The Wechsler Memory Scale Revised - Home - Springer · PDF fileCHAPTER 3 The Wechsler...
35
CHAPTER 3 The Wechsler Memory Scale- Revised Current Status and Applications Gordon J. Chelune, Robert A. Bornstein, and Aurelio Prifitera In 1945 David Wechsler published the Wechsler Memory Scale (WMS) as "a rapid, simple, and practical memory examination" (p. 87). His explicit purpose was to develop a quantitative scale that would assist clinicians in evaluating patients' memory functions in relation to their other cognitive abilities. While the WMS was never intended to be a comprehensive measure of memory function, it was widely accepted and quickly became the clinical standard for memory assessment. Despite a long list of conceptual and psychometric issues that arose over the years concerning the content and structure of the WMS (Erickson & Scott, 1977; Prigatano, 1978), it has remained the most frequently used standardized measure of memory function (Chelune, Ferguson, & Moehle, 1986; Ser- etny, Dean, Gray, & Hartlage, 1986). GORDON J. CHELUNE, Head, Section of Neuropsychology, Department of Psy- chiatry, Cleveland Clinic Foundation, Cleveland, Ohio. ROBFRT A. BORNSTEIN, Associate Professor of Psychiatry, Neurosurgery, and Neurology, Ohio State University School of Medicine, Columbus, Ohio. AUREUO PRIFlTERA, Senior Project Director, PsycholOgical Measurement Group, The Psychological Corpora- tion, San Antonio, Texas. 65 P. McReynolds et al., Advances in Psychological Assessment © Plenum Press, New York 1990
Transcript of The Wechsler Memory Scale Revised - Home - Springer · PDF fileCHAPTER 3 The Wechsler...
CHAPTER 3
The Wechsler Memory ScaleRevised Current Status and Applications
Gordon J. Chelune, Robert A. Bornstein, and Aurelio Prifitera
In 1945 David Wechsler published the Wechsler Memory Scale (WMS) as "a rapid, simple, and practical memory examination" (p. 87). His explicit purpose was to develop a quantitative scale that would assist clinicians in evaluating patients' memory functions in relation to their other cognitive abilities. While the WMS was never intended to be a comprehensive measure of memory function, it was widely accepted and quickly became the clinical standard for memory assessment. Despite a long list of conceptual and psychometric issues that arose over the years concerning the content and structure of the WMS (Erickson & Scott, 1977; Prigatano, 1978), it has remained the most frequently used standardized measure of memory function (Chelune, Ferguson, & Moehle, 1986; Seretny, Dean, Gray, & Hartlage, 1986).
GORDON J. CHELUNE, Head, Section of Neuropsychology, Department of Psychiatry, Cleveland Clinic Foundation, Cleveland, Ohio. ROBFRT A. BORNSTEIN, Associate Professor of Psychiatry, Neurosurgery, and Neurology, Ohio State University School of Medicine, Columbus, Ohio. AUREUO PRIFlTERA, Senior Project Director, PsycholOgical Measurement Group, The Psychological Corporation, San Antonio, Texas.
65 P. McReynolds et al., Advances in Psychological Assessment© Plenum Press, New York 1990

66 CHELUNE ET AL
Acknowledging some of the major limitations of the WMS and the need to restandardize the scale within the context of current cognitive and neuropsychological theory, Wechsler began work on a revision of the WMS along with the test's publisher, Psychological Corporation, in the late 1970's. Although Wechsler died in 1981, the publisher cpntinued with his initial work, and the Wechsler Memory Scale-Revised (WMS-R) was formally published in September 1987 (Wechsler, 1987). Because the publisher had involved a number of investigators in clinical field trials with the WMS-R prior to its publication, the ISO-page WMS-R manual not only contains a wide range of psychometric data but a considerable amount of useful clinical data. In addition, a number of clinical and psychometric studies have already begun to emerge in the research literature.
As noted in a recent review of the WMS-R (powell, 1988), the transition from test development to acceptance in clinical practice is always arduous. The clinician must "balance psychometric developments against years of data and experience with 'tried and true' measures, however outdated" (p. 403). The decision of "should I change?" is not to be taken lightly for any test procedure, and should always be made as an informed consumer. The purpose of this chapter is to review the major revisions and changes in the WMS-R, critically evaluate its psychometric properties, and review the growing body of clinical research that has already emerged. In providing this review of the WMS-R, it is hoped that potential test users can: a) better make an informed judgment as to whether or not to explore the use of the WMS-R in their clinical/research practices, and; b) if they choose to further explore the WMS-R, to do so wisely with a better understanding of the nuances of the test.
ASSESSING MEMORY F1JNCTIONS It is now generally accepted that "memory" is not a unitary ability that
can be localized within a discrete area of the brain. Rather, memory is currently seen as a multidimensional and multifaceted cognitive process that is mediated by equally complex systems of neural substates located in disparate regions of the brain. While it is beyond the scope of this chapter to review the complexities of memory in detail, three useful distinctions can be made (Chelune & Liiders, 1988).
The first distinction that can be made is between "learning" and "memory." Squire (1987) notes that learning is the process by which new information is acquired, whereas memory is the persistence of the process of learning over time. It is this "temporal" nature of memory (the persistence of learning) that gives rise to distinctions between information that is temporarily accessible in immediate awareness (variously

WECHSlER MEMORY SCALES-REVISED 67
termed "primary memory," "working memory," and "short-term memory") versus that which is encoded in a more stable and permanent manner and must be reconstructed for recall (long-term memory). This distinction not only reflects differences in the temporal availability of information, but also potential differences in neural substrates for the encoding and decoding processes. The final distinction to be considered is the further division of long-term memories into those that can be retrieved on a conscious level (i.e., "declarative memory," "explicit memory," and simply "memory") verses those that are primarily demonstrated on a perceptual-motor basis (i.e., "procedural memory," "implicit memory," and "habits"). There is growing experimental data to suggest that different neuroanatomical structures and possibly neurotransmitters mediate these two types of long-term memory systems (see Mishkin & Appenzeller, 1987; Squire, 1987).
Given the apparent complexity of memory functions intimated by even this limited and sketchy review of basic concepts, it is not surprising that both clinicians and researchers have begun to look for alternative test procedures that provide for a more differentiated and comprehensive approach to memory assessment than afforded by the WMS. While it is doubtful whether anyone measurement instrument can provide a fully comprehensive assessment of memory functions, a number of new memory "batteries" have appeared in recent years that attempt to address, with more or less success, some of the problems inherent in the original WMS. Among these are the Randt Memory Test for Longitudinal Measurement (Randt, Brown, & Osborne, 1980), the Vermont Memory Scale (Williams, 1983), the California Verbal Learning Test (Delis, Kramer, Kaplan, & Ober, 1987), the Rivermead Behavioral Memory Test (Wilson 1987), and Warrington's Recognition Memory Test (1984). To be sure there are other clinical and experimental memory procedures, varying in both breadth and emphasis, but virtually all of these, including the WMSR, focus on what can be construed as "declarative" information. In the following section we will briefly review some of the major limitations of the WMS, and then proceed with a description and critique of the WMSR and its characteristics.
Wechsler Memory Scale (WMS)
As originally described (Wechsler, 1945), the WMS consists of seven subtests: Personal and Current Information, Orientation, Mental Control, Logical Memory (prose passages), Digit Span, Visual Reproduction (figural drawings), and Associate Learning (verbal paired-associates). The WMS yields a single, global index or Memory Quotient for ages 20 thru 64. The scale was standardized on "approximately" 200 normal subjects between the ages of 25 and 50, and mean WMS total scores were computed

68 CHELUNE ET AL
for each 5 or 10 year interval. Data from the Wechsler-Bellevue was available in about 100 cases, and the mean WMS scores were plotted against the mean weighted Wechsler-Bellevue scores and an empiricallyderived constant was added to keep the mean MQ for any age group equivalent to the mean IQ for that group.
Despite its long history as a useful and valid clinical measure of memory (see reviews by Chelune, Ferguson, & Moehle, 1986; Wechsler, 1987), the WMS has a number of major limitations (see Erickson & Scott, 1977; Prigatano, 1978). Use of a single Memory Quotient implies that "memory" is a unitary ability much the same as "organicity" once implied that all neurological disturbances resulted in a singular pattern of cognitive dysfunction. Even early factor analytic studies of the WMS demonstrated a fairly consistent multi-factor structure, with the Logical Memory, Visual Reproduction, and Associate Learning subtests clustering to form the primary "memory" dimension, and the Mental Control, Digit Span, and typically Orientation subtests comprising an "attention" factor (e.g., Davis & Swenson, 1970; Kear-ColweU, 1973).
With the exception of the Visual Reproduction subtest, all of the WMS subtests involve audio-verbal stimuli and verbal responses, rendering it largely a measure of verbal memory (Milner, 1975). Additionally, only immediate or short-term memory for newly acquired material is assessed. The latter difficulty was, in part, addressed by Russell in 1975 when he proposed the addition of delayed recall trials as well as percentretention scores (delayed/immediate indexes) for the Logical Memory and Visual Reproduction subtests. Until most recently (Russell, 1988), there were no adequate norms or means for equating the two subtests or correcting for biases due to differences in age or education.
Normative data and psychometric information presented in the WMS manual (Wechsler, 1945) are inadequate by today's standards, and the age range is quite limited considering the increasing number of individuals 65 and older who clinically present with complaints of memory loss (Kaszniak, 1987). Since the WMS was "linked" to IQ scores from the Wechsler-Bellevue to assist clinicians in comparing IQ-MQ differences, revisions of the Wechsler's adult intelligence scale (WAIS and WAIS-R) have changed the inherent relationship between these two variables, resulting in problems of interpretation (Larrabee, 1987; Prifitera&Barley, 1985). Finally, scoring criteria for the Logical Memory and Visual Reproduction subtests are loosely defined and have resulted in poor reliability (prigatano, 1978). Several alternative scoring approaches have been proposed (e.g., Power, Logue, McCarthy, Rosentiel, &Ziesat, 1979; Sweet & Wysocki, 1982) to increase the reliability of these subtests, but none have been widely accepted.

