The use of biochemical markers of bone remodeling in ... · The use of biochemical markers of bone...
13
REVIEW The use of biochemical markers of bone remodeling in multiple myeloma: a report of the International Myeloma Working Group E Terpos 1 , MA Dimopoulos 1 , O Sezer 2 , D Roodman 3 , N Abildgaard 4 , R Vescio 5 , P Tosi 6 , R Garcia-Sanz 7 , F Davies 8 , A Chanan-Khan 9 , A Palumbo 10 , P Sonneveld 11 , MT Drake 12 , J-L Harousseau 13 , KC Anderson 14 and BGM Durie 5 on behalf of the International Myeloma Working Group 1 1 Department of Clinical Therapeutics, University of Athens School of Medicine, Athens, Greece; 2 Department of Hematology, Oncology and Stem cell Transplantation, University Medical Center Hamburg, Hamburg, Germany; 3 Department of Medicine, University of Pittsburgh Medical Center, Pittsburgh, PA, USA; 4 Department of Hematology, Odense University, Odense, Denmark; 5 Cedars-Sinai Outpatient Cancer Center at the Samuel Oschin Comprehensive Cancer Institute, Los Angeles, CA, USA; 6 Institute of Hematology and Oncology, University of Bologna, Bologna, Italy; 7 Department of Hematology, Hospital Universitario de Salamanca, Salamanca, Spain; 8 Institute of Cancer Research and Royal Marsden Hospital, Section of Haemato-oncology, Sutton, Surrey, UK; 9 Department of Medicine, Roswell Park Cancer Institute, Buffalo, NY, USA; 10 Divisione di Ematologia, University of Torino, Torino, Italy; 11 Department of Hematology, Erasmus Medical Center, Rotterdam, The Netherlands; 12 Division of Endocrinology, Mayo Clinic, Rochester, MN, USA; 13 Institut de Biologie, Laboratoire d’Hematologie, Nantes, France and 14 Division of Hematologic Malignancies, Department of Medical Oncology, Dana-Farber Cancer Institute, Boston, MA, USA Lytic bone disease is a frequent complication of multiple myeloma (MM). Lytic lesions rarely heal and X-rays are of limited value in monitoring bone destruction during anti- myeloma or anti-resorptive treatment. Biochemical markers of bone resorption (amino- and carboxy-terminal cross-linking telopeptide of type I collagen (NTX and CTX, respectively) or CTX generated by matrix metalloproteinases (ICTP)) and bone formation provide information on bone dynamics and reflect disease activity in bone. These markers have been investigated as tools for evaluating the extent of bone disease, risk of skeletal morbidity and response to anti-resorptive treatment in MM. Urinary NTX, serum CTX and serum ICTP are elevated in myeloma patients with osteolytic lesions and correlate with advanced disease stage. Furthermore, urinary NTX and serum ICTP correlate with risk for skeletal complications, disease progression and overall survival. Bone markers have also been used for the early diagnosis of bone lesions. This International Myeloma Working Group report summarizes the existing data for the role of bone markers in assessing the extent of MM bone disease and in monitoring bone turnover during anti-myeloma therapies and provides information on novel markers that may be of particular interest in the near future. Leukemia (2010) 24, 1700–1712; doi:10.1038/leu.2010.173; published online 2 September 2010 Keywords: myeloma; bone markers; NTX; CTX; ICTP Introduction Multiple myeloma (MM) is characterized by the presence of osteolytic bone lesions that result in skeletal-related events (SREs), such as pathologic fractures, need for radiation or surgery to bone, spinal cord compression and hypercalcemia. In the absence of effective bisphosphonate therapy, more than 50% of patients with Durie–Salmon stage III MM will experience at least one SRE over 2 years. 1 The development of lytic bone lesions is not only related to increased osseous breakdown but also to uncoupling of the bone remodeling process, in which osteoclast-mediated bone resorption is normally tightly coupled both temporally and spatially with osteoblast-mediated bone formation. 2–4 Lytic lesions rarely heal even in patients at complete remission. 4 Further, owing to the marked decrease in osteoblast activity, bone scans are often negative in myeloma patients with extensive lytic lesions and offer very little in the follow-up of bone disease in these patients. 5,6 Finally, sequential measurement of bone mineral density using Dual-energy X-ray Absorptiometry scans produce heterogeneous local bone mineral density changes; as such the routine use of sequential Dual-energy X-ray Absorptiometry scans is not recommended to assess bone disease in MM. 6,7 Although osteolytic lesions are usually assessed by plain radiographs, conventional radiography cannot provide informa- tion about ongoing bone remodeling. 6 Accordingly, biochem- ical markers of bone metabolism have been used in MM to assess the rate of bone turnover (defined as the prevalent rates of both bone formation and bone resorption) and to improve monitoring of bone destruction in MM. Moreover, bone turnover markers have been used to follow myeloma bone disease during specific therapies. 8–10 However, at present there is no consensus for the use of bone turnover markers in MM. This report of the International Myeloma Working Group summarizes the existing data for the role of markers of bone remodeling in assessing the extent of myeloma bone disease and in monitoring bone turnover during anti-myeloma treatment. It also proposes markers that can be used in clinical practice, and presents novel markers that may be of particular interest in the future. Markers of bone remodeling Throughout life, bone undergoes continuous remodeling with removal of old bone by osteoclasts and replacement with new bone by osteoblasts; a process that is balanced under normal conditions. 11 However, in MM, there is increased activation of osteoclasts and suppression of osteoblast function. 2–4 Over the past two decades, the isolation and characterization of cellular and extracellular components of the skeletal matrix have resulted in the development of biochemical markers that reflect Received 9 April 2010; revised 20 June 2010; accepted 5 July 2010; published online 2 September 2010 Correspondence: Dr E Terpos, Department of Clinical Therapeutics, University of Athens School of Medicine, Alexandra General Hospital, 80 Vas. Sofias Avenue, Athens 11528, Greece. E-mail: [email protected] 1 See appendix Leukemia (2010) 24, 1700–1712 & 2010 Macmillan Publishers Limited All rights reserved 0887-6924/10 www.nature.com/leu
Transcript of The use of biochemical markers of bone remodeling in ... · The use of biochemical markers of bone...

REVIEW
The use of biochemical markers of bone remodeling in multiple myeloma: a report of theInternational Myeloma Working Group
E Terpos1, MA Dimopoulos1, O Sezer2, D Roodman3, N Abildgaard4, R Vescio5, P Tosi6, R Garcia-Sanz7, F Davies8,A Chanan-Khan9, A Palumbo10, P Sonneveld11, MT Drake12, J-L Harousseau13, KC Anderson14 and BGM Durie5 on behalfof the International Myeloma Working Group1
1Department of Clinical Therapeutics, University of Athens School of Medicine, Athens, Greece; 2Department of Hematology,Oncology and Stem cell Transplantation, University Medical Center Hamburg, Hamburg, Germany; 3Department of Medicine,University of Pittsburgh Medical Center, Pittsburgh, PA, USA; 4Department of Hematology, Odense University, Odense,Denmark; 5Cedars-Sinai Outpatient Cancer Center at the Samuel Oschin Comprehensive Cancer Institute, Los Angeles, CA, USA;6Institute of Hematology and Oncology, University of Bologna, Bologna, Italy; 7Department of Hematology, HospitalUniversitario de Salamanca, Salamanca, Spain; 8Institute of Cancer Research and Royal Marsden Hospital, Section ofHaemato-oncology, Sutton, Surrey, UK; 9Department of Medicine, Roswell Park Cancer Institute, Buffalo, NY, USA; 10Divisionedi Ematologia, University of Torino, Torino, Italy; 11Department of Hematology, Erasmus Medical Center, Rotterdam,The Netherlands; 12Division of Endocrinology, Mayo Clinic, Rochester, MN, USA; 13Institut de Biologie, Laboratoired’Hematologie, Nantes, France and 14Division of Hematologic Malignancies, Department of Medical Oncology, Dana-FarberCancer Institute, Boston, MA, USA
Lytic bone disease is a frequent complication of multiplemyeloma (MM). Lytic lesions rarely heal and X-rays are oflimited value in monitoring bone destruction during anti-myeloma or anti-resorptive treatment. Biochemical markers ofbone resorption (amino- and carboxy-terminal cross-linkingtelopeptide of type I collagen (NTX and CTX, respectively) orCTX generated by matrix metalloproteinases (ICTP)) and boneformation provide information on bone dynamics and reflectdisease activity in bone. These markers have been investigatedas tools for evaluating the extent of bone disease, risk ofskeletal morbidity and response to anti-resorptive treatment inMM. Urinary NTX, serum CTX and serum ICTP are elevated inmyeloma patients with osteolytic lesions and correlate withadvanced disease stage. Furthermore, urinary NTX and serumICTP correlate with risk for skeletal complications, diseaseprogression and overall survival. Bone markers have also beenused for the early diagnosis of bone lesions. This InternationalMyeloma Working Group report summarizes the existing datafor the role of bone markers in assessing the extent of MM bonedisease and in monitoring bone turnover during anti-myelomatherapies and provides information on novel markers that maybe of particular interest in the near future.Leukemia (2010) 24, 1700–1712; doi:10.1038/leu.2010.173;published online 2 September 2010Keywords: myeloma; bone markers; NTX; CTX; ICTP
Introduction
Multiple myeloma (MM) is characterized by the presence ofosteolytic bone lesions that result in skeletal-related events(SREs), such as pathologic fractures, need for radiation or surgeryto bone, spinal cord compression and hypercalcemia. In theabsence of effective bisphosphonate therapy, more than 50% ofpatients with Durie–Salmon stage III MM will experience at leastone SRE over 2 years.1 The development of lytic bone lesions isnot only related to increased osseous breakdown but also to
uncoupling of the bone remodeling process, in whichosteoclast-mediated bone resorption is normally tightly coupledboth temporally and spatially with osteoblast-mediated boneformation.2–4 Lytic lesions rarely heal even in patients atcomplete remission.4 Further, owing to the marked decreasein osteoblast activity, bone scans are often negative in myelomapatients with extensive lytic lesions and offer very little in thefollow-up of bone disease in these patients.5,6 Finally, sequentialmeasurement of bone mineral density using Dual-energy X-rayAbsorptiometry scans produce heterogeneous local bonemineral density changes; as such the routine use of sequentialDual-energy X-ray Absorptiometry scans is not recommended toassess bone disease in MM.6,7
Although osteolytic lesions are usually assessed by plainradiographs, conventional radiography cannot provide informa-tion about ongoing bone remodeling.6 Accordingly, biochem-ical markers of bone metabolism have been used in MM toassess the rate of bone turnover (defined as the prevalent rates ofboth bone formation and bone resorption) and to improvemonitoring of bone destruction in MM. Moreover, bone turnovermarkers have been used to follow myeloma bone disease duringspecific therapies.8–10 However, at present there is no consensusfor the use of bone turnover markers in MM. This report of theInternational Myeloma Working Group summarizes the existingdata for the role of markers of bone remodeling in assessing theextent of myeloma bone disease and in monitoring boneturnover during anti-myeloma treatment. It also proposesmarkers that can be used in clinical practice, and presentsnovel markers that may be of particular interest in the future.
