This month - hkma.org · Apart from Typhoon Molave, ... Like the SARS attack, ... economy will...
24
August 2009 n Spotlight Classification of venous disease n Cardiology A 22-year-old man was seen for on-and-off low grade fever n Dermatology A 19-year-old female with good past health complained of a rash over the bilateral lower limbs n Neurology A 6-year-old girl who recently began stuttering n General Medicine A 35-year-old female with complaints of jaw pain and swelling This month
Transcript of This month - hkma.org · Apart from Typhoon Molave, ... Like the SARS attack, ... economy will...

August 2009
n SpotlightClassification of venous disease
n CardiologyA 22-year-old man was seen for on-and-off low grade fever
n DermatologyA 19-year-old female with good past health complained of a rash over the bilateral lower limbs
n NeurologyA 6-year-old girl who recently began stuttering
n General MedicineA 35-year-old female with complaints of jaw pain and swelling
This month

1www.hkmacme.org HKMA August 2009
3
HKMA CME Bulletin 持續醫學進修專訊 August 2009
CME Calendar 23
Spotlight: Classification of venous disease 4
Cardiology: A 22-year-old man was seen for on-and-off low grade fever 10
Dermatology: A 19-year-old female with good past health complained of 11 a rash over the bilateral lower limbs
Neurology: A 6-year-old girl who recently began stuttering 12
General Medicine: A 35-year-old female with complaints of jaw pain and swelling 14
Answer Sheet 16
EDITORIAL
EVENT INFORMATION
CME COURSES
CME NOTIFICATIONS
Elsevier (Singapore) Pte. LtdTel: 2965 1300
The Hong Kong Medical Association is dedicated to providing a coordinated CME programme for all members of the medical profession. Under the HKMA CME Programme, a CME registration process has been created to document the CME efforts of doctors and to provide special CME avenues. The Association strives to foster a vibrant environment of CME throughout the medical profession. Both members as well as non-members of the Association are welcome to join us. You may contact the HKMA Secretariat for details of the programme.
香港醫學會致力推動持續醫學進修,醫學會體察到業界有必要設立完善的持續進修計劃,為同僚建立有系統的進修記錄機制,以及為全科醫生
提供適切的進修課程。藉著這個計劃,我們期望將優良的進修傳統推展至醫學界中每一角落,同時為業界締造一個充滿活力的進修文化。我們
誠意邀請你參與醫學會持續進修計劃,不論你是否醫學會的會員,均歡迎你同來與我們一同學習,以及享用醫學會為所有醫生設立的進修記錄
機制。如欲了解香港醫學會持續醫學進修計劃的詳情,請聯絡本會秘書處查詢。
HKMA CME Bulletin – MONTHLY SELF-STUDY SERIES to help you grow!Please read the following articles and answer the questions. Participants in the HKMA CME Programme will be awarded credit points under the Programme for returning the completed answer sheet via fax (28650943) or by mail to the HKMA Secretariat on or before 15 September 2009. Answers to questions will be provided in the next issue of the HKMA CME Bulletin. (Questions may also be an-swered online at www.hkmacme.org)
請細閱本期文章,並利用答題紙完成自我評估測驗,於 2009 年 9 月 15 日前,將已填妥之答題紙傳真(號碼:2865 0943)或寄回本會秘書處,
您將可獲持續醫學進修的積分點 ;至於是期自我評估測驗之答案,將刊於下一期《持續醫學進修專訊》之中。(您亦可透過網站 www.hkmacme.org完成自我評估測驗。)
HKMA CME Enquiry Hotline:Tel: 2527 8452 2861 1979
Hong Kong Medical Association
19

3www.hkmacme.org HKMA August 2009
CME Bulletin & Online Editorial Board 持續醫學進修專訊及網上版編輯委員會
Chief Editor 總編輯:
Dr. WONG Bun Lap, Bernard 黃品立醫生
Board Members 委員會成員:
Dr. CHAN Hau Ngai, Kingsley 陳厚毅醫生
Dr. CHAN Man Kam 陳文岩醫生
Dr. CHAN Yee Shing, Alvin 陳以誠醫生
Dr. CHENG Chi Man 鄭志文醫生
Dr. CHEUNG Hon Ming 張漢明醫生
Dr. CHU Kin Wah 朱建華醫生
Dr. CHIU Shing Ping, James 趙承平醫生
Dr. CHOI Kin, Gabriel 蔡 堅醫生
Dr. CHOW Pak Chin 周伯展醫生
Dr. FONG Chung Yan, Gardian 方頌恩醫生
Dr. FUNG Yee Leung, Wilson 馮宜亮醫生
Dr. HO Chung Ping, MH 何仲平醫生
Dr. HO Hung Kwong, Duncan 何鴻光醫生
Dr. KONG Kam Fu, James 江金富醫生
Dr. KWOK Ka Ki 郭家麒醫生
Dr. LAM Tzit Yuen, David 林哲玄醫生
Dr. LEUNG Chi Chiu 梁子超醫生
Dr. LI Siu Lung, Steven 李少隆醫生
Dr. LI Sum Wo, MH 李深和醫生
Dr. POON Tak Lun 潘德鄰醫生
Dr. SHIH Tai Cho, Louis 史泰祖醫生
Dr. TSE Hung Hing 謝鴻興醫生
Dr. WONG Shou Pang, Alexander 王壽鵬醫生
Dr. YEUNG Chiu Fat, Henry 楊超發醫生
EDITORIAL
Published by Elsevier (Singapore) Pte Ltd.1102, 11/F Sing Pao Building New Wing, 101 King’s Road, North Point, Hong KongTel: 2965 1300 Fax: 3764 0374
Publishing Editor Richard Henderson
CME Programme Consultant Karen Berry
Senior Production/Design Controller Tommy Wong
Page Layout Ann Fong
Advertising Enquiry Doreen Chang
© Elsevier (Singapore) Pte Ltd. 2009
ISSN: 1793-5393
NoTiCEMedical knowledge is constantly changing. Standard safety precautions must be followed, but as new research and clinical experience broaden our knowledge, changes in treatment and drug therapy may become necessary or appropriate. Readers are advised to check the most current product information provided by the manufacturer of each drug to be administered to verify the recommended dose, the method and duration of administration, and contraindications. It is the responsibility of the practitioner, relying on experience and knowledge of the patient, to determine dosages and best treatment for each individual patient. Neither the Publisher nor the Authors assume any liability for any injury and/or damage to persons or property arising from this publication.
Although all advertising material is expected to conform to ethical (medical) standards, inclusion in this publication does not constitute a guarantee or endorsement of the quality or value of such product or of the claims made of it by its manufacturer.
EDITORIAL
Typhoon Molave just left Hong Kong. All typhoon signals were removed one hour ago. After my Sunday lunch, in my study room, enjoying the cool natural wind, with today’s newspaper, and a cup of green tea at hand, I suddenly realized how modern and safe we are in Hong Kong. Last night, despite the typhoon signal No. 9 — a near direct hit —there were no serious injuries or mortalities.
Apart from Typhoon Molave, we are also very lucky that the H1N1 swine influenza is not all that “toxic”. Despite the fact that the infectivity and rate of spread is high and fast, the serious morbidity and mortality is very low indeed.
This wave of the “Financial Tsunami” also seems to be milder than expected. Our stock market slowly but happily regained some of her momentum in the past 8 months. She is recovering slowly from the horrifying attack of the first wave — HSI 10,676.300 (November 2008) to 18,805.660 at closing on the 17th July 2009.
The property market is also doing well. Recently, Le Prestige in Tseung Kwan O sold an amazing 500 units on the first day of public offer.
Like the SARS attack, I sincerely hope that the swine influenza will fade away after the summer holidays. I also wish that the global and local economy will continue to recover and grow. If my hopes and wishes come true, together with this CME Bulletin, my dearest colleagues, we can concentrate all our efforts in preparing ourselves to provide a better service to the Hong Kong community, so that all of us, doctors and fellow Hong Kong citizens will have safer, better and brighter lives!
“Many of life’s failures are people who did not realize how close they were to success when they gave up.”
Thomas A. Edison, US Inventor (1847–1931)
Dr. WoNG Bun Lap BernardEditor-in-Chief

SPOTLIGHT
4 www.hkmacme.orgHKMA August 2009
Venous disease has very diverse clinical presentations, ranging from simple spider veins, unsightly varicose veins to debilitating venous ulcers. All of these are now grouped under the term chronic venous disorder (CVD). In order to systemically categorize the disorder with uniform terminology around the world, the CEAP classification has been introduced and accepted globally. The four categories selected for classification were: clinical state (C), (a)etiology (E), anatomy (A), and pathophysiology (P). The key element is the clinical state, which is the first and the most important assessment, and is usually done by the attending physicians clinically. Clinical state also determines the need for further investigation on aetiology, anatomy and pathophysiology. With diverse choices in treatment such as minimally invasive options and conventional surgery, the CEAP classification helps to provide guidance in choosing the appropriate treatment for such patients. The aim of this article is to describe the CEAP classification with relevance to physicians in general practice.
Introduction
Varicose veins of the lower extremities are a common presentation in general practice. However, this is only one of the many manifestations of a pathology called chronic venous disorder (CVD), which includes a spectrum of clinical presentations ranging from uncomplicated telangiectasias and varicose veins to disabling venous ulceration. Clinical manifestations of CVDs may result from primary venous insufficiency with no identifiable mechanism of venous dysfunction, or be secondary to other processes, primarily deep vein thrombosis. The diversity of presentations and the aetiology of venous disorder call for a uniform language for classifying the findings of CVD.
The CEAP Classification for CVD was introduced in 1994 by the American Venous Forum [1] and revised in 2004 [2]. It is now widely adopted around the world and is considered as the reporting standard for venous disease today. The aim of this article is to describe the CEAP Classification with relevance to community practice, so that physicians can be aware of these disorders more readily.
Epidemiology
Varicose veins or re lated condit ions are common presentations in general practice. In the US it is estimated that 10–35% of the adult population has some form of CVD [3]. In industrialized nations, up to 1.5% of people will suffer from venous ulceration and in patients 65 years and older, the incidence increases to 4% [4,5]. The problem is more common in women as a result of pregnancy and child bearing. Although venous disease is rarely a life or limb threatening problem, the disease greatly impacts quality of life. Many of the people affected are in the most productive years of their careers. They seek medical advice for cosmetic and health reasons.
Risk factors
The aetiology of CVD is multifactorial and is associated with: increased intravenous pressure caused by prolonged standing; increased intra-abdominal pressure arising from a tumour, pregnancy, obesity, or chronic constipation; familial and congenital factors; secondary vascularization caused by deep venous thrombosis; or less commonly, arteriovenous shunting [6].
Venous disease resulting in valve reflux appears to be the underlying pathophysiology for the formation of varicose veins. Rather than blood flowing from distal to proximal and superficial to deep, failed or incompetent valves in the venous system allow blood to flow in the reverse direction. With increased pressure on the local venous system, the larger affected veins may become elongated and tortuous. Although no specific aetiology is noted, in most cases the valvular dysfunction is presumed to be caused by a loss of elasticity in the vein wall, with failure of the valve leaflets to fit together [7].
Risk factors for development of varicose veins include age older than 50 years, female sex hormones, heredity, gravitational hydrostatic force, and hydrodynamic force due to muscular contraction [8]. Venous unction is undoubtedly influenced by hormonal changes. In particular, progesterone
Classification of venous disease Complete this courseand earn
1 CME POINT1 CME POINT
Dr. TSE Cheuk Wa, ChadSpecialist in General Surgery

