Therapeutic Foster Care for Antisocial Youth Justine Harris Clinical Director Youth Horizons Trust...
47
Therapeutic Foster Care for Antisocial Youth Justine Harris Clinical Director Youth Horizons Trust Auckland, New Zealand
-
Upload
roxanne-hoover -
Category
Documents
-
view
214 -
download
0
Transcript of Therapeutic Foster Care for Antisocial Youth Justine Harris Clinical Director Youth Horizons Trust...
Therapeutic Foster Care for Antisocial Youth
Justine Harris
Clinical Director
Youth Horizons Trust
Auckland, New Zealand

Who is Youth Horizons Trust? NGO who specialises in working with young
people diagnosed with Severe Conduct Disorder Provide both community, foster care and
residential options Provides treatment to the young person, their
family and work with the community using systemic principles, parent management training and cognitive behavioural therapy

What is SCD?
Severe Conduct Disorder (DSM IV)
A pattern of behaviour where the rights of others or major age appropriate norms or rules are violated
Criteria for Conduct Disorder
Aggression Destruction of property Deceitfulness or theft Serious violation of
rules
Epidemiology 3-5% of children Increase in prevalence
after 12 years of age More common in boys
than girls 2:1
Aetiology
Studies suggest Parental antisocial behaviour Marital discord Poor parenting strategies Impaired patterns of interaction Genetic factors driving environmental
vulnerability.

What works for this client group?
“…not for the faint hearted” Emeritus Professor John Werry
Consistent parenting High monitoring Behaviour management Intervening across systems, peers, school etc Ensuring treatment generalisability
Why use therapeutic foster care?
Routes in deinstitutionalisation and foster care system
Cost effective Least restrictive environment Minimises the influence of peers with similar
problems Reduction in antisocial behaviour
Oregon Social Learning Centre Eugene, Oregon Part of University Parent Management Training (PMT) Multidimensional treatment foster care (MTFC) Started delivering services in 1983 High rates of incarceration in Oregon compared to other
states Treatment group – antisocial youth, hospitalised youth
with mental health problems, medical problem

MDFC
Model and theory Evidence and cost Caregiver interventions System intervention
Individual family therapySchool and peer interventions
Special Issues
Recruitment Training Supervision and case coordination Females Early intervention
Model and Theory
OSLC – pre MDFCProblems with delivering PMT in the communityProblem solving componentClinically difficult to treat
Conflict in familyInfluence of peer groupSafety of the community
Model and Theory continued
Residential option – influence of the peer groupE.g. positive peer cultureNo evidence for peer approaches Longitudinal research suggests that association with
delinquent peers result in development and escalation of delinquency
Long-term success based on support once the youth returns to the community
Group Home continued
Teaching families home Some successSmaller numbersSchool interventionsBehaviour mangmentRelationship with family home staff

Research on Delinquency & Drug Use
Condensed Longitudinal Model
Family
School
DelinquentPeers
DelinquentBehavior
Prior DelinquentBehavior
Low Parental MonitoringLow AffectionHigh Conflict
Low School InvolvementPoor Academic Performance
Elliott, Huizinga & Ageton (1985)
-
-
+
+
MDFC
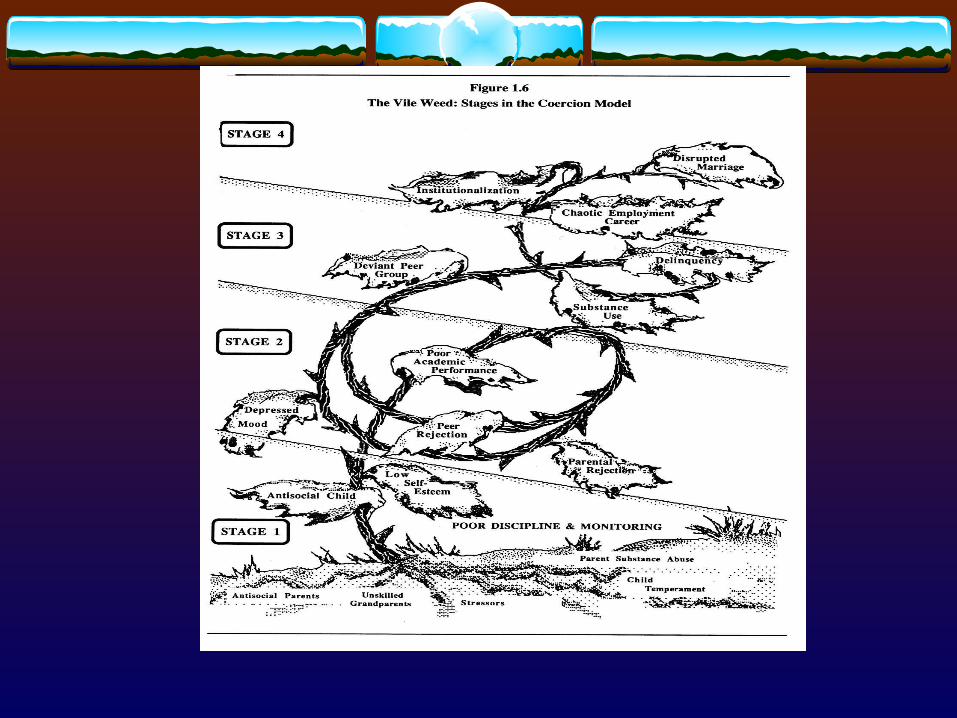
Began in 1983 Alternative to incarceration Based on the vile weed model – Stages in the
Coercion Model (Figure 9.1) Case study

