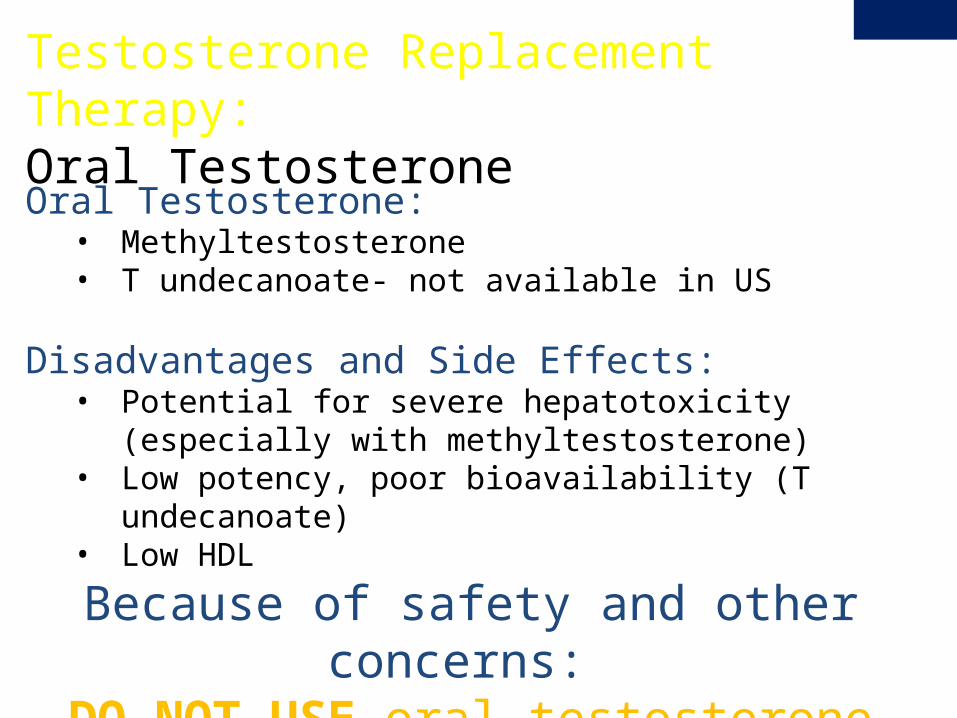
Testosterone Replacement Therapy: Oral Testosterone
Oral Testosterone: • Methyltestosterone• T undecanoate- not available in US
Disadvantages and Side Effects:• Potential for severe hepatotoxicity (especially with
methyltestosterone)• Low potency, poor bioavailability (T undecanoate) • Low HDL
Because of safety and other concerns: DO NOT USE oral testosterone
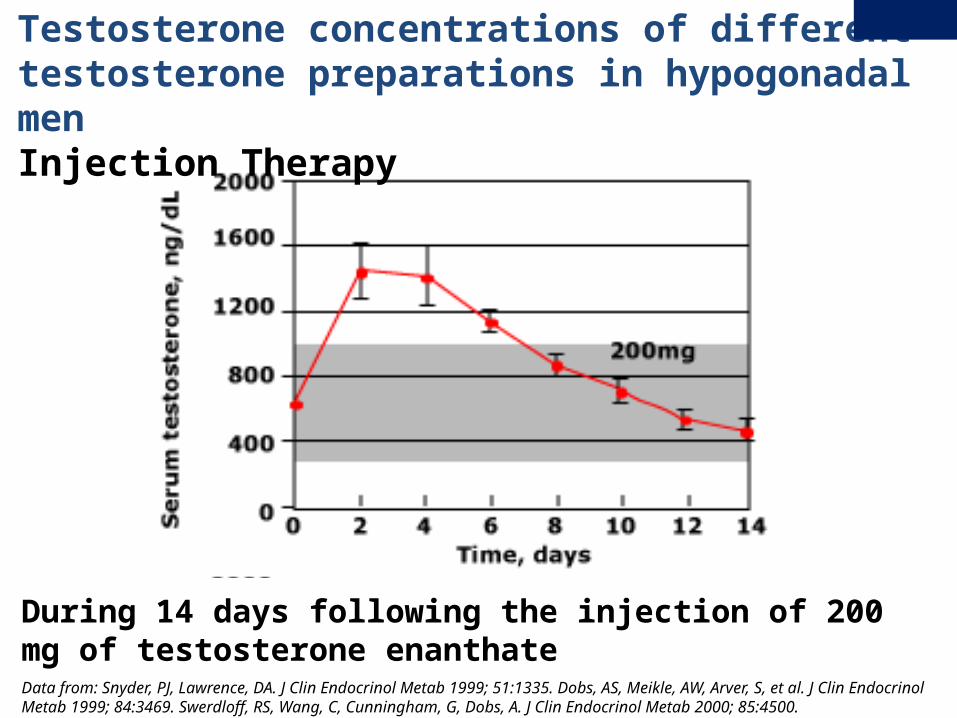
Testosterone concentrations of different testosterone preparations in hypogonadal menInjection Therapy
Data from: Snyder, PJ, Lawrence, DA. J Clin Endocrinol Metab 1999; 51:1335. Dobs, AS, Meikle, AW, Arver, S, et al. J Clin Endocrinol Metab 1999; 84:3469. Swerdloff, RS, Wang, C, Cunningham, G, Dobs, A. J Clin Endocrinol Metab 2000; 85:4500.