SPOTLIGHT
5www.hkmacme.org HKMA August 2009
liberated by the corpus luteum stabilizes the uterus by causing relaxation of smooth muscle fibres [9]. This effect directly influences venous function. The result is passive venous dilation, which, in many instances, causes valvular dysfunction. Although progesterone is implicated in the first appearance of varicosities in pregnancy, oestrogen also has profound effects. It produces the relaxation of smooth muscle and a softening of collagen fibres. Further, the oestrogen-to-progesterone ratio influences venous distensibility. This ratio may explain the predominance of venous insufficiency symptoms on the first day of a menstrual period when a profound shift occurs from the progesterone phase of the menstrual cycle to the oestrogen phase [10]. Although heredity is widely acknowledged as a risk factor for varicose vein development, the precise genetic mechanism has yet to be elucidated [11].
Terminology and definitions
The CEAP classification covers all forms of venous diseases. The term chronic venous disorder (CVD) includes the full spectrum of morphological and functional abnormalities of the venous system from telangiectasias to venous ulcers. Some of these, like telangiectasias, are highly prevalent in the normal adult population, and in many cases the use of the term “disease” is not appropriate. The term chronic venous insufficiency (CVI) implies a functional abnormality
of the venous system and usually is reserved for patients with more advanced disease, including those with oedema, skin changes or venous ulcers.
The following are the recommended definitions based on the CEAP classification.
The CEAP Classification
An international ad hoc committee of the American Venous Forum developed the CEAP classification for CVD in 1994. The goal was to stratify clinical levels of venous insufficiency. The four categories selected for classification were: clinical state (C), (a)etiology (E), anatomy (A), and pathophysiology (P). The CEAP classification has been endorsed worldwide despite its acknowledged deficiencies.
One decade fo l lowing the or ig ina l consensus conference, a revised version of the CEAP classification was published, which includes a less complex reporting option (basic CEAP) and increased flexibility. Publication of these documents in multiple international journals and widespread acceptance of the classification have resulted in international uniformity of the current literature focused on venous problems.
The first step in evaluating a patient with CVD is to establish the patient’s clinical class. The patient’s clinical class will dictate the need for further evaluation. This is also the part most relevant to physicians in general practice.
CEAP Definitions
Telangiectasia: a confluence of dilated intradermal venules of less than 1 mm in calibre. Synonyms include spider veins, hyphen webs, and thread veins.
Reticular veins: dilated bluish intradermal veins, usually from 1 mm in diameter to less than 3 mm in diameter. They are usually tortuous. This excludes normal visible veins in people with transparent skin. Synonyms include blue veins, intradermal varices, and venulectasias.
Varicose veins: subcutaneous dilated veins equal to or more than 3 mm in diameter in the upright position. Varicose veins are usually tortuous, but refluxing tubular veins may be classified as varicose veins. These may involve saphenous veins, saphenous tributaries, or nonsaphenous veins. Synonyms include varix, varices, and varicosities.
Corona phlebectatica: fan-shaped pattern of numerous small intradermal veins on the medial or lateral aspects of the ankle and foot. Its significance is unclear, but commonly thought to be an early sign of advanced venous disease. Synonyms include malleolar flare and ankle flare.
Oedema: perceptible increase in volume of fluid in the skin and subcutaneous tissue characterized by indentation with pressure. Venous oedema usually occurs in the ankle region, but it may extend to the leg and foot. It can be difficult to differentiate from lymphedema which usually involves the toes.
Pigmentation: brownish darkening of the skin initiated by extravasated blood which usually occurs in the ankle region but may extend to the leg and foot.
Eczema: erythematous dermatitis, which may progress to a blistering, weeping, or scaling eruption of the skin of the leg. It is often located near varicose veins but may be located anywhere in the leg. Eczema is usually caused by CVD or by sensitization to local therapy. Synonyms include stasis dermatitis.
Lipodermatosclerosis: localized chronic inflammation and fibrosis of the skin and subcutaneous tissues, sometimes associated with scarring or contracture of the Achilles tendon. It is sometimes preceded by diffuse inflammatory oedema of the skin which may be painful and which is often referred to as hypodermitis. The absence of lymphangitis, lymphadenitis and fever differentiates this condition from erysipelas or cellulitis. Lipodermatosclerosis is a sign of severe CVD.
Atrophie blanche or white atrophy: circumscribed, often circular, whitish, and atrophic skin areas surrounded by dilated capillary spots and, sometimes, hyperpigmentation. This is a sign of severe CVD. Scars of healed ulceration are excluded in this definition.
Venous ulcer: chronic defect of the skin most frequently around the ankle that fails to heal spontaneously because of CVD.
SPOTLIGHT
6 www.hkmacme.orgHKMA August 2009
The Clinical Classification (C1,2,3,4,5,6&0(A,S))
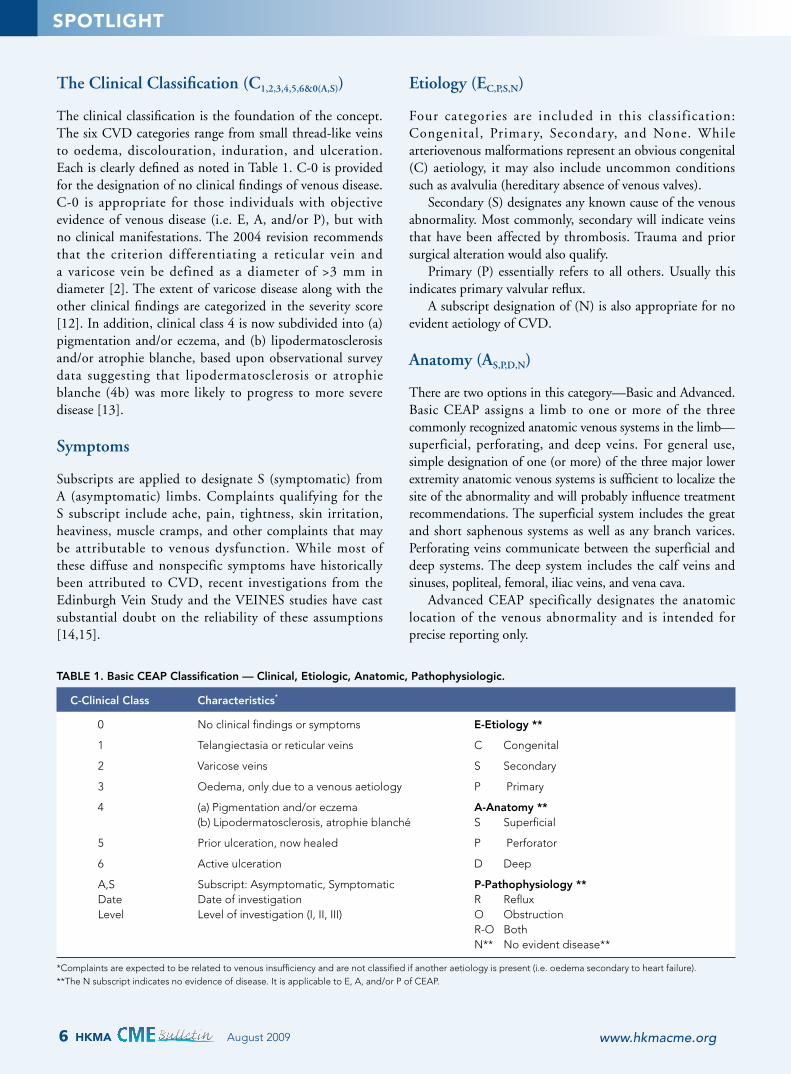
The clinical classification is the foundation of the concept. The six CVD categories range from small thread-like veins to oedema, discolouration, induration, and ulceration. Each is clearly defined as noted in Table 1. C-0 is provided for the designation of no clinical findings of venous disease. C-0 is appropriate for those individuals with objective evidence of venous disease (i.e. E, A, and/or P), but with no clinical manifestations. The 2004 revision recommends that the criterion differentiating a reticular vein and a varicose vein be defined as a diameter of >3 mm in diameter [2]. The extent of varicose disease along with the other clinical findings are categorized in the severity score [12]. In addition, clinical class 4 is now subdivided into (a) pigmentation and/or eczema, and (b) lipodermatosclerosis and/or atrophie blanche, based upon observational survey data suggesting that lipodermatosclerosis or atrophie blanche (4b) was more likely to progress to more severe disease [13].
Symptoms
Subscripts are applied to designate S (symptomatic) from A (asymptomatic) limbs. Complaints qualifying for the S subscript include ache, pain, tightness, skin irritation, heaviness, muscle cramps, and other complaints that may be attributable to venous dysfunction. While most of these diffuse and nonspecific symptoms have historically been attributed to CVD, recent investigations from the Edinburgh Vein Study and the VEINES studies have cast substantial doubt on the reliability of these assumptions [14,15].
Etiology (EC,P,S,N)
Four categories are included in this classification: Congenital, Primary, Secondary, and None. While arteriovenous malformations represent an obvious congenital (C) aetiology, it may also include uncommon conditions such as avalvulia (hereditary absence of venous valves).
Secondary (S) designates any known cause of the venous abnormality. Most commonly, secondary will indicate veins that have been affected by thrombosis. Trauma and prior surgical alteration would also qualify.
Primary (P) essentially refers to all others. Usually this indicates primary valvular reflux.
A subscript designation of (N) is also appropriate for no evident aetiology of CVD.
Anatomy (AS,P,D,N)
There are two options in this category—Basic and Advanced. Basic CEAP assigns a limb to one or more of the three commonly recognized anatomic venous systems in the limb—superficial, perforating, and deep veins. For general use, simple designation of one (or more) of the three major lower extremity anatomic venous systems is sufficient to localize the site of the abnormality and will probably influence treatment recommendations. The superficial system includes the great and short saphenous systems as well as any branch varices. Perforating veins communicate between the superficial and deep systems. The deep system includes the calf veins and sinuses, popliteal, femoral, iliac veins, and vena cava.
Advanced CEAP specifically designates the anatomic location of the venous abnormality and is intended for precise reporting only.
TABLE 1. Basic CEAP Classification — Clinical, Etiologic, Anatomic, Pathophysiologic.
C-Clinical Class Characteristics*
0 No clinical findings or symptoms E-Etiology **
1 Telangiectasia or reticular veins C Congenital
2 Varicose veins S Secondary
3 Oedema, only due to a venous aetiology P Primary
4 (a) Pigmentation and/or eczema A-Anatomy ** (b) Lipodermatosclerosis, atrophie blanché S Superficial
5 Prior ulceration, now healed P Perforator
6 Active ulceration D Deep
A,S Subscript: Asymptomatic, Symptomatic P-Pathophysiology ** Date Date of investigation R Reflux Level Level of investigation (I, II, III) O Obstruction R-O Both N** No evident disease**
*Complaints are expected to be related to venous insufficiency and are not classified if another aetiology is present (i.e. oedema secondary to heart failure). **The N subscript indicates no evidence of disease. It is applicable to E, A, and/or P of CEAP.

