Therapeutic Results of a Direct Aspiration First Pass ...
8
58 58 DOI: 10.5797/jnet.oa.2018-0041 Therapeutic Results of a Direct Aspiration First Pass Technique Using the Penumbra 4MAX Aspiration Catheter for Middle Cerebral Artery M2 Occlusion Takumi Asai, Kazunori Shintai, Takahiro Oyama, Mizuka Ikezawa, Takuma Miyazawa, Kinya Yokoyama, Tomomi Kawaguchi, Masasuke Ohno, Noriyuki Susaki, Yasukazu Kajita, and Tatsuo Takahashi Objective: While the effectiveness of thrombectomy for anterior circulation proximal intracranial arterial occlusions has been established, there is no solid evidence concerning its therapeutic effect on acute ischemic stroke due to middle cerebral artery M2 occlusion. In this study, we evaluated the efficacy and safety of a direct aspiration first pass technique (ADAPT) using the Penumbra 4MAX aspiration catheters (4MAX; Medico’s Hirata Inc., Osaka, Japan) for M2 occlusion. Methods: Of the 17 patients with acute ischemic stroke who underwent thrombectomy for M2 occlusion between January 2016 and December 2017 at our institution, 12 patients in whom ADAPT using the 4MAX was performed as the first-line procedure were evaluated. The stent retriever (SR) was used concomitantly in patients in whom recanalization could not be achieved by ADAPT using the 4MAX only. The retrospective evaluation was performed according to effective recanalization (thrombolysis in cerebral infarction [TICI] scale 2b-3) and independence in daily activities (modified Rankin Scale [mRS] score 0-2 after 3 months) as the efficacy endpoints and symptomatic intracranial hemorrhage as a safety endpoint. Results: The median age of the 12 subjects was 77 (interquartile range [IQR] 69–80) years, 9 (75.0%) were males, and the median preprocedural National Institutes of Health Stroke Scale (NIHSS) score was 19.5 (IQR: 16–24.5). The 4MAX reached the clot in 11 (91.7%), and effective recanalization was obtained by ADAPT alone in 8 (66.7%). Effective recanalization was achieved in 11 (91.7%) at the end of all procedures, the outcome was favorable in 8 (66.7%), and no symptomatic intracranial hemorrhage was observed. Conclusion: In M2 occluded region, a high recanalization rate could be achieved by ADAPT using the 4MAX without causing symptomatic intracranial hemorrhage, and the results suggested high efficacy and safety of the technique. Keywords▶ M2 occlusion, Penumbra 4MAX reperfusion catheter, mechanical thrombectomy, stent retriever Introduction The efficacy of thrombectomy in acute ischemic stroke due to proximal large vessel occlusion in the anterior circulation have been demonstrated by several randomized controlled trials, and the treatment is now strongly recommended in guidelines. According to the meta-analysis by Highly Effec- tive Reperfusion evaluated in Multiple Endovascular Stroke trials (HERMES) Collaborators, endovascular treatment was effective in the internal carotid artery or horizontal segment (M1) of the middle cerebral artery, but its efficacy was simi- lar to that of medical treatment in the second segment (M2) of the middle cerebral artery. 1) In clinical situations, there are cases of occlusion of the M2 segment, which has a large per- fusion territory, similar in severity to M1 occlusion, and endo- vascular treatment is considered effective in some of them. Since the evidence concerning M2 occlusion has not been established, safe procedures must be performed, and reca- nalization must be achieved consistently, to further improve the results of endovascular treatment. However, endovascu- lar treatment of peripheral lesions is difficult because it requires delivery of the device to a more distal, and there is the risk of complications such as intracranial hemorrhage in Department of Neurosurgery, National Hospital Organization Nagoya Medical Center, Nagoya, Aichi, Japan Received: March 2, 2018; Accepted: August 27, 2018 Corresponding author: Takumi Asai. Department of Neurosurgery, National Hospital Organization Nagoya Medical Center, 4-1-1 Sannomaru, Naka-ku, Nagoya, Aichi 460-0001, Japan Email: [email protected] This work is licensed under a Creative Commons Attribution-NonCommercial- NoDerivatives International License. ©2019 The Japanese Society for Neuroendovascular Therapy Journal of Neuroendovascular Therapy Vol. 13, No. 2 (2019) Journal of Neuroendovascular Therapy 2019; 13: 58–65 Online October 11, 2018
Transcript of Therapeutic Results of a Direct Aspiration First Pass ...

