The Syed-Neblett interstitial template in locally advanced gynecological malignancies
7
Inr. J Radiorion Oncology Biol. Phys.. Vol. 9. pp. 1897-1903 036&3016/83/$3.M) + 00 Printed in the U.S A All rights reserved. Copyright 0 1983 Pergamon Press Ltd. ?? Brief Communication THE SYED-NEBLETT INTERSTITIAL TEMPLATE IN LOCALLY ADVANCED GYNECOLOGICAL MALIGNANCIES FRANCISCO AMPUERO, M.D.,* LARRY L. Doss, M.D.,? MIRKUTUB KHAN, M.D.,? BETTY SKIPPER, PH.D.,$ AND ROBERT D. HILGERS, M.D.* Divisions of *Gynecologic Oncology, ?Radiation Oncology and $Family, Community and Emergency Medicine, Cancer Research and Treatment Center, University of New Mexico Medical Center, Albuquerque, NM Twenty-eight patients with locally advanced malignancies of the cervix and vagina were treated with a combination of external radiation therapy and afterloading Syed-Neblett iridium template. There were 22 patients with squamous cell cancer and two patients with adenocarcinomas of the cervix. Four patients with squamous cell cancer of the vagina were treated with this method. Only patients with locally advanced disease (cervical lesion r4 cm in diameter) and poor vaginal anatomy were selected for this modality of therapy. In our series the incidence of distant failures of 39 % seems to confirm the significance of local volume of disease as a prognostic indicator; despite a local control rate of 59 %, only 33 % of our patients are alive from 25-51 months. Complications occurred in 12 patients (42 %). Six patients (22 %) developed severe rectal stricture or rectovaginal fistula necessitating diverting sigmoid colostomy; five patients (18 % ) developed hemorrhagic proctitis with diarrhea and tenesmus; one patient developed vaginal vault necrosis. Complications occurred 7 to 24 months following therapy. Six of the 12 patients developing complications are dead of disease. On the basis of this study and be-causeof the low cure rate and high incidence of complications, the value of the Syed-Neblett template in locally advanced gynecologic malignancies should be reconsidered. Syed Neblett, Transperineal gynecological implant, Transperineal volume implant, Carcinoma of the cervix, Ckcinoma of the vagina. INTRODUCTION During the past 12 years, afterloading techniques for the delivery of radiation to the vagina, cervix, uterus, and parametria have changed rapidly. Delcos et al.* in 1970, introduced afterloading vaginal cylinders of variable diameters for the irradiation of primary vaginal tumors. The Delcos applicator can be combined with a central, Fletcher tandem to simultaneously irradiate the cervix and uterine cavity. The Fletcher tandem can be used with colpostats to distribute the dose into the proximal para- metria. These systems are adequate for early vaginal and cervical disease; however, bulky disease in the perivaginal and distal parametrial regions will not be uniformly treated by such brachytherapy devices. To facilitate the application of the uniform radiation field to the entire paracolpium and parametrium, interstitial implants to deliver radiation therapy to these anatomical areas have been used in the past. Since the original description by Pitts and Watterman in 19309 the use of interstitial volume implants for treatment of gynecological malig- nancies has been reintroduced several times, only to be abandoned despite the quoted good results obtained with this therapeutic modality. The theoretical benefits of this treatment modality are to treat the disease precisely in its anatomical location and to provide a wider and more uniform distribution of radiation in the pelvis. In 1974, Feder et al. reintroduced the use of interstitial implants in pelvic tumors and in 1978 reported their own experience using the afterloading technique with iridium- 1 92.4 This technique was particu- larly recommended for patients with distorted vaginal anatomy where central tandem and colpostats could not be adequately applied. The Syed-Neblett afterloading template consists of the vaginal obturator and an acrylic perineal plate. The template allows the insertion of 44 trochars in five concentric rings around the lateral plane of the vagina. The trochars are afterloaded with the iridium- 192 in nylon ribbons and a tandem is provided for the placement of intrauterine cesium or radium sources. The technique for the use of Syed-Neblett template has been described by Fleming et al.’ Since the reintroduction of the interstitial perineal implants by Syed and Neblett, occasional reports have Reprint requests to: Francisco Ampuero, M.D., Cancer Research and Treatment Center, 900 Camino de Salud N.E., Albuquerque, NM 87 131. Accepted for publication 21 July 1983. 1897
-
Upload
francisco-ampuero -
Category
Documents
-
view
215 -
download
1
Transcript of The Syed-Neblett interstitial template in locally advanced gynecological malignancies

Inr. J Radiorion Oncology Biol. Phys.. Vol. 9. pp. 1897-1903 036&3016/83/$3.M) + 00 Printed in the U.S A All rights reserved. Copyright 0 1983 Pergamon Press Ltd.
