
Therapeutic Options Insulins. 1 Insulin Preparations ClassAgents Human insulinsRegular, NPH, lente,...
35
Therapeutic Options Insulins
-
Upload
katrina-hopkins -
Category
Documents
-
view
227 -
download
0
Transcript of Therapeutic Options Insulins. 1 Insulin Preparations ClassAgents Human insulinsRegular, NPH, lente,...
Therapeutic OptionsInsulins
2
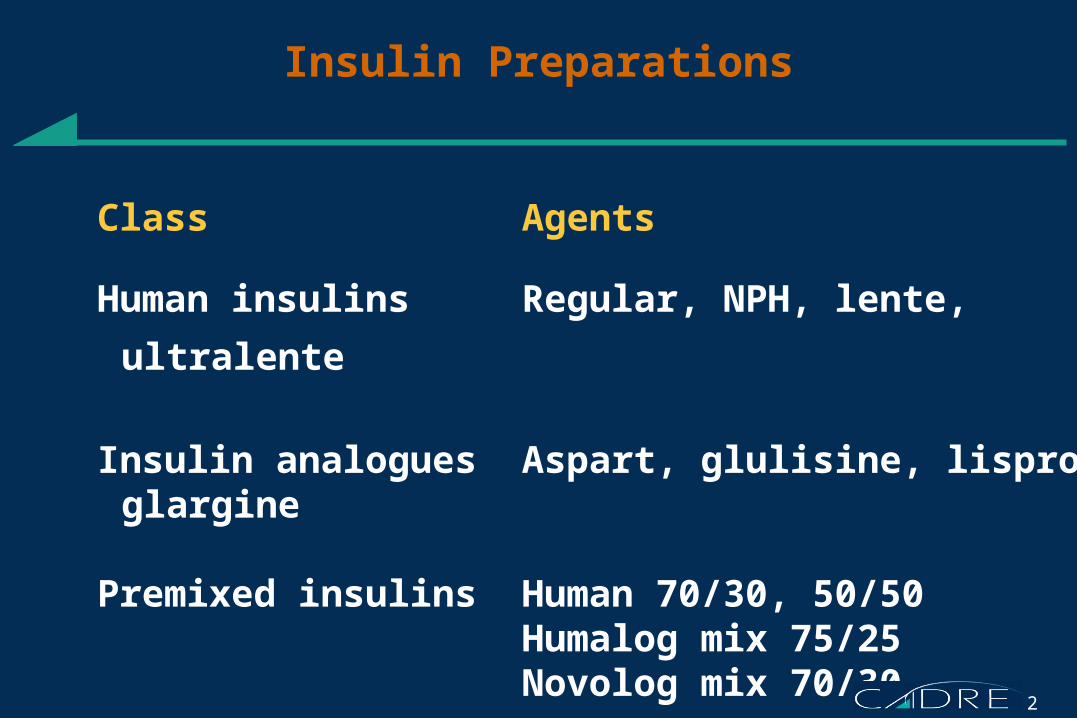
Insulin Preparations
Class Agents
Human insulins Regular, NPH, lente, ultralente
Insulin analogues Aspart, glulisine, lispro, glargine
Premixed insulins Human 70/30, 50/50Humalog mix 75/25Novolog mix 70/30
3
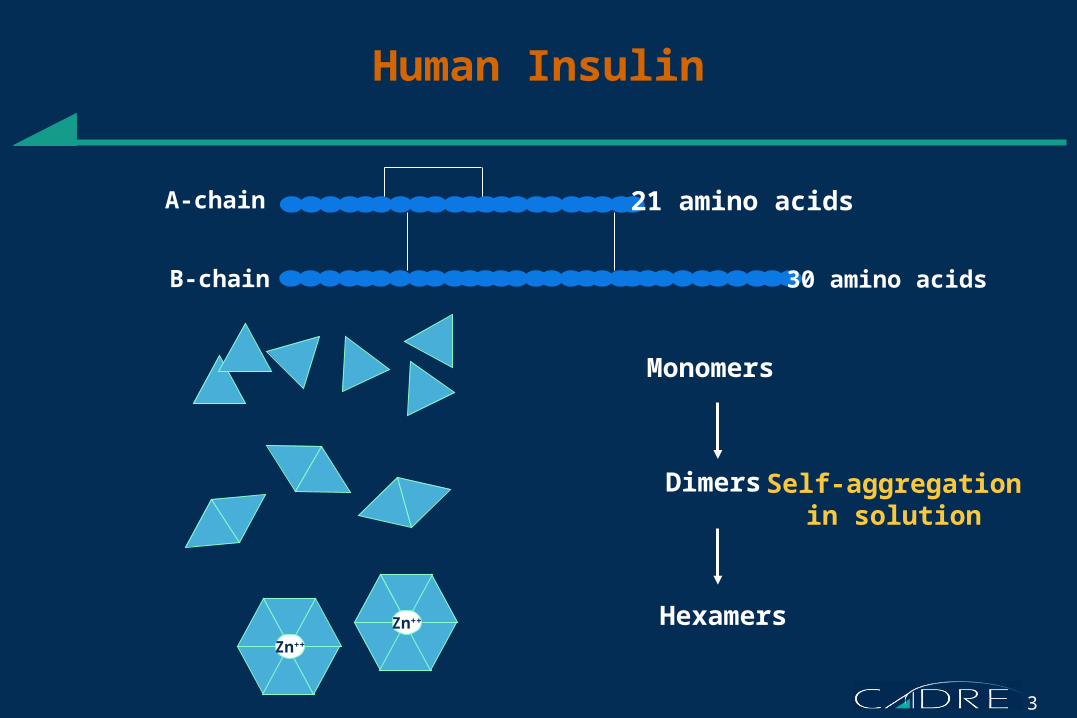
Human Insulin
A-chain
B-chain
Zn++
Zn++
Self-aggregationin solution
Monomers
Dimers
Hexamers
21 amino acids
30 amino acids
4
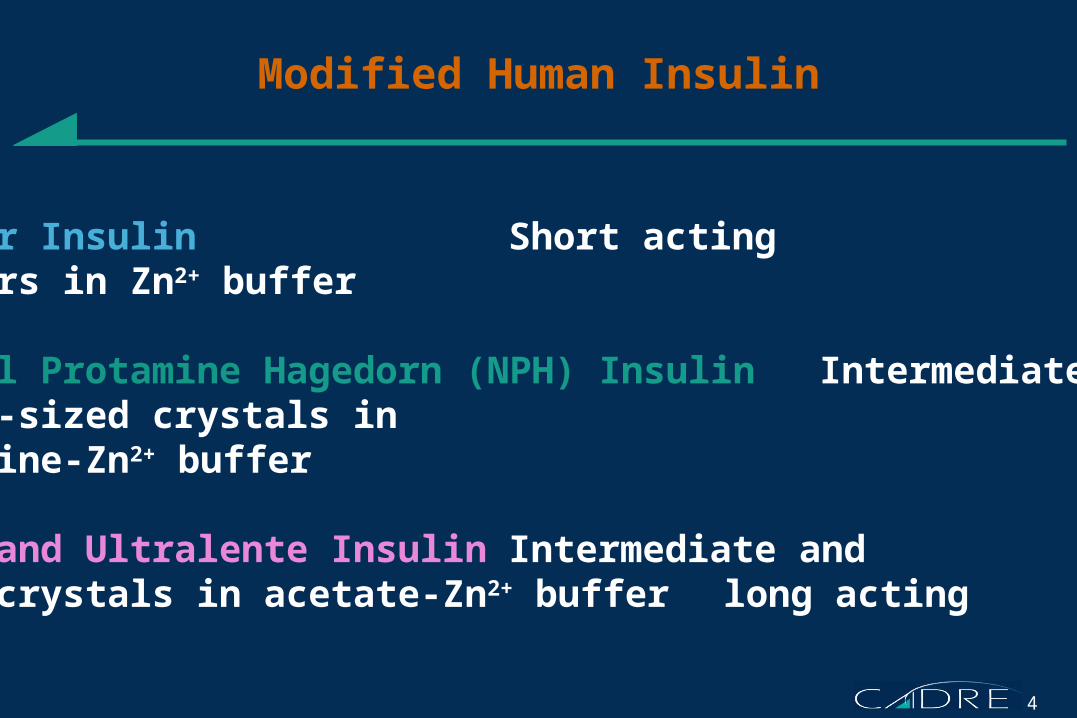
Modified Human Insulin
Regular Insulin Short actingHexamers in Zn2+ buffer
Neutral Protamine Hagedorn (NPH) Insulin Intermediate actingMedium-sized crystals in protamine-Zn2+ buffer
Lente and Ultralente Insulin Intermediate andLarge crystals in acetate-Zn2+ buffer long acting
5
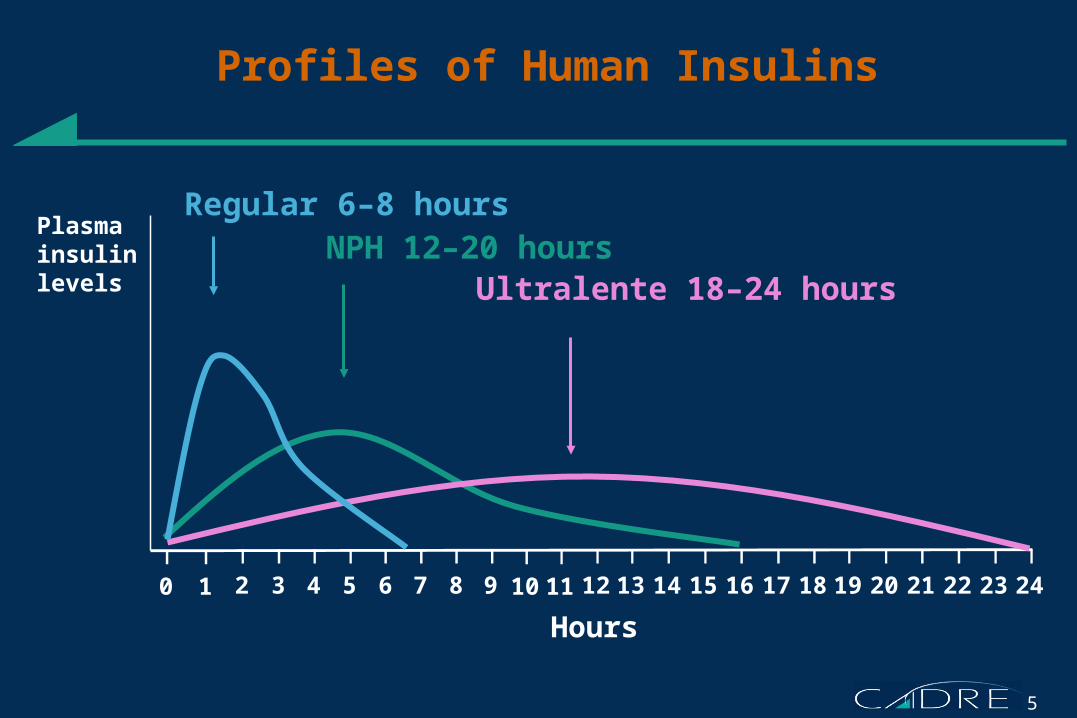
Profiles of Human Insulins
0 1 2 53 4 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Plasmainsulinlevels
Regular 6–8 hours
NPH 12–20 hours Ultralente 18–24 hours
Hours
6
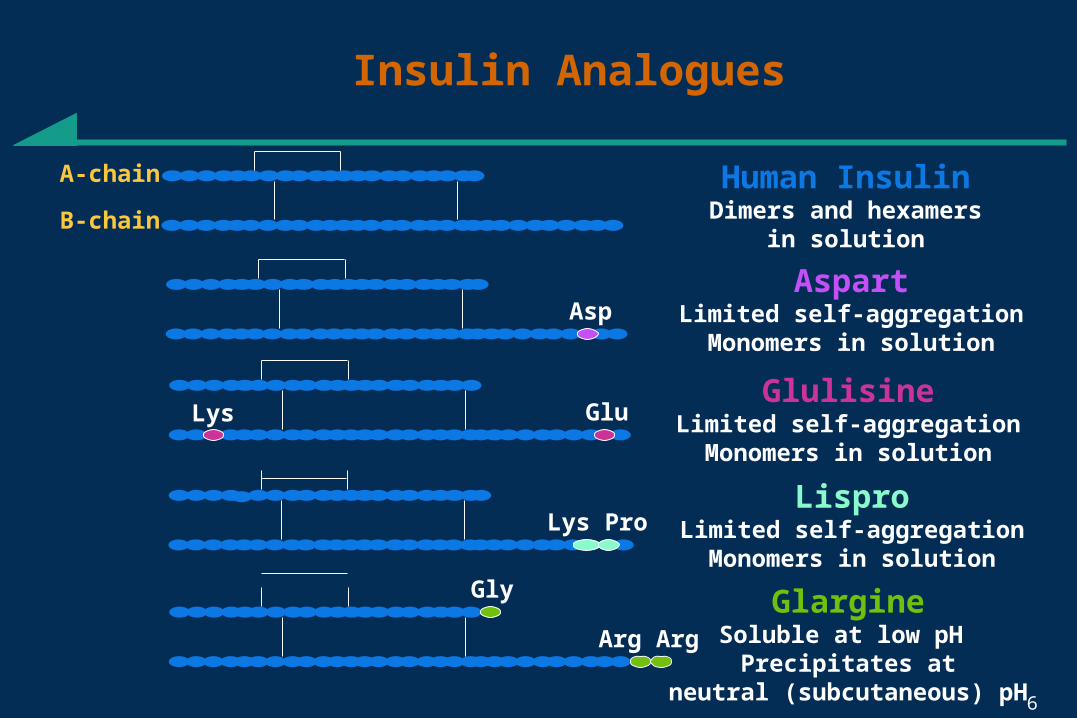
Insulin Analogues
Human InsulinDimers and hexamers
in solution
A-chain
B-chain
Lys Pro
Gly
Arg Arg
Asp