SPOTLIGHT
7www.hkmacme.org HKMA August 2009
Class 1: telangiectasia. Class 3: oedema.
Class 2: varicose vein only. Class 4: pigmentation, eczema, lipodermatosclerosis.

SPOTLIGHT
8 www.hkmacme.orgHKMA August 2009
Class 5: prior ulceration, now healed. Class 6: venous ulcer.
Pathophysiology (PR,O,R-O,N)
The two major categories—Reflux (R) and Obstruction (O)—are not mutually exclusive; they may occur alone or in combination (R-O). Reflux is defined as reverse flow with a duration of >0.5 sec by duplex analysis. Ideally, obstruction is defined objectively by imaging or noninvasive testing. A subscript designation (N) indicating no abnormality is again appropriate.
Summary
This classification is targeted at all forms of venous insufficiency. Physicians in general practice should be aware that CVD consists of a spectrum of clinical manifestations, ranging from simple telangiectasias, to the commonly seen varicose veins and the debilitating venous ulcers. The transition from one clinical stage to the other is progressive, but the rate of deterioration and symptoms depends on the underlying aetiology, anatomy and pathophysiology. In the presence of minimally invasive options in addition to conventional surgery in treating CVD, treatment can now be tailored to individual patients based on their clinical status and symptoms. The utility of a uniform classification and severity grading system permits more accurate and meaningful dialogue between the generalist practitioner, the specialist, and the patient.
References1. Bergan JJ. Classification and grading of chronic venous disease in the lower
limbs. A conensus statement. Vasc Surg 1996;30:5–11.2. Eklof B. Revision of the CEAP classification for chronic venous disorder:
Consensus statement. J Vasc Surg 2004;40:1248–52.3. Criqui MH. Chronic venous disease in an ethnically diverse population: the
San Diego Population Study. Am J Epidemiol 2003;58:448–56.4. White GH. Chronic venous insufficiency. In: Veith F, Hobson RW, Williams
RA, Wilson SE, editors. Vascular surgery. 2nd edn. New York: McGraw-Hill, Inc; 1993: 865–88.
5. Reporting Standards in Venous Disease. Prepared by the Subcommittee on Reporting Standards in Venous Disease, Ad Hoc Committee on Reporting Standards, Society for Vascular Surgery/North American Chapter, International Society for Cardiovascular Surgery. J Vasc Surg 1988;172–81.
6. Sadick NS. Advances in the treatment of varicose veins: ambulatory phlebectomy, foam sclerotherapy, endovascular laser, and radiofrequency closure. Dermatol Clin 2005;23(3):443–55.
7. Clarke GH, Vaskedis SN, Hobbs JT, Nicolaides AN. Venous wall function in the pathogenesis of varicose veins. Surgery 1992;111(4):402–8.
8. Gourgou S. Lower limb venous insufficiency and tobacco smoking: A case control study. Am J Epidemiol 2002;155:1007–15.
9. van Bemmelen PS, Beach K, Bedford G et al. The mechanism of venous valve closure: Its relationship to the velocity of reverse flow. Arch Surg 1990;125:617–9.
10. van Bemmelen PS, Bedford G, Beach K et al. Quantitative segmental evaluation of venous valvular reflux with duplex ultrasound scanning. J Vasc Surg 1989;10:425–31.
11. Komsulglu B, Goldeli O, Kulan K. Prevalence and risk factors of varicose veins in an elderly population. Gerontology 1994;40:25–31.
12. Rutherford RB, Padberg FT, Comerota AJ. Venous severity scoring an adjunct to venous outcome assessment. J Vasc Surg 2000;31:1307–12.
13. Allegra C, Antignani PL, Bergan JJ, The “C” of CEAP: suggested definitions and refinement: an International Union of Phlebology conference of experts. J Vasc Surg 2003;37:129–31.
14. Bradbury A, Evans C, Allan PC. What are the symptoms of varicose veins? The Edinburgh Vein Study cross-sectional population survey. Br Med J 1999;381:353–6.
15. Kurz X, Lamping DL, Kahn SR. Do varicose veins affect quality of life? Results of an international population-based study. J Vasc Surg 2001;34:641–8.
SPOTLIGHT
9www.hkmacme.org HKMA August 2009
Answer these on page 16 or make an online submission at:
www.hkmacme.org
1. Chronic venous disorder (CVD) includes a spectrum of clinical presentations ranging from uncomplicated telangiectasias and varicose veins to disabling venous ulceration.
2. Loss of vein wall elasticity, resulting in the failure of valve leaflets to seal, is a presumed cause of CVD.
3. Less than 10% of the US adult population suffers from some form of CVD.
4. Progesterone and oestrogen both influence the onset of varicose veins through relaxation of smooth muscle.
5. In CEAP classification, the four categories selected for classification were: clinical state (C), (a)etiology (E), anatomy (A), and pathophysiology (P).
6. Simple varicose veins without complications belongs to clinical class 3 in the CEAP classification.
7. The definition of varicose veins in the CEAP classifi-cation is subcutaneous dilated veins equal to or more than 3 mm in diameter in the upright position.
8. The presence of lipodermatosclerosis and/or atrophie blanche indicate a higher likelihood of progression to more severe disease than the presence of pigmentation and/or eczema.
9. The superficial system includes the great and short saphenous systems but not the branch varices.
10. The two major pathophysiological categories — Reflux (R) and Obstruction (O)—never occur in combination.
11. Telangiectasias (spider veins) is not a chronic venous disorder.
ANSWERS TO JULY 2009
Posterior cruciate ligament (PCL) injuries — An update on current management – part 2
1. False 2. True 3. True 4. True 5. False6. False 7. False 8. True 9. False 10. True
Please indicate whether the following questions are true or false