??Brief Communication
THE SYED-NEBLETT INTERSTITIAL TEMPLATE IN LOCALLY ADVANCED GYNECOLOGICAL MALIGNANCIES
FRANCISCO AMPUERO, M.D.,* LARRY L. Doss, M.D.,?
MIRKUTUB KHAN, M.D.,? BETTY SKIPPER, PH.D.,$
AND ROBERT D. HILGERS, M.D.*
Divisions of *Gynecologic Oncology, ?Radiation Oncology and $Family, Community and Emergency Medicine, Cancer Research and Treatment Center, University of New Mexico Medical Center, Albuquerque, NM
Twenty-eight patients with locally advanced malignancies of the cervix and vagina were treated with a combination of external radiation therapy and afterloading Syed-Neblett iridium template. There were 22 patients with squamous cell cancer and two patients with adenocarcinomas of the cervix. Four patients with squamous cell cancer of the vagina were treated with this method. Only patients with locally advanced disease (cervical lesion r4 cm in diameter) and poor vaginal anatomy were selected for this modality of therapy. In our series the incidence of distant failures of 39 % seems to confirm the significance of local volume of disease as a prognostic indicator; despite a local control rate of 59 % , only 33 % of our patients are alive from 25-51 months. Complications occurred in 12 patients (42 % ). Six patients (22 %) developed severe rectal stricture or rectovaginal fistula necessitating diverting sigmoid colostomy; five patients (18 % ) developed hemorrhagic proctitis with diarrhea and tenesmus; one patient developed vaginal vault necrosis. Complications occurred 7 to 24 months following therapy. Six of the 12 patients developing complications are dead of disease. On the basis of this study and be-cause of the low cure rate and high incidence of complications, the value of the Syed-Neblett template in locally advanced gynecologic malignancies should be reconsidered.
Syed Neblett, Transperineal gynecological implant, Transperineal volume implant, Carcinoma of the cervix, Ckcinoma of the vagina.
INTRODUCTION During the past 12 years, afterloading techniques for the delivery of radiation to the vagina, cervix, uterus, and parametria have changed rapidly. Delcos et al.* in 1970, introduced afterloading vaginal cylinders of variable diameters for the irradiation of primary vaginal tumors. The Delcos applicator can be combined with a central, Fletcher tandem to simultaneously irradiate the cervix and uterine cavity. The Fletcher tandem can be used with colpostats to distribute the dose into the proximal para- metria.
These systems are adequate for early vaginal and cervical disease; however, bulky disease in the perivaginal and distal parametrial regions will not be uniformly treated by such brachytherapy devices. To facilitate the application of the uniform radiation field to the entire paracolpium and parametrium, interstitial implants to deliver radiation therapy to these anatomical areas have been used in the past. Since the original description by Pitts and Watterman in 19309 the use of interstitial volume implants for treatment of gynecological malig- nancies has been reintroduced several times, only to be
abandoned despite the quoted good results obtained with this therapeutic modality.