LisproLimited self-aggregation
Monomers in solution
AspartLimited self-aggregation
Monomers in solution
GlargineSoluble at low pH
Precipitates atneutral (subcutaneous) pH
GluGlulisine
Limited self-aggregationMonomers in solution
Lys
7
500
400
300
200
100
0
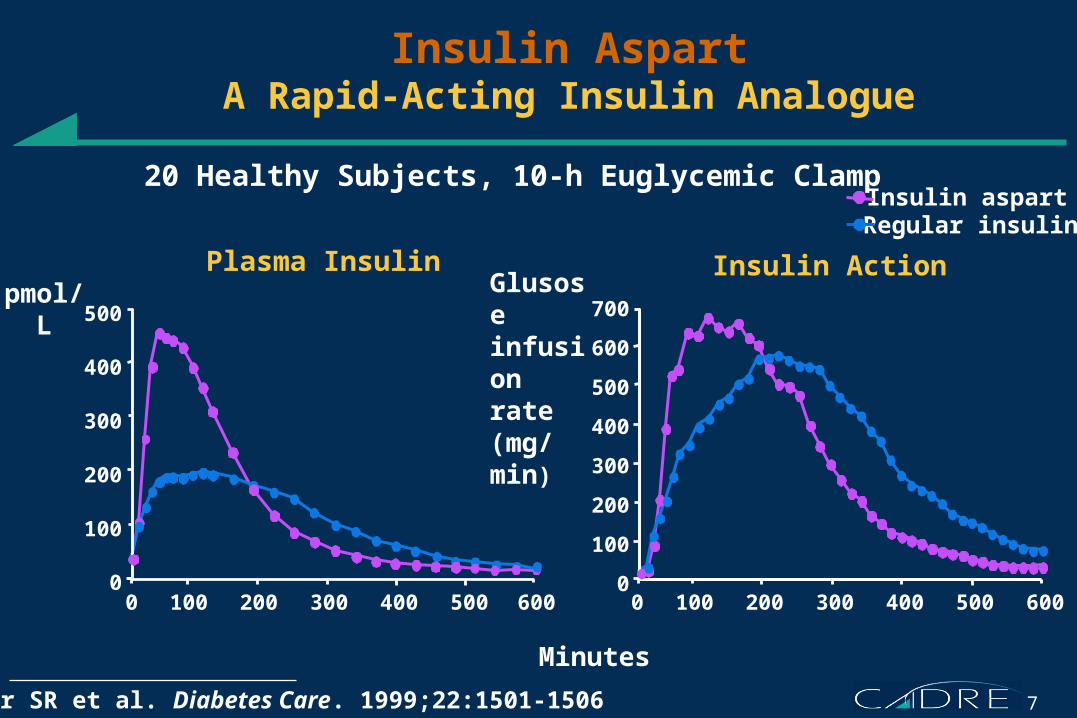
Insulin AspartA Rapid-Acting Insulin Analogue
Plasma Insulin
Mudaliar SR et al. Diabetes Care. 1999;22:1501-1506
Insulin Action pmol/L
700
600
500
400
300
200
100
0
Minutes
0 100 200 300 400 500 600 0 100 200 300 400 500 600
Glusoseinfusion rate(mg/min)
Insulin aspartRegular insulin
20 Healthy Subjects, 10-h Euglycemic Clamp
8
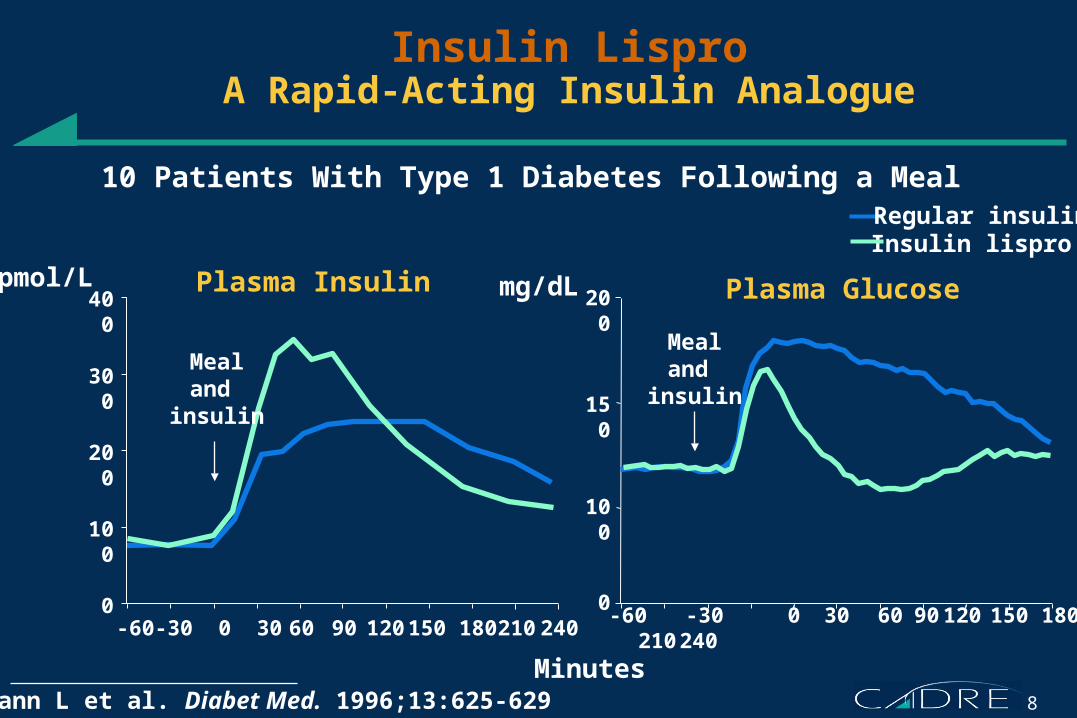
Insulin LisproA Rapid-Acting Insulin Analogue
Heinemann L et al. Diabet Med. 1996;13:625-629
Insulin lisproRegular insulin
-60 -30 0 30 60 90 120 150 180 210 240
Minutes
mg/dLpmol/L400
-60 -30 0 30 60 90 120 150 180 210 240
Mealand
insulin
Mealand
insulin
Plasma Insulin Plasma Glucose
10 Patients With Type 1 Diabetes Following a Meal
300
200
100
0
200
150
0
100
9
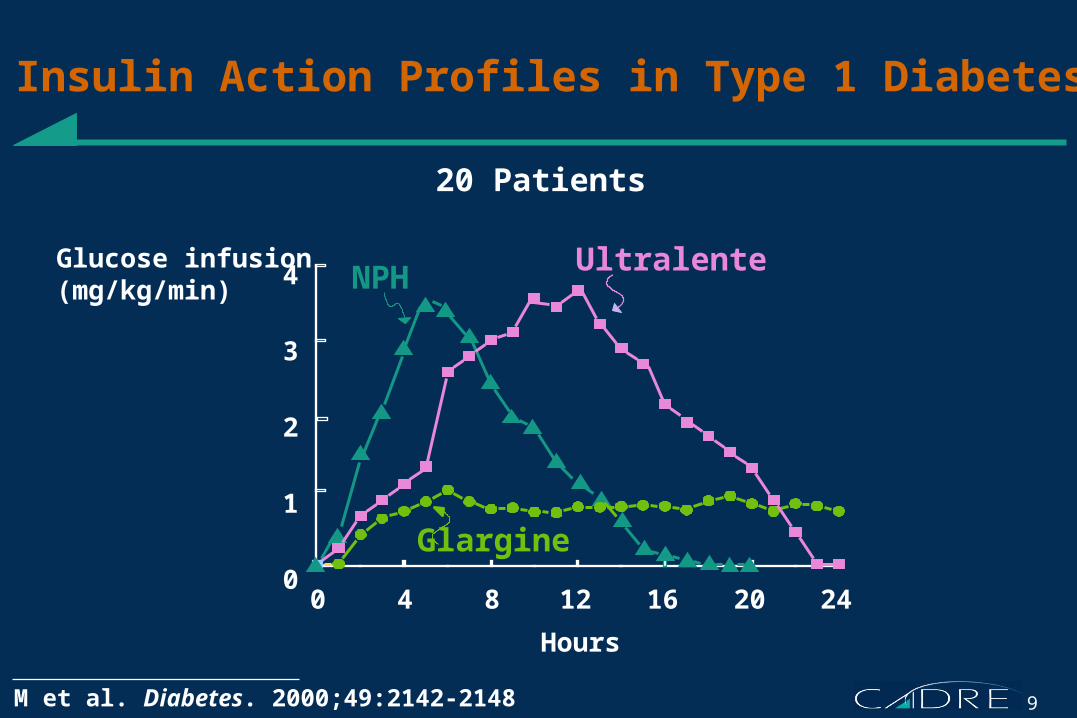
0 4 8 12 16 20 24
Insulin Action Profiles in Type 1 Diabetes
Lepore M et al. Diabetes. 2000;49:2142-2148
Glucose infusion(mg/kg/min)
20 Patients
4
3
2
1
0
Glargine
NPHUltralente
Hours
10
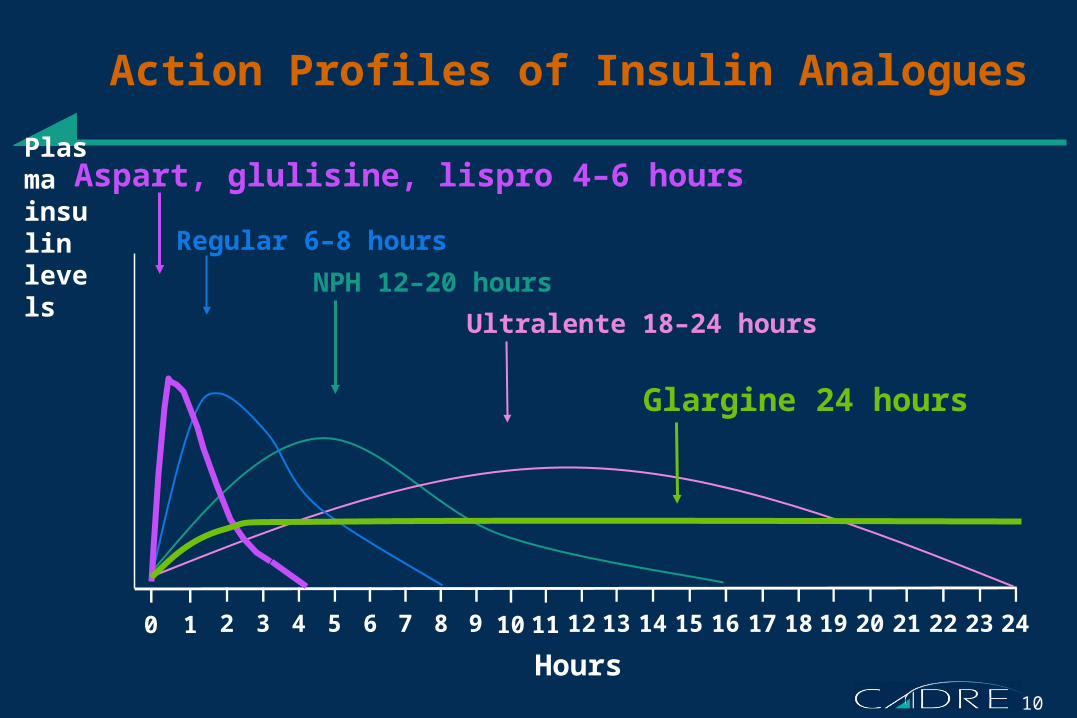
Action Profiles of Insulin Analogues
0 1 2 53 4 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Plasmainsulinlevels
Regular 6–8 hours
NPH 12–20 hours
Ultralente 18–24 hours
