Thiopurines have no role in the management of Pediatric IBD Robert N. Baldassano, MD Colman...
24
Thiopurines have no role in the management of Pediatric IBD Robert N. Baldassano, MD Colman Professor of Pediatrics University of Pennsylvania, Perelman School of Medicine Director, Center for Pediatric IBD The Children's Hospital of Philadelphia
-
Upload
suzan-maxwell -
Category
Documents
-
view
216 -
download
0
Transcript of Thiopurines have no role in the management of Pediatric IBD Robert N. Baldassano, MD Colman...
Thiopurines have no role in the management of Pediatric IBD
Robert N. Baldassano, MD
Colman Professor of PediatricsUniversity of Pennsylvania, Perelman School of Medicine
Director, Center for Pediatric IBDThe Children's Hospital of Philadelphia
Thiopurines have a limited role in the management of Pediatric IBD
Robert N. Baldassano, MD
Colman Professor of PediatricsUniversity of Pennsylvania, Perelman School of Medicine
Director, Center for Pediatric IBDThe Children's Hospital of Philadelphia

I have the following financial relationships to disclose
Products or services produced by this company are relevant to my presentation
• Janssen Pharmaceuticals • Takeda Pharmaceuticals• AbbVie, Inc.• Avaxia Biologics, Inc.
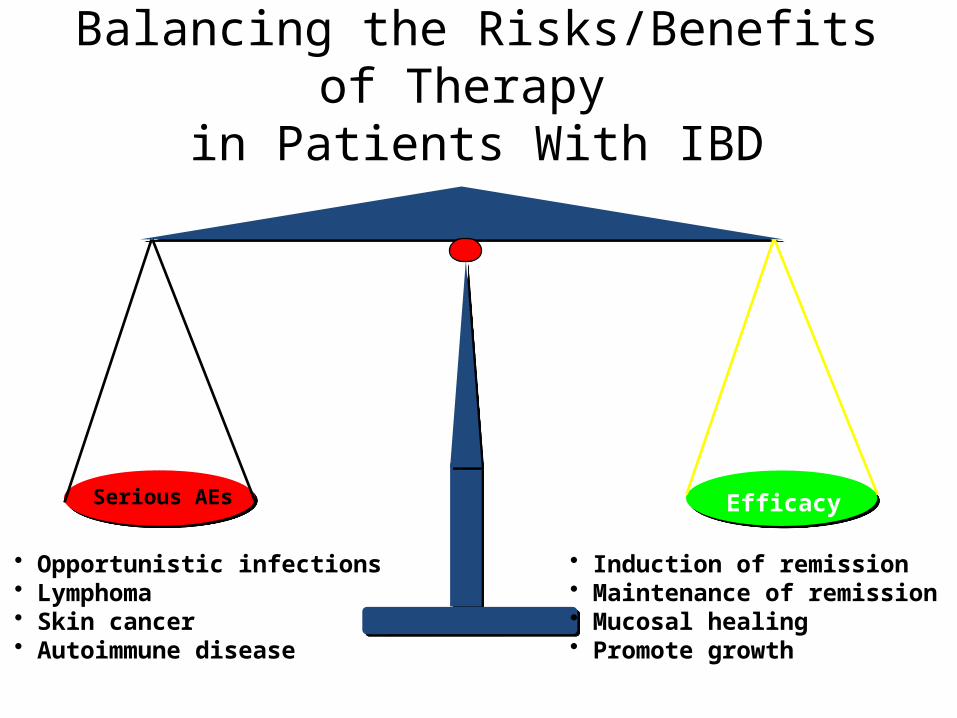
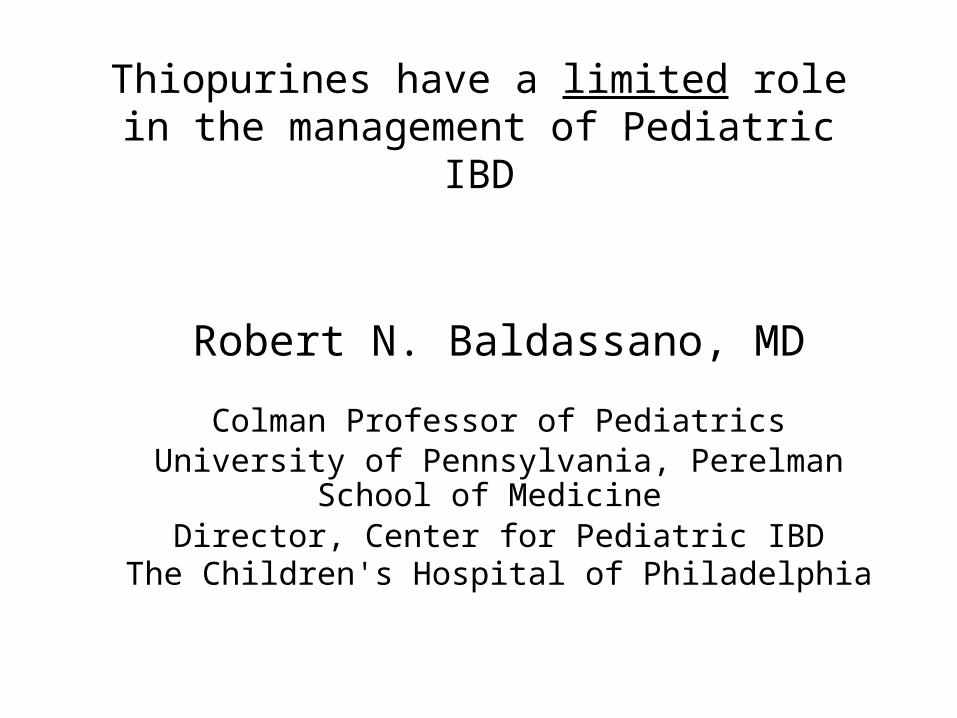
Balancing the Risks/Benefits of Therapy in Patients With IBD
Serious AEs Efficacy
• Opportunistic infections• Lymphoma• Skin cancer• Autoimmune disease
• Induction of remission• Maintenance of remission• Mucosal healing• Promote growth
Questions you need to address before treating a patient:
• What are the risks of serious infection with IM and anti-TNFα therapy?
• What is the risk of malignancy with IM alone?ThiopurinesMethotrexate
• What is the risk of malignancy with anti-TNFα alone?• What is the risk of combination therapy with IM and anti-
TNFα?With thiopurineWith methotrexate
• Can we mitigate these risks?
Risks are important to patients – even small risk!!

FEAR!
It is all about cancer.
Courtesy of J. Hyams
Is There Risk of Malignancy With Thiopurines?
• Azathioprine is known to be a human carcinogen based on sufficient evidence of carcinogenicity from studies in humans.
• First listed in the Fourth Annual Report on Carcinogens (1985)
• Initial evidence from transplantation but over time with chronic inflammatory disorders
