The Thorax - An Integrated Approach
141
-
Upload
elin-taopan -
Category
Documents
-
view
71 -
download
10
description
surgery
Transcript of The Thorax - An Integrated Approach
-
MCPA I'CAMT
-
THE THORAX
An Integrated Approach
DIANE LEE BSR (Honours), FCAMT
Wh ite Rock, British Columbia, Canada
Copyright 2003 Diane C. Lee Physiotherapist Corporation
ISBN 0-9732363-0-2
-
For my mom-I will always remember for both of us
For my dad and my brother -unconditional love
-
PREFACE, 1ST EDITION
In the literature pertaining to back pain, the musculoskeletal components of the thorax have received little attention. The reference list at the end of this text reRects the paucity of research available for review. And yet, clinicians are presented daily with the challenge of treating both acute and chronic thoracic pain. It was this challenge which initiated the clinical work presented in this text.
A biomechan ical approach to treatment of the thorax requires an understanding of its normal behaviour. Without a working model, the clinician is limited to using unreliable symptoms for direction and treatment planning. If the optimal behavior of the thorax is understood, then this knowledge can be applied to the examination of the painful thorax. A systematic examination of mobility/stability of the associated bones and joints can then be done. Since function is related to structure, an understanding of the anatomy is required.
The clinical investigation began in J 990 when Jan Lowcock presented a paper on stability testing of the thorax to the Canadian Orthopaedic Manipulative Physiotherapists. I am indebted to her, and many others, for the subsequent academic and clinical discussions which lead to the evolution of the biomechanical model presented here. Much of this material remains empirical and requires validation through research.
The First chapter reviews the anatomy of the thorax as it pertains to the biomechanical model. The emphasis has been placed on osseous and articular anatomy although the muscular and neural contribution to function is acknowledged. Chapter two describes the biomechanical model and chapters three to five the clinical application of this model to examination and treatment of the thorax. The purpose of this text is to provide the clinician with the ability to assess and treat articular dysfunction of the thor
-
on human performance. This model was developed in conjunction with Dr. Andry Vleeming (Lee & Vleeming 1998, 2002) and has been applied to the thorax in this edition, the principles of lhis model are described in Chapter 2. Chapter 3, biomechanics of the thorax, has been updated lo include research since the first edition was published.
Chapter 4 has been updated with video clips on a CDROM to demonstrate the aClive and passive mobility and stability techniques previously described in the first edition. In addition, new techniques are presented which analyse the force closure mechanism (dynamic stability) of a thoracic segmenl. The classification of dysfunction within the thorax has been changed to follow the integraled model of function. Chapter 6 has been updated with video clips on a CDROM lo demonstrate the passive and aClive mobilization and manipulation techniques for the thorax.
Chapter 7 is brand new for this edition and contains vital information for an exercise program aimed al stabilization of the thorax. Some of the exercises are illustrated via still photos while olhers can be seen on the CDROM. The information is still empirical since research is lacking in this area and comes primarily from clinical experience. This chapter reviews some of the concepts of load transfer through the body, the analomy and function of the lumbopelvic core (Lee D G, 1999) and the application of lhis protocol {'or stabilization of the thorax. Chapter 7 is written by Linda-Joy Lee (BScPT,FCAMT) and demonstrates her phenomenal ability to integrate concepts from many models. She is a superb clinician, excited by clinical and educational challenges and I thank her for laking on lhis one.
A project such as this does not come together through individual effort and 1 would like to acknowledge the production team whose ideas and guidance have resulted in an educational producl that goes beyond my original intent. Edi Osghian from DV Media Inc. co-ordinated the project and was instrumental in putting it all together, thank you Edi and yes you were righl- a make-up artisl was a greal ideal The still photos were taken by a superb photographer, Goran l3asaric whose attenlion to detail and lighting drove us crazy for two days but in the end - I was impressed with what a little bil of light in the righl place could dol Steve Sara filmed the video clips with a camera that was almost as big as he was. No rewinds or reviews were possible - "trust me, [ got it right" - and he did. And none of the photos or video clips would have been possible without the assistance or our model, Melanie Coffey, Thanks Mel For saying "Sure, J can do that." Little did she know all that we would expect from her. 1 have collaborated on several projects with artist Frank Crymble; and once again he came lo my rescue redrawing the complicated, combined biomechanics of the thorax meeting my demands for visual simplicity, yet accuracy. His patience for my persistence has always impressed me, thank you Frank. And last, but certai n Iy not least, than k you to Lau ra Galloway for design i ng the layoul for a II of th is materia I in such a visually pleasing and easy to read format.
There are many people who have contributed to my educational and personal growth that has ultimately allowed me to give this material to you, the clinician. J would like to acknowledge my heartfelt appreciation to Dr. Andry Vleeming, who challenged me to let go of my biases and see the human experience from a different perspective and to Karen Angelucci, who taught me to explore a different way of living in my own body through exercise in the method of Pilates. As always, I am especially grateful for my family, Tom, Michael and Chelsea who allow me the time, and provide the encouragement, so necessary to continue along lhis path of enquiry.
British Columbia, 2003 D.L.
-
CONTENTS
CHAPTER 1 ANATOMY OF THE THORAX
OSTEOLOGy ....
Vertebromanubrial Region.
Vertebrosternal Region . . .
Vertebrochondral Region
Thoracolumbar Region ...
ARTHROLOGy ................... .
Zygapophyseal Joints . .. . . . . .. . . .. .
Costal Joints .. .................... .
Intervertebral Disc .. .. . . .
MYOLOGY . .. ................................... .
Local System - Classification
Global System - Classification ................ .
Local System - Anatomy ................... .
Global System - Anatomy ................ .
CHAPTER 2
... 13
. ......... 1 4
. ... 1 4
. ... 16
.......... 18
. ......... 20
. ......... 20
. .......... 20
. .... 21
. .... 22
. .... 22
..... 22
. .... 22
. .... 22
. .... 25
PRINCIPLES OF THE INTEGRATED MODEL OF FUNCTION .. . .. 29
INTRODUCTION.
FIRST COMPONENT - FORM CLOSURE .
SECOND COMPONENT - FORCE CLOSURE ................ .
Lumbopelvic Stabilization - The Research Reviewed
The inner unit - Local system - The core ..
The outer unit - The global system - The slings ........... ... . .
THIRD COMPONENT - MOTOR CONTROL .. ... ..................... .
FOURTH COMPONENT - EMOTIONS & AWARENESS
CONCLUSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CHAPTER 3 BIOMECHANICS OF THE THORAX ..
TERMINOLOGY.
LITERATURE REVIEW
. .. 30
. ..... 31
. ..... 32
....... 33
. ..... 33
. ...... 36
. .... 38
....... 38
. ...... 39
. .. .... 41
. . ... ..... ....... 42
.... 42
-
.. CONTENTS
FUNCTIONAL MOVEMENTS
Vertebrosternal Region ......................... .
Flexion ..................... . .
Extension .. . ........... .
Lateral bending
Rotation .... ... .... . . ..
Vertebrochondral Region
Flexion/extension
Lateral bending
Rotation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Vertebromanubrial and Thoracolumbar Region
F lexion/extension .................................................. . .
Lateral bending ... .......... .
Rotation ...
RESPIRATION
SUMMARY
CHAPTER 4 DIAGNOSING THE THORACIC DYSFUNCTION
SUBJECTIVE EXAMINATION
Pain/Dysaesthesia
Sleep ..
Occupation/Leisure activities/Sports
General Information ..................... ............... .
OBJECTIVE EXAMINATION
Postural Analysis .
Functional Movement Tests - Regional Tests
Forward and backward bending .. ................ .
Lateral bending ......................................... .
Axial rotation
Respiration ............................................................... .
Functional Movement Tests - Segmental Tests
Forward bending. . . . . . . . . . . . . . . .
Backward bending
Lateral bending ........... ......... .. .. .... .............. .
Rotation .................... .
Respiration
......... 43
. ........ 43
. ... ... 43
. ....... 46
........ 48
....... 5 1
...... 53
...... 5 4
.... 5 4
..... 55
... 55
. .... 55
. .. 56
............ 56
........... 57
................... 57
........... 59
......... . 60
....... 60
......... 60
. .... ... 60
.... ..... 60
. .......... 60
........... 60
. ....... 60
..... 63
. .... 63
6 4
... 6 4
. ...... 6 4
........ 6 4
. ... 6 4
........ 65
. ........ 66
..67
. . . . . 67
-
Articular Function - Form Closure .... ......... ..... ......................... .
Passive mobility tests of ost.eokinematic function
Passive mobility tests of arthrokinematic function
Zygapophysea/ joints. . . . . . . . .. . . . . . . . ... . .
Costotransverse joints
Lateral translation.
Passive stability t.ests of arthrobnetic function
Vert ical (traction!compression) .................................... .
Anterior translation - spinal
Posterior translation - spinal
Transverse rotation - spinal ........................ ..
Anterior translat ion - posterior costal ............ .............. . .
Anterior/Posterior translation - anterior costal ............... . .
Lat.eral translation. . . . . . .. . . . . . . . .. . . . . .
Neuromyofascial Function - Force Closure and Motor Control
Palpation of the segmental local st.abilizers .
une ann / ................... . . . . . .. . . .. . . . . . ... .
Test for the integrity of the active force closure mechan:isrn
Neural Conduction and Mobility .
Adjunctive Tests ...................................... .
CHAPTER 5 CLASSIFYING THE THORACIC DYSFUNCTION
INTEGRATED MODEL OF FUNCTION CLASSIFICATION
Excessive Articular Compression .. .............................. ..
Excessive Articular Compression with an Underlying Instability
Insufficient Articular Compression. . . . ... . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . .
CHAPTER 6 RESTORING FORM CLOSURE OF THE THORAX
EXCESSIVE ARTICULAR COMPRESSION - STIFF JOINT
Bilateral Restriction of Flexion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Vertebromanubrial regi.on ................................. .
Vertebrosternal/vertebrochondral region
Unilateral Restriction of Flexion .................................. .
Verlebromanubrial region
CONTENTS ..
. ...... 67
... ... 67
. .. .... . 68
. ............. 69
.... 70,71
. .............. 72
........ 73
..73
74
......... 74
. ....... 75
. ....... 76
. ........ 76
. ........ 76
......... 77
. ........ 77
. ........ 77
......... 78
. ........ 78
. ........ 79
......... 81
. . . . . . . . . 83
. . . . . . . . . . 83
......... 83
. ......... 83
.......... 85
. .. .. . . . 86
......... 88
. ...... 88
..... 89
. .... 90
.. 90
-
m CONTENTS
Vertebrosternal/vertebrochondral region
Thoracolumbar region ........ .. . ........ .... .
Bilateral Restriction of Extension
Vertebrornanubrial regiol1
Unilateral Restriction ofExtension
Vertebrornanubrial region. . . . . . .. . . . . . .. .. . .. . . . .. .
Vertebrosternal/vertebrochol1dral region
T horacoluntbar region ......................................... .
Unilateral Restriction of Rotation - Rib .............................. ............................ .
Vertebromanubrial region - restricted anterior rotatiol1 . .. . .
Vertebrol1lanubrial region - restricted posterior rotat iOIl
.......... 90
. ........ 91
......... 91
......... 91
................. 91
. ........ 92
. ......... 92
. ...... 92
. ....... 93
. .... 93
.. ..... 93
Vertebrosternal/vertebrochondral regiol1s ..................................................... . . ...... 9-+
EXCESSIVE ARTICULAR COMPRESSION - COMPRESSED JOINT 94
Unilateral Restriction of Flexion/Right Sideflexion/Right Rotation. . .. . .. ..... 95
Unilateral Restriction of Inspiration . . ...... 96
Unilateral Restriction of Expiration . .. . .. . . . .. ..... ..... .. ... .. .. .. .. . . ... .. .. .. ... . . .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. ..... .. ..... 96
EXCESSIVE COMPRESSION WITH AN UNDERLY ING INSTABILITy .. . . . 96
Fixation ofthe Costotransverse/Costovertebral Joint ............................................ . . ..... 9 7
Vertebro",wl1ubrial region
Vertebrosternal/vertebrochondral region
'n1.oracolumbar region ......................................... .
Fixation of the 'Ring' .................... .
CHAPTER 7 RESTORING FORCE CLOSURE IMOTOR CONTROL
OF THE THORAX . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
INTRODUCTION ................................................... ..
CONCEPTS OF LOAD TRANSFER ........................ . .
Optimal Load Transfer Through the Thorax ................ .
Dysfunctional Load Transfer Through the Thorax
DEVELOPING THE EXERCISE PROGRAM
THE EXERCISE PROGRAM.
Introduction to Stabilization Exercises for the Lumbopelvic Region.
Pelvic floor. . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . .. .. . . . . . .. . . . . . . . . . . . . . . . .. . . . . . . . . . . . . .. . . .. . . ..
Transversus abdo' millis
Deep fibres Of'llIII ltifidlls
Stabilization of the Thorax
Breath.ing ......................... . .
. .. . . .... 9 7
...... 97
. ...... 98
. ...... 99
. ......... 103
.. 10-+
.. 105
.. 105
.. 106
. 10 7
108
..108
. .... 109
..... 109
.111
. . . . . 112
. ... I j 3
-
Neutral spine. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Isolation of the local thoracic segmental stabilizers ................. .
Exercise Progression - Adding the Global Muscles ........................ .
Maintaining neutral spine while adding load
Trunl-arm dissociation. . . .. .. . ... . . .
Trunk-leg dissociation
Moving out: of neutral spine
[niraihoracic .................. ........ .
T horacopelvic ..................... . . . . . . .
Integrated functional bnetic chain
REFERENCES
CONTENTS
. .... 11 4
. .... 120
. ... 124
... 125
. .... 125
..... 129
. 131
. .... 131
. ... 133
... . 134
.... 137
..
-
I
ANATOMY OF
THE THORAX
A biomechanical approach to treatment of the thorax
requires an understanding of its normal behavior.
Without a working model, the clinician is limited to
using unreliable symptoms for direction and treatment
planning. If the optimal behavior of the thorax is
understood, then this knowledge can be applied to the
examination of the painful thorax. A systematic
examination of mobility-stability of the associated bones
and joints can then be done. Since function is related to
structure, an understanding of the anatomy is required.
-
I!I C I I APTER I ANATOMY OF TH E THORAX
INTRODUCT ION
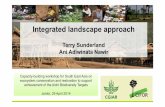
The thorax can be divided into four regions (Fig. ] . 1) according to anatomical and biomechanical difFerences. The vertebromanubrial region (upper thorax) includes the first two thoracic vertebrae, ribs one and two and the manubrium. The vertebrosternal region (middle thorax) includes T3 to T7, the third to seventh ribs and the sternum. T8, T9 and T 10 together with the eighth, ninth and tenth ribs form the vertebrochondral region (middle/lower thorax). The lowest region is the thoracolumbar region which includes the T J J and TI2 vertebrae and the eleventh and twelfth ribs. The regional anatomy pertinent to the biomechanical model will be described in this chapter and comes From the following sources - Cray's
Figure 1.1. Four regions of the thorax - vertebromanubrial, vertebrosternal, vertebrochondral and thoracolumbar.
Anatomy (37th edition), Clinical Anatomy of the Lumbar Spine and Sacrum by likolai Bogduk, Clinical Anatomy and Management of Thoracic Spine Pain (cds. LCF Giles and KP Singer) and Primal Pictu res 3 D J nteractive Series.
OSTEOLOGY
Vertebromanubrial Region The first thoracic vertebra is atypical (Figs. 1.2, 1.3. 1.4). I t has a large, non bifid spinous process, clublike at its end. The superior aspect of the spinous process tends to lie in the same transverse plane as the Tl-2 zygapophyseal joints. The facets on the superior articular processes lie in the coronal body plane while those on the inferior articular process present a gentle curve in both the transverse and sagittal planes. The transverse processes are long and thicle They are located betvveen the superior and inFerior alticular processes at the dorsal aspect of the pedicle and are ideally situated For palpation of intervertebral motion. On the ventral aspect or the transverse process there is a deep, concave Facet which articulates with a convex racet on the first rib to rorm the costotransverse joint. I n the normal upright posture, the orientation of this joint is anteroinrerior.
Figure 1.2. The superior aspect of the first thoracic vertebra. The zygapophyseal joints lie in the coronal plane.
-
Figure 1.3. The inferior aspect of the f irst thoracic vertebra. The zygapophyseal joints are gently convex in both the transverse and sagittal planes. The ventral aspect of the transverse process contains a concave facet for articulation with the first rib.
The superior aspecl of the vertebral body of T] is concave in the coronal plane. This concavity is formed by the uncinate process at each posterolateral corner. These processes articulate with the inferior aspecl of the body of C7 to form the nonsynovial, uncovertebral joint (Hayashi & Yabuki 1985). There are lwo ovoid facets on either side or the vertebral body for articulation with the head of the fll'Sl rib. The inferior aspect of the vertebral body of TI is flat and contains a small facet at each poslerolaleral corner for articulation with the head or the second rib. This articulation is incomplete unlil early adolescence when a secondary ossificalion cenlre appears to complete the formation of the head of the rib (Penning & Wilmink 1987, Williams et aI 1989). In children, the head of the second rib only articulates with T2.
The firsl rib (Fig. 1.5) is the shortest of the twelve and the broadesl at its anterior end. The first sternochondral joinl is unique in that it is fibrous rather lhan synovial. The first costocartilage is
ANATOMY OF THE THOIv\x CHAPTER I
Figure 1.4. Anterolateral view of the f irst thoracic vertebra. The uncinate process at each posterolateral corner creates a concavity on the superior aspect ofthe vertebral body. There is a full facet at the superolateral aspect ofthe vertebral body for the head of the first rib. A demi-facet on the inferolateral aspect articulates with the head of the second rib in the second decade of life. Note the concave facet on the transverse process for articulation with the f irst rib.
the shortesl and lhis, together with the fibrous sternochondral joinl, contributes to the stability of the firsl ring. The convex head of the first rib articulates with the body of T 1 at the costovertebral joint. The neck of the rib is located between the head and the tubercle. The articular portion of the tubercle is convex and directed posterosuperiorly "vhen the head and neck are in l he
Figure 1.5. Superior aspect ofthe first rib.
-
m CIIAPTER I ANATOMY OF THE THORAX
Figure 1.6. The manubrium.
normal upright posture. The second rib is about twice as long as the first and its features are similar to the vertebrosternal region described below. Anteriorly, the cartilage of the second ring articulates with both the manubrium and the sternum at the manubriosternal symphysis.
The manubrium (Fig. 1.6) is a broad triangular sha ped bone which articulates with the clavicle and the costocartilage of the First and second ribs.
Figure 1.7. The manubriostemal symphysis is usually maintained through life, however ossification can occur.
The manubriosternal symphysis remains separate throughout life although ossification can occur (Fig. 1.7).
Vertebrosternal Region The vertebrae in this region (T3 to T7) have long, thin, overlapping spinous processes. The tip of the spinous process can be three finger widths inferior to the transverse process of the same vertebra and frequently deviates from the midline. Consequently, it is an unreliable point for palpating intervertebral motion.