WECHSlER MEMORY SCALES-REVISED 69
Wechsler Memory Scale-Revised (WMS-R)
Descrlptlon. The WMS-R (Wechsler, 1987) consists of 13 subtests. With the exception of the Information and Orientation Questions, these subtests are combined to yield five age-eorrected summary indexes or quotients that have a mean of 100 and a standard deviation of 15. The overall structure of the WMS-R and the composition of the summary index scores are shown in Table l. Tasks of attention and concentration are treated separately, and comprise a separate Attention/Concentration Index. The General Memory Index is a composite index of immediate or short-term recall for both verbal and nonverbal material, and is the index that most closely resembles the original WMS Memory Quotient. The subtests that comprise the General Memory Index are further subdivided to yield separate Verbal Memory and Visual Memory Indexes of shortterm recall. The final summary index is Delayed Memory, which is a composite index of the delayed recall trials of four subtests, two verbal (Logical Memory and Verbal Paired Associates) and two nonverbal (Visual Reproduction and Visual Paired Associates).
Table 1
Structure and Content of the Wechsler Memory Scale-Revised
Subtests
Information & Orientation
Mental Control Digit Span Visual Memory Span
Logical Memory I Verbal Paired Associates I
Figural Memory Visual Reproductions I Visual Paired Associates I
Logical Memory II Verbal Paired Associates II Visual Paired Associates II Visual Reproductions II
Index Scores
No Index Score
} Attention/Concentration
}
} Verbal Memory
} Gen.,a/ Memo,y
Visual Memory
} Delayed Memory
In addition to providing multiple measures of memory function rather than a single global score as in the original WMS, the subtest content of the WMS-R has been substantially revised and expanded. Three of the WMS-R subtests are new, nonverbal tasks, and include: 1) Figural Mem-

70 CHELUNE EI' AL
ory, a short-term visual recognition task in which the subject is briefly exposed to complex abstract designs and then must identify them from among a stimulus array of similar designs; 2) Visual Memory Span, a twodimensional Corsi block-tapping task (Milner, 1971), akin to Digit Span, in which the subject must reproduce examiner-modeled block-tapping sequences of varying lengths both forward and in reverse; and 3) Visual Paired Associates, a nonverbal analog to Verbal Paired Associates in which the subject must first learn the association between six "meaningless" line drawings and a paired-color and then select the appropriate color when shown only the nonsense figure. The Logical Memory, Visual Reproduction, Digit Span, and Verbal Paired Associates (previously called Associate Learning) tasks have all been substantially revised and updated, and the scoring criteria for Logical Memory and Visual Reproduction subtests have been carefully delineated. The only original WMS subtest to remain unchanged is the Mental Control subtest, which is now combined with the scores from the Digit Span and Visual Memory Span subtests to yield the Attention/Concentration Index.
Standardization of the WMS-R was based on a sample of 316 normals who were stratified by age, sex, race, geographic region, and level of education within six age groups of approximately 50 subjects according to the demographic characteristics derived from the 1980 U.S. Census (U.S. Bureau of the Census, 1983; 1984). Raw subtest scores were weighted to maximize the reliabilities of the five summary Indexes. These weighted raw score sums were normalized and smoothed, and then scaled to have a mean of 100 and standard deviation of 15, similar to the scaling of the Wechsler Adultlntelligence Scale-Revised (W AIS-R: Wechsler, 1981). Data for three age ranges (18-19, 25-34, and 45-54) were not collected. Norms for these groups were prepared by interpolation, resulting in age-corrected normative scales for each of the five indexes for nine age groups corresponding to the nine age groups represented in the WAIS-R norms. In addition, an elderly sample is currently being collected by the publisher to provide normative information for individuals over 74 years of age.
Crldque. It is evident from even a cursory examination of the WMSR that it represents a substantial revision and extension of the original WMS, and that it "incorporates many features that should make it an attractive instrument for clinical assessment" (Herman, 1988, p. 106). However, closer examination of some of these "features" suggests that they are not entirely perfect. In this section we will critique each of the major changes In the WMS-Ras they are enumerated the Manual (Wechsler, 1987, p. 2).
1. The single WMS Memory Quotient has been replaced by five summary Index scores. These indexes are based on standard score distributions, which facilitate, if not encourage, intraindividual compari-
WECHSLER MEMORY SCALES-REVJSID 71
sons among the index scores. While it is possible to compare such indexes as General Memory versus Delayed Memory and Verbal versus Visual Memory on the basis of standard scores, the content and weighting of the subtests that comprise these indexes are not the same. For example, Figure Memory, which is included in the calculation of the General Memory Index, is not included in the Delayed Memory Index, and the weighting of the remaining common subtests is different in the calculation of both of these two indexes. Similarly, a superficial examination of the Verbal and Visual Memory Indexes suggests that they may not be equally weighted and seem to contribute differentially to the General Memory Index (Loring, 1989), although this is not entirely correct from the psychometric perspective of test construction (Gulliksen, 1950; see section on Verbal-Visual Biases for further discussion of this point). The Delayed Memory Index is an absolute score that is scaled independent of the subject's level of immediate recall. Thus, the Delayed Memory Index reflects subjects' absolute standing in terms of how much they recall, and tells us little about the efficiency of their long-term memory (retention) for what they initially grasp.
2. The WM~R provides age-corrected stratified norms for each of the indexes at nine age levels. However, only six age levels were actually sampled, with interpolated norms being provided for subjects 18-19,25-34, and 45-54. Interpolation of norms for the 1 O-year span between ages 45 and 54 is especially unfortunate since this is an epoch in which aging and memory are known to interact in a complex manner (poon, 1986). Furthermore, the norms for the six age levels actually sampled are based on samples of only 50 to 55 subjects, sample sizes that are considerably smaller than the 160 to 300 subjects per age level used in the standardization of the WA~R (Wechsler, 1981). Loring (1989) has suggested that the relatively smaller sample sizes for the WM~R results in a standard error of the mean that is twice as large as in the WA~R. For a scale with a standard deviation of 15 such as the Wechsler scales, this amounts to ± I-point for a sample of 200, compared to ± 2-points for the WMS-R Indexes. Thus, while the standard error of the mean on the WMS-R is twice that of the WAIS-R, the magnitude of the difference between the two sample sizes amounts to only I-point. In addition, the stratification and control of IQ level in the WMS-R standardization process assisted in securing a representative sample. Thus, while the WMS-R samples are smaller than those used in the development of the WAIS-R, they are certainly adequate and compare very well to other "memory" scales frequently used by neuropsychologists (Lezak, 1983).
3. Inclusion of new measures of nonverbal, visual memory in the WMSR provides a more balanced assessment of material-specific memory functions than the WMS. While this was certainly the intent, some investigators have questioned whether these new tasks actually achieve this

72 CHFJ.UNE IT AL
goal. The manner of presentation used in the Visual Paired Associates task has been particularly criticized as being susceptible to verbal mediation (Delis, 1989; Loring, 1989), and it has been suggested that such mediation might be dampened by reversing the order of stimulus-response (e.g., cuing figure recall with a color rather than color recall with a design). The designs used in the Visual Reproduction subtest may also be subject to a certain degree of verbal mediation (Bornstein & Chelune, 1988; Chelune & Bornstein, 1988b). From a theoretical perspective it is desirable to have relatively pure measures of verbal and visual memory; however, in daily living it is likely that most individuals use both verbal and nonverbal encoding strategies when confronted by complex stimuli. Hence, the creation of "pure" nonverbal memory paradigms and stimuli may require tasks that have little ecological validity in terms of everyday memory.
4. The WMS-R provides delayed recall trials on four tasks, and scores on these tasks are combined to yield a Delayed Memory Index. As noted earlier, this is an absolute score that does not take into account level of initial recall and, therefore, does not assess "efficiency" of delayed retention. Because it also is a composite score, encompassing both verbal and nonverbal content, it does not allow the test user to directly compare material-specific short-term and long-term memory. One may apprOximate these material-specific temporal comparisons by using the age-corrected percentile scores for the immediate and delayed recall trials of the Logical Memory and Visual Reproduction subtests, which are presented in Table C-5 of the WMS-R manual. However, "interpretation of these percentiles should take into account ... the reliabilities of these subtests ..... and "users should exercise caution when interpreting subtests or parts of subtests with low reliabilities" (Wechsler, 1987, p. 57). Even using appropriate caution in the interpretation of these age-percentile scores, one must be cognizant of an additional bias that may be introduced if subjects fail the free-recall trial of these subtests. As noted by Loring (1989), subjects are given a prompt if they cannot initiate recall on either of the Logical Memory passages, but no prompts are given if subjects cannot recall one of the Visual Reproduction designs. The differential use of prompting introduces the potential for significant variability in the amount of verbal versus visual material that is recalled on the delayed trials of these subtests.
5. The WMS-R has revised the scoring procedures for several subtests, notably Logical Memory and Visual Reproduction, to improve scoring accuracy. lnterscorer reliabilities of .99 and .97 for the Logical Memory and Visual Reproduction subtests, respectively, attest to the clarity of the scoring criteria for these subtests (Wechsler, 1987). However, rigid adherence to the scoring rules for the Visual Reproduction designs often requires use of a ruler and protractor, and places an

WECHSlER MEMORY SCALES-REVlSD> 73
emphasis on drawing "accuracy" rather than amount of information retained. As such, the Visual Reproduction subtest may be highly associated with differences in visuo-constructional praxis, especially among clinical populations (Chelune, Goormastlc, & Naugle, 1989).
Summary. While the structure and content of WMS-R are not without problems and limitations, the test is a "significant improvement over its predecessor" (powell, 1988, p. 402). Whether these improvements are sufficient to outweigh the potential problems inherent in the test is an individual decision. There is no "perfect" test. A test is merely a tool for gathering data in a standard, objective manner that is publicly verifiable. The utility of a test depends on the sophistication and skill of the researcher or clinician using it and the nature of the task for which the test is used. The WMS-R is essentially a new tool, and its ultimate utility will depend on an adequate knowledge of its psychometric nuances and potential clinical applications.
PSYCHOMETRIC PROPERTIES OF THE WECHSLER MEMORY SCALE-REVISED
It is not our intention to simply review the psychometric data already presented in the WMS-R manual, although the interested reader is encouraged to do so. Rather, this section will highlight those psychometric properties and data in the WMS-R manual that have a potential bearing on clinical practice and application. In addition, we will review some of the emerging research data on the factor structure of the WMS-R and use of IQ-Memory discrepancy scores.
Reliability
Unlike the WAIS-R, scaled scores for each of the WMS-R subtests are not provided, making it difficult to directly compare subtest performances or examine subtest profile patterns. The means and standard deviations for the raw WMS-R subtest scores at each of the six age levels sampled are presented in WMS-R manual (Wechsler, 1987, p. 52), and it is tempting to consider using these data to generate scaled score distributions to facilitate subtest comparisons. However, such standard score distributions were deliberately avoided by the publisher because the subtests have different distributions and several are not normally distributed, making comparison of standard scores problematic. In addition, the relatively greater amount of error variance in some subtests compared to others can lead to misleading conclusions if all of the obtained scores are assumed to equally approximate true scores. The average reliability