Report on Carcinogens, Twelfth Edition (2011) http://ntp.niehs.nih.gov/go/roc12

Multiple Mechanisms of Carcinogenesis With Thiopurines
• DNA damage• Decreased immunosurveillance
– TP are cytotoxic for NK and cytotoxic T cells• restrict proliferation of EBV infected and immortalized B cells• Emergence of oncogenic viruses (EBV)
• Taking 6MP/AZA results in 6-TG accumulating in cellular DNA in skin– 6-TG has an absorption peak at 342 nm
• ultraviolet radiation (320-400 nm)– Results in a significant absorption of ultraviolet radiation
leading to DNA-damageKarran and Attard. Nat Rev Cancer 2008;8:24, Allan and Travis, Nat Rev Cancer 2005;5:943
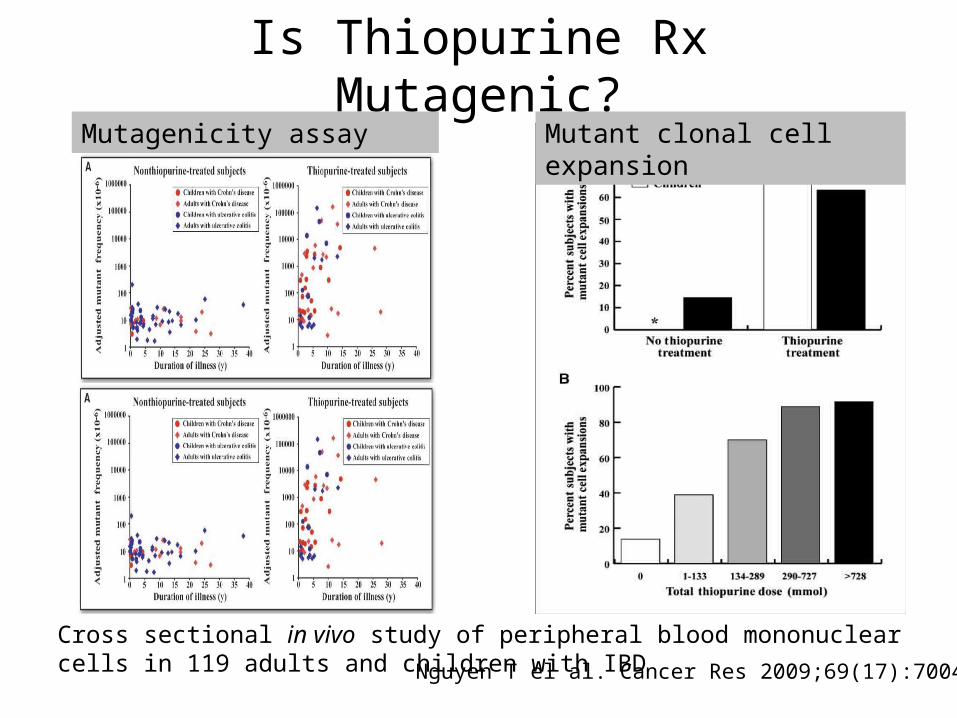
Is Thiopurine Rx Mutagenic?
Cross sectional in vivo study of peripheral blood mononuclear cells in 119 adults and children with IBD
Mutagenicity assay Mutant clonal cell expansion
Nguyen T el al. Cancer Res 2009;69(17):7004-12
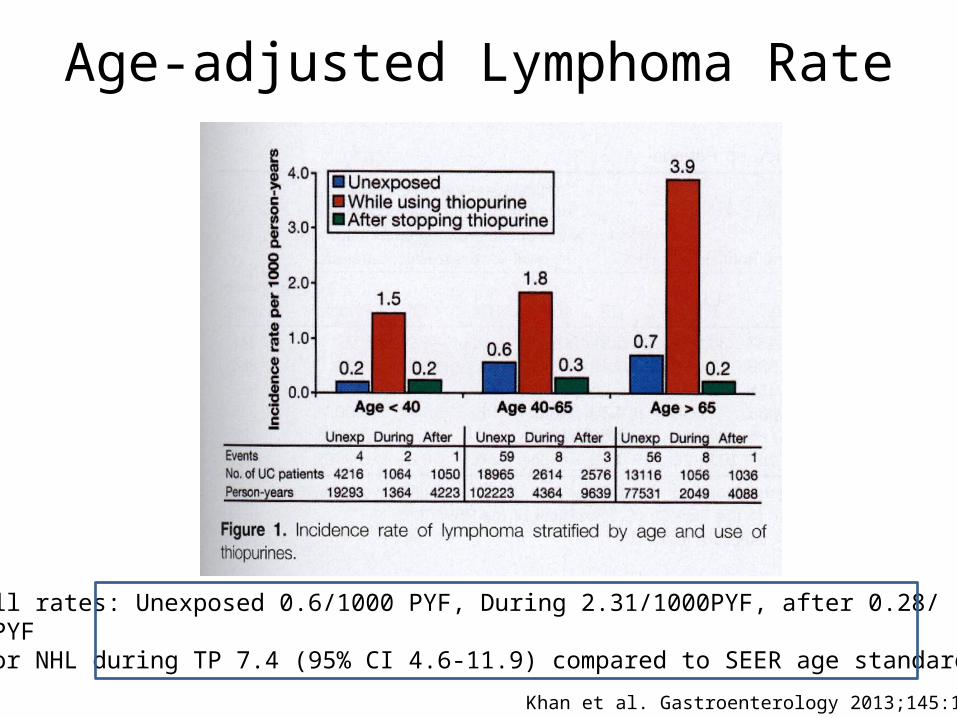
Age-adjusted Lymphoma Rate
Khan et al. Gastroenterology 2013;145:1007
Overall rates: Unexposed 0.6/1000 PYF, During 2.31/1000PYF, after 0.28/1000 PYFSIR for NHL during TP 7.4 (95% CI 4.6-11.9) compared to SEER age standardized data
