The Urinary System Part 4: Regulation & Maintenance.
79
The Urinary System Part 4: Regulation & Maintenance
-
Upload
james-hampton -
Category
Documents
-
view
219 -
download
0
Transcript of The Urinary System Part 4: Regulation & Maintenance.

The Urinary System
Part 4: Regulation & Maintenance

The Urinary System
Goals of the Urinary System: Regulate chemical composition of the bodily fluids & eliminate waste products from the body.
Organs of the Urinary System: Two kidneys, two ureters, the urinary bladder, & the urethra.


The Kidneys
The Kidneys: Bean-shaped organs, part of the urinary system, that filter wastes & excess products from the bloodstream so they can be removed from the human body. Retroperitoneal: Located posterior to the
peritoneum of the abdominal cavity – technically outside the abdominal cavity.
0.5% of the total body weight. 20-25% of the total arterial blood is received
by the kidneys.

Functions of the Kidneys
Filter waste products from the blood, returning useful materials & eliminating wastes and excesses of normal components.
Regulate the chemical composition of blood. Regulate volume & composition of bodily fluids. Regulate blood volume & pressure. Regulate the osmolarity of bodily fluids. Secrete renin (an enzyme that helps to control blood pressure & electrolyte
balance). Secrete erythropeitin (hormone that stimulates red blood cell production). Help regulate acid-base balance of body fluids. Synthesize calcitriol (hormone that helps regulate calcium balance). Detoxify free radicals & some drugs. Gluconeogensis: The synthesis of glucose from non-carbohydrates to
release glucose in the blood & maintain blood glucose levels at normal. Regulate blood ion levels. Participate in Vitamin D synthesis.

External Kidney Anatomy
The Kidneys: Bean-shaped reddish-colored organs, lying just above the waist between the peritoneum & the posterior wall of the abdomen, behind the abdominal cavity. The right kidney is slightly lower than the left due to
the placement of the liver superior to the right kidney.
Lateral Surface is convex. Medial Surface is concave.
Renal Hilus: The point at which the ureter, blood vessels, lymphatic vessels, & nerve endings connect.


Kidney Anatomy
Three layers of tissue surrounding each kidney: Renal Capsule: The deep inner layer of smooth,
transparent dense irregular connective tissue that is continuous with the other layer of the urethral covering.
Provides a barrier against trauma & helps maintain the shape of the organ.
Adipose Capsule: The fatty tissue surrounding the renal capsule – helps protect the kidney & hold it in place.
Renal Fascia: Outermost layer of thin, dense irregular connective tissue hat anchors the kidneys to the surrounding structure & the abdominal wall.

Internal Kidney Anatomy
Two internal regions: Renal Cortex: The superficial, reddish, smooth
textured area running from the renal capsule to the bases of the renal pyramids.
Divided into the cortical and juxtamedullary zones. Renal Columns: The portions of the renal cortex that
extends between the renal pyramids. Renal Medulla: The deep, reddish-brown inner
region. Renal Pyramids: 8-18 fan-shaped structures consisting of
the straight segmented renal tubules & the vasa recta. The base facing the renal cortex and the apex (aka renal palilla)
pointing toward the renal hilus. Renal Lobe: The renal pyramid, its overlaying cortex, and ½
of each adjacent renal column.


Internal Kidney Anatomy
Parenchyma: Composed of the renal cortex & the renal pyramids. Nephrons: 1 million microscopic structures designed
to filter the blood – located within the parenchyma. Papillary Ducts: Ducts that drain the urine formed in
the nephrons into the… Minor Calyces: 8-18 in each kidney, which receive urine from
the papillary ducts & delivering it to the major calyces. Major Calyces: 2-3 in each kidney, receive urine from the
minor calyces & drain it into the large cavity of the renal pelvis.
Renal Pelvis: Drains the urine into the ureter to be taken to the urinary bladder.

Blood Supply to the Kidneys
Renal Arteries: The main blood vessel bringing blood into the renal area.
Segmental Arteries: The subdivisions of the renal arteries that branch into the parenchyma.
Interlobar Arteries: Pass through the renal columns between the renal pyramids.
Arcuate Arteries: The branches that arch between the renal medulla & renal cortex.
Interlobular Arteries: The divisions of the arcuate arteries.

Blood Supply to the Kidneys
Golmerulus: The ball-shaped capillary network serving the nephrons – these are part of both the cardiovascular & urinary systems. This is a unique capillary bed since it is located between two
arterioles instead of an arteriole & an a venule! Afferent Arterioles: The divisions of the interlobular arteries
that enter the renal cortex & supply the glomerulus with blood. Efferent Arterioles: Carry blood back out of the glomerulus.
Peritubular Capillaries: Further divisions of the efferent arterioles that surround the tubular portions of the nephron & reclaim most of the filtrate the glomerulus produces.
Vasa Recta: The long loop-shaped capillaries that extend from some efferent arterioles that supply the tubular portions of the nephron in the renal medulla.