74 CHD.UNE El' AL
coefficients across age groups for the individual subtests ranged from only.41 (Verbal Paired Associates II) to .88 (Digit Span), with a median reliability coefficient of .74. Reliability coefficients for the summary indexes ranged from .70 (Visual Memory) to .90 (Attention/Concentration), reflecting the greater consistency or precision of these summary scores.
Even given the greater reliability of the summary indexes, the standard error of measurement of these indexes ranged from about 5 points on the average across the age levels for the Attention/Concentration Index to about 8.5 pOints for the Visual Memory Index. That is, "for an individual with a 'true' Visual Memory Index of 100, the individual's observed score would fall between 91 and 109 approximately two-thirds of the time over a large number of testings on that individual" (Wechsler, 1987, p. 63). The astute test user will appreciate the potential implications of these standard errors of measurement (see Wechsler, 1987, Table 13) when attempting to evaluate the meaning of intraindividual differences between WMS-R Index scores or the relationship of these scores to other cognitive measures. Confidence intervals at the .15 and .05 probability levels for differences between selected Index scores are presented in Table 14 of the WMS-R manual. Differences in the range of 15 points between General Memory and Attention/Concentration are needed to be statistically significant at the .05 level, whereas differences of about 20 pOints are needed between the Verbal and Visual Memory Indexes and between General Memory and Delayed Memory to be significant at the .05 level. These confidence intervals refer to the reliability of the difference scores as due to something other than measurement error. They do not refer to the probability of base-rate occurrence in a normal sample (see Matarazzo & Herman, 1984).
While these confidence intervals do not address the issue of "clinical meaningfulness," they do suggest that the band of measurement error surrounding each of the WMS-R summary Index scores is such that even relatively large discrepancies between Indexscorescan occur by "chance. " Similarly, correlations between the WMS-R subtest and Index scores and other cognitive test measures should also be interpreted in light of the reliability of the measures being correlated. It is not uncommon in research to generate hypotheses and draw conclusions based on correlations among new measures, indexes, or clinical ratings without regard to the precision of the measures being used. This has been a particular problem in neuropsychology where the "reliability of neuropsychological examinations has taken a distinctly secondary position to that of validity" (Boll, 1981, p. 600).

WECHSLER MEMORY SCALFS-REVISED 75
Stability
To assess the stability of the WMS-R subtests and Index scores, subjects in the standardization sample who were in the 20-24, 55-64, and 70-74 year old age ranges were retested after four to six weeks. Test-retest reliability coefficients for the subtest scores ranged from a low of .30 (Verbal Paired Associates) among the 20-24 year olds to .84 (Digit Span) among the 70-74 year olds, with an overall positive relationship between age and magnitude of stability being evident in the data (see WM~R Table 12). Stability coefficients for the Index scores ranged from .57 to .93 for the three age groups.
Test-retest coefficients reflect the relative (ordinal) stability of scores between two points in time and not necessarily the "absolute" stability of a score from one test administration to the next. Examination of the net changes in absolute raw Index scores over the retest interval reveals rather substantial "practice" effects (approximately 10-15 raw score points) on all of the Index scores except Attention/Concentration. However, the test user should also note that there appears to be an inverse relationship between age and magnitude of practice effect. For example, young individuals (20-24) may be expected, on the average, to demonstrate a net gain of 18 raw pOints on the Delayed Memory Index if retested within a six week interval, whereas older individuals (70-74) can be expected to only show an average net gain of five raw pOints on retesting.
Test users need to exercise some caution when conSidering testretest changes on the WM~R, or any form of memory test. The notion of a "practice effect" implies that the experience gained on the first exposure to a test is carried over and affects performance on the second testing. This persistence of learning over time is identical to Squire's (1987) operational definition of "memory," which we advanced early in this chapter. Thus, test-retest practice effects on a memory test such as the WM~R cannot be separated from the construct under investigation. While it has not been formally investigated, it is likely that magnitude of test-retest change on the WMS-R (correcting for ceiling effects) is influenced by initial level of performance. Until base-rate data on individual test-retest changes are forthcoming, clinical inferences concerning the observation of whether or not a given individual demonstrates the "expected" mean practice effect on retesting should be tempered by knowledge of his or her initial level of performance.
Verbal-Visual Biases
Since the WMS was often criticized as largely a measure of verbal memory (Milner, 1975; Prigatano, 1978), one of the major objectives of the WM~R was to provide a better balance of verbal and nonverbal content
76 CHEUJNE ET AL
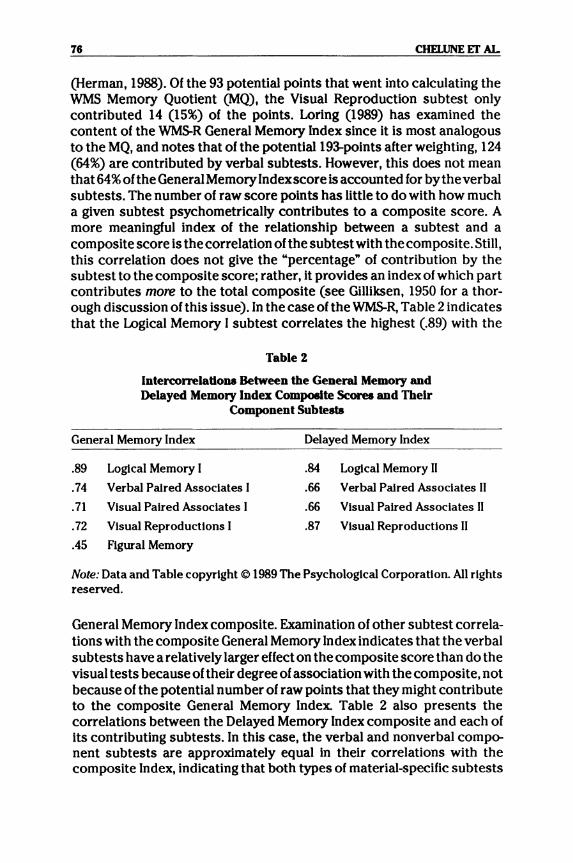
(Herman, 1988). Of the 93 potential pOints that went into calculating the WMS Memory Quotient (MQ), the Visual Reproduction subtest only contributed 14 (15%) of the pOints. Loring (1989) has examined the content of the WM~R General Memory Index since it is most analogous to the MQ, and notes that of the potential 19~points after weighting, 124 (64%) are contributed by verbal subtests. However, this does not mean that 64% of the General Memory Indexscore is accounted for by the verbal subtests. The number of raw score points has little to do with how much a given subtest psychometrically contributes to a composite score. A more meaningful index of the relationship between a subtest and a composite score is the correlation of the subtest with the composite. Still, this correlation does not give the "percentage" of contribution by the subtest to the composite score; rather, it provides an index of which part contributes more to the total composite (see Gilliksen, 1950 for a thorough discussion of this issue). In the case of the ~R, Table 2 indicates that the Logical Memory I subtest correlates the highest (.89) with the
Table 2
IntercoJTelations Between the General Memory and Delayed Memory Index Composite Scores and Their
Component Sublests
General Memory Index Delayed Memory Index
.89 Logical Memory I .84 Logical Memory II
.74 Verbal Pal red Associates I .66 Verbal Pal red Associates II
.71 Visual Paired Associates I .66 Visual Paired Associates II
.72 Visual Reproductions I .87 Visual Reproductions II
.45 Figural Memory
Note: Data and Table copyright © 1989 The Psychological Corporation. All rights reserved.
General Memory Index composite. Examination of other subtest correlations with the composite General Memory Index indicates that the verbal subtests have a relatively larger effect on the composite score than do the visual tests because of their degree of association with the composite, not because of the potential number of raw pOints that they might contribute to the composite General Memory Index. Table 2 also presents the correlations between the Delayed Memory Index composite and each of its contributing subtests. In this case, the verbal and nonverbal component subtests are approximately equal in their correlations with the composite Index, indicating that both types of material-specific subtests

WECHSLER MEMORY SCALES-REVISED 77
contribute about equally to the Delayed Memory Index. Thus, because of the correlations of the "parts to the whole," the General Memory Index does show a slight "verbal" bias whereas the Delayed Memory Index appears to equally represent verbal and nonverbal content.
Relationship of Demographic Variables to WMS-R Performance
Sex. The WMS-R standardization sample was recruited with approximately equal numbers of men and women included at each age level, despite the trend for women to begin to outnumber men after the age of 50 (U.S. Census Bureau, 1983). Multivariate and univariate gender comparisons for the WMS-R subtests and summary Index scores yielded no statistically significant differences between men and women, suggesting that "adjustment of scores for the gender of the examinee [on the WMSR] is not required" (Wechsler, 1987, p. 77).
Age. The WMS-R Index scores are norm-referenced and standardized for each age group such that a standard score of 100 on an Index should place individuals at the 50th percentile among their peers regardless of the age group in which they fall. However, this does not imply equivalence of performance across age. It is well known that memory and other cognitive functions decline with age (poon, 1986), and that an "average" performance for a 25 year old is not the same in an absolute sense as that for a 72 year old. Multivariate and univariate analyses of the standardization data across age groups for raw subtest scores as well as for the composite raw Index scores yielded highly significant results (Wechsler, 1987), supporting this proposition.
For most purposes it may be sufficient to be mindful that "equal Index scores for individuals of different ages do not necessarily imply that the individuals have equivalent abilities in an absolute sense" (Wechsler, 1987, p. 77). However, in other cases it may be necessary to examine more closely the meaning of the WMS-R Index scores across the age span. Since the Indexes are composite scores, age-related changes must be examined in terms of the relative changes in the subtests comprising the given Index. To evaluate the effects of age at the subtest level, we computed best-fit regression lines between the median ages for the six age groups in the standardization sample and their mean raw score performances. The resulting multiple Rs ranged from .95 (Digit Span and Logical Memory I) to .99 (Figure Memory, Visual Memory Span, Visual Paired Associate I and II, and Visual Reproduction I and II). However, as seen in Figure 1, the best-fitting regression lines were not always linear. That is, while performance on some subtests showed a gradual, steady decline with age, mean performance on others demonstrated an accelerated rate of decline with advancing age.
Because performances on the individual WMS-R subtests appear to