The facets on both the superior and inferior articular processes present a gentle curve in both the transverse and sagitta l planes (Davis 1959, Singer & Goh 2000) (Fig. 1.8). This orientation permits multidirectional movement. If two mixing bowls are placed one inside the other, a model of the zygapophyseal joints can be made (Fig. 1.9). The top bowl can rotate forward, backwa rd, sideways and around the bottom bowl. Translation of the top bowl meets immediate resistance. The coronal orienta tion of the superior articula r processes resists posteroanterior translation of the superior vertebra.
Figure 1.8. The superior aspect of the fourth thoracic vertebra. The zygapophyseal joint is gently convex in both the transverse and sagittal planes. The ventral aspect of the transverse process contains a concave facet for articulation with the fourth rib.
-
Figure 1.9. Two mixing bowls model the potential biomechanics of the zygapophyseal joints in the thorax.
The transverse processes, located at the dorsal aspect or the pedicle between the superior and inferior articular processes, are ideally situated
ANATOMY OF THE THORAX CHAPTER I -
Figure 1.10. Anterolateral view of the fourth thoracic vertebra. Note the concave facet on the transverse process for articulation with the fourth rib as well as the two demi-facets on the lateral aspect of the vertebral body for articulation with the heads of the fourth and fifth ribs.
for palpation of intervertebral joint Illotion. The ventral aspect of the transverse process (Fig. 1.10) contains a deep , concave facet for articulation
Figure 1.11. Posterolateral view of the articulated thorax, vertebrosternal region. Note the curvature of the fifth costotransverse joint (arrow).
-
.. CIIAPTER 1 ANATOMY OFTHE THORAX
Figure 1.12. The fourth rib.
with the rib of the same number. This curvature (Fig. 1. 11) influences the conjunct rotation that occurs when the rib glides in a superoinferior direction (see Chapter 3 - biomechanics). In the normal upright posture, the orientation of the facet on the transverse process is anterolateral.
The posterolateral corners of both the superior and inferior aspects of the vertebral body contain an ovoid demifacet for articulation with the head of the rib. Development of the superior costovertebral joint is delayed until early adolescence (Penning & Wilmink 1987, Wil liams et a1 1989) accounting for the flexibility of the young thorax.
The shaft of the rib is long and thin and twists to a variable degree at the posterior angle (Fig. 1. 12) .
Tl1e sternum (Figs. 1.7, 1. 13) has eight full concave facets which articulate with the costocartilages
Figure 1.13. The sternum.
of ribs three to six. Superiorly, the second rib articulates with the sternum at a demi-facet; inferiorly, the seventh rib articulates with both the xiphoid and the sternum.
Vertebrochondral Region The vertebrae in this region (Fig. 1. 14) (T8, 9, 10) differ from the vertebrosternal region in the following aspects. The spinous process is shorter, although still c1irected inferiorly such that the tip lies close to the transverse plane of the transverse process of the inferior vertebra. The facet on the ventral aspect of the transverse process is flat and faces anterolateral and superior (Fig. 1. 15) . Therefore, when the tubercle of the rib glides superiorly, it also glides posteromeclially with minimal conjunct rotation. When the tubercle of the rib glides inferiorly, it also glides anterolaterall y following the plane of the costotrans-
-
Figure 1.14. Anterolateral view of the eighth thoracic vertebra. Note the planar facet on the transverse process for articulation with the eighth rib as well as the large superior demi-facet for articulation with the head of the eighth rib and the small demifacet for articulation with the head of the ninth rib.
Figure 1.16. Anterior view of the articulated thorax.
ANATOMY OF THE THORAX C I IAPTER I
Figure 1.15. Posterolateral view of the articulated thorax, vertebrochondral region. Note the planar nature ofthe ninth costotransverse joint (arrow).
verse joint (see Chapter 3 - biomechanics) . The orientation of the facet for the costotransverse joint changes to accommodate greater loading from the upper limb and thorax (Ciles & Singer 2000). At T2, the facet on the transverse process faces anteroinferiorly when the thorax is viewed in a normal upright posture. At TlO, the facet on the transverse process faces superolaterally such that the rib rests on top of the transverse process.
T8 and T9 have four demiFacets for articulation with the head of the eighth and ninth ribs. TlO is variable. Often, there is onl y a small articulation between the superior aspect of the head of the tenth rib and the inferior aspect of the vertebral body ofT9. Occasional ly, the tenth rib will articulate only with TIO at the base of the pedicle via an unmodified ovoid joint.
Anteriorly, the eighth, ninth and tenth ribs articulate indirectly with the sternum via a series of cartilaginous bars which blend with the seventh costocarlilage (Fig. 1. 16). There are a variable number of synovial joints between the costocartilages (interchondral joints) . This arrangement permits greater flexibility.
-
m CHAPTER I ANATOMY OF THE THORAX
Figure 1.17. The eleventh and twelfth thoracic and the first lumbar vertebrae. Note the orientation ofthe zygapophyseal joints.
Figure 1.18. Lateral view of the twelfth thoracic vertebra. Note the change in direction of the facets on the superior and inferior articular processes. There is one facet on the lateral aspect of the vertebral body for articulation with the head of the twelfth rib. There is no facet on the small transverse process, there is no costotransverse joint.
Figure 1.19. The transverse processes of the twelfth thoracic vertebrae are small tubercles (arrow) and cannot be used for palpating inteNertebral motion.
Thoracolumbar Region The spinous processes ofT! 1 and TI2 are short, stout and contained entirely within the lamina of their own vertebra (Figs. 1.17). The facets on the articular processes of TIl (Fig. 1. j 8) resemble those of both the vertebrosternal and vertebrochondral regions. The facets on the inferior articular process of T12 resemble the lumbar region. They have a coronal and sagittal component and when articulated with Ll restrict axial rotation. The orientation of TIl-12 does not restrict axial rotation.
Laterally, the transverse processes are small tubercles (Fig. 1.19), the mamillary processes are larger and more superficial. The spinous process is a more reliable point for palpating intervertebral motion in this region.
The heads of the eleventh and twelfth ribs articulate only with the vertebral body at the base of the pedicle via an unmodified ovoid joint (Fig. 1.20). There is no costotransverse joint in this region. The ribs do not have a neck and do not twist significantly. They remain detached from the rest of the thorax anteriorly (Fig. 1.21) and provide attachment for the diaphragm and trunk musculature. The shape of the costovertebral joint facilitates multi-directional movement of the vertebral body even when the large muscles contract and fix the eleventh and twelfth ribs. The eleventh segment (TIl, T12, eleventh rib) is the most flexible in the thorax.
ARTHROLOGY
Zygapophyseal Joints The zygapophyseal joints of the thorax are synovial and, like other synovial joints, contain small intraarticular folds comprised of fibrous or fibro-fatty tissue (Giles & Singer 2000). These folds originate medially from within the joint space and extend a variable distance into the joint cavity. The capsule
-
or the zygapophysea I joi nt is su pported by the I igamentum Aavum medially and the rotatores muscle laterally (Bogduk 1997), the deepest fibers of this muscle insert into the capsule.
Costa/Joints The costotransverse joints are synovial and also contain small intra-articular Folds (Giles & Singer 2000). 1l1e lateral costotransverse ligament SUPPOltS the lateral aspect of the joint and is transversely oriented (Fig. 1.22). It attaches to the tip or the transverse process and inserts into the non-articular portion of the tubercle of the rib. The superior
Figure 1.20. Lateral view of the thoracic spine. Note the unmodified ovoid facet (arrow) for the head of the twelfth rib.
ANATOMY OF TH E THORAX CHAPTER I EI
costotransverse ligament has a variable number of bands that run in a superoinFerior direction from the inferior aspect of the transverse process to the neck of the rib below. The neurovascular elements of the thoracic segment emerge between the bands of this ligament.
The second to tenth costovertebral joints are divided into two synovial cavities, each cavity is separated by an intra-articular ligament. The capsule is supported by the radiate ligament (Fig. 1.23) which has fibres extending from the head of the rib both anteriorly and posteriorly to blend with the vertebral body of the level above, the intervertebral disc and the vertebral body of the level below. The costotransverse ligament connects the neck of the rib to the ventral aspect of the adjacent transverse process. The first, eleventh and twelth costovertebral joints contain a single Facet located at the base of the ped icle. They are essentially unmodified ovoid in shape.
Figure 1.21. Posterior view of the articulated thorax, thoracolumbar region. Occasionally the spinous processes are bifid.
-
m CHAPTER 1 ANATOMY OF THE THORAX
Figure 1.22. The ligaments of the posterior aspect of the thorax. LC= lateral costotransverse ligament SC=superior costotransverse ligament (Reproduced with permission from Primal Pictures).
With the exception of the first, the sternocostal joints are synovial, unlike the lateral costochondral joints which are fibrous, the periosteum and perichondrium continuous.
Intervertebral Disc The intervertebral discs of the thoracic spine are narrower than those in the cervical and lumbar regions and constitute approximatel y one-sixth of the length of the thoracic vertebral column. Since the ratio of the height of the disc to the vertebral body is 1:5, motion bet\,yeen the segments of the thorax is small. There is a linear increase in the cross-sectional area of the disc in the lower thorax reflecting an increase in the weight bearing function of these levels.
Figure 1.23. The costovertebral joint and the ligaments of the anterior aspect of the thoracic spine. RL=radiate ligament (Reproduced with permission from Primal Pictures).
MYOLOGY
The muscl es of the thorax can be divided into deep and superficial layers. Functionally, these muscles can be classified into two systems; the local and the global (Bergmark ]989, Richardson et al 1999).