Markers of bone remodeling
Throughout life, bone undergoes continuous remodeling withremoval of old bone by osteoclasts and replacement with newbone by osteoblasts; a process that is balanced under normalconditions.11 However, in MM, there is increased activation ofosteoclasts and suppression of osteoblast function.2–4 Over thepast two decades, the isolation and characterization of cellularand extracellular components of the skeletal matrix haveresulted in the development of biochemical markers that reflect
Received 9 April 2010; revised 20 June 2010; accepted 5 July 2010;published online 2 September 2010
Correspondence: Dr E Terpos, Department of Clinical Therapeutics,University of Athens School of Medicine, Alexandra General Hospital,80 Vas. Sofias Avenue, Athens 11528, Greece.E-mail: [email protected] appendix
Leukemia (2010) 24, 1700–1712& 2010 Macmillan Publishers Limited All rights reserved 0887-6924/10
www.nature.com/leu

either bone formation or bone resorption.12–15 Markers of boneresorption and formation are depicted in Tables 1 and 2.Measurement of bone turnover markers is noninvasive, compara-tively inexpensive and when applied and interpreted correctly,can be of significant help in the assessment of bone disorders.However, factors that affect bone turnover marker levels,including circadian rhythm, diet, age, gender, renal functionand drugs, should be clearly defined and appropriately adjustedfor whenever possible. It is also important to recognize that thesebiochemical measurements reflect whole-body bone turnoverand give little information about the function of local changes inskeletal homeostasis. All these issues are discussed below.
Biochemistry of bone markers
Bone resorption markersHydroxyproline (Hyp) and hydroxylysine (Hyl). Hyp isformed in the cell from the post-translational hydroxylation ofproline and is the predominant amino acid within all collagens.Hyl is another structural amino acid of collagenous proteins.11
However, both Hyp and Hyl are also contained in certain serumproteins, such as the C1q component of complement. Thisdisadvantage, in combination with the effect of age andcircadian rhythm (both Hyp and Hyl have their peak excretionafter midnight) on their circulating levels, makes both Hyp andHyl less specific indices of bone resorption. As such, both havebeen largely replaced by newer markers.17–19
Pyridinoline (PYD) and deoxypyridinoline (DPD) cross-links of type I collagen. PYD and DPD are formed by theenzymatic action of lysyl oxidase on lysine and Hyl. PYD andDPD act as mature cross-links in type I collagen of all majorconnective tissues (Figure 1).20 The products of bone collagendegradation by osteoclasts include amino- and carboxy-terminalpeptide fragments (NTX and CTX, respectively) of various sizesthat remain attached to helical portions of nearby collagenmolecules by a pyridinium cross-link. These molecules arereleased into the circulation. Further degradation occurs in theliver and kidney, where the fragments are finally degraded totheir constituent amino acids and the pyridiniums, PYD and
Table 1 Markers of bone resorption
Marker Abbreviationa Tissue of origin Analytical method Analytical specimen
Hydroxyproline Hyp All tissues and all genetictypes of collagen
Colorimetric, assay,HPLC
Urine
Hydroxylysine Hyl All tissues and all genetictypes of collagen
Reversed-phase HPLC Urine
Galactosyl-hydroxylysine
Gal-Hyl Both Gal-Hyl and Glc-Gal-Hyl appears to be specificfor bone collagendegradation
Reversed-phase HPLC Urine
Glucosyl- galactosyl-hydroxylysine
Glc-Gal-Hyl Bone, cartilage, tendon,blood vessels
Reversed-phase HPLC Urine
Pyridinoline PYD Bone, dentin HPLC, ELISA UrineDeoxypyridinoline DPD All tissues containing type-I
collagenRIA Urine (free DPD can be
also measured in serumor plasma)
N-terminal cross-linkingtelopeptide of type-Icollagen
NTX All tissues containing type-Icollagen
ELISA, RIA Urine, serum
C-terminal cross-linkingtelopeptide of type-Icollagen
CTX All tissues containing type-Icollagen
ELISA, RIA Urine, serum (b-formonly)
C-terminal cross-linkingtelopeptide of type-Icollagen generated byMMPs
CTX-MMP orICTP
All tissues containing type-Icollagen
RIA Serum
Tartrate-resistant acidphosphatase isoform 5b
TRACP-5b Bone (osteoclasts) Colorimetric RIA, ELISA Serum, plasma
Bone sialoprotein BSP Bone, dentin, hypertrophiccartilage, cancer cells
RIA, ELISA Serum
Abbreviations: ELISA, enzyme-linked immunosorbent assay; HPLC, high-performance liquid chromatography; MMP, matrix metalloproteinase;RIA, radioimmunoassay.aAccording to the bone marker nomenclature by the Committee of Scientific Advisors of the International Osteoporosis Foundation.16
Table 2 Markers of bone formation
Marker Abbreviationa Tissue of origin Analytical method Analytical specimen
Osteocalcin (or bone gla-protein) OC Bone, platelets RIA, ELISA, IRMA SerumBone-specific alkaline phosphatase Bone ALP Bone ELISA, IRMA, colorimetric assay SerumProcollagen type-I N-propeptide PINP Bone, soft tissue, skin RIA, ELISA SerumProcollagen type I C-propeptide PICP Bone, soft tissue, skin RIA, ELISA Serum
Abbreviations: ELISA, enzyme-linked immunosorbent assay; RIA, radioimmunoassay; IRMA, immunoradiometric assay.aAccording to the bone marker nomenclature by the Committee of Scientific Advisors of the International Osteoporosis Foundation.16
Bone markers in multiple myelomaE Terpos et al
1701
Leukemia

DPD. The measurement of urinary DPD and PYD is notinfluenced by the degradation of newly synthesized collagenfibrils or by dietary collagen intake. Further, unlike Hyp, thePYD amino acids are fully excreted with no known pathway ofmetabolic degradation.21
Amino- and Carboxy-terminal cross-linking telopeptideof type I collagen. During bone collagen degradation byosteoclasts, NTX and CTX fragments are released into thecirculation.21 These fragments represent a spectrum of proteinsof different molecular weights. The proteolytic activities ofcathepsin K and matrix metalloproteinases result in theproduction of a variety of degradation peptides with differentantigenic properties.22 The majority of these peptides isrelatively small and is freely filtered by the glomerulus into theurine. NTX fragments are considered specific for bone tissuebreakdown, as other tissues that contain type I collagen, forexample, skin, do not undergo osteoclast-mediated metabolism.Thus, different type I collagen fragments are formed during thebreakdown of non-skeletal tissues.15
An enzyme-linked immunosorbent assay method has beendeveloped to recognize a discrete pool of NTX isolated fromurine, namely the a2-chain N-telopeptide fragment.23 Althoughthis fragment contains the pyridinium cross-links, the assay doesnot recognize the PYD and DPD per se. This confers bonespecificity, as the PYD cross-link in bone primarily involves thea2-chain, whereas in other tissues the a1-chain predominates.23
NTX contains the cross-linked a2 N-telopeptide sequenceQYDGKGVG, which is a product of osteoclastic proteolysis,in which lysine (K) is embodied in a trivalent cross-linkage.Collagen must be degraded to small cross-linked peptides thatcontain this exact sequence before the antibody will recognizethe NTX antigen. This ensures that the NTX peptide is a directproduct of osteoclastic proteolysis that does not require furthermetabolism in the liver or kidney for generation, and is rapidlycleared by the kidney.24 Urinary NTX results are expressedrelative to creatinine as nM of bone collagen equivalent per mM
of creatinine.Other assays have also been developed for the measurement
of epitopes associated with CTX (a-CTX, b-CTX and CTXgenerated by matrix metalloproteinases (ICTP)) in both serumand urine.25,26 These include a radioimmunoassay that detectsICTP by rabbit polyclonal antibodies directed against a largeantigen (10 000 Da) with a preserved trivalent cross-linkedstructure.27 This antigen is liberated when type I collagen isdegraded by matrix metalloproteinases.22,28 In contrast to theapproach used in the ICTP assay, the CTX-I (b-CTX) antigen isliberated when type I collagen is degraded by cathepsin K, butnot by matrix metalloproteinases.26 The recognized antigen
must be cross-linked, but can be imbedded into fragments ofthe C-terminal telopeptide of variable size (1000–10 000 Da).As half of the recognized antigens in normal sera are smallerthan 3000 Da, it is smaller than the ICTP antigen.
Owing to specificity for type I collagen and their uniquecharacteristics, the bone resorption markers NTX, ICTP and CTXhave almost completely replaced the use of older resorptionindices in the diagnostic assessment of bone disease.
Tartrate-resistant acid phosphatase isoform 5b (TRACP-5b). Two forms of TRACP circulate in humanserum, macrophage-derived TRACP-5a and osteoclast-derivedTRACP-5b.29–31 In human serum, TRACP-5b circulates in alarge complex that contains a2-microglobulin and calcium.32
Osteoclasts secrete TRACP-5b into the circulation as a cata-lytically active enzyme that is inactivated and degraded tofragments in the circulation. Thus, TRACP-5b molecules mea-sured in serum are freshly liberated from osteoclasts, providing aresorptive index that is useful as a surrogate marker for totalactivated osteoclast numbers.29
Bone formation markersBone-specific alkaline phosphatase (ALP). ALP is aubiquitously expressed, cell membrane-associated enzyme.33
Liver and bone (bALP) isoforms account for almost 95% of thetotal ALP activity in the serum. bALP is produced by osteoblastsand has been demonstrated in matrix vesicles deposited as‘buds’ derived from the cell membrane. These deposits have animportant role in bone formation.15 bALP is produced inextremely high amounts during the bone formation phase ofbone turnover, and is, therefore, an excellent indicator of totalbone formation activity.33
Osteocalcin (OC). OC is one of the most abundant non-collagenous proteins within bone. It is produced by osteoblasts,odontoblasts and hypertrophic chondrocytes. Most of thecirculating OC is a product of osteoblast activity. OC isincorporated into bone matrix, where it serves to bind calcium;as such, OC is considered a marker of bone formation. OC is asmall protein of 49 amino acids. In serum, OC is degraded sothat both the intact peptide and fragments coexist in thecirculation.34–38 Thus, assays that evaluate both intact OC andOC fragments are more accurate for the measurement of serumOC. Serum levels of OC are significantly influenced by gender,age and renal function.36
Type I procollagen propeptides. Collagen type I is a300-kDa protein that comprises 90% of the organic bone matrix.It is synthesized by osteoblasts in the form of procollagen.Extracellular processing of procollagen before collagen fiberassembly includes cleavage of the amino- and carboxy-terminalextension propeptides (termed procollagen type I N-propeptide(PINP) and C-propeptide (PICP)).39 Circulating PINP is clearedby the scavenger endothelial system in the liver, whereas PICP isremoved from the circulation by the mannose receptors on liverendothelial cells.40 Because PINP and PICP peptides aregenerated in a stoichiometric 1:1 ratio with newly formedcollagen molecules, their serum levels are considered an indexof collagen synthesis and thus of bone formation.41 Most studiessuggest that the PINP has a greater diagnostic validity than PICPin metastatic bone disease.42
Figure 1 Fibrils of collagen showing the N- and C-terminal endsbonding to helical areas of adjacent fibrils by pyridinoline anddeoxypyridinoline crosslinks.
