The Yellow Cat: Diagnostic & Therapeutic Strategies · Due to septic peritonitis, hepatic abscess,...
13
TODAY’S VETERINARY PRACTICE | September/October 2016 | tvpjournal.com THE YELLOW CAT: DIAGNOSTIC & THERAPEUTIC STRATEGIES Peer Reviewed 38 There is no mystery when it comes to a “yellow” cat. Icterus and jaundice—both of which describe a yellowish pigmentation of the skin—indicate hyperbilirubinemia, a 5- to 10-fold elevation in serum bilirubin concentration. However, this is where the certainty ends and the diagnostic challenge begins. The icteric cat presentation is not a sensitive or specific marker of disease, despite the visually obvious and impressive clinical sign (Figure 1). 1 The objective of this article is to briefly review differentials for hyperbilirubinemia in the cat, and present a diagnostic and therapeutic strategy that will help practitioners approach this problem in an efficient and effective manner. HYPERBILIRUBINEMIA: ORGANIZATION BY LOCATION The differentials for hyperbilirubinemia should be organized by location: prehepatic, hepatic, and posthepatic. While, in cats, it is common to find concurrent disease processes, starting from this foundation is the first step toward an effective and efficient diagnostic workup of icteric cats. Prehepatic Disease Hemolysis releases hemoglobin, which is then metabolized through biliverdin to bilirubin in the liver. Hepatocytes in the healthy feline liver have a large capacity for uptake, conjugation, and excretion of bilirubin. Prehepatic icterus is most likely due to the combination of a large increase in bilirubin from hemolysis and a degree of intrahepatic cholestasis secondary to hypoxia. 2 In dogs, the most common cause of prehepatic hyperbilirubinemia is immune- mediated hemolytic anemia (IMHA), but that condition appears to be quite rare in cats. The list of prehepatic causes of hyperbilirubinemia in cats is extensive (Table 1, page 40). Hepatic Disease A significant decrease, or loss, of hepatocellular function effects bilirubin metabolism, and frequently results in intrahepatic cholestasis (Table 1, page 40). Unconjugated bilirubin from damaged hepatocytes is present, although the majority of bilirubin that appears in the cat’s circulation is conjugated, having completed the metabolic step prior to encountering the cholestatic overflow into the vasculature. 2 Posthepatic Disease Extrahepatic biliary disease interferes with the normal flow of bile and the final steps in bilirubin excretion, resulting in extrahepatic cholestasis (Table 1, page 40). As with intrahepatic disease, both unconjugated and conjugated bilirubin appear in the serum, rendering the biochemical distinction between conjugated and unconjugated serum bilirubin of minimal diagnostic importance. The Yellow Cat: Diagnostic & Therapeutic Strategies Craig B. Webb, PhD, DVM, Diplomate ACVIM (Small Animal Internal Medicine) Colorado State University CE ARTICLE FIGURE 1. Icteric pinna of a cat in the critical care isolation unit; prehepatic hemolysis and anemia are a result of Cytauxzoon felis infection. Hyperbilirubinemia results when serum bilirubin concentrations reach 2 to 3 mg/dL (35–50 mcmol/L).
Transcript of The Yellow Cat: Diagnostic & Therapeutic Strategies · Due to septic peritonitis, hepatic abscess,...

TODAY’S VETERINARY PRACTICE | September/October 2016 | tvpjournal.com
THE YELLOW CAT: DIAGNOSTIC & THERAPEUTIC STRATEGIESPeer Reviewed
38
There is no mystery when it comes to a “yellow” cat. Icterus and jaundice—both of which describe a yellowish pigmentation of the skin—indicate hyperbilirubinemia, a 5- to 10-fold elevation in serum bilirubin concentration.
However, this is where the certainty ends and the diagnostic challenge begins. The icteric cat presentation is not a sensitive or specific marker of disease, despite the visually obvious and impressive clinical sign (Figure 1).1
The objective of this article is to briefly review differentials for hyperbilirubinemia in the cat, and present a diagnostic and therapeutic strategy that will help practitioners approach this problem in an efficient and effective manner.
HYPERBILIRUBINEMIA: ORGANIZATION BY LOCATION The differentials for hyperbilirubinemia should be organized by location: prehepatic, hepatic, and posthepatic. While, in cats, it is common to find concurrent disease processes, starting from this foundation is the first step toward an effective and efficient diagnostic workup of icteric cats.
Prehepatic DiseaseHemolysis releases hemoglobin, which is then metabolized through biliverdin to bilirubin in the liver. Hepatocytes in the healthy feline liver have a large capacity for uptake, conjugation, and excretion of bilirubin.
Prehepatic icterus is most likely due to the combination of a large increase in bilirubin from hemolysis and a degree of intrahepatic cholestasis secondary to hypoxia.2 In dogs, the most common cause of prehepatic hyperbilirubinemia is immune-mediated hemolytic anemia (IMHA), but that condition appears to be quite rare in cats. The list of prehepatic causes of hyperbilirubinemia in cats is extensive (Table 1, page 40).
Hepatic DiseaseA significant decrease, or loss, of hepatocellular function effects bilirubin metabolism, and frequently results in intrahepatic cholestasis (Table 1, page 40). Unconjugated bilirubin from damaged hepatocytes is present, although the majority of bilirubin that appears in the cat’s circulation is conjugated, having completed the metabolic step prior to encountering the cholestatic overflow into the vasculature.2
Posthepatic DiseaseExtrahepatic biliary disease interferes with the normal flow of bile and the final steps in bilirubin excretion, resulting in extrahepatic cholestasis (Table 1, page 40). As with intrahepatic disease, both unconjugated and conjugated bilirubin appear in the serum, rendering the biochemical distinction between conjugated and unconjugated serum bilirubin of minimal diagnostic importance.
The Yellow Cat: Diagnostic & Therapeutic StrategiesCraig B. Webb, PhD, DVM, Diplomate ACVIM (Small Animal Internal Medicine) Colorado State University
CE ARTICLE
FIGURE 1. Icteric pinna of a cat in the critical care isolation unit; prehepatic hemolysis and anemia are a result of Cytauxzoon felis infection.Hyperbilirubinemia
results when serum bilirubin concentrations reach 2 to 3 mg/dL (35–50 mcmol/L).

tvpjournal.com | September/October 2016 | TODAY’S VETERINARY PRACTICE
THE YELLOW CAT: DIAGNOSTIC & THERAPEUTIC STRATEGIES Peer Reviewed
39
COMMON CAUSES OF PREHEPATIC HYPERBILIRUBINEMIAInfectious DiseaseInfectious disease is a relatively common cause of prehepatic hemolysis in cats.
Mycoplasma species, particularly Mycoplasma haemofelis, can cause significant erythrocyte destruction, anemia, hyperbilirubinemia, and clinical disease. Outdoor, male, and/or shelter cats appear to be at increased risk, and coinfection with feline immunodeficiency virus (FIV) is common.3-5
Concurrent diseases, immunosuppression, and stress appear to impact the course and severity of disease and outcome of treatment. An eventual recurrence of disease is seen with some frequency in those cats that show a clinical response to treatment.
Feline leukemia virus (FeLV) infection can trigger a host immune response that results in immune-mediated prehepatic erythrocyte destruction. This may be the result of a virus-induced expression of antigens on the red blood cell (RBC) surface. Immune-mediated thrombocytopenia may accompany IMHA in cats with underlying FeLV infection.6
Cytauxzoon felis is transmitted by ticks (Am-blyomma americanum) and appears to be increasing in prevalence and geographical distribution in the United States, expanding from the southeastern portion of the country. Risk for infection increases with increased exposure to the tick vector, and the progression of clinical disease is rapid and often fatal.