QUESTIONS
1. What is the usual loading dose? a. 1 mg b. 2 mg c. 5 mg d. 20 mg
2. What are the common drugs that may inhibit its function?
a. Cholestyramine b. Barbiturates c. Rifampin d. Sucralfate e. All of the above
3. What are the common drugs that may potentiate its effect?
a. Amiodarone b. Erythromycin c. Fluconazole d. Cimetidine e. All of the above
4. What are the antidotes for warfarin? a. Vitamin K b. Fresh frozen plasma c. Recombinant factor VIIa d. All of the above
JULY ANSWERS ANSwERS
1. c 2. e 3. e 4. d
Warfarin is rapidly and almost completely absorbed from the gastrointestinal tract and circulates bound to albumin with a mean plasma half life of approximately 40 hours. It inactivates vitamin K in the liver, thereby interfering with the vitamin K dependent clotting factors including prothrombin. Metabolism is affected by inherited allelic variants of P450 CYP2C9, which catalyzes the conversion of S-warfarin to its inactive metabolite. Subjects homozygous for the least active alleles are more likely to require a low warfarin dose and to experience warfarin-released bleeding complications. That explains the frequently encountered variation of dosages for different individuals to achieve an optimal anticoagulation effect. The common loading dose is 5–10 mg, followed by 2–3 mg daily but depending on the known response from different individuals, these may be somewhat variable. The usual titrating dose interval is 0.5 mg daily. It may require several days for the optimal dose to be reached. After stabilization of the international normalized ratio (INR) with a maintenance dose, regular monitoring of INR every 4–8 weeks is recommended. The effect of warfarin is often affected by food and drugs. Dietary variations in vitamin K alter warfarin’s anticoagulation effects; high vitamin K intake in the diet reduces the anticoagulant response to warfarin. Drug interactions are common through different mechanisms; altered platelet function (antiplatelet agents), direct gastrointestinal injury (NSAIDs), altered gut vitamin K synthesis (antibiotics), altered warfarin metabolism (amiodarone, fluconazole), and interference with the vitamin K cycle (acetaminophen). The common drug classes that may cause drug interactions are: antibiotics, antifungals, antidepressants, antiplatelet drugs, amiodarone, anti-inflammatory agents, acetaminophen and alternative remedies. Careful monitoring with INR is needed if these drugs are used concomitantly with warfarin. The chief side effect of warfarin, like heparin, is bleeding. If reversal is not urgently needed, cessation of warfarin generally stabilizes the INR within 3–5 days. If rapid reversal is needed, transfusion of fresh frozen plasma and administration of vitamin K will effectively stabilize the INR quickly. However, vitamin K administration may induce transient resistance in subsequent re-anticoagulation. In serious bleeding with excessive INR, a single dose of recombinant factor VIIa may be useful.
10 www.hkmacme.orgHKMA August 2009
A 22-year-old man was seen for on-and-off low grade fever
CARDIOLOGY
A 22-year-old man was seen for on-and-off low grade fever for 4 months. He is a non-smoker and a non-drinker with good past health. There was no history of heart disease during his childhood and teenage years. He was seen twice in general government out-patient clinics with a normal chest X-ray. His haemoglobin was found to be 9.5 g/dL and his white cell and platelet counts were normal. There was no feature of gastrointestinal bleeding. A few courses of empirical antibiotics were intermittently given in the recent few months with no improvement. His exercise capacity was gradually decreased to a few blocks on level ground. Physical examination revealed marked tachycardia at 130/min with a grade 4/6 pansystolic murmur at the apex radiating to the axilla. His chest was clear with no sign of fluid overload and there was no ankle oedema. Jugular venous pressure was not elevated. Several vasculitic skin lesions were noted at his finger tips.
Please answer ALL questions
1. What is your clinical diagnosis?
a. Chest infection b. Pyrexia of unknown origin c. Infective endocarditis
2. What further history would you like to obtain from the patient?
a. Travel history b. Dental treatment history c. Physical examination
findings by family doctors, if any
d. All of the above
Answer these on page 16 or make an online submission at:
www.hkmacme.org
3. What further investigations would you like to order?
a. Urine examination b. Blood culture c. Echocardiogram d. All of the above
4. What treatment would he need for your diagnosis?
a. Full intravenous course of antibiotic
b. Blood transfusion c. Diuretic d. Beta-blockade therapy
The content of the Office Cardiology Series is provided by:
Dr. LI Siu Lung, Steven FHKAM (Med), FRCP (Glasg), FRCP (Edin), FRCP (Lond), Specialist in Cardiology.
Dr. wONG Shou Pang, Alexander FRCP, FHKAM (Med.), FHKCP, Specialist in Cardiology
臨床心臟科個案研究之內容誠蒙李少隆醫生及王壽鵬醫生提供。
11www.hkmacme.org HKMA August 2009
DERMATOLOGY
Complete BOTH Dermatology and
Cardiology courses and earn
BOTH
0.5 CME POINT0.5 CME POINT
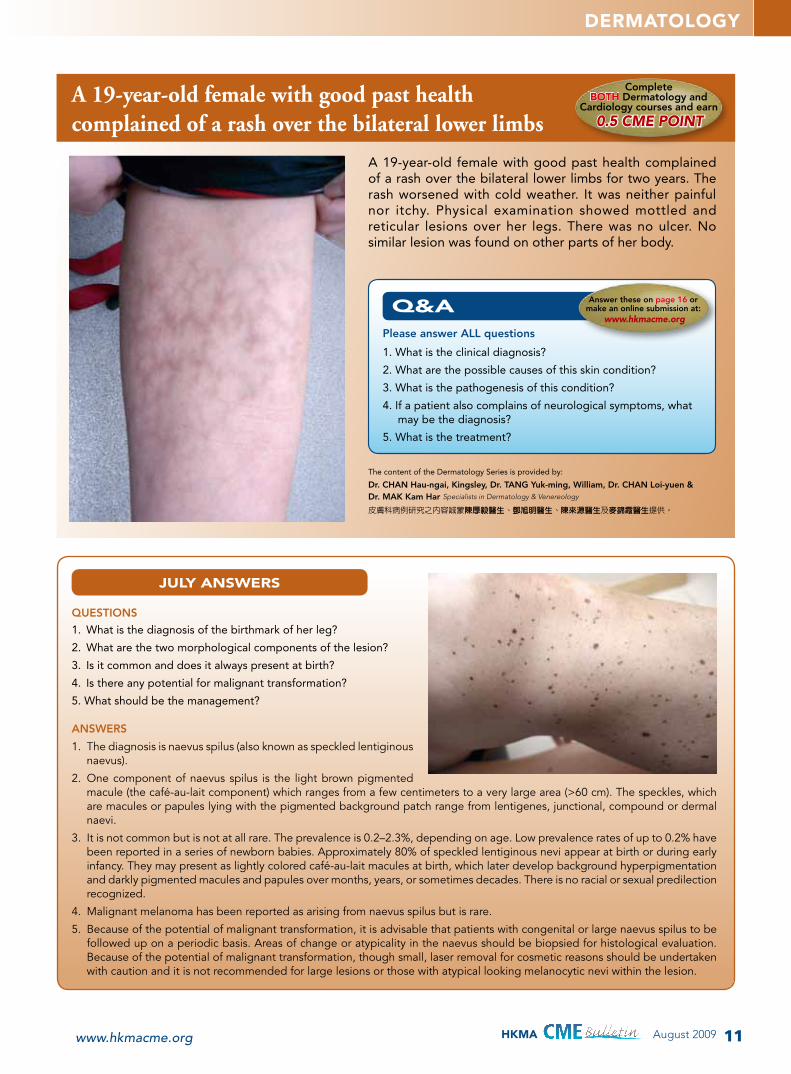
A 19-year-old female with good past health complained of a rash over the bilateral lower limbs
A 19-year-old female with good past health complained of a rash over the bilateral lower limbs for two years. The rash worsened with cold weather. It was neither painful nor itchy. Physical examination showed mottled and reticular lesions over her legs. There was no ulcer. No similar lesion was found on other parts of her body.
QUESTIONS
1. What is the diagnosis of the birthmark of her leg?
2. What are the two morphological components of the lesion?
3. Is it common and does it always present at birth?
4. Is there any potential for malignant transformation?
5. What should be the management?
JULY ANSWERS
ANSwERS
1. The diagnosis is naevus spilus (also known as speckled lentiginous naevus).
2. One component of naevus spilus is the light brown pigmented macule (the café-au-lait component) which ranges from a few centimeters to a very large area (>60 cm). The speckles, which are macules or papules lying with the pigmented background patch range from lentigenes, junctional, compound or dermal naevi.
3. It is not common but is not at all rare. The prevalence is 0.2–2.3%, depending on age. Low prevalence rates of up to 0.2% have been reported in a series of newborn babies. Approximately 80% of speckled lentiginous nevi appear at birth or during early infancy. They may present as lightly colored café-au-lait macules at birth, which later develop background hyperpigmentation and darkly pigmented macules and papules over months, years, or sometimes decades. There is no racial or sexual predilection recognized.
4. Malignant melanoma has been reported as arising from naevus spilus but is rare.
5. Because of the potential of malignant transformation, it is advisable that patients with congenital or large naevus spilus to be followed up on a periodic basis. Areas of change or atypicality in the naevus should be biopsied for histological evaluation. Because of the potential of malignant transformation, though small, laser removal for cosmetic reasons should be undertaken with caution and it is not recommended for large lesions or those with atypical looking melanocytic nevi within the lesion.
The content of the Dermatology Series is provided by:
Dr. CHAN Hau-ngai, Kingsley, Dr. TANG Yuk-ming, william, Dr. CHAN Loi-yuen & Dr. MAK Kam Har Specialists in Dermatology & Venereology
皮膚科病例研究之內容誠蒙陳厚毅醫生、鄧旭明醫生、陳來源醫生及麥錦霞醫生提供。
Please answer ALL questions
1. What is the clinical diagnosis?
2. What are the possible causes of this skin condition?
3. What is the pathogenesis of this condition?
4. If a patient also complains of neurological symptoms, what may be the diagnosis?
5. What is the treatment?
Answer these on page 16 or make an online submission at:
www.hkmacme.org

12 www.hkmacme.orgHKMA August 2009
NEUROLOGY
A 6-year-old girl who recently began stuttering Complete this courseand earn
1 CME POINT1 CME POINT
A 6-year-old girl was brought to the clinic by her parents, who were concerned because she had begun stuttering. They noted that the problem seemed to have gotten worse after she started kindergarten at age 5. The child had been in good general health, with no growth or developmental abnormalities. She had been born at term, and her mother had had no complications during pregnancy. When the child spoke, she seemed unconcerned about the stuttering. She frequently repeated the initial sounds of words and prolonged vowel sounds in some words. She did not seem anxious and did not seem to be exerting effort to control the stuttering.
Developmental stuttering is stuttering that is not caused by a neurological or psychiatric disorder. It affects 1% of the adult and paediatric population. Stuttering that develops before the age of 4 years and resolves spontaneously is considered a developmental stutter and may be related to the difficulty of mastering complex speech. It is somewhat more common in boys than in girls.
Stuttering of sudden onset, particularly in an older child or in an adult, may be the result of neurological or psychiatric pathology and warrants a careful evaluation. Examples of medical conditions that can cause stuttering include stroke, head injury, psychological trauma, and Parkinson’s disease. In some cases, stuttering has been brought on by medications such as theophylline and serotonin reuptake inhibitors (SSRIs). Medication-induced stutters stop when the medication is discontinued.
The actual cause of developmental stuttering is unknown. At one time, it was thought that stuttering was caused by abnormalities in the tongue or larynx, and treatments were directed toward improving the muscle strength of both. It is now clear some neurological component is involved, though the mechanism is not yet fully understood.
In addition, a genetic component appears to be associated with stuttering. About 15% of patients who stutter have a parent who stutters, and the concordance rate between monozygotic twins is about 70%. In up to 75% of paediatric patients, the condition resolves over the course of several years, but about 25% continue stuttering, which is referred to as persistent developmental stuttering.
Evidence suggests that stuttering results from a central neuromotor dysfunction that leads to disorganized timing for generating fluent speech. Because symptoms can improve with treatment with haloperidol, it has been theorized that dopamine abnormalities contribute to the disorder. Positron emission tomography studies have demonstrated increased activity in a pattern that suggests overactivity in the presynaptic dopamine system in areas that modulate speech. Neuroleptic drugs and SSRIs can cause persons with normal fluency to stutter, and the drugs worsen the symptoms in
stutterers; these findings support the theory of involvement of the dopamine receptors.
Increased white-matter volume in the prefrontal and sensorimotor areas and in the perisylvian speech and language areas has been found in magnetic resonance imaging studies of patients who stutter. It is not clear whether these changes are related to the cause of stuttering or whether they are a response to stuttering, but they demonstrate that neuroanatomic differences are present in persons who stutter.
Stuttering is a dysfluency in speech that is characterized by involuntary repetitions, pauses, and prolongation of sounds or syllables. The symptoms may be mild or severe. Patients with more severe symptoms often become anxious and embarrassed about their speech, causing them to avoid social situations. The physical attempts to overcome the stuttering also may cause them to grimace or to make a movement similar to a tic, and anxiety makes the speech difficulties worse.
Children or adults with a developmental stutter demonstrate: 1) 3 or more stuttering dysfluencies per 100 syllables of speech; 2) frequent purposeful efforts to control the stutter; and 3) anxiety about the speech difficulties. Dysfluencies include repetition of syllables (e.g. “th … th … there”) and prolongation of sounds (e.g. “ssssstop” or “liiiiiittle”). Purposeful efforts to control the stutter include interjection of sounds (e.g. “uh”) in an attempt to slow the speech. The child may also grimace or tense his or her shoulders in an attempt to control the stuttering.
The speech of the child presented is dysfluent, but she appears relaxed and is not using purposeful efforts to control the stutter. She may have a stutter related to a sudden demand (e.g. related to starting school) for more complex speech that she is not yet able to produce easily rather than a true developmental stutter. However, no accurate test exists to determine whether her stuttering is definitely related to a normal difficulty as she masters complex speech or whether it is a developmental stuttering that will persist. The quality of her speech, the degree of anxiety she exhibits over time,

