THE UNINTENDED OUTCOME OF A SUPPLEMENTAL FORMULARY IN HOMEBOUND SENIORS
3
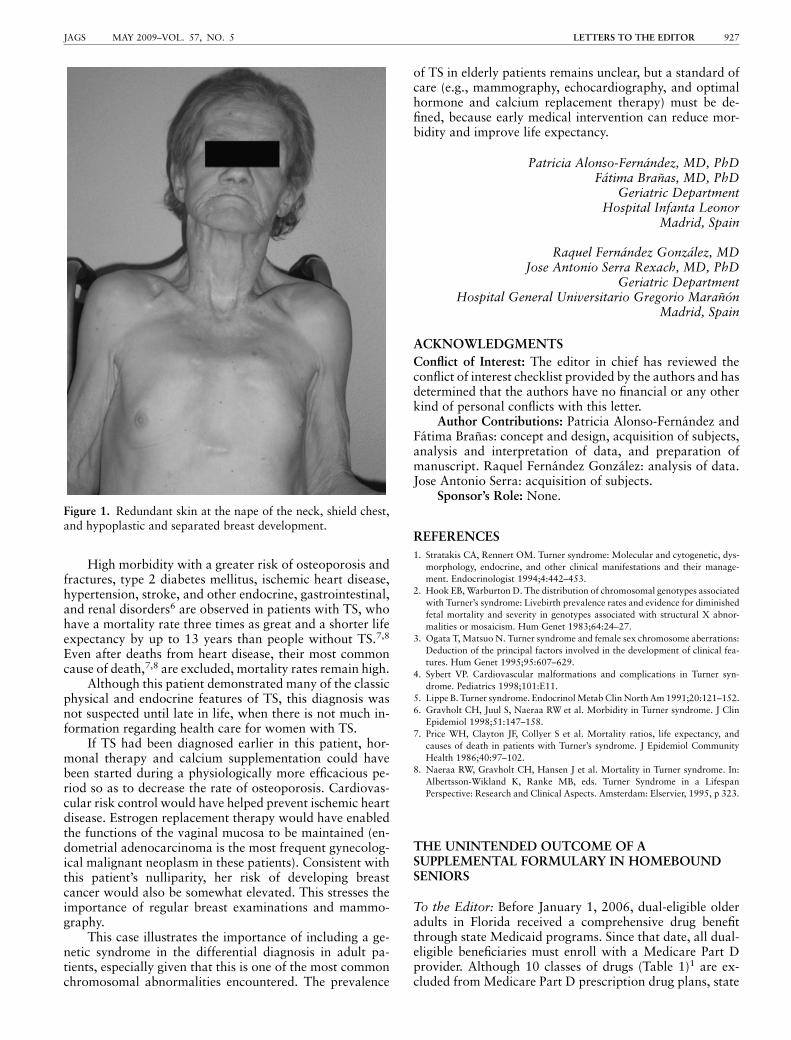
High morbidity with a greater risk of osteoporosis and fractures, type 2 diabetes mellitus, ischemic heart disease, hypertension, stroke, and other endocrine, gastrointestinal, and renal disorders 6 are observed in patients with TS, who have a mortality rate three times as great and a shorter life expectancy by up to 13 years than people without TS. 7,8 Even after deaths from heart disease, their most common cause of death, 7,8 are excluded, mortality rates remain high. Although this patient demonstrated many of the classic physical and endocrine features of TS, this diagnosis was not suspected until late in life, when there is not much in- formation regarding health care for women with TS. If TS had been diagnosed earlier in this patient, hor- monal therapy and calcium supplementation could have been started during a physiologically more efficacious pe- riod so as to decrease the rate of osteoporosis. Cardiovas- cular risk control would have helped prevent ischemic heart disease. Estrogen replacement therapy would have enabled the functions of the vaginal mucosa to be maintained (en- dometrial adenocarcinoma is the most frequent gynecolog- ical malignant neoplasm in these patients). Consistent with this patient’s nulliparity, her risk of developing breast cancer would also be somewhat elevated. This stresses the importance of regular breast examinations and mammo- graphy. This case illustrates the importance of including a ge- netic syndrome in the differential diagnosis in adult pa- tients, especially given that this is one of the most common chromosomal abnormalities encountered. The prevalence of TS in elderly patients remains unclear, but a standard of care (e.g., mammography, echocardiography, and optimal hormone and calcium replacement therapy) must be de- fined, because early medical intervention can reduce mor- bidity and improve life expectancy. Patricia Alonso-Ferna ´ ndez, MD, PhD Fa ´ tima Bran ˜ as, MD, PhD Geriatric Department Hospital Infanta Leonor Madrid, Spain Raquel Ferna ´ ndez Gonza ´lez, MD Jose Antonio Serra Rexach, MD, PhD Geriatric Department Hospital General Universitario Gregorio Maran ˜o ´n Madrid, Spain ACKNOWLEDGMENTS Conflict of Interest: The editor in chief has reviewed the conflict of interest checklist provided by the authors and has determined that the authors have no financial or any other kind of personal conflicts with this letter. Author Contributions: Patricia Alonso-Ferna ´ndez and Fa ´ tima Bran ˜ as: concept and design, acquisition of subjects, analysis and interpretation of data, and preparation of manuscript. Raquel Ferna ´ndez Gonza ´lez: analysis of data. Jose Antonio Serra: acquisition of subjects. Sponsor’s Role: None. REFERENCES 1. Stratakis CA, Rennert OM. Turner syndrome: Molecular and cytogenetic, dys- morphology, endocrine, and other clinical manifestations and their manage- ment. Endocrinologist 1994;4:442–453. 