Blood Supply to the Kidneys
Peritubular Venules: The first veins that the peritubular capillaries reunite into.
Interlobular Veins: The merged peritubular venules, also receiving blood from the vasa recta.
Arcuate Veins: The next largest set of veins the interlobular veins drain into.
Interlobar Veins: Drain the blood from between the renal pyramids.
Renal Vein: The large, single vein that all blood exits the kidneys through. Exits from the renal hilus & varies venous blood back
to the inferior vena cava.


Blood Flow to the Kidneys
Control of blood flow to the kidneys occurs via the renal nerves, formed in the celiac ganglion & pass through the renal plexus along with the renal arteries.
The sympathetic division of the Autonomic Nervous System regulates the flow of blood through the kidneys via vasodilation or vasoconstriction.

Blood Flow to the Kidneys
Path of Blood Flow through the kidneys: Renal Arteries Segmental Arteries Arcuate Arteries Interlobular Arteries Afferent Arterioles Glomerular Capillaries Efferent Arterioles Peritubular Capillaries Interlobular Veins Arcuate Veins Interlobar Veins Renal Vein


The Nephron
Nephron: The functional unit of the kidney consisting of a microscopic tube open at one end and closed at the other. Over 1 million nephrons in each kidney. Nephrons are the unit that form the urine.
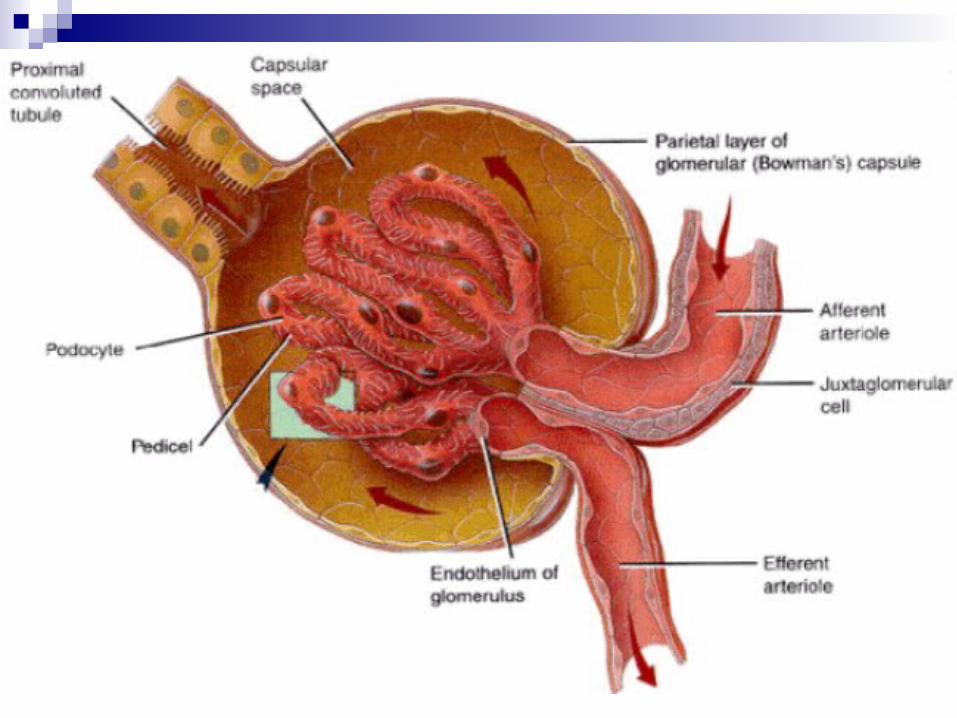
Two Parts to a Nephron: Renal Corpuscle: The portion where the blood
plasma is filtered. Glomerulus: The capillary network where blood enters to be
filtered. Glomerular (Bowman’s) Capsule: The double-walled
epithelial cup that surrounds the glomerular capillaries. Renal Tubule: The tube into which the filtered fluid is
passed.


The Nephron
Glomerular (Bowman’s) Capsule: The double-walled epithelial cup that surrounds the glomerular capillaries. This is where blood plasma is actually filtered before moving into
the renal tubule. Capsular Space aka Lumen of the Bowman’s Capsule: The
place where plasma leaves the glomerular capillaries – plasma is now known as filtrate.
Filtrate: Similar to blood, but lacking blood cells & large proteins.
Two layers of the Bowman’s Capsule: External Parietal Layer: The simple squamous epithelium layer
– not involved in filtrate formation. Visceral Layer: Made up of podocytes (highly branching
epithelial cells) and is involve in filtrate formation.