) ~
3 2 2 2 2
'r'
r 5 • !
2 o
5"
~
2,
I 2
lie
>02 i 2
•
• 5 ! I
~ 2
0 )
'i
u 'iii o ~
~ , r 16
IS
14
13
I I
Lo
gic
al
Me
mo
ry I
& I
I
Lo
g'c
.' ~em
or,
I
~ ~
"" "" ~
~
~
'" ~
"'" L
og c
eil
lem
lor,
II
~ ~ r"-
.. "'" I
I I
I I
I I
I I II
I
I I
I III I
I II I
I I
III
I I
I
3, 3 3 3 3' 2' J
-_
2:
• ! 2
o .x 21
.21
:2
~2
1)2
.;
2
o D. 21 :1
:1
~I S ! I ) iI ! 7 S 5 • 5 ! I ) ! B
7 S 5 • 5 2 I I 10 --
'--'
Vis
ua
l R
ep
rod
uct
ion
s I
& I
I
:--
-........
.. ~
~
~
~ "" V'I
U.'
ReD
roc
ctl
on
l'
1\ \ \
\ \ \ V
'lue'
1\ R
... r
od
cll
one
..
\ L
L_
J I
11
I
I I
I I
I I
I I
I I
I I
I I
I I
I
~~~~2~~~~~~~M~nn~
~~~~~~~~~~~~M~nn~
18
22
2
6
30
3
4
38
4
2
46
!S
O 5
4
58
6
2
66
7
0
74
7
8
18
22
26
30
3
4
38
42
4
6
50
5
4
58
62
66
7
0
74
78
Ag
. A
ge
I I
Hgu
re 1
. Bes
t-fi
t age
reg
ress
ion
line
s fo
r pr
edic
ting
raw
sco
re p
erfo
rman
ce o
n th
e Im
med
iate
and
del
ayed
tri
als
of L
ogic
al M
emor
y an
d V
isua
l R
epro
duct
ions
on
the
basi
s of
age
. R
egre
ssio
n li
nes
wer
e de
rive
d fr
om m
edia
n ag
e an
d m
ean
raw
sco
res
pres
ente
d In
the
WM
S-R
Man
ual (
Wec
hsle
r, 1
987)
.
~ I ~ ~
WECHSlER MEMORY ~REVlSED 79
decline at different rates with age, the nature of the Index scores that they comprise also may change with age. For example, the Logical Memory and Visual Reproduction subtests, which are depicted in Figure 1, both contribute to the General Memory and Delayed Memory Indexes. While absolute performance on the Logical Memory trials seems to decline at a steady pace with age, performance on the Visual Reproduction trials is relatively stable from 16 to 40 and then declines in an exponential manner. Absolute changes in the General Memory and Delayed Memory Indexes will be affected to a greater extent by changes in Logical Memory than by changes in Visual Reproductions early in the age span, with the reverse being true in the later stages of the life span. Since the absolute composite scores for the General Memory and Delayed Memory Indexes are normreferenced at each age level, their intrinsic compositions and meanings are apt to differ at different points in the age span.
EducadoD. Consistent with previous studies on measures of general intelligence (Matarazzo, 1972) and cognitive functioning (Heaton, Grant, &Matthews, 1986), Wechsler (1987) indicates that years of formal education were moderately correlated with each of the five WMS-R Index scores (range .42 to .49). Multivariate and subsequent univariate analyses of the Index scores across three education levels (less than 12 years, 12 years, and more that 12 years) yielded Significant education effects for each of the Index scores. Mean standard score differences in the magnitude of 1 ~ 15 points were observed between the "less than 12 years" and "more than 12 years" of education groups for the Indexes. Because level of WMS-R performance is related to educational level, it is suggested that interpretation of any given Index score should be done in light of the person's educational background, especially "when premorbid memory functioning is unknown" (Wechsler, 1987, p. 78).
Although it is not delineated in the WMS-R manual, the moderating effects of education on level of WMS-R performance are further complicated by their interaction with age. When standardization samples for tests such as the WMS-R or WAIS-R are selected to match the demographic characteristics of the U.S. population on the basis of census data, there is a tendency for age to be inversely related to years of formal education. That is, older cohorts do not, on the average, have the same degree of educational experiences as do younger cohorts. When the median age of the WMS-R age groups is correlated with their mean education level (derived from data in Table 5 of the WMS-R manual), the relationship is rather striking (r '" -.98).
Clinically, interpretation of a given Index score must not only take into account absolute level of education, but also its interaction with age. Consider the data presented in Table 17 of the WMS-R manual (Wechsler, 1987, p. 78), which reveals a mean Verbal Memory Index of 99.98 for individuals with 12 years of education. Theoretically, a standard score of

80 CHFllJNE ET AL
100 should place a person at the 50th percentile within his or her age cohort since each age group is norm-referenced. However, a 72 year old with 12 years of education who obtains a Verbal Memory Index of 100 is actually performing below expectations since 60% of his or her age cohort had less than a high school education. That is, since the performance norms for the 70-74 year old age group were derived from a sample with a mean education level of less than 12 years, one would expect a person with 12 or more years of education to perform at a level above the norm of 100. Similarly, a 23 year old male with 12 years of education who obtains a Verbal Memory Index of 100 is probably doing somewhat better than his educationally-matched peers since the "average" male in this age group has a mean educational level of more than 12 years. While the interactional bias that age and education introduces into the interpretation of the WMS-R Index scores is apt to be slight, and perhaps not clinically meaningful on a case-by-case basis, the researcher should be aware of this bias when dealing with group data where small differences may reach statistical significance.
~R Venus WMS Comparisons
Questions about the equivalency of test scores are always of concern when attempting to relate performance on a revised measure with that on the original. Unlike the manual fortheWAIS-R(Wechsler, 1981), theWMSR manual (Wechsler, 1987) contains no data comparing WMS-R Index scores with the MQ from its predecessor, the WMS. However, Butters, Salmon, Cullum, Cairns, Troster, and Jacobs (1988, p. 144) note that the "WMS-R is far superior to the original WMS for assessing memory disorders in amnesic and demented patients" because it "yields more valid quantitative measures of severe anterograde memory disorders than the original scale." This observation is based on their finding that amnesiacs obtained average General and Delayed Memory Index scores of 69 and 56, respectively, compared to the expected WMS MQs in the 70-80 range, typically seen among such patients. Unfortunately, no direct comparisons were made to support this inference.
One study has attempted to directly compare WMS-R Index scores with performance on the WMS (Daniel, Dwarshuis, & Nelk, 1988). The WMS and WMS-R were administered in a counterbalanced manner to a mixed group of 20 patients, with the two procedures separated by the administration of the WAIS-R. Consistent with the inference drawn by Butters and his colleagues (1988), the mean WMS-R Index scores were conSistently 8-15 points lower than the WMS MQ, with the patients showing an average 14-point difference between theirWMS MQ (97.4) and General Memory Index (83.3). While it is an empirical question as to whether the WMS-R yields a more accurate assessment of memory deficit

WECHSlER MEMORY SCALFS-REVJSED 81
than the WMS, it does appear that the WMS-R will yield scores considerably lower than the WMS. Thus, clinicians should exercise caution when attempting to interpret differences between patients' WMS MQs and their WMS-R Index scores.
Percent-Retendon Scores
Russell (1975) introduced the use of percent-retention scores as material-speclfic memory indexes by comparing the amount of material subjects recalled after a half-hour delay with the amount they immediately recalled on the Logical Memory and Visual Reproduction subtests from the WMS. These ratios are heuristically appealing in that they reflect the efficiency of delayed-memory relative to the individual's ipsative level of immediate-recall. Unfortunately, when immediate-recall (the denominator) is limited, the ratio changes dramatically with minimal changes in delayed-recall (the numerator). If one examines the age-related changes depicted in Figure 1 for the immediate and delayed trials of these two subtests, it is also clear that percent-retention scores are age-dependent and should be normed in the same age-corrected fashion as the WMS-R Index scores. A final problem with percent-retention scores concerns their reliability. While no formal reliability study has been conducted, percent-retention scores are based on the ratio of test scores that, themselves, have less than perfect reliabilities, and will have a limiting effect on the potential reliability of the percent-retention scores.
Despite the psychometric problems inherent in percent-retention indexes, several studies employing the WMS-R immediate and delayed trials of the Logical Memory and Visual Reproduction subtests have found these percent-retention indexes to be useful. Butters and colleagues (1988) found that amnesic groups had lower percent-retention scores (described by these authors as "savings" scores) than did normal controls. Troster, Butters, Salmon, Jacobs, Cullum, and Moss (1989) also found these percent-retention indexes helpful in differentiating Huntington's and Alzheimer's disease patients with mild and moderate degrees of dementia. Chelune and Bomstein (l988b) found a within-subjects double dissociation ofWMS-R-derived Logical Memory and Visual Reproduction percent-retention scores among patients with unilateral brain lesions, which in a related study (Chelune & Bomstein, 1988) was more pronounced in patients with temporal compared to extra-temporal lesions. Finally, Chelune, Katz, Awad, Naugle, Liiders, and Kong (1989) report significant correlations between changes in these material-specific percent-retention scores and extent of mesial resection among seizure patients undergoing temporal lobectomies.

82 CHELUNE ET AL
Factor Analytic Shldles
Factor analytic studies of the WMS generally have revealed a two- or three-factor structure. Learning and immediate recall of verbal and visual material typically compose one factor, attention and concentration measures comprise a second factor, with general orientation occasionally emerging as a third factor (e.g., Bachrach &Mintz, 1974; Kear-Colwell, 1973; Skilbeck & Woods, 1980). Inclusion of delayed recall trials for the Logical Memory and Visual Reproduction subtests have generally not added differential validity to the WMS factor structure (Russell, 1982), although some Investigators have suggested that different factor loadings would emerge if the WMS subtests were examined within a broader context of neuropsychological tests (Larrabee, Kane, Schuck, & Francis, 1985; Trahan & Larrabee, 1984).
A number of factor analytic studies of the WMS-R have been reported in both the WMS-Rmanual (Wechsler, 1987) and in the research literature (Bornstein & Chelune, 1988, 1989; Chelune, Goormastic, & Naugle, 1989; Roid, Prifitera, & Ledbetter, 1988). The WMS-R manual (Wechsler, 1987) reports the results of principal components factor analyses of the agecorrected raw scores (raw score residuals after age effects were partialed out) on the WMS-R immediate-recall subtests, with and without WAIS-R Full Scale IQ scores, computed separately for the standardization sample (N = 316) and a mixed clinical sample (N = 346). These analyses revealed a consistent two-factor structure, with a general memory and an attention/concentration factor emerging in each of the analyses. Delayedrecall subtests were not considered since earlier exploratory analyses found that these subtests loaded on the same factors as their immediaterecall counterparts. W AIS-R IQ scores loaded on the attention/concentration factor in both the standardization and clinical samples. In subsequent confirmatory factor analyses of the same data, Roid, Prifitera, and Ledbetter (1988) found that a 2-factor solution was the best fitting model for both the clinical and standardization data when only the immediaterecall subtests were considered.
Bornstein and Chelune (1988) also examined the factor structure of the WMS-R among a large clinical sample (N = 434), with and without W AI5-R Verbal (VIQ) and Performance (PIQ) IQ scores. Consistent with the results of Wechsler (1987) and Roid, Prifitera, and Ledbetter (1988), a twofactor (general memory and attention/concentration) principal components solution was obtained when only the immediate-recall subtests were considered. The W AIS-R IQ scores loaded on the attention/concentration factor. However, when the delay-recall subtests were included in the analysis, a three-factor solution was obtained, accounting for 73% of the variance. Attention/concentration tasks again loaded together, but the remaining subtests loaded on what were interpreted to be verbal and