Hours
Glargine 24 hours
Aspart, glulisine, lispro 4–6 hours
11
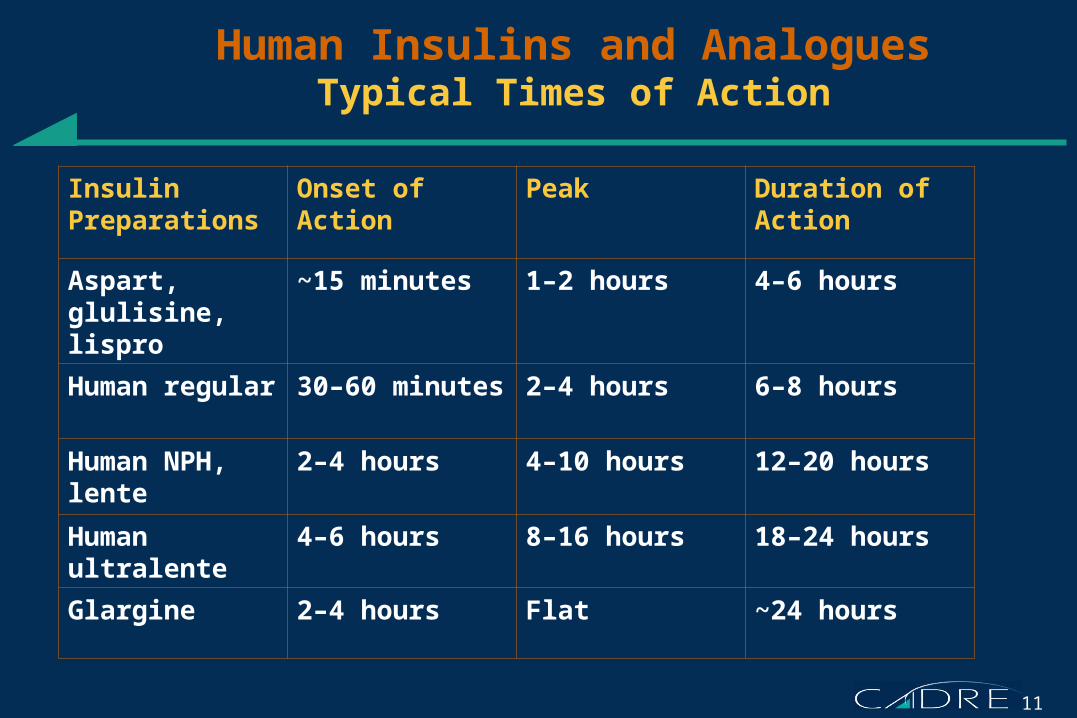
Human Insulins and AnaloguesTypical Times of Action
Insulin Preparations
Onset of Action Peak Duration of Action
Aspart, glulisine, lispro
~15 minutes 1–2 hours 4–6 hours
Human regular 30–60 minutes 2–4 hours 6–8 hours
Human NPH, lente
2–4 hours 4–10 hours 12–20 hours
Human ultralente
4–6 hours 8–16 hours 18–24 hours
Glargine 2–4 hours Flat ~24 hours
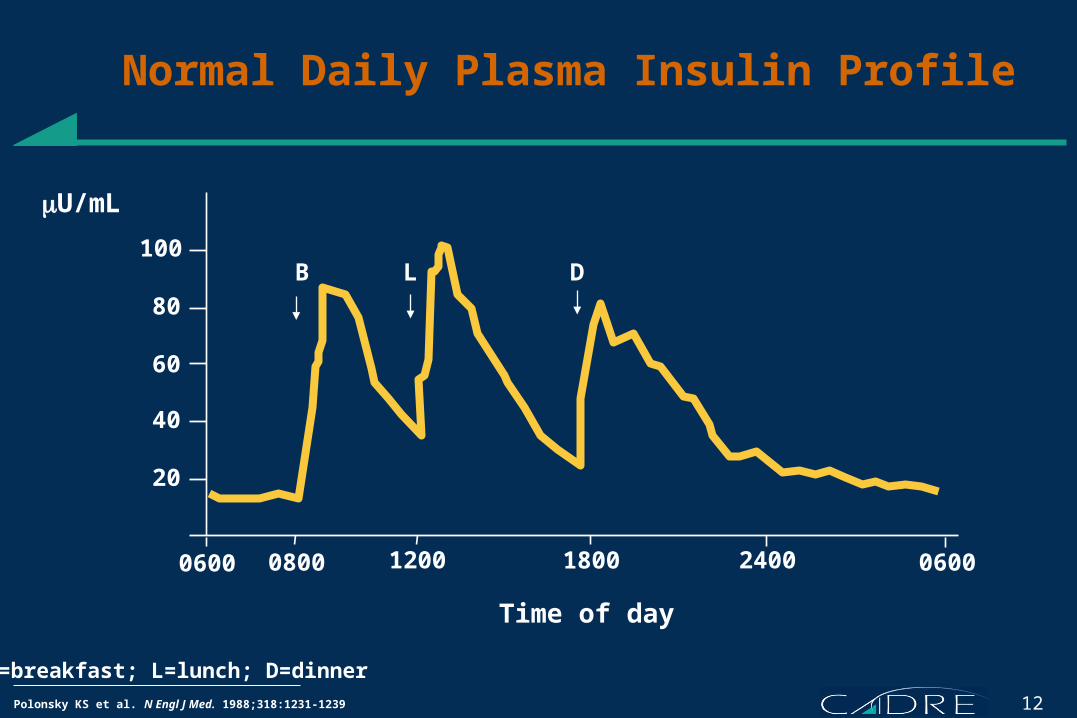
12Polonsky KS et al. N Engl J Med. 1988;318:1231-1239
0600 0600
Time of day
20
40
60
80
100 B L D
Normal Daily Plasma Insulin Profile
B=breakfast; L=lunch; D=dinner
0800 18001200 2400
U/mL
13
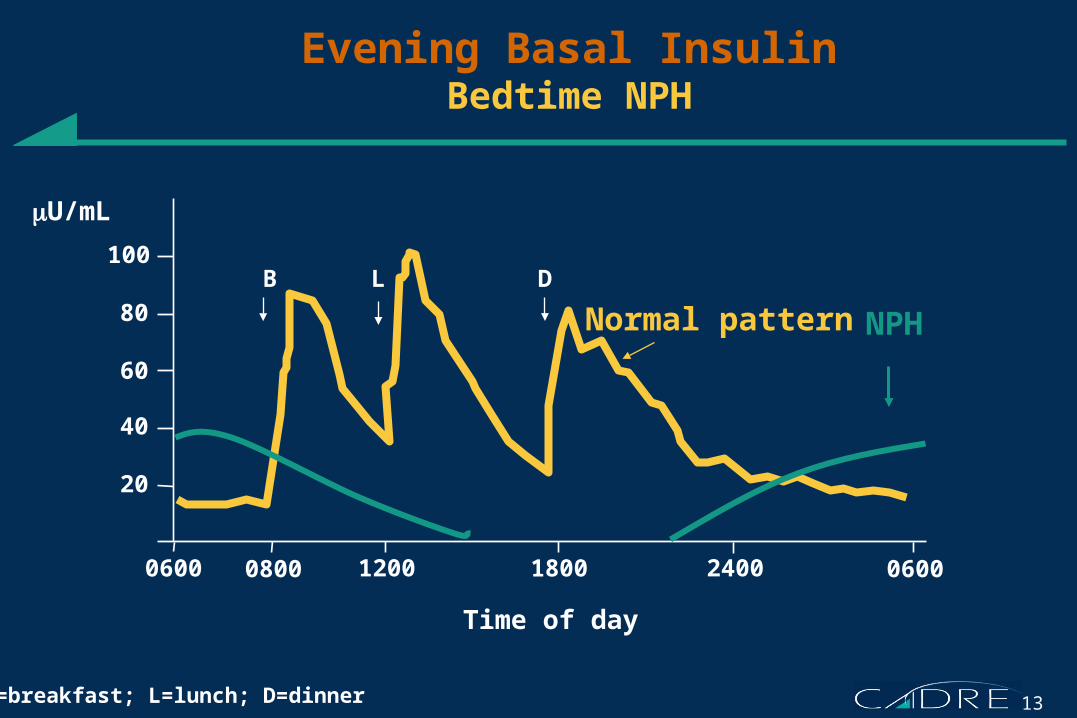
Time of day
20
40
60
80
100 B L D
Evening Basal InsulinBedtime NPH
B=breakfast; L=lunch; D=dinner
0600 06000800 18001200 2400
NPHNormal pattern
U/mL
14
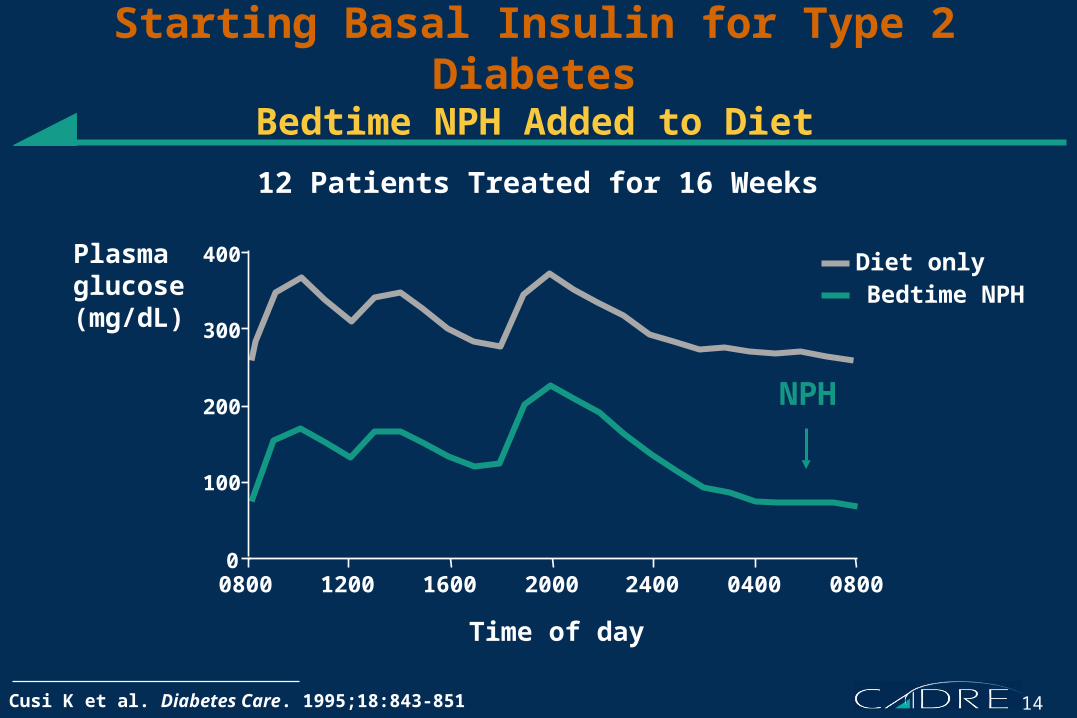
Starting Basal Insulin for Type 2 DiabetesBedtime NPH Added to Diet
Cusi K et al. Diabetes Care. 1995;18:843-851
300
200
00800 1200 1600
Time of day
2000 2400 0400 0800
400
100
Diet onlyBedtime NPH
Plasmaglucose(mg/dL)
NPH
12 Patients Treated for 16 Weeks
15
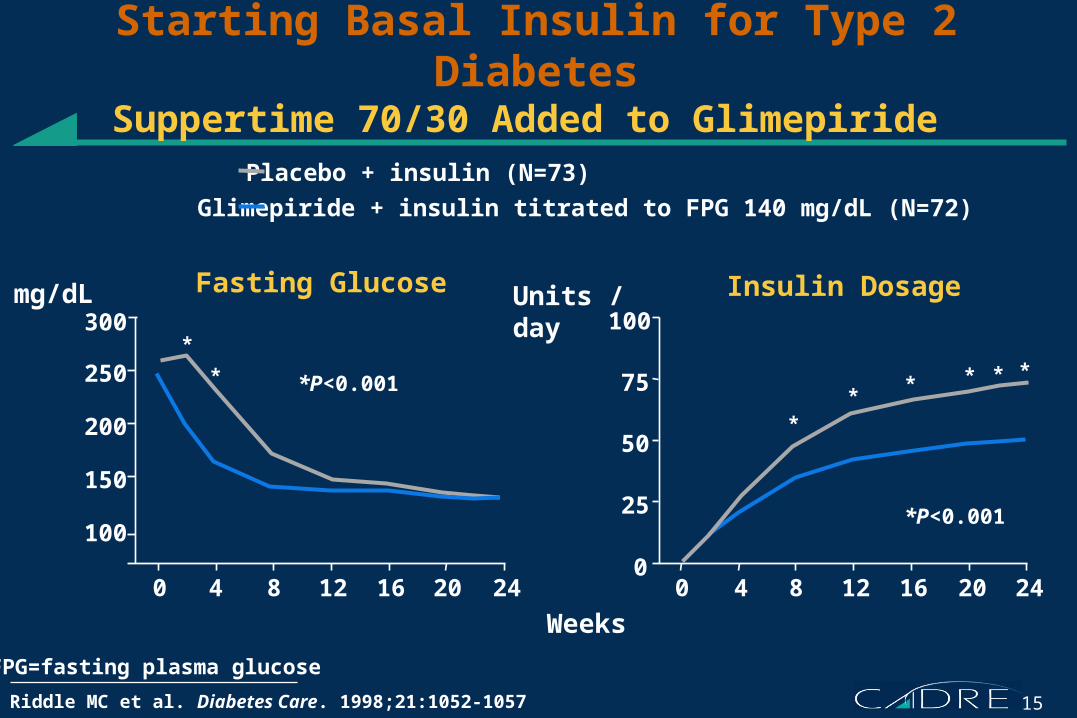
Starting Basal Insulin for Type 2 DiabetesSuppertime 70/30 Added to Glimepiride
Riddle MC et al. Diabetes Care. 1998;21:1052-1057
0
100
150
200
250
300*
*
12 1684 20 24
Weeks
Fasting Glucose
00
25
50
75
100
12 1684 20 24
*P<0.001
Insulin Dosage