The Nephron
Renal Tubule: The tube into which the filtered fluid is passed. 3 sections… Proximal Convoluted Tubule (PCT): The part of the tubule that is
attached to the flomerulus. Fluid flows from the PCT into the… Loop of Henle aka the Nephron Loop: The portion of the loop that
connects the proximal & distal convoluted tubules. Descending Limb of the Loop of Henle: The portion that dips into the renal
medulla. Ascending Limb of the Loop of Henle: The portion that makes a U-turn &
returns to the renal cortex. Distal Convoluted Tubule (DCT): The part of the tubule that is farthest
away from the glomerulus. Two cell types exit here: Principal Cells: Have receptors for antidiuretic hormone & aldosterone to
regulate fluid & electrolyte balance. Intercalated Cells: Help in the homeostasis regulation of blood pH.
Collecting Duct: The vessel that collects the filtrate from the distal convoluted tubule. Papillary Ducts: The convergence of the collecting ducts (several
hundred in the body). They drain into the minor calyces.


The Nephron
Glomerular Tubule: The tube formed by the wall of the nephron pushing into the glomerolar capsule at the closed end of the nephron.
Renal Tubule: The final part of the ascending limb of each nephron, which makes contact with the afferent arteriole. Juxtaglomerular Apparatus (JGA): Helps regulate
the blood pressure in the kidneys. Made up of.. Macula Densa: The crowded area of columnar tubules
found in the renal tubule. Juxtaglomerular (JG) Cells: The afferent arteriole
containing modified, smooth muscle fibers that runs along side the macula densa.

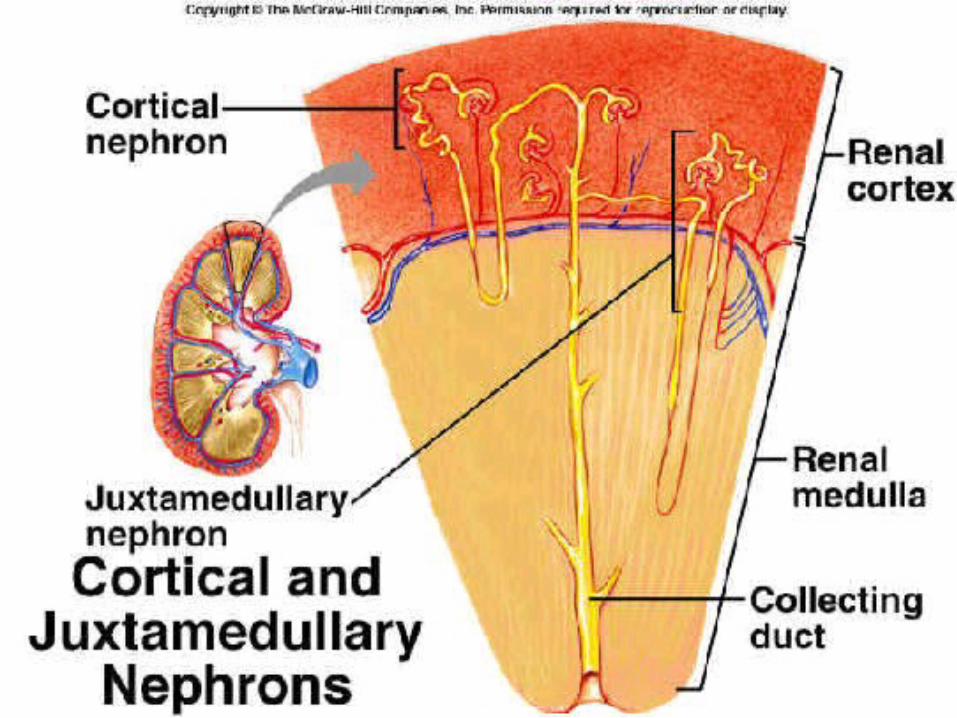
Types of Nephrons
Cortical Nephrons: Nephrons whose renal corpuscles are located in the outer portion of the renal cortex. Have short Loops of Henle (not entering too deeply into the renal
medulla) with blood supplied by peritubular capillaries. Vital in assuring blood has the correct chemical & ionic makeup. The most common type - 85% of nephrons.
Juxtamedullary Nephrons: Nephrons whose renal corpuscles located deep in the cortex, close to the medulla. Have long Loops of Henle extending deep into the medulla with
blood supplied by the peritubular capillaries & the vasa recta. Ascending limbs divide into two portions.. The thin ascending
limb & thick ascending limb. Allow the kidneys to produce very dilute or very concentrated
urine. Make up the remaining 15-20% of nephrons.
Urine Formation
Blood flows into the kidneys and into the glomerular capillaries. Some of the blood in the glomerular capillaries is forced into the
renal tubules, which flow alongside of the peritubular capillaries. 99% of water forced into the renal tubules gets reabsorbed into these
vessels. Fluid is filtered from the blood into the renal tubules – any particle
small enough to pass through the membranes will be filtered out. This includes glucose, amino acids, vitamins, & minerals. Any needed items are reabsorbed back into the blood stream while still
in the renal tubules. Waste products, including creatinine, toxins, & drugs are not reabsorbed
& are excreted via urine. Kidneys can regulate how much sodium, potassium, hydrogen, &
bicarbonate remain in the plasma. Urine formed through 3 basic processes:
Glomelular filtration Tubular secretion Tubular reabsorpton