During 14 days following the injection of 200 mg of testosterone enanthate
Testosterone Replacement Therapy: Intramuscular InjectionsIntramuscular Injections: • Testosterone Esters (Enanthate and Cypionate)• Least expensive form of therapy• Natural testosterone esterified for slow release from IM sites
Disadvantages and Side Effects:• Non-physiologic with wide swings in serum levels• Increased risk of negative effects on mood and risk of
erythrocytosis• Local pain• Contra-indicated with bleeding tendency
Usual Dose: • 200-250 mg IM every 2-3 weeks• 100 mg IM week decreases variation in levels
Intramuscular:• Check trough testosterone on day of injection (before injection)
and peak testosterone 24-48 hrs after injection.• Goal is to avoid too low of a trough and too of a excessive peak • Smaller doses given more frequently decreases severity of peaks
and troughs (100 mg IM q week)• Alternative testing is to measure testosterone mid-way between
injections and aim for testosterone 400-700 ng/dl• Decrease or increase dose as needed.• If too much variation in levels, consider switching to transdermal
preparations
Testosterone Intramuscular Injections: Monitoring Testosterone Levels During Therapy
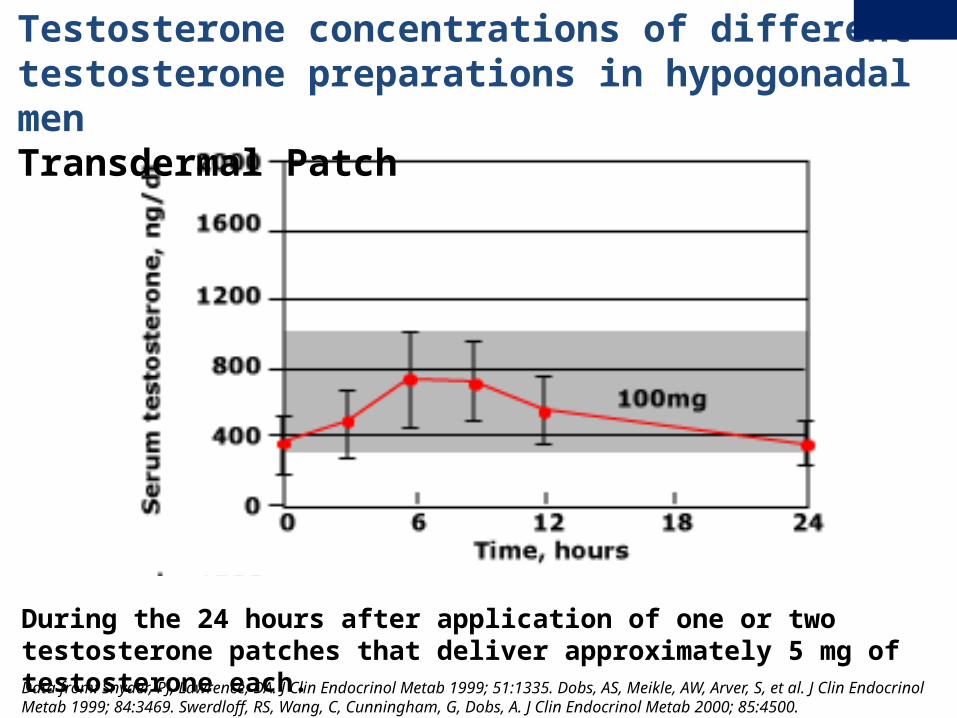
Testosterone concentrations of different testosterone preparations in hypogonadal menTransdermal Patch
Data from: Snyder, PJ, Lawrence, DA. J Clin Endocrinol Metab 1999; 51:1335. Dobs, AS, Meikle, AW, Arver, S, et al. J Clin Endocrinol Metab 1999; 84:3469. Swerdloff, RS, Wang, C, Cunningham, G, Dobs, A. J Clin Endocrinol Metab 2000; 85:4500.