Babesia felis can cause severe prehepatic hemolysis and anemia in cats, but appears to be rare outside of costal South Africa.7
Immune-Mediated Hemolytic AnemiaPrimary IMHA appears to be quite rare in cats. It is difficult to characterize feline IMHA or determine risk factors because of the paucity of cases in the literature, but younger male cats may be overrepresented. The prognosis is guarded, with a mortality rate of 25%.8
Inherited Erythrocyte DisordersErythrocyte pyruvate kinase (PK) deficiency is a very rare inherited disorder transmitted as an autosomal recessive trait, causing prehepatic hemolysis.
Cats usually present as young adults, and the severity of the anemia and clinical signs is variable and may change over time, ranging from asymptomatic to hemolytic crisis.
The disease is most frequently described in Abyssinian and Somali breeds but may also be
present in a variety of other purebred and domestic shorthair cats.9 Interestingly, Abyssinian and Somali breeds have also been shown to suffer from another inherited cause of prehepatic hemolysis: increased erythrocyte osmotic fragility. Genetic testing has been developed for screening cats for PK deficiency and is commercially available (vgl.ucdavis.edu/services/pkdeficiency.php)
Other Causes of HemolysisHemolysis secondary to hypophosphatemia has become rare due to heightened awareness, diligent monitoring, and proactive intervention during the treatment of diabetic ketoacidosis.
Disseminated intravascular coagulation is also a rare occurrence, seen predominantly in the critical care setting, but serving as a reminder that prehepatic hemolysis can occur as a secondary consequence in a variety of diseases.
Feline erythrocytes are susceptible to oxidative stress, and a large variety of toxins and drugs (including acetaminophen, benzocaine, methylene blue, phenazopyridine, onions/onion powder, propylene glycol, and propylthiouracil) can cause Heinz body anemia or hemolytic destruction of RBC membranes.
COMMON CAUSES OF HEPATIC HYPERBILIRUBINEMIAFeline Hepatic LipidosisHepatic lipidosis appears to be a unique feline phenomenon, highlighting that hepatic metabolism in the cat is different from many other species.10 Although feline hepatic lipidosis may be an idiopathic (Figure 2) and, therefore, primary problem, it quite frequently occurs secondary to another disease that caused the cat to stop eating.
FIGURE 2. The liver (seen laparoscopically) of a cat with idiopathic hepatic lipidosis.

TODAY’S VETERINARY PRACTICE | September/October 2016 | tvpjournal.com
THE YELLOW CAT: DIAGNOSTIC & THERAPEUTIC STRATEGIESPeer Reviewed
40
TABLE 1. Hyperbilirubinemia in Cats: Differential Diagnoses & Clinical Signs
Ano
rexi
a
Leth
arg
y
Feve
r
Lym
pha
den
op
athy
Vo
mit
ing
/dia
rrhe
a
Wei
ght
loss
Ane
mia
Ab
do
min
al p
ain
OTHER CLINICAL SIGNS
PREHEPATIC HYPERBILIRUBINEMIA
Mycoplasma species23
x x xHypothermiaPhysiologic murmurIncreased heart rate/respiratory effort secondary to anemia
Cytauxzoon felis24
x x xDehydrationEvidence of shock Progression to moribund dyspnea and hypothermia
Feline infectious peritonitis x x x x Effusive/wet FIP: Ascites, pleural effusionDry FIP: Ocular and neurologic signs
Babesia species x x x x
Feline leukemia virus x Immune suppressionSecondary infection
Feline immunodeficiency virus x x x Oral inflammationSecondary infection and lymphoma
Immune-mediated hemolytic anemia8,25 x x x Signs of primary IMHA, excluding identifiable causes
Pica
Erythrocyte PK deficiency26
x x x xPica
Increased erythrocyte osmotic fragility27
Neonatal isoerythrolysis28
xCessation of nursing, failure to thriveDisseminated intravascular coagulationPigmenturia
Acute kidney injury Death
Transfusion reaction29
x x
Erythema or pruritusVocalizationDyspnea or tachypneaTachycardia or bradycardia
Tremor, convulsionShockCardiopulmonary arrest
Hypophosphatemia30,31,a
x x xClinical signs usually consistent with acute hemolysisWeaknessTachypnea, tachycardia
Microangiopathic hemolytic anemia32,b
x x x x
Clinical signs vary with condition and severityHyperthermiaObtundationCardiopulmonary arrest
Drugs, toxins, envenomation, oxidative stress c
Clinical signs nonspecific and depend on underlying etiology; may include clinical signs associated with Microangiopathic hemolytic anemia (above) and allergic reaction (eg, swelling, pain, redness, focal inflammation)
CholangitisIn contrast to dogs—in which hepatic disease is usually located in the liver parenchyma—feline liver disease typically targets the biliary system, and is most commonly seen as cholangitis. The World Small Animal Veterinary Association Liver Standardization Group clarified the terminology, defining feline cholangitis as neutrophilic (acute or chronic), lymphocytic, or secondary to liver flukes.11
COMMON CAUSES OF POSTHEPATIC HYPERBILIRUBINEMIAExtrahepatic Bile Duct ObstructionCholelithiasis may be obstructive and is, thus, approached as a cause of extrahepatic bile duct ob-struction (EHBO). Other causes of EHBO include tumors, nonneoplastic masses, cholecystitis, inspissat-ed bile, cholangitis, and pancreatitis. The prognosis, even following successful surgery, is guarded.
tvpjournal.com | September/October 2016 | TODAY’S VETERINARY PRACTICE
THE YELLOW CAT: DIAGNOSTIC & THERAPEUTIC STRATEGIES Peer Reviewed
41
TABLE 1. (continued)Hyperbilirubinemia in Cats: Differential Diagnoses & Clinical Signs
Ano
rexi
a
Leth
arg
y
Feve
r
Lym
pha
den
op
athy
Vo
mit
ing
/dia
rrhe
a
Wei
ght
loss
Ane
mia
Ab
do
min
al p
ain
OTHER CLINICAL SIGNS
HEPATIC HYPERBILIRUBINEMIA
Hepatic lipidosis33,34 x x x
Idiopathic or secondary hepatic lipidosisClinical signs vary with underlying etiologyHiding, decreased interaction
Cholangitis35,36 x x x x x
Bacterial, acute or chronic neutrophilic, lymphocyticDehydrationHepatomegaly