**
* * **
Placebo + insulin (N=73)
Glimepiride + insulin titrated to FPG 140 mg/dL (N=72)
mg/dL Units /day
*P<0.001
FPG=fasting plasma glucose
16
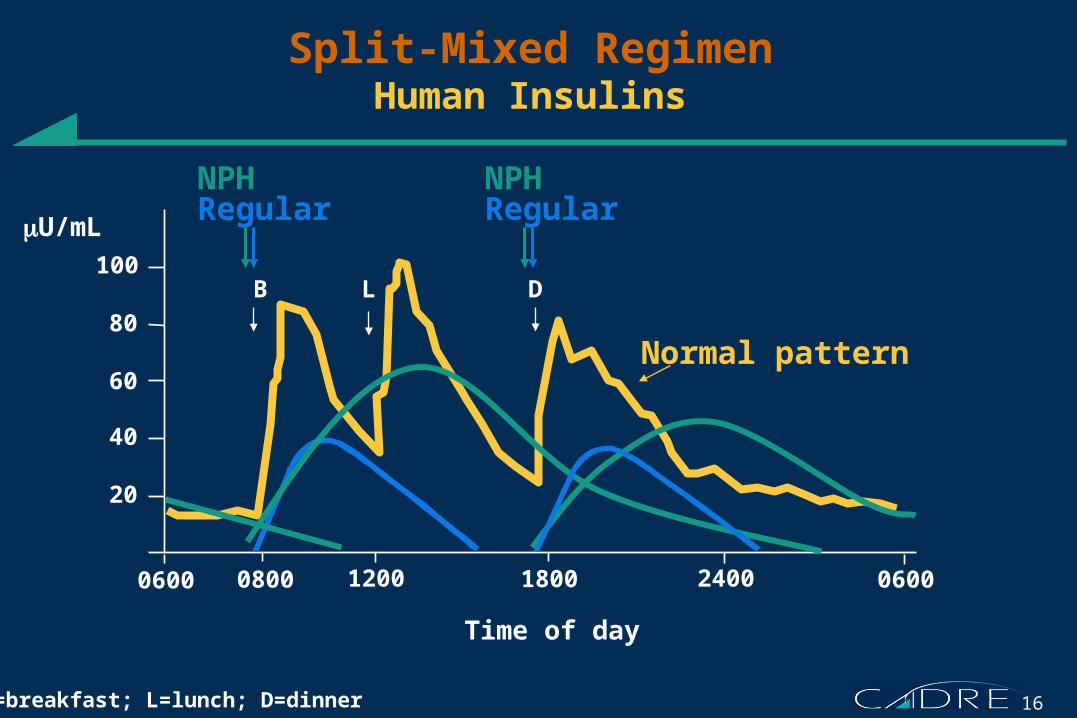
Time of day
20
40
60
80
100 B L D
Split-Mixed RegimenHuman Insulins
B=breakfast; L=lunch; D=dinner
0600 0600 0800 18001200 2400
NPHRegular
NPHRegular
Normal pattern
U/mL
17
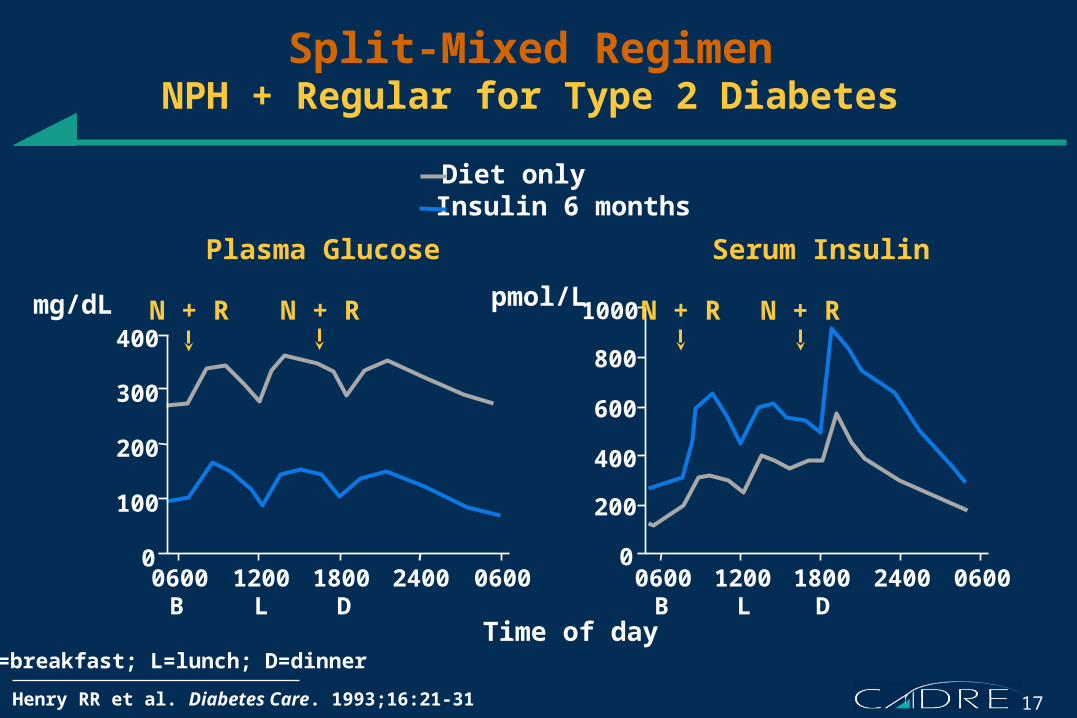
Split-Mixed RegimenNPH + Regular for Type 2 Diabetes
Henry RR et al. Diabetes Care. 1993;16:21-31
200
400
100
300
00
200
600
1000
400
800
0600 06001800 24001200
Time of day
0600 06001800 24001200
Diet onlyInsulin 6 months
Plasma Glucose Serum Insulin
B L D
N + R N + Rmg/dL pmol/L
B L D
N + R N + R
B=breakfast; L=lunch; D=dinner
18
Time of day
20
40
60
80
100 B L D
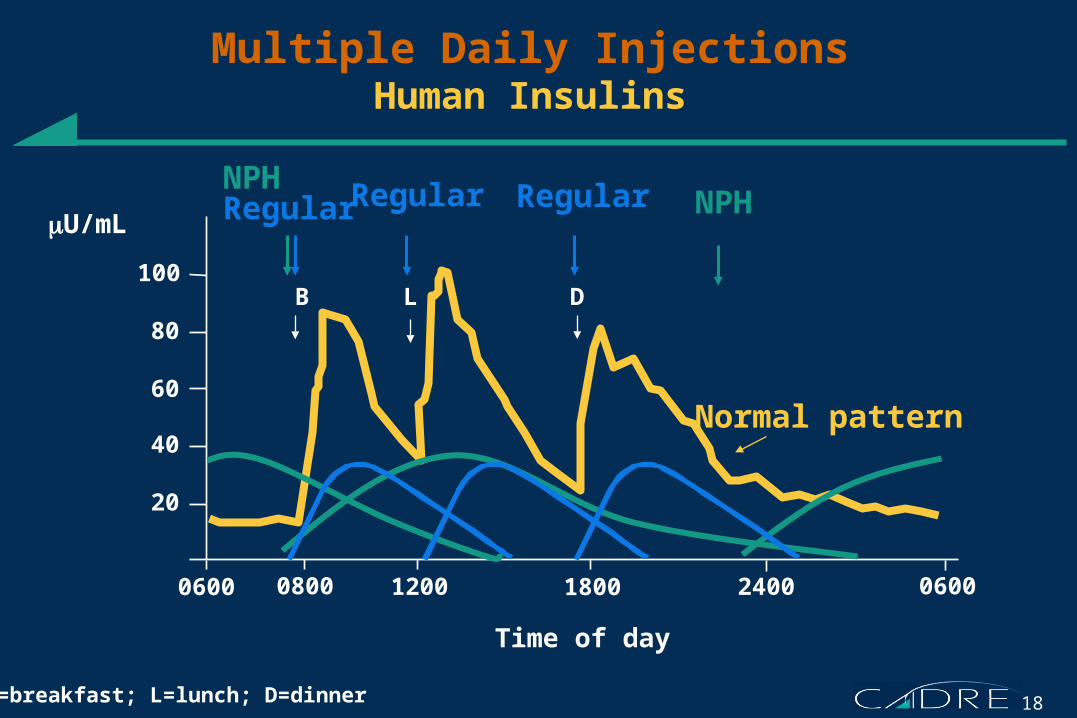
Multiple Daily InjectionsHuman Insulins
B=breakfast; L=lunch; D=dinner
0600 06000800 18001200 2400
Regular NPHNPHRegular
Normal pattern
U/mLRegular
19
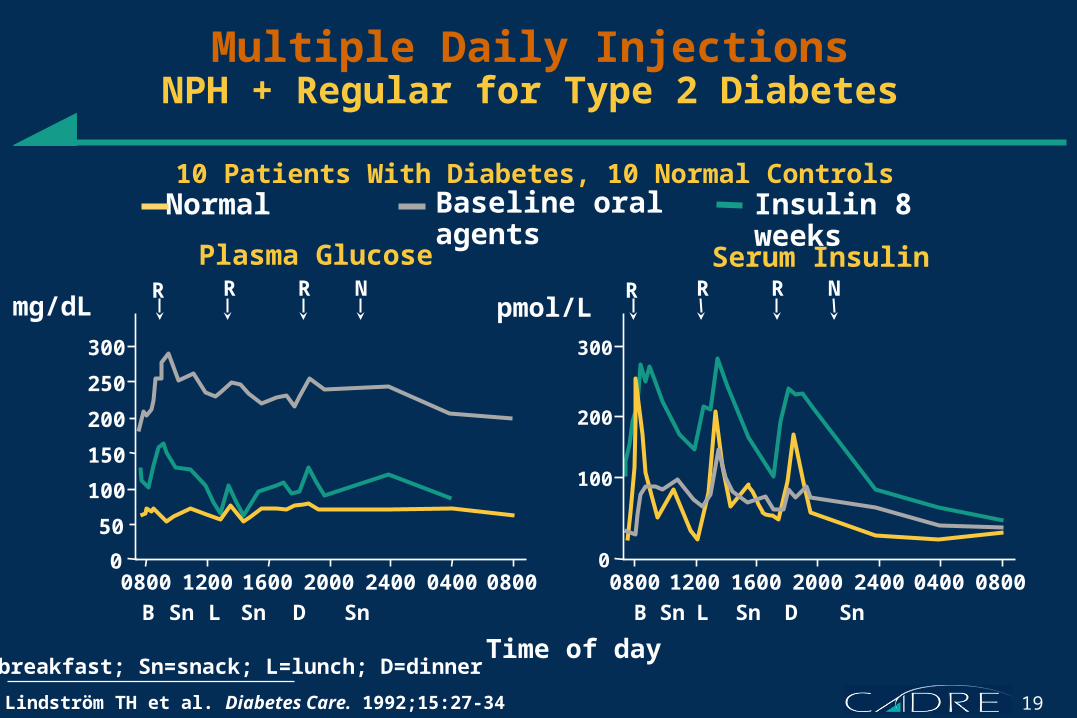
Multiple Daily InjectionsNPH + Regular for Type 2 Diabetes
0
300
250
200
150
100
50
0800 1200 1600 2000 2400 0400 0800
Time of day
0800 1200 1600 2000 2400 0400 0800
Plasma Glucose Serum InsulinR NR R
0
300
200
100
Baseline oral agents Insulin 8 weeksNormal
mg/dL pmol/L
B L D B L D
R NR R
Sn Sn SnSn Sn Sn
Lindström TH et al. Diabetes Care. 1992;15:27-34
B=breakfast; Sn=snack; L=lunch; D=dinner
10 Patients With Diabetes, 10 Normal Controls
20