WECHSLER MEMORY SCALES-REVISED 83
nonverbal memory dimensions. Interestingly, VIQ and PIQ continued to load on the attention/concentration factor. Although tentative, these results seem to support current theories of hemispheric specialization of memory functions for material-specific stimuli (Lezak, 1983).
Since the WMS-R manual (Wechsler, 1987) clearly documents the effects of age and education on level of performance, Bornstein and Chelune (1989) further examined the factor structure of the WMS-R in their clinical sample according to three age groups and three educational levels. In the analyses of age groups, the factor structures for each age group was similar, although there was a trend for the visual subtests to load more highly on the "verbal factor" with increasing age, suggesting that older individuals may increasingly rely on verbal strategies in the recall of "nonverbal" material. Inclusion of IQ scores in the age group analyses had an impact on only the youngest age cohort (16-39) where PIQ and the nonverbal memory subtests emerged as the first factor, possibly reflecting the relative importance of "fluid" compared to "crystallized" verbal abilities (Horn, 1976) in this age group. Principal component analyses of WMS-R and IQ scores by educational level yielded a three-factor solution for each group. Verbal and nonverbal factors were identified followed by an IQ-attention/concentration factor.
Chelune, Goormastic, and Naugle (1989) examined the construct validity of the WMS-R Index scores and individual subtests in principal components factor analyses of the WMS-R within the broader context of a preoperative neuropsychological battery for patients with intractable seizure disorders. Although the subject-to-variable ratio was less than optimal, the WMS-R Delayed Memory Index loaded with percent-retention scores for the Logical Memory and Visual Reproductions subtests, and emerged as a unique factor accounting for 10% of the explained variance. Inclusion of the individual immediate and delayed trials of the Verbal and Visual Paired AsSOCiates, Logical Memory, and Visual Reproduction subtests resulted in a factor structure in which a material-specific verbal learning and retention dimension emerged. The Visual Paired Associates subtests clustered with visuo-perceptual and motor tasks, whereas the Visual Reproduction trials loaded on a constructional praxis dimension. The latter finding is consistent with earlier observations that the WMS Visual Reproduction subtest appears to load on factors other than "memory" when the WMS is examined together with other neuropsychological tests (Larrabee et aI., 1985; Trahan & Larrabee, 1984).
In reviewing these early factor analytic studies, there is consistent evidence to support the psychometric basiS for the separate reporting of the WMS-R General Memory and Attention/Concentration Indexes (Bornstein & Chelune, 1988; Roid et aL, 1988; Wechsler, 1987). Separate verbal and nonverbal memory dimensions have also been noted (Bornstein &

84 CHELUNE Ef AL
Chelune, 1988, 1989), but only when both WMS-R immediate and delayed recall subtests are considered together. Tentative support for the separate reporting of the Delayed Memory Index within the context of a broad neuropsychological battery for seizure patients has been advanced by Chelune and his colleagues (1989), but this finding needs to be replicated in other, larger clinical samples.
IQ Versus ~R Index Discrepancy Scores
Discrepancies between the WAIS Full Scale IQ (FSIQ) and WMS Memory Quotient of 1~12 pOints have been suggested to be indicative of a specific memory deficit (Milner, 1975). Since the WMS is verbally biased, these discrepancies have been thought to reflect largely a verbal memory deficit (Milner, 1975; Prigatano, 1978). The WMS-Ryields separate Verbal and Visual Memory Index scores, providing the potential for examination of material-specific memory deficits in relation to W AIS-R IQ scores. The separate comparison of Verbal IQ (VIQ) versus the Verbal Memory Index and Performance IQ (PIQ) versus the Visual Memory Index is supported by several of the WMS-R factor analytic studies (Bomstein & Chelune, 1988; 1989), which not only indicate that the verbal and nonverbal WMSR subtests load on separate factors but that IQ scores are independent of these factor dimensions.
In a preliminary investigation, these material-specific IQ-Memory Index discrepancies were examined in a heterogenous clinical sample of 434 patients and in 110 normal subjects from the WMS-R standardization sample (prifitera, Bomstein, & Chelune, 1988). Results indicate that the distributions of these material-specific IQ-Memory Index discrepancies are very similar among the clinical and normal groups, and that it is not possible to identify a cutoff score that effectively discriminates the two groups. The previously suggested IQ-MQ discrepancy rule of 12 or more pOints identifies a large percentage of the patient group, but also misclassHies an almost equal percentage of the normal group. Clearly, these findings do not support the discriminative validity of VIQ-Verbal Memory Index or PIQ-Visual Memory Index discrepancies as indicators of material-specific memory deficits. It is not yet known whether discrepancies between WAIS-R FSIQ and the General Memory or Delayed Memory Indexes would provide useful clinical indicators of a general memory deficit. The results of this study underscore the need for test users to avoid application of clinical decision rules derived from research and practice with the WMS to data obtained with the WMS-R until they are empirically confirmed.

WECHSlER MEMORY SCALES-REVJSFJ>
Table 3 WMS-R Memory and W AJS.R IQ Dlacrepancles In Normal
and Clinical Samples
VIQ - Verbal Memory PIQ - Visual Memory
NormaP Cllnlcal NormaP Cllnlcal
85
(N =110) (N = 434) (N =110) (N = 434)
Mean 1.95 2.59 3.69 5.39
S.D. 13.02 16.49 11.97 13.45
Range -33 to 37 -41 to 44 -29 to 31 -37 to 46
Discrepancy > 12 24% 29% 25% 33% > 15 15% 23% 18% 24% > 22 5% 11% 5% 11%
Wote: Data for Normals copyright © 1988 The Psychological Corporation. All rights reserved.
VAUDITY STUDIFS
In the previous section we examined some of the psychometric properties of the WMS-R and several variables that affect its scores. In this section we examine some of the data that has emerged from the clinical application of the WMS-R among various patient populations. That is, we will turn our attention from issues of precision and reliability of measurement to those concerning the meaning of these measurements. As we will see, the potential validity of the WMS-R as a measure of memory function has been approached in a variety of ways.
Concurrent Validity
One approach to establishing the validity of a new measure is to correlate it with other measures that are presumed to assess the same construct. Since the WMS-R is a revision and extension of the original WMS, one would expect the WMS MQ to correlate with the various WMSR Index scores, especially the General Memory Index since it is most analogous to the MQ in content. In their comparison of the WMS and WMSR, Daniel, Dwarshuis, and Nelk (1988) found moderately strong correlations (.54 to .76) between the WMS MQ and the WMS-R Index scores. The weakest correlation was between the WMS MQ and the WMS-RAttention/ Concentration Index (.54), whereas the strongest correlation was be-

86 CHEUJNE IT AL
tween MQ and the WMS-R Delayed Memory Index (.76); the General Memory Index was correlated. 71 with WMS MQ scores.
The convergence between the WMS-R and the California Verbal Learning Test (CVL1), another new memory procedure (Delis, Kramer, Kaplan, & Ober, 1987), has been reported by Delis, Cullum, Butters, Cairns, and Prifitera (1988). While the WMS-R assesses the amount of information recalled on a number of tasks, the CVL T examines the multidimensional manner in which verbal information is acquired. A number of strong positive correlations were observed, including correlations of .927 between the WMS-R Delayed Memory Index and the Long Delay Free Recall score of the CVLT and .910 between the WMS-R Verbal Memory Index and the CVLT Ust A Trials 1-5 Total Recall index, a global index of learning efficiency. Similar convergence between several of the WMS-R verbal subtests (Logical Memory II and Verbal Paired Associates I and II) and measures of learning and retention from the Rey Auditory Verbal Learning Test (Rey, 1964) were observed in the factor study by Chelune, Goormastic, and Naugle (1989).
WM5-R and Subjective Ratings of Memory Deficit
Subjective complaints of memory impairment are associated with a wide variety of neurological and psychiatric conditions, and are often the reason that an individual comes to the attention of a clinician. While clinical decisions are sometimes influenced by a patient's or a relative's subjective report of memory dysfunction, studies of the relationship between memory self-ratings and objective memory performance often reveal low correlations (e.g., Chelune, Heaton, & Lehman, 1986; Larrabee & Levin, 1986; Sunderland, Harris, & Baddeley, 1983). However, the subjective impressions of patients, their relatives, and health-care professionals represent important external criteria in the evaluation of memory function, and several investigators have examined the relationship between subjective ratings of memory deficit and performance on theWMS-R.
As part of the clinical validation data that were collected during the field trials with the WMS-R (Wechsler, 1987), knowledgeable caregivers were asked to rate the frequency of patients' everyday memory difficulties (e.g., misplacing personal belongings, forgetting appOintments, etc.) using a specially designed 14item Memory Impairment Rating Form (MIRF). The WMS-R manual (Wechsler, 1987, p. 79) reports significant negative correlations for a sample of 317 clinical patients between the MIRF and the General Memory and Verbal Memory Indexes (-.38), the Delayed Memory Index (-.36), the Visual Memory Index (-.31), and the Attention/Concentration Index (-.26). Ryan and Lewis (1988) also used the MlRF to examine the relationship of both self-reports and reports of

WECHSLER MEMORY SCALES-REVlSFD 87
knowledgeable caregivers and actual WMS-R performances among a sample of 40 recently detoxified alcoholics. Self-rated MIRF scores did not correlate with any of the WMS-R Indexes or subtest scores. However, MIRF observer ratings were significantly correlated with performance on the Visual Memory Span (-.35), Verbal Paired Associates I (-.33), and Visual Reproductions I and II (-.41 and -.38, respectively).
Fischer (1988) investigated the relationship between performance on the WMS-R by a group of multiple sclerosis patients (N = 45) and subjective judgments of memory impairment made by the patients, their relatives, a neurologist and a psychologist, controlling for differences in demographic variables, disease characteristics, and depression. Similar to the findings of Ryan and Lewis (1988), self-rated memory difficulties, using the Patient Assessment of Own Functioning Inventory (PAF: Chelune, Heaton, & Lehman, 1986), did not correlate with WMS-R performance, although they did correlate (.43) with self-reported depression. Relative's ratings of everyday memory disturbances using the MIRF and a relative's version of the PAFwere correlated with the General Memory (-.39 and -.29) and Delayed Memory (-.18 and -.28) Indexes. The psychologist's subjective ratings of memory impairment also correlated with the General Memory Index (-.41) and the Delayed Memory Index (-.38), as did the neurologist's ratings (-.26 and -.39, respectively).
While patients' subjective experiences of memory difficulty often bring them to the attention of health-care professionals, they do not necessarily predict their level of performance on objective measures of memory function such as the WMS-R. The lack of correspondence may, in part, be due to the fact that objective measures are norm-referenced while self-reports are inherently ipsative in nature and reflect withinsubject changes from a personal baseline. The association of WMS-R scores with ratings of memory disturbance by caregivers and health-care professionals is more encouraging, and suggests that the WMS-R can be used to document these subjective impressions.
WMS-R and Work Status
An increasingly important issue in neuropsychological research and practice is whether test procedures have ecological validity in terms of everyday functioning as weil as neurodiagnostic validity (Chelune & Moehle, 1986; Loring & Papanicolaou, 1987; Sunderland, Harris, & Gleave, 1984). Crossen and Wiens (1988, p. 185) were the first "to assess the criterion validity of the WMS-R with reference to competitive employment, and [sic] important aspect of real-world functioning." They examined WMS-R performances among a sample of 20 industrial painters with a history of solvent exposure and evidence of memory impairment on a series of previously administered memory tests. At the time of evaluation