Feline infectious peritonitis37 See clinical signs of FIP (previous page)
Virulent systemic feline calicivirus
x
Oral ulcerationUpper respiratory signsEdemaUlcerative dermatitisConjunctivitis
Francisella tularensis38 x x x Tachypnea and tachycardia
Drugs, toxins39,40,d Nonspecific signs of intoxicationAcute hepatic failureDeath
Amyloidosis41 x
Familial, Siamese, and other types of amyloidosisSudden deathAcute abdominal bleeding
Sepsis Systemic inflammatory response syndrome42,e
x x xClinical signs associated with specific underlying etiologyCollapseBradycardia and hypotension
POSTHEPATIC HYPERBILIRUBINEMIA
Cholelithiasis43,44 See clinical signs associated with EHBO (below)
Extrahepatic biliary obstruction45
x x x x x CoagulopathyHypotension and shock
Triaditis46
x x x x x x Clinical signs may progress in cases of EHBO Hepatomegaly
Liver flukes47 (Platynosomum concinnum) x x x x
a. As a result of enteral alimentation, diabetes mellitus, diabetic ketoacidosis treatmentb. As a result of disseminated intravascular coagulation, neoplasia, pancreatitis, sepsis, systemic lupus erythematosus, heat strokec. As a result of exposure to zinc, onion, garlic, propylene glycol, naphthalene, benzocaine, methimazole, bees, spidersd. Such as oral benzodiazepines, acetaminophen, amanitin mushroomse. Due to septic peritonitis, hepatic abscess, pyothorax, pyometra
EHBO = extrahepatic bile duct obstruction; FIP = feline infectious peritonitis; IMHA = immune-mediated hemolytic anemia
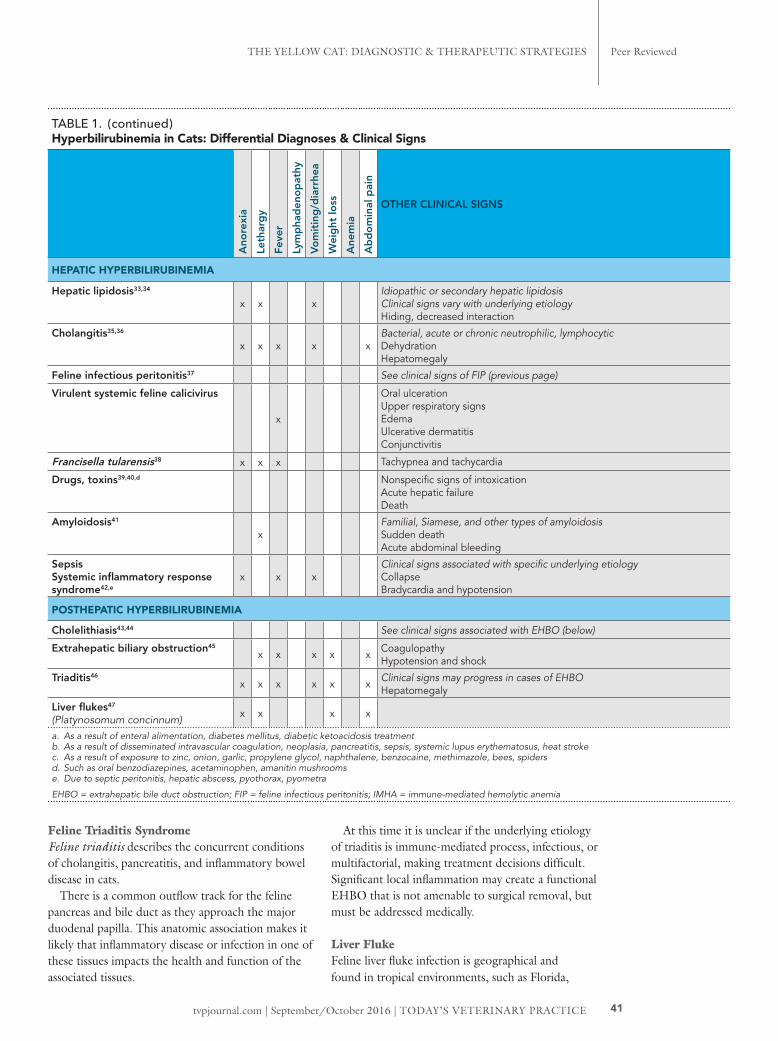
Feline Triaditis SyndromeFeline triaditis describes the concurrent conditions of cholangitis, pancreatitis, and inflammatory bowel disease in cats.
There is a common outflow track for the feline pancreas and bile duct as they approach the major duodenal papilla. This anatomic association makes it likely that inflammatory disease or infection in one of these tissues impacts the health and function of the associated tissues.
At this time it is unclear if the underlying etiology of triaditis is immune-mediated process, infectious, or multifactorial, making treatment decisions difficult. Significant local inflammation may create a functional EHBO that is not amenable to surgical removal, but must be addressed medically.
Liver FlukeFeline liver fluke infection is geographical and found in tropical environments, such as Florida,

TODAY’S VETERINARY PRACTICE | September/October 2016 | tvpjournal.com
THE YELLOW CAT: DIAGNOSTIC & THERAPEUTIC STRATEGIESPeer Reviewed
42
the Caribbean, and Hawaii, where land snails, lizards, and toads are the hosts. Infection is usually subclinical, although cats may present with nonspecific signs (Table 1).
DIAGNOSTIC APPROACH TO AN ICTERIC CATAs with any diagnostic approach, the clinical evaluation of an icteric cat begins with signalment, history, and physical examination.
SignalmentThe list of differentials for hyperbilirubinemia (Table 1) include breed-specific entries (eg, Abyssinian) and diseases that occur in certain age groups (eg, feline infectious peritonitis [FIP]). For many differentials the patient history is similar.
History & Clinical SignsAnorexia is a key component in the presentation of cats with hepatic lipidosis and appears to be an early clinical manifestation of anemia in cats. Lethargy
TABLE 2. Hyperbilirubinemia in Cats: Differential Diagnoses, Diagnostics, & Treatment
DIFFERENTIAL DIAGNOSES DIAGNOSTICS TREATMENT OPTIONS
PREHEPATIC HYPERBILIRUBINEMIA
Mycoplasma species23 Complete blood count (CBC)Blood smearSerum biochemical profilePolymerase chain reaction (PCR)
Doxycycline, 5 mg/kg PO Q 12 H for 14 dPradofloxacin, 5 mg/kg PO Q 24 H for 14 d Enrofloxacin, 5 mg/kg PO Q 24 H for 14 d
Cytauxzoon felis24 CBCBlood smearPCR
Atovaquone, 15 mg/kg PO Q 8 HAzithromycin, 10 mg/kg PO Q 24 H
Feline infectious peritonitisBabesia species
CBCBlood smearPCR
FIP: Supportive carePolyprenyl Immunostimulant (sassandsass.com)Pentoxifylline, 10 mg/kg PO Q 12 HPrednisolone, 2–4 mg/kg PO Q 24 H
Babesiosis: Imidocarb diproprionate, 2.5 mg/kg IMDoxycycline, 10 mg/kg/day PO for 21 d
Feline leukemia virusFeline immunodeficiency virus
FeLV: p27 antigen testFIV: Antibody test
Blood transfusionSupportive careAntiviral treatmentMedical therapy:• Prednisolone, 2.2 mg/kg Q 12 H• Cyclosporine, 5 mg/kg Q 24 H• Chlorambucil, 2 mg/cat Q 3 days• Mycophenolate mofetil, 10 mg/kg Q 12 H
Immune-mediated hemolytic anemia8,25 (primary, excluding identifiable causes)
Saline agglutinationCoombs’ testIn one report:8 Anemia was severe, with
median packed cell volume of 12%
Prednisolone, 2.2 mg/kg PO Q 12 HMycophenolate mofetil, 10 mg/kg Q 12 H
Erythrocyte PK deficiency26 Genetic testing Breeding practices Supportive careUrsodeoxycholic acid, 5−15 mg/kg Q 24 H
Increased erythrocyte osmotic fragility27
Neonatal isoerythrolysis28 Appropriate blood typing prior to breeding
Supportive careCardiovascular support
Transfusion reaction29 Pretesting donorsBlood-typingCrossmatching
Supportive careCardiovascular support
Hypophosphatemia30,31 Electrolyte monitoring Supportive careTreatment of underlying conditions
Microangiopathic hemolytic anemia32
CBC with plateletsClotting times
Intensive monitoringCardiovascular supportTreatment of underlying conditions
Drugs, toxins, envenomation, oxidative stress
Various toxin assaysBlood smear
Remove exposureReduce remaining burden (eg, emesis)Support of target organsPlasmapharesis
tvpjournal.com | September/October 2016 | TODAY’S VETERINARY PRACTICE
THE YELLOW CAT: DIAGNOSTIC & THERAPEUTIC STRATEGIES Peer Reviewed
43
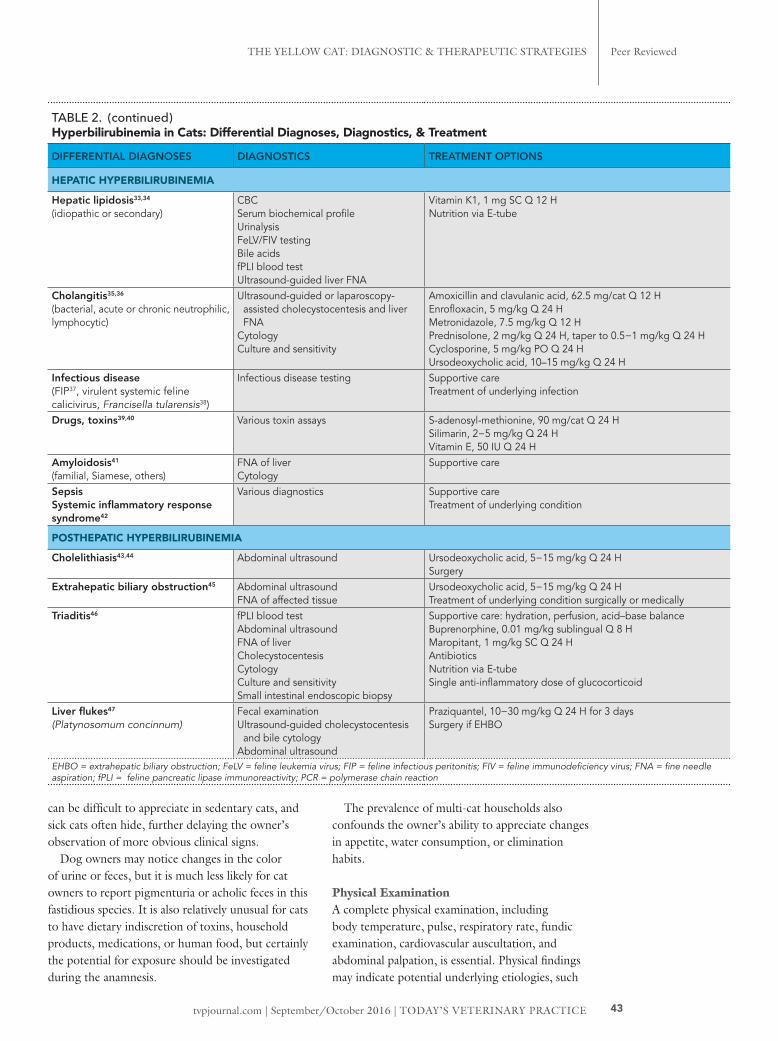
can be difficult to appreciate in sedentary cats, and sick cats often hide, further delaying the owner’s observation of more obvious clinical signs.