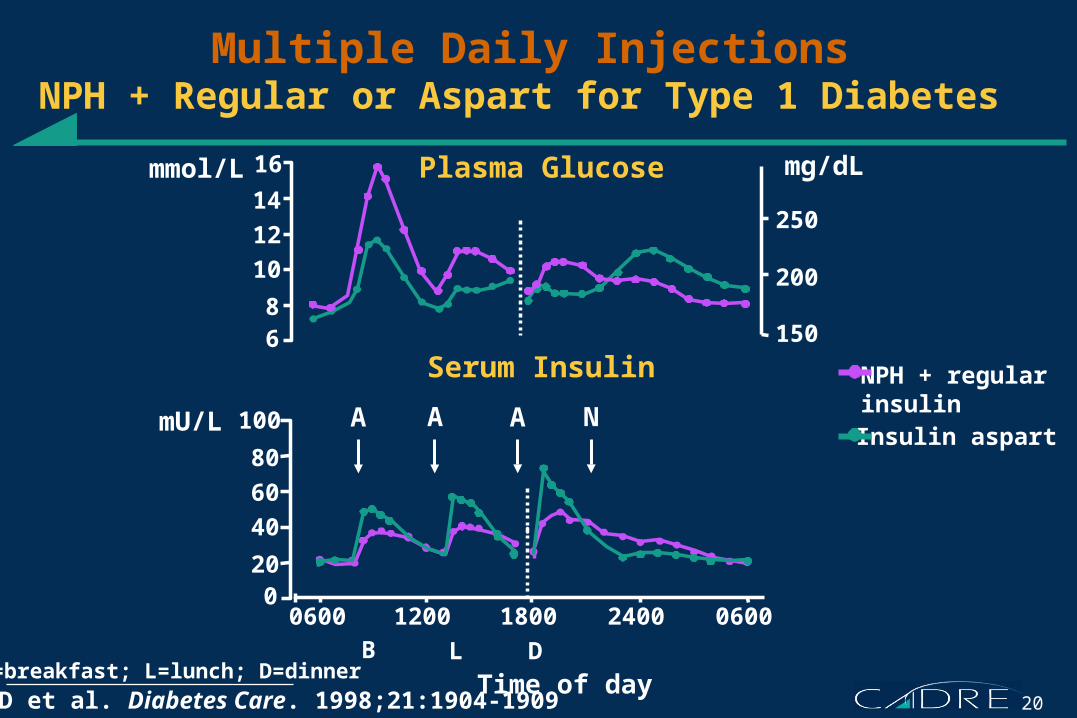
Multiple Daily InjectionsNPH + Regular or Aspart for Type 1 Diabetes
Home PD et al. Diabetes Care. 1998;21:1904-1909
100
80
60
40
200
mU/L
0600 1200 1800 2400 0600
Plasma Glucose
Serum Insulin
A A A N
NPH + regular insulin
B=breakfast; L=lunch; D=dinnerB L D
250
200
150
mg/dL14
12
10
86
mmol/L 16
Time of day
Insulin aspart
21
The Basal-Bolus Insulin Concept
• Basal insulin– Controls glucose production between meals and overnight– Nearly constant levels – 50% of daily needs
• Bolus insulin (mealtime or prandial)– Limits hyperglycemia after meals– Immediate rise and sharp peak at 1 hour postmeal – 10% to 20% of total daily insulin requirement at each meal
• For ideal insulin replacement therapy, each component should come from a different insulin with a specific profile
22
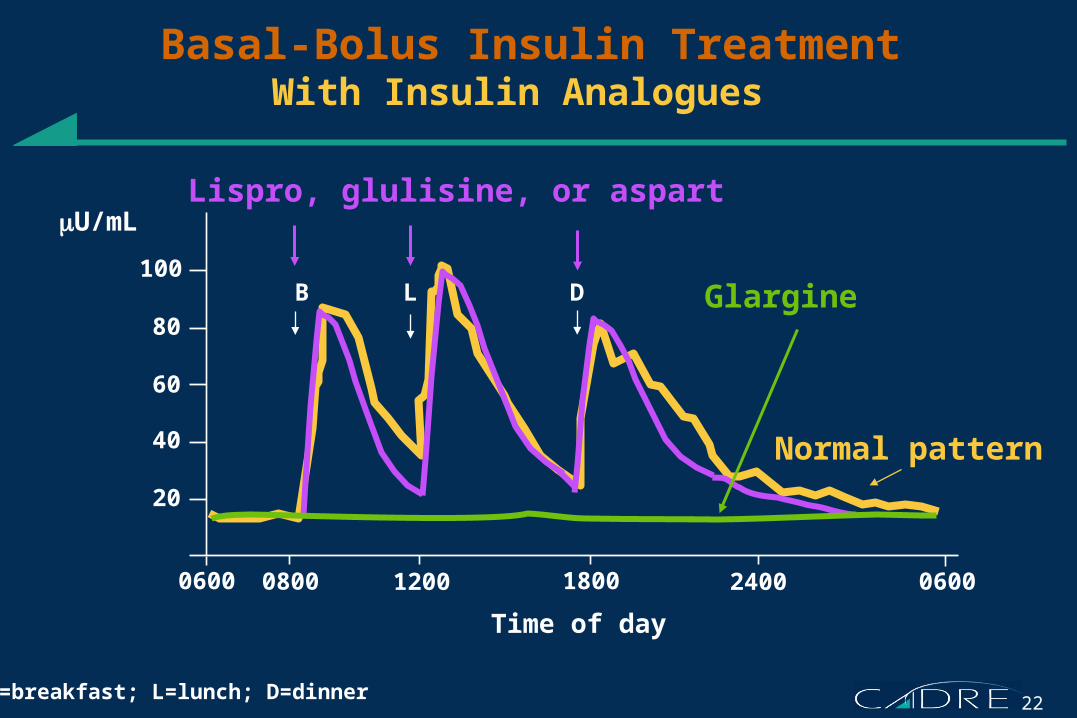
0600 0800 18001200 2400 0600
Time of day
20
40
60
80
100 B L D
Basal-Bolus Insulin TreatmentWith Insulin Analogues
B=breakfast; L=lunch; D=dinner
Glargine
Lispro, glulisine, or aspart
Normal pattern
U/mL
23
Barriers to Using Insulin
• Patient resistance– Perceived significance of needing insulin– Fear of injections– Complexity of regimens– Pain, lipohypertrophy
• Physician resistance– Perceived cardiovascular risks– Lack of time and resources to supervise treatment
• Medical limitations of insulin treatment– Hypoglycemia– Weight gain
24
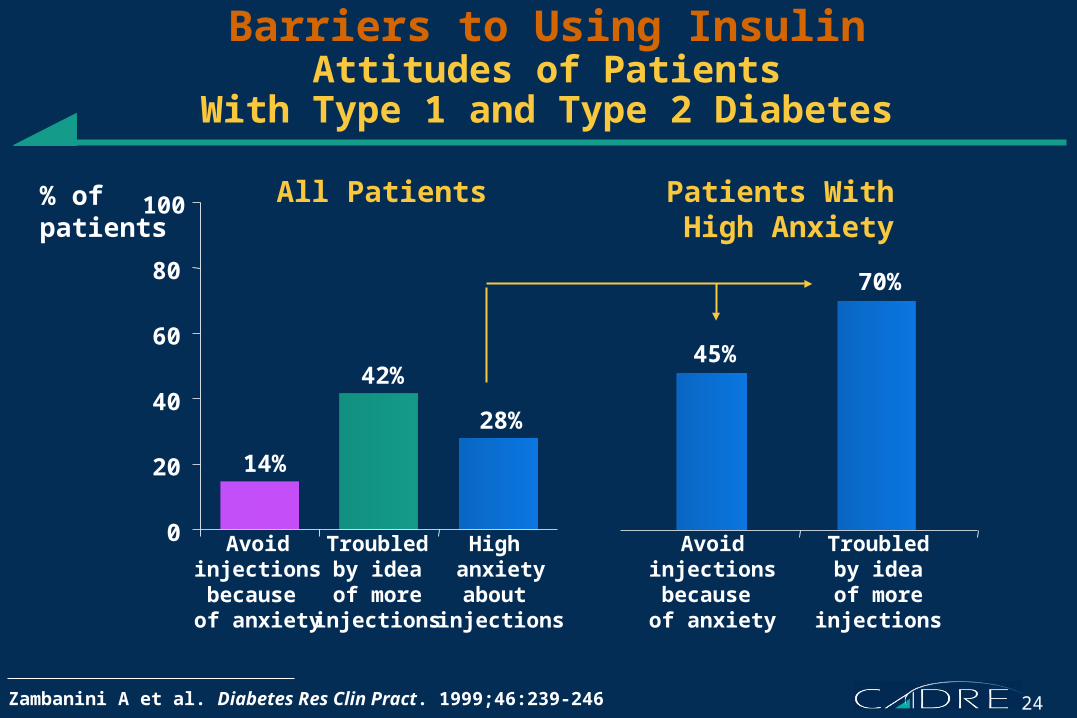
Barriers to Using InsulinAttitudes of Patients