13www.hkmacme.org HKMA August 2009
NEUROLOGY
and the persistence of the difficulty are general markers that should be monitored. If she has decreasing quality of speech, develops anxiety, or has persistence of the stutter, she might benefit from intervention.
Speech therapy is the main option for treatment. Unfortunately, it is not always clear who would benefit from intervention, as many children have transient developmental stuttering related to the difficulties of mastering complex speech patterns. Most children who stutter “outgrow” it over the course of several years. However, waiting until a child is older before beginning a speech therapy program can reduce the effectiveness in restoring normal fluency. Adults can still benefit from speech therapy, though they often do not achieve total fluency, or they may have relapses during times of stress.
One speech therapy treatment method for stuttering is the Lidcombe programme. This consists of training parents to praise the child for fluent speech and to intervene with nonfluent speech by encouraging the child to restate the phrase in a more fluent manner. A demands-and-capacities treatment model is grounded by the theory that stuttering
results when the demands on a child to produce complex speech exceed the child’s speaking ability. In this model, parents are encouraged to speak to the child more slowly and to allow more time for the child to answer.
Although neuroleptic drugs (e.g. haloperidol) have been shown to reduce stuttering, the adverse-effect profile limits their usefulness. For patients with more severe symptoms that have not responded as well as desired to speech therapy, risperidone, sertraline, and paroxetine may offer some improvement, though none has been evaluated in large controlled studies. Anecdotal reports exist of patients benefiting from treatment with antidepressants because of an overall reduction in anxiety, which is known to aggravate stuttering.
Ongoing studies of the neurological findings associated with stuttering may lead to improved medical intervention in the future.
1. Developmental stuttering is stuttering that is not caused by a neurological or psychiatric disorder and it affects ___% of the adult and paediatric population.
a. 10 b. 20 c. 1 d. 2
2. Children or adults with a developmental stutter demonstrate 3 characteristics.
a. True b. False
3. One speech therapy treatment method for stuttering is the ________ programme.
a. Sidcup b. Lidcombe c. Bidwell d. Wycombe
4. For patients with more severe symptoms that have not responded as well as desired to speech therapy, which treatment may offer some improvement?
a. Risperidone b. Sertraline c. Paroxetine d. All of the above
Please indicate 1 answer to each question
Answer these on page 16 or make an online submission at:
www.hkmacme.org
GASTROINTESTINAL MEDICINE JULY ANSWERS
1. b 2. e 3. a 4. e
CURRENT STUDIES
Tics and developmental stutteringMulligan HF, et al / Parkinsonism and Related Disorders / 2003;9:281–9
Background. Developmental stuttering affects 1% of the population but its cause remains unclear. Recent PET studies of metabolism in the central nervous system suggest that it may be related to dysfunction in the basal ganglia or its connections with regions of the cortex associated with speech and motor control. objective. To determine the presence and characteristics of involuntary movements (IMs) in people who stutter and to investigate the hypothesis that these movements may be of a very similar nature to the IMs seen in patients with movement disorders due to basal ganglia dysfunction. Methods. Sixteen adults with developmental stuttering and 16 controls matched for sex and age were audio–videotaped while freely speaking 300 words in conversation and reading aloud 300 words. The audio data was inspected for dysfluencies and the video data was scrutinised for the presence and characteristics of IMs. Results. Subjects who stuttered produced more IMs than controls during free speech (354 vs 187, p <0.05) and reading (297 vs 47, p <0.001). Most of the IMs in both groups were tics, with a greater number of both simple and complex motor tics (CMTs) in subjects who stuttered. CMTs were more frequent than simple motor tics in those who stuttered, but not in controls... For full article please go to www.hkmacme.org
COMPLETE THIS COURSE ONLINE AND RECEIVE
1 CME POINT 1 CME POINT

14 www.hkmacme.orgHKMA August 2009
GENERAL MEDICINE
A 35-year-old female with complaints of jaw pain and swelling
Complete this courseand earn
1 CME POINT1 CME POINT
A 35-year-old woman presented with complaints of jaw pain and swelling. The symptom of jaw pain had occurred intermittently for several months. Yesterday, she began having swelling in the lower jaw, and it was worse this morning. She denied fever, throat pain, or neck pain. She was in good general health, and her past medical history was negative except for a tonsillectomy as a child. She was a current smoker, with a history of 1 to 1.5 packs per day for 15 years. On examination, the patient’s temperature was normal at 36.5°C; remaining vital signs were also normal. She had noticeable swelling over the lower right jaw area. No erythema or discolouration was present. The areas of the parotid gland and submandibular gland were not swollen or tender. She had pain to percussion with a tongue depressor over the first and second lower right molar teeth. She had several teeth with significant caries, including the teeth that exhibited pain to percussion. The gums were mildly inflamed at the gum line, but were not fluctulant and there was no focal swelling. She had no cervical adenopathy or tenderness in the soft tissue structures of the face and neck, but did have a single palpable submental lymph node. Results of the remainder of the head and neck examination were normal.
The finding of tenderness to percussion over the affected tooth is strongly suggestive of an apical abscess of the tooth. She does not have any apparent involvement of the salivary glands. In addition, she has no tenderness or erythema of the cheek and no fever, so it is unlikely she has a cellulitis. The acute onset of symptoms makes malignancy an unlikely cause. Sinusitis can cause pain and swelling in the upper jaw, but it is unlikely to affect the lower jaw. It is useful to bear in mind that dental pain is mediated by the fifth cranial nerve, and referred pain may develop in any areas supplied by the nerve, including the meninges.
Other dental conditions should also be considered. Pulpitis is an inflammation of the pulp that results in sensitivity to cold and hot and may be aggravated by lying down. Periodontal disease is common and presents with inflammation of the gingiva and loss of alveolar bone due to the chronic inflammation. It is usually painless, though the patient may find the gums bleed easily. With periodontal disease, the space between the gum and tooth deepens, resulting in a potential space that can trap food and become infected.
Other dental problems that can present with pain include acute necrotizing ulcerative gingivitis, a cracked tooth or root, acute alveolar osteitis (dry socket), and postextraction periostitis. Acute necrotizing ulcerative gingivitis manifests with swelling and tenderness of the interdental papillae, with ulceration and pseudomembrane formation. This is more common in patients with stress, smoking, systemic illness, and local trauma to the gums. Postextraction periostitis is common but benign and usually resolves after 24 hours. Acute alveolar osteitis may develop after an extraction if the local clot in the socket is lost. This should be treated with irrigation and packing but not with manipulation to create a new clot (this increases the risk of osteomyelitis). The history and physical examination results rule these out for
this patient.Other medical problems such as temporomandibular
joint syndrome, neuropathic pain, lesions of the buccal mucosa (e.g. pemphigus, Sjögren’s syndrome), cranio- mandibular disorders of the musculature or joint space or of the temporomandibular joint, and rarely coronary artery disease can cause pain to radiate to the neck and jaw.
The tooth is composed of the crown, which is the enamel-covered portion of the tooth, and the root, which is covered with the softer cementum. The pulp of the tooth contains the neurovascular supply.
Most dental infections begin with caries. Bacterial metabolism of carbohydrate produces acid, which in turn causes decalcification of the enamel. Once enough enamel is eroded, the dentin is exposed, and bacteria and saliva enter the pulp of the tooth. The pulp becomes inflamed and eventually degenerates; this is referred to as pulpitis. The infection then can track downward through the apex of the root, resulting in a periapical infection. At this stage, the infection is still within the alveolar bone, but it can spread to subperiosteal spaces and eventually into the soft tissue of the neck and face.
The soft tissues of the face, mouth, and neck should be examined for evidence of infection. Check the tongue, Wharton’s duct, and Stensen’s duct for swelling or drainage, suggesting infection. Percussion of the involved teeth with a tongue blade is a useful way to determine tenderness in the tooth. If irritation to the pterygoid or masseter muscle is present, trismus may develop, and the patient will be unable to fully open his or her mouth.
Periapical films are the best way to examine the bony structure of the teeth, but they usually are not available outside of a dental facility. Panoramic radiographs may be useful in some cases.