Glomerular Filtration
Glomerular Filtration: The first step of urine formation! Water & most dissolved solutes in the blood plasma
cross the capillary walls in the glomerulus to move into the glomerular capsule & then the renal tubule.
Glomerular Filtrate: The fluid that enters the capsular space. Filtration Fraction: The fraction of blood plasma in
the afferent arterioles of the kidneys that becomes glomerular filtrate – typically 16-20%
Men produce 180 liters in filtrate daily while women produce 150 liters of filtrate daily.
99% of filtrate returns to the blood via reabsorption. 1-2 liters are excreted as urine.

Glomerular Filtration
Filtration Membrane: A layer of 3 barriers that fluid must pass through to move from the bloodstream to the capsular space. Fenestrated Epithelium: Found in the glomerular capillaries –
large pores permit entry of blood plasma into the capillaries, but prevent blood & platelets from passing.
Mesangial Cells: Cells specifically in charge of regulating glomerular filtration.
Basal Lamina: Layer of acellular material located between the endothelium & podocytes, consisting of collagen fibers & proteoglycans – prevets the filtration of larger plasma proteins.
Slit Membrane: Extends across each filtration slit to permit the passage of small diameter (less than 6-7nm) molecule
E.g., water, glucose, vitamins, amino acids, small proteins, ammonia, urea, & ions.
Pedicels: Footlike processes located on the podocytes (thousands on each) that wrap around glomerular cavities.
Filtration Slits: Spaces between the pedicles.


Glomerular Filtration
In order for filtration to occur, pressure is needed to force fluids & solutes through the membranes.
Renal corpuscles filter the largest volume of fluid of all capillaries due to…. Large surface areas of the glomerular capillaries –
mesangial cells can relax to maximize surface area & increase filtration or contract to decrease surface area and filtration.
Filtration membrane is thin & porous. Glomerular capillary blood pressure is high due to
afferent arteriole diameter exceeding efferent arteriole diameter.

Glomerular Filtration
Glomerular Pressure dependent on 3 processes: Glomerular Blood Hydrostatic Pressure (GBHP):
The blood pressure in the glomerular capillaries – promotes filtration by forcing water & solutes from the blood plasma through the filtration membrane. Normally 55 mm Hg.
Capsular Hydrostatic Pressure (CHP): The measure of the hydrostatic pressure exerted against the filtration membrane by fluid already in the capsular space & renal tubule, which opposes filtration & creates a “back pressure”. Normally 15 mm Hg.
Blood Colloid Osmotic Pressure (BCOP): Opposes filtration – also due to the presence of proteins. Normally 30 mm Hg.
Glomerular Filtration
Net Filtration Pressure (NFP): The total pressure that promotes filtration. Normally 10 mm Hg Determined as…
NFP = GBHP – CHP – BCOP 10 mm Hg = 55 – 15 – 30 mm Hg
Glomerular Filtration
Glomerular Filtration Rate (GFR): The amount of filtration formed in all the renal corpuscles of both kidneys each minute. Regulated via net filtration rate, adjustment of blood
flow into & out of the glomerulus, and altering of the glomerular capillary surface area.
Efferent & afferent arteriole diameters can coordinate control.
Rate increases with capillary blood flow increase. If too high… urine output increases & dehydration &
electrolyte depletion may occur due to shortened tubular reabsorption.
If too low… Tubular reabsorption is increased and wastes may be reabsorbed that should be eliminated.