The theoretical benefits of this treatment modality are to treat the disease precisely in its anatomical location and to provide a wider and more uniform distribution of radiation in the pelvis. In 1974, Feder et al. reintroduced the use of interstitial implants in pelvic tumors and in 1978 reported their own experience using the afterloading technique with iridium- 1 92.4 This technique was particu- larly recommended for patients with distorted vaginal anatomy where central tandem and colpostats could not be adequately applied. The Syed-Neblett afterloading template consists of the vaginal obturator and an acrylic perineal plate. The template allows the insertion of 44 trochars in five concentric rings around the lateral plane of the vagina. The trochars are afterloaded with the iridium- 192 in nylon ribbons and a tandem is provided for the placement of intrauterine cesium or radium sources. The technique for the use of Syed-Neblett template has been described by Fleming et al.’
Since the reintroduction of the interstitial perineal implants by Syed and Neblett, occasional reports have
Reprint requests to: Francisco Ampuero, M.D., Cancer Research and Treatment Center, 900 Camino de Salud N.E., Albuquerque, NM 87 13 1.
Accepted for publication 21 July 1983.
1897

1898 Radiation Oncology 0 Biology 0 Physics December 1983, Volume 9, Number 12
appeared in the recent literature describing the use of the procedure in different pelvic malignancies. However, the literature in recent years does not elaborate on the guidelines for the use of interstitial implants in gynecolog- ical malignancies nor describe the late complications.
tion from all t;le variables involved in the treatment planning.’
RESULTS
Since 1978, at the University of New Mexico, Cancer Research and Treatment Center, we have treated 28 patients with cancers of the cervix or vagina with a combination of the Syed-Neblett implant and external irradiation therapy. Details of the technique, dosages, side effects, late complications, and results are described.
METHODS AND MATERIALS
This study group consisted of 28 patients with biopsy proven advanced carcinoma of the cervix and vagina, treated between 1978 and 1980, at the University of New Mexico Cancer Research and Treatment Center.
Of these patients, four had carcinomas of the vagina and 24 had carcinomas of the cervix. All patients had a pretreatment metastatic workup consisting of chest X ray, IVP, bone scan, lymphangiogram, liver function test, proctoscopy-cystoscopy, and were clinically staged under anesthesia according to the International Federation of Gynecologists and Obstetricians staging system. The patients’ age ranged from 23-86 years, with 18 patients being between the fifth and sixth decade of life.
Of the 28 patients, four had squamous cell carcinoma of the vagina treated first with external radiation therapy followed by a Syed-Neblett template (Table I). There was one patient for each of the clinical stages of vaginal carcinoma. Three of these patients have been followed for more than three years and are alive without evidence of disease for 49 to 51 months. The remaining patient died five months following therapy; at the time of postmortem examination, a wide-spread non-Hodgkin’s lymphoma was found. There was no evidence of either local or distant spread squamous cell cancer of the vagina nor had she developed complications from therapy.
Twenty-four patients with carcinoma of the cervix were treated. There were 21 patients with squamous cell carcinomas and three with adenocarcinomas of the cervix. One patient had Stage IB disease of the cervical stump, six had Stage II, I I had Stage 111, three had Stage IV, and three had recurrent disease and were not candidates for pelvic exenteration. One patient with Stage II disease has been lost to follow-up.
All patients received initial whole pelvis external radia- tion therapy followed by the transperineal Syed-Neblett parametrial butterfly template using the technique pre- viously described by Feder et ~1.~
The patient selection was based on the local extent of the tumor and the anatomic characteristics of the vagina. Only patients with large, bulky tumors (cervical lesion >4 cm in diameter) that obliterated the fornices or extended in to the upper vagina, decreasing the extensability of the mucosa, were selected for the use of the Syed-Neblett template.