Dog owners may notice changes in the color of urine or feces, but it is much less likely for cat owners to report pigmenturia or acholic feces in this fastidious species. It is also relatively unusual for cats to have dietary indiscretion of toxins, household products, medications, or human food, but certainly the potential for exposure should be investigated during the anamnesis.
The prevalence of multi-cat households also confounds the owner’s ability to appreciate changes in appetite, water consumption, or elimination habits.
Physical ExaminationA complete physical examination, including body temperature, pulse, respiratory rate, fundic examination, cardiovascular auscultation, and abdominal palpation, is essential. Physical findings may indicate potential underlying etiologies, such
TABLE 2. (continued)Hyperbilirubinemia in Cats: Differential Diagnoses, Diagnostics, & Treatment
DIFFERENTIAL DIAGNOSES DIAGNOSTICS TREATMENT OPTIONS
HEPATIC HYPERBILIRUBINEMIA
Hepatic lipidosis33,34 (idiopathic or secondary)
CBCSerum biochemical profileUrinalysisFeLV/FIV testingBile acidsfPLI blood testUltrasound-guided liver FNA
Vitamin K1, 1 mg SC Q 12 HNutrition via E-tube
Cholangitis35,36 (bacterial, acute or chronic neutrophilic, lymphocytic)
Ultrasound-guided or laparoscopy-assisted cholecystocentesis and liver FNA
CytologyCulture and sensitivity
Amoxicillin and clavulanic acid, 62.5 mg/cat Q 12 HEnrofloxacin, 5 mg/kg Q 24 HMetronidazole, 7.5 mg/kg Q 12 HPrednisolone, 2 mg/kg Q 24 H, taper to 0.5−1 mg/kg Q 24 HCyclosporine, 5 mg/kg PO Q 24 HUrsodeoxycholic acid, 10–15 mg/kg Q 24 H
Infectious disease (FIP37, virulent systemic feline calicivirus, Francisella tularensis38)
Infectious disease testing Supportive careTreatment of underlying infection
Drugs, toxins39,40 Various toxin assays S-adenosyl-methionine, 90 mg/cat Q 24 HSilimarin, 2−5 mg/kg Q 24 HVitamin E, 50 IU Q 24 H
Amyloidosis41 (familial, Siamese, others)
FNA of liverCytology
Supportive care
Sepsis Systemic inflammatory response syndrome42
Various diagnostics Supportive careTreatment of underlying condition
POSTHEPATIC HYPERBILIRUBINEMIA
Cholelithiasis43,44 Abdominal ultrasound Ursodeoxycholic acid, 5−15 mg/kg Q 24 HSurgery
Extrahepatic biliary obstruction45 Abdominal ultrasoundFNA of affected tissue
Ursodeoxycholic acid, 5−15 mg/kg Q 24 HTreatment of underlying condition surgically or medically
Triaditis46 fPLI blood testAbdominal ultrasoundFNA of liverCholecystocentesisCytologyCulture and sensitivitySmall intestinal endoscopic biopsy
Supportive care: hydration, perfusion, acid–base balanceBuprenorphine, 0.01 mg/kg sublingual Q 8 HMaropitant, 1 mg/kg SC Q 24 HAntibioticsNutrition via E-tubeSingle anti-inflammatory dose of glucocorticoid
Liver flukes47 (Platynosomum concinnum)
Fecal examinationUltrasound-guided cholecystocentesis
and bile cytologyAbdominal ultrasound
Praziquantel, 10−30 mg/kg Q 24 H for 3 daysSurgery if EHBO
EHBO = extrahepatic biliary obstruction; FeLV = feline leukemia virus; FIP = feline infectious peritonitis; FIV = feline immunodeficiency virus; FNA = fine needle aspiration; fPLI = feline pancreatic lipase immunoreactivity; PCR = polymerase chain reaction

TODAY’S VETERINARY PRACTICE | September/October 2016 | tvpjournal.com
THE YELLOW CAT: DIAGNOSTIC & THERAPEUTIC STRATEGIESPeer Reviewed
44
as hepatomegaly with hepatic lipidosis, cranial abdominal discomfort with pancreatitis, and tachycardia with anemia.
The physical examination is often dominated by the color of the cat. Icterus is best appreciated as a discoloration of the mucous membranes, the sclera (Figure 3), and/or the inner aspect of the pinnae (Figure 4). The intensity and actual color may be influenced by the normal tissue color, degree of anemia, and perfusion.
The clinical condition and color of the cat are influenced by both the degree of anemia—mild to severe—and the time course of RBC destruction—acute or chronic.
Laboratory AnalysisChanges on the serum biochemical profile are nonspecific. The degree of elevation in total bilirubin is cited as a nonspecific but generally guides to the most likely location or etiology of the problem:
• 3 to 6 mg/dL is associated with prehepatic hemolysis, FIP, pancreatitis, and sepsis
• Greater than 12 mg/dL is associated with hepatic lipidosis and EHBO.
PREHEPATIC HYPERBILIRUBINEMIA DIAGNOSTICSBlood AnalysisThe laboratory diagnostic workup for the vast majority of icteric cats starts with determining whether prehepatic hemolysis is present.
Complete Blood CountHemolysis can often be an extravascular antibody-mediated process in which the serum turns icteric. A simple hematocrit tube can be expected to identify a significant degree of anemia and a relatively normal serum total protein. Less frequently, the hemolysis occurs within the vasculature itself, in which case the serum may appear pink, while both the plasma (hemoglobinemia) and urine (hemoglobinuria) appear red.
A complete blood count (CBC) more accurately and completely characterizes the anemia as regenerative or nonregenerative; however, the regenerative process may take up to 5 days to manifest as an appropriate increase in the absolute reticulocyte count (> 40,000–60,000/mcL, depending on the laboratory). A CBC also identifies other potentially important erythrocyte characteristics.