Bone markers in multiple myelomaE Terpos et al
1702
Leukemia

Markers of bone remodeling in myeloma bone disease
Bone turnover markers and extent of myelomabone diseaseMarkers of both resorption and formation have been used inattempts to better evaluate the extent of bone disease in MM.Table 3 summarizes the results of the most important studies todate regarding the levels of bone markers in MM patients.43–60
As has been shown in multiple studies, urine levels of PYD,DPD and NTX and serum levels of CTX, ICTP and TRACP-5bwere elevated in MM patients compared with healthy controls,and correlated with the extent of osteolytic disease.46,48,51–56,58–60
Urinary NTX levels were increased even in myeloma patientswho had reached a clinical plateau phase of their disease,61
whereas PYD, DPD and NTX were also elevated in myelomapatients before autologous transplantation.62,63
A histomorphometric study in bone marrow biopsies ofmyeloma patients showed that urinary NTX correlated mostpositively with dynamic histomorphometric indices of boneresorption, followed by serum ICTP and urine DPD; urine PYDdid not correlate with the histomorphometric findings.64 More-over, comparison between these four markers (PYD, DPD, NTXand ICTP) revealed that serum ICTP and urinary NTXbetter reflected the extent of myeloma bone disease and couldbetter predict early progression of the bone disease afterconventional chemotherapy (CC).6,54 However, serum ICTPremained more sensitive than the urinary assays whenpatients with impaired renal function were excluded from thatanalysis.54
Jakob et al. demonstrated that serum ICTP was elevated inMM patients who did not have detectable osteolytic lesions byplain radiograph, but had abnormal bone magnetic resonanceimaging scans.65 Urinary NTX also correlated with the overallscore of skeletal involvement as measured by Tc-99m-MIBIscintigraphy and bone marrow infiltration by plasma cells.66
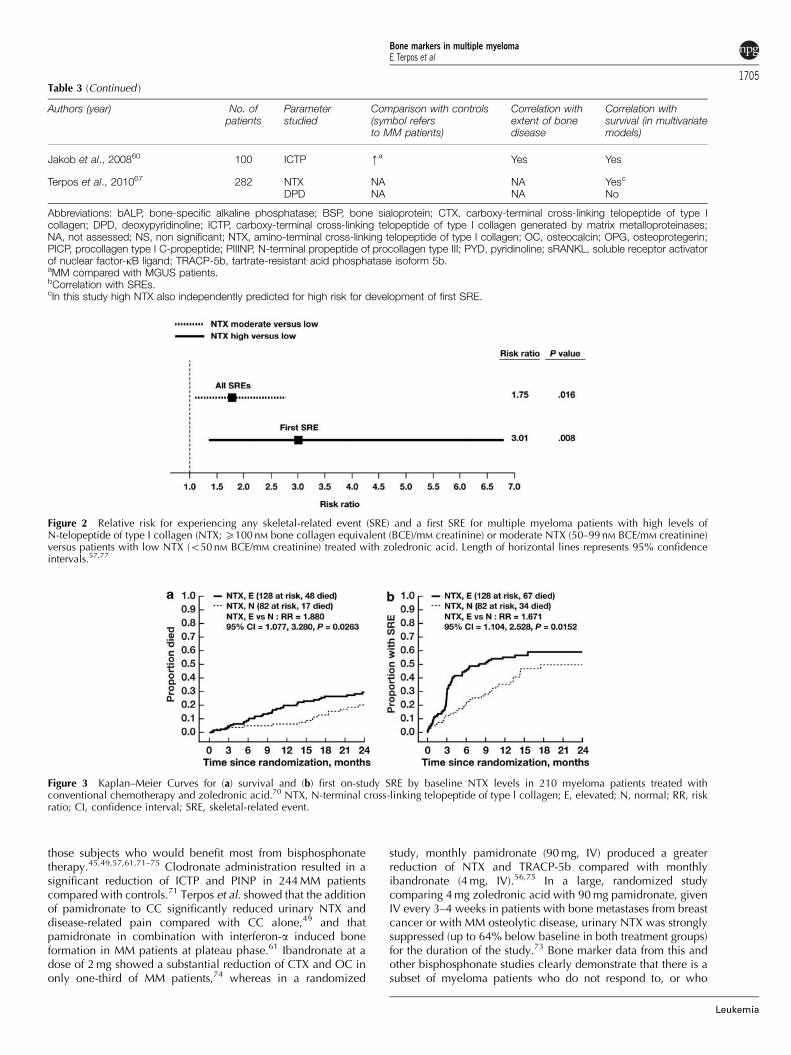
Coleman et al. showed in 210 MM patients that high orintermediate urinary NTX correlated with an increased risk forSRE development compared with low NTX values (risk ratio (RR)2.25, P¼ 0.032 and RR 1.75, P¼ 0.016, respectively).57 HighNTX values also correlated with a three-fold increased risk fordeveloping a first SRE (Figure 2), whereas there was also a trendtoward increased risk for progression of osteolytic lesions in thehigh NTX group (P¼ 0.08).57 A recent study by Terpos et al. in282 myeloma patients who participated in a randomized phaseIII study comparing zoledronic acid and pamidronate showedthat high urinary NTX was independently associated withelevated risk for the development of first SRE (68% increase inrisk for SRE development per 100-unit increase of NTX;P¼ 0.005).67 In summary, these results suggest that serum ICTPand urinary NTX strongly correlate with the extent of MM bonedisease, the risk for the development of SREs, and possibly withrisk for MM progression.
Markers of bone formation have been evaluated in severalstudies, but the results have been more variable than thosefound with bone resorption markers.43–46,48–51,53,55,56 In somestudies, bALP and OC were elevated in myeloma patientscompared with controls, whereas in others they were eitherreduced or within normal limits. In a study by Fonseca et al.,which included a large number of myeloma patients (n¼ 313),serum bALP correlated with bone pain, lesions and fractures,whereas OC levels were lower in myeloma patients than incontrols but did not correlate with the extent of bone disease.48
Furthermore, Coleman et al. showed that myeloma patientswith high bALP levels are at increased risk for developing a SRE(RR 3.29; Po0.001) and for disease progression (RR 2.42;
Po0.001).57 Terpos et al. showed that OC levels were reducedin myeloma patients and correlated with the extent of bonedisease, whereas bALP levels were not.55 Why differencesbetween the studies exist is not clear, but may reflect differentstudy populations and/or different phases of bone turnover ineach population. PICP values do not seem to reflect the extent ofmyeloma bone disease.43–46,48 As shown in Table 3, althoughmarkers of bone formation may be of some value in myeloma,they do not appear to reflect the extent of myeloma bonedestruction. Thus at present, their clinical utility is doubtful.
Correlations of bone turnover markers with myelomaactivity and survivalIn several studies, biochemical markers of bone resorptionstrongly correlated with stage of MM. Serum ICTP and urinaryNTX were higher in myeloma stage II/III than in stage Idisease.44,48,53 High DPD urinary levels also correlated withadvanced myeloma stage.51,52 In 121 newly diagnosed myelo-ma patients, NTX and TRACP-5b, but not OC or bALP, stronglycorrelated with disease stage.55 Two additional studies alsofailed to show a correlation between OC and bALP withmyeloma stage.48,51
Markers of bone remodeling have also correlated with well-characterized markers of disease activity, such as b2-micro-globulin and interleukin-648,51,55,64 and also with overallsurvival (OS).44,46,48,52,68,69 Fonseca et al. showed that themedian survival was 4.1 and 3.5 years for patients who receivedCC and had low or high ICTP levels, respectively (P¼ 0.02).48
Jakob et al. also reported that ICTP is a prognostic factor for OSin MM patients treated with CC (Po0.03), whereas urinary NTXwas only of borderline prognostic value (P¼ 0.05).52 The samegroup showed in 100 patients with newly diagnosed sympto-matic MM that disease stage, according to International StagingSystem, del(13q14), high dose therapy and ICTP independentlypredicted for OS, with ICTP having the most powerfulprognostic value (hazard ratio: nine-fold increase; Po0.001).Incorporation of ICTP in the International Staging Systemseparated four risk groups with a 5-year OS rate of 95, 65, 46and 22%, respectively.60
Abildgaard et al., using sequential measurements of both ICTPand NTX showed that high levels of ICTP and NTX correlatedwith an increased risk for early progression of bone lesionsduring CC, suggesting that their measurements are clinicallyuseful for identifying patients with increased risk of early diseaseprogression.7 In a recent study, Terpos et al. analyzed the effectof urinary NTX on survival in 210 patients participating in arandomized study comparing treatment with either zoledronicacid or pamidronate. Increased baseline levels of urinary NTX(X50 nM bone collagen equivalent per mM creatinine) corre-lated with an 88% increased risk of death and a 67% increasedrisk of first SRE (Figure 3).70 The update of this study in 282patients confirmed that high urinary NTX independentlypredicted for poor survival (RR¼ 1.60; P¼ 0.017).67 These datasuggest that the bone resorption markers serum ICTP and urinaryNTX have prognostic significance for disease progression andsurvival in MM under CC, and that their routine measurement infuture clinical trials may be of prognostic value in the current eraof novel anti-MM agents. In contrast, measurement of boneformation markers seem to be of limited prognostic value.71
Bone markers during anti-resorptive therapyBiochemical markers of bone turnover have been used in MMboth to monitor bisphosphonate treatment, and to determine
Bone markers in multiple myelomaE Terpos et al
1703
Leukemia
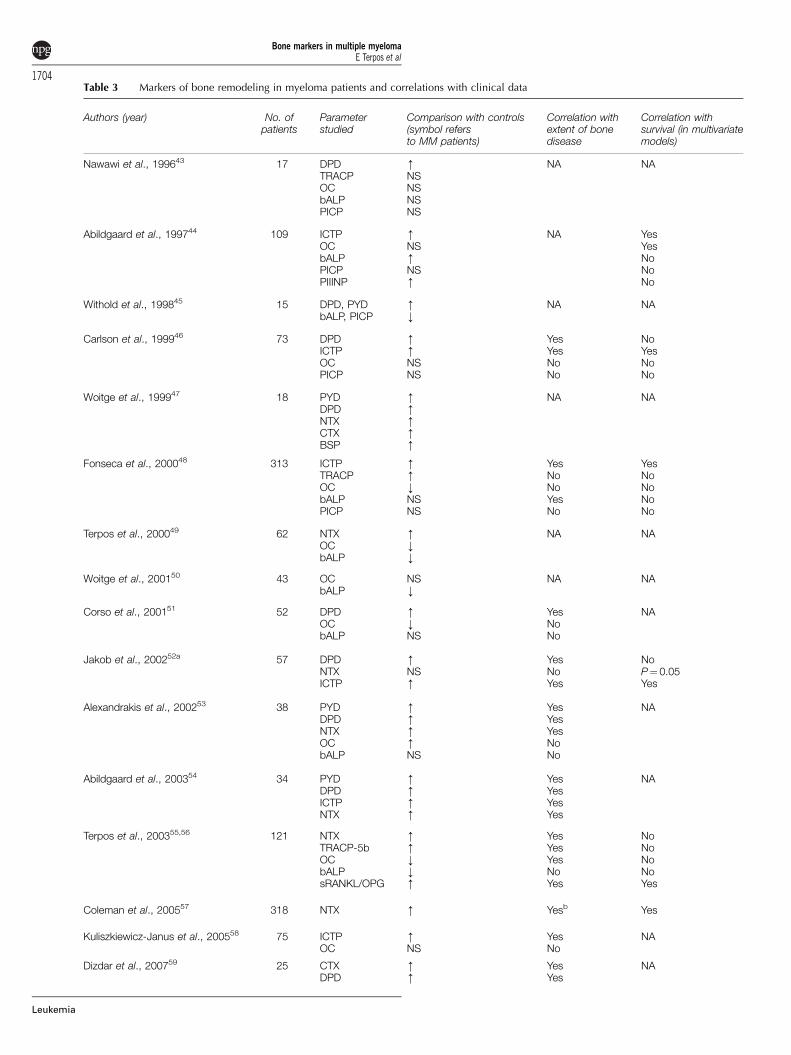
Table 3 Markers of bone remodeling in myeloma patients and correlations with clinical data
Authors (year) No. ofpatients
Parameterstudied
Comparison with controls(symbol refersto MM patients)
Correlation withextent of bonedisease
Correlation withsurvival (in multivariatemodels)
Nawawi et al., 199643 17 DPDTRACPOCbALPPICP
mNSNSNSNS
NA NA
Abildgaard et al., 199744 109 ICTPOCbALPPICPPIIINP
mNSmNSm
NA YesYesNoNoNo
Withold et al., 199845 15 DPD, PYDbALP, PICP
mk
NA NA
Carlson et al., 199946 73 DPDICTPOCPICP
mmNSNS
YesYesNoNo
NoYesNoNo
Woitge et al., 199947 18 PYDDPDNTXCTXBSP
mmmmm
NA NA
Fonseca et al., 200048 313 ICTPTRACPOCbALPPICP
mmkNSNS
YesNoNoYesNo
YesNoNoNoNo
Terpos et al., 200049 62 NTX m NA NAOC kbALP k
Woitge et al., 200150 43 OC NS NA NAbALP k
Corso et al., 200151 52 DPDOCbALP
mkNS
YesNoNo
NA
Jakob et al., 200252a 57 DPD m Yes NoNTX NS No P¼ 0.05ICTP m Yes Yes
Alexandrakis et al., 200253 38 PYD m Yes NADPD m YesNTX m YesOC m NobALP NS No
Abildgaard et al., 200354 34 PYD m Yes NADPD m YesICTP m YesNTX m Yes
Terpos et al., 200355,56 121 NTX m Yes NoTRACP-5b m Yes NoOC k Yes NobALP k No NosRANKL/OPG m Yes Yes
Coleman et al., 200557 318 NTX m Yesb Yes