With Type 1 and Type 2 Diabetes
0
20
40
60
80
100% of patients
High anxietyabout
injections
Troubledby ideaof more
injections
Avoidinjectionsbecause of anxiety
Troubledby ideaof more
injections
Avoidinjectionsbecause of anxiety
All Patients Patients With High Anxiety
Zambanini A et al. Diabetes Res Clin Pract. 1999;46:239-246
14%
42%
28%
45%
70%
25
Barriers to Insulin TherapyCardiovascular Risk Is Not Supported by Trials
6-14
Type 2 Diabetes in the UKPDSRisk of myocardial infarctionConventional treatment 17.4 events/1000 pt-yrIntensive insulin 14.7 events/1000 pt-yr (P=0.052)
Type 1 and 2 Diabetes in the DIGAMI StudyLong-term survival after acute myocardial infarctionConventional treatment 44% mortality Intensive insulin 33% mortality (P=0.011)
UKPDS Group. Lancet. 1998;352:837-853; Malmberg K. BMJ. 1997;314:1512-1515
26
Barriers to Insulin TherapySevere Hypoglycemia
DCCT Research Group. Diabetes. 1997;46:271-286; UKPDS Group. Lancet. 1998;352:837-853
6-14
Type 1 Diabetes in the DCCTConventional insulin 35% of pts 19 events/100 pt-yrA1C ~9%, 6.5 yr
Intensive insulin 65% of pts 61 events/100 pt-yrA1C 7.2%, 6.5 yr
Type 2 Diabetes in the UKPDSIntensive policy insulin 37% of pts 2.3% pts/yr A1C 7.0%, 10 yr
27
Barriers to Insulin TherapyWeight Gain
DCCT Research Group. Diabetes. 1997;46:271-286; DCCT Research Group. N Engl J Med. 1993;329:977-986; UKPDS Group. Lancet. 1998;352:837-853