15www.hkmacme.org HKMA August 2009
GENERAL MEDICINE JULY ANSWERS
1. b 2. d 3. d 4. a
GENERAL MEDICINE
1. Pulpitis is an inflammation of the pulp that results in sensitivity to cold and hot and may be aggravated by rapid movement.
a. True b. False
2. Acute necrotizing ulcerative gingivitis is more common in patients with:
a. Stress b. Smoking c. Systemic illness d. Local trauma to the gums e. All of the above
3. Some medical problems such as ___________can cause pain to radiate to the neck and jaw.
a. Sjögren’s syndrome b. Sven’s syndrome c. Jaansen’s disease d. Munchausen’s disease
4. Ludwig’s angina is a soft tissue infection that can result from spread of infection into the submental and sublingual spaces.
a. True b. False
Please indicate 1 answer to each question
Answer these on page 16 or make an online submission at:
www.hkmacme.org
For uncomplicated dental infections, empiric treatment is acceptable, and penicillin is usually effective. It is active against most oral bacteria, though resistance can be found in some species of Bacteroides. Cephalosporins, clindamycin, and erythromycin are also effective treatment options.
Ultimately, treatment of the caries with endodontic dental procedures is necessary, and all patients should follow up with a dentist as soon as possible. If the tooth has intact alveolar support, the tooth may be amenable to treatment for the cavity. If the infection has damaged the root or the alveolar support, it will have to be extracted.
An abscess, if present, will require incision and drainage. Local anaesthetic with a simple, small incision is appropriate, but extensive debridement and drainage should be left to the dentist.
If the patient has pain but no signs of infection, such as tenderness to percussion (in the tooth), then treatment with just an analgesic and follow-up with a dentist is appropriate. The infection can track into potential spaces in the head, neck, and mediastinum. This can be life threatening, so any patient who has a toxic appearance should undergo further evaluation. Ludwig’s angina is a soft tissue infection that can result from spread of infection into the submental
and sublingual spaces. Symptoms include elevation of the tongue and swelling, and it is critical to recognize, as it can quickly progress and compromise the airway. Infection can also spread into the periorbital space and cause a periorbital cellulitis. It can even provoke a cavernous sinus thrombosis if it extends into the venous drainage system of the face. Submandibular infections can potentially extend into the mediastinum.
Any patient who has symptoms that suggest extension of the infection into the face or neck should be evaluated by a specialist. Computed tomography is useful to determine involvement of deeper structures, including the soft tissue of the neck and the mediastinum, if indicated.
CURRENT STUDIES
A review of dental implants and infectionPye AD, et al / Journal of Hospital Infection / 2009;72:104-10
Dental implants have become increasingly common for the management of tooth loss. Despite their placement in a contaminated surgical field, success rates are relatively high. This article reviews dental implants and highlights factors leading to infection and potential implant failure. A literature search identified studies analysing the microbial composition of peri-implant infections. The microflora of dental peri-implantitis resembles that found in chronic periodontitis, featuring predominantly anaerobic Gram-negative bacilli, in particular Porphyromonas gingivalis and Prevotella intermedia, anaerobic Gram-negative cocci such as Veillonella spp. and spirochaetes including Treponema denticola. The role of Staphylococcus aureus and coagulase-negative staphylococci that are typically encountered in orthopaedic infections is debatable, although they undoubtedly play a role when isolated from clinically infected sites. Likewise, the aetiological involvement of coliforms and Candida spp. requires further longitudinal studies. Currently, there are neither standardised antibiotic prophylactic regimens for dental implant placement nor universally accepted treatment for peri-implantitis. The treatment of infected implants is difficult and usually requires removal. In the UK there is no systematic post-surgical implant surveillance programme. Therefore, the development of such a project would be advisable and provide valuable epidemiological data
COMPLETE THIS COURSE ONLINE AND RECEIVE
1 CME POINT 1 CME POINT
16 www.hkmacme.orgHKMA August 2009
Please return completed answer sheet to the HKMA Secretariat (Fax: 2865 0943) on or before 15 September 2009 for documentation. However, if you choose to do the exercises online, you do not need to return this answer sheet by fax.
請回答所有問題,並於 2009 年 9 月 15 日前將答題紙傳
真或寄回香港醫學會(傳真號碼:2865 0943)。但如果
選擇在網上做練習,便不需要把答題紙傳真給秘書處。
答題紙 August 2009
ANSWER SHEET
Name 姓名: _______________________________________________________
HKMA Membership No. or HKMA CME No.香港醫學會會員編號或持續進修號碼: _________________________________
HK ID No. 香港身份証號碼:□□-□□□xxx (x)
Signature 簽名: ___________________________________________________
Contact Tel No. 聯絡電話: __________________________________________
✂
3 CME POINTS
THIS MONTH GO ONLINE AND COMPLETE UP TO 3 OTHER
MONTHLY COURSES FOR AN EXTRA
3 CME POINTSwww.hkmacme.orgwww.hkmacme.org
ANSWER BOX
Please answer ALL questions and write the answers in the space provided. Both the Cardiology and Dermatology courses must be completed to earn 0.5 CME point. The other courses attract 1 CME point each.
SPOTLIGHT
1 2 3 4 5 6 7 8 9 10 11
DERMATOLOGY
1. ______________________________________________________________________________________________________________
______________________________________________________________________________________________________________
2. ______________________________________________________________________________________________________________
______________________________________________________________________________________________________________
3. ______________________________________________________________________________________________________________
______________________________________________________________________________________________________________
4. ______________________________________________________________________________________________________________
______________________________________________________________________________________________________________
5. ______________________________________________________________________________________________________________
______________________________________________________________________________________________________________
NEUROLOGY
1 2 3 4
GENERAL MEDICINE
1 2 3 4
CARDIOLOGY
1 2 3 4
CME NOTIFICATION
19www.hkmacme.org HKMA August 2009
CME EVENT 講課簡介 VENUE & TIME 地點及時間
10 September 2009 (Thursday)HKMA Structured CME Programme with HKS&H Session IX: New Trends in Management of Vitreo-Retinal-Macular Diseases – From Diagnosis to Treatment
Dr. CHAN wai ManMBBS (HK), MRCP (UK), FRCS (Edin), FRCP (Edin), FCOphth (HK), FRCOphth (UK), FHKAM (Ophthalmology), Specialist in Ophthalmology This symposium is co-organized with Hong Kong Sanatorium & Hospital
The HKMA Dr. Li Shu Pui Professional Education Centre2/F, Chinese Club Building 21-22 Connaught Road Central, HK Lecture: 2:00–3:00 p.m. (Light lunch will begin at 1:15 p.m.)
香港中環干諾道中二十一至二十二號華商會所大廈二樓香港醫學會李樹培醫生專業教育中心講課:下午二時至三時正 (茶點於下午一時十五分開始)
REGISTRATION:Please fill in and return the Registration Form together with a cheque of adequate amount made payable to “The Hong Kong Medical Association” to 5/F Duke of Windsor Social Service Building, 15 Hennessy Road, Hong Kong. Each lecture will carry 1 CME point under the MCHK/HKMA CME Programme (unless otherwise stated). Accreditation from other colleges is pending. (The Secretariat fax no.: 2865 0943)
Please be informed that Confirmation Letter of Registration is required. If you have not received any replies, please do not hesitate to contact us at 2527 8452.
報名方法:
請填妥表格連同支票寄交香港灣仔軒尼詩道十五號溫莎公爵社會服務大廈五樓,支票抬頭請書明支付「香港醫學會」。
參加者可獲醫務委員會/香港醫學會持續醫學進修計劃積分一分 (除特別註明外)。其他專科學院之學分尚在申請中。
(秘書處傳真號碼:2865 0943) 參加者需持有講課確認通知書出席持續醫學進修講課。假若你沒有收到任何通知,請致電 2527 8452 查詢。
Please register for participation. First come, first served. 名額有限 請早登記
I enclose herewith a cheque of 現隨表格附上支票一張作為講課之報名費用:HK$港幣 _________
Name 姓名:__________________________ Tel No 電話:___________________ Fax No.傳真 : ___________________
HKMA Membership No. 會員編號
or HKMA CME No. 或進修號碼:_____________________________ Signature 簽名: _________________________________
Data collected will be used and processed for the purposes related to the MCHK/HKMA CME Programme only. All registration fees are not refundable or transferable.
個人資料將用於有關香港醫學會持續醫學進修計劃之事宜。所有報名費用將不給予退還或轉授予其他會員。
Please “✔” as appropriate.
請在適用處加上 ✔ 號
HKMA Structured CME Programme with HKS&H HKMA Member CME Participants
10 September 2009 HKMA Structured CME Programme with HKS&H Year 2009 Session IX – New Trends in Management of Vitreo-Retinal-Macular Diseases – From Diagnosis to Treatment
HK$50 □ HK$80 □
HKMA CME Programme 香港醫學會持續進修計劃CME Lecture – September 2009 進修講課 – 二零零九年九月
Reply Slip 回條
I would like to register for the following CME lecture(s) 本人欲報名參加以下講課:
CME NOTIFICATION
20 www.hkmacme.orgHKMA August 2009
DATE TOPIC
13 September 2009 1. The Lonely Family Doctor: Access to Information, Resources and Colleagues Dr. TANG Kuen Yan, Alfred Family Physician in private practice
2. E-medical Record Dr. HO Chung Ping, MH Council Member, HKMA
11 October 2009 1. Management of Chronic Illness in Family Practice Dr. Kenny KUNG Specialist in Family Medicine
2. Pain Management in Family Practice Prof. CHAN Kwok Wai Director of Postgraduate Programme in Family Medicine, School of Public Health, CUHK
Registration: PleasefillinandreturntheRegistrationFormonp21togetherwithachequeofadequateamountmade payable to “The Hong Kong Medical Association” to 5/F Duke of Windsor Social Service Building, 15HennessyRoad,HongKongbefore the date of the function.
報名方法 : 請於講課日前填妥第 21 頁之表格連同支票寄交香港灣仔軒尼詩道十五號溫莎公爵社會服務大廈五樓
支票抬頭請書明支付「香港醫學會」。
First come, first served. 名額有限 請早登記
HKMA Certificate Course on Family Medicine香港醫學會 ─ 家庭醫學證書課程
Hong Kong Medical Association Department of Community and Family Medicine, CUHK
Jointly organized by
地點:伊利沙伯醫院 M座地下演講廳
時間:下午二時至五時
持續醫學進修計劃積分:三分
報名費用:醫學會會員 -每課堂港幣五十元正
持續進修參加者 -每課堂港幣八十元正
敬備茶點
Venue : Lecture Theatre, G/F., Block M, QEHTime : 2:00–5:00 p.m.CME points : 3Fee : HK$50 per lecture for HKMA Members HK$80 per lecture for CME ParticipantsLight snacks will be provided.
Certification Requirement: 75% attendance
Queen Elizabeth Hospital
Supported By
HKMA KECN-UCH CME Course for Health Personnel 2009Registration Form Please return completed form to Gary WONG (UCH) by fax at 3513 5548.I would like to register to the following lecture:
15 August 2009Pain management: Anesthetist perspective: (1) Neck and back pain (2) Post herpetic neuralgiaDr. LIM Huey Sing (AC, Ana&PM, UCH)
19 September 2009Paediatric OphthalmologyDr. Emily TANG (Res, Eye, UCH)
My clinic is located At Kowloon East (Please specify*): ___________________________________________)
Outside Kowloon East Region
Name: _______________________________________________Tel: ________________________________ Fax: _________________________________
Address: ______________________________________________________________________________________________________________________
Signature:____________________________________________ Date: _____________________________________________________________________
CME NOTIFICATION
21www.hkmacme.org HKMA August 2009
DATE TOPIC
23 August 2009 General Surgery1. Approach to Breast Mass Dr. HO Leung Sing Consultant (Surgery), PMH
2. Management of Goiter Dr. LUK Hung To Chief of Service, Dept of Surgery, PMH/YCH
27 September 2009 Geriatrics1. Use of Drugs in Old Age Dr. KONG Tak Kwan Consultant (Medicine & Geriatrics), PMH
2. Hypertension in Old Age Dr. AU Kai Man Associate Consultant (Medicine & Geriatrics), PMH
Registration: PleasefillinandreturntheRegistrationFormbelowtogetherwithachequeofadequateamountmade payable to “The Hong Kong Medical Association” to 5/F Duke of Windsor Social Service Building, 15HennessyRoad,HongKongbefore the date of the function.
報名方法 : 請於講課日前填妥下面之表格連同支票寄交香港灣仔軒尼詩道十五號溫莎公爵社會服務大廈五樓
支票抬頭請書明支付「香港醫學會」。
First come, first served. 名額有限 請早登記
HKMA Structured CME Programme at Princess Margaret Hospital香港醫學會 ─ 瑪嘉烈醫院分科進修課程
Jointly organized by
Hong Kong Medical Association Princess Margaret Hospital
地點:瑪嘉烈醫院 G座八樓大堂
時間:下午二時至四時
持續醫學進修計劃積分:兩分
報名費用:醫學會會員 -每課堂港幣五十元正
持續進修參加者 -每課堂港幣八十元正
Venue : Hospital Hall, 8/F., Block G, PMH
Time : 2:00–4:00 p.m.
CME points : 2
Fee : HK$50 per lecture for HKMA Members HK$80 per lecture for CME Participants
I enclose herewith a cheque of 現隨表格附上支票一張作為講課之報名費用:HK$港幣 ______________
Name 姓名:______________________________________ Tel No. 電話:__________________________ Fax No.傳真 : __________________________
HKMA Membership No. 會員編號:
or HKMA CME No. 或進修號碼:____________________________________ Signature 簽名: _________________________________________________
Data collected will be used and processed for the purposes related to the MCHK/HKMA CME Programme only. All registration fees are not refundable or transferable.
個人資料將用於有關香港醫學會持續醫學進修計劃之事宜。所有報名費用將不給予退還或轉授予其他會員。
Please “✔” as appropriate. 請在適用處加上 ✔ 號
I would like to register for the following lecture(s) 本人欲參加下列講課:
HKMA Structured CME Programme at QEH/PMH — Registration Form 香港醫學會分科進修課程報名表格
HKMA Member 香港醫學會會員
CME Participants (Non-HKMA member)
持續進修參加者(非香港醫學會會員)
HK$50 HK$80
QEH13 September 2009 Family Medicine
11 October 2009 Family Medicine
PMH23 August 2009 General Surgery
27 September 2009 Geriatrics