Kuliszkiewicz-Janus et al., 200558 75 ICTPOC
mNS
YesNo
NA
Dizdar et al., 200759 25 CTX m Yes NADPD m Yes
Bone markers in multiple myelomaE Terpos et al
1704
Leukemia
those subjects who would benefit most from bisphosphonatetherapy.45,49,57,61,71–75 Clodronate administration resulted in asignificant reduction of ICTP and PINP in 244 MM patientscompared with controls.71 Terpos et al. showed that the additionof pamidronate to CC significantly reduced urinary NTX anddisease-related pain compared with CC alone,49 and thatpamidronate in combination with interferon-a induced boneformation in MM patients at plateau phase.61 Ibandronate at adose of 2 mg showed a substantial reduction of CTX and OC inonly one-third of MM patients,74 whereas in a randomized
study, monthly pamidronate (90 mg, IV) produced a greaterreduction of NTX and TRACP-5b compared with monthlyibandronate (4 mg, IV).56,75 In a large, randomized studycomparing 4 mg zoledronic acid with 90 mg pamidronate, givenIV every 3–4 weeks in patients with bone metastases from breastcancer or with MM osteolytic disease, urinary NTX was stronglysuppressed (up to 64% below baseline in both treatment groups)for the duration of the study.73 Bone marker data from this andother bisphosphonate studies clearly demonstrate that there is asubset of myeloma patients who do not respond to, or who
Table 3 (Continued )
Authors (year) No. ofpatients
Parameterstudied
Comparison with controls(symbol refersto MM patients)
Correlation withextent of bonedisease
Correlation withsurvival (in multivariatemodels)
Jakob et al., 200860 100 ICTP ma Yes Yes
Terpos et al., 201067 282 NTX NA NA Yesc
DPD NA NA No
Abbreviations: bALP, bone-specific alkaline phosphatase; BSP, bone sialoprotein; CTX, carboxy-terminal cross-linking telopeptide of type Icollagen; DPD, deoxypyridinoline; ICTP, carboxy-terminal cross-linking telopeptide of type I collagen generated by matrix metalloproteinases;NA, not assessed; NS, non significant; NTX, amino-terminal cross-linking telopeptide of type I collagen; OC, osteocalcin; OPG, osteoprotegerin;PICP, procollagen type I C-propeptide; PIIINP, N-terminal propeptide of procollagen type III; PYD, pyridinoline; sRANKL, soluble receptor activatorof nuclear factor-kB ligand; TRACP-5b, tartrate-resistant acid phosphatase isoform 5b.aMM compared with MGUS patients.bCorrelation with SREs.cIn this study high NTX also independently predicted for high risk for development of first SRE.
Figure 2 Relative risk for experiencing any skeletal-related event (SRE) and a first SRE for multiple myeloma patients with high levels ofN-telopeptide of type I collagen (NTX; X100 nM bone collagen equivalent (BCE)/mM creatinine) or moderate NTX (50–99 nM BCE/mM creatinine)versus patients with low NTX (o50 nM BCE/mM creatinine) treated with zoledronic acid. Length of horizontal lines represents 95% confidenceintervals.57,77
Figure 3 Kaplan–Meier Curves for (a) survival and (b) first on-study SRE by baseline NTX levels in 210 myeloma patients treated withconventional chemotherapy and zoledronic acid.70 NTX, N-terminal cross-linking telopeptide of type l collagen; E, elevated; N, normal; RR, riskratio; CI, confidence interval; SRE, skeletal-related event.
Bone markers in multiple myelomaE Terpos et al
1705
Leukemia

become refractory to bisphosphonate therapy.76 Patients withpersistently elevated bone marker levels are at higher risk forSREs and disease progression compared with patients whorespond to bisphosphonate therapy and have normalized boneresorption. Lipton et al. showed that among breast cancer ormyeloma patients (n¼ 170) who had high baseline NTX levels(X64 nM bone collagen equivalent per mM creatinine), thosewith persistently elevated NTX levels after 3 months ofzoledronic acid therapy (n¼ 26, 15%) had a significantlyincreased risk of developing a first SRE (RR¼ 1.71; P¼ 0.035)and shorter SRE-free survival (RR¼ 1.65; P¼ 0.039) comparedwith subjects who normalized NTX in response to bispho-sphonate treatment (n¼ 137, 81%).77 In this study, amongpatients with high NTX at baseline, 15% treated with zoledronicacid and 30% treated with pamidronate did not normalize NTXlevels after 3 months of bisphosphonate therapy. Althoughunknown, one might speculate that patients who did not havebiochemical improvement in their NTX levels may have anosteoclast-independent mechanism of bone resorption andmight, therefore, benefit from additional therapies.77
Denosumab is a fully human monoclonal antibody againstreceptor activator of nuclear factor-kB ligand (RANKL), the mostpotent osteoclast activator to-date (see below). In a recent study,1776 adult patients with solid tumors or MM (n¼ 10% of thetotal) who were naive to intravenous bisphosphonates wererandomized to receive either subcutaneous denosumab 120 mgor intravenous zoledronic acid every 4 weeks. Denosumabproduced similar results regarding the delay in time to first on-study SRE or subsequent SREs compared with zoledronic acid,whereas it also rapidly and potently reduced (by more than 80%within the first month) urinary NTX levels.78
Novel molecules related to bone remodeling andmyeloma bone diseaseRANKL and Osteoprotegerin (OPG). RANKL and OPGhave crucial roles in the development of myeloma bone disease.Although RANKL increases osteoclastogenesis and osteoclastactivity, OPG serves as a soluble inhibitor of RANKL activity.Within the myeloma bone marrow microenvironment, theRANKL/OPG ratio is shifted in favor of RANKL, leading toincreased osteoclastogenesis and increased bone resorption.2–4
Multiple studies have now documented that in MM, serum OPGlevels are reduced, whereas the soluble RANKL/OPG ratio isincreased.63,79–82 This altered ratio correlates with extent ofbone disease, markers of bone resorption, such as NTX andTRACP-5b and myeloma stage.63,81 The administration ofzoledronic acid in patients with asymptomatic myeloma wasfound to increase serum levels of OPG and thus reduce theRANKL/OPG ratio, likely accounting for the effect of zoledronicacid on osteoblast and/or bone marrow stromal cells togetherwith its direct effect on osteoclasts.83 The RANKL/OPG ratio hasbeen found to correlate with OS in MM. This result has not beenconfirmed in all reported studies to date,63,69,83,84 may be due todifferences in patient populations and/or therapies administered.Further studies are needed before measurement of serumRANKL and OPG levels in the everyday clinical setting shouldbe considered.
Other potential molecules reflecting bone destruction inMM. Bone sialoprotein is a phosphorylated 70–80 kDAglycoprotein that accounts for 5–10% of the non-collagenousbone matrix. Bone sialoprotein is involved in the adhesion ofbone resorbing cells to the extracellular bone matrix.82 In onestudy of MM, bone sialoprotein levels were associated with
skeletal involvement and tumor cell burden.14 However, furtherevaluation is needed to support its value in MM bone disease.
Dickkopf-1 (Dkk-1) protein is an inhibitor of the Wingless-type and Int (Wnt) pathway, a pathway crucial for stimulation ofosteoblast activity. Tian et al. were the first to describe thatincreased expression of Dkk-1 in plasma cells correlates withthe presence of lytic lesions both by plain radiography andmagnetic resonance imaging.85 Bone marrow plasma Dkk-1levels were increased in MM patients, and associated with Dkk-1concentrations in peripheral blood, levels of Dkk-1 transcripts inmyeloma cells and the presence of osteolytic lesions.86–88 Geneexpression studies in 171 newly diagnosed MM patients showedthat overexpression of Dkk-1 correlated with the degree ofosteolytic bone disease.89 Similarly, serum Dkk-1 levels wereelevated in myeloma patients with lytic bone disease comparedwith those without lytic lesions by conventional radiography,and also correlated with the number of bone lesions.87 Incontrast, patients with monoclonal gammopathy of undeter-mined significance had lower serum levels of Dkk-1 comparedwith MM subjects, with levels similar to those found in controlsubjects. High values of serum Dkk-1 also correlated withadvanced ISS stage.87 It is interesting that, a recent report fromYaccoby and colleagues demonstrated that Dkk-1-negativemyeloma cells in trephine biopsies had more aggressive featuresand plasmablastic morphology, whereas Dkk-1 was rarelyexpressed by plasma cells of plasma cell leukemia.90 Thecurrent role of Dkk-1 in the clinical assessment of myelomabone disease, however, remains to be determined.