During the 24 hours after application of one or two testosterone patches that deliver approximately 5 mg of testosterone each.
Testosterone Replacement Therapy: Transdermal PatchTransdermal Patch• Reservoir, alcohol based• Physiological serum testosterone profile
Disadvantages and Side effects• Delayed skin hypersensitivity in up to ~20-30% • Can be relieved/prevented with corticosteroid cream• Patch falls off
Usual Dose: • 2.5 – 5mg patch applied nightly
• Transdermal Patch:
• Measure early morning testosterone level
• Goal is mid-normal range 400-600 ng/dl
• If too low or skin irritation, consider changing to gel.
• If too high, may decrease to lower dose patch
Testosterone Transdermal Patch: Monitoring Testosterone Levels During Therapy
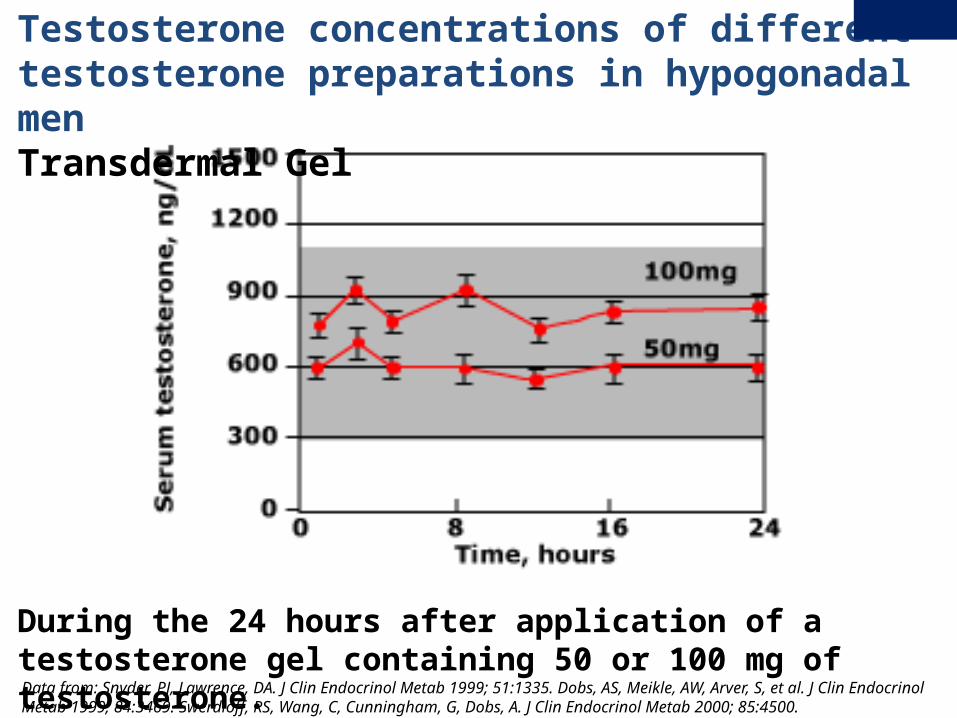
Testosterone concentrations of different testosterone preparations in hypogonadal menTransdermal Gel
Data from: Snyder, PJ, Lawrence, DA. J Clin Endocrinol Metab 1999; 51:1335. Dobs, AS, Meikle, AW, Arver, S, et al. J Clin Endocrinol Metab 1999; 84:3469. Swerdloff, RS, Wang, C, Cunningham, G, Dobs, A. J Clin Endocrinol Metab 2000; 85:4500.