5858
DOI: 10.5797/jnet.oa.2018-0041
Therapeutic Results of a Direct Aspiration First Pass Technique Using the Penumbra 4MAX Aspiration Catheter for Middle Cerebral Artery M2 Occlusion
Takumi Asai, Kazunori Shintai, Takahiro Oyama, Mizuka Ikezawa, Takuma Miyazawa, Kinya Yokoyama, Tomomi Kawaguchi, Masasuke Ohno, Noriyuki Susaki, Yasukazu Kajita, and Tatsuo Takahashi
Objective: While the effectiveness of thrombectomy for anterior circulation proximal intracranial arterial occlusions has been established, there is no solid evidence concerning its therapeutic effect on acute ischemic stroke due to middle cerebral artery M2 occlusion. In this study, we evaluated the efficacy and safety of a direct aspiration first pass technique (ADAPT) using the Penumbra 4MAX aspiration catheters (4MAX; Medico’s Hirata Inc., Osaka, Japan) for M2 occlusion.Methods: Of the 17 patients with acute ischemic stroke who underwent thrombectomy for M2 occlusion between January 2016 and December 2017 at our institution, 12 patients in whom ADAPT using the 4MAX was performed as the first-line procedure were evaluated. The stent retriever (SR) was used concomitantly in patients in whom recanalization could not be achieved by ADAPT using the 4MAX only. The retrospective evaluation was performed according to effective recanalization (thrombolysis in cerebral infarction [TICI] scale 2b-3) and independence in daily activities (modified Rankin Scale [mRS] score 0-2 after 3 months) as the efficacy endpoints and symptomatic intracranial hemorrhage as a safety endpoint.Results: The median age of the 12 subjects was 77 (interquartile range [IQR] 69–80) years, 9 (75.0%) were males, and the median preprocedural National Institutes of Health Stroke Scale (NIHSS) score was 19.5 (IQR: 16–24.5). The 4MAX reached the clot in 11 (91.7%), and effective recanalization was obtained by ADAPT alone in 8 (66.7%). Effective recanalization was achieved in 11 (91.7%) at the end of all procedures, the outcome was favorable in 8 (66.7%), and no symptomatic intracranial hemorrhage was observed.Conclusion: In M2 occluded region, a high recanalization rate could be achieved by ADAPT using the 4MAX without causing symptomatic intracranial hemorrhage, and the results suggested high efficacy and safety of the technique.
Keywords▶ �M2 occlusion, Penumbra 4MAX reperfusion catheter, mechanical thrombectomy, stent retriever
Introduction
The efficacy of thrombectomy in acute ischemic stroke due to proximal large vessel occlusion in the anterior circulation have been demonstrated by several randomized controlled trials, and the treatment is now strongly recommended in
guidelines. According to the meta-analysis by Highly Effec-tive Reperfusion evaluated in Multiple Endovascular Stroke trials (HERMES) Collaborators, endovascular treatment was effective in the internal carotid artery or horizontal segment (M1) of the middle cerebral artery, but its efficacy was simi-lar to that of medical treatment in the second segment (M2) of the middle cerebral artery.1) In clinical situations, there are cases of occlusion of the M2 segment, which has a large per-fusion territory, similar in severity to M1 occlusion, and endo-vascular treatment is considered effective in some of them. Since the evidence concerning M2 occlusion has not been established, safe procedures must be performed, and reca-nalization must be achieved consistently, to further improve the results of endovascular treatment. However, endovascu-lar treatment of peripheral lesions is difficult because it requires delivery of the device to a more distal, and there is the risk of complications such as intracranial hemorrhage in
Department of Neurosurgery, National Hospital Organization Nagoya Medical Center, Nagoya, Aichi, Japan
Received: March 2, 2018; Accepted: August 27, 2018Corresponding author: Takumi Asai. Department of Neurosurgery, National Hospital Organization Nagoya Medical Center, 4-1-1 Sannomaru, Naka-ku, Nagoya, Aichi 460-0001, JapanEmail: [email protected]
This work is licensed under a Creative Commons Attribution-NonCommercial- NoDerivatives International License.
©2019 The Japanese Society for Neuroendovascular Therapy
Journal of Neuroendovascular Therapy Vol. 13, No. 2 (2019)
Journal of Neuroendovascular Therapy 2019; 13: 58–65
Online October 11, 2018

59
Therapeutic Results of ADAPT Using Penumbra 4MAX for M2 Occlusion
thrombectomy procedures for small-diameter, vulnerable vessels. At our institution, we have performed a direct aspi-ration first pass technique (ADAPT) using the Penumbra 4MAX aspiration catheters (Medico’s Hirata Inc., Osaka, Japan) as the first-line treatment for occlusion of the M2 with a large perfusion territory2) since January 2016. In this study, the efficacy and safety of the procedure were evalu-ated retrospectively.