The effect of novel anti-myeloma agents on markers of boneremodeling
During the last decade, immunomodulatory drugs, includingthalidomide and lenalidomide and proteasome inhibitors, suchas bortezomib, have been increasingly used for the treatment ofMM. Thalidomide, lenalidomide and bortezomib are effectiveagents for the treatment of both newly-diagnosed and relapsed/refractory MM. The role of these drugs in bone metabolism hasbeen evaluated in several studies.
Immunomodulatory drugsTwo clinical phase II trials have studied the effect of thalidomideon bone metabolism of MM patients (Table 4). In the first study,Terpos et al showed that in relapsed/refractory MM patients, thecombination of thalidomide (200 mg per day) with dexametha-sone (TD) produced a significant reduction of serum levels ofCTX, TRACP-5b and sRANKL/OPG after 6 months of therapy.There was a strong correlation between changes in the sRANKL/OPG ratio and changes in TRACP-5b and CTX, suggesting thatthe reduction of bone resorption by TD is at least in part due tothe reduction of RANKL. TD showed no effect on boneformation in that study.76 In the second study, Tosi et al showedin newly diagnosed MM patients that the combination of TD andzoledronic acid for 4 months produced a significant reduction ofurinary NTX and serum CTX, but only in patients whoresponded to therapy. This reduction was accompanied by areduction in bone pain in 60% of the patients, and also by areduction of bALP and OC levels in both responding andrefractory patients. This negative effect of TD on bone formationmay be due to the concomitant use of high-dose dexamethasonein these patients.91
Limited data exists for the effects of lenalidomide on boneremodeling in myeloma patients. In a small study, lenalidomide
Bone markers in multiple myelomaE Terpos et al
1706
Leukemia

reduced serum RANKL and increased serum OPG levels,leading to a reduction of the RANKL/OPG ratio.92 From theavailable data, it seems that immunomodulatory drugs reduceosteoclast function but have little or no effect on osteoblastactivity.
BortezomibAn increasing number of studies have now reported thebeneficial effects of bortezomib on bone formation in theclinical setting, confirming preclinical observations.93,94 Asdescribed by Heider et al., the combination of bortezomib±dexamethasone produced significant increases in serum bALPand OC in both responders and non-responders.95 Giuliani et al.found significant increases in the number of osteoblasts per mm2
of bone tissue in trephine biopsies of patients responding tobortezomib, but not in subjects who did not respond.96 Terposet al. showed that, in 34 patients bortezomib monotherapyreduced serum Dkk-1 and RANKL levels. This was asso-ciated with a concomitant reduction in bone resorption (serumTRACP-5b and CTX) and increase in markers of bone formation(serum bALP and OC), changes that occurred irrespective ofresponse to therapy.97
However, when bortezomib was combined with other anti-myeloma agents (VMDT regimen, combination of bortezomib,melphalan, dexamethasone and thalidomide), the reduction ofDkk-1, sRANKL and CTX was not accompanied by increases inbALP and OC.83 This observation suggests that bortezomib maylose its beneficial effect on osteoblasts when it is combined withother anti-myeloma agents. Indeed, Heider et al. found anattenuated increase in bALP in patients who received VD
compared with those who received bortezomib monotherapy.95
Thus, although different effective anti-myeloma regimens incombination with bisphosphonates can reduce bone resorptionthrough reduction of tumor burden and inhibition of osteoclastfunction,63 to-date only bortezomib has clearly shown ananabolic bone effect in MM.
Conclusions and future directions
Biochemical markers of bone resorption faithfully reflectchanges in bone metabolism associated with the malignantprocess in myeloma. Serum ICTP and urinary NTX seem to bemore accurate than other bone resorption markers in reflectingboth the severity of bone destruction and the efficacy ofresponse to bisphosphonate treatment. To date, data on CTXremain sparse, but studies are ongoing. There is also a strongcorrelation between serum ICTP and urinary NTX withincreased risk for progressive bone disease, development ofSREs and OS (Table 5). However, it should be kept in mind thatICTP and CTX undergo renal elimination, a fact that will affectthe potential utility of these measurements in many patientsbecause of the high prevalence of renal dysfunction in MM.
Symptomatic patients who continue to have increased levelsof NTX after 3 months of anti-myeloma and anti-resorptivetherapy remain at high risk for both SREs and shortened OS;accordingly such patients may require more aggressive therapy.
The value of bone markers in the setting of asymptomaticmyeloma has also to be evaluated as it may reveal patients athigh risk for progression (Table 5).
Table 4 Clinical studies for the effect of novel anti-myeloma agents on bone metabolism
Agent MM studypopulation
No. ofpatients
Results Subpopulationanalysis
Thalidomide (+Dexa)Tosi et al.91a Newly diagnosed 40 k Bone resorption markers (CTX & NTX)
k bone formation markers (bALP & OC)In respondersIn all patients
Terpos et al. 76a Refractory/relapsed 35 k Bone resorption markers (CTX & TRACP-5b)k osteoclast stimulators (sRANKL, sRANKL/OPG ratio)2 bone formation markers (bALP & OC)
In all patientsIn all patientsIn all patients
LenalidomideBreitkreutz et al.92 Refractory/relapsed 11 k osteoclast numbers
k osteoclast differentiationk bone resorption
ND
Bortezomib (±Dexa)Heider et al.95a Refractory/relapsed 58 m bone formation markers (bALP & OC) In all patientsTerpos et al.97a Refractory/relapsed 34 k bone resorption markers (CTX & TRACP-5b)
k osteoclast stimulators (sRANKL, sRANKL/OPG ratio)m bone formation markers (bALP & OC)k osteoblast inhibitors (Dkk-1)
In all patientsIn all patientsIn respondersb
In all patientsGiuliani et al.96a Refractory/relapsed 21 k bone resorption markers (CTX)
m osteoblast numbersIn all patientsc
In respondersTerpos et al.83a
(VMDT regimen)Refractory/relapsed 62 k bone resorption markers (CTX & TRACP-5b)
k osteoclast stimulators (sRANKL, sRANKL/OPG, MIP-1a)2 bone formation markers (bALP & OC)k osteoblast inhibitors (Dkk-1)
In all patientsIn all patientsIn all patientsIn all patients
Abbreviations: bALP, bone alkaline phosphatase; CTX, carboxy-terminal cross-linking telopeptide of type I collagen; Dkk-1, dickkopf-1;MIP-1a, macrophage inflammatory protein 1a; NTX, amino-terminal cross-linking telopeptide of type I collagen; OC, osteocalcin;OPG, osteoprotegerin; RANKL, receptor activator of nuclear factor-kB ligand; TRACP-5b, tartrate-resistant acid phosphatase isoform type 5b.aConcomitant bisphosphonates administration in majority of patients.bbALP was increased only in responders whereas OC was elevated in all patients.cThis reduction did not reach statistical significance.
Bone markers in multiple myelomaE Terpos et al
1707
Leukemia

In the current era of concern about bisphosphonate-associated adverse side-effects (that is, renal impairment,osteonecrosis of the jaw, subtrochanteric femoral fractures),bone turnover markers may be of particular use: that is, lowlevels of serum ICTP/CTX or urinary NTX may provide impetusfor deciding to lengthen bisphosphonate dosing regimens (thatis, changing from monthly to 3-month intervals). Clinical studieshave started in patients with breast cancer and bone metastases(BISMARK trial) and are eagerly anticipated in myeloma.Further, with the development of novel anti-resorptive agents(denosumab, other anti-RANKL agents) and drugs that enhanceosteoblast function (anti-Dkk-1 antibodies), the measurement ofbone biochemical indices will likely be of particular value.However, additional trials, such as those described above areurgently needed (and indeed should be highly encouraged)before final conclusions are made about the introduction ofbiochemical markers of bone remodeling into the routineclinical care of MM patients.
Conflict of interest
The authors declare no conflict of interest.
Authors’ Contributions
ET collected data and wrote paper; MAD collected data andwrote paper; OS contributed comments and edited paper; DRcontributed comments and edited paper; RV contributedcomments and edited paper; NA contributed comments andedited paper; PT contributed comments and edited paper;RG-S contributed comments and edited paper; FD contributedcomments and edited paper; AC-K contributed comments andedited paper; AP contributed comments and edited paper;PS contributed comments and edited paper; MTD contributedcomments and edited paper; J-LH contributed comments and
edited paper; KCA contributed comments and edited paper;BGMD contributed comments and edited paper
References
1 Coleman RE. Bisphosphonates: clinical experience. Oncologist2004; 9 (Suppl 4): 14–27.
2 Terpos E, Dimopoulos MA. Myeloma bone disease: pathophysio-logy and management. Ann Oncol 2005; 16: 1223–1231.
3 Roodman GD. Pathogenesis of myeloma bone disease. Leukemia2009; 23: 435–441.
4 Sezer O. Myeloma bone disease: Recent advances in biology,diagnosis and treatment. Oncologist 2009; 14: 276–283.
5 Mileshkin L, Blum R, Seymour JF, Patrikeos A, Hicks RJ, PrinceHM. A comparison of fluorine-18 fluoro-deoxyglucose PET andtechnetium-99 m sestamibi in assessing patients with multiplemyeloma. Eur J Haematol 2004; 72: 32–37.
6 Dimopoulos M, Terpos E, Comenzo RL, Tosi P, Beksac M, Sezer Oet al. International myeloma working group consensus statementand guidelines regarding the current role of imaging techniques inthe diagnosis and monitoring of multiple Myeloma. Leukemia2009; 23: 1545–1556.
7 Abildgaard N, Brixen K, Eriksen EF, Kristensen JE, Nielsen JL,Heickendorff L. Sequential analysis of biochemical markers ofbone resorption and bone densitometry in multiple myeloma.Haematologica 2004; 89: 567–577.
8 Terpos E, Sezer O, Croucher PI, Garcıa-Sanz R, Boccadoro M,San Miguel J et al. The use of bisphosphonates in multiplemyeloma: recommendations of an expert panel on behalf of theEuropean Myeloma Network. Ann Oncol 2009; 20: 1303–1317.
9 Terpos E, Dimopoulos MA, Sezer O. The effect of novel anti-myeloma agents on bone metabolism of patients with multiplemyeloma. Leukemia 2007; 21: 1875–1884.
10 von Metzler I, Krebbel H, Hecht M, Manz RA, Fleissner C,Mieth M et al. Bortezomib inhibits human osteoclastogenesis.Leukemia 2007; 21: 2025–2034.
11 Calvo MS, Eyre DR, Gundberg CM. Molecular basis and clinicalapplication of biological markers of bone turnover. Endocrine Rev1996; 17: 333–368.