CME CALENDAR
23www.hkmacme.org HKMA August 2009
持續進修日程Note: For each issue of the CME Bulletin, we shall try our best to include all the CME activities for the month, which are made known to the Association Secretariat. Members interested in any of these functions are encouraged to check with the individual Colleges for credit points awarded by the Colleges and with respective organizers for confirmation of the details. Pharmaceutical advertisements are welcome. For advertising rates and placement details, please contact Doreen Chang at Tel: 2965 1300, Fax: 3764 0374 or email: [email protected]
Your comments to the HKMA CME Bulletin are most welcome. Please send your opinion to Dr. Wong Bun Lap, Bernard, Editor of HKMA CME Bulletin, by fax at 2865 0943 or via e-mail at [email protected]
August 2009
15 (Sat)2:00-4:00 pm
HA – Pamela Youde Nethersole Eastern Hospital, Family Medicine Dept
Diabetes Mellitus on Public Private InterfaceLecture Theatre, LG1, Ruttonjee HospitalsW L Kwong – Tel: 25956941
➋
16 (Sun)1:00–4:00 pm
Hong Kong Doctors Union
The 164th HKDU Sunday Afternoon SymposiumLecture Hall, 8/F, Block G, Princess Margaret Hospital, Kwai Chung, NTTel: 2388 2728
16 (Sun)3:30–6:00 pm
Hong Kong Doctors Union
The 165th HKDU Sunday Afternoon SymposiumLecture Hall, 8/F, Block G, Princess Margaret Hospital, Kwai Chung, NTTel: 2388 2728
➋
17 (Mon)12:00–1:00 pm
HKU-Dept of Medicine
HKW Geriatric Grand Round6/F, KTSH Centre, GHMs. Joanne Hui – Tel: 2855 3315
➊
17 (Mon)1:00–2:00 pm
HKU-Dept of Medicine
HKW Geriatric Academic Meeting6/F, KTSH Centre, GHMs. Joanne Hui – Tel: 2855 3315
➊
18–19 (Tue–Wed)
HK College of Emergency Medicine American Heart Assn
American Heart Association (AHA) Advanced Cardiovascular Life Support CourseA&E Training Centre, 3/F, Tang Shiu Kin HospitalMs. Cherry Kwok – Tel: 2871 8877
➓
19 (Wed)1:00–3:00 pm
HKDU-Tseung Kwan O Study Group
Mechanical Pain in OA Knee – A Shift in the Management ParadigmMaxim’s Chinese Restaurant, Shop No. 2008, Level 2, Metro City Plaza II, Tseung Kwan O, KowloonTel: 2388 2728
➊
19 (Wed)2:00–4:00 pm
HA-KLN East Cluster/ HA-UCH-Dept of Obstetrics & Gynaecology HA-TKOH-Dept of Obstetrics & Gynaecology Postgraduate Seminar of Department O&G, Kowloon East Cluster (UCH / TKOH)Conference Room, Hospital Library, 1/F, Block H, UCHTel: 3513 4851
➋
19 (Wed)4:30–6:30 pm
HA-QEH-Dept of Accident & Emergency
Multi-Disciplinary Trauma Mortality & Morbidity Meetings 2009Room 4, Lower Ground, Block J, QEHTel: 2958 6473
➋
20 (Thu)6:00–8:00 pm
HK College of Community Medicine
Review Meeting in Areas Related to Public Health MedicineWu Chung House or Centre for Health Protection in Argyle StreetMs. Mavis Chan – Tel: 2871 8745
➋
21 (Fri)10:00 am– 12:00 pm
HKU-Dept of Microbiology
Infectious Disease Rounds for Year 2009Conference Room, Room 405, Clinical Pathology Building, Queen Mary Hospital, 102 Pokfulam Road, Hong KongMs. Karis Larm – Tel: 2855 3243
➋
21 (Fri)1:00–2:00 pm
HA-TMH-Dept of Obstetrics & Gynaecology
Clinical Pathological ConferenceAB1038, 1/F, Main Block, Tuen Mun HospitalMs. Angela Cheung – Tel: 2468 5404
➊
22 (Sat)2:00–3:30 pm
HKMA-Shatin Doctors Network
Lecture Series on Type 2 DM Management: 1) Strategies in Managing Diabetic Complications 2) Managing DM in Primary Care Clinics – Practical InsightsRoyal Park Hotel, ShatinMs. Mabel Chow – Tel: 3189 8770
22 (Sat)2:15–5:15 pm
HK College of Family Physicians
Assessment Enhancement Course for Family Physicians 20098/F, Duke of Windsor Social Service Building, 15 Hennessy Road, Wanchai, HKMs. Charlotte Sham – Tel: 2861 1808
➓
22 (Sat)2:30–4:00 pm
DH-Professional Development & Quality Assurance HK College of Family Physicians
Update Management of Tobacco DependenceLecture Room, 2/F, Ngau Tau Kok Jockey Club Clinic, 60 Ting On Street, Ngau Tau Kok, KowloonAdmin Unit of PDQA – Fax: 2379 5034
23 (Sun)2:00–4:00 pm
Hong Kong Medical Association HA-Princess Margaret Hospital
HKMA Structured CME Programme with Princess Margaret Hospital Session 7: 1) Approach to Breast Mass 2) Management of GoiterG8 HAllHKMA CME Dept. – Tel: 2527 8452
➋
24 (Mon)12:00–1:00 pm
HKU-Dept of Medicine
HKW Geriatric Grand Round5/F, FYKHMs. Joanne Hui – Tel: 2855 3315
➊
24 (Mon)1:00–2:00 pm
HKU-Dept of Medicine
HKW Geriatric Academic Meeting5/F, FYKHMs. Joanne Hui – Tel: 2855 3315
➊
25 (Tue)2:30–5:45 pm
HK College of Psychiatrists
Central Academic Course Module E – Lecture 13; Lecture 14; Lecture 15Conference Room, 1/F, Adm Block, KCHMs. Laura Wong – Tel: 2636 7754
➌
25 (Tue)3:00–5:30 pm
HK College of Psychiatrists
Central Academic Course: Module C – Lecture 13UCHMs. Connie Lo – Tel: 2959 8020
➌
25 (Tue)3:00–5:30 pm
HK College of Psychiatrists
1) Psychological Treatment – an overview2) Descriptive psychopathology: disorder of mood and other symptomsLecture Theatre, G073-074, Block D, CPHMs. Jennifer Mo – Tel: 2456 7152
➌
25 (Tue)5:30–7:30 pm
HA-HK East Cluster
Cluster Trauma AuditPamela Youde Nethersole Eastern HospitalMs. Amelia Lee – Tel: 2595 6442
➋
26 (Wed)1:00–3:00 pm
HKDU-Tsuen Wan Study Group
Update Management in AsthmaCrystal Room, 30/F, Panda Hotel, 3 Tsuen Wah Street, Tsuen Wan, NT Tel: 2388 2728
➊

CME CALENDAR
24 www.hkmacme.orgHKMA August 2009
26 (Wed)4:30-5:30 pm
HA – Pamela Youde Nethersole Eastern Hospital, Paediatrics Dept co-joint with Comprehensive Paediatric Rehabilitation Centre
Education Programme on Paediatric Rehabilitation – Developmental Co-ordination DisordersChild and Youth Health Link (Ward D6, 6/F, Main Block, PYNEH)Lai Pui Shan – Tel: 25956706
➊
27 (Thu)1:00–3:00 pm
HKDU-Hung Hom Study Group
How Does UPLIFT Impact on COPD Management?Spotlight Recreation Club, 4/F, Screen World, Site 8, Whampoa Garden, Hung Hom, Kowloon Tel: 2388 2728
➊
28 (Fri)10:00 am–12:00 pm
HKU-Dept of Microbiology
Infectious Disease Rounds for Year 2009Conference Room, Room 405, Clinical Pathology Building, Queen Mary Hospital, 102 Pokfulam Road, Hong KongMs. Karis Larm – Tel: 2855 3243
➋
28 (Fri)1:00–2:00 pm
HA-TMH-Dept of Obstetrics & Gynaecology
Diagnosis & Treatment of Ovarian Cyst AccidentsAB1038, 1/F, Main Block, Tuen Mun HospitalMs. Angela Cheung – Tel: 2468 5404
➊
28 (Fri)1:30–3:15 pm
HKMA-Shatin Doctors Network
When and How to Start InsulinRoyal Park HotelMs. Sandra Chu – Tel: 2387 8555
➊
29 (Sat)9:00 am–12:00 pm
Hong Kong Medical Association Medical Protection Society
Mastering Your RiskHKMA Central PremisesHKMA CME Dept – Tel: 2527 8452
29 (Sat)9:30–11:30 am
Hospital Authority HK College of Community Medicine
Case Presentations and Journal Presentations in Areas Related to Administrative MedicineRoom 524N, 5/F, Hospital Authority Building, 147B Argyle Street, KowloonMs. Wendy Li – Tel: 2300 6529
➋
29 (Sat)9:30 am–12:00 pm
HK Society of Nuclear Medicine
Clinical Meeting – Journal and Case Presentations; Audits and Projects; Technology SessionPET Centre, LG Floor, Block P, QEHMs. Jenny Cho – Tel: 2958 6437
➌
29 (Sat)2:00–5:00 pm
Hong Kong Medical Association Medical Protection Society
Mastering Your RiskHKMA Central PremisesHKMA CME Dept – Tel: 2527 8452
29 (Sat)2:30–5:00 pm
HK Paediatric Society HK Paediatrics Nurse Assn HK College of Paediatricians Update Series on Child Health 20091) Attention Deficit Hyperactivity Disorders: Presentation and Management2) Advocating for Play: Perspective from Paediatrician3) Therapeutic Play by Hospital Play SpecialistLecture Theatre, M/F, Hospital Authority Building,147B Argyle Street, KowloonTel: 2388 2728
➌
30 (Sun)2:00–5:00 pm
Hong Kong Medical Association Medical Protection Society
Mastering Your RiskHKMA Central PremisesHKMA CME Dept – Tel: 2527 8452
September 2009
1 (Tue)2:30–5:45 pm
HK College of Psychiatrists
Central Academic Course Module E – Lecture 16; Lecture 17; Lecture 18Conference Room, 1/F, Block, CPHMs. Laura Wong – Tel: 2636 7754
➌
1 (Tue)3:00–5:30 pm
HK College of Psychiatrists
Central Academic Course: Module C – Lecture 14 & WorkshopUCHMs. Connie Lo – Tel: 2959 8020
➌
2 (Wed)11:00 am-1:00 pm
HA – Castle Peak Hospital, Psychiatry Dept
Seminar – Violence and Mental DisorderLecture Theatre, Blk D, CPHMs. Cherry Man – Tel: 2456 7855
➋
2 (Wed)2:00–4:00 pm
HA-KLN East Cluster HA-UCH-Dept of Obstetrics & Gynaecology HA-TKOH-Dept of Obstetrics & Gynaecology
Postgraduate Seminar of Department O&G, Kowloon East Cluster (UCH / TKOH)Conference Room, Hospital Library, 1/F, Block H, UCHTel: 3513 4851
➋
3 (Thu)1:15–3:30 pm
HKMA-Tin Shui Wai North Community Network HK Alzheimer’s Disease Assn Lundbeck Institute Hong Kong
Certificate Course in Treating Alzheimer’s Disease in Community: Practical Tips on Early Diagnosis of Alzheimer’s Disease, Illustrated with CasesBallroom C&D, Harbour Plaza Resort City, 18 Tin Yan Road, Tin Shui Wai, NTMs. Jaclyin Lee – Tel: 2877 1106
3 (Thu)2:30-3:30 pm
HA – Queen Mary Hospital, Psychiatry Dept
Interpretation of EEG with Particular Reference to PsychiatryJ2 Seminar Room, Department of Psychiatry, Queen Mary HospitalElaine Tse – Tel: 2855 3066
➊
3 (Thu)5:30-7:00 pm
HA – Tuen Mun Hospital, Family Medicine Dept
ENT Seminar: Topic – Management of Common ENT Conditions (Part 2) – Approach to Hearing Loss, Approach to Hoarseness, Update on Otitis MediaRoom 614, 6/F Ambulatory Care Centre Tuen Mun HospitalCowin Tang – Tel: 2468 6601
➋
3 (Thu)6:00–8:00 pm
HK College of Community Medicine
Review Meeting in Areas Related to Public Health MedicineWu Chung House or Centre for Health Protection in Argyle StreetMs. Mavis Chan – Tel: 2871 8745
➋
4 (Fri)10:00 am–12:00 pm
HKU-Dept of Microbiology
Infectious Disease Rounds for Year 2009Conference Room, Room 405, Clinical Pathology Building, Queen Mary Hospital, 102 Pokfulam Road, Hong KongMs. Karis Larm – Tel: 2855 3243
➋
4 (Fri)8:00–9:00 pm
HKU-Dept of Surgery HK Sanatorium & Hospital-Surgery Centre
Latest Achievements and DevelopmentsAuditorium, 4/F, Li Shu Pui Block Phase II, Hong Kong Sanatorium & Hospital, Happy Valley, HKHKS&H Dept. of Surgery – Tel: 2835 8698
➊
5 (Sat)8:30 am–1:00 pm
HA-NDH-Institute of Clinical Simulation
Medical Intervention of Clinical Emergencies (MICE) WorkshopThe Institute of Clinical Simulation, 3/F, North District Hospital, 9 Po Kin Road, Sheung Shui, NTMs. Katherine Ip – Tel: 2683 8307
➌
CME CALENDAR
26 www.hkmacme.orgHKMA August 2009
5 (Sat)9:00 am–12:00 pm
Hong Kong Medical Association Medical Protection Society
Mastering Your RiskHKMA Central PremisesHKMA CME Dept – Tel: 2527 8452
5 (Sat)2:00–5:00 pm
Hong Kong Medical Association Medical Protection Society
Mastering Your RiskHKMA Central PremisesHKMA CME Dept – Tel: 2527 8452
6 (Sun)2:00–5:00 pm
Hong Kong Medical Association Medical Protection Society
Mastering Your RiskHKMA Central PremisesHKMA CME Dept – Tel: 2527 8452
7 (Mon)12:00–1:00 pm
HKU-Dept of Medicine
HKW Geriatric Grand RoundK2, QMHMs. Joanne Hui – Tel: 2855 3315
➊
7 (Mon)1:00–2:00 pm
HKU-Dept of Medicine
HKW Geriatric Academic MeetingK2, QMHMs. Joanne Hui – Tel: 2855 3315
➊
7 (Mon)6:00–9:00 pm
Hong Kong Medical Association Medical Protection Society
Mastering Your RiskHKMA Central PremisesHKMA CME Dept – Tel: 2527 8452
8 (Tue)8:30 am–2:30 pm
HA – Our Lady of Maryknoll Hospital co-joint with American Heart Association
Basic Life Support for Health Care Provider (Fee: HK$400)Resuscitation Training Site, 1st Floor, OPD Block, Our Lady of Maryknoll Hospital, 118 Shatin Pass Road, Wong Tai SinMs Nerissa Law / Mr. Edward Chow – Tel: 2354 2248
➌
8 (Tue)2:30–5:45 pm
HK College of Psychiatrists
Central Academic Course Module E – Case Conference V or Video Demonstration; Lecture 19; Case Conference VI or Video DemonstrationConference Room, 1/F, Block, CPHMs. Laura Wong – Tel: 2636 7754
➌
8 (Tue)3:00–5:30 pm
HK College of Psychiatrists
1) ECT 2) Psychiatric Formulation and management planLecture Theatre, G073-074, Block D, CPHMs. Jennifer Mo – Tel: 2456 7152
➌
8 (Tue)3:00–5:30 pm
HK College of Psychiatrists
Central Academic Course: Module C – Lecture 15 to Lecture 16UCHMs. Connie Lo – Tel: 2959 8020
➌
8 (Tue)6:00–9:00 pm
Hong Kong Medical Association Medical Protection Society
Mastering Your RiskHKMA Central PremisesHKMA CME Dept – Tel: 2527 8452
C
M
Y
CM
MY
CY
CMY
K
HalfPage-PI-out.pdf 11/27/08 6:42:13 PM