2. Hook EB, Warburton D. The distribution of chromosomal genotypes associated with Turner’s syndrome: Livebirth prevalence rates and evidence for diminished fetal mortality and severity in genotypes associated with structural X abnor- malities or mosaicism. Hum Genet 1983;64:24–27. 3. Ogata T, Matsuo N. Turner syndrome and female sex chromosome aberrations: Deduction of the principal factors involved in the development of clinical fea- tures. Hum Genet 1995;95:607–629. 4. Sybert VP. Cardiovascular malformations and complications in Turner syn- drome. Pediatrics 1998;101:E11. 5. Lippe B. Turner syndrome. Endocrinol Metab Clin North Am 1991;20:121–152. 6. Gravholt CH, Juul S, Naeraa RW et al. Morbidity in Turner syndrome. J Clin Epidemiol 1998;51:147–158. 7. Price WH, Clayton JF, Collyer S et al. Mortality ratios, life expectancy, and causes of death in patients with Turner’s syndrome. J Epidemiol Community Health 1986;40:97–102. 8. Naeraa RW, Gravholt CH, Hansen J et al. Mortality in Turner syndrome. In: Albertsson-Wikland K, Ranke MB, eds. Turner Syndrome in a Lifespan Perspective: Research and Clinical Aspects. Amsterdam: Elservier, 1995, p 323. THE UNINTENDED OUTCOME OF A SUPPLEMENTAL FORMULARY IN HOMEBOUND SENIORS To the Editor: Before January 1, 2006, dual-eligible older adults in Florida received a comprehensive drug benefit through state Medicaid programs. Since that date, all dual- eligible beneficiaries must enroll with a Medicare Part D provider. Although 10 classes of drugs (Table 1) 1 are ex- cluded from Medicare Part D prescription drug plans, state Figure 1. Redundant skin at the nape of the neck, shield chest, and hypoplastic and separated breast development. LETTERS TO THE EDITOR 927 JAGS MAY 2009–VOL. 57, NO. 5
-
Upload
adam-golden -
Category
Documents
-
view
212 -
download
0
Transcript of THE UNINTENDED OUTCOME OF A SUPPLEMENTAL FORMULARY IN HOMEBOUND SENIORS
High morbidity with a greater risk of osteoporosis andfractures, type 2 diabetes mellitus, ischemic heart disease,hypertension, stroke, and other endocrine, gastrointestinal,and renal disorders6 are observed in patients with TS, whohave a mortality rate three times as great and a shorter lifeexpectancy by up to 13 years than people without TS.7,8
Even after deaths from heart disease, their most commoncause of death,7,8 are excluded, mortality rates remain high.