Materials and Methods
SubjectsOf the 17 patients with acute ischemic stroke who under-went thrombectomy for M2 occlusion between January 2016 and December 2017, 12 patients who received ADAPT using the 4MAX as the first-line treatment were selected as the subjects. Endovascular treatment of M2 occlusion was indicated for 1) patients with no indication for intravenous tissue plasminogen activator (IV-tPA) or those in whom M2 occlusion persisted on angiography and no alleviation of neu-rological symptoms was observed after IV-tPA, and 2) patients with the National Institutes of Health Stroke Scale (NIHSS) score was ≥5 and those with clinical-diffu-sion-weighted image (DWI) mismatch. Concerning the thrombectomy procedure, ADAPT using the 4MAX was attempted when the guiding catheter could be inserted to the internal carotid artery and when the surgeon judged that delivery of the Penumbra catheter to the site of occlusion would be possible from the tortuosity and diameter of the access route. ADAPT using the 5MAX ACE (Medico’s Hirata) was selected when the occluded M2 was thought to be a large trunk and similar size to the M1(3/17). If the guid-ing catheter could not be ascended to the internal carotid artery, or if the surgeon judged that the 4MAX would be dif-ficult to deliver to the lesion due to marked tortuosity, it was used as an intermediate catheter for stent retriever (SR; 2/17).
Thrombectomy procedureIn all patients, a 9 Fr OPTIMO guiding catheter (Tokai Medical Products, Aichi, Japan) was placed in the internal carotid artery ipsilateral to the occluded M2 by the femoral artery approach. As an inner microcatheter, the PX Slim 160 cm (Medico’s Hirata) or Rebar-18 153 cm (Medtronic, Minneapolis, MN, USA) was guided to the lesion using the ASAHI CHIKAI 14 200 cm microguidewire (Asahi Intecc Co., Ltd, Aichi, Japan), and the 4MAX was coaxially delivered to the site of occlusion. If the 4MAX could be brought into contact with the clot, the microcatheter was extracted, the 4MAX was connected to the Penumbra
MAX Pump, and aspiration was performed at the maxi-mum aspiration pressure for about 2 minutes. Then, the balloon of the OPTIMO was inflated, and continuing aspira-tion, the clot was retrieved by slowly withdrawing the 4MAX into the guiding catheter (ADAPT). If recanaliza-tion could not be achieved within three passes, or if clot retrieval was judged to be impossible due to misalignment of the axis of the catheter with the vessel, ADAPT was judged as the failure. In this case, the 4MAX was advanced to a point closest to the clot, the microcatheter was guided to distal of the clot, Solitaire 2 (Medtronic) or Trevo XP (Stryker, Kalamazoo, MI, USA) was deployed, and the clot was retrieved by withdrawing it into the 4MAX while applying an aspiration pressure.
EndpointsAs efficacy endpoints, a thrombolysis in cerebral infarction (TICI) scale score of 2b-3 was defined as effective recanal-ization, and a modified Rankin Scale (mRS) score of 0-2 after 3 months was defined as a favorable outcome. As a safety endpoint, symptomatic intracranial hemorrhage (intra-cranial hemorrhage showing exacerbation of NIHSS score by 4 or more points) was evaluated. In addition, the punc-ture to recanalization time and the number of attempts of ADAPT were also evaluated. In this article, continuous variables were presented as median values (interquartile range [IQR]). This study was carried out with approval by the Clinical Research Review Board of our institution.
Results
Table 1 shows the baseline characteristics of the 12 patients. The median age was 77 (69–80) years, 9 (75.0%) were males, and the preprocedural NIHSS score was 19.5 (16–24.5). The occluded vessel was a well-developed branch with a large per-fusion territory in all cases, and it was a large inferior trunk that perfused from the central artery to the angular artery ter-ritories in nine patients (75.0%). The lesion was located in the dominant hemisphere in 8 (66.7%), and included 2 (16.7%) with tandem occlusion of the cervical internal carotid artery and M2. The median preprocedural DWI-Alberta Stroke Pro-gram Early CT Score (DWI-ASPECTS) was 8 (7.5–9), and IV-tPA was performed in 7 (58.3%).
The therapeutic results are shown in Table 2. The 4MAX could be successfully guided to the site of occlusion in 11 (91.7%) of the 12 patients. In eight patients (66.7%) effec-tive recanalization could be achieved by ADAPT alone with a single attempt. The SR was used concomitantly in the remaining four patients (33.3%). Effective recanalization at
Journal of Neuroendovascular Therapy Vol. 13, No. 2 (2019)

60
Asai T, et al.
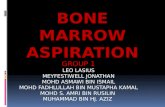
hyperintensity in the left temporal lobe (DWI-ASPECTS: 9) (Fig. 1A). On MRA, the left M2 inferior trunk was occluded. Since the symptoms were not alleviated even after IV-tPA, endovascular treatment was performed (onset to puncture time: 231 minutes). Occlusion of the left M2 inferior trunk was confirmed by preprocedural angiography (Fig. 1B and 1C). The occluded vessel had a large perfusion territory including the central artery to the angular artery. The 4MAX was guided to the site of occlusion using PX Slim 160 cm and ASAHI CHIKAI 200 cm, and thrombectomy was performed by ADAPT (Fig. 1D). Small clots were retrieved (Fig. 1E), and complete recanalization (TICI 3) was achieved (Fig. 1F). The puncture to recanalization time was 22 minutes and no postprocedural SAH was observed. Her symptoms were improved rapidly to an NIHSS score of 0 on the day after treatment, no clear infarcted region was observed on DWI-MRI (Fig. 1G), and the outcome was favorable (mRS: 0).