88 CHELUNE ET AL
with the WMS-R, 12 of the painters were gainfully employed on a full or part-time basis and eight were chronically unemployed. Employed individuals obtained higher WMS-R Index scores than those who were unemployed, with the group comparisons being significant for all of the WMSR Indexes except Visual Memory. These differences could not be accounted for by differences in age or education. While Crossen and Wiens' (1988) findings are encouraging, additional research is needed to explore the everyday correlates of various WMS-R memory patterns.
W~R Perfonnance Patterns Among Selected Clinical Groups
Since memory deficits are a hallmark of many psychiatric and neurologic disorders, one would expect patients with these disorders to perform more poorly on the WMS-R than normal controls. The WMS-R man ual (Wechsler, 1987, p. 78-86) provides preliminary data on anum ber of these patient populations, which generally support the clinical validity of the WMS-R as a useful measure of memory function in these patient populations. While we strongly encourage the interested reader to review these data, we will focus our review on those data that have been published elsewhere in the research literature or have been presented at scientific meetings.
Dementia. Dementia is a cognitive/behavioral syndrome associated with a number of neurologic disorders in which memory impairment is often a central component. Butters and his colleagues (Butters et al., 1988; Jacobs, Troster, Salmon, & Butters, 1988; Jacobs, Troster, Salmon, Cermak, Chelune, & Butters, 1989; Troster et al., 1989) have examined WMS-R performances among a number of these patient groups. In their initial study, Butters and others (1988) compared the WMS-R performances of groups of Alzheimer's Disease and Huntington's Disease patients to normal controls and amnesic patients with presumed diencephalic and mesial temporal dysfunction. They found that amnesic patients could be differentiated from controls and demented patients on the basis of difference scores between the Attention/Concentration and General Memory Indexes and between the General Memory and Delayed Memory Indexes. In addition, Alzheimer's Disease and amnestic patients had lower percent-retention scores on the WMS-R Logical Memory and Visual Reproduction subtests than normal controls and Huntington's Disease patients, suggesting that they have an abnormal rate of forgetting. Based on these findings, Butters et al. (1988) report that the WMS-R appears to be useful in not only distinguishing demented patients from amnesiacs but also a potential aid in differentiating some forms of "cortical" versus "subcortical" dementia.
In an extension of the Butters et al. (1988) study, Troster and his colleagues (1989) examined WMS-R performance patterns among Alz-

WECHSlER MEMORY SCALES-REVISFD 89
heimer's Disease and Huntington's Disease patients with mild and moderate degrees of dementia as determined by their Mattis (1976) Dementia Rating Scale scores. The patient groups not only performed more poorly than their respective control groups, but within-patient group comparisons demonstrated that the moderately demented groups earned significantly lower WMS-R Index scores than their mildly demented counterparts. The latter finding provides support for the incremental sensitivity of the WMS-R. The Huntington's Disease patients had significantly lower Attention/Concentration and Visual Memory Indexes than the Alzheimer's patients at both levels of dementia, but the Alzheimer's patients demonstrated a faster rate of forgetting Qower percent-retention scores) than the Huntington's Disease patients across levels of dementia. These findings are consistent with previous research (Moss, Albert, Butters, & Payne, 1986), and suggest that the WMS-R is sensitive to the progressive memory impairment seen in these dementing illnesses and can also be used to distinguish disorders with presumed differential deficits in consolidation versus retrieval.
Unilateral Braln LesloD8. The functional asymmetry of verbal and nonverbal abilities within the left and right cerebral hemispheres is a basic tenet in neuropsychological theory (Lezak, 1983). While the original WMS has been criticized as largely a measure of verbal memory (Milner, 1975), material-specific memory deficits following unilateral brain lesions have been demonstrated using experimental procedures (Kimura, 1963; Milner, 1968; Weingartner, 1968) and modifications of the WMS (Bomstein, 1982; Delaney, Rosen, Mattson, & Novelly, 1980; Russell, 1975). Generally, individuals with left hemisphere lesions manifest difficulties with verbal memory, whereas those with right hemisphere lesions reveal deficits in visual/perceptual memory. That is, there is a double dissociation of material-specific memory function associated with unilateral brain lesions. Several investigations of the WMS-R among patients with unilaterallesions have been conducted.
Chelune and Bornstein (1988b) examined WMS-R patterns of performance among 115 patients with unilateral lesions. Group comparisons of the WMS-R Index scores between the 56 patients with right-hemisphere (RH) lesions and the 59 patients with left-hemisphere (LH) lesions demonstrated a significant difference on only the Verbal Memory Index, with the LH group performing more poorly than the RH group. Multivariate group comparisons of the WMS-R subtests was significant, with univariate differences being found for Logical Memory I and II and Verbal Paired Associates I and II. Consistent with the earlier analysis, the LH group was more impaired on these "verbal" subtests than the RH group. Withinsubject comparisons of the percent-retention scores for the Logical Memory and Visual Reproduction subtests yielded a significant interaction effect, reflecting a double dissociation of function. To further explore
90 CHELUNE IT AI-
the double dissociation of verbal and nonverbal memory functions with the WMS-R, Chelune and Bomstein (1988b) conducted a multivariate repeated measures analysis of five memory dimensions with verbal and nonverbal WMS-R analogs (e.g., Verbal versus Visual Paired Associates). A significant multivariate interaction was obtained, with four of the five univariate interaction effects being Significant. Based on these withinsubject double dissociation effects, the authors conclude that there is "strong, albeit preliminary, support for the validity of the new WMS-R as a measure of modality-specific memory deficits" (p. 127).
Expanding on their earlier work, Chelune and Bomstein (1988a) examined WMS-R performance patterns among a larger sample (N = 182) of patients with unilateral leSions, subdivided into temporal and nontemporal groups. It was hypothesized that between-group differences would be more evident for those patients with temporal lobe lesions than those with extra-temporal lesions because of the temporal lobe's critical role in the formation of new memories. Significant between-group laterality effects were found for the General Memory, Verbal Memory, and Delayed Memory Indexes, with the LH patients performing more poorly than RH patients, regardless of location within the hemisphere. When withinsubject discrepancies between the Verbal Memory and Visual Memory Indexes were examined, there was a significant Laterality X Location interaction. However, the expected double dissociation of verbal versus visual memory deficit was primarily evident in the nontemporal rather than temporal groups. In contrast, a significant Laterality X Location interaction was observed for Logical Memory versus Visual Reproduction percent-retention discrepancy scores, but with the temporal lobe groups showing the expected double dissociation of function. These results highlight potential differences in the meaning of various WMS-R Indexes and derived scores as well as neuroanatomical substrates that mediate immediate recall of material-specific information (Le., the WMSR Verbal and Visual Memory Indexes) and the effiCiency of memory over time (Le., percent-retention scores).
Seizure Disorders. Complaints of memory impairment are common among patients with seizure disorders, especially those with temporal lobe epilepsy (fLE). Consistent with the literature on unilateral lesions, patients with longstanding epileptogenic lesions often manifest materialspecific memory deficits depending on the hemisphere of origin. These "hemisphere-specific memory deficits are often exacerbated following temporal lobectomy for seizure control" (Novelly, Augustine, Mattson, Glaser, Williamson, Spenser, & Spenser, 1984, p. 64). These general observations are qualified by such variables as seizure type, underlying etiology, location, seizure frequency, age of onset, duration, and type of EEG abnormality (Bomstein, Pakalnis, Drake, & Suga, 1988).
Bomstein and his colleagues (1988) have examined the WMS-Rcorre-

WECHSlER MEMORY SCALB-REV5D 91
lates of seizure type and waveform abnormality. Patients with primary generalized seizures have typically been found to perform less well on neuropsychological batteries than those with complex-partial seizures (CPS) (Dodrill, 1981; Klove & Matthews, 1974); however, measures of memory function are generally not included in these comparisons. Bornstein and colleagues (1988) found that patients with primary generalized seizures did not differ from controls on the WMS-R, whereas those with CPS did show some deficits on WMS-R measures of learning and delayed retention, especially for nonverbal material. Patients with spike-andwave abnormalities were also more impaired than those with EEG slowing on nonverbal WMS-R subtests, possibly due to the greater number of patients right-sided foci in the spike-and-wave group. The authors (Bomstein et al., 1988, p. 887) suggestthat "the finding of greater memory deficit in the current series of patients with CPS, and the previous reports of greater neuropsychological deficit in patients with generalized or mixed disorders, represents a form of double dissociation of deficits, ie, [sic] certain seizure types are related to different types of cognitive deficit."
In a small, mixed group of operated and non-operated TLE seizure patients, Loring, Lee, Martin, and Meador (1988) found that WMS-R differences between the Verbal and Visual Memory Indexes incorrectly lateralized the seizure focus in some patients. This contrasts with the findings of Troster, Watson, Iragui, and Butters (1988) who found that patients with well-defined left TLE foci not only obtained lower General Memory Index scores than those with right TLE foci, but also had lower mean Verbal Memory Index scores but slightly higher Visual Memory Index scores than patients with right TLE foci. Similar to the findings of Loring and colleagues (1988), Bomstein, Pakalnis, and Drake (1989) also found no differences on any of the WMS-R Index scores between unoperated patients with complex-partial seizure disorders of right versus left temporal origin. However, the authors did observe significant group differences in percent-retention scores. Patients with left TLE showed a 22% superiority in their rate of retention of the Visual Reproduction stimuli compared to the Logical Memorystimuli. In contrast, the right TLE group revealed a 29% superiority in their delayed retention of Logical Memory versus Visual Reproduction material. The contradictory nature of the findings in these studies could well reflect differences in subject selection procedures and the homogeneity and extent of underlying pathology.
With advances in mapping techniques and more refined diagnostic criteria, surgical intervention has become an effective treatment approach for many TLE patients with intractable seizure disorders (Chelune & Liiders, 1988). However, memory deficits remain a major complication of epilepsy surgery, especially when the dominant hemisphere is resected in high functioning individuals (Ojemann & Dodrill, 1985).
92 CHELUNE Ef AL
Naugle, Chelune, and Liiders (1988) examined the relationship between presurgical memory ability and extent of change in memory functioning following temporal lobectomy using the WMS-R. Consistent with the concerns raised by Ojemann and Dodrill (1985), patients with higher presurgical WMS-R Index scores showed the greatest degrees of memory loss on all of the WMS-R Index scores following left temporal lobectomy. However, no relationship was found between WMS-R presurgical memory levels and subsequent changes from baseline among the right temporal lobectomy patients. This is not to say that patients undergoing right temporal lobectomies are not at risk for some decrement in memory function, but rather that presurgical level of memory ability is not a good predictor of outcome in this group.
Chelune, Liiders, and Dinner (1988) examined WMS-R patterns of performance pre- and post-temporal lobectomy among 23 patients with intractable seizure disorders of well-defined temporal origin. Eleven patients underwent right temporal lobectomies and 12 had left temporal lobectomies. Both groups were matched on demographic variables, testretest interval, and presurgical IQ scores. No differences were observed on any of the WMS-R Index scores prior to surgery. However, following surgery the left temporal lobectomy group performed significantlyworse than the right lobectomy group on the Verbal Memory Index, with trends in the same direction also observed for the General Memory and Delayed Memory Indexes. Examination of Verbal Memory versus Visual Memory Index discrepancy scores before and after surgery demonstrated a surgically-induced double dissociation effect for material-specific immediate memory. Using the WMS-R age-percentile scores from the manual (Wechsler, 1987, p.I38-141) for the Logical Memory and Visual Reproduction subtests, Similar surgically-related double dissociation effects were found for both the immediate and delayed memory trials of these material-specific subtests. Consistent with previous research (Rausch & Crandall, 1982), there was not only the expected decrement in materialspecific delayed memory in the operated hemisphere, but a slight increase in delayed memory for material thought to be mediated by the contralateral hemisphere.
WMS-R and Other Padent Groups. Fischer (1988b) compared the WMS-R performances of 45 patients with documented multiple sclerosis (MS) with those of 25 matched normal controls. The MS patients performed more poorly than the controls on all five of the WMS-R Index scores. Cluster analysis of the MS patients' performances yielded three clinical subgroups with different levels and patterns of memory ability. One group appeared essentially intact, whereas a second group manifested a marked, global memory impairment. The third group appeared to have "intact attention/short-term memory but displayed milder deficits in learning and long-term memory. There was suggestive evidence