Although this patient demonstrated many of the classicphysical and endocrine features of TS, this diagnosis wasnot suspected until late in life, when there is not much in-formation regarding health care for women with TS.
If TS had been diagnosed earlier in this patient, hor-monal therapy and calcium supplementation could havebeen started during a physiologically more efficacious pe-riod so as to decrease the rate of osteoporosis. Cardiovas-cular risk control would have helped prevent ischemic heartdisease. Estrogen replacement therapy would have enabledthe functions of the vaginal mucosa to be maintained (en-dometrial adenocarcinoma is the most frequent gynecolog-ical malignant neoplasm in these patients). Consistent withthis patient’s nulliparity, her risk of developing breastcancer would also be somewhat elevated. This stresses theimportance of regular breast examinations and mammo-graphy.
This case illustrates the importance of including a ge-netic syndrome in the differential diagnosis in adult pa-tients, especially given that this is one of the most commonchromosomal abnormalities encountered. The prevalence
of TS in elderly patients remains unclear, but a standard ofcare (e.g., mammography, echocardiography, and optimalhormone and calcium replacement therapy) must be de-fined, because early medical intervention can reduce mor-bidity and improve life expectancy.
Patricia Alonso-Fernandez, MD, PhDFatima Branas, MD, PhD
Geriatric DepartmentHospital Infanta Leonor
Madrid, Spain
Raquel Fernandez Gonzalez, MDJose Antonio Serra Rexach, MD, PhD
Geriatric DepartmentHospital General Universitario Gregorio Maranon
Madrid, Spain
ACKNOWLEDGMENTS
Conflict of Interest: The editor in chief has reviewed theconflict of interest checklist provided by the authors and hasdetermined that the authors have no financial or any otherkind of personal conflicts with this letter.
Author Contributions: Patricia Alonso-Fernandez andFatima Branas: concept and design, acquisition of subjects,analysis and interpretation of data, and preparation ofmanuscript. Raquel Fernandez Gonzalez: analysis of data.Jose Antonio Serra: acquisition of subjects.
Sponsor’s Role: None.
REFERENCES
1. Stratakis CA, Rennert OM. Turner syndrome: Molecular and cytogenetic, dys-
morphology, endocrine, and other clinical manifestations and their manage-
ment. Endocrinologist 1994;4:442–453.
2. Hook EB, Warburton D. The distribution of chromosomal genotypes associated
with Turner’s syndrome: Livebirth prevalence rates and evidence for diminished
fetal mortality and severity in genotypes associated with structural X abnor-
malities or mosaicism. Hum Genet 1983;64:24–27.
3. Ogata T, Matsuo N. Turner syndrome and female sex chromosome aberrations:
Deduction of the principal factors involved in the development of clinical fea-
tures. Hum Genet 1995;95:607–629.
4. Sybert VP. Cardiovascular malformations and complications in Turner syn-
drome. Pediatrics 1998;101:E11.
5. Lippe B. Turner syndrome. Endocrinol Metab Clin North Am 1991;20:121–152.
6. Gravholt CH, Juul S, Naeraa RW et al. Morbidity in Turner syndrome. J Clin
Epidemiol 1998;51:147–158.
7. Price WH, Clayton JF, Collyer S et al. Mortality ratios, life expectancy, and
causes of death in patients with Turner’s syndrome. J Epidemiol Community
Health 1986;40:97–102.
8. Naeraa RW, Gravholt CH, Hansen J et al. Mortality in Turner syndrome. In:
Albertsson-Wikland K, Ranke MB, eds. Turner Syndrome in a Lifespan
Perspective: Research and Clinical Aspects. Amsterdam: Elservier, 1995, p 323.