Isodoses for the template implants were obtained in three dimensions, i.e., AP, transverse and lateral, from our treatment planning computer.* The computer plan used for computation of dose distributions can handle up to 300 iridium- 192 seeds and has been described previous- ly.” Seed coordinates were entered using a sonic digitizer from orthogonal views of the seed locations. The area of the prescribed dose (reference dose), was determined by planimetry in 1:1 scale, from computer printouts of the the 0.5 and 1.5 reference isodoses (1.5 reference isodoses hereafter called “hot spots”). The areas contained by these rad per hour lines was determined by a compensat- ing polar planimeter with 0 setting device. For each implant, three areas were calculated for the three isodose lines.
Each of the patients with cervical carcinoma received external radiation followed by a Syed-Neblett template interstitial volume implant (Table 2).
The patient with Stage IB cervical stump disease received 4000 cGy followed by iridium-192 implants delivering a total dose of 2500 cGy. Each of the six patients with bulky Stage II, (one patient with Stage IlA, five patients with Stage IIB) were treated with standard radiation to 4000 cGy followed by cesium application to approximately 3500 mg hours. Each course of radiation was routinely followed by a Syed-Neblett template implant delivering a dose of 2500 to 3000 cGy. One of these patients received two iridium- 192 implants follow- ing external radiation therapy to 4000 cGy.
Eleven patients had Stage 111 tumors. Nine of them received 4000 to 5000 cGy external radiation therapy to the pelvis followed by one cesium application to 4000 mg hours or bilateral parametrial boost delivering 1000 to
Table 1. Stage and dosage in patients with carcinoma of the vagina
The stepwise logistic multiple regression procedure was used to estimate the probability of developing a complica-
External Syed-Neblett radiation dose template dose
Patient no. Stage* (CGY) (CGY)
I I 4000 2000 2 II 5000 2500 3 III 6500 3400 4 IVA 5000 2800
*FIG0 staging system.
*DEC 1 I /60 Digital Equipment Corporation, Albuquerque, NM.

Syed template in gynecology 0 F. AMPUERO et al. 1899
Table 2. Implant and external radiation in patients with cervical carcinoma
Dose (cGy) from Syed-Neblett Template No. of patients
Implant dose 1500-1999 2 2000-2499 3 2500-2999 14 3000-3499 4
3500 I
Total 24
External dose 35OOG3999 4000-4999 5000-5999 6000 or above
Total
5 II I I
24
2000 cGy. Their external radiation was followed by a Syed-Neblett template implant to a regional dose of 2000 to 3000 cGy. Two patients with Stage III disease were treated at Los Alamos Pion Medical Facility with nega- tive pi-meson irradiation. Each received a dose of 4400 to 4500 pion rad (maximum) to the whole pelvis followed by a boost to the parametria before template implant. Three patients with Stage IV disease (two patients with Stage IVA and one patient with Stage IVB) received external radiation therapy to 5000 cGy followed by template implant for a dose between 2500 to 3000 cGy. There were three patients with recurrent cervical disease; in original staging, one was Stage IV, one Stage IIB, and one was unstaged post-surgically. These three patients received 3000, 4080, 4000 cGy whole pelvis radiation therapy respectively. All three patients receiving re-irradation developed recurrence.
Complications as a result of therapy occurred in the three living patients with vaginal carcinoma. One patient developed intermittent hemorrhagic proctitis controlled
with cortisone enemas and diet adjustment. The second patient had severe necrosis of the vaginal mucosa con- trolled with medical treatment and a third developed a severe rectal stricture with profuse bleeding, tenesmus and rectal pain 12 months following therapy. A diverting colostomy was performed and no evidence of either local or distant disease was found at the time.
In the group of patients with cervical cancer, nine developed complications related to treatment. Four had severe hemorrhagic proctitis requiring treatment with cortisone enemas and diet adjustment. Of these patients, one had Stage IB cervical stump, one Stage IlB, one Stage IIIB and one recurrent cervical cancer. Three of them eventually died of disease. One patient with Stage IIIB disease developed a recta-vaginal fistula 1 I months following treatment. She refused a diverting colostomy and died of disease 18 months after therapy. Four patients had severe rectal stricture, bleeding, pain, and tenesmus necessitating diverting colostomy; one patient had Stage IIB and three had Stage IIIB cervical cancer, two of them are dead of disease. Complications in these patients appeared from 7 to 24 months following treatment (Table
3). Of the 24 patients with cervical carcinoma, six are alive
with no evidence of disease 25 to 41 months following treatment. Of these six living patients, four were Stage III, three were Stage IIIB, and one was Stage IIIA. Two patients were Stage IVA (bladder involvement).