Type 1 Diabetes in the DCCTIntensive insulin + 10.1 lb more A1C 7.2%, 6.5 yr than conventional insulin
Type 2 Diabetes in the UKPDSIntensive insulin + 8.8 lb moreA1C 7.0%, 10 yr than diet treatment
28
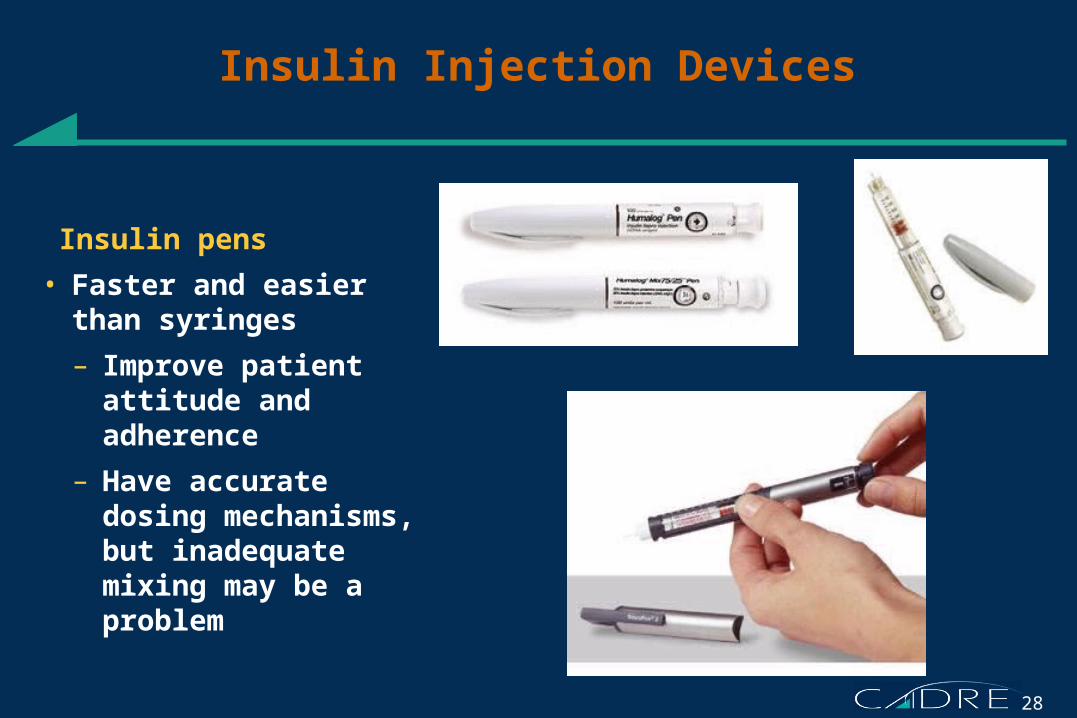
Insulin Injection Devices
Insulin pens
• Faster and easier than syringes
– Improve patient attitude and adherence
– Have accurate dosing mechanisms, but inadequate mixing may be a problem
29
Insulin Pumps
Continuous subcutaneous insulin infusion (CSII)
– External, programmable pump connected to an indwelling subcutaneous catheter to deliver rapid-acting insulin
Intraperitoneal insulin infusion– Implanted, programmable
pump with intraperitoneal catheter. Not available in the United States
30
New Insulins in Clinical Development
• Long-acting insulin analogue – Insulin detemir– Acylated insulin analogue– Soluble, binds to albumin
• Rapid-acting insulin analogue – Insulin 1964– Limited aggregation, like lispro and aspart– Rapid absorption from injection site
• Inhaled insulins – Aerodose, AERx, Exubera
– Liquid aerosol or particulate cloud– Delivered by portable devices
• Buccally absorbed insulin – Oralin
– Liquid aerosol – Delivered by portable device
31
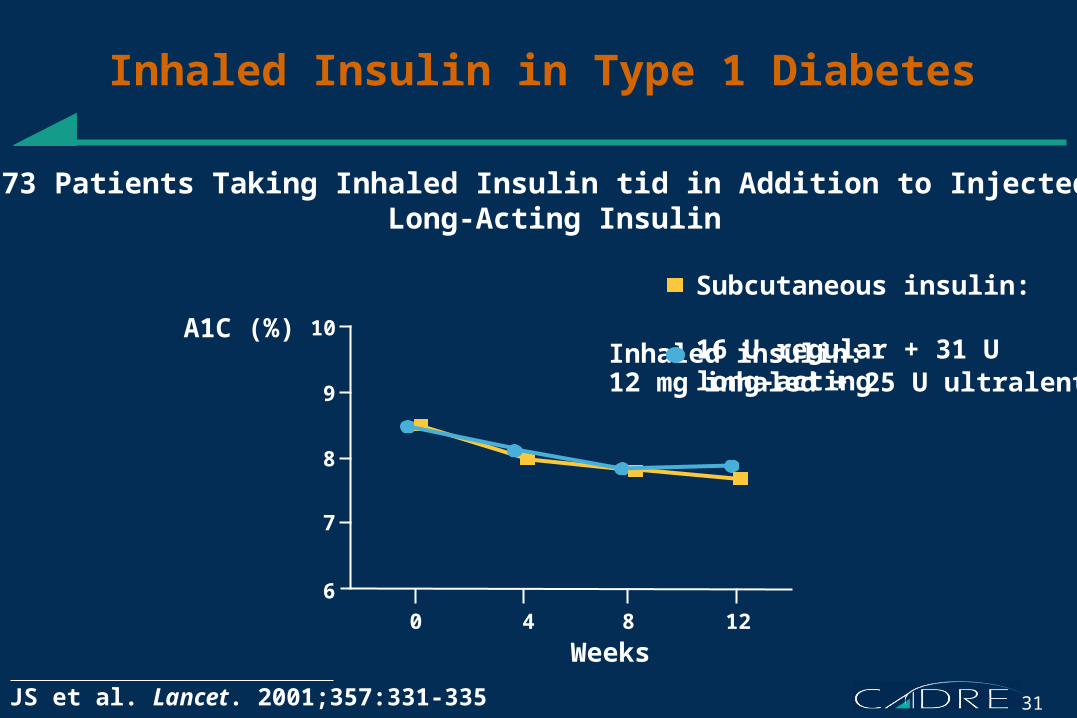
Subcutaneous insulin: 16 U regular + 31 U long-actingInhaled insulin: 12 mg inhaled + 25 U ultralente
Inhaled Insulin in Type 1 Diabetes
Skyler JS et al. Lancet. 2001;357:331-335
10
Weeks
A1C (%)
0 4 8 12
73 Patients Taking Inhaled Insulin tid in Addition to Injected Long-Acting Insulin