THE UNINTENDED OUTCOME OF ASUPPLEMENTAL FORMULARY IN HOMEBOUNDSENIORS
To the Editor: Before January 1, 2006, dual-eligible olderadults in Florida received a comprehensive drug benefitthrough state Medicaid programs. Since that date, all dual-eligible beneficiaries must enroll with a Medicare Part Dprovider. Although 10 classes of drugs (Table 1)1 are ex-cluded from Medicare Part D prescription drug plans, state
Figure 1. Redundant skin at the nape of the neck, shield chest,and hypoplastic and separated breast development.
LETTERS TO THE EDITOR 927JAGS MAY 2009–VOL. 57, NO. 5

Medicaid programs, including Florida, are required to con-tinue to cover many of these medications for their dual-eligible enrollees.2 Nationwide, there are approximately 6million dual-eligible beneficiaries, with 407,000 residing inFlorida.3,4
As part of a quality-improvement project, we studied2,959 persons aged 65 and older who were enrolled in aFlorida Home and Community-Based Medicaid Waiverprogram for dual-eligible, homebound older adults meetingnursing home eligibility. Clients in this program are free tochoose from a variety of Medicare Part D providers. Allclients receive a supplemental pharmacy benefit adminis-tered by a single pharmacy benefit management company.At no cost to the client, the supplemental plan covers ben-zodiazepines, barbiturates, cough and cold agents, quinine,aspirin, acetaminophen, nicotine patch, hemorrhoidcreams, over-the-counter antifungal creams, and variousvitamin and mineral products (B-complex, multivitamin,iron, and folic acid) otherwise excluded under Medicare.
All non-Part D supplemental prescriptions filled duringMarch 2008 and demographic information regarding age,sex, and ethnicity for all clients who received a benzodiaze-pine were analyzed. The care management company pro-vided recent medication profiles of the clients receivingbenzodiazepines.
Two hundred three (6.9%) of the 2,959 clients receiveda total of 241 medications and vitamins through this sup-plemental drug plan. Benzodiazepines accounted for 70.1%of all prescriptions filled. For the 134 clients receiving abenzodiazepine, 95.4% of their prescriptions were refillsrather than a new prescription. The prevalence of ben-zodiazepines was 137 of 2,959 (4.6%). The average age ofthe clients receiving a benzodiazepine was 81.8 � 8.6(range 69–102); there were 22 (16.0%) men and 115(83.9%) women. Seven persons were taking two ben-zodiazepines concurrently. The mean number of medica-tions for each client was 10.5 � 4.7 (range 2–26). Onehundred eleven clients (81.0%) were using other psycho-tropic medications.
Benzodiazepines are excluded from Medicare Part Dformularies purposefully to limit the use of these potentially‘‘dangerous’’ drugs in elderly people, but as describedabove, this population of frail, dual-eligible recipients con-tinues to receive benzodiazepines through a separate sup-plemental pharmacy benefit. Indeed, the main outcome of
the supplemental plan is to provide benzodiazepines. Al-though the diagnostic indications for benzodiazepine usefor these clients were not available, the continual use ofthese drugs in frail homebound older adults remains causefor concern.5 The use of benzodiazepines for longer than 1month is an Assessing Care of Vulnerable Elders indicatorof poor-quality care in vulnerable older adults.6
Under this supplementary formulary program, ben-zodiazepines and other medications excluded from Part Dmay escape all clinically oriented drug utilization review.There is no mechanism for the Part D provider to monitorpatients taking benzodiazepines for potential drug–druginteractions, drug–disease interactions, and duplication oftherapy. The need to coordinate and monitor drug therapyis especially important in a high-risk population, such asours, with the clients on an average of 10.5 medications.
Whether benzodiazepines should be excluded fromMedicaid formularies for seniors or included in Part D planswith clinically based restrictions remains unclear, but thecurrent system of drug coverage for dual-eligible beneficia-ries circumvents thoughtful consideration of this issue.
