
Therapeutic Drug Monitoring (TDM) of Tyrosine Kinase Inhibitors (TKI) in MRCC
Upload
paula-gibbsCategory
view
220download
1
Therapeutic Drug Monitoring (TDM)
Arthur G. Roberts

Therapeutic Drug Monitoring (TDM)
• A.K.A.– clinical pharmacokinetic (laboratory) services
(CPKS)• Purpose– evaluate the response of the patient to the
recommended dosage regimen.• Benefits– Reduce cost and adverse affects


Appropriate Use of TDM
1. Maximizing & speeding up efficacy 2. Minimizing toxicity 3. Patient's drug history uncertain 4. Poor response to initial drug or deterioration after good
response5. Changing hepatic or renal function6. Drug-drug interactions (DDIs)7. Individualization of therapy8. Assist in future decisions about therapy9. Pharmacokinetic profiling

Considerations
• Number of drugs to monitor• How to monitor? – urine, [blood]P, response
• How many times to sample?– daily, hourly and continuous
• Personal, reagents and equipment needed

Monitoring
• [drug]P
– therapeutic response– adverse effects
• pharmacodynamic or “surrogate parameters”– clotting warfarin anticoagulant therapy– blood glucose monitoring in patients receiving
insulin products– chemotherapy severity of side effects and
patient’s ability to tolerate the drug
Situations where TDM is a limited value
• [drug]P doesn’t correlate to response.• Active metabolites complicate interpretation• Toxic effects can occur at any [drug]P
• No consequences with [drug]P
– wide therapeutic window (high therapeutic index)

Do not need TDM
• Clinical Endpoints Easily Monitored– blood pressure, heart rate, cardiac rhythm, body
temperature, urine volume and inflammation.
• [drug]p do correlate well to therapeutic or toxic effects

Do not need TDM (Example Drugs)
• wide therapeutic window– nonsteroidal anti-inflammatory drugs (NSAIDs)• ibuprofen
– calcium channel blocking agents• nifedipine
– over-the-counter (OTC) drugs• cough and cold remedies

Other potential problems and roadblocks to TDM
• Hospital personnel do not know the existence of a TDM service
• Physicians do not understand the principles, benefits, and the limitations of TDM service
• Inappropriate sampling times • Insufficient patient’s history and other
necessary data


Therapeutic Range for Commonly Monitored Drugs

Drugs Commonly Measured in Serum, Plasma, or Other Tissues

Functions
• Drug Selection• Dosage Regimen Design• Evaluate Patient Response• Need for measuring serum drug concentrations• [Drug] in bodily fluids• Pharmacokinetic evaluation• Dosage regimen adjustments• Drug abuse screening

Drug Selection

Designing Dosage Regimens

Designing Dosage Regimens: Factors
• Pregnancy, labor and delivery• Nursing mothers• Pediatric use• Geriatric use• Hepatic/Renal impairment• Gender• Pharmacogenomics (Ethnic groups)

Designing Dosage Regimens: Types
• Individualized– Pharmacokinetic
• Partial pharmacokinetic (Assumptions)
• Population Averages• Calculated from nomograms
and tabulations• Emperical
Characteristics of Drug Assays
• Specificity• Sensitivity• Linearity and Dynamic Range• Precision• Accuracy• Drug stability• Ruggedness/Robustness

Pharmacokinetic Evaluation of [Drug]P
• [Drug]P lower than anticipated
• [Drug]P higher than anticipated
• [Drug]P correct, but little/no response

Theophylline
caffeine
PDE=PhosphodiesterasePKA=Protein Kinase A

TDM
• Patient variability• DDIs• Fatty meals – dose dumping
• Adverse drug reactions– CNS excitation– heart problems
• low therapeutic index
FEV= Forced expiratory volume in asthmatic patients.
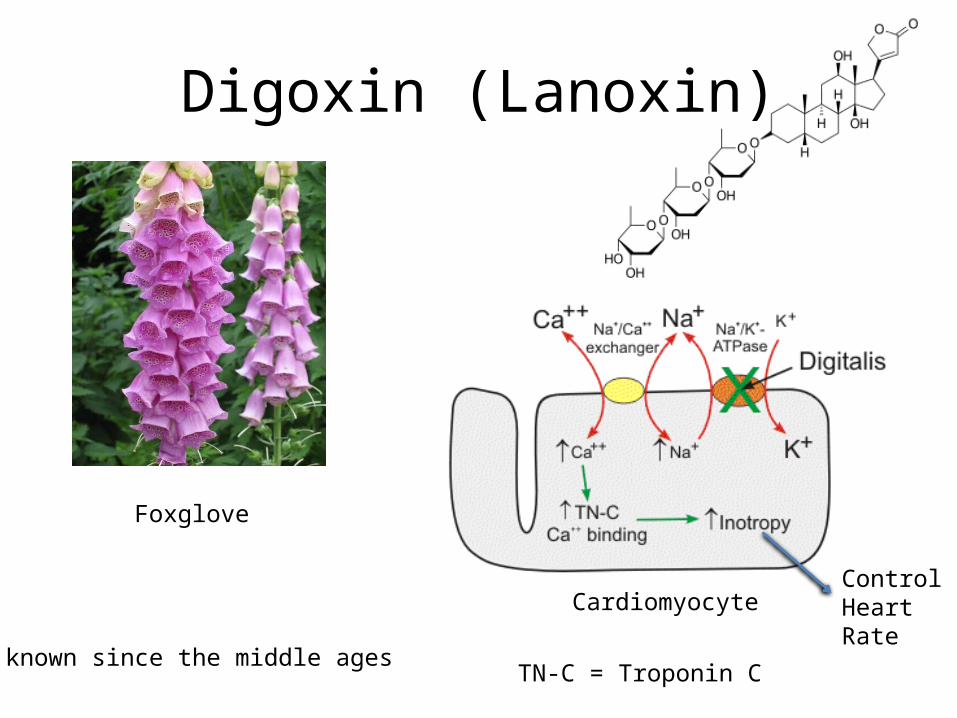
Digoxin (Lanoxin)
Cardiomyocyte
TN-C = Troponin C
Foxglove
known since the middle ages
ControlHeartRate

TDM
• Reasons and Concerns– Low Therapeutic Index
• [Drug]toxic/[Drug]therapeutic
• Therapeutic (0.5-2.0 ng/L)• Toxic (>2 ng/L)
– Electrolytes• Low [K+] (Hypokalemia)• High [Ca2+] or [Mg2+]
• Adverse Drug Reactions– worsening heart problems– xanthopsia (Vincent van Gogh’s “Yellow Period”)

Factors Considered
• Weight• Renal Function (Creatine Clearance)• Age– infants– advanced age (reduced renal function)

Antidote
• Digoxin immune fab (ovine)


