During the 24 hours after application of a testosterone gel containing 50 or 100 mg of testosterone.
Testosterone Replacement Therapy: Transdermal Gel
Transdermal Gels
• Hydroalcoholic gels
• Rapidly dries and absorbed into skin
• Excellent acceptability
• Physiological serum testosterone profile
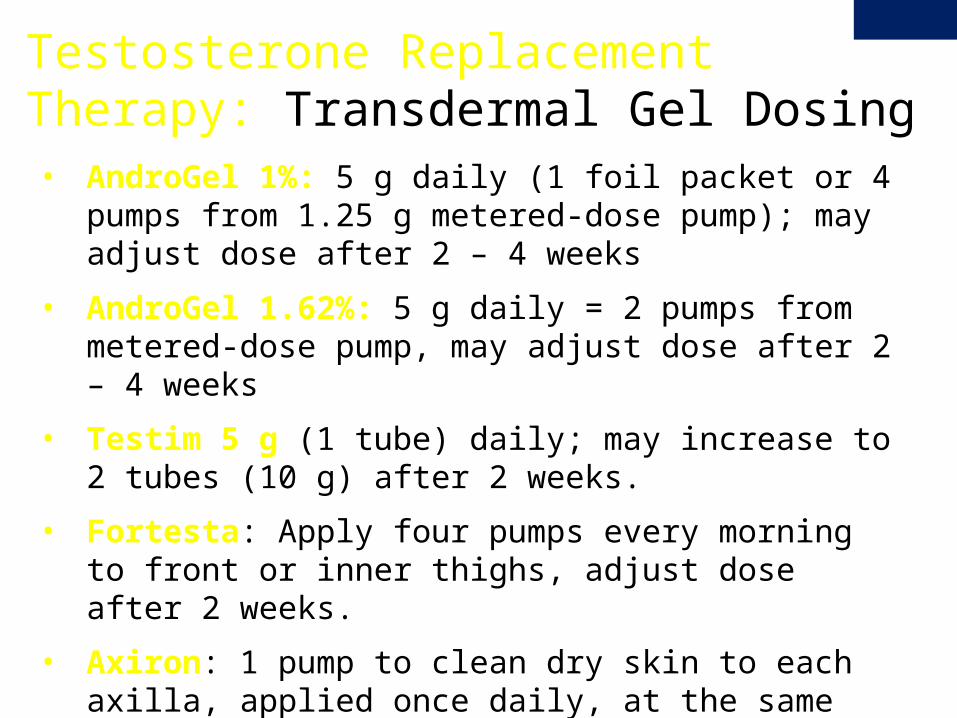
Testosterone Replacement Therapy: Transdermal Gel Dosing• AndroGel 1%: 5 g daily (1 foil packet or 4 pumps from 1.25 g
metered-dose pump); may adjust dose after 2 – 4 weeks
• AndroGel 1.62%: 5 g daily = 2 pumps from metered-dose pump, may adjust dose after 2 – 4 weeks
• Testim 5 g (1 tube) daily; may increase to 2 tubes (10 g) after 2 weeks.
• Fortesta: Apply four pumps every morning to front or inner thighs, adjust dose after 2 weeks.