Adam Golden, MD, MBABernard A. Roos, MD
Geriatric Research, Educationand Clinical Center and Research Service
Miami Veterans Affairs Healthcare SystemMiami, Florida
Division of Gerontology and Geriatric MedicineMiller School of Medicine
University of MiamiMiami, Florida
Bernard A. Roos, MDStein Gerontological Institute
Miami, Florida
Mark H. Beers, MDDivision of Gerontology and Geriatric Medicine
Miller School of MedicineUniversity of Miami
Miami, Florida
ACKNOWLEDGMENTS
Conflict of Interest: The editor in chief has reviewed theconflict of interest checklist provided by the authors and hasdetermined that the authors have no financial or any otherkind of personal conflicts with this letter.
Adam Golden was a paid consultant of American El-dercare Inc. (the Medicaid Waiver program discussed in thisletter).
Author Contributions: Adam G. Golden: study conceptand design, acquisition of data, analysis and interpretationof data, and preparation of manuscript. Bernard A. Roosand Mark H. Beers: study concept and design, analysis andinterpretation of data, and preparation of manuscript.
Sponsor’s Role: American Eldercare, Inc. had no in-volvement in the design of the study, analysis and interpre-tation of the data, writing of the report, or submission ofthis letter for publication.
Table 1. Drugs Excluded from Coverage under MedicarePart D
Agents when used for anorexia, weight loss, or weight gain
Agents when used to promote fertility
Agents when used for cosmetic purposes or hair growth
Agents when used for the symptomatic relief of cough and colds
Prescription vitamins and mineral products, except prenatal vitamins andfluoride preparations
Nonprescription drugs
Outpatient drugs for which the manufacturer seeks, as a condition of sale, torequire the purchase of associated tests or monitoring services exclusivelyfrom the manufacturer or its designee
Barbiturates
Benzodiazepines
928 LETTERS TO THE EDITOR MAY 2009–VOL. 57, NO. 5 JAGS

REFERENCES
1. Medicare Part D. Challenges in Enrolling New Dual-Eligible Beneficiaries.
GAO-07-272 (May 2007). United States Government Accountability Office
[on-line]. Available at http://www.gao.gov/new.items/d07272 Accessed July 25,
2008.
2. Smith DG. Letter to State Medicaid Directors, SMDL #05-002 (June 3, 2005).
Baltimore, MD: DHSS, Centers for Medicare & Medicaid Services, Center for
Medicaid and State Operations [on-line]. Available at http://www.ascp.com/
medicarerx/upload/CMS2MedicaidDirectors.pdf Accessed July 24, 2008.
3. Office of Inspector General. Dual Eligibles’ Transition: Part D Formularies’
Inclusion of Commonly Used Drugs. Department of Health and Human Ser-
vices. Publication #OEI-05-06-0090, January 2006. Available at http://www.
oig.hhs.gov/oei/reports/oei-05-06-00090.pdf Accessed March 22, 2009.
4. Kaiser Commission on Medicaid and the Uninsured. Perspectives on Medicare
Part D and Dual Eligibles: Key Informants’ Views from Three States (May 2007)
[on-line]. Available at http://www.kff.org/kcmv Accessed July 24, 2008.
5. Golden AG, Daiello L, Silverman MA et al. Inappropriate medication pre-
scribing: Going beyond the Beers’ criteria. Long-Term Care Interface
2005;6:31–34.
6. Shrank WH, Polinski JM, Avorn J. Quality indicators for medication use in
vulnerable elders. J Am Geriatr Soc 2007;55:S373–S382.
MEMORY IMPAIRMENT IN ELDERLY PATIENTSWITH DEMENTIA WITH LEWY BODIES: MORETHAN ONE PATTERN?
To the Editor: Dementia with Lewy bodies (DLB) is the sec-ond most common cause of degenerative dementia after Alz-heimer’s disease (AD) and is diagnosed according to clinicalcriteria described previously.1 However, these criteria havesuboptimal sensitivity,1 especially in patients with DLB withhigh burdens of AD lesions, which often coexist;2 neuropsy-chological evaluation has been advocated to help.1,3 Memoryimpairment is usually related to subcortical dysfunction inDLB, contrasting with patients with AD, in whom episodicmemory impairment includes encoding and retrieval defi-cits.4,5 This AD amnestic pattern, named medial temporal,was proposed for the diagnosis of prodromal AD.5 Its fre-quency in DLB has not been studied.