Glomerular Filtration
Glomerular Filtration Rate controlled by 3 mechanisms… Renal Auto Regulation: The ability of the kidneys to maintain a relatively stable
GFR despite blood pressure changes. Occurs via.. Myogenic Mechanism: Stretching triggers smooth muscle contractions – afferent
arterioles can constrict to reduce blood flow into the glomerulus, while efferent arterioles can be dilated to allow increased outflow of blood. Can be reversed to compensate for decreased blood pressure.
Tubuloglomerular Feedback: Sodium, chlorine, & water build up in the loop of Henle due to increased blood pressure & faster blood flow through the renal tubules – Macula densa cells detect the imbalance & inhibit nitric oxide (NO) production.
Nitric Oxide (NO): Produced in the juxtaglomerular apparatus (JGA) – causes vasodilation. Decrease leads to vasoconstriction in the afferent arterioles & slows blood flow into the glomerular capillaries & decrease in GRF. Increases occur if blood pressure & GRF fall too low.
Neural Regulation: Sympathetic nervous system activation causes adrenal epinephrine to stimulate vasoconstriction in the afferent arterioles to reduce GRF & urine production.
Conserves blood volume & redirects blood to the heart, brain, & skeletal muscles. Hormonal Regulation: Hormones are produced to change the GRF rate.
Angiotensin II: Reduces GRF through vasoconstriction of the afferent & efferent arterioles – reduces renal blood flow.
Atrial Natriuretic Peptide (ANP): Hormone secreted by cells in the atria of the heart – increases capillary surface area by relaxing the mesangial cells – GRF increases due to faster filtration.
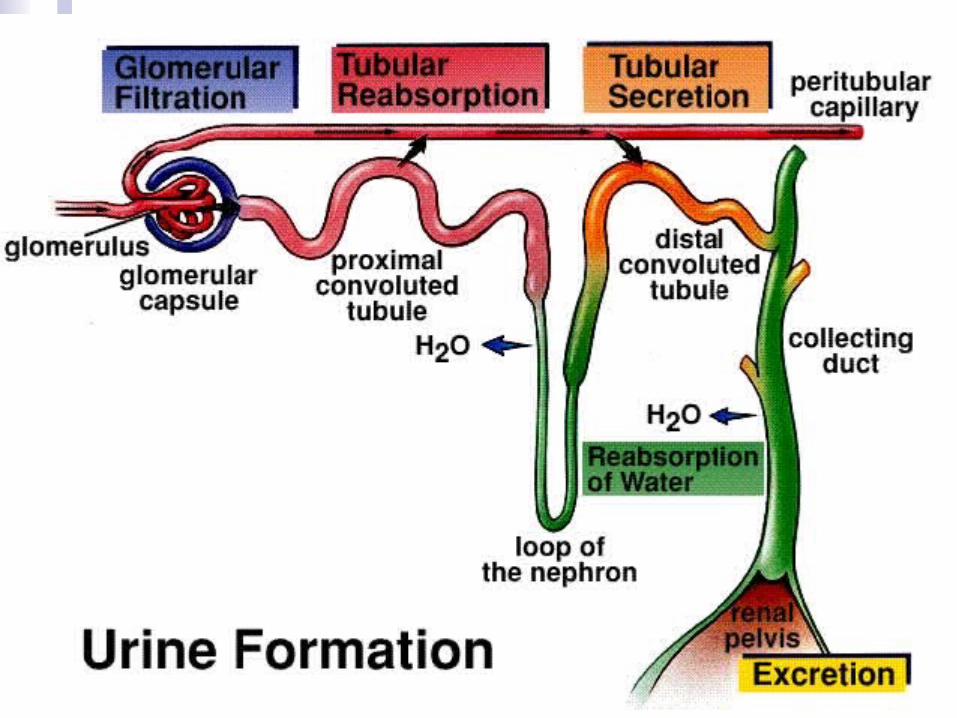

Tubular Reabsorption
Tubular Reabsorption: The return of most of the filtered water & solutes back into the bloodstream from the renal tubules – 99% of the filtered water is reabsorbed. Any substances not reabsorbed is secreted via the
urine.
3 Membranes substances must pass through to re-enter the blood stream: Luminal Membrane of the Tubule Cell Basolateral membrane of the Tubule Cell Capillary Endothelium

Tubular Reabsorption
Two paths for fluid absorbed into the tubule lumen: Moving between adjacent tubule cells Passing through an individual tubule cell.
Tight junctions join neighboring cells to one another. Atypical Membrane: Contacts the tubular fluid – lacks a
sodium-potassium pump to ensure the reabsorption of Na+ only goes one way.
Most sodium ions crossing this membrane will be pumped into the interstitial fluid.
Basolateral Membrane: Contacts the interstitial fluid at the base & sides of the cells.
Cells lining the renal tubule have a low Na+ concentration in the cytosol due to sodium-potassium pumps. Sodium-Potasium Pumps eject Na+ from the renal tubule cells.