12 Hannon RA, Eastell R. Biochemical markers of bone turnover andfracture prediction. J Br Menopause Soc 2003; 9: 10–15.
Table 5 Summary of the role of markers of bone metabolism in multiple myeloma
Parameter Reflection of theextend of myeloma
bone disease
Prediction forSRE
Prediction for OS Future possible use
Bone resorption markersUrinary NTX +++ +++ +++ 1. Symptomatic patients to drive initial therapy (NTX)Serum ICTP +++ ++ ++ 2. Asymptomatic patients to drive decision for anti-
resorptive therapy (NTX, ICTP, CTX)Serum CTX ++ � � 3. Symptomatic patients under bisphosphonates to decide
the duration and intervals of therapy (NTX, ICTP, CTX)Serum TRACP-5b + � �
Bone formation markersSerum bALP +/� � � 1. Use for the evaluation of bone anabolic agents, such as
bortezomib, anti-Dkk1, anti-SOST antibodies (bALP only)Serum OC +/� � � 2. No future use is seen for other bone formation markersSerum PINP or PICP � � �
Osteoclast/osteoblastregulators
Serum sRANKL ortRANKL
+/� � +/� 1. Use for the follow-up of novel therapies (denosumab-anti-RANKL, anti-Dkk1 etc)
Serum OPG +/� � �Serum Dkk-1 + � �
Abbreviations: (�), no evidence; (+/�), conflicting evidence; (+), low evidence; (++), intermediate evidence; (+++), strong evidence; bALP, bonealkaline phosphatase; CTX, carboxy-terminal cross-linking telopeptide of type I collagen; Dkk-1, dickkopf-1; ICTP, carboxy-terminal cross-linkingtelopeptide of type I collagen generated by matrix metalloproteinases; NTX, amino-terminal cross-linking telopeptide of type I collagen; OC,osteocalcin; OPG, osteoprotegerin; PICP, procollagen type I carboxy-propeptide; PINP, procollagen type I amino-propeptide; SOST, sclerostin;sRANKL, soluble receptor activator of nuclear factor-kB ligand; TRACP-5b, tartrate resistant acid phosphatase isoform 5b; tRANKL, total RANKL.
Bone markers in multiple myelomaE Terpos et al
1708
Leukemia

13 Hannon RA, Clowes JA, Eagleton AC, Al Hadari A, Eastell R,Blumsohn A. Clinical performance of immunoreactive tartrate-resistant acid phosphatase isoform 5b as a marker of boneresorption. Bone 2004; 34: 187–194.
14 Woitge HW, Pecherstorfer M, Horn E, Keck AV, Diel IJ, Bayer Pet al. Serum bone sialoprotein as a marker of tumour burden andneoplastic bone involvement and as a prognostic factor in multiplemyeloma. Br J Cancer 2001; 84: 344–351.
15 Seibel MJ. Biochemical markers of bone turnover: part I:biochemistry and variability. Clin Biochem Rev 2005; 26:97–122.
16 Delmas PD. Bone marker nomenclature. Bone 2001; 28:575–576.
17 Prockop DJ, Keiser HR, Sjoerdsma A. Gastrointestinal absorptionand renal excretion of hydroxyproline peptides. Lancet 1962; 2:527–528.
18 Al-Dehaimi AW, Blumsohn A, Eastell R. Serum galactosylhydroxylysine as a biochemical marker of bone resorption.Clin Chem 1999; 45: 676–681.
19 Leigh SD, Ju HS, Lundgard R, Daniloff GY, Liu V. Development ofan immunoassay for urinary galactosylhydroxylysine. J ImmunolMethods 1998; 220: 169–178.
20 Eyre DR, Paz MA, Gallop PM. Cross-linking in collagen andelastin. Annu Rev Biochem 1984; 53: 717–748.
21 Knott L, Bailey AJ. Collagen cross-links in mineralizing tissues:a review of their chemistry, function, and clinical relevance.Bone 1998; 22: 181–187.
22 Garnero P, Ferreras M, Karsdal MA, Nicamhlaoibh R, Risteli J,Borel O et al. The type I collagen fragments ICTP and CTX revealdistinct enzymatic pathways of bone collagen degradation. J BoneMiner Res 2003; 18: 859–867.
23 Hanson DA, Weis MA, Bollen AM, Maslan SL, Singer FR, Eyre DR.A specific immunoassay for monitoring human bone resorption:quantitation of type I collagen cross-linked N-telopeptides in urine.J Bone Miner Res 1992; 7: 1251–1258.
24 Apone S, Lee MY, Eyre DR. Osteoclasts generate cross-linkedcollagen N-telopeptides (NTx) but not free pyridinolines whencultured on human bone. Bone 1997; 21: 129–136.
25 Bonde M, Garnero P, Fledelius C, Qvist P, Delmas PD,Christiansen C. Measurement of bone degradation products inserum using antibodies reactive with an isomerized form of an 8amino acid sequence of the C-telopeptide of type I collagen.J Bone Miner Res 1997; 12: 1028–1034.
26 Rosenquist C, Fledelius C, Christgau S, Pedersen BJ, Bonde M,Qvist P et al. Serum crosslaps one step ELISA. First application ofmonoclonal antibodies for measurement in serum of bone-relateddegradation products from C-terminal telopeptides of type Icollagen. Clin Chem 1998; 44: 2281–2289.
27 Risteli J, Elomaa I, Niemi S, Novamo A, Risteli L. Radio-immunoassay for the pyridinoline cross-linked carboxy-terminaltelopeptide of type I collagen: a new serum marker of bonecollagen degradation. Clin Chem 1993; 39: 635–640.
28 Sassi ML, Eriksen H, Risteli L, Niemi S, Mansell J, Gowen M et al.Immunochemical characterization of assay for carboxyterminaltelopeptide of human type I collagen: loss of antigenicity bytreatment with cathepsin K. Bone 2000; 26: 367–373.
29 Janckila AJ, Takahashi K, Sun SZ, Yam LT. Tartrate-resistant acidphosphatase isoform 5b as serum marker for osteoclastic activity.Clin Chem 2001; 47: 74–80.
30 Janckila AJ, Neustadt DH, Nakasato YR, Halleen JM, Hentunen T,Yam LT. Serum tartrate-resistant acid phosphatase isoforms inrheumatoid arthritis. Clin Chim Acta 2002; 320: 49–58.
31 Lam WK, Eastlund DT, Li CY, Yam LT. Biochemical properties oftartrate-resistant acid phosphatase in serum of adults and children.Clin Chem 1978; 24: 1105–1108.
32 Ylipahkala H, Halleen JM, Kaija H, Vihko P, Vaananen HK.Tartrate-resistant acid phosphatase 5B circulates in human serumin complex with alpha2-macroglobulin and calcium. BiochemBiophys Res Commun 2003; 308: 320–324.
33 Moss DW. Perspectives in alkaline phosphatase research. ClinChem 1992; 38: 2486–2492.
34 Gallop PM, Lian JB, Hauschka PV. Carboxylated calcium-bindingproteins and vitamin K. N Engl J Med 1980; 302: 1460–1466.
35 Nelsestuen GL, Shah AM, Harvey SB. Vitamin K-dependentproteins. Vitam Horm 2000; 58: 355–389.
36 Young MF, Kerr JM, Ibaraki K, Heegaard AM, Robey PG. Structure,expression, and regulation of the major noncollagenous matrixproteins of bone. Clin Orthop Relat Res 1992; 281: 275–294.
37 Sierra J, Villagra A, Paredes R, Cruzat F, Gutierrez S, Javed A et al.Regulation of the bone-specific osteocalcin gene by p300 requiresRunx2/Cbfa1 and the vitamin D3 receptor but not p300 intrinsichistone acetyltransferase activity. Mol Cell Biol 2003; 23:3339–3351.
38 Koeneman KS, Kao C, Ko SC, Yang L, Wada Y, Kallmes DF et al.Osteocalcin-directed gene therapy for prostate-cancer bonemetastasis. World J Urol 2000; 18: 102–110.
39 Christenson RH. Biochemical markers of bone metabolism: anoverview. Clin Biochem 1997; 30: 573–593.
40 Smedsrod B, Melkko J, Risteli L, Risteli J. Circulating C-terminalpropeptide of type I procollagen is cleared mainly via the mannosereceptor in liver endothelial cells. Biochem J 1990; 271: 345–350.
41 Risteli J, Risteli L. Assays of type I procollagen domains andcollagen fragments: problems to be solved and future trends.Scand J Clin Lab Invest Suppl 1997; 227: 105–113.
42 Fohr B, Dunstan CR, Seibel MJ. Clinical review 165: Markers ofbone remodeling in metastatic bone disease. J Clin EndocrinolMetab 2003; 88: 5059–5075.
43 Nawawi H, Samson D, Apperley J, Girgis S. Biochemical bonemarkers in patients with multiple myeloma. Clin Chim Acta 1996;253: 61–77.
44 Abildgaard N, Bentzen SM, Nielsen JL, Heickendorff L. Serummarkers of bone metabolism in multiple myeloma: prognosticvalue of the carboxy-terminal telopeptide of type I collagen (ICTP).Br J Haematol 1997; 96: 103–110.
45 Withold W, Arning M, Schwarz M, Wolf HH, Schneider W.Monitoring of multiple myeloma patients by simultaneouslymeasuring marker substances of bone resorption and formation.Clin Chim Acta 1998; 269: 21–30.
46 Carlson K, Larsson A, Simonsson B, Turesson I, Westin J, Ljunghall S.Evaluation of bone disease in multiple myeloma: a comparisonbetween the resorption markers urinary deoxypyridinoline/creati-nine (DPD) and serum ICTP, and an evaluation of the DPD/osteocalcin and ICTP/osteocalcin ratios. Eur J Haematol 1999; 62:300–306.
47 Woitge HW, Pecherstorfer M, Li Y, Keck AV, Horn E, Ziegler Ret al. Novel serum markers of bone resorption: clinical assessmentand comparison with established urinary indices. J Bone Miner Res1999; 14: 792–801.
48 Fonseca R, Trendle MC, Leong T, Kyle RA, Oken MM, Kay NEet al. Prognostic value of serum markers of bone metabolism inuntreated multiple myeloma patients. Br J Haematol 2000; 109:24–29.
49 Terpos E, Palermos J, Tsionos K, Anargyrou K, Viniou N,Papassavas P et al. Effect of pamidronate administration onmarkers of bone turnover and disease activity in multiplemyeloma. Eur J Haematol 2000; 65: 331–336.
50 Woitge HW, Horn E, Keck AV, Auler B, Seibel MJ, Pecherstorfer M.Biochemical markers of bone formation in patients with plasmacell dyscrasias and benign osteoporosis. Clin Chem 2001; 47:686–693.
51 Corso A, Arcaini L, Mangiacavalli S, Astori C, Orlandi E, Lorenzi Aet al. Biochemical markers of bone disease in asymptomatic earlystage multiple myeloma. A study on their role in identifying highrisk patients. Haematologica 2001; 86: 394–398.
52 Jakob C, Zavrski I, Heider U, Brux B, Eucker J, Langelotz C et al.Bone resorption parameters [carboxy-terminal telopeptide of type-Icollagen (ICTP), amino-terminal collagen type-I telopeptide (NTx),and deoxypyridinoline (Dpd)] in MGUS and multiple myeloma.Eur J Haematol 2002; 69: 37–42.
53 Alexandrakis MG, Passam FH, Malliaraki N, Katachanakis C,Kyriakou DS, Margioris AN. Evaluation of bone disease in multiplemyeloma: a correlation between biochemical markers of bonemetabolism and other clinical parameters in untreated multiplemyeloma patients. Clin Chim Acta 2002; 325: 51–57.