The degree of anemia is cited as a nonspecific but general indictor of the likelihood that feline icterus is the result of prehepatic hemolysis. As a rule of thumb, prehepatic hemolysis usually results in a packed cell volume (PCV) of less than 13% to 20%; however, the cat’s baseline or normal PCV, hydration status, and the time frame over which the hemolysis occurred may all impact the clinical signs, measured PCV, and elevation in total bilirubin.
Blood SmearCareful examination of the blood smear is a critical step in any attempt to identify infectious organisms or indicators of immune-mediated agglutination.
Infectious DiseaseInfectious disease testing is commonly used for prehepatic hyperbilirubinemia (Table 2, page 42).
MycoplasmosisIn addition to hyperbilirubinemia, cats with mycoplasmosis are frequently hyperglobulinemic as a
FIGURE 3. The sclera of the feline immune-mediated hemolytic anemia patient.
FIGURE 4. The pinna of the feline immune-mediated hemolytic anemia patient.
tvpjournal.com | September/October 2016 | TODAY’S VETERINARY PRACTICE
THE YELLOW CAT: DIAGNOSTIC & THERAPEUTIC STRATEGIES Peer Reviewed
45
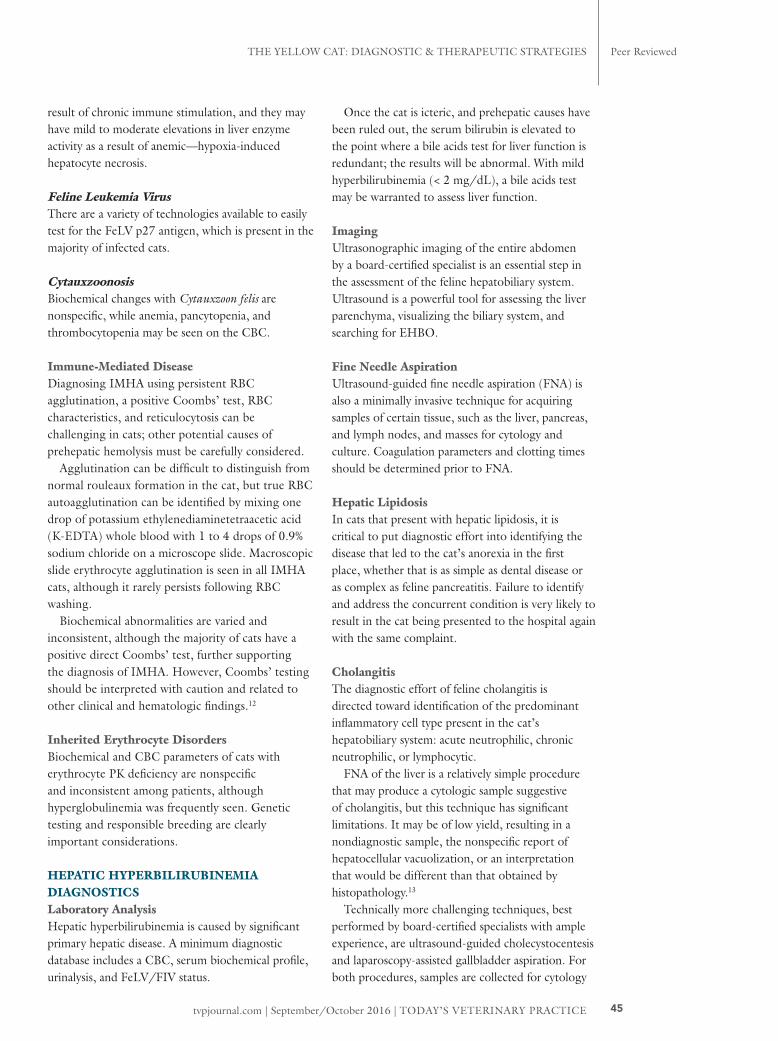
result of chronic immune stimulation, and they may have mild to moderate elevations in liver enzyme activity as a result of anemic—hypoxia-induced hepatocyte necrosis.
Feline Leukemia VirusThere are a variety of technologies available to easily test for the FeLV p27 antigen, which is present in the majority of infected cats.
CytauxzoonosisBiochemical changes with Cytauxzoon felis are nonspecific, while anemia, pancytopenia, and thrombocytopenia may be seen on the CBC.
Immune-Mediated DiseaseDiagnosing IMHA using persistent RBC agglutination, a positive Coombs’ test, RBC characteristics, and reticulocytosis can be challenging in cats; other potential causes of prehepatic hemolysis must be carefully considered.
Agglutination can be difficult to distinguish from normal rouleaux formation in the cat, but true RBC autoagglutination can be identified by mixing one drop of potassium ethylenediaminetetraacetic acid (K-EDTA) whole blood with 1 to 4 drops of 0.9% sodium chloride on a microscope slide. Macroscopic slide erythrocyte agglutination is seen in all IMHA cats, although it rarely persists following RBC washing.
Biochemical abnormalities are varied and inconsistent, although the majority of cats have a positive direct Coombs’ test, further supporting the diagnosis of IMHA. However, Coombs’ testing should be interpreted with caution and related to other clinical and hematologic findings.12
Inherited Erythrocyte DisordersBiochemical and CBC parameters of cats with erythrocyte PK deficiency are nonspecific and inconsistent among patients, although hyperglobulinemia was frequently seen. Genetic testing and responsible breeding are clearly important considerations.
HEPATIC HYPERBILIRUBINEMIA DIAGNOSTICSLaboratory AnalysisHepatic hyperbilirubinemia is caused by significant primary hepatic disease. A minimum diagnostic database includes a CBC, serum biochemical profile, urinalysis, and FeLV/FIV status.
Once the cat is icteric, and prehepatic causes have been ruled out, the serum bilirubin is elevated to the point where a bile acids test for liver function is redundant; the results will be abnormal. With mild hyperbilirubinemia (< 2 mg/dL), a bile acids test may be warranted to assess liver function.
ImagingUltrasonographic imaging of the entire abdomen by a board-certified specialist is an essential step in the assessment of the feline hepatobiliary system. Ultrasound is a powerful tool for assessing the liver parenchyma, visualizing the biliary system, and searching for EHBO.
Fine Needle AspirationUltrasound-guided fine needle aspiration (FNA) is also a minimally invasive technique for acquiring samples of certain tissue, such as the liver, pancreas, and lymph nodes, and masses for cytology and culture. Coagulation parameters and clotting times should be determined prior to FNA.
Hepatic LipidosisIn cats that present with hepatic lipidosis, it is critical to put diagnostic effort into identifying the disease that led to the cat’s anorexia in the first place, whether that is as simple as dental disease or as complex as feline pancreatitis. Failure to identify and address the concurrent condition is very likely to result in the cat being presented to the hospital again with the same complaint.
CholangitisThe diagnostic effort of feline cholangitis is directed toward identification of the predominant inflammatory cell type present in the cat’s hepatobiliary system: acute neutrophilic, chronic neutrophilic, or lymphocytic.
FNA of the liver is a relatively simple procedure that may produce a cytologic sample suggestive of cholangitis, but this technique has significant limitations. It may be of low yield, resulting in a nondiagnostic sample, the nonspecific report of hepatocellular vacuolization, or an interpretation that would be different than that obtained by histopathology.13
Technically more challenging techniques, best performed by board-certified specialists with ample experience, are ultrasound-guided cholecystocentesis and laparoscopy-assisted gallbladder aspiration. For both procedures, samples are collected for cytology

TODAY’S VETERINARY PRACTICE | September/October 2016 | tvpjournal.com
THE YELLOW CAT: DIAGNOSTIC & THERAPEUTIC STRATEGIESPeer Reviewed
46
and culture, since bile has been shown to be the sample most likely to yield an informative bacterial culture result.14,15
Liver biopsy is required for a definitive diagnosis of hepatic disease.16
The most common infectious organisms found in patients with neutrophilic cholangitis are enteric bacteria (eg, E coli, Enterobacter, Clostridia) and antibiotics for treatment should be selected based on sensitivity.