Case 2A 66-year-old man had a history of cardiogenic stroke of the left middle cerebral artery territory due to atrial fibrilla-tion. He was admitted with a recurrent stroke of the left
the end of all procedures could be achieved in 11 patients (91.7%) with a mean of 1.5 passes. The median puncture to recanalization time was 45 (22–64) minutes. The mRS score after 90 days was 0-2 in eight patients (66.7%). Of the nine patients in whom the premorbid mRS score was 0-2, the outcome was favorable in eight patients (88.9%). No patient developed symptomatic intracranial hemor-rhage. While subarachnoid hemorrhage (SAH) was noted immediately after the procedure in four (33.3%), they all remained asymptomatic and showed no enlargement.
In the eight patients in whom recanalization could be achieved by ADAPT alone, the time to recanalization was 28.5 (21–45) minutes, the outcome was favorable in 87.5%, and symptomatic intracranial hemorrhage or post-procedural SAH was observed in 0%. If the occluded ves-sel was the superior trunk, recanalization could not be achieved by ADAPT alone, and the SR was used concom-itantly in all such patients. However, recanalization could be achieved by ADAPT alone in 88.9% of patients with the inferior trunk occlusion.
Representative cases
Case 1A 75-year-old woman presented with a complaint of right hemiplegia and total aphasia and the preprocedural NIHSS score was 16. MRI-DWI on admission showed slight
Table 1 Baseline characteristics
Variable (N = 12)Demographic characteristics Age 77 (69–80) Male (%) 9 (75.0) Premorbid mRS ≥3 (%) 3 (25.0)Clinical charasteristics Baseline NIHSS 19.5 (16–24.5)Imaging characteristics DWI-ASPECTS 8 (7.5–9)Site of occlusion (%) M2 superior trunk 3 (25.0) M2 inferior trunk 9 (75.0) Dominant side 8 (66.7) Ipsilateral ICA occlusion 2 (16.7)Cause of stroke (%) Cardiogenic 9 (75.0) Atherosclerotic 3 (25.0)Medical history (%) Previous stroke 2 (16.7) Hypertension 10 (83.3) Diabetes 4 (33.3) Atrial fibrillation 6 (50.0) Smoking 7 (58.3) Intravenous t-PA 7 (58.3)
DWI-ASPECTS: diffusion-weighted image-Alberta Stroke Program Early CT Score; ICA: internal carotid artery; mRS: modified Rankin Scale; NIHSS: National Institutes of Health Stroke Scale; t-PA: tissue plasminogen activator
Table 2 Procedural and clinical results
Procedural results Successful contact to clot (%) 11 (91.6) Number of ADAPT procedure (%) 1 10 (83.3) 2 1 (8.3) 3 1 (8.3) Reperfusion after ADAPT with 4MAX (%) TICI 2b-3 8 (66.7) TICI 2c-3 7 (58.3) TICI 3 4 (33.3) Reperfusion after all procedure (%) TICI 2b-3 11 (91.7) TICI 2c-3 9 (75.0) TICI 3 6 (50.0) Use of stent retriever (%) 4 (33.3) Trevo XP 3 (25.0) Solitaire 1 (8.3) Number of stent passes (%) 1 2 (16.7) 2 2 (16.7) Puncture to Reperfusion 45 (22–64)Clinical results mRS 0-2 (90d) (%) 8 (66.7) NIHSS (24h) 9.5 (3–16) NIHSS (14d) 3.5 (1.5–9) Symptomatic ICH (%) 0 (0) Any SAH (%) 4 (33.3) Any ICH (%) 6 (50.0)
ADAPT: a direct aspiration first pass technique; ICH: intracranial hemorrhage; mRS: modified Rankin Scale; NIHSS: National Institutes of Health Stroke Scale; SAH: subarachnoid hemorrhage; TICI: thrombolysis in cerebral infarction; 4MAX: Penumbra 4MAX aspiration catheters, Medico’s Hirata Inc., Osaka, Japan; Trevo XP, Stryker, Kalamazoo, MI, USA; Solitaire, Medtronic, Minneapolis, MN, USA
Journal of Neuroendovascular Therapy Vol. 13, No. 2 (2019)

61
Therapeutic Results of ADAPT Using Penumbra 4MAX for M2 Occlusion
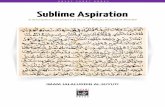