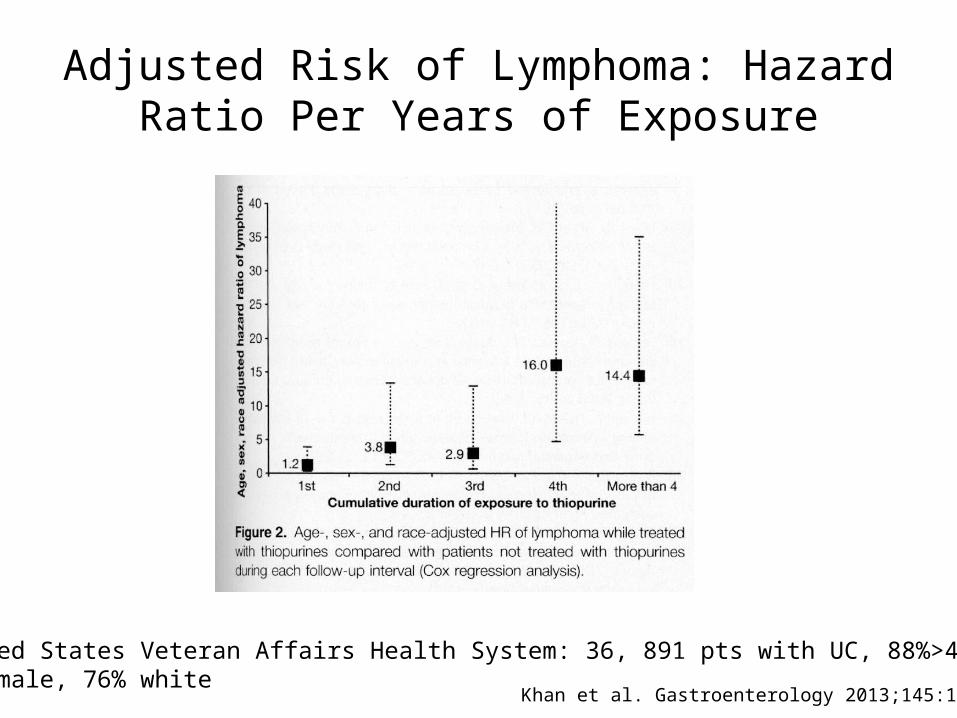
Adjusted Risk of Lymphoma: Hazard Ratio Per Years of Exposure
Khan et al. Gastroenterology 2013;145:1007
United States Veteran Affairs Health System: 36, 891 pts with UC, 88%>40yr,93% male, 76% white

Non-melanoma Skin Cancer: CESAME French National Cohort
Peyrin-Biroulet et al. Gastroenterology 2011;141:1621
YearlyIncidencePer1,000Pt-years
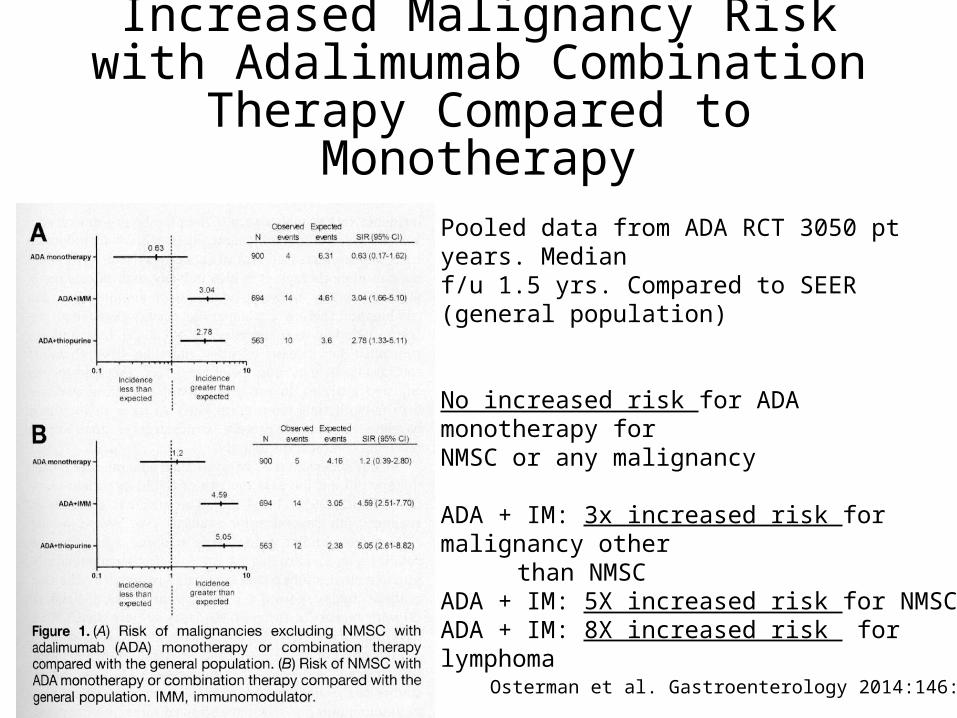
Increased Malignancy Risk with Adalimumab Combination Therapy
Compared to Monotherapy
Pooled data from ADA RCT 3050 pt years. Medianf/u 1.5 yrs. Compared to SEER (general population)
No increased risk for ADA monotherapy forNMSC or any malignancy
ADA + IM: 3x increased risk for malignancy other than NMSC
ADA + IM: 5X increased risk for NMSCADA + IM: 8X increased risk for lymphoma
Osterman et al. Gastroenterology 2014:146:941
Hepatosplenic T Cell Lymphoma: The 900 Pound Gorilla in the Room That Changed
Everything for Pediatricians
Courtesy of J. Hyams

Hepatosplenic T Cell Lymphomas
• Most common associations– Male, 10-35 y of age (69.5%)– Hepatosplenomegaly– Cytopenia– Elevated aminotransferases– No adenopathy– Symptoms (fever, weight loss, night sweats)