Local System - Classification Functionally, stability is maintained via low force continuous activity of the local musculature. These muscles work in all positions of the joint and during alJ directions of joint molion. This activity increases the stiffness at a segmental level and helps to control excessive physiological and translational motion, especiall y in the neulral joint position where passive support from the ligaments and capsule is minimal. The activity of the local system often increases in anticipalion of impending load or motion, thus proviclingjoint
-
Figure 1.24. The local stabilizers ofthe thorax include the rotatores (R), levator costarum brevis (LCB) and longus (LCL) and the deep fibers of multifidus (M). (Reproduced with permission from Primal Pictures).
protection and supp0l1 (80 & Stein 1994, Comerford & iVlottram 200 I , I lodges et al 1997b, Richardson el al 1999).
Global System - Classification The primary role of the global system is to generate lorque and provide control of inner and outer range o[joinl motion. These muscles are required to concenlrically shorten into the full physiological inner range position, isometrically hold this position as well as eccentricall y control or decelerate loads against gravity (Comerford & Mottram 200 I, Richardson et al 1999). They are necessary for stability under conditions of high load.
I n general , the deeper layers of the spinal muscul ature arc segmental and are thought to play a significant role in local stabilization of the spine (Bergmark 1989, Hides et ai, 199-+ Moseley et al 2002). The superficial muscles of the thorax tend lo span sevcral segments/ribs and function to move the thorax '"Clalive to the lumbar spinc and
ANATOMYOF THETI-IORAX CHAPTER I IJII
Figure 1.25. The intercostals are classified as local stabilizers while spinal us (5), longissimus thoracis (LT) and iliocostalis thoracis (IT) are global muscles. (Reproduced with permission from Primal Pictures).
pelvis and therefore function globally. Co-activation of diFFerent muscle groups results in flexion, extension, lateral bending and axial rotation of the thorax.
Local System - Anatomy SpeCiFically, the local muscles which stabilize the thorax are thought to include the rotatores thoracis, the deep Fibers of multiFidus, the levator costar-um breves and longus and the internal and external intercostal muscles. The rotatores thoracis and multiFidus are part of the transversospinalis group. The research has yet to be done to confirm the inclusion of these muscles into this cl assification, they are here based on clinical impression and extrapolation From research done in the lumbar spine and pelvis.
The cleven pairs of rotatores thoracis (Fig. 1.24 ) arise from the inFerior border and lateral surface of the lamina of the thoracic vertebra and run inferolaterally to insert onto the superoposterior
-
III C I I APTER l ANATOMY OF TH E THORAX
Figure 1.26. The global stabilizers and mobilizers of the thorax connect the thorax to the pelvic girdle and function to control sagittal and transverse plane motion. (Reproduced with permission from DeRosa & Porterfeld 2001.)
aspect of the base of the transverse process of the subjacent segment. These muscle Fibers attach to the capsule of the zygapophyseal joint.
The multifidus muscle (Fig. 1.24) overlies the rotatores thoracis and fills the gutter between the spinous processes and the base of the transverse processes. The deepest layers arise from the lateral aspect of the spinous process and pass inferolaterally to attach to the base of the transverse process. The deep Fibers are segmental whereas the more
superfical fibers span two to four vertebral segments before attaching. I n the lumbar spine, these superficial fibers are known (Moseley et al 2002, Richardson et al 1999) to be phasic in [unction (responsible For angular motion) whereas the deep Fibers have a more tonic function (are non-direction specific and responsible for stabilization) . The research is still lacking for the thorax - however the clinical impression is that the Function is similar. All fascicles arising from the spinous process of a given vertebra are innervated by the medial branch of the dorsal ramus of that segment (Bogduk 1997) regardless of the length or depth of the muscle.
The levator costarum breves (Fig. 1.24) are found from C7 to T J J and arise from the tip of the transverse process. The short fibers pass inferolaterally to insert onto the subjacent rib between the tubercle and the angle. The levator costarum longus is comprised of four muscular slips which arise from the transverse processes oFT7, T8, T9 and Tl 0 (vertebrochondral region only) . The fibers are longer than those of levator costarum breves and pass inferolaterally to insert between the tubercle and angle or the rib two segments below their origin.
The intercostal muscles (internal and external) (Fig. 1.25) fill the gap between the ribs and although their action is facilitated with expiration and inspiration respectively, their main function is to stiffen the chest wall during respiration. In this regard, they are non-direction specific thus meeti ng the criteria for bei ng loca I sta bi I i7.ers. The internal intercostal muscle lies deep to the external intercostal muscle and arises From the subcostal groove and costal cartilage and passes inferolateral anteriorly and inferomedial posteriorly. The external intercostal muscle arises From the lower border or the rib passing inrerolateral posteriorly and inferomedial anteriorly until the costochondral joint beyond which it continues to attach to the sternum as the external intercostal membrane.
-
Global System - Anatomy The global muscles of the thorax (Fig. 1.26) include the external and internal oblique abdominals, semispinalis thoracis, erector spinae , rectus abdominis and possibly the upper fibers of transverses abdominis. All of these muscles generate torque and function to control direction specific movements. The obi iq ue a bdom ina Is con tro I rotation of the thorax relative to the lumbar spine and pelvic girdle concentrically, isometrically and eccentrica lly.
The external oblique is the largest and most superficial abdominal with eight digitations arising from the external surfaces and inFerior borders of the lower eight ribs. This origin interdigitates with fibers of serratus anterior and latissimus dorsi. The upper attachments of the external oblique arise close to the costochondral joints, the middle attachments to the body of the ribs and the lowest to the tip of the cartilage of the 12th rib. Inferiorly, the posterior fibers descend vertically to attach to the outer lip of the anterior J /2 o[ the iliac crest. The upper and middle fibers end in the anterior abdominal aponeurosis (Fig. J .27) . Rizk (1980) investigated this structure in 41 specimens and discovered that the aponeurosis of the external oblique was bilaminar. The two layers cross the midline to blend with the fascia of the opposite side with the deep layer being continuous with the contralateral internal oblique. The superficial layer merges with the superficial layer of the contralateral side. The deep and superficial layers produce a cross hatched appearance as their orientation is 90 to one another.
The internal oblique lies between the external oblique and the transversus abdominis and arises from the lateral 2/3 of the inguinal ligament, anterior 2/3 of the intermediate line of the iliac crest and the lateral raphe of the thoracodorsal fascia. The posterior fibers ascend laterally to reach the tips of the 11 th and 12th ribs and the J Oth rib ncar the costochondral junction. The
ANATOMY OF TH E THORAX CHAPTER I 111
anterior fibers arising from the inguinal ligament arch inferomedially to blend with the aponeurosis of transversus abdominis and aLlach to the pubic crest. The intermediate fibers pass superomedially to insert into a bilaminar aponeurosis (H.izk 1980) blending with the aponeurosis of the external oblique forming a decussating network of fascia across the midline of the body.
Semispinalis thoracis is part of the transversospinalis group and is superficial to multifidus and deep to spinalis thoracis (part of the erector spinae group). It arises from tendinous slips [Tom the transverse processes of T6 - TI 0 and inserts cranially into the l ateral aspect of the spinous processes of C6-T4.
Spinalis thoracis (Fig. 1.25) (medial part of the erector spinae group) lies medial to the thoracic component of longissimus thoracis (Fig. 1.25) and posterior to the thoracic component of sem ispinalis. Tt arises From the lateral aspect of the spinous process from TII-L2. From these 4 slips it forms a small muscle which inserts cranially into the lateral aspect of the spinous process of Tl-T8.
The thoracic component of longissimus thoracis (Fig. J .25) is the largest part of the erector spinae group in the thoracic spine and forms the bulk of the paravertebral muscle mass adjacent to the spine. It arises from the ribs and transverse processes ofTI - T12 and descends to attach via the aponeurosis of the erector spinae to the spinous processes of the lumbar spine and sacrum. Each fascicle descends a variable length with those from the upper thorax reaching to L3 while the lower fascicles bridge the lumbar spine completely.
Iliocostalis thoracis (Fig. 1.25) (lateral part of the erector spinae) lies lateral to longissimus and medial to the thoracic component of iliocostalis lumborum. It arises from the superior border of
-
m C I IAPTER 1 ANATOMY OF TH E THO RAX
Figure 1.27. The anterior fibers of the external oblique muscle insert into the abdominal fascia strongly connecting to the interdigitations separating the rectus abdominis. (Reproduced with permission from DeRosa & Porterfield 2001).
the angle 0 [" ribs seven to twelve inserting inlo the superior border of the angle of ribs one to six and lhe transverse process of C7. This Illuscle is conlained enlirely within the thorax.
The thoracic component of iliocoslalis lumborum (Bogduk 1997) is large and the Illost laleral part of the ereclor spinae Illuscle group. Fascicles from lhe inferior borders or the a ngles or the l ower seven to eighl ribs originate lateral to the attachmenl o[ iliocoslalis thoracis and descend to auach to the i l ium a nd sacrulll with the l horacic
Figure 1.28. Transversus abdominis. (Reproduced with permission from DeRosa & Porterfield 2001).
cOIllPonent of the longissimus thoracis lo form the aponeurosis of ereclor spinae. These thoracic fascicles have no altachlllenl to the lumbar vertebra bridging the gap between the thorax and the pelvis. Since the thoracic component of iliocoslalis lumborum lies lateral lo the axis of spinal rOlalion and the distance between the rib cage and lhe pelvis is greatly increased during conlra laleral rotation, Bogduk ( 1997) suggests that this muscle can serve to derotale the thoracic cage and thus could also qualify as a global muscle [or this region.
-
l iectus abdominis (Fig. 1.27) lies posterior to the anterior abdominal Fascia separated from its counterpart by the linea alba. I L is divided by three tendinous intersections which are connected to the external oblique laterally ( Deliosa 200 J ) . It arises From the f- irth to seventh ribs and the xyphoid process and descends to attach to the pubic crest and tubercle.