POSTHEPATIC HYPERBILIRUBINEMIA DIAGNOSTICSExtrahepatic Bile Duct ObstructionAbdominal ultrasound of cats with EHBO frequently identifies distension of the gallbladder, common bile duct, and intrahepatic ducts (Figure 5).
TriaditisDiagnosis of triaditis is based on identification of disease in each of the 3 tissues involved; the gold standard for diagnosis is histopathology. Less invasive diagnostics include the feline pancreatic lipase immu-noreactivity (fPLI) blood test, abdominal ultrasound, liver FNA, cholecystocentesis, cytology, culture and sensitivity, and small intestinal endoscopic biopsy; however, these patients may have increased anesthetic risks.
Although not widely available in private practice, feline abdominal laparoscopy can be performed with equipment sized for pediatrics and allows the collection of tissue for histopathology (liver and pancreas) as well as direct aspiration of the gallbladder (Figure 6).
Liver FlukeLiver fluke eggs can sometimes be found in the feces or by bile cytology. A recent study assessing the use of percutaneous ultrasound-guided cholecystocentesis in cats known to be infected with Platynosomum species flukes found the technique to be technically feasible and safe in cats with cholangitis.17
THERAPEUTIC APPROACHDetailed treatment protocols for specific differentials are beyond the scope of this article. However, some selected therapies are described.
Hydration status, pain (buprenorphine, 0.01 mg/kg sublingual Q 8 H), and vomiting (maropitant, 1 mg/kg SC Q 24 H) can all be addressed in a relatively effective manner and can significantly impact the clinical outcome.
Ursodeoxycholic acid (5−15 mg/kg Q 24 H) is an adjunct therapy that has been used in the successful treatment of bilirubin cholelithiasis, EHBO, and a Somali cat with PK deficiency, but it should not be used in place of antibiotics or prednisolone for lymphocytic cholangitis and neutrophilic cholangitis, respectively.18
Adjunct therapy may include S-adenosyl-methionine (90 mg/cat Q 24 H), silimarin (2−5 mg/kg Q 24 H), and/or vitamin E (50 IU Q 24 H); however, there may be a limit to the number of medications an owner can administer to a cat.
Selected Prehepatic Hyperbilirubinemia Treatment OptionsImmune-Mediated Hemolytic AnemiaIn addition to supportive care, including blood products, cats with IMHA appeared to respond
FIGURE 6. Laparoscopic-assisted aspiration of the gallbladder in an icteric cat.
FIGURE 5. Abdominal ultrasound demonstrating a distended gallbladder and enlarged biliary outflow tract in a cat with EHBO.
tvpjournal.com | September/October 2016 | TODAY’S VETERINARY PRACTICE
THE YELLOW CAT: DIAGNOSTIC & THERAPEUTIC STRATEGIES Peer Reviewed
47
to prednisolone therapy, although additional immunosuppressive drugs have also been used.
Anecdotal and case reports discuss the addition of cyclosporine (5 mg/kg Q 24 H), chlorambucil (2 mg/cat every 3 days), and mycophenolate mofetil (10 mg/kg Q 12 H) to treatment protocols, especially if prednisolone fails to improve the cat’s anemia.19,20
Feline Leukemia VirusAlthough immunosuppression in FeLV positive cats is best avoided, in those patients with clear evidence of IMHA secondary to FeLV infection, blood transfusions are indicated and, if those fail, prednisolone (2.2 mg/kg Q 12 H) may be used as with primary IMHA patients.8,21
Erythrocyte PK DeficiencyTherapy for erythrocyte PK deficiency is supportive and nonspecific, and outcome depends, in large part, on the severity of presentation and use of transfusions to stabilize critical patients.
Selected Hepatic Hyperbilirubinemia Treatment OptionsTreatment of hepatic causes of hyperbilirubinemia is best guided by histopathology, when possible, or cytology and culture.
Hepatic LipidosisThe foundation of treatment for hepatic lipidosis is relatively simple: provide nutrition to the cat. The logistics may be challenging but the advent of esophagostomy tubes (E-tube) makes both nutrition and medication administration easier (Figure 7).
Nutrition is critical; therefore, placement of an E-tube should be encouraged early in the disease process if the cat is anorectic.
Vitamin K1 (1 mg SC Q 12 H) should be administered prior to E-tube placement if evidence of a coagulopathy is present.
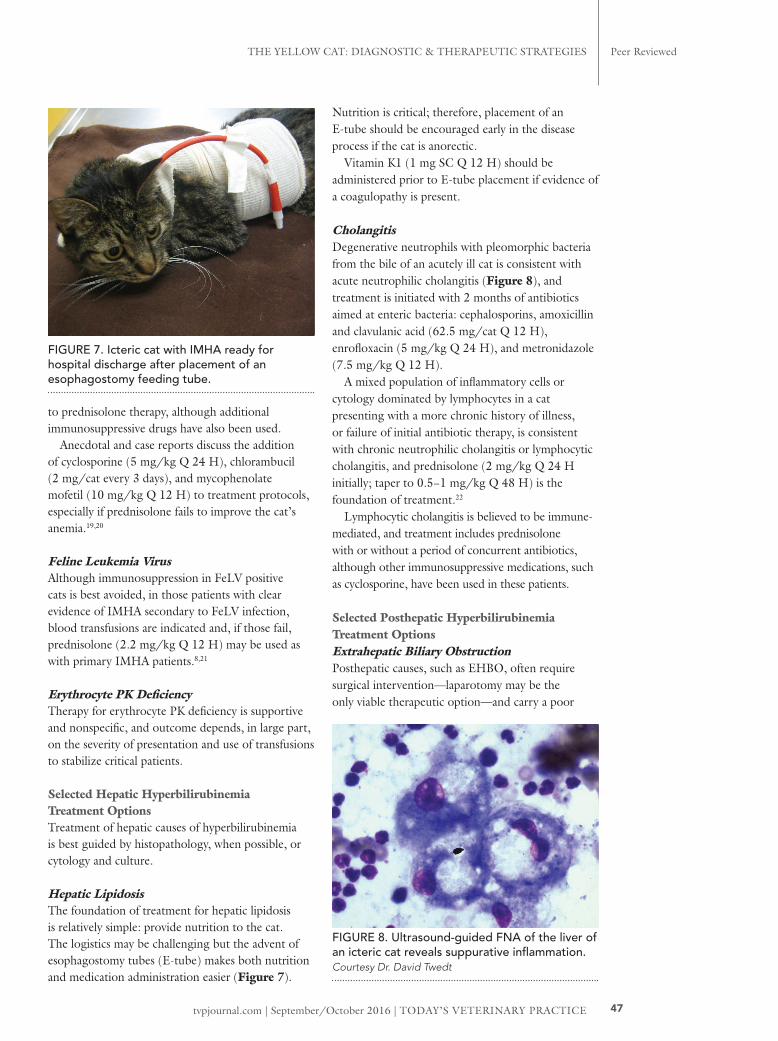
CholangitisDegenerative neutrophils with pleomorphic bacteria from the bile of an acutely ill cat is consistent with acute neutrophilic cholangitis (Figure 8), and treatment is initiated with 2 months of antibiotics aimed at enteric bacteria: cephalosporins, amoxicillin and clavulanic acid (62.5 mg/cat Q 12 H), enrofloxacin (5 mg/kg Q 24 H), and metronidazole (7.5 mg/kg Q 12 H).