• Axiron: 1 pump to clean dry skin to each axilla, applied once daily, at the same time each morning

Transdermal Gel: • Obtain testosterone about 6 to 8 hrs after placement. • Goal is level in mid-normal range 400-600 ng/dl• Increase or decrease dose of gel applied as needed.• If levels lower than expected, make certain men are
applying correctly
Testosterone Transdermal Gel: Monitoring Testosterone Levels During Therapy
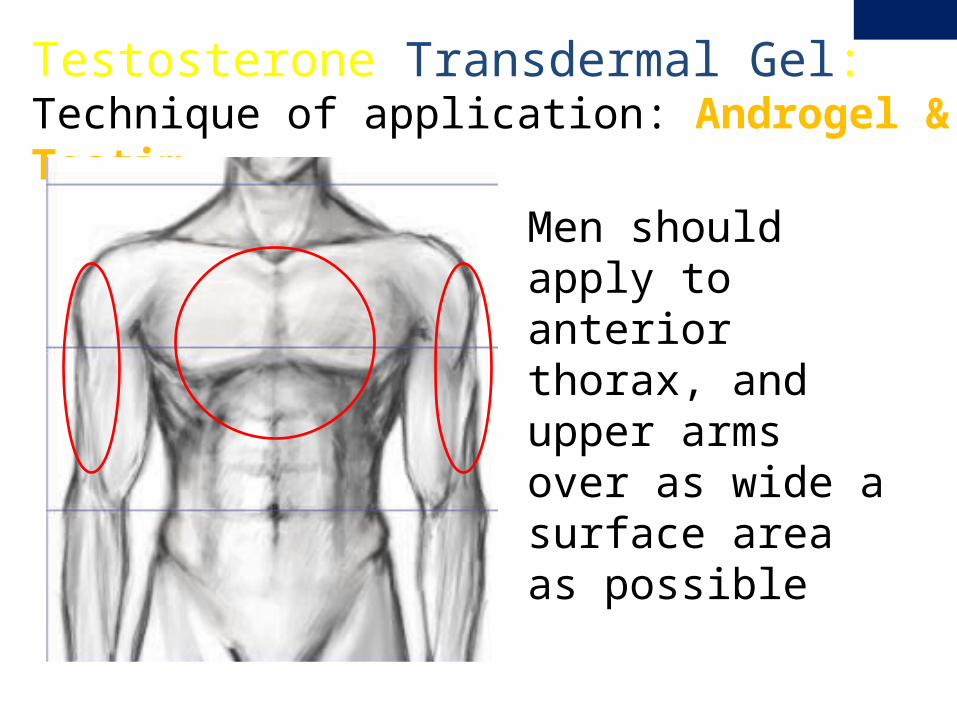
Men should apply to anterior thorax, and upper arms over as wide a surface area as possible
Testosterone Transdermal Gel: Technique of application: Androgel & Testim
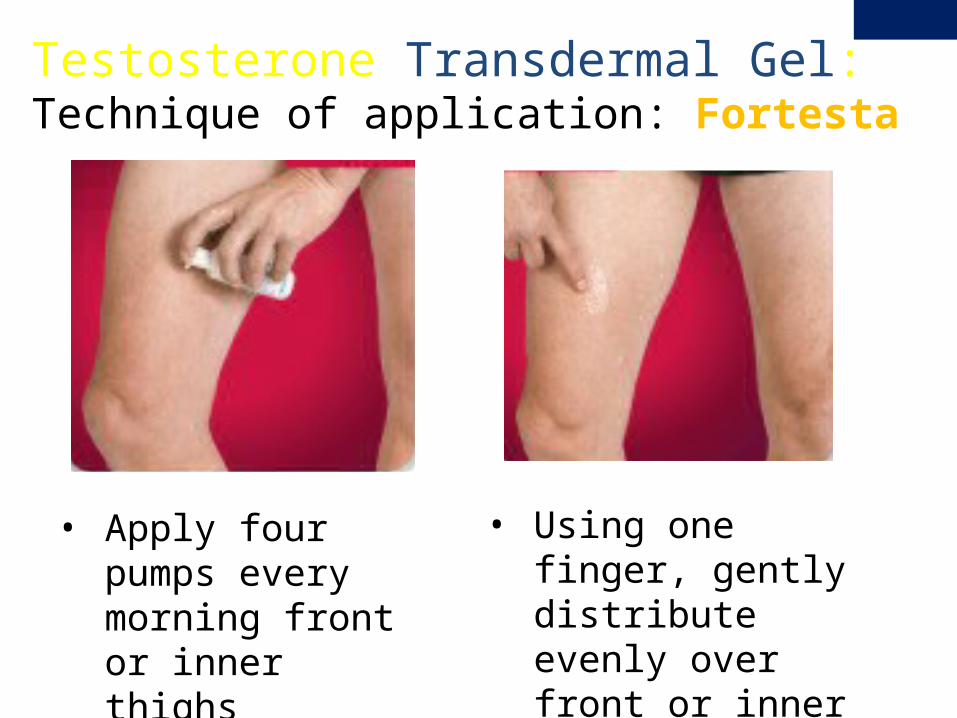
• Using one finger, gently distribute evenly over front or inner thighs
Testosterone Transdermal Gel: Technique of application: Fortesta
• Apply four pumps every morning front or inner thighs
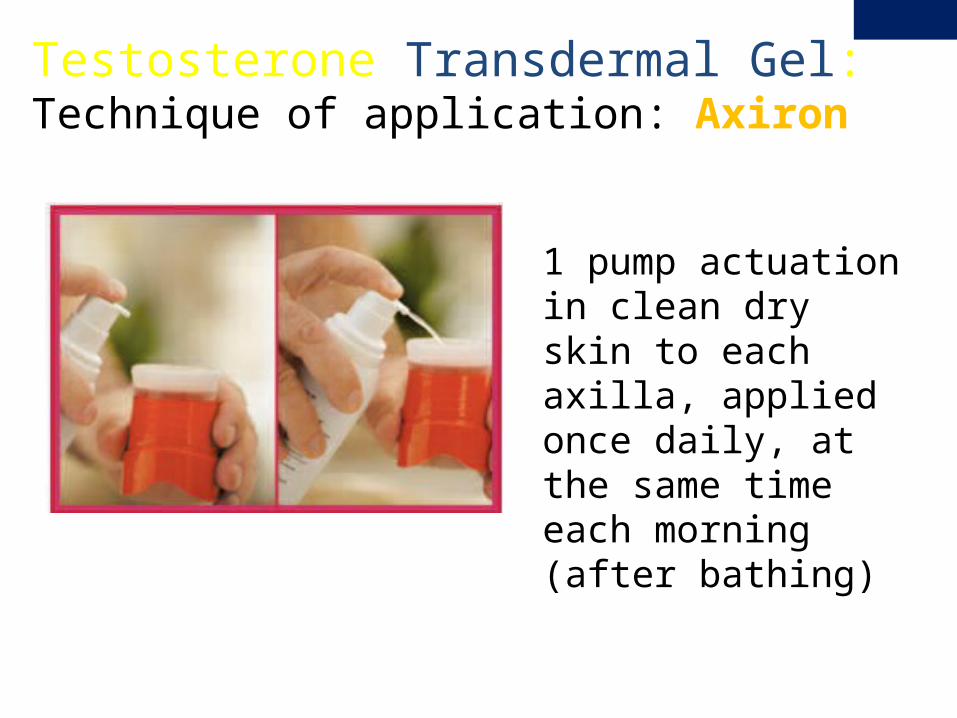
1 pump actuation in clean dry skin to each axilla, applied once daily, at the same timeeach morning (after bathing)
Testosterone Transdermal Gel: Technique of application: Axiron
Testosterone Replacement Therapy: Transdermal Gel – continued-
Disadvantages and Side effects• Technique of application important for
consistent absorption- teach patients how to apply correctly
• Sticky feeling on skin
• Odor
• Skin irritation- rare
• Risk of inter-personal transfer