Tubular Reabsorption
Paracellular Reabsorption: When fluid leaks between the cells. Accounts for up to 50% of the reabsorption of certain
ions & the water that follows via osmosis.
Transcellular Reabsorption: Where a substance passes from the fluid in the tubular lumen through the apical membrane of a tubule cell, across the cytosol, & out into the interstitial fluid through the basolateral membrane.

Tubular Reabsorption
Primary Active Transport: Occurs when energy is derived from hydrolysis of ATP & is used to pump a substance across a membrane.
Secondary Active Transport: Occurs when the energy stored in an ion’s electrochemical gradient drives a substance across the membrane. Symporters: Membrane proteins that perform secondary active
transport. Antiporters: Move two or more substances in opposite
directions across a membrane. Transport Maximum (Tm): The upper limit on how fast
each transporter can work – measured in mg/min.
Tubular Reabsorption
Osmosis: The method by which water is reabsorbed – occurs when water moves from an area of high concentration to an area of low concentration.
Obligatory Water Reabsorption: Water that is reabsorbed along with solutes – it’s “obligated” to follow solutes. 90% of water reabsorption. Occurs in the PCT & descending loop of Henle.
Facultative Water Reabsorption: Water reabsorption that is not dependent on solutes. Remaining 10% of water reabsorption. Occurs in the collecting ducts. Regulated via antidiuretic hormone.
Tubular Reabsorption
PCT: The site where most reabsorption of water & solutes occurs.
Loop of Henle: Accounts for 20-35% of filtered solute reabsorption & 85% of filtered water reabsorption. Creates the osmotic gradient between the renal cortex & renal
medulla. Aldosterone: Stimulates active NaCl reabsorption and
indirectly stimulates passive water reabsorption. Antidiuretic Hormone (ADH): Triggers water
reabsorption to occur in the collecting duct & produces more concentrated urine. If not present, more diluted urine is produced.


Tubular Secretion
Tubular Secretion: The transfer of materials from the blood and tubule cells into the tubular fluid – materials are transported from the peritubular capillaries into the renal tubule lumen via active transport. Secretes hydrogen, creatine, potassium, etc. from the
peritubular capillaries into the renal tubules if not filtered at the glomerulus.
Hydrogen secretion is increased to raise blood pH & decreased to lower pH – maintains homeostasis.
Eliminates other substances from the body to remove wastes and regulate blood levels of certain ions – includes substances in excessive levels & natural poisons.
Ions removed from the blood stream are deposited into the fluid within the tubules.

The Countercurrent Multiplier
Countercurrent Mechanism: Creates an osmotic gradient in the interstitial fluid of the renal medulla. Enables formation of concentrated urine when
ADH is preset. Countercurrent Flow: Where the
descending limb of the loop of Henle transports tubular fluid from the renal cortex to the medulla & the ascending limb carries it in the reverse direction.

The Countercurrent Multiplier
Descending Limb of the Loop of Henle: Permeable to water, but impermeable to most solutes. Water leaves this limb via osmosis, causing the
osmolarity (concentration) of the tubular fluid to increase.
Ascending Limb of the Loop of Henle: Not permeable to water, but permeable to salt (Na+Cl-) – salt is secreted into the surrounding interstitial fluid. The osmolarity (concentration) of tubular fluid
decreases as it flows through the ascending limb.
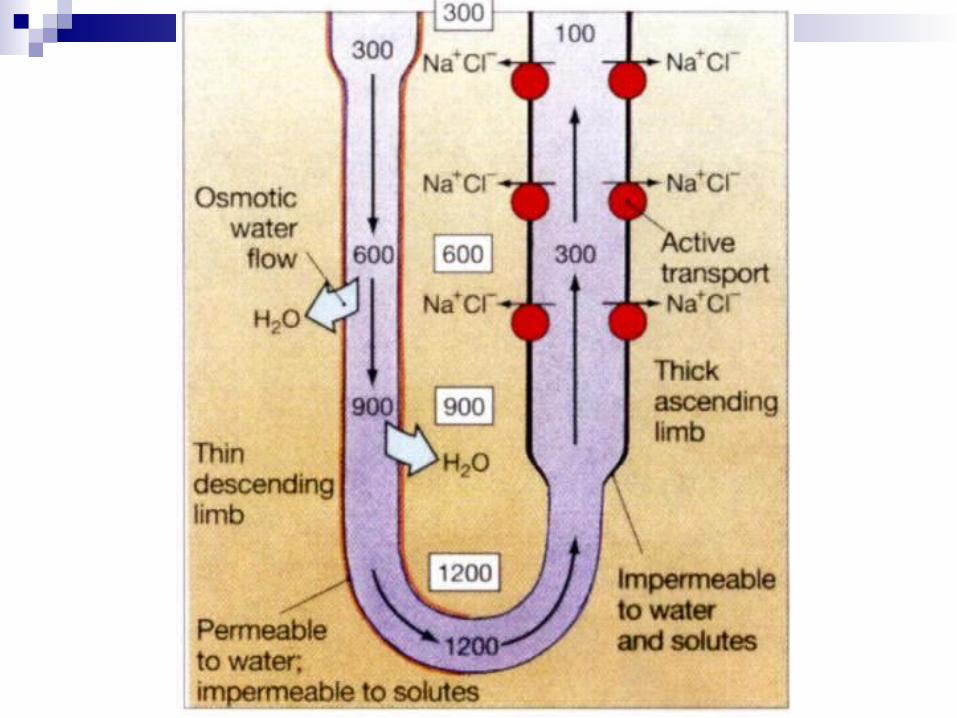