• Aggressive course, median survival 16 months, almost universally fatal
Belhadj K, et al. Blood. 2003;102:4261–4269.

Incidence of HSTCL• SEER data: Non-Hodgkin’s lymphoma incidence
10-19 yrs: 20/1,000,000 (1:50,000)20-29 yrs: 30/1,000,000 (1:33,000)
• Peripheral T cell lymphomas: 10-15% of NHL• HSTCL: 5% of peripheral T cell lymphomas or <1% of
all NHL• Therefore, incidence of HSTCL 1:5,000,000• In U.S. 50,000 to 100,000 children with IBD. One
would therefore expect one case every 50-100 years as background incidence
Courtesy of J. Hyams

Hepatosplenic T-Cell Lymphoma in IBD
Risk Estimates for HSTCL in IBD
All patients on thiopurine only Rx 1:45,000
All patients on infliximab ± thiopurine 1:21,947
All males <35 yrs on thiopurine only Rx 1:7404
All males <35 yrs on thiopurine + anti-TNF 1:3534
Kotlyar D et al. Clin Gastroenterol Hepatol 2011;9:36-41
The risk appears to be particularly increased in patients receiving thiopurines, either as monotherapy or in combination with anti-TNF agents. IBD patients receiving longterm thiopurine therapy are possibly at even greater risk.

Conclusions
• Thiopurine use is associated with increased cancer risk.