54 Abildgaard N, Brixen K, Kristensen JE, Eriksen EF, Nielsen JL,Heickendorff L. Comparison of five biochemical markers of boneresorption in multiple myeloma: elevated pre-treatment levels ofS-ICTP and U-Ntx are predictive for early progression of the bonedisease during standard chemotherapy. Br J Haematol 2003; 120:235–242.
Bone markers in multiple myelomaE Terpos et al
1709
Leukemia

55 Terpos E, Szydlo R, Apperley JF, Hatjiharissi E, Politou M, Meletis Jet al. Soluble receptor activator of nuclear factor kappaB ligand-osteoprotegerin ratio predicts survival in multiple myeloma:proposal for a novel prognostic index. Blood 2003; 102:1064–1069.
56 Terpos E, de la Fuente J, Szydlo R, Hatjiharissi E, Viniou N, Meletis Jet al. Tartrate-resistant acid phosphatase isoform 5b: a novel serummarker for monitoring bone disease in multiple myeloma. Int JCancer 2003; 106: 455–457.
57 Coleman RE, Major P, Lipton A, Brown JE, Lee KA, Smith Met al. Predictive value of bone resorption and formationmarkers in cancer patients with bone metastases receivingthe bisphosphonate zoledronic acid. J Clin Oncol 2005; 23:4925–4935.
58 Kuliszkiewicz-Janus M, Ma"ecki R, Zo"taszek A, Zastawny M. Thesignificance of carboxy-terminal telopeptide of type I collagen(ICTP) and osteocalcin (OC) in assessment of bone diseasein patients with multiple myeloma. Leuk Lymphoma 2005; 46:1749–1753.
59 Dizdar O, Barista I, Kalyoncu U, Karadag O, Hascelik G,Cila A et al. Biochemical markers of bone turnover indiagnosis of myeloma bone disease. Am J Hematol 2007; 82:185–191.
60 Jakob C, Sterz J, Liebisch P, Mieth M, Rademacher J, Goerke Aet al. Incorporation of the bone marker carboxy-terminal telopep-tide of type-1 collagen improves prognostic information of theInternational Staging System in newly diagnosed symptomaticmultiple myeloma. Leukemia 2008; 22: 1767–1772.
61 Terpos E, Palermos J, Viniou N, Vaiopoulos G, Meletis J, Yataganas X.Pamidronate increases markers of bone formation in patients withmultiple myeloma in plateau phase under interferon-alpha treatment.Calcif Tissue Int 2001; 68: 285–290.
62 Clark RE, Flory AJ, Ion EM, Woodcock BE, Durham BH, FraserWD. Biochemical markers of bone turnover following high-dosechemotherapy and autografting in multiple myeloma. Blood 2000;96: 2697–2702.
63 Terpos E, Politou M, Szydlo R, Nadal E, Avery S, Olavarria E et al.Autologous stem cell transplantation normalizes abnormal boneremodeling and sRANKL/osteoprotegerin ratio in patients withmultiple myeloma. Leukemia 2004; 18: 1420–1426.
64 Abildgaard N, Glerup H, Rungby J, Bendix-Hansen K, Kassem M,Brixen K et al. Biochemical markers of bone metabolism reflectosteoclastic and osteoblastic activity in multiple myeloma. Eur JHaematol 2000; 64: 121–129.
65 Jakob C, Zavrski I, Heider U, Bollow M, Schulz CO, Fleissner Cet al. Serum levels of carboxy-terminal telopeptide of type-Icollagen are elevated in patients with multiple myeloma showingskeletal manifestations in magnetic resonance imaging but lackinglytic bone lesions in conventional radiography. Clin Cancer Res2003; 9: 3047–3051.
66 Alexandrakis MG, Kyriakou DS, Passam FH, Malliaraki N,Vlachonikolis IG, Karkavitsas N et al. Urinary N-telopeptide levelsin multiple myeloma patients, correlation with Tc-99m-sestaMIBIscintigraphy and other biochemical markers of disease activity.Hematol Oncol 2003; 21: 17–24.
67 Terpos E, Berenson J, Cook RJ, Lipton A, Coleman RE. Prognosticvariables for survival and skeletal complications in patients withmultiple myeloma osteolytic bone disease. Leukemia 2010; 24:1043–1049.
68 Turesson I, Abildgaard N, Ahlgren T, Dahl I, Holmberg E, Hjorth Met al. Prognostic evaluation in multiple myeloma: an analysis ofthe impact of new prognostic factors. Br J Haematol 1999; 106:1005–1012.
69 Schutt P, Rebmann V, Brandhorst D, Wiefelsputz J, Ebeling P,Opalka B et al. The clinical significance of soluble humanleukocyte antigen class-I, ICTP, and RANKL molecules in multiplemyeloma patients. Hum Immunol 2008; 69: 79–87.
70 Terpos E, Berenson J, Lipton A, Coleman R, Cook R. High baselineNTX predicts for inferior survival and shorter time to first SRE inMultiple Myeloma. Clin Lymphoma Myeloma 2009; 9 (Suppl 1):50–51.
71 Elomaa I, Risteli L, Laakso M, Lahtinen R, Virkkunen P, Risteli J.Monitoring the action of clodronate with type I collagenmetabolites in multiple myeloma. Eur J Cancer 1996; 32A:1166–1170.
72 Berenson JR, Rosen LS, Howell A, Porter L, Coleman RE, Morley Wet al. Zoledronic acid reduces skeletal-related events in patientswith osteolytic metastases. Cancer 2001; 91: 1191–1200.
73 Rosen LS, Gordon D, Kaminski M, Howell A, Belch A, Mackey Jet al. Zoledronic acid versus pamidronate in the treatment ofskeletal metastases in patients with breast cancer or osteolyticlesions of multiple myeloma: a phase III, double-blind, compara-tive trial. Cancer J 2001; 7: 377–387.
74 Menssen HD, Sakalov A, Fontana A, Herrmann Z, Boewer C,Facon T et al. Effects of long-term intravenous ibandronate therapyon skeletal-related events, survival, and bone resorption markers inpatients with advanced multiple myeloma. J Clin Oncol 2002; 20:2353–2359.
75 Terpos E, Viniou N, de la Fuente J, Meletis J, Voskaridou E,Karkantaris C et al. Pamidronate is superior to ibandronate indecreasing bone resorption, interleukin-6 and beta 2-micro-globulin in multiple myeloma. Eur J Haematol 2003; 70: 34–42.
76 Terpos E, Mihou D, Szydlo R, Tsimirika K, Karkantaris C, Politou Met al. The combination of intermediate doses of thalidomidewith dexamethasone is an effective treatment for patients withrefractory/relapsed multiple myeloma and normalizes abnormalbone remodeling, through the reduction of sRANKL/osteo-protegerin ratio. Leukemia 2005; 19: 1969–1976.
77 Lipton A, Cook RJ, Coleman RE, Smith MR, Major P, Terpos E et al.Clinical utility of biochemical markers of bone metabolism forimproving the management of patients with advanced multiplemyeloma. Clin Lymphoma Myeloma 2007; 7: 346–353.
78 Henry D, von Moos R, Vadhan-Raj S, Hungria V, Spencer A, Hirsh Vet al. A double-blind, randomized study of denosumab versuszoledronic acid for the treatment of bone metastases in patients withadvanced cancer (excluding breast and prostate cancer) or multiplemyeloma. Eur J Cancer 2009: (Suppl 3): 12 (abstract 20LBA).
79 Seidel C, Hjertner +, Abildgaard N, Heickendorff L, Hjorth M,Westin J et al. Serum osteoprotegerin levels are reduced in patientswith multiple myeloma with lytic bone disease. Blood 2001; 98:2269–2271.
80 Lipton A, Ali SM, Leitzel K, Chinchilli V, Witters L, Engle L et al.Serum osteoprotegerin levels in healthy controls and cancerpatients. Clin Cancer Res 2002; 8: 2306–2310.
81 Goranova-Marinova V, Goranov S, Pavlov P, Tzvetkova T. Serumlevels of OPG, RANKL and RANKL/OPG ratio in newly-diagnosedpatients with multiple myeloma. Clinical correlations. Haemato-logica 2007; 92: 1000–1001.
82 Martini G, Gozzetti A, Gennari L, Avanzati A, Nuti R, Lauria F. Theeffect of zoledronic acid on serum osteoprotegerin in early stagemultiple myeloma. Haematologica 2006; 91: 1720–1721.
83 Terpos E, Kastritis E, Roussou M, Heath D, Christoulas D,Anagnostopoulos N et al. The combination of bortezomib,melphalan, dexamethasone and intermittent thalidomide is aneffective regimen for relapsed/refractory myeloma and isassociated with improvement of abnormal bone metabolism andangiogenesis. Leukemia 2008; 22: 2247–2256.
84 Kraj M, Owczarska K, Soko"owska U, Centkowski P, Pog"od R,Kruk B. Correlation of osteoprotegerin and sRANKL concentrationsin serum and bone marrow of multiple myeloma patients.Arch Immunol Ther Exp 2005; 53: 454–464.
85 Nanci A. Content and distribution of noncollagenous matrixproteins in bone and cementum: relationship to speed of formationand collagen packing density. J Struct Biol 1999; 126: 256–269.
86 Tian E, Zhan F, Walker R, Rasmussen E, Ma Y, Barlogie B et al. Therole of the Wnt-signaling antagonist DKK1 in the development ofosteolytic lesions in multiple myeloma. N Engl J Med 2003; 349:2483–2494.
87 Politou MC, Heath DJ, Rahemtulla A, Szydlo R, Anagnostopoulos A,Dimopoulos MA et al. Serum concentrations of Dickkopf-1 proteinare increased in patients with multiple myeloma and reducedafter autologous stem cell transplantation. Int J Cancer 2006; 119:1728–1731.
88 Kaiser M, Mieth M, Liebisch P, Oberlander R, Rademacher J,Jakob C et al. Serum concentrations of DKK-1 correlate with theextent of bone disease in patients with multiple myeloma. Eur JHematol 2008; 80: 490–494.
89 Haaber J, Abildgaard N, Knudsen LM, Dahl IM, Lodahl M,Thomassen M et al. Myeloma cell expression of 10 candidategenes for osteolytic bone disease. Only overexpression of DKK1
Bone markers in multiple myelomaE Terpos et al
1710
Leukemia

correlates with clinical bone involvement at diagnosis. Br JHaematol 2008; 140: 25–35.
90 Yaccoby S, Ling W, Zhan F, Walker R, Barlogie B, Shaughnessy Jr JDet al. Antibody-based inhibition of DKK1 suppresses tumor-inducedbone resorption and multiple myeloma growth in vivo. Blood 2007;109: 2106–2111.
91 Tosi P, Zamagni E, Cellini C, Parente R, Cangini D, Tacchetti Tet al. First-line therapy with thalidomide, dexamethasone andzoledronic acid decreases bone resorption markers in patients withmultiple myeloma. Eur J Haematol 2006; 76: 399–404.