Conduct problem development model
MDFC – research guiding practice
CD stable over time
Without intervention problems escalate
Childhood onset more severe
Impact on the environment and vice versa
Relating research to intervention
What works Interventions that target child, parent and environment“Multimodal interventions that simultaneously target
multiple settings and systems, although more expensive, complex, intensive and restrictive than single focused approaches to outpatient family therapy, show promise, for the treatmetn of such youths”
Chamberlain, 2003
Barriers that need to be overcome if treatment is to be successful
AttritionLikely to be severe casesImportance of engagement
Family stress and lack of social supportFamily therapy less successful when children are olderParents resistance to treatment
Family
DisciplinePermissive or rigidcoercion
Monitoring or supervision Structure consistency

Deviant Peer Group
Avoid aggregating peers Support and skill yp’s for association with
prosocial peer group
School
Coercive style with teachers and classmates Clear consistent rules Good supervision Reinforcement Social skills

Evidence Evaluations of MTFC have demonstrated that program youth
compared to control group youth: Spent 60% fewer days incarcerated at 12 month follow-up; Had significantly fewer subsequent arrests; Ran away from their programs, on average, three time less
often; Had significantly less hard drug use in the follow-up period;
and Quicker community placement from more restrictive settings
(e.g., hospital, detention).
Cost
The cost of the program per participant is $2,052 (extra to a group home)
Net financial benefits$21,836 to $87,622 (American $)
YHT caregiver programmeCaregivers receive contract fee per year of $30,000 Yp’s costCase coordination costs
Caregiver Interventions Emphasis on daily encouragement and reinforcing youths Individualised points systems – behaviour management
system Reinforcement and feedback
Material rewards more power for SCD yp’s
Teach prosocial behaviour Sanctions for behaviour problems
Tangible punishments more powerful
Three level system – less supervision as they go up the levels
Foster home environment Consistent tangible
rewards and sanctions
Immediately delivered
Teenage learn from feedback
Young Person’s Response
Low level of social skills Feel “hard done by” “destructive entitlement” Firm but fair approach with some room for
negotiation
Privileges and Rewards
They are well defined The fit the yp’s level of interest and maturity They must be affordable and readily available Criteria for reward should be realistic
Fines
Level 1 and 2 – points are taken for small infractions e.g. swearing, sulking
Caregivers take them away in a nonhostile and sympathetic way
Try to catch behaviours early in the sequence Lecturing ineffective
Working with the Family Preparing the family for the yp’s return from pre-entry Engagement – working with resistance Training and support PMT – weekly family therapy sessions
Behaviour management Discipline Supervision Improving communication and problem solving

Family Discipline
Taught to give corrective feedbackConsequences e.g. taking away pointsWays to control the parents own angerSequencing
Roleplays Communication, negotiation and problem solving Rules and regulations regarding home visits

Individual Therapy for the yp
Therapist seen as advocate and coach Steady support and encouragement Problem solving focus Facilitate adjustment to the programme and school Reenactment sessions Decreasing zapping amongst family members

Liaison with Schools
Wherever possible young people attend mainstream schools
Provide close supervision and follow-through Teach key staff principles of the programme Yp’s monitored On-call assistance for school staff School liaison worker

Peers
Close supervision and monitoring Teach pro-social skills so youth can attract non-
delinquent peer group Teach problems solving, and conflict resolution
Recruitment
Placing adds in local newspapers
Gulp!!I need a home for about a year! 12 year old girl who likes school needs a stable home. Prefer home with skilled parents where she can get plenty of attention. OSLC foster care program provides training, lots of support and monthly payment. For details contact….

Do You?Understand Impressionistic Art
Existential Philosophy, Quantum Physics …..
Then you are more than qualified to become a foster parent for the Oregon
Social Learning Centre. OSLC is looking for stable homes for children of various ages who need care for between 6 month – 1 yr. We provide training (no physics test
involved), lots of support (by a lively and philosophical staff), and $500 to $1200 per month (not just and impression) at
least phone in for details

4 Step Screening Process
Initial contact where programme is explained Application form and reference checks Home visit Screening with welfare services

Training
20 hour pre-service – with overview of TFC4 step process for analysing behaviour
Knowing when a problem is a problemDefining the problem behaviourExamine the antecedents of the problemChange the consequences that maintain the problem
Training cont
Procedure for using a 3-level system Working with the child’s natural family Common sources of stress on the team Treatment foster care policies and procedures On-call system and daily contact Foster parent support

Foster Parent Support
Foster parent meeting Clinical meeting Foster parent daily
structured feedback 24 / 7 on call support Respite care

Case consultation Case Manager (5 to 7
cases at a time) Daily contact Coordinate roles of
treatment team Supervises foster parents 24 hour crisis intervention Revises treatment plan as
needed

Females
In treatment girls behaviour worsened No differences in sexual behaviour or significant
female outcome Current adaptation of treatment programme

Adaptation of treatment programme (Patricia Chamberlain)
Address relational aggression
Address emotional dysregulation
Address risky sexual behaviour Female mentor
Focus on safety, stability and containment
Early Intervention
Preschoolers with behaviour problems Children with developmental delay Maltreated children

Summary MDFC – cost effective approach to dealing with SCD Provide a successful community living experience Effective principles
Consistent reinforcing environment Clear structure and limits Close supervision Prevent association with the youth and deviant peers and help
then develop appropriate peer relations