• Risk of cancer with mtx appears to be small to negligible, but more data are needed
• Anti-TNF therapy alone does not appear to increase cancer risk
• Anti-TNF + thiopurine is associated with increased cancer risk, though not clear what amount is from thiopurine alone. Particularly problematic in young males

P=.007Markowitz J et al. Gastroenterology. 2000;119:895.
6-MP: Maintenance Therapy in Children With Crohn’s Disease
0 100 200 300 400 500 6000.00
0.25
0.50
0.75
1.00
6-MPControl
Remission Duration (days)
Frac
tiona
l Su
rviv
al
n=55
Modified Harvey Bradshaw (Not a validated disease activity index)
Endpoint ?????
Remission???No difference in linear growth
Sample size???Selection biasWide confidence interval
If it is too good to be true!Predicting the Crohn’s Disease Activity Index From the Harvey-Bradshaw Index (HBI)
Conclusion: ” HBI is not recommended for prospective trials in Crohn’s disease” Best WR IBD 2006;12;4:304-310
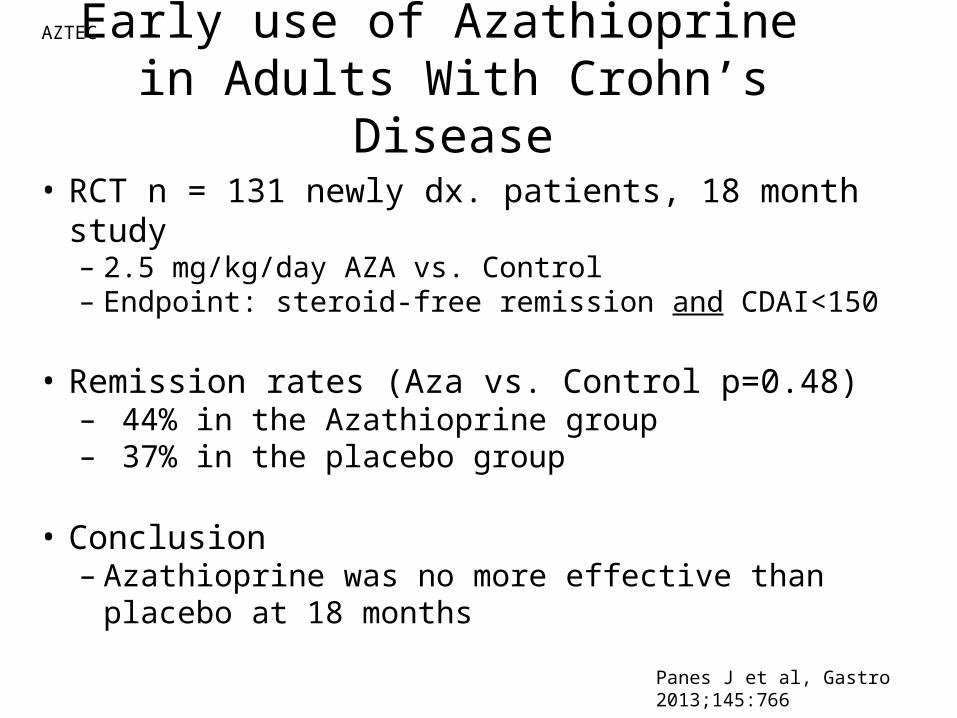
Early use of Azathioprine in Adults With Crohn’s Disease
• RCT n = 131 newly dx. patients, 18 month study– 2.5 mg/kg/day AZA vs. Control– Endpoint: steroid-free remission and CDAI<150
• Remission rates (Aza vs. Control p=0.48)– 44% in the Azathioprine group– 37% in the placebo group
• Conclusion– Azathioprine was no more effective than placebo at 18
monthsPanes J et al, Gastro 2013;145:766
AZTEC
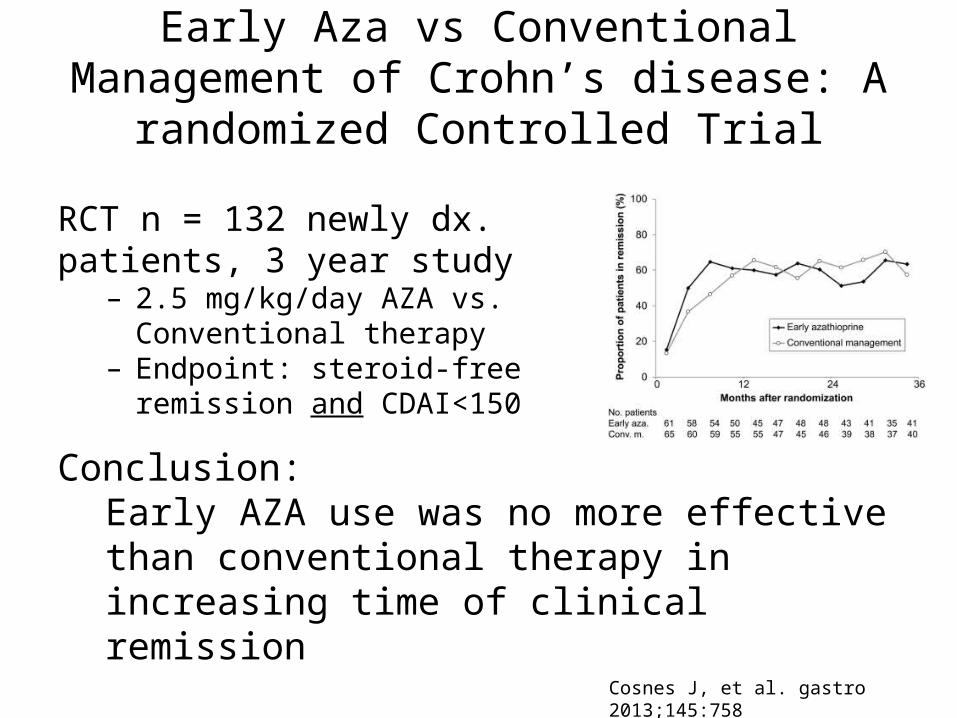
Early Aza vs Conventional Management of Crohn’s disease: A randomized Controlled Trial
RCT n = 132 newly dx. patients, 3 year study
– 2.5 mg/kg/day AZA vs. Conventional therapy
– Endpoint: steroid-free remission and CDAI<150
Conclusion:Early AZA use was no more effective than conventional therapy in increasing time of clinical remission
Cosnes J, et al. gastro 2013;145:758
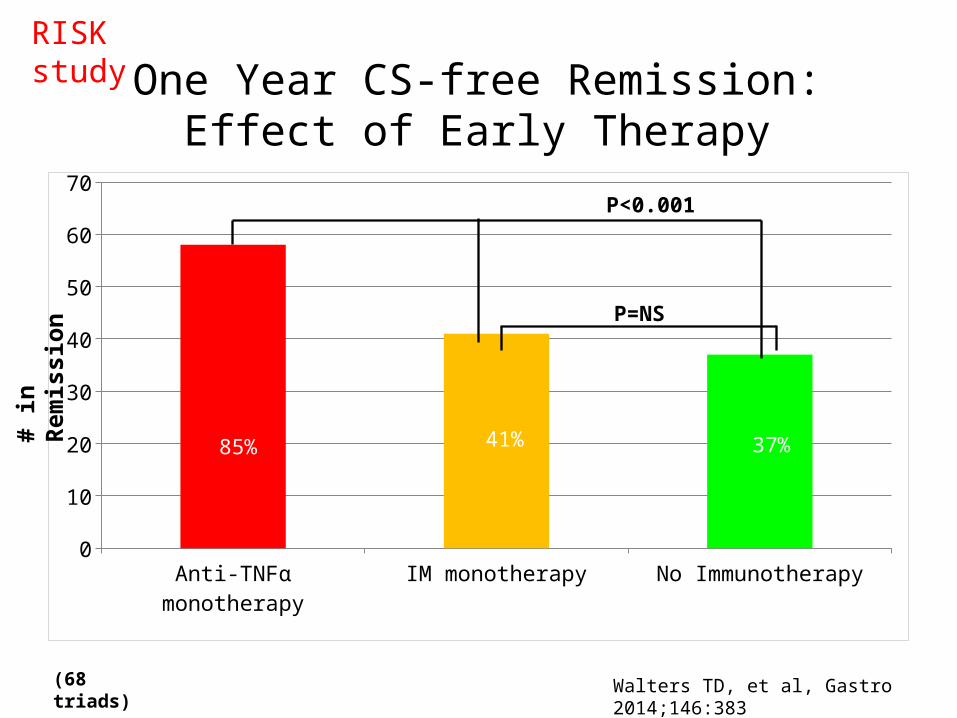
One Year CS-free Remission:Effect of Early Therapy
Anti-TNFα monotherapy IM monotherapy No Immunotherapy0