Transversus abdominis (Fig. J .28) is the deepest abdominal and arises from the lateral 1/3 of the inguinal l igament, the anterior 2/3 of the inner l ip or the iliac crest, the lateral raphe of the thoracodorsal Fasc ia and the internal aspect of the lower six cost al cartilages interdigitating with the costal fibers or the diaphragm. From this broad attachment, the muscle runs transversely around the trunk where its upper and middle fibres blend with the fascial envelope or the rectus abdominis reaching the linea alba in the midline. Inferiorly, the muscle blends with the insertion of the internal oblique musc le to reach the pubic c rest. The lower fibers of transversus abdominis are known (H odges et al J 997a,b) to locally stabil ize the lumbopelvic region. U rquhart et al (200 1 ) noted that t he upper and middle Fibers of transverses abdominis lend to be more direction specific with respect to rotation or the thorax. I t is possible that these fibers are part of the global system.
ANATOMY OF TH E THORAX CHAPTER I III
-
The Integrated Model of Function
FUNCTION
P
-
2
PRINCIPLES OF
THE INTEGRATED
MODEL OF
FUNCTION
The following text is taken in part from material
jointly written by the author and Dr. Andry Vleeming
(Lee & Vleeming 2002). The integrated model of
function was developed from scientific and
clinical studies on the anatomy and function
of the lumbopelvic region and has been adapted
for the thorax by D GLee.
-
m CIIAPTER 2 PRINCIPLES OFTHE INTEGRATED MODEL OF FUNCTION
INTRO DUCTION
Scientific research has led to the dcvelopment of models that enha nce our knowledge, facilitate communication and foster a unified approach to futurc rcsca rch. The in ten t ion of thc biomecha nical model presen ted in the f-irst edition of this tcxt was to focus on how the joi nts of the thorax behaved normally and how dysfunction could be assessed and treated to alJeviate symptoms. Whilc t his model did a d d ress t he a rticu l a r componcnt of the patient 's problem, it has become cvident that two other factors can have an equal impact on rccovery. These components are neuromyofascial and emotional.
The integratcd model (Fig. 2 . 1) has four components - three tha t are physical
form closure (structure),
force closure (forces produced by myofascial action) and
motor con t ro l (specific timing of muscle act ion/i naction d u ri ng load i ng)
and onc that is psychological
emotions.
The proposal is that join t mechanics can be inAuenced by multiple factors (articular, neuromuscular and cmotional) and that management requires atten tion to all.
Living on earth requires a constant response to gravity. Our upright posture requires that the gravitational force be t ransferred through thc thorax, low back, and pelvis to the legs. How well this load is transferred over a lifetime, dictates how efficient function will be. Impairmcnt implies that the individual has lost the ability to perform and this loss is usually associated with symptoms significant enough to motivate them to seek help. Thoracic impairment , therefore, can be dcfined as an inability to perform due to problems within the thorax. This impairment may be neuromus-
culoskcletal in naturc or due to thc thoracic \nsccra.
According to Panjabi ( J 992) stabi I ity is achicvcd when thc passivc, activc and control systcms work togcther. Vlccming ct al (l99 0a ,b) believc that the passive, activc and cont rol systems produce approximation of' thc joint surfaccs; essential if stability is to bc insurcd. The amount of approximation required is variable and difficult to quantify since i t is cssentially dependent on an individual's structure (form closurc) and the forces they need to control (force closure). The term "adequate" (Lee & Vlecming J 998) has been used to describc how much approximation is necessary and rcflects t he non-qua ntitative aspect of this mcasure . Essentially, it mcans "not too much" and "not too li ttle", in other words just enough to suil thc existing situation. Consequently, the ability to effectively transfer load through the thorax is dynamic and depends on:
1. optimal function of the boncs, join ts and ligamcnts (form closure or joint congruency)
2. optimal function of the musc lcs and f'ascia (forcc closure)
3. appropriate neural Function (motor control, emotional state)
For every individual, there a re ma ny st rategies available to achievc stability. These are based on
The Integrated Model of Function
t7 FUNCTION
tJ
Figure 2.1. The integrated model offunction - Lee & Vleeming 2002.
-
PHINCIPLES OFTHE INTEGHATED MODEL OF FUNCTION CHAPTEH 2 ..
the individual's anatomicallbiomechanical factors (i.e. connective tissue extensibility, muscle strength , body weight, joint su rface shape, motor control patterns), psychosocial Factors and the loads t hey need to cont rol.
Stability is not only about how much a joint is moving (quantity of motion) o r how resistant structu res are that restrict it, but abou t motion control which allows load to be transferred smoothly. When mot ion control is inadequate, t he re may be too much , or too little, approximation of t he joint su rFaces. Too much compression over a long period of time will wear out t he joint s and can lead to osteoarthritis. Too litt l e compression leads to episodes of giving way and coll apse. E ach component of the integrated model contributes to functional stability.
FI RST COM paN ENT -FORM CLOSURE
This term was coined by Vleeming & Snijders (Vleeming et aI 1990a,b, Snijders et al 1993) and is used to describe how t he joint's structu re, orien ta t ion and shape cont ribu te to s tabilit y. All joints have a variable amount of form closure and the individual's inherent anatomy will dictate how much additional Force is needed to ensure s tabilization when loads are increased. The "form" of the thorax (the bones, joints and ligaments) has been described in detail in Chapter 1.
The thorax transfers large loads, generated primarily from the upper extremity, and its overall shape is well adapted to t his task. This is mainly due to the rib cage and the effec t i t has on motion of the spinal segments. Andriacchi et al (1974) noted that the rib cage increased the bending s tiffness of the spine by a factor of two in extension. He fou nd that when t he rib cage was left intact , the spine could support t h ree t imes the load in com-
pression before lateral instability occurred. Form closu re of the t horax, t herefore, depends on an in tact rib cage.
There have been few in vivo s tudies of t horacic spin al motion a n d most of the biomechanics described in this text a re a clinical extrapolation from Panjabi, Brand and White's in vitro inves tigation ( 1976) of t he t horacic spine (see Chapter 3). Th i s research addressed t he q uestion how much does the thoracic spinal segment move and which motions are coupled? The answer -it moves a lit tle bit and is always coupled. Since t his s tudy was published, Willems et al ( 1996) investigated in vivo the direction of motion coupling and found it to be consistent for flexion/extension and variable for lateral bending and rotation. They fou n d this to be true th roughout alJ four regions of the thorax.
To date, no manual diagnost ic tests have shown inter-tester reliability for determining how much the joints of the vertebral column and/or pelvis are moving i n e i t he r symptomatic or asymptomatic subjects (Carmichael 1987, Dreyfuss et al 1994, Dreyfuss et al 1996, Herzog et al 1989, Laslet t & Williams 1994). Given the wide individual variation and the limited potential range of motion, i t is no wonder we have not been able to demonstrate reliabil i ty wit h manual testing when amplit ude is considered. And yet, how can a diagnosis of hypomobility or hypermobi l ity/instab ility be made wit hout clinically reliable passive mot ion tests of mobility? Subsequent research has helped to clarify t his dilemma.
Buyruk et al (1995a) established that t he Ec ho Dopple r could be u sed to measure s tiffness of the Sl]. Subsequent research (Buyruk et al 1995b, 1997, 1999) u sing t his methodology on subjects wit h and wi thout pelvic pain, revealed the h igh degree of individual variance in t h e s tiffness of the SI] . Wit hin the same subject, t he asymptomatic individual demonst ra ted similar values for both SI]s, whereas t he symptomatic individual
-
.. CHAPTER 2 PRINCIPLES OFTHE INTEGRATED IVlODELOF FUNCTION
demonst rated diFferent stiffness values For the left a nd right Sl]. In other words, asymmetry of stiFfness correlated with the symptomatic individ u al . Cli n i c a lly, there appears to be a wide variation in the amount of resistance or stiFfness within the thorax both between individuals of the same age and also within the same individu al as a result of i ncreasing age. In keeping with this research , the emphasis of manual motion testing should Focus less on how much a joint is moving and more on the symmetry, or asymmetry of t he motion palpated. A clinical reasoning approach which considers all of the Fi ndings from the examination is required to determine if the amplitude of motion is less, or more, than optimal for that individual.
Form closure ana lysis requ i res an eval uation of both the neutral zone and elastic zone of motion (Fig. 2.2 ) (Panjabi 1992). The neutral zone is a small range of movement near the joint's neutral position where minimal res istance is given by the osteol igamentou s structures. The clastic zone is the part of the motion I' Tom the end of the neutral zone up to the joint's physiological limit.
Panjabi ( 1 992) fou nd that the size of the neutral zone increased with i nju ry, a rtic ular degeneration and/or weakness of the stabilizing muscula-
. ' .
Load
. .
.
. .
. .
R2 .'
..
'
. .
. . o R1
Range of motion
Panjabi 1992
Elastic zone
Displacement
Figure 2.2. The zones of articular motion - the neutral zone (O-R1) and the elastic zone (R1-R2) (Panjabi 1992).
tu re and that t h i s was a more sensitive indicator than angular range of motion for detecting instability. Lee & Vleeming ( 1998) suggest that the neutral zone is not only a ffected quantitatively, but also qualitatively when compression is applied (or reduced) across the joint. This compression can a Ffect the stiFfness of the neutral zone of motion . To explain this fu rther we need to understand what compresses the thorax, in other words what p rovides force closu re.
SECON D COM PONENTFORCE CLOSURE
]J the artic ular su rfaces 01' the thorax were consta ntly a n d completely compressed, mobil ity would not be possible. I l0wever, compression du ring loading is variable and thereFore motion is possible and stabilization req uired. This is ac hieved by increasing compression across the jo i nt su rFace at the moment of loading - force closure (Vleeming et al 1990, Snijders et al 1993). The anatomical structu res responsible for th i s a rc the ligaments, muscles and fascia . Several ligaments, muscles and fascial systems contribute to Corce closure of the thorax. When working el'F i cien tly, the shear Forces between the vertebrae and ribs are adequately controlled and loads can be t ran s ferred between the tru n k, pelvis a rms and legs.