middle cerebral artery territory, and anticoagulant therapy was initiated, but the therapy was discontinued due to the occurrence of hemorrhagic infarction. The patient exhibited disturbance of consciousness and left hemiplegia (NIHSS: 31) early in the morning 2 days after the discontinuation, and MRA revealed occlusion of the right M2 inferior trunk. However, no clear hyperintensity was noted on MRI-DWI (DWI-ASPECTS: 11) because MRI was performed shortly after the onset. His premorbid mRS score was 4 due to con-tralateral stroke; however, endovascular treatment was attempted because of the in-hospital case with a contraindi-cation of IV-tPA. The time from the last confirmation of being well to puncture was 201 minutes. On initial angiog-raphy, the right M2 inferior trunk was occluded. Although ADAPT using the Penumbra 4MAX was performed three times, only a small amount of clots were retrieved, and recanalization was not achieved (Fig. 2A). After the 4MAX was guided to a position proximal to the site of occlusion, the PX Slim was advanced to distal to the clot (Fig. 2B). The Solitaire 2 4 mm × 15 mm was deployed, and the PX Slim was carefully extracted (Fig. 2C). When the Solitaire
2 was drawn into the 4MAX with aspiration and recovered into the OPTIMO, clots were retrieved in the 4MAX and Solitaire (Fig. 2D). Final angiography confirmed recanali-zation of the occluded M2 (TICI 3, puncture to recanaliza-tion time: 56 minutes), but slight contrast extravasation was observed in the subarachnoid space distal to the site where the Solitaire was deployed (Fig. 2E). Although CT imme-diately after the procedure showed a small area of contrast extravasation in the subarachnoid space (Fig. 2F), it disap-peared on the next day by controlling the systolic blood pressure to ≤140 mmHg (Fig. 2G). His left hemiplegia and disturbance of consciousness were relieved, and the condi-tion improved nearly to the level before the episode with an NIHSS score of 16 after 2 weeks (mRS: 4).
Discussion
Natural history of M2 occlusion/results of intravenous thrombolysis with t-PAThere have been several reports about the natural history of acute ischemic stroke by M2 occlusion. According to
Fig. 1 Case 1 (A) Slight hyperintensity (dotted circle) was noted in the left temporal lobe on preprocedural MRI-DWI. (B) Cerebral angio-gram: frontal view (C) and lateral view; occlusion was observed in the left M2 inferior trunk (arrow). (D) Lateral view: the penumbra 4MAX was guided to the site of occlusion. (E) Clots retrieved in the 4MAX by aspiration. (F) The site of occlusion could be completely recanalized (arrow). (G) On the day after the procedure, no clear hyperintensity was noted on MRI-DWI. DWI: diffusion-weighted image; 4MAX: Penumbra 4MAX aspiration catheters, Medico’s Hirata Inc., Osaka, Japan
A B C
D E F G
Journal of Neuroendovascular Therapy Vol. 13, No. 2 (2019)

62
Asai T, et al.
recanalization rate was 62.5% 6 hours after administration and 81.3% after 24 hours, and that the mRS score was 0-2 after 3 months in 81.3% of the patients. However, these patients included many mild cases as suggested by a median NIHSS score of 11 (range: 5–21). In addition, according to Kimura et al.,6) the occluded M2 was completely recana-lized 1 hour after IV-tPA in 6/37 (16.2%) and partially recanalized in 9/37 (24.3%), and as recanalization could not be achieved in a short period in about 60.0% of the patients. Thrombectomy can achieve recanalization in a short period and may be effective in M2 occlusion cases with severe symptoms that lack collateral blood flow.
Comparison between thrombectomy and medical treatmentSubgroup analysis concerning M2 occlusion was con-ducted in the meta-analysis by HERMES Collaborators.1) The percentage of those with a favorable outcome with an mRS
Lima et al.,3) who studied 48 patients with M2 occlusion (mean age: 69.5 ± 6.1 years, median NIHSS score: 7), the outcome was favorable with an mRS score 0-2 after 6 months in 54.2% of the patients. The favorable outcome was achieved in 80.8% of patients with baseline NIHSS score ≤9 (26 patients), whereas it was achieved only in 22.7% of patients with baseline NIHSS ≥10 (22 patients). In addition, Rai et al.4) proposed baseline NIHSS score of 9 as a cutoff value for an unfavorable outcome, reporting that the outcome was favorable in 22.6% of patients with NIHSS score ≥9 but in 78.4% of patients with NHISS score <9 (odds ratio [OR]: 0.08, 95.0% confidence interval [CI]: 0.03–0.21, p <0.0001). From these reports, thrombec-tomy is considered a reasonable option for those with a high NIHSS score because of the poor natural history.