A mixed population of inflammatory cells or cytology dominated by lymphocytes in a cat presenting with a more chronic history of illness, or failure of initial antibiotic therapy, is consistent with chronic neutrophilic cholangitis or lymphocytic cholangitis, and prednisolone (2 mg/kg Q 24 H initially; taper to 0.5−1 mg/kg Q 48 H) is the foundation of treatment.22
Lymphocytic cholangitis is believed to be immune-mediated, and treatment includes prednisolone with or without a period of concurrent antibiotics, although other immunosuppressive medications, such as cyclosporine, have been used in these patients.
Selected Posthepatic Hyperbilirubinemia Treatment OptionsExtrahepatic Biliary ObstructionPosthepatic causes, such as EHBO, often require surgical intervention—laparotomy may be the only viable therapeutic option—and carry a poor
FIGURE 8. Ultrasound-guided FNA of the liver of an icteric cat reveals suppurative inflammation. Courtesy Dr. David Twedt
FIGURE 7. Icteric cat with IMHA ready for hospital discharge after placement of an esophagostomy feeding tube.

TODAY’S VETERINARY PRACTICE | September/October 2016 | tvpjournal.com
THE YELLOW CAT: DIAGNOSTIC & THERAPEUTIC STRATEGIESPeer Reviewed
48
prognosis. Nonsurgical causes, such as pancreatitis and cholangitis, are medically managed and the prognosis is impacted by the severity of disease, response to treatment, and owner commitment.
TriaditisThe effective treatment of triaditis is complicated, but is initiated with supportive care targeting hydration, perfusion, electrolyte and acid–base balance, pain, and vomiting; then targets the aspect of the disease constellation that appears to be having the greatest impact on the patient.
Antibiotics are administered in patients in which there is the potential for sepsis, gastrointestinal translocation, positive bacterial cultures, or a left shift with band neutrophils on the CBC.
Corticosteroids are usually avoided in the face of a positively identified bacterial component, although a single anti-inflammatory dose of glucocorticoid may be used to counter the inflammatory mediators. With-out strong evidence of a bacterial infection, corticoste-roids are often used to treat each separate component of feline triaditis: inflammatory bowel disease, pancre-atitis, and lymphocytic-plasmacytic cholangitis.
Nutritional support in the form of E-tube placement is often implemented.
Liver FlukeMedical treatment for liver fluke infection may be attempted with praziquantel (20−30 mg/kg Q 24 H for 3 days), but rare, severe cases may require surgery to remove a posthepatic biliary obstruction as identified with abdominal ultrasound.
IN SUMMARYA thoughtful approach to hyperbilirubinemia, starting with localization of the disease and including the calculated consideration of differentials unique to that location, greatly enhances the efficient and effective diagnosis and treatment of the “yellow cat.” Orga-nizing the effort in terms of pre-hepatic, hepatic, and post-hepatic conditions is a logical and time-tested approach that has been successfully applied to many icteric cats.
CBC = complete blood count; EBHO = extrahepatic biliary obstruction; E-tube = esophagostomy tube; FeLV = feline leukemia virus; FIP = feline infectious peritonitis; FIV = feline immunodeficiency virus; FNA = fine needle aspiration; IMHA = immune-mediated hemolytic anemia; PCV = packed cell volume; PK = pyruvate kinase; RBC = red blood cell
References1. Sherding RG. Feline jaundice. J Fel Med Surg 2000; 2(3):165-
169.2. Sherding RG. Icterus. In Washabau RJ, Day MJ (eds): Canine
and Feline Gastroenterology. St. Louis: Elsevier, 2013, pp 140-147.
3. Jenkins KS, Dittmer KE, Marschall JC, et al. Prevalence and risk factor analysis of feline haemoplasma infection in New Zealand domestic cats using a real-time PCR assay. J Feline Med Surg 2013; 15:1063-1069.
4. Duarte A, Marques V, Correia JH, et al. Molecular detection of haemotropic Mycoplasma species in urban and rural cats from Portugal. J Feline Med Surg 2015;17:516-522.
5. Walker VR, Morera GF, Gómez JM, et al. Prevalence, risk factor analysis, and hematological findings of hemoplasma infection in domestic cats from Valdivia, Southern Chile. Comp Immunol Microbiol Infect Dis 2016; 46:20-26.
6. Hartmann K. Clinical aspects of feline retroviruses: A review. Viruses 2012; 4:2684-2710.
7. Hartmann K, Addie D, Belák S, et al. Babesiosis in cats: ABCD guidelines on prevention and management. J Feline Med Surg 2013; 15(7):643-646.
8. Kohn B, Weingart C, Eckmann V, et al. Primary immune-mediated hemolytic anemia in 19 cats: Diagnosis, therapy, and outcome (1998-2004). J Vet Intern Med 2006; 20(1):159-166.
9. Grahn RA, Grahn JC, Penedo MC, et al. Erythrocyte pyruvate kinase deficiency mutation identified in multiple breeds of domestic cats. BMC Vet Res 2012; 8:207-217.
10. Verbrugghe A, Bakovic M. Peculiarities of one-carbon metabolism in the strict carnivorous cat and the role in feline hepatic lipidosis. Nutrients 2013; 5:2811-2835.
11. Van den Ingh TS, Van Winkle T, Cullen JM, et al. Morphological classification of parenchymal disorders of the canine and feline liver: 2. Hepatocellular death, hepatitis and cirrhosis. In Rothuizen J, Bunch SE, Charles JE, et al: WSAVA Standards for Clinical and Histological Diagnosis of Canine and Feline Liver Diseases. Philadelphia: Elsevier, 2006, pp 85-101.
12. Wardrop KJ. Coombs’ testing and its diagnostic significance in dogs and cats. Vet Clin North Am Small Animal Pract 2012; 42:43-51.
13. Wang KY, Panciera DL, Al Rukivat RK, et al. Accuracy of ultrasound-guided fine-needle aspiration of the liver and cytologic findings in dogs and cats: 97 cases (1990-2000). JAVMA 2004; 224(1):75-78.
14. Wagner KA, Hartmann FA, Trepanier LA. Bacterial culture results from liver, gallbladder, or bile in 248 dogs and cats evaluated for hepatobiliary disease: 1998-2003. J Vet Intern Med 2007; 21:417-424.
15. Peters LM, Glanemann B, Garden OA, et al. Cytological findings of 140 bile samples from dogs and cats and associated clinical pathological data. J Vet Intern Med 2016; 30:123-131.
16. Rothuizen J, Twedt DC. Liver biopsy techniques. Vet Clin North Am Sm Anim Pract 2009; 39:469-480.8.
17. Koster L, Shell L, Illanes O, et al. Percutaneous ultrasound-guided cholecystocentesis and bile analysis for detection of Platynosomum spp.-induced cholangitis in cats. J Vet Intern Med 2016; 30(3):787-793.
18. Harvey AM, Holt PE, Barr FJ, et al. Treatment and long-term follow-up of extrahepatic biliary obstruction with bilirubin cholelithiasis in a Somali cat with pyruvate kinase deficiency. J Feline Med Surg 2007; 9(5):424-431.
CRAIG B. WEBBCraig B. Webb, PhD, DVM, Diplomate ACVIM (Small Animal Internal Medicine), is a professor in the clinical sciences department at Colorado State University (CSU) and head of the small animal medicine section. Dr. Webb specializes in gastroenterology and hepatology and, along with Drs. David Twedt and Eric Monnet, teaches the CSU CE Endoscopy & Laparoscopy course as well as the ACVIM Dry-Lab Laparoscopy course. Dr. Webb’s research interests include chronic enteropathies, oxidative stress, nutraceuticals, and the use of stem cell therapy in small animal patients. He received his DVM from the University of Wisconsin–Madison.

tvpjournal.com | September/October 2016 | TODAY’S VETERINARY PRACTICE
THE YELLOW CAT: DIAGNOSTIC & THERAPEUTIC STRATEGIES Peer Reviewed
49
19. Black V, Adamantos S, Barfield D, et al. Feline non-regenerative immune-mediated anaemia: Features and outcome in 15 cases. J Feline Med Surg 2015; 26:1-6.