Pa njabi et al (J 981) tested the stability of the thoracic spinal unit by loading it to failure in both flexion a n d exte nsion . Fail u re was defined as complete separation of the two vertebrae or more than 10 mm of translation or 45 degrees or rotation. The ligaments were then cut sequentially and the contribution of the various ligaments to stability was noted. In flexion , they fou nd that the u nit remained stable until the costovertebral joint was cut. The integrity of the posterior one-third of the disc and the costovertebral joints is c ritical to anterior tra nslation stability in the thorax.
-
PRINCIPLES OF T HE INTEGRATED MODEL OF FUNCTION CHAPTER 2
Panjabi et al ( 198 1) then sequentially cut t h e an terior longit udinal ligament, the anterior half of the intervertebral disc, the costovertebral joints and the posterior half of the intervertebral disc and noted t he contribu tion of each to stability in extension. In extension, t hey found t ha t t he unit remained stable u ntil the posterior longitudinal ligament was cut. All of the ligaments anterior to and including the posterior longitudinal ligament limit extension of the thoracic spinal uni t .
Wi th respect to the neuromyofascial system, stabilization of the t horax requires both segmental ( Ioca I) and globa I control. Segmentally, t he local muscles (deep fibers of mul ti fid us, rotatores breves, levator costarum and t he intercostals) are important. Globally, t he thorax is part of a larger system whose stabilization begins with t he lumbopelvic core. To understand t he exercise program in Chapter 7 it is essential to review how stability is ach ieved in the entire trunk and the research that has led to the proposals presented later in this text for stabilization of the thorax.
Lumbopelvic Stabilization -The Research Reviewed There are two important groups of muscles that contribute to stability of the trunk. Collectively they have been called t he inner unit (Richardson et al 1999) or local system (Bergmark 1989, Comerford & Mottram 200 1)) and t he outer unit (R.ichardson et al 1999) or global system (Bergmark J989, Comerford & Mottram 200 1 ). The local stabilizers of t he lumbopelvic region consist of the muscles of the pelvic floor, the transversus abdominis, t he deep fibers of m ul t i fidus, t he diaphragm and possibly t he posterior fibers of psoas (Gibbons 2002). The outer unit or global system consists of several slings or systems of muscles t hat are anatomically connected and fu nctionally related (Meyers 200 1, Vleeming e t a l 1995b).
The Inner Unit - Local System -The Core The function of the local muscles is t o apply adequa te compression such tha t t h e system is stabilized in preparation for t he addition of external loads. Research h as shown (Bo & Stein 1994, Constantinou & Govan 1982, Hodges 1997b, Hodges & Gandevia 2000, Sapsford et al 200 1) tha t the local muscle system is anticipatory when fu nct io n ing opt imally. In o ther words , t hese muscles work at low levels at all times and increase their action before any further loading or motion occurs.
Hodges & Richardson ( 1996, 1997a) have shown t ha t t ransversus abdominis is an anticipa tory muscle for stabilization of the low back and pelvis. Although i t doesn't directly cross t he SIJ, it h as an impact on compression of the pelvis (Richardson et al 2002) t hrough, in part, its direct pull on t he large attachment to the middle layer and the deep lamina of the posterior layer of the thoracodorsal fascia (TDF) (Barker & Briggs 1999, Vleeming e t al 1995a) (Fig. 2. 3a,b). As an anticipatory m uscle, it is recruited prior to t he initiation of any movement of the upper or lower extremity (Hodges & Richardson 1996).
I n a study of patients with chronic low back pain, a timing delay was found in which t ransversus abdominis failed to anticipate t he initiation of arm and/or leg motion ( Hodges & R.ichardson 1997a). Delayed activation of transversus abdominis means t h a t t h e TOF is not pretensed and t he pelvis is therefore not compressed in preparation for external loading. Therefore, it is potentially vulnerable to t he loss of intr insic s tabilization.
M ul tifidus also plays a crucial role i n stabilization of t he pelvic girdle. This muscle is contained between the lamina of t he vertebrae/dorsal aspect of the sacrum and t he deep layers of the t horacodorsal fascia. W hen it contracts, it broadens and therefore increases the tension of t he t hora-
-
III CIIAPTER 2 PRINCIPLES OFTHE INTECRATED MODEL OF FUNCTI ON
Figure 2.3Q. The superficial fibers of the thoracodorsal fascia bridge the pelvis connecting the latissimus dorsi and the gluteus maximus muscles. (Reproduced with permission from Andry Vleeming).
codorsal fascia (Fig. 2.4a,b). This creates a "pumping up" (hydraulic amplification) (Gracovetsky 1990, Vleeming et al 1995a) effect which tenses the thoracodorsal fascia and therefore compresses the posterior pelvis (Richardson et aI 2002).
The Echo Dopple r has been used to measure stiFFness, or compression, of the S I ] under valying conditions (13uyruk et al1995a,b, 1997 , 1999). I ecently, the impact of the activation of the local muscle system on compression of the S I J has been studied (Richardson et aI2002). The results of this research supports what is clinically noted in well trained individuals, that is - co-activation of transversus abdominis and multifidus increases
Figure 2.3b. The deep fibers of the thoracodorsal fascia form a roof over the sacral multifidus and directly connect the sacrotuberous ligament to the aponeurosis of the erector spinae muscle. (Reproduced with permission from Andry Vleeming).
the stiFfness of the S I J, facilitating the Force closure mechanism of the pelvis. Further study is necessary to analyze which other muscles co-contract besides the multifidus and transversus abdominis and influence compression of the S I J.
Hides et al ( 1994), O'Sullivan (2000) and Danneels et al (2000) have studied the response of multifidus in low back and pelvic pain patients and note that multifidus becomes inhibited and reduced in size in these individuals. The normal " pumpup" effect of multifidus on the TDF, and thereFore its ability to compress the pelvis posteriorly, is lost when the size or Function of this muscle is impaired. Rehabilitation requires both retraining
-
PRINCIPLES OF THE iNTEGRATED MODEL OF FUNCTiON CHAPTER 2 m
(Hides et al 1996, O'Sull ivan et al 1997) and hypertrophy or the muscle ( Danneels et al 2001) for the restoration or proper Force closure of the lumbopelvic region. Together, multifidus and transversus abdominis form a corset of support For the lumbopelvic region. The "roof and Aoor' of t h is cannister are supported by the muscles of the pe lvic Aoor and the respiratory diaph ragm.
The muscles or the pelvic Aoor play a critical role in both stabil ization of the pelvic girdle as well as urinary and fecal continence (Ashton-Miller et al 200 1 , 130 & Ste in 1 994, Constantinou & Govan 1982, SapsFord et al 200 1). Contstantinou & Govan (] 982) measured the intra-urethral and intra-bladder p ressures in healthy continent women during coughing and valsalva (bearing down) and found that during a cough the intraurethral pressure increases approximately 250ms before any pressure increase is detected in the bladder. This suggests an anticipatory reflex. The increase in urethral pressure occurred s imultaneously with the increase in bladder p ressu re during a valsalva. They suggest the d ifference may be due to the role of the pelvic Aoor during a cough (cont raction) ve rsus a valsalva ( relaxation).
Figure 2.40. The sacral multifidus is contained within an fibroosseus container dorsal to the sacrum. (Reproduced with permission from Lee 2001).
Sapsford et al. ( 2001 ) investigated the co-activation pattern of the pelvic floor and the abdominals via needle EMG for the abdominals and surface EMG for the pelvic Aoor. They Found that the abdominals contract in response to a pelvic floor contraction command and that the pe lvic floor contracts in response to both a 'hollowing' and 'bracing' abdominal command. The results from this research suggest that the pelvic floor can be facilitated by co-activating the abdominals and visa versa.
When the local muscle system is functioning optimally, it applies comp ress ion to the pelviS (Richardson et al 2002) and thus stabil izes the SIJs, augmenting the form closure and helps to prevent excessive shearing of the S1Js. The pelvis is then prepared to 'accept' additional load from outside the pelvis.
Figure 2.4b. When the sacral multifidus contracts it broadens posteriorly. (Reproduced with permission from Lee 2001).
-
III CHAPTER 2 PRINCIPLES OF THE INTEGRATED MODEL OF FUNCTION
The Outer Unit - The Global SystemThe Slings In the past, four muscle systems (slings) which stabilize the pelvis regionally (between the thorax and legs) have been described (Vleeming et al 1995a,b, Snijders et al 1995). The posterior oblique
Figure 2.5. The posterior oblique sling contains, in part, the latissimus dorsi, the thoracodorsal fascia and the contralateral gluteus maximus muscles. (Reproduced with permission from Lee '999 and Churchill Livingstone).
sling (Fig. 2.5) contains connections between the latissimus dorsi and the gluteus maximus through the thoracodorsal fascia, the anterior oblique sling (Fig. 2 .6) contains connections between the external oblique, the anterior abdominal fascia and the contralateral internal oblique and adductors of the thigh, the longitudinal sling (Fig. 2. 7) connects the perone ii, the biceps femoris, sacrotuberous ligament, deep lamina of the thoracodorsal fascia and the erector spinae, and the lateral sling which contains the primary stabilizers for the hip joint namely the gluteus
Figure 2.6. The anterior oblique sling contains, in part, the external oblique abdominal and the contralateral adductors of the thigh. (Reproduced with permission from Lee '999 and Churchill Livingstone).