In a study of healthy male volunteers who received testosterone gel
• Subjects were pretreated with norethisterone 400 mg IM to suppress endogenous testosterone
• Intense skin contact with a second pre-treated male volunteer did not result in an increase in serum testosterone concentrations
Testosterone Transdermal Gel: Risk of inter-personal transfer
Rolf, C, et al. Interpersonal testosterone transfer after topical application of a newly developed testosterone gel preparation. Clin Endocrinol (Oxf) 2002; 56:637.
• However, after receiving reports of secondary exposure in 8 children ages 9 months to 5 years, the FDA added a boxed warning to testosterone gels1,2
• Reports included penile or clitoral enlargement, premature development of pubic hair, advanced bone age, increased libido, and aggressive behavior3
• Most symptoms regressed after testosterone eliminated (with exception of penile/clitoral enlargement).3
Testosterone Transdermal Gel: Risk of inter-personal transfer
1. Repas T. “New Boxed Warning for Testosterone Gels” Endocrine Today. May 27, 2009. http://www.endocrinetoday.com/comments.aspx?rid=40285#com
2. http://www.fda.gov/bbs/topics/NEWS/2009/NEW02011.html (Accessed on 5/26/09).3. Bhowmick, SK, et al. Sexual precocity in a 16-month-old boy induced by indirect topical exposure to
testosterone. Clin Pediatr (Phila) 2007; 46:540.