Overall, 15 out of the 27 patients available for follow- up (55%) are dead, of or with, disease (one patient with Stage IIB died of intercurrent carcinoma of the stomach, but had recurrent cervical cancer in the pelvis at the time of death).
We examined the study group for patterns of recur- rence and metastasis and found the following: in six patients, recurrence occurred in the pelvis only; four patients had distant recurrence, and five both pelvic and distant recurrent disease (Table 4).
A total of 11 patients or 40% had pelvic failure. There
Table 3. Interval from treatment to complications
Patient Diagnosis
stage Tandem Obturator loading ring loading Complication
Interval of treat.-camp. Colostomy A&W? DOD*
I Sq. Ca. Cx. IIIB No 2 Sq. %a. Cx. IIIB No 3 Sq. Ca. Cx. IIB Yes 4 Sq. Ca. Cx. IIIB Yes 5 Sq. Ca. Cx. Stump IB Yes 6 Sq. Ca. Cx. IIB No 7* Sq. Ca. Cx. IIIB Yes 8 Adenoca. Cx. Rec. Adenoca. Yes 9* Ca. Cx. IIIB Yes
IO Sq. Vagina III Yes II Sq. Vagina IVA No I2 Sq. Vagina II Yes
Yes No No No Yes No Yes Yes Yes No Yes No
Hemorragic proctitis R-V fistula Hemorragic proctitis Severe strict. Hemorragic proctitis Severe strict. Severe strict. Hemorragic proctitis Severe strict. Severe strict. Vag. vault net. Hemorragic proctitis
12 mos. I I mos. IO mos. I2 mos. I2 mos. IO mos. IO mos. I mos.
19 mos. 12 mos. 24 mos. I2 mos.
I8 mos. ‘_ I8 mos.
29 ‘mos. xx 38 mos.
l3.mos. xx I2 mos. xx 12 mos.
I4 mos. xx 24 mos. xx 48 mos.
48 mos. 50 mos.
*Pion external beam therapy. ?AIive and well. $Dead of disease.

1900 Radiation Oncology 0 Biology 0 Physics December 1983, Volume 9, Number 12
Table 4. Site of failure
Patient Diagnosis
1 Cervix 2 Cervix
3 Cervix 4 Cervix
5 Cervix
6 Cervix I Cervix 8 Cervix 9 Cervix
10 Cervix
11 Cervix 12 Cervix adeno. 13 Cervix 14 Cervix 15 Cervix adeno.
Stage
IIIB IIIB
IIIB IIIB
IIIB
IIIB IIIB IIB IIB IIB
IIB IVB
Recurrent Recurrent Recurrent
Pelvic recurrence
Vaginal Local
(persistent) -
Cervical vag. persis.
Pelvic Pelvic Pelvic Pelvic
(persistent) Pelvic Pelvic Pelvic
- Pelvic
Distant metastasis
Intraperitoneal Intraperitoneal
Left supraclavicular Mediastinum
left supraclavicular Lungs
Lungs
Lungs -
Subcutaneous L. Lumbar Lungs
-
Both
xx xx
- xx
xx
-
-
-
were a total of nine patients or 33% with distant failure; the sites of failure were the lungs in four patients, intraperitoneal disease in two, mediastinum and left supraclavicular area in two, and subcutaneous metastasis in the left lumbar area in one.
Of the three patients treated for recurrent pelvic dis- ease one had local and distant failure, one failed in the pelvis, and one in the lungs only.