CME CALENDAR
27www.hkmacme.org HKMA August 2009
9 (Wed)8:30–9:30 am
Union Hospital
Mortality and Morbidity MeetingTraining Rm, 8/F MIC, Union Hospital, 18 Fu Kin Street, Tai Wai, Shatin, NTMs. Yonnie Chung – Tel: 2608 3312
➊
9 (Wed)2:00–4:00 pm
HA-KLN East Cluster HA-UCH-Dept of Obstetrics & Gynaecology HA-TKOH-Dept of Obstetrics & Gynaecology
Postgraduate Seminar of Department O&G, Kowloon East Cluster (UCH / TKOH)Conference Room, Hospital Library, 1/F, Block H, UCHTel: 3513 4851
➋
9 (Wed)6:00–9:00 pm
Hong Kong Medical Association Medical Protection Society
Mastering Your RiskHKMA Central PremisesHKMA CME Dept – Tel: 2527 8452
10 (Thu)1:15–3:30 pm
HKMA-Tin Shui Wai North Community Network HK Alzheimer’s Disease Assn Lundbeck Institute Hong Kong
Certificate Course in Treating Alzheimer’s Disease in Community:1) Drug Targeting in Alzheimer’s Disease:
From Bench to Office2) Case-Based Discussion on the Application of
Memantine and CHEIs to Achieve Clinical ResponseBallroom C&D, Harbour Plaza Resort City, 18 Tin Yan Road, Tin Shui Wai, NTMs. Jaclyin Lee – Tel: 2877 1106
10 (Thu)8:00–10:00 am
HK Sanatorium & Hospital-Orthopaedic & Sports Medicine Ctr
Orthopaedic Clinical MeetingHong Kong Sanatorium & HospitalMs. Irene Shek – Tel: 2835 7890
➋
10 & 11 (Thu & Fri)8:30 am–5:30 pm
HA – Caritas Medical Centre
American Heart Association Advanced Cardiovascular Life Support Provider Course (Fee: HK$1,500 )Resuscitation Training Centre, Caritas Medical Centre (CMCRTC) Rm 303 Wai Oi Block, 111 Wing Hong Street, Shumshuipo, KowloonMs Irene Shiu – Tel: 3408 7444
➓
10 (Thu)2:00–4:00 pm
Hong Kong Medical Association Hong Kong Sanatorium & HospitalHKMA Structured CME Programme with HKS&H Session 9: New Trends in Management of Vitreo-Retinal- Macular Diseases – From Diagnosis to TreatmentThe HKMA Dr. Li Shu Pui Professional Education Centre, 2/F, Chinese Club Building, 21-22 Connaught Road Central, Hong Kong HKMA CME Dept – Tel: 2527 8452
➊
10 (Thu)6:00–9:00 pm
Hong Kong Medical Association Medical Protection SocietyMastering Your RiskHKMA Central PremisesHKMA CME Dept – Tel: 2527 8452
11 (Fri)10:00 am–12:00 pm
HKU-Dept of MicrobiologyInfectious Disease Rounds for Year 2009Conference Room, Room 405, Clinical Pathology Building, Queen Mary Hospital, 102 Pokfulam Road, Hong KongMs. Karis Larm – Tel: 2855 3243
➋
11 (Fri)1:00–2:00 pm
HA-TMH-Dept of Obstetrics & GynaecologyVaccination in PregnancyAB1038, 1/F, Main Block, Tuen Mun HospitalMs. Angela Cheung – Tel: 2468 5404
➊
11 (Fri)1:00–3:00 pm
HKDU-Hong Kong East Study Group
Asthma Management – New Concepts and ApproachesCheers Restaurant - Tao Heung 88, Heng Fa Chuen Comm Block, Chai Wan, HKTel: 2388 2728
➊
11 (Fri)6:00–9:00 pm
Hong Kong Medical Association Medical Protection Society
Mastering Your RiskHKMA Central PremisesHKMA CME Dept – Tel: 2527 8452
11–13 (Fri–Sun)
HKU-Dept of SurgeryAdvanced Trauma Life Support (ATLS) Student CourseSkills Development Centre, Department of Surgery, Li Ka Shing Faculty of Medicine, University of Hong Kong Medical Centre, Queen Mary Hospital, Pokfulam Road, HKProgram Manager – Tel: 2855 4885
➓
12 (Sat)9:00 am–12:00 pm
Hong Kong Medical Association Medical Protection Society
Mastering Your RiskHKMA Central PremisesHKMA CME Dept – Tel: 2527 8452
12 (Sat)2:00–5:00 pm
Hong Kong Medical Association Medical Protection Society
Mastering Your RiskHKMA Central PremisesHKMA CME Dept – Tel: 2527 8452
12 (Sat)2:30–5:00 pm
HK Paediatric Society / HK Paediatrics Nurse Assn HK College of PaediatriciansUpdate Series on Child Health 20091) Common Paediatric Orthopaedic Problems2) Common Paediatric ENT ProblemsLecture Theatre, M/F, Hospital Authority Building, 147B Argyle Street, KLNTel: 2388 2728
➌
13 (Sun)2:00–5:00 pm
Hong Kong Medical Association CUHK-Dept of Community & Family Medicine
HKMA Certificate Course on Family Medicine 20091) The Lonely Family Doctor: Access to Information,
Resources and Colleagues2) E-medical RecordLecture Theatre, G/F, Block M, QEHHKMA CME Dept – Tel: 2861 1979HKMA Member: $50 • Non-HKMA Member: $80
➌
14 (Mon)12:00–1:00 pm
HKU-Dept of MedicineHKW Geriatric Grand RoundC9, TWHMs. Joanne Hui – Tel: 2855 3315
➊
14 (Mon)1:00–2:00 pm
HKU-Dept of MedicineHKW Geriatric Academic MeetingC9, TWHMs. Joanne Hui – Tel: 2855 3315
➊
15 (Tue)2:30–5:45 pm
HK College of Psychiatrists
Central Academic Course Module E – Lecture 20; Lecture 21; Case Conference VII or Video DemonstrationConference Room, 7/F, 7AB, SHMs. Laura Wong – Tel: 2636 7754
➌
15 (Tue)3:00–5:30 pm
HK College of PsychiatristsCentral Academic Course: Module C – Lecture 17 to Lecture 18UCHMs. Connie Lo – Tel: 2959 8020
➌
15 (Tue)3:00–5:30 pm
HK College of Psychiatrists
1) Clinical psychopharmacology: anxiolytic, mood stabilizers, and others
2) Psychiatric emergenciesLecture Theatre, G073-074, Block D, CPHMs. Jennifer Mo – Tel: 2456 7152
➌
15 (Tue)6:00–9:00 pm
Hong Kong Medical Association Medical Protection SocietyMastering Your RiskHKMA Central PremisesHKMA CME Dept – Tel: 2527 8452