20. Bacek LM, Macintire DK. Treatment of primary immune-mediated hemolytic anemia with mycophenolate mofetil in two cats. J Vet Emerg Crit Care 2011; 21:45-49.
21. Hartmann K. Feline leukemia virus infection. In Greene CE. Infectious Diseases of the Dog and Cat, 3rd ed. Philadelphia: Saunders Elsevier, 2006, p 124.
22. Otte CM, Penning LC, Rothuizen J, Favier RP. Retrospective comparison of prednisolone and ursodeoxycholic acid for the treatment of feline lymphocytic cholangitis. Vet J 2013; 195(2):205-209.
23. Weingart C, Tasker S, Kohn B. Infection with haemoplasma species in 22 cats with anaemia. J Feline Med Surg 2016; 18(2):129-136.
24. Sherrill MK, Cohn LA. Cytauxzoonosis: Diagnosis and treatment of an emerging disease. J Feline Med Surg 2015; 17(11):940-948.
25. Bacek LM, Macintire DK. Treatment of primary immune-mediated hemolytic anemia with mycophenolate mofetil in two cats. J Vet Emerg Crit Care 2011; 21(1):45-49.
26. Kohn B, Fumi C. Clinical course of pyruvate kinase deficiency in Abyssinian and Somali cats. J Feline Med Surg 2008; 10(2):145-153.
27. Tritschler C, Mizukami K, Raj K, Giger U. Increased erythrocyte osmotic fragility in anemic domestic shorthair and purebred cats. J Feline Med Surg 2016; 18(6):462-470.
28. Silvestre-Ferreira AC, Pastor J. Feline neonatal isoerythrolysis and the importance of feline blood types. Vet Med Int 2010; 2010:1-8.
29. Tocci LJ. Transfusion medicine in small animal practice. Vet Clin North Am Small Anim Pract 2010; 40(30):485-494.
30. Justin RB, Hohenhaus AE. Hypophosphatemia associated with enteral alimentation in cats. J Vet Intern Med 1995; 9(4):228-233.
31. Adams LG, Hardy RM, Weiss DJ, Bartges JW. Hypophosphatemia and hemolytic anemia associated with diabetes mellitus and hepatic lipidosis in cats. J Vet Intern Med 1993; 7(5):266-271.
32. Estrin MA, Wehausen CE, Jessen CR, Lee JA. Disseminated intravascular coagulation in cats. J Vet Intern Med 2006; 20(6):1334-1339.
33. Armstrong PJ, Blanchard G. Hepatic lipidosis in cats. Vet Clin North Am Small Anim Pract 2009; 39(3):599-616.
34. Center SA. Feline hepatic lipidosis. Vet Clin North Am Small Anim Pract 2005; 35(1):225-269.
35. Brain PH, Barrs VR, Martin P, et al. Feline cholecystitis and acute neutrophilic cholangitis: Clinical findings, bacterial isolates and response to treatment in six cases. J Feline Med Surg 2006; 8(2):91-103.
36. Callahan Clark JE, Haddad JL, Brown DC, et al. Feline cholangitis: A necropsy study of 44 cats (1986-2008). J Feline Med Surg 2011; 13(8):570-576.
37. Pedersen NC. An update on feline infectious peritonitis: Diagnostics and therapeutics. Vet J 2014; 201(2):133-141.
38. Pennisi MG, Egberink H, Hartmann K, et al. Francisella tularensis infection in cats: ABCD guidelines on prevention and management. J Feline Med Surg 2013; 15(7):585-587.
39. Weingarten MA, Sande AA. Acute liver failure in dogs and cats. J Vet Emerg Crit Care 2015; 25(4):455-473.
40. Park FM. Successful treatment of hepatic failure secondary to diazepam administration in a cat. J Feline Med Surg 2012; 14(2):158-160.
41. Beatty JA, Barrs VR, Martin PA, et al. Spontaneous hepatic rupture in six cats with systemic amyloidosis. J Small Anim Pract 2002; 43(8):355-363.
42. Cooper J, Webster CRL. Acute liver failure. Compend Contin Educ Pract Vet 2006; 28(7):498-515.
43. Center SA. Diseases of the gallbladder and biliary tree. Vet Clin North Am Small Anim Pract 2009; 39(3):543-598.
44. Eich CS, Ludwig LL. The surgical treatment of cholelithiasis in cats: a study of nine cases. JAAHA 2002; 38(3):290-296.
45. Mayhew PD, Holt DE, McLear RC, Washabau RJ. Pathogenesis and outcome of extrahepatic biliary obstruction in cats. J Small Anim Pract 2002; 43(6):247-253.
46. Simpson KW. Pancreatitis and triaditis in cats: Causes and treatment. J Small Anim Pract 2015; 56(1):40-49.
47. Haney DR, Christiansen JS, Toll J. Severe cholestatic liver disease secondary to liver fluke (Platynosomum concinnum) infection in three cats. JAAHA 2006; 42(3):234-237.
tvpjournal.com | September/October 2016 49
THE YELLOW CAT

TODAY’S VETERINARY PRACTICE | September/October 2016 | tvpjournal.com
THE YELLOW CAT: DIAGNOSTIC & THERAPEUTIC STRATEGIESPeer Reviewed
50
1. True/False: Icterus is a sensitive marker of the cause of hyperbilirubinemia in cats.a. Trueb. False
2. Locating the source of hyperbilirubin-emia is an important diagnostic step. Which of the following is not normally a component of this localizing step?a. Prehepaticb. Hepaticc. Intrahepaticd. Posthepatic
3. Which of the following is the first and most cost-effective step toward the diagnosis of prehepatic hemolysis?a. Hematocrit tube (PCV/TP)b. Complete blood countc. Serum biochemical profiled. Coombs’ test
4. Which of the following is not considered a cause of hemolytic anemia in cats?a. FeLVb. Cytauxzoon felisc. Toxoplasmosis d. Mycoplasma hemofelis
5. Which of the following is the single most important component of the treatment plan for idiopathic hepatic lipidosis?a. Antibioticsb. Nutritionc. Glucocorticoidsd. Vitamin E
CE TEST. THE YELLOW CAT: DIAGNOSTIC & THERAPEUTIC STRATEGIESThis article is RACE-approved for 1 hour of continuing education credit. To receive credit, take the approved test online at vetmedteam.com/tvp.aspx (CE fee of $5/article).
Learning Objectives After reading this article clinicians should be able to differentiate the disease processes in cats with hyperbilirubinemia, formulate an efficient diagnostic path, and prepare an effective treatment protocol for these patients.
OverviewThis article provides an overview of the differentials for feline hyperbilirubinemia, a diagnostic plan for identifying the underlying etiology of the condition, and a number of therapeutic options for these patients.
Note Questions online may differ from those here; answers are available once CE test is taken at vetmedteam.com/tvp.aspx. Tests are valid for 2 years from date of approval.
6. Which of the following is not one of the WSAVA classifications of feline cholangitis?a. Acute neutrophilicb. Chronic neutrophilicc. Lymphocyticd. Acute eosinophilic
7. Cytology can be used to guide treatment in cases of feline cholangitis. If ultrasound-guided FNA of the liver revealed degenerative neutrophils with intracellular bacteria, the foundation of treatment would be which of the following?a. Interferonb. Amoxicillin and clavulanic acidc. Prednisoloned. Ursodeoxycholic acid
8. Which of the following is not considered a component of feline triaditis?a. Kidneyb. Liverc. Pancreasd. Intestines
9. Which of the following is the treatment of choice in a cat in which biliary choleliths are causing an extrahepatic biliary obstruction?a. Ursodeoxycholic acidb. Prednisolonec. Surgeryd. Antibiotics
10. Placement of an esophagostomy feeding tube allows the owner to administer which of the following to an icteric cat at home?a. Fluidsb. Nutritionc. Medicationsd. All of the above