WECHSlER MEMORY ~REVlSED 93
that relapsing/progressive MS patients were more likely than others to be globally impaired" (Fischer, 1988b, p. 149).
Ryan and Lewis (1988) contrasted the WMS-R performances of 40 recently detoxified male alcoholics with a matched group of normal male controls drawn from the WMS-R standardization sample (Wechsler, 1987). The alcoholic group performed more poorly than the controls on the WMS-R Digit Span, Logical Memory I and II, and Visual Reproduction I and II subtests and on each of the five WMS-R Index scores. While the two groups differed significantly in terms of level of performance, they manifested a similar pattern of performance. Since previous research has failed to show an alcohol-related decrement in WMS MQ (Lorberg, 1980; Parsons & Prigatano, 1977), Ryan and Lewis (1988, p. 178) suggest that "the WMS-R composite scores, including the General Memory Index, are more sensitive to alcohol-related memory deficits than is the composite MQ from the original WMS."
SUMMARY In this chapter we have attempted to critically review and evaluate
both the strengths and limitations of the Wechsler MemoryScale-Revised (WMS-R). It is clear that the test is a substantial departure from its predecessor, the Wechsler Memory Scale (WMS), both in terms of structure and content. Its psychometric properties are adequately detailed in the manual, the scoring criteria are carefully delineated in an objective manner, age norms are provided for much of the life-span, and memory is treated as a multidimensional construct. Data from a variety of clinical studies suggest that the WMS-R is more sensitive than the WMS to memory impairments in general, and its multidimensional structure provides a means for characterizing differences in memory impairment associated with different neurological diseases and syndromes. However, it is equally clear that the WMS-R is not without limitations and intrinsic biases. The reliability of the individual subtests is marginal in some cases, the standard errors of measurement for the summary Index scores are rather large, the visual subtests may not be truly "nonverbal" in that they are susceptible to verbal mediation, little attention is given to recognition memory and cued recall, and the content of the General Memory and Delayed Memory Indexes are verbally-biased, especially in terms of practice effects.
In evaluating the WMS-R, the test user must decide what the comparison standard should be. If one wants a measurement device that comprehensively and precisely assesses the various facets of memory within a conceptual framework that is consistent with state-Qf-the-art cognitive and neuropsychological theory, the WMS-R will undoubtedly fall far

94 CHELUNE EI' AL
short. However, it is unlikely that any of the memory scales that are currently available would come close to meeting this standard. Thus, if the test user is content with using the WMS-R within the constraints of its limitations, and perhaps in conjunction with other memory tests, then it may prove to be a highly useful measure of memory function. Final acceptance of the WMS-R as a worthy successor of the WMS will depend on how useful it proves to be in clinical practice and research. To date, the research literature suggests that its prospects are optimistic.
REFERENCFS Bachach, H., & Mintz, J. (1974). The Wechsler Memory Scale as a tool for the
detection of mild cerebral dysfunction. Journal of Clinical Psychology, 3D, 58-60.
Boll, T.J. (1981). The Halstead-Reitan Neuropsychological Battery. In S.B. Fllskov & TJ. Boll (Eds.), Handbook of clinical neuropsychology (pp. 577-607). New York: Wiley.
Bornstein, R.A. (1982). Effects of unilateral lesions on the Wechsler Memory Scale. Journal of Clinical Psychology, 38, 389-392.
Bornstein, RA, & Chelune, G.J. (1988). Factor structure of the Wechsler Memory Scale-Revlsed. The Clinical Neuropsychologist, 2, 107-115.
Bornstein, RA, & Chelune, GJ. (1989). Factor structure ofthe Wechsler Memory Scale-Revlsed In relation to age and educational level. Archives of Clinical Neuropsychology, 4, 15-24.
Bornstein, RA, Pakalnls, A., & Drake, M.E. (1989). Verbal and nonverbal memory and learning In patients with complex partial seizures of temporal lobe origin. Journal of Epilepsy, I, 203-208.
Bornstein, RA, Pakalnls, A., Drake, M.E., &Suga, LJ. (1988). Effects of seizure type and waveform abnormality on memory and attention. Archives of Neurology, 45. 88~87.
Butters, N., Salmon, D.P., Cullum, C.M., Carlns, P., Troster, A.I., &Jacobs, D. (1988). Differentiation of amnesic and demented patients with the Wechsler Memory Scale-Revlsed. The Clinical Neuropsychologist, 2, 133-148.
Chelune, GJ., & Bornstein, R.A. (1988a). Memory characteristics of patients with unilateral temporal and nontemporal lesions. The Clinical Neuropsychologist. 2.275.
Chelune, G.J., & Bornstein, RA (1988b). WMS-R patterns among patients with unilateral brain lesions. The Clinical Neuropsychologist, 2. 121-132.
Chelune, GJ., Ferguson, W., & Moehle, K. (1986). The role of standard cognitive and personality tests In neuropsychological assessment. In T. Incagnoli, G. Goldstein, & C.J. Golden (Eds.), Clinical application of neuropsychological test batteries (pp. 75-119). New York: Plenum.
Chelune, G.J., Goormastlc, M., & Naugle, R.I. (1989). Construct validity of the Wechsler Memory Scale-Revised (WMS-R) within the context of a neuropsychological battery for seizure patients. Journal of Clinical and Experimental Neuropsychology, II, 63.

WECHSLER MEMORY SCALES-REVISED 95
Chelune, GJ., Heaton, R.K., & Lehman, R.A.W. (1986). Neuropsychological and personality correlates of patients' complaints of disability. In G. Goldstein & R.E. Tarter (Eds.), Advances in clinical neuropsychology: Vol. 3 (pp. 95-126). New York: Plenum.
Chelune, G.J., Katz, A., Awad, I., Naugle, R.I., Liiders, H., & Kong, A. (1989). Relationship of memory changes to resection parameters In temporallobectomy patients. Journal of Clinical and Experimental Neuropsychology, II, 23.
Chelune, G.J., & Liiders, H. (1988). Memory functions and electrical stimulation of the temporal lobe In man. Advances in Neurological Sciences, 32, 70~717.
Chelune, G.J., Liiders, H., & Dinner, D. (1988). Patterns of memory performance pre- and post-temporallobectomy. The Clinical Neuropsychologist, 2, 284.
Chelune, G.J., & Moehle, K. (1986). Neuropsychological assessment and everyday functioning. In D. Wedding, A.M. Horton, & J. Webster (Eds.), The neuropsychology handbook (pp. 488-525). New York: Springer.
Crossen, J.R., & Wiens, A.N. (1988). Wechsler Memory Scale-Revised: Deficits In performance associated with neurotoxic solvent exposure. The Clinical Neuropsychologist, 2, 181-187.
Daniel, L.A., Dwarshuls, L., & Nelk, K. (1988, November). Comparisons of the Wechsler Memory Scale (WM5) and Wechsler Memory Scale-Revised (WMS"-R) in a population of neuropsychologically impaired patients using three methods of data collection. Paper presented at the 8th annual meeting of the National Academy of Neuropsychologists, Orlando, FL.
Davis, L.J., & Swenson, W.M. (1970). Factor analysis of the Wechsler Memory Scale. Journal of Consulting and Clinical Psychology, 35, 430.
Delaney, R.C., Rosen, A.J., Mattson, R.H., & Novelly, R.A. (1980). Memory function in focal epilepsy: A comparison of nonsurgical unilateral temporal lobe and frontal lobe samples. Cortex, 16, 103-117.
Dells, D.C. (1989). Neuropsychological assessment of learning and memory. In F. Boller &J. Grafman (Eds.), Handbook of neuropsychology. Amsterdam: Elsevier.
Dells, D.C., Cullum, C.M., Butters, N., Calms, P., & Prlfitera, A. (1988). Wechsler Memory Scale-Revised and California Verbal learning Test: Convergence and divergence. The Clinical Neuropsychologist, 2, 188-196.
Dells, D.C., Kramer, J, Kaplan, E., & Ober, B. (1987). The California Verbal Learning Test-Research Edition. New York: Psychological Corporation.
Dodrill, C.B. (1981). Neuropsychology of epilepsy. In S.B. Filskov & T .J. Boll (Eds.), Handbook of clinical neuropsychology: Vol. I (pp. 366-395). New York: Wiley.
Erickson, R.C., & Scott, M.L. (1977). Clinical memory testing: A review. Psychological Bulletin, 84, 11~1149.
Fischer, J.S. (1988a). Dissociation between subjective and objective memory measures in multiple sclerosis. The Clinical Neuropsychologist, 2, 275.
Fischer, J.S. (1988b). Using the Wechsler Memory Scale-Revised to detect and characterize memory deficits In multiple sclerosis. The Clinical Neuropsychologist, 2, 149-172.
Gulliksen, H. (1950). Theory of mental tests. Hillsdale, N.J.: Lawrence Erlbaum Associates.
Heaton, R.K., Grant, I., & Matthews, C.G. (1986). Differences In neuropsychological test performance associated with age, educatlonand sex. In I. Grant & K.M. Adams (Eds.), Neuropsychological assessment of neuropsychiatric disorders (pp. 1O~120). New York: Oxford.