Osmolarity
Osmolarity: The measure of the total number of dissolved particles (solutes) per liter of soution. Kidneys maintain a constant osmolarity of 300
milliosmoles per liter via regulation of the concentration & volume of urine.
Osmotic Gradient: The difference in osmolarity of two solutions on opposite sides of a semi-permeable membrane. Maintained via.. Differences in permeability in the ascending &
descending limbs of the loops of Henle & the collecting ducts.
Countercurrent flow in the two limbs of the loops of Henle.

Osmotic Gradient

Hormones that Regulate Reabsorption & Secretion
Renin-Angiotensin-Aldosterone System: System that activates when blood pressure & blood volume decreaseAfferent arterioles are less stretched,
triggering juxtaglomerular cells to secrete renin enzymes into the blood.
Renin causes angio tensinogen to convert to angiotensin IO.
Angiotensin I changes to the active hormone Angiotensin II.

Hormones that Regulate Reabsorption & Secretion
Angiotensin II: A hormone converted from Angiotensin I that serves 3 main roles… Decrease glomerular filtration rate via
casoconstriction of the afferent arterioles. Enhance reabsorption of Na+, Cl-, & water in the
proximal convoluted tubules via stimulation of the sodium-hydrogen antiporters.
Stimulates the release of aldosterone to stimulate the principal cells in the collecting ducts to reabsorb more Na+ and Cl- & secrete more potassium – also increases water reabsorption to increase blood volume.

Hormones that Regulate Reabsorption & Secretion
Antidiuretic Hormone (ADH) aka Vasopressin: Causes increased water reabsorption in the distal convoluted tubules & collecting ducts, producing less urine volume but higher urine concentration. Osmotic pressure of bodily fluids increase as the
concentration of water in the blood decreases. This stimulates osmoreceptors in the hypothalamus
that then trigger the posterior pituitary gland to release ADH.
ADH controls whether concentrated or diluted urine is formed, depending on the fluid intake and kidney functioning of the individual.

Hormones that Regulate Reabsorption & Secretion
Atrial Natriuretic Factor (ANF) aka Atrial Natriuretic Peptide (AND): Secreted by the heart in response to high blood pressure & stretching of the atria - inhibits sodium & water reabsorption & inhibits aldosterone and ADH secretion. Increases the excretion of sodium & water in
urine, which reduces blood volume & blood pressure.

Urine Composition
Urine: A combination of metabolic wastes (including urea), dissolved salts, and organic material.
Color: Ranges from pale or colorless (dilute) to deep yellow (concentrated). Urochrome: The pigment caused by the breakdown
of bib, contributing to the yellow color of urine. Degredation of bilirubin & urobilin affect yellow color. Medications can cause a reddish-brown color. Can also be affected by bacteria, blood, sperm,
mucous, and some dietary components.

Urine Composition
Chemical Composition: Composed of 95% water & 5% electrolytes – can be changed by certain diseases. Urea: The main waste product of nitrogen
detoxification & the breakdown of protein – composes 2%.
Creatine: A product of creatine phosphate breakdown in muscle tissue.
Uric Acid: The final oxidation product of purine metabolism in the body.

Urine Composition
Specific Gravity: The measure of the kidney’s ability to form concentrated or dilute urine in relation to plasma - measures to amount of substances dissolved in urine. Urine’s Specific Gravity: Typically is 1 – the higher
the concentration of solutes, the higher the specific gravity.
Dehydration or low fluid intake causes an increase in concentration & therefore a higher specific gravity.
Low specific gravity can be caused by diabetes insipidus, glomerulonephritis, & renal failure.

Urine Composition
pH: The measure of the acidity or alkalinity of the urine. Glomerular filtrate of blood plasma goes
through acidification by the renal tubules & collecting ducts – moves from a pH of 7.4 to 6.
pH range is 4.6 to 8 & can vary with diet.