Regarding IV-tPA for M2 occlusion, Hirano et al. evalu-ated 16 patients in the J-ACTII study5) and reported that the thrombolysis in myocardial infarction (TIMI) grade 2-3
Fig. 2 Case 2 (A) Angiogram: lateral view, occlusion persisted as a clot (arrow) could not be removed by ADAPT using the Penumbra 4MAX. The 4MAX (arrowhead) was guided to the proximal side of the clot. (B) The PX SLIM was advanced from the 4MAX (arrowhead) and guided to distal to the clot (arrow). (C) When the Solitaire 2 4 mm × 15 mm was deployed, the clot were captured (arrow). (D) Clots retrieved by the Solitaire and 4MAX. (E) The occluded part was completely recanalized (arrow), but contrast extravasation was observed in a limited area (arrowhead). (F) Immediately after the procedure, plain CT SAH was noted in the right temporal region (arrow) (hem-orrhage in the left hemisphere was hemorrhagic infarction that was present from before the procedure). (G) On the day after the proce-dure, plain CT SAH was gradually obliterated. ADAPT: a direct aspiration first pass technique; SAH: subarachnoid hemorrhage; 4MAX: Penumbra 4MAX aspiration catheters, Medico’s Hirata Inc., Osaka, Japan; Solitaire 2: Medtronic, Minneapolis, MN, USA; PX SLIM: Penumbra, Inc., Alameda, CA, USA
A B C D
E F G
Journal of Neuroendovascular Therapy Vol. 13, No. 2 (2019)

63
Therapeutic Results of ADAPT Using Penumbra 4MAX for M2 Occlusion
the results of thrombectomy for M2 occlusive lesions pub-lished before July 2017, the effective recanalization rate by all treatments was 81.0%, rate of mRS 0-2 after 3 months was 59.0%, and symptomatic intracranial hemorrhage rate was 10.0% and no differences between thrombectomy methods were observed in the recanalization rate or the percentage of patients with a favorable outcome.
In the Systematic Evaluation of Patients Treated With Stroke Devices for Acute Ischemic Stroke (STRATIS) registry,10) which is the result of post-marketing research of the Solitaire at 55 institutions in the United States, 172 patients with M2 occlusive lesions (17.3%) (median age: 71 years, NIHSS score: 16) were included, the effective recanalization rate was 82.0%, and the rate of mRS 0-2 after 3 months was 58.7%. The percentage of patients with a favorable outcome was comparable to that in patients with M1 occlusion (M1: 59.2% vs. M2: 58.7%, p = 0.914), but the effective recanalization rate was lower in those with M2 occlusion (M1: 91.4% vs. M2: 82.0%, p = 0.002).
However, in the report by Vargas et al.11) that reviewed 35 patients treated by ADAPT for distal lesions including 28 patients (80.0%) with M2 occlusion, the effective reca-nalization was achieved in 77.8% by aspiration alone and in 97.1% after a rescue treatment such as the SR, and ADAPT was also considered to be effective for peripheral lesions. In the study, Penumbra 3MAX to 5MAX ACE60 were used as aspiration catheters, and the authors consid-ered that, if they can be guided to the lesion, stronger aspi-ration force was obtained using larger bore catheters.
Results of thrombectomy therapy by aspiration using the 4MAXThe reports of treatment using the 4MAX are shown in Table 3. Park et al.12) performed manual aspiration using the 4MAX as the first-line treatment in 32 patients with M2 occlusion, resulting in effective recanalization in 84.0%, a favorable outcome in 78.0%, and treatment-re-lated symptomatic intracranial hemorrhage in 0% of the patients. Kim et al.13) reported the results of forced artery suction thrombectomy (FAST) using the 4MAX in 25 patients: Effective recanalization was achieved in 72.0% (64.0% by FAST alone), a favorable outcome was obtained in 84.0%, and symptomatic intracranial hemorrhage was observed in 4.0%.
At our institution, thrombectomy for M2 occlusive lesions has been performed with ADAPT using the Penumbra 4MAX as the first-line procedure since 2016 based on pre-vious experience and reports. The recanalization could be achieved in a short period in 66.7% of the patients by
score of 0-2 after 3 months was 49.0% in the endovascular treatment group and 44.2% in the control group (common OR: 1.58, 95.0% CI: 0.51–3.21), and the effectiveness of endo-vascular treatment was not indicated. However, patients with M2 occlusion were included only in Multicenter Ran-domized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands (MR CLEAN) and Extending the Time for Thrombolysis in Emergency Neurological Deficits - Intra-Arterial (EXTEND-IA) among the five studies, accounting for only 95 (7.4%) of the 1278 patients, so validation of the efficacy or risk was consid-ered difficult.