96 CHELUNE IT AL
Herman, D.O. (1988). Development of the Wechsler Memory Scale-Revised. The Clinical Neuropsychologist, 2, 102-106.
Horn, J.L. (1976). Human abilities: A review of research and theory in the early 1970's. Annual Review of Psychology, 27, 437-485.
Jacobs, D., Troster, A.l., Salmon, D.P., & Butters, N. (1988). Intrusion errors in figural memory performance of demented patients. The Clinical Neuropsychologist, 2, 274.
Jacobs, D., Troster, A.I., Salmon, D.P., Cermak, L.S., Chelune, GJ., & Butters, N. (1989). Intrusion errors in the figural memory of amnesic and demented patients. Journal of Clinical and Experimental Neuropsychology, II, 62.
Kaszniak,A. W. (1987). Neuropsychological consultation to geriatricians: Issues in the assessment of memory complaints. The Clinical Neuropsychologist, I, 35-46.
Kear-ColweII, JJ. (1973). The structure of the Wechsler Memory Scale and Its relationship to 'brain damage: British Journal of Social and Clinical Psychology, 12, 3~92.
Kimura, D. (1963). Right temporal lobe damage. Archives of Neurology, 8, 264-271. Kiove, H., & Matthews, C.G. (1974). Neuropsychological studies of patients with
epilepsy. In R.M. Reitan & LA Davison (Eds.), Clinical neuropsychology: Current status and applications (pp. 237-265). New York: Wiley.
Larrabee, G.J. (1987). Further cautions In Interpretation of comparisons between the W AlS-R and Wechsler Memory Scale. Journal of Clinical and Experimental Neuropsychology, 9, 456-460.
Larrabee, GJ., Kane, R.L., Schuck, J.R., & Francis, D.J. (1985). Construct validity of various memory testing procedures. Journal of Clinical and Experimental Neuropsychology, 7, 497-504.
Larrabee, G.J., & levin, H.S. (1986). Memory seU.f"atings and objective test performance In a normal elderly sample. Journal of Clinical and Experimental Neuropsychology, 8, 275-284.
Lezak, M.D. (1983). Neuropsychological assessment (2nd Ed.). New York: Oxford. Lorberg, T. (1980). Alcohol misuse and neuropsychological deficits in men. Journal of Studies on Alcohol, 41, 119-128.
Loring, D.W. (1989). The Wechsler Memory Scale-Revised, or the Wechsler Memory Scale-Revisited? The Clinical Neuropsychologist, 3, 59-69.
Loring, D.W., Lee, G.P., Martin, R.C., & Meador, K.J. (1988). The WMS-R Incorrectly predicts lateralized temporal-lobe dysfunction. The Clinical Neuropsychologist, 2, 284.
Loring, D.W., & Papanicolaou, A.C. (1987). Memory assessment In neuropsychology: Theoretical considerations and practical utility. Journal of Clinical and Experimental Neuropsychology, 9, 340-358.
Matarazzo, J.D. (1972). Wechsler's measurement and appraisal of adult intell igence (5th Ed). Baltimore, MD: Wllliams & Wilkins.
Matarazzo, J.D., & Herman, D.O. (1984). Base rate data for the W AlS-R: Test-retest stability and VIQ-PIQ differences. Journal of Clinical Neuropsychology, 6,351-366.
Mattis, S. (1976). Mental status examination for organic mental syndrome in the elderly patient. In L. Bellack & T.B. Karasu (Eds.), Geriatric psychiatry (pp. 77-121). New York: Grune & Stratton.

WECHSlER MEMORY SCALFS-REVlSFD 97
Milner, B. (1968). Visual recognltlonand recall after right temporal lobe excision In man. Neuropsychologia, 6, 11-26.
Milner, B. (1971). Interhemispheric differences In the localization of psychological processes In man. British Medical Bulletin, 27, 272-277.
Milner, B. (1975). Psychological aspects of focal epilepsy and Its neurosurgical management. Advances in Neurology, 8, 299-321.
Mishkin, M., & Appenzeller, T. (1987). The anatomy of memory. Scientific American, 256, 8()..89.
Moss, M.B., Albert, M.S., Butters, N., & Payne, M. (1986). Differential patterns of memory loss among patients with Alzheimer's disease, Huntington's disease and alcohol Korsakoffs syndrome. Archives of Neurology, 43, 239-246.
Naugle, R.I., Chelune, G.J., & L\iders, H. (1988). The relationship between presurgical memory function and memory changes following temporal lobectomy. Epilepsia, 29, 669.
Novelly, R.A., Augustine, E.A., Mattson, R.H., Glaser, G.H., Williamson, P.O., Spenser, D.O., & Spenser, S.S. (1984). Selective memory Improvement or impairment In temporal lobectomy for epilepsy. Arch ives of Neurology, 15, 64-67.
Ojemann, G., & Dodrill, C.B. (1985). Verbal memory deficits after temporal lobectomy for epilepsy. Journal of Neurosurgery, 62, 101-107.
Parsons, O.A., & Prlgatano, G.P. (1977). Memory functioning In alcoholics. In I.M. Burnbaum & E.S. Parker (Eds.), Alcohol and human memory (pp. 185-194). Hillsdale, NJ: Erlbaum.
Poon, L.W. (Ed.) (1986). Handbook for clinical memory assessment of older adults. Washington, DC: American Psychological Association.
Powell, J. (1988). Wechsler Memory Scale-Revised: Test review. Archives of Clinical Neuropsychology, 3, 397-403.
Power, D.G., Logue, P.E., McCarthy, S.M., Rosenstlel, A.K., & Ziesat, H.A. (1979). Inter-rater reliability of the Russell Revision of the Wechsler Memory Scale: An attempt to clarify some ambiguities In scoring. Journal of Clinicai Neuropsychology, I, 343-345.
Prifitera, A., & Barley, W.O. (1985). Cautions in Interpretation of comparisons of the W Al~R and the Wechsler Memory Scale. Journal of Consulting and Clinical Psychology, 53, 564-656.
Prifitera, A., Bornstein, R.A., & Chelune, G.J. (1988).IQ/memory discrepancies on the Wechsler Memory Scale-Revised. The Clinical Neuropsychologist, 2, 273.
Prlgatano, G.P. (1978). Wechsler Memory Scale: A selective review of the literature. Journal of Clinical Psychology, 34, 816-832.
Randt, C.T., Brown, E.R., & Osborne, D.P. (1980). A memory test for longitudinal measurement of mild to moderate deficits. Clinical Neuropsychology, 2, 184-194.
Rausch, R., & Crandall, P.H. (1982). Psychological status related to surgical control of temporal lobe seizures. Epilepsia, 23, 191-202.
Rey, A. (1964). L'examen cllnique en psychologie. Paris: Presses Universitalres de France. Rold, G.H., Prifitera, A., & Ledbetter, M. (1988). Confirmatory analysis of the structure of the Wechsler Memory Scale-Revised. The Clinical Neuropsychologist. 2. 116-120.
Russell, E.W. (1975). A multiple scoring method for the assessment of complex memory functions. Journal of Consulting and Clinical Psychology, 43, 80()..809.

98 CHELUNE EI' AL
Russell, E.W. (1982). Factor analysis of the revised Wechsler Memory Scale tests In a neuropsychological battery. Perceptual and Motor Skills, 54, 971-974.
Russell, E.W. (1988). Renormlng Russell's version of the Wechsler Memory Scale. Journal ofOinical and Experimental Neuropsychology, 10,235-249.
Ryan, J.J., & lewis, C.V. (1988). Comparison of normal controls and recently detoxified alcoholics on the Wechsler Memory Scale-Revised. The Clinical Neuropsychologist, 2, 173-180.
Seretny, M.L., Dean, R.S., Gray, J.W., & Hartlage, L.C. (1986). The practice of clinical neuropsychology In the United States. Archives of Oinical Neuropsychology, I, 5-12.
Skllbeck, C.E., & Woods, R.T. (1980). The factorial structure of the Wechsler Memory Scale: Samples of neurological and psychogeriatrtc patients. Journal of Clinical Neuropsychology, 2, 293-300.
Squire, L.R. (1987). Memory and brain. New York: Oxford. Sunderland, A., Harrls, J.E., & Baddeley, A. (1983). Do laboratory tests predict
everydaymemory? A neuropsychological study. Journal of Verbal Learning and Verbal Behavior, 22, 341-357.
Sunderland, A., Harris, J.E., & Gleave, J. (1984). Memory fallures in everyday life following severe head Injury. Journal of Clinical Neuropsychology, 6, 127-142.
Sweet, J J., & Wysocki, J J. (1982).lmprovlng interscorerrellabillty ofthe Wechsler Memory Scale: A pilot study. Clinical Neuropsychology, 4, 159-161.
Trahan, D.E., & Larrabee, G.J. (1984, February). Construct validity and normative data for some recently developed measures of visual and verbal memory. Paper presented at the annual meeting of the International Neuropsychological Society, Houston, TX.
Troster, AJ., Butters, N., Salmon, D.P., Jacobs, D., Cullum, C.M., & Moss, M. (1989). Differentiation of mild and moderate Alzheimer's and Huntington's Disease with the Wechsler Memory Scale-Revised. Journal of Clinical and Experimental Neuropsychology, II, 52.
Troster, A.I., Watson, D.P., Iraqul, V., & Butters, N. (1988). Interlctal memory performance In unilateral temporal lobe epilepsy: An Initial evaluation with the Wechsler Memory Scale-Revised. Epilepsia, 29, 681.
U.S. Bureau of the Census. (1983). Census of population: 1980, General population characteristics, Part I, United States Summary PC 80-I-BI, Table 54. Washington, DC: U.S. Government Printing Office.
U.S. Bureau ofthe Census. (1984). Census of population: 1980, Detailed population characteristics. United States Summary PC 80-I-DI-A, Section A: United States, Table 262. Washington, DC: U.S. Government Printing Office.
Warrington, E.K. (1984). Recognition Memory Test. Berkshire, GB: Nfer-Neslon. Wechsler, D.A. (1945). A standardized memory scale for clinical use. Journal of
Psychology, 19,87-95. Wechsler, D, A. (1981). Wechsler Adult Intelligence Scale-Revised: Manual. New
York: Psychological Corporation. Wechsler, D.A. (1987). Manual for the Wechsler Memory Scale-Revised. New York:
Psychological Corporation. Weingartner, H. (1968). Verballeamlng In patients with temporal lobe lesions.
Journal of Verbal Learning and Verbal Behavior, 7, 520-526.

WECHSlER MEMORY ~REVJSEI) 99
Williams, J.M. (1983). The Vennont Memory Scale: Initial studies of reliability and validity. UnpubUshed doctoral dissertation, University of Vermont.
Wllson, B.A. (1987). Rehabilitation of memory. New York: GtUord.