-
PRINCIPLES OF TI-IEINTEGRATED MODEL OF FUNCTION CHAPTER 2 iii
medius/minimus, tensor fascia lata and the cont ralateral adductors of the thigh. These muscle slings were initially classified to gain a better understanding of how local and global stability of the pelvis could be achieved by specific muscles. It is now recognized that although individual muscles are important for regional stabilization as well as for mobility, it is critica I to understand how they connect and function together. A muscle contraction produces a force that spreads beyond the origin and insertion of the active muscle. This force is transmitted to other muscles, tendons,
Figure 2.7. The longitudinal sling connects the peroneii, the biceps femoris, sacrotuberous ligament, deep lamina of the thoracodorsal fascia and the erector spinae. (Reproduced with permission from Lee '999 and Churchill Livingstone).
fasciae, ligaments, capsules and bones t hat lie both in series and in parallel to the active muscle. In th is manner, forces are produced quite distant from the origin of the initial muscle contraction. These integrated l1luscle systems produce slings of forces that assist in the transfer of load. Van Wingerden et al (2001) used the Echo Doppler to analyze the effect of contraction of the biceps femoris, erector spinae, gluteus maxil1lus and latissiumus dorsi on compression of the SI ]. None of these muscles directly crosses the SI] yet each was found to effect compression (increase stiffness) of the SI].
The global system of muscles is essentially an integrated sling system which represents forces and is comprised of several muscles. A muscle may participate in more than one sling and the slings may overlap and interconnect depending on the task being demanded. The hypothesis is that the slings have no beginning or end but rather connect to assist in the t ransference of forces. I t is possible that the slings are all part of one interconnected myofascial system and the particular sling (anterior oblique, posterior oblique, lateral, longitudinal) which is identified during any motion is merely due to the activation of selective parts of the whole sling.
The identification and treatment of a specific muscle dysfunction (weakness, inappropriate recruitment , t i gh tness) is impo r tant w h en resto ring global stabilization and mobility (between the thorax and pelvis or between the pelvis and legs) and for understand ing why parts of a sling may be inextensible (tight) or too flexible (lacking in support).
-
Ell CHAPTER 2 P R I N CIPLES OFTHE INTECRATED MODEL OF FUNCTION
TH IR D COM PONENTMOTOR CONTROL
M otor control pertains to patterning of m u scle activation (Coillerford & Mottram 200 1 , Danneels et al 200 I , Hichardson et al 1 999, O'Sullivan e t a l 1 997) in other words, t he tillling of specific m uscle action and inaction. Efficient movement requ ires coordinated ill u scle action , s uch t hat stability is ensured while motion is controlled and not restrained. Wit h respect to the thorax, it is the coordina ted action between the local and global muscle systems that ensures stability without rigidity of" postu re and without episodes of collapse. Exercises that focus on sequ encing muscle activation are necessary for restoring motor cont rol ( Lee 200 1 ). The exercises in chapter 7 Focus on balancing tension wit h i n the slings of Ill usc le systeill s and invo lve an extensive use of i magery. I magery has been shown (Yue & Cole 1 992) to be e Ffective in restoring neu ral patterning and increasing strength . U s i ng imagery and specif ic sequencing of Illuscle activation, individual muscles a re strengthened, lengthened and appropriately tillled du ring Functional tasks.
FOURTH COM PONENT EMOTIONS & AWARENESS
Fro lll Andry Vleeming
E illotional states can play a significa nt role in h u man function, including the Fu nction 0 1" the neuroillusculoskeletal system. Many chronic pain patients present with traumatized lif"e experiences in addition to their f"unctional cOlllplaints. Several of t hese patients adopt motor patterns indicative of defensive posturing which suggest a negative past experience. A negative eillotional state leads to fu rther stress . Stress is a nori l lal response intended to energize our syste lll for quick right and Right reactions. When this response is sustained, high levels of adre nal ine and cort isol remain in the system ( I- I olstege et al 1996, Sternberg 2000) in part d u e to circu lating s t ress related ne uropeptides (Sapolsky et al 1 997a,b) which are released in anticipation of defensive or ol"fensive behavior.
Emotional states ( f ight, Right or free7.e react ions) are physically expressed through Ill uscle action and when sustained, influence basic muscle tone and patterning (Holstege et aI 1996). It is illlportant to understand the patient's e illotional state since the detrimental motor pattern can often only be changed by affecting the eillotional state. Sometillles, i t can be as simple as restoring h ope th rough education and awareness of the underlying Illechanical probleill. Other times, proFessional cognitive behavioral therapy is requirecl to ret rain Illore positive thought patterns.
A bas ic require illent Cor cogn itive and physical learning is Focused, or attentive, training - in other words not being absent-minded . 1eaching an individual to be " mindful" or aware of what is happening in t h eir body d u r i n g times of physical and/or emotional loading can reduce sustained, unnecessary m uscle tone and t hereFore joint cOlllpression ( M u rphy 1 992).
-
CONCLUS ION
PH INC I PLES OF T HE INTEC HATED MODEL OF FUNCT I ON CHAPTER 2 m
It has been long recognized that physical factors impacL jo i nt motion. The model presented here suggests that joi n t mechan ics are in fl uenced by multiple factors, some i n t r i nsic to the jo int i tself while others are produced by muscle act ion which in turn is i n fluenced by t he emotiona l state. The e ffect i ve ma nageme n t of back pa i n a n d dysfu nct ion requ i res aLten t ion to all fou r components - form closure, Force closure, motor control and emot ions with the goal being to guide patients towards a healt h ier way to l ive i n t heir body.
-
\"
T1
T2
-
3
BIOMECHANICS
OF THE THORAX
Managing dysfunction requires an
understanding of function. The biomechanics
of the thorax presented in the first edition of
this text were derived from clinical observation
and influenced primarily by the study of
Panjabi, Brand & White (1976). Few studies
have added to our knowledge base since. In
1996, Willems, Jull and Ng reported on their in
vivo findings of coupled motion in the thorax.
The results from this study, and the influence it
has had on the original biomechanics, will be
discussed in this chapter.
-
EI CHAPTER 3 BIOMECHANICS OF THE THORAX
TER MINOLOGY
To fac il i tate the s ubsequen t d i scuss ion, the terminology used requires definition. Osteokinematics (MacCona i l l & Basmaj i an 1977) refe rs to the study of motion of bones regard less of the mot ion of the joints. Angular motions are osteokinematic motions and are named according to the axis about which the bone rotates. Flexion/extension occurs about a coronal axi s , anterior/posterior rota t ion a b o u t a paracoronal ax i s , s i de flexi on ( la teral bend ing) abou t a sagi t tal axis and axial rotat ion about a vert ical axis. Coup led mot ion refers to the combinat ion of movements which occu r as a conseq uence of an induced mot ion .
Linear, or translatoric, motions are named according to the axis along which the bone t ranslates. Lateral t ranslation occurs along a coronal axis , anteromed ial/posterolateral translat ion along a paracoronal axis, t ract ionlcompression along a vertical axis, and anteroposterior t ranslat ion along a sagittal axis.
Arthrokinematics (MacConai l l & Basmajian 1977) refers to the s tudy of motion of joints regardless of the mot ion of the bones . These movements a re nailled accord ing t o the d i rect ion the joint su rfaces glide.
LITERATURE REV I EW
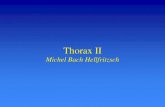
Panjab i , B rand and White (1976) invest i gated the pr imary and coupled Il lot ions of the thorax in an in v i t ro study of several cadavers ranging i n age (before death) from 19-59 years. Three hundred and n inety s i x load d i splaceillent c u rves were obtained for s i x degrees of Illot ion; three t ransl a t ions and three rota t ions a long and abou t the X, Yancl Z axes ( Fig . 3.1) for each of the eleven Illotion segillents of the thoracic spine. The Illotion seOlllent included t he ant er ior interbody joint , b the poster ior zygapophyseal jo ints and the cos-tovertebral and costotransverse joints. The ribs
z
were cut 3 Clll lateral to the costotransverse joints and the front of the chest was reilloved . The spinal uni t was intact , however, the costal uni t was not.
In 1996, W i l l e llls , Ju l l and Ng Illeasu red t h e pril l lary and coupled illotions o f the thoracic spine in an in v ivo s tudy. Sixty subjects between the ages of l 8 and 24 were stud ied us ing a 3 S PAC E Fastrak Systeill. The subjects were screened and excluded jf they had a current or past history of thorac ic pain, long terlll respi ratory d i sorder or a significant scoliosis. An exaillinat ion of the thoracic spine for segillental Funct ion was not done prior to the study. Sensors were attached to one spinous process in each of three regions of the thora'(, one between T l -T4, a second between T4-T8 and the t h i rd between T8-Tl2 . Each s u bjec t was seated , the pelv i s and thighs secu red and the lumbar sp ine s upported . Wi th the i r arills folded across the i r chests, each subject was asked to Illove to the i r Illax imal range in thoracic Aexion, extension, axial rotat ion and lateral Aexion. Each motion was carefully taught to ensure the Illot ion
y
Figure 3.11n an in vitro study by Panjabi, Brand and White (1976), 396 load displacement curves were obtained for 6 degrees of motion at each thoracic segment noting both amplitude and coupling of motion for each.
-
BIOMECHANICS OF THE THOHAX CHAPTEB 3
des ired was aCLual ly occurr ing in Lhe thorax. "fhe Fastrak is an elecLromagnetic sy stem which t racks Lhe motion in 3D and sends the i nFormat ion to a com puter whose software i n Le rpre t s t h e da ta "a l lowing the calcu lation of Lhe pos i t ion of each sensor in space" (Wil lems et al J 996). The methods and resu l t s from Lh i s s tudy have been carefu l l y cons idered wi Lh respect to t he b iomec ha n ica l model of Lhoracic mOL ion and w i l l be d i sc ussed .