To test the hypothesis that several amnestic patternscould be observed in DLB, given the variability in patho-logical lesions, it was decided to retrospectively analyze theneuropsychological evaluations of 28 consecutive patientswith DLB according to the established criteria. All patientshad clinical examination, blood analysis, brain imaging,and a complete neuropsychological evaluation includingseveral memory subtests. Verbal episodic memory was as-sessed using the Free and Cued Selective Reminding Test(FCRST)6 (adapted from the Grober and Buschke’s test),because it uses semantic cuing, which facilitates retrieval,and controls for an effective registration. During learning,each word is associated with its semantic category. Then,
immediate recall controls that registration occurred. There-after, each free recall is followed by a cued recall for themissing words, three times. Results of the FCRST are ex-pressed as a free recall score, a total recall score, and anindex of sensitivity to cuing. Whereas a low free recall scoredefines amnestic syndrome, sensitivity to semantic cuingdetermines the amnestic pattern. According to previousdata, amnestic patterns were defined as medial temporal(sensitivity to cuing o72%), subcortical (sensitivity to cu-ing 480%), and intermediate (72–80%).4,7
Patients had an average age of 81.3 � 5.0, with symp-toms for 2.3 � 1.1 years and a mean Mini-Mental StateExamination8 score of 23.3 � 4.4 at the time of evaluation.All patients had fluctuations; these were associated withparkinsonism in 14, visual hallucinations in three, and bothin 10. Parkinsonism was present for less than 1 year beforedementia. Neuropsychological findings were in agreementwith previous literature with respect to executive, attention,and visuospatial deficits. All patients had an amnestic syn-drome. The amnestic pattern was medial temporal in 14patients (50%), subcortical in 11 (39%), and intermediatein three (11%) (Table 1).
For the whole group, the preserved sensitivity to se-mantic cuing is in favor of a subcortical pattern, in accor-dance with previous literature,9 but the current studyconfirms for the first time that several amnestic patterns canbe encountered, given the variability of clinical and patho-logical findings. The presence of a medial temporal patternin half of the patients highlights the difficulty of distin-guishing DLB from AD in elderly patients. Although nodefinite diagnosis was available in the patients studied, theresults may suggest interindividual differences in neuro-pathological lesions. The coexistence of cortical Lewy bod-ies and AD lesions is established in DLB.1 Cognitiveimpairment could be correlated with the location and den-sity of Lewy bodies10 but also with AD lesions.11 Twostudies have analyzed the neuropsychological findings inpatients classified as AD, the Lewy body variant of AD(LBV, in which AD lesions are sufficient for a neuropatho-logical diagnosis of AD but with significant presence ofLewy bodies), or DLB according to neuropathological re-sults.3,11 Memory impairment was comparable in the ADand LBV groups, suggesting an important role of AD le-sions. Patients with DLB performed better, but none of thetests permitted the same pattern analysis of episodic verbalmemory as does the FCSRT.11
The results of the current study support the hypothesisthat a medial temporal amnestic syndrome described astypical of AD can be observed in patients with a clinicaldiagnosis of DLB. It may be that these clinically diagnosed
Table 1. Results of the Free and Cued Selective Reminding Test Results, According to Pattern of Memory Impairment
Memory
Impairment
Mini Mental State
Examination (range 0–30)
Free Recall
(range 0–48)
Total Recall
(range 0–48)
Sensitivity to
Cuing (%)
Mean � Standard Error of the Mean
All patients (n 5 28) 23 � 4 11 � 6 36 � 10 68 � 24
Medial temporal (n 5 14) 20 � 4 7 � 4 28 � 8 49 � 18
Subcortical (n 5 11) 25 � 4 16 � 5 45 � 2 90 � 7
Intermediate (n 5 3) 25 � 3 11 � 5 39 � 1 76 � 4
LETTERS TO THE EDITOR 929JAGS MAY 2009–VOL. 57, NO. 5