Sarraj et al.7) compared 288 patients treated with throm-bectomy (endovascular group) and 234 treated with medical therapy (medical group) with M2 occlusion at 10 institutions in the United States. Concerning the background factors, patients in the endovascular group were younger (median: 68 [IQR: 56–78] vs. 73 [60–81], p = 0.003), had lower rates of IV-tPA (59.7% vs. 74.4%, p = 0.001), and were transferred later to the hospital (158 [73–262] min vs. 86 [48–190] min, p = 0.001), but the other factors were similar between the two groups. Effective recanalization (TICI 2b-3) was achieved in 78.0%, and the proportion of patients with a mRS score 0-2 after 3 months was higher in the endovascular group (62.8% vs. 35.4%, OR: 3.1, 95.0% CI: 2.1–4.4, p <0.001). While symptomatic intracranial hem-orrhage occurred slightly more frequently, the difference was not significant (5.6% vs. 2.1%, p = 0.10). The effec-tiveness and safety of thrombectomy in acute ischemic stroke due to M2 occlusion was suggested.
Comparison between the SR and aspirationIn thrombectomy for M2 occlusion, it is important to achieve early and safe recanalization with a high recanali-zation rate in severe cases to demonstrate its efficacy. How-ever, it is not easy to navigate the thrombectomy devices to distal lesions, and, because of anatomical factors such as the small diameter, tortuousness, and presence of many branches, the selection of the thrombectomy method is vital. According to subgroup analysis concerning M2 occlusive lesions in the Contact Aspiration vs Stent Retriever for Successful Revascularization (ASTER) Trial, which was a randomized study that compared contact aspiration (CA) with the SR,8) there were no significant differences between two first-line thrombectomy devices in effective recanaliza-tion (89.6% by CA vs. 83.9% by SR, p = 0.36), mRS 0-2 after 3 months (54.4% vs. 50.0%, p = 0.84), and symptom-atic intracranial hemorrhage (6.3% vs. 3.2%). Also, according to meta-analysis by Saber et al.9) that reviewed
Journal of Neuroendovascular Therapy Vol. 13, No. 2 (2019)

64
Asai T, et al.
ADAPT alone and in 91.7% after all procedure using the SR. In addition, while the patients treated at our institution were old and showed a high preprocedural NIHSS score, the outcome was favorable in 8 (66.7%) of all 12 patients, and in 8 (88.9%) of the 9 in whom the premorbid mRS score was 0-2, comparing favorably with other studies.
At our institution, the PX SLIM (Penumbra, Inc., Alameda, CA, USA) or Rebar-18 (Medtronic) was successfully deliv-ered to the site of M2 occlusion as an inner microcatheter in all patients, and also, the 4MAX itself could be delivered successfully in 11 (91.7%) of the 12 patients, and the deliver-ability of the 4MAX is considered to be satisfactory. In addi-tion, since the aspiration force of the 4MAX, which has a larger diameter than the 3MAX, is stronger, the 4MAX is con-sidered more effective in ADAPT.
Characteristics of this treatmentThe SR was used in 3 of the 11 patients in whom 4MAX could contact to the clot, and effective recanalization by ADAPT alone was not achieved because of the hard clot in one patient and misalignment of the axis of 4MAX with the vessel due to curving lesions in two patients. Even if the aspiration axis is deviated by the tortuosity, retrieval of the clot becomes possible by the concomitant use of the SR, which straightens vessel and corrects the axis, and by sucking the clot into the aspiration catheter. In this method, since the stent can be used by the same navigation system for the 4MAX, it is unnecessary to set up new equipment, which is important for shortening the procedural time. Since the 4MAX is present very close to the clot, the dis-tance of deployment and traction of the SR can be reduced, and displacement of the blood vessel can be minimized, resulting in a reduced risk of vascular damage. Also, by placing the 4MAX in the M2 during the concomitant use of the stent, the risk of scattering the clot to other branches during the retrieval procedure can be reduced. However, the external diameter of the tip of 4MAX is 4.3 Fr (1.42 mm), and 4MAX is a large device to deliver to peripheral lesions, and vascular damage may be induced if it is forced to advance into M2 branches ≤1.5 mm in diameter. Therefore, precautions, such as selecting the 3MAX or a SR with a small diameter, are necessary.
LimitationsThis study was a retrospective study with a small number of patients at a single institution, and the statistical power is deficient for establishing the efficacy or safety of this treatment. Therefore, further accumulation of cases and a
Tabl
e 3
Lite
ratu
re o
f asp
iratio
n th
rom
bect
omy
usin
g Pe
num
bra
4MAX
for M
2 oc
clus
ion
Aut
hor
Year
Num
ber
Age
NIH
SS
TIC
I 2b
-3 (%
)R
escu
e (%
)P
to
Rm
RS
0-2
(9
0d) (
%)
SIC
H (%
)
Par
k et
al.12
)20
1632
70.1
± 1
0.8
10.9
± 5
.127
(84.
0)N
A33
.2 ±
12.
625
(78.
0)0
(0)
Kim
et
al.13
)20
1725
7
1 (6
0.5–
75)
15 (8
–17)
18 (7
2.0)
5 (2
0.0)
53 (4
1–74
)21
(84.