10
20
30
40
50
60
70
RISK study
85% 41% 37%
P<0.001
P=NS
# in
Rem
issi
on
(68 triads) Walters TD, et al, Gastro 2014;146:383
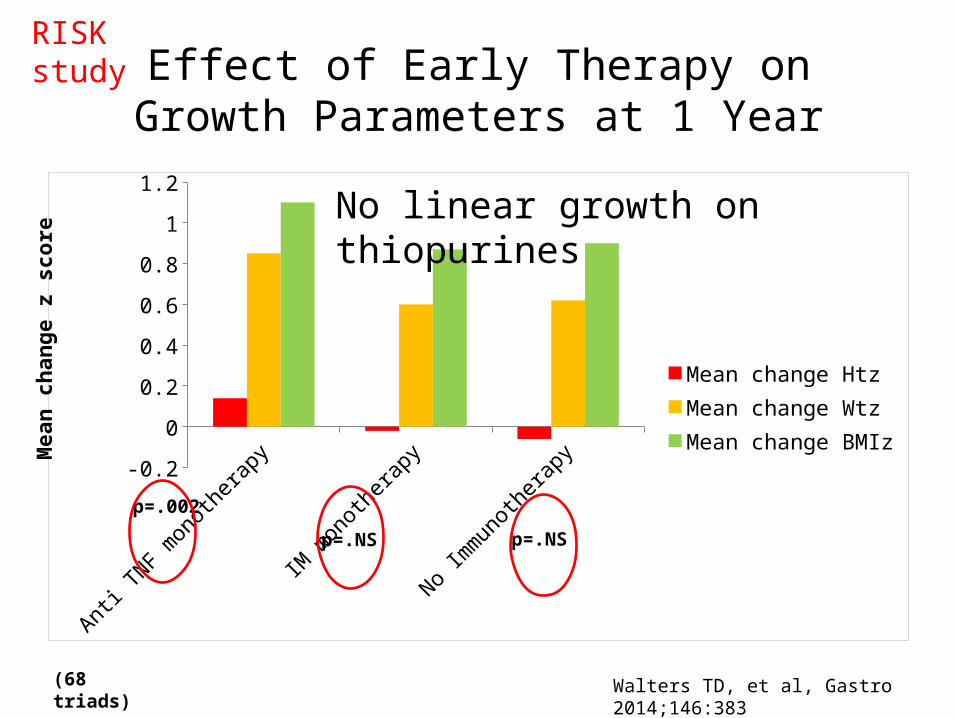
Effect of Early Therapy onGrowth Parameters at 1 Year
-0.2
0
0.2
0.4
0.6
0.8
1
1.2
Mean change HtzMean change WtzMean change BMIz
RISK study
p=.002
p=.NS p=.NS
Mea
n ch
ange
z s
core
(68 triads) Walters TD, et al, Gastro 2014;146:383
No linear growth on thiopurines
Risk Mitigation Strategy
• Consider stopping thiopurines when clinically possible Reduced risk after time off therapy
• Consider drug holiday; change to mtx• Yearly skin checks• Avoid ionizing radiation• Consider primary anti-TNF therapy in moderate to
severe IBD prior to thiopurine*; role of combination with mtx to increase durability needs further data
• Potential role of emerging drugs in decreasing cancer risk from therapy (e.g., anti-adhesion molecule therapy)
*off label useCourtesy of J. Hyams