92 Breitkreutz I, Raab MS, Vallet S, Hideshima T, Raje N, Mitsiades Cet al. Lenalidomide inhibits osteoclastogenesis, survival factors andbone-remodeling markers in multiple myeloma. Leukemia 2008;22: 1925–1932.
93 Zangari M, Esseltine D, Lee CK, Barlogie B, Elice F, Burns MJ et al.Response to bortezomib is associated to osteoblastic activation inpatients with multiple myeloma. Br J Haematol 2005; 131: 71–73.
94 Zangari M, Yaccoby S, Cavallo F, Esseltine D, Tricot G. Responseto bortezomib and activation of osteoblasts in multiple myeloma.Clin Lymphoma Myeloma 2006; 7: 109–114.
95 Heider U, Kaiser M, Muller C, Jakob C, Zavrski I, Schulz CO et al.Bortezomib increases osteoblast activity in myeloma patientsirrespective of response to treatment. Eur J Haematol 2006; 77:233–238.
96 Giuliani N, Morandi F, Tagliaferri S, Lazzaretti M, Bonomini S,Crugnola M et al. The proteasome inhibitor bortezomib affectsosteoblast differentiation in vitro and in vivo in multiple myelomapatients. Blood 2007; 110: 334–338.
97 Terpos E, Heath DJ, Rahemtulla A, Zervas K, Chantry A,Anagnostopoulos A et al. Bortezomib reduces serum dickkopf-1and receptor activator of nuclear factor-kappaB ligand concentrations and normalises indices of bone remodelling inpatients with relapsed multiple myeloma. Br J Haematol 2006;135: 688–692.
Appendix
International myeloma working group
Rafat Abonour, Indiana University School of Medicine,Indianapolis, Indiana, USARay Alexanian, MD Anderson, Houston, Texas, USAKenneth C. Anderson, DFCI, Boston, Massachusetts, USAMichael Attal, Purpan Hospital, Toulouse, FranceHerve Avet-Loiseau, Institute de Biologie, Nantes, FranceAshraf Badros, University of Maryland, Baltimore, Maryland, USABart Barlogie, M.I.R.T. UAMS Little Rock, Arkanas, USARegis Batille, Institute de Biologie, Nantes, FranceMeral Beksac, Ankara University, Ankara, TurkeyAndrew Belch, Cross Cancer Institute, Alberta, CanadaBill Bensinger, Fred Hutchinson Cancer Center, Seattle,Washington, USAP. Leif Bergsagel, Mayo Clinic Scottsdale, Scottsdale, Arizona,USAJenny Bird, Bristol Haematology and Oncology Center, Bristol,UKJoan Blade, Hospital Clinica, Barcelona, SpainMario Boccadoro, University of Torino, Torino, ItalyMichele Cavo, Universita di Bologna, Bologna, ItalyWen Ming Chen, MM Research Center of Beijing, Beijing,ChinaTony Child, Leeds General Hospital, Leeds, United KingdomJames Chim, Department of Medicine, Queen Mary Hospital,Hong KongWee-Joo Chng, National University Health System, SingaporeRay Comenzo, Tufts Medical School, Boston, Massachusetts,USAJohn Crowley, Cancer Research and Biostatistics, Seattle,Washington, USAWilliam Dalton, H. Lee Moffitt, Tampa, Florida, USAFaith Davies, Royal Marsden Hospital, London, EnglandCarmino de Souza, Univeridade de Campinas, Caminas, BrazilMichel Delforge, University Hospital Gasthuisberg, Leuven,BelgiumMeletios Dimopoulos, University of Athens School of Medicine,Athens, GreeceAngela Dispenzieri, Mayo Clinic, Rochester, Minnesota, USAMatthew Drake, Mayo Clinic, Rochester, Minnesota, USABrian G.M. Durie, Cedars-Sinai Outpatient Cancer Center, LosAngeles, California, USAJohannes Drach, University of Vienna, First Dept. of InternalMedicine, Vienna, Austria
Hermann Einsele, Universitatsklinik Wurzburg, Wurzburg,GermanyTheirry Facon, Centre Hospitalier Regional Universitaire deLille, Lille, FranceDorotea Fantl, Socieded Argentinade Hematolgia, Buenos Aires,ArgentinaJean-Paul Fermand, Hopitaux de Paris, Paris, FranceRafael Fonseca, Mayo Clinic Arizona, Scottsdale, Arizona, USAGosta Gahrton, Karolinska Institute for Medicine, Huddinge,SwedenChristina Gasparetto, Duke University Medical Center, Durham,North Carolina, USAMorie Gertz, Mayo Clinic, Rochester, Minnesota, USAJohn Gibson, Royal Prince Alfred Hospital, Sydney, AustraliaSergio Giralt, MD Anderson Cancer Center, Houston, Texas,USAHartmut Goldschmidt, University Hospital Heidelberg,Heidelberg, GermanyPhilip Greipp, Mayo Clinic, Rochester, Minnesota, USARoman Hajek, Brno University, Brno, Czech RepublicIzhar Hardan, Tel Aviv University, Tel Aviv, IsraelJean-Luc Harousseau, Institute de Biologie, Nantes, FranceHiroyuki Hata, Kumamoto University Hospital, Kumamoto,JapanYutaka Hattori, Keio University School of Medicine, Tokyo,JapanTom Heffner, Emory University, Atlanta, Georgia, USAJoy Ho, Royal Prince Alfred Hospital, Sydney, AustraliaVania Hungria, Clinica San Germano, Sao Paolo, BrazilShinsuke Ida, Nagoya City University Medical School, Nagoya,JapanPeter Jacobs, Constantiaberg Medi-Clinic, Plumstead, SouthAfricaSundar Jagannath, St. Vincent’s Comprehensive Cancer Center,New York, New York, USAHou Jian, Shanghai Chang Zheng Hospital, Shanghai, ChinaDouglas Joshua, Royal Prince Alfred Hospital, Sydney, AustraliaArtur Jurczyszyn, The Myeloma Treatment Foundation, PolandAsher Chanan Kahn, Roswell Park Cancer Institute, Buffalo,New York, USAMichio Kawano, Yamaguchi University, Ube, JapanNicolaus Kroger, University Hospital Hamburg, Hamburg,GermanyShaji Kumar, Department of Hematology, Mayo Clinic,Minnesota, USARobert Kyle, Department of Laboratory Med. and Pathology,Mayo Clinic, Minnesota, USA
Bone markers in multiple myelomaE Terpos et al
1711
Leukemia
Juan Lahuerta, Grupo Espanol di Mieloma, Hospital Universi-tario, Madrid, SpainOla Landgren, National Cancer Institute, Bethesda, Maryland,USAJacob Laubach, Dana-Farber Cancer Institute, Boston,Massachusetts, USAJae Hoon Lee, Gachon University Gil Hospital, Incheon, KoreaXavier LeLeu, Hospital Huriez, CHRU Lille, FranceSuzanne Lentzsch, University of Pittsburgh, Pittsburgh,Pennsylvania, USAHenk Lokhorst, University Medical CenterUtrecht, Utrecht, TheNetherlandsSagar Lonial, Emory University Medical School, Atlanta,Georgia, USAHeinz Ludwig, Wilhelminenspital Der Stat Wien, Vienna,AustriaAngelo Maiolino, Rua fonte da Saudade, Rio de Janeiro, BrazilMaria Mateos, University of Salamanca, Salamanca, SpainJayesh Mehta, Northwestern University, Chicago, Illinois, USAGiamPaolo Merlini, University of Pavia, Pavia, ItalyJoseph Mikhael, Mayo Clinic Arizona, Scottsdale, Arizona, USAAngelina Rodriquez Morales, Bonco Metro Politano de Sangre,Caracas, VenezuelaPhilippe Moreau, University Hospital, Nantes, FranceGareth Morgan, Royal Marsden Hospital, London, EnglandNikhil Munshi, Diane Farber Cancer Institute, Boston, Massa-chusetts, USARuben Niesvizky, Weill Medical College of Cornell University,New York, New York, USAAmara Nouel, Hospital Rutz y Paez, Bolivar, VenezuelaYana Novis, Hospital SırioLibanes, Bela Vista, BrazilRobert Orlowski, MD Anderson Cancer Center, Houston, Texas,USAAntonio Palumbo, Cathedra Ematologia, Torino, ItalySantiago Pavlovsky, Fundaleu, Buenos Aires, ArgentinaLinda Pilarski, University of Alberta, Alberta, CanadaRaymond Powles, Leukemia & Myeloma, Wimbledon, EnglandS. Vincent Rajkumar, Mayo Clinic, Rochester, Minnesota, USADonna Reece, Princess Margaret Hospital, Toronto, CanadaTony Reiman, Cross Cancer Institute, Alberta, CanadaPaul G. Richardson, Dana Farber Cancer Institute, Boston,Massachusetts, USADavid Roodman, University of Pittsburgh Medical Center,Pittsburgh, PA, USA
Laura Rosinol, Hospital Clinic, Barcelona, SpainJesus San Miguel, University of Salamanca, Salamanca, SpainOrhan Sezer, Universitat Hamburg, Hamburg, GermanyJatin Shah, MD Anderson Cancer Institute, Houston, Texas, USAJohn Shaughnessy, M.I.R.T. UAMS, Little Rock, Arkansas, USAKazuyuki Shimizu, Nagoya City Midori General Hospital,Nagoya, JapanChaim Shustik, McGill University, Montreal, CanadaDavid Siegel, Hackensack, Cancer Center, Hackensack, NewJersey, USASeema Singhal, Northwestern University, Chicago, Illinois, USAPieter Sonneveld, Erasmus MC, Rotterdam, The NetherlandsAndrew Spencer, The Alfred Hospital, Melbourne, AustraliaEdward Stadtmauer, University of Pennsylvania, Philadelphia,Pennsylvania, USAKeith Stewart, Mayo Clinic Arizona, Scottsdale, Arizona, USAEvangelos Terpos, University of Athens School of Medicine,Athens, GreecePatrizia Tosi, Italian Cooperative Group, Istituto di EmatologiaSeragnoli, Bologna, ItalyGuido Tricot, Huntsman Cancer Institute, Salt Lake City, Utah,USAIngemar Turesson, Department of Hematology, Malmo Uni-versity, Malmo, SwedenKarin Vanderkerken, Vrije University Brussels VUB, Brussels,BelgiumBrian Van Ness, University of Minnesota, Minneapolis, Minne-sota, USAIvan Van Riet, Brussels Vrija University, Brussels, BelgiumRobert Vescio, Cedars-Sinai Cancer Center, Los Angeles,California, USADavid Vesole, Hackensack Cancer Center, Hackensack, NewJersey, USAAnders Waage, University Hospital, Trondheim, Norway NSMGMichael Wang, M.D. Anderson, Houston, Texas, USADonna Weber, MD Anderson, Houston, Texas, USAJan Westin, Sahlgrenska University Hospital, Gothenburg,SwedenKeith Wheatley, University of Birmingham, Birmingham, UnitedKingdomDina B. Yehuda, Department of Hematology, HadassahUniversity Hospital, Hadassah, IsraelJeffrey Zonder, Karmanos Cancer Institute, Detroit, Michigan,USA
Bone markers in multiple myelomaE Terpos et al
1712
Leukemia