0)
1 (4
.0)
Pre
sent
stu
dy
2018
1277
(69–
80)
19.
5 (1
6–24
.5)
11 (9
1.7)
4 (3
3.3)
45 (2
2–64
) 8
(66.
7)0
(0)
Tota
l69
56 (8
1.2)
54 (7
8.2)
1
(1.4
)
mR
S: m
odifi
ed R
anki
n S
cale
; NIH
SS
: Nat
iona
l Ins
titut
es o
f Hea
lth S
trok
e S
cale
; P to
R: p
unct
ure
to re
cana
lizat
ion
time,
SIC
H: s
ympt
omat
ic in
trac
rani
al h
emor
rhag
e; T
ICI:
thro
mbo
lysi
s in
cer
ebra
l in
farc
tion
Journal of Neuroendovascular Therapy Vol. 13, No. 2 (2019)

65
Therapeutic Results of ADAPT Using Penumbra 4MAX for M2 Occlusion
large vessel occlusions amenable to endovascular therapy. J Neurointerv Surg 2018; 10: 510–515.
5) Hirano T, Sasaki M, Mori E, et al: Residual vessel length on magnetic resonance angiography identifies poor respond-ers to alteplase in acute middle cerebral artery occlusion patients: exploratory analysis of the Japan Alteplase Clinical Trial II. Stroke 2010; 41: 2828–2833.
6) Kimura K, Sakamoto Y, Aoki J, et al: Clinical and MRI pre-dictors of no early recanalization within 1 hour after tissue- type plasminogen activator administration. Stroke 2011; 42: 3150–3155.
7) Sarraj A, Sangha N, Hussain MS, et al: Endovascular therapy for acute ischemic stroke with occlusion of the middle cere-bral artery M2 segment. JAMA Neurol 2016; 73: 1291–1296.
8) Gory B, Lapergue B, Blanc R, et al: Contact aspiration ver-sus stent retriever in patients with acute ischemic stroke with M2 occlusion in the ASTER randomized trial (contact aspi-ration versus stent retriever for successful revascularization). Stroke 2018; 49: 461–464.
9) Saber H, Narayanan S, Palla M, et al: Mechanical throm-bectomy for acute ischemic stroke with occlusion of the M2 segment of the middle cerebral artery: a meta-analysis. J Neurointerv Surg 2018; 10: 620–624.
10) Mueller-Kronast NH, Zaidat OO, Froehler MT, et al: Sys-tematic evaluation of patients treated with neurothrombec-tomy devices for acute ischemic stroke: primary results of the STRATIS registry. Stroke 2017; 48: 2760–2768.
11) Vargas J, Spiotta AM, Fargen K, et al: Experience with a direct aspiration first pass technique (ADAPT) for thrombec-tomy in distal cerebral artery occlusions causing acute isch-emic stroke. World Neurosurg 2017; 99: 31–36.
12) Park JS, Kwak HS: Manual aspiration thrombectomy using penumbra catheter in patients with acute M2 occlusion: a single-center analysis. J Korean Neurosurg Soc 2016; 59: 352–356.
13) Kim YW, Son S, Kang DH, et al: Endovascular thrombec-tomy for M2 occlusions: comparison between forced arterial suction thrombectomy and stent retriever thrombectomy. J Neurointerv Surg 2017; 9: 626–630.
prospective setup are necessary. In addition, during the study period, five patients who received ADAPT using the 5MAX ACE or SR thrombectomy as the first-line treat-ment were included in the 17 patients with M2 occlusion. Effective recanalization could be achieved in 16 (94.1%) of the 17 patients, and the results of thrombectomy were also satisfactory in patients treated by methods other than ADAPT using the 4MAX.
Conclusion
In M2 occluded region, a high recanalization rate could be achieved by ADAPT using the 4MAX without causing symptomatic intracranial hemorrhage, and the results sug-gested high efficacy and safety of the technique.
Disclosure Statement
Neither the first author nor any of the coauthors have any conflicts of interest to disclose.
References 1) Goyal M, Menon BK, van Zwam WH, et al: Endovas-
cular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five ran-domised trials. Lancet 2016; 387: 1723–1731.
2) Turk AS, Spiotta A, Frei D, et al: Initial clinical experience with the ADAPT technique: a direct aspiration first pass tech-nique for stroke thrombectomy. J Neurointerv Surg 2014; 6: 231–237.
3) Lima FO, Furie KL, Silva GS, et al: Prognosis of untreated strokes due to anterior circulation proximal intracranial arte-rial occlusions detected by use of computed tomography angiography. JAMA Neurol 2014; 71: 151–157.
4) Rai AT, Domico JR, Buseman C, et al: A population-based incidence of M2 strokes indicates potential expansion of
Journal of Neuroendovascular Therapy Vol. 13, No. 2 (2019)