Urine Composition
Quantity: The overall amount of urine produced – typically 1-2 liters per day for a healthy adult. Hydration, activity level, environmental factors, body
size, & health affect the volume produced. Polyuria: The excessive output of urine, typically due
to a high concentration of glucose in the renal tubules. Oliguria: The scanty output of urine, typically due to
fluid retention. Diuretics: Chemicals that increase the volume of
urine produced – decrease the fluid volume in the body via increasing glomerular filtration or decreasing tubular reabsorption.
Used to treat hypertension, congestive heart failure, and some lung disorders.

Urine Composition
Things that Shouldn’t Be In Urine: Proteins: Due to hypertension or
glomerulonephritis. Ketone Bodies: Due to starvation or diabetes
mellitus. Leukocytes: Due to urinary tract infection.Erythrocytes: Due to bleeding in the urinary
tract.Glucose: Due to diabetes mellitus.

What if the Kidneys Shut Down?
Dialysis: The artificial filtering of the blood. Hemodialysis: The use of an artificial kidney
machine that takes blood in through dialysis tubing, filters the blood, & returns it to the patient once cleansed.
Continuous Ambulatory Peritoneal Dialysis (CAPD): The use of the periotoneal lining of the abdominal cavity as a dialysis membrane, allowing waste products to be drained out of the cavity into a sterile bag via gravity.


Ureters
Ureters: Two muscular tubes leading from the renal pelvis of each kidney to the urinary bladder. Peristaltic Contractions: Muscle contractions in the walls of the
ureters that pushes urine down toward the bladder. Urethral Valves: Valves located at the oblique openings of the
ureters to prevent backflow of urine into the kidneys – triggered to close by increased pressure from the bladder when full.
Ureter Walls: 3 layers! Adventitia: Outermost later that helps anchor the ureters. Muscularis: The middle muscular layer. Mucosa: The innermost mucosal layer.


Urinary Bladder
Urinary Bladder: A hallow muscular sac located on the floor of the pelvic cavity. Highly distensible – expands superiorly –
700-800mL capacity.Located directly anterior to the rectum in
males. Located anterior to the vagina & inferior to the
uterus in females. Serosa: The layer of visceral peritoneum
covering the superior surface.

Urinary Bladder
Trigone: The small triangular area on the floor of the urinary bladder containing the openings for the ureters & the urethra.
Internal Urethral Orifice: The opening into the urethra, lying in the anterior corner.

Urinary Bladder
Urinary Bladder Wall: 3 layers total. Adventitia: The superficial coat consisting of areolar
connective tissue anchoring the urethra in place – contains the blood vessels, lymphatic vessels, & nerves that serve the muscularis and mucosa layers.
Muscularis: Two layers of smooth muscle (outer circular & inner longitudinal) contract via peristaltic contraction to move urine.
Mucosa: The deepest coat made of transitional epithelium (that can change shape to expand!) and lamina propria (full of collagen elastic fibers & lymphatic tissue).
Goblet Cells: Secrete mucous to prevent the bladder wall’s tissue from coming in contact with the acidic urine.


Urethra
Urethra: The small tube that leads from the internal urethral orifice in the floor of the bladder to the exterior of the body.
In Females: 3-4 centimeters long, with the external urethral orifice (opening) lying between the opening of the vagina & the clitoris.
In Males: 15-20 centimeters long & 3 regions: Prostatic Urethra: Passes through the prostate. Membranous Urethra: Passes through the urogenital
diaphragm. Penile Urethra aka Spongy Urethra: Passes
through the penis.

Urethra
Mucosal Wall: Consists of a deep mucosa layer & a superficial muscularis layer.
Internal Urethral Sphincter: The circular muscle fibers around the opening from the bladder to the urethra – provides involuntary control of urination.
External Urethral Sphincter: Inferior to the internal urethral sphincter – circular muscle fibers close to the opening from the urethra to the outside – provides voluntary control of urination.


Micturition
Micturition: The discharge of urine from the urinary bladder. AKA urination or voiding.
Micturition Reflex: The reflexive muscular reactions that trigger micturition. Once the bladder exceeds 300-400mL, the pressure increases &
stretch receptors within the bladder walls transmit nerve impulses to the spinal cord.
Micturition Center: The section of the spinal cord between S2 & S3 where stretch impulses are propagated & trigger the micturition reflex.
The micturition reflex sends parasympathetic impulses to the bladder wall & the internal urethral sphincter.
The sphincters open, the bladder wall & detrusor muscles contract, & micturition occurs.

Micturition
Potty Training: The process of learning to control the micturition reflex! Fortunately for us, we
learn this fairly easily during very early childhood.