9
8
7
6
32
Δ A1C (%)(mean baseline, 8.7%)
2
Baseline Week 8 Week 12Week 4
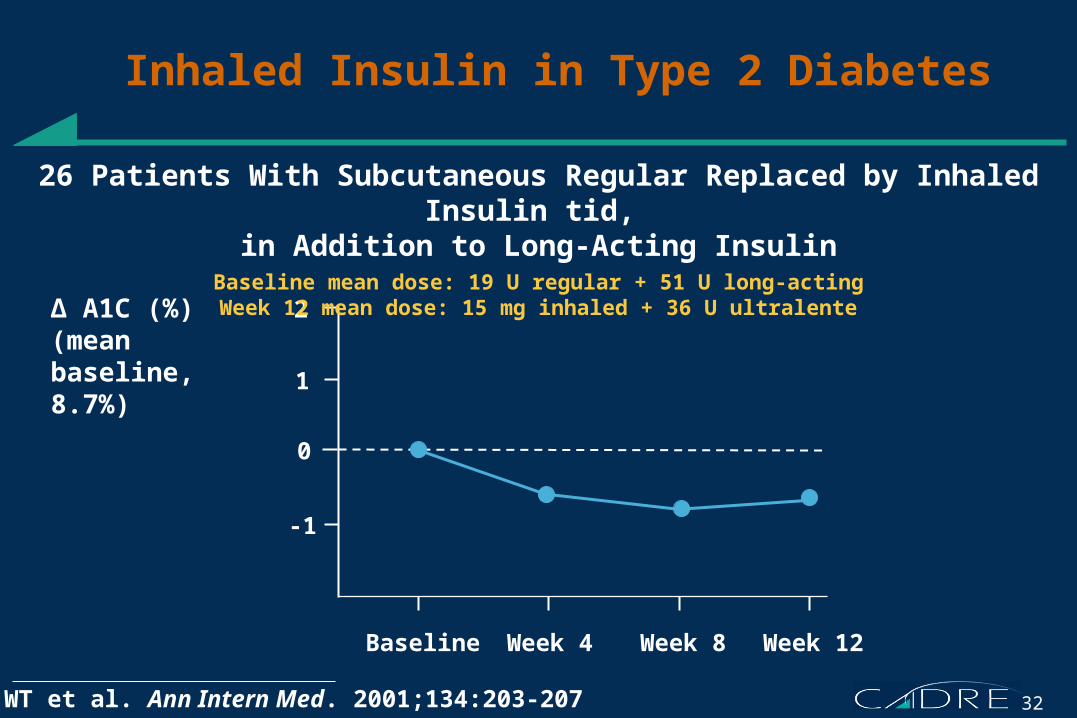
Inhaled Insulin in Type 2 Diabetes
Cefalu WT et al. Ann Intern Med. 2001;134:203-207
26 Patients With Subcutaneous Regular Replaced by Inhaled Insulin tid, in Addition to Long-Acting Insulin
Baseline mean dose: 19 U regular + 51 U long-actingWeek 12 mean dose: 15 mg inhaled + 36 U ultralente
1
0
-1
33
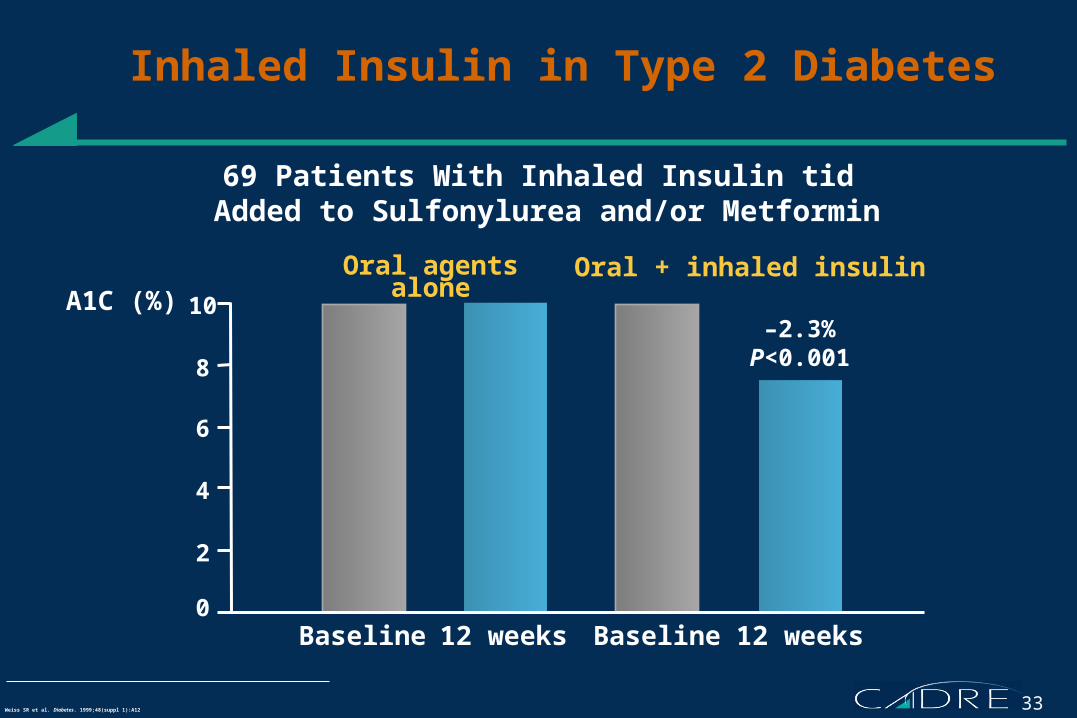
Inhaled Insulin in Type 2 Diabetes
Weiss SR et al. Diabetes. 1999;48(suppl 1):A12
10
8
6
4
0Baseline 12 weeks Baseline 12 weeks
–2.3%P<0.001
2
A1C (%)Oral agents alone Oral + inhaled insulin
69 Patients With Inhaled Insulin tid Added to Sulfonylurea and/or Metformin
34
11A1C (%)
Baseline 60 days 90 days30 days
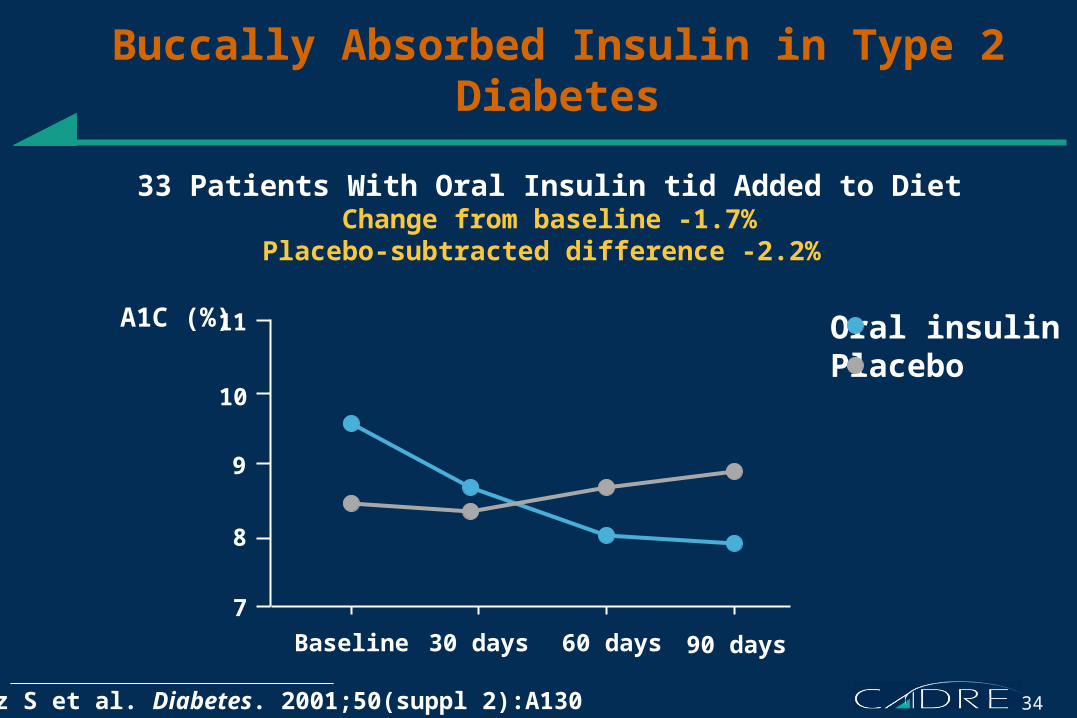
Buccally Absorbed Insulin in Type 2 Diabetes
Schwartz S et al. Diabetes. 2001;50(suppl 2):A130
Oral insulinPlacebo
33 Patients With Oral Insulin tid Added to DietChange from baseline -1.7%
Placebo-subtracted difference -2.2%
10
9
8
7
35
SummaryInsulin Therapy
• Replaces complete lack of insulin in type 1 diabetes
• Supplements progressive deficiency in type 2 diabetes
• Basal insulin added to oral agents can be used to start
• Full replacement requires a basal-bolus regimen
• Hypoglycemia and weight gain are the main medical risks
• New insulin analogues and injection devices facilitate use


