Accord i ng Lo maLhemat i ca l (Sa m a u rez J 986, Andriacchi eL a l 1 974, Ben-Haim & Saidel J 990) and t heoret ica I (Lee 1 993 , 1 994 ) mode ls , t he Lhorax is capable of s ix degrees of motion along and abouL t he Lhree cardina l axes of the body; however, it is known tha t no movement occu rs i n i so la t ion ( Pa nja b i et a l 1 976 , W illem s et a l 1 996) . Al l angu lar motion ( rotaL ion) i s coupled wiLh a l i near mot ion ( t rans laL ion) and visa versa. As t he thorax moves to meet it s b iomechan ical demands, iL Illust accommodate Lhe requiremenLs of respiraLion. To do th i s , it needs flex ib i l i t y i n mot ion patLerni ng.
z
- -----
Flexion
I
VI
FU NCTIO NAL MOVE ME NTS
Vertebrosternal Region Flexion Flexion of the t horac ic vertebrae occu rs du ring forward bend ing of the t ru nk. Panjabi eL a J (1976) found that forward sagittal rotation (nexion) around the X axis coupled wi th anterior t rans lat ion a long the Z ax i s (.5 111111 ) a n d very s l ighL d i stract ion (Fig.3 .2 ) . When anterior trans lat ion along the Z axi s was induced, forward sagittal rOLation around the X axis and very slight compression also occurred. I n the in vivo study of Wi llems et al ( J 996), sagittal p lane motion was the pu rest and showed the leasL i nc idence of coup led illot ion . No ax ia l rotat ion or laLeral Aexion should occur during sagitLal plane Illat ion of the thorax.
The oSLeok i ne matic Illot i on of t h e r ibs w h i c h occu rs d uring flex ion of the thorac ic verteb rae was not noted i n either study ( Panjab i et aJ 1976, Wil lems et al 1996). Sauillarez (1986) noted thaL
Anterior Translation
y
Figure 3.2. Flexion around the X axis induced anterior translation along the Z axis and slight distraction along the Y axis. Anterior translation along the Z axis induced forward sagittal rotation around the X axis and slight compression along the Y axis (Panjabi et aI1976).
-
m CHAPTER 3 BIOMECHANICS OF THE THORAX
..................
........ .
.. ' .' ........ ........ ..
..................
Figure 3.3. The osteokinematic and arthrokinematic motion proposed to occur in the mobile thorax during forward bending - vertebrosternal region.
con s i d e rab l e i n d e p e n d e n t move m e n t o f t h e sternum and t he spine i s possible, "th us allowing mobi l ity of the spi ne without forcing concomitant movements of (the) rib cage". Th is i s supported cl i n ica lly i n t hat th ree movement pat terns a re apparent i n t h is region of t he t horax and depend on the relative flexibility between the spinal column and t he rib cage. [n t he very young, (less t han 12 years of age) the head of t he rib does not fu lly art iculate with the i n ferior aspect of the superior vertebra (Wi l l i ams et al 1 989) . In other words, the superior costovertebral joint is not completely developed prior to puberty. The secondary ossifica t ion centres for the head of the r i b do n o t deve lop u ntil puberty; therefore, the young chest
Flexion
i s much more mobi le. I n the skeleta l l y mature, the superior costovertebral joi n ts I imit t he degree of rotat ion possible in a l l t h ree planes . I n old age, t he costal cart i l ages tend to oss i fy su perficia l ly and decrease the pliab i l ity and relative f lexibil ity of the t horax. This change i n re lal ive flex ib i l ity i s appare n t when exa m i n i ng the spec i fic cos t a l osteokinematics during forward/backward bending of t runk .
1. Dur ing flexion of the mobile t horax ( Fig. 3.3) , f lex ion of the super ior vertebra occurs . The r ibs anteriorly rotate about a paracorDnal axis a long the l i ne of the neck of t he r ib such that the anter ior aspect trave ls i nferiorly whi le the posterior aspect trave ls superiorly. At the ! im it
-
BIOMECHAN I CS OF THE THORAX CHAPTER 3 _
Figure 3.4. The osteokinematic and arthrokinematic motion proposed to occur in the stiffer thorax during forward bending - vertebrosternal region.
of forward bend ing, the vertebrae stop and the r ibs cont i nue to anteriorly rotate relative to the vertebrae.
Art h rokinemal ical ly, the inFerior facets of t he su perior t horacic vertebra gl ide su peroanteriorly at t he 7,ygapophyseal join t s . The su perior art icu lar processes of the infer ior t horac ic vertebra present a gentle curve convex posterior in bot h t he sagi t t a l and corona l p la ne. The superior motion of t he inferior art icular processes fo l lows t he curve of t h i s convex i t y a n d the resu l t i s a su peroanterior g l ide . The anterior rotat ion of t he r ib resu lts in a su perior g l ide cou pled w i th an anterior rol l of t he tu bercle at t he costotransverse joi nt.
2. I n the stiFf t horax ( F ig. 3.4), the r ibs are less Rexible t han the spinal column. During rlexion, the anterior aspect of the rib trave ls i nFeriorly w h i le the poster ior aspect trave l s su perior ly. Once the range of mot ion of the r ib cage is exhausted , the t horac ic vertebrae cont inue to Rex on t he now stationary ribs. The arthroki nemat ics of the zygapophyseal jo in t s remain a su peroan terior gl ide. At t he costotran sverse join t s , t he arthrokinematics are d i fferen t . As the thoracic vertebrae cont inue to forward Rex, the concave facets on the transverse processes travel su periorly relative to the t ubercle of t he ribs. The result is a relative inferior glide coupled with a posterior rol l of the t ubercle of t he rib at the costotransverse joi n t .
-
CI-IAPTER 3 B IOMECHANICS OF THE THORAX
3. The third movement pattern occurs when the relat ive flex ibil i ty between the spi nal colu m n a n d the r i b cage i s the same. During flexion o f the thora,'(, the quantity o f movement is reduced and there is no apparen t movement between t he t horacic ver tebrae a n d t he ribs . Some superoanterior gliding occurs a t the zygapophyseal jo in t s , however very l i t t l e , i f a ny, costot ransverse jo in t motion can be fel t .
Extension Extension of the thoracic vertebra occu rs during backward bending of the trunk and during b ilateral eleva t ion of the arms. Panjabi et a l ( 1 976) found that extens ion a round the X ax i s coupled w i th pos ter ior t rans l a t i on a long the Z axi s and very sl ight distraction (Fig. 3.5) . When backward translat ion a long the Z axis was i nduced in the experimenta l mode l , extension a round the X axis and very s l ight compress ion a l so occurred.
Extension
The osteo k inemat i c Illo t i on of t he r ibs whic h occurs duri ng extens ion 01' the thorac ic vertebra was not noted in e i t h er st udy by Pa njab i et a l ( 1 976) or Wil lems e t a l ( 1 996). Cl i n ica l l y, t he movement patterns observed appear once aga in to depend on relative f lexibil ity between the spinal col u m n and the rib cage . Three pat terns have been noted.
1 . Dur ing extens ion 01' t he mobile lhorax ( F ig. 3.6), extension of the superior vertebra occurs. The ribs posteriorly rotate about a paracorona l ax is a long the l i ne of t he neck 01' the rib such that the anterior aspect trave l s superi or ly whi l e the poslerior aspect t ravels i n ferior ly. At the l i m i t of backward bend i ng, lhe vertebrae stop and the r ibs cont i nue to posteriorly rotate re lat ive to the vertebrae.
Posterior Translation
Figure 3.5. Extension around the X axis induced posterior translation along the Z axis and slight distraction along the Y axis. Posterior translation along the Z axis induced backward sagittal rotation around the X axis and slight compression along the Y axis (Panjabi et aI1976).
-
BIOMECHANLCS OFTHE THORAX CHAPTER 3 n
I .' , .
, . , .
: J:'* . . . _,f
....
....
...
. ' .'
. ' .. '
.-- ..
..
. '
Figure J.6. The osteokinematic and arthrokinematic motion proposed to occur in the mobile thorax during backward bending - vertebrosternal region.
Arthrokineillatically, the i nFerior Facets of the su perior lhoracic vertebra glide i n feroposter iorly at the zygapophyseal joi nts. The superior articular processes present a gentle curve convex posterior in both the sagittal and coronal plane. The i nFerior Illol ion of the i n fer ior art icular processes follows the cu rve of this convexity and the resu l t is an inFcroposterior g l ide . The posterior rotat ion of lhe neck of the rib resu lts i n an inrer ior g l ide coup led with a posterior roll of the lubercle al the costotransverse joint.
2. During extension of the stiff thorax (Fig. 3.7), the ribs are less flexible than the spinal column.
.........
.. ..
....
....
....
. '
. '
.
.
.
I ni t ia l ly, the a nterior aspect of the r ib travels superior ly wh i l e t he posterior aspect travels i n feriorly. Once the range of Illot ion of the r ib c age i s exhauste d , t he t horac ic verteb rae continue to exten d on the now stationary r ibs. The a rt h rokinematics of the zygapophyseaJ joints remain an i n feroposterior glide. At the costotran sverse joints, t he arthroki neil latics are different. As the thoracic vertebrae continue to extend, the concave facets on the transverse processes travel inferiorly relative to the tubercle of the r ibs . The resul t is a re lat ive s u perior glide coupled with an anterior roll of the tubercle of the r ib at the costotransverse joint.
-
III CHAPTER 3 BIOMECHANICS OF THE THORAX
Figure 3.7. The osteokinematic and arthrokinematic motion proposed to occur in the stiffer thorax during backward bending - vertebrosternal region.
3. The th i rd movement pattern occurs when the relative f lexib i l i ty between the sp ina l column and the r ib cage is the same. During extension of t h e thorax, the quantity o