Testosterone Transdermal Gel: Risk of inter-personal transfer• Risk of this complication is extremely rare (8 cases/1.8
million prescriptions)
• However, patients must be advised to take appropriate precautions to prevent exposing others.
Always remind patient to:
• Wash hands thoroughly after application. • Avoid skin contact until the gel has dried completely. • Keep the application site covered.
1. Repas T. “New Boxed Warning for Testosterone Gels” Endocrine Today. May 27, 2009. http://www.endocrinetoday.com/comments.aspx?rid=40285#com
2. http://www.fda.gov/bbs/topics/NEWS/2009/NEW02011.html (Accessed on 5/26/09).
Testosterone Replacement Therapy: Buccal Bio-adhesive Testosterone
Buccal Testosterone• Testosterone is released across the
buccal mucosa into the systemic circulation
Disadvantages and Side effects• Altered sense of taste• Gum irritation in 16%Usual Dose: • 30 mg BID to a depression in the gum
above the upper incisors
Testosterone Replacement Therapy: Testosterone Implants
Testosterone Implants• Pure crystalline testosterone cylinders• Excellent profile of release over 4-6 monthsDisadvantages and Side effects• Need for surgery• Pellet extrusion ~ 10%• Risk of infectionUsual Dose: • 600-800 mg implanted every 4-6 months (three
cylinders of 200 mg)
Testosterone Replacement Therapy: Other Considerations“Bioidentical” testosterone replacement therapy• Trendy and popular, some proponents claim more
“natural” and safer than traditional options
• Never shown to be safer/more effective in any RCT
• Long term safety and efficacy unknown
• Not approved or monitored by the FDA
• The Endocrine Society and American Association of Clinical Endocrinology have position statements advising against the use of “bioidentical” HRT
AACE Hypogonadism Guidelines, Endocr Pract. 2002;8(No. 6)
Baseline • Testosterone (total, calculated free/bioavailable)• Hgb, Hct • In those who are older than age 40: DRE and PSA
Repeat labs at 3 months, 6 months then annually• Maintain testosterone in mid-normal range expected in
young men (400-600 ng/dl)• In elderly men may consider keeping testosterone in
lower to mid normal range (300-400 ng/dl)
Testosterone Replacement Therapy: Monitoring for Adverse Effects
1. Nieschlag E, Swerdloff R, Behre HM et al. The Aging Male 2005;8(2):56-8.2. Bhasin S, Cunningham GR, Hayes FJ et al. J Clin Endocrinol Metab 2006;1995-2010.
LFTs: not necessary with non-oral TRT formulations.
Lipid profile: not necessary when using non-oral TRT preparations. However, many hypogonadal men have type 2 diabetes, metabolic syndrome and/or dyslipidemia, for which lipid profile may be indicated.
BMD: In hypogonadal men especially > age 50, consider baseline BMD.
In those with prior low-trauma fracture or with confirmed osteoporosis2 may obtain BMD every 2 years1
Testosterone Replacement Therapy: Monitoring for Adverse Effects
1. Nieschlag E, Swerdloff R, Behre HM et al. The Aging Male 2005;8(2):56-8.2. Bhasin S, Cunningham GR, Hayes FJ et al. J Clin Endocrinol Metab 2006;1995-2010.
Male Hypogonadism and Testosterone
Replacement Therapy Conclusion
Male Hypogonadism and Testosterone Replacement Therapy: Summary
• Always obtain testosterone levels in AM
• Obtain bioavailable or calculated free testosterone to rule out unreliable total testosterone due to abnormality in SHBG
• Provide testosterone therapy only in those with confirmed androgen deficiency and only after ruling out other causes of symptoms and/or low testosterone
• Be cautious to avoid supratherapeutic levels
• Monitor treatment response and for potential adverse effects
Male Hypogonadism and Testosterone Replacement Therapy: Clinical Practice Guidelines
Endocrine Society:• http://www.endo-
society.org/guidelines/
American Association of Clinical Endocrinologists:• http://www.aace.com/pub/
guidelines/
Thomas Repas DO FACP FACOI FNLA FACE CDE
Thank You!
Regional Medical Clinic- EndocrinologyAspen Centre640 Flormann Street- 3rd FloorRapid City, South Dakota 57701Office: 605 718 3300Blog: http://www.endocrinetoday.com/blogs.aspx