Three patients in this series died of causes not directly related to the cancer. One died of rectal bleeding and disseminated intravascular coagulation and had no evi- dence of cancer at the time of postmortem examination. A second patient died of a myocardial infarction at the time of hospitalization for rectal bleeding, and did not have clinical evidence of disease at the time of death. A third patient with vaginal cancer died of a non-Hodgkin’s lymphoma with no evidence of pelvic or distant disease at the time of autopsy.
DISCUSSION
Locally advanced, extensive carcinomas of the cervix or vagina often distort the pelvic anatomy preventing ade- quate treatment with intracavitary irradiation sources. With the advent of megavoltage irradiation, such patients were usually treated with external X-ray therapy prior to an attempt at intracavitary or interstitial implant. Often the external X-ray therapy will not shrink such tumor masses to the point where afterloading systems such as the Fletcher-Suit tandem and ovoids can be used. The Syed-Neblett template is then used to accomplish an interstitial implant with a standardized pattern within the tumor volume. The Syed-Neblett template is a relatively new device, whose originators claim it should increase the cure rate in advanced gynecological malignancies. The basis of this claim is three-fold: 1) the ease of insertion and reproducibility of the template, 2) the homogeneous
distribution of radiation dose obtained throughout the implant volume, and 3) the option of differential radiation dose delivery. The template device is commercially avail- able and has been used by our oncologists since 1978.
Volume of local disease, regardless of the clinical stage, seems to correlate well with the incidence of both pelvic and distant failure. In 1975, Piver and Chung” reported a five year survival of 85.5% for Stage IB and 75.0% for Stage IIA in patients with lesions up to 3 cm in diameter; however, patients with bulky tumors had a 65.4% survival for Stage IB and 39.3% in Stage IIA disease.
Wharton et al.13 have suggested that the majority of patients with bulky cancers and metastasis to the lymph nodes may actually have systemic disease. In our series the incidence of distant failures of 39% seems to confirm the significance of local volume of disease as a prognostic indicator. Despite a local control rate of 59%, only 33% of our patients are alive from 25 to 51 months (Table 5). Whether pre-treatment exploration of patients with locally advanced disease will improve the survival of these patients has yet to be proved.
A point of interest in our series is that all the patients with Stage IVA disease are alive with no evidence of disease 33 to 49 months. This suggests that patients with central disease may benefit from this form of therapy.
Although our series consists of only 28 patients, 12 had significant complications, presumably attributable to treatment. These complications can be divided into tem- porary or permanent, depending upon the need for surgi- cal intervention. Six patients had complications con- trolled with conservative medical treatment, but another six (22%) had serious complications necessitating divert- ing colostomy. This is higher than has been previously reported by others in patients with locally advanced cancers treated with either conventional therapy’** or with the transperineal volume implant.4”2

Syed template in gynecology 0 F. AMPUERO et al. 1901
Table 5. Patient living without disease
Patient Diagnosis Stage Survival mos. Complications
Cervix Cervix Cervix Cervix Cervix Cervix Vagina Vagina Vagina
IIIB IIIB IIIB IIIA IVA(B) IVA(B) II III IVA( B)
31 Proctitis 41 Colostomy 25 Colostomy 27 None 33 None 33 None 51 Proctitis 49 Colostomy 49 Vag. vault necrosis
To test the hypothesis that these complications were treatment related, we analyzed the characteristics of each patient’s implant for prediction of complications.
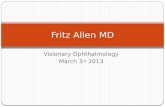
Eleven variables were studied: dose from iridium- 192 implant(s), dose rate in prescribed volume of template, number of seeds in implant, radium equivalent (total of Ir’92 + CS’~‘), individual iridium seed strength, template volume, percent area of “hot spot” in template, external XRT dose (total of cGy), iridium-192 in obturator ring trochars, tandem loaded with Cesium- 137, and number of seeds per ribbon. Using a stepwise logistic regression procedure, with the dependent variable being the develop- ment of a complication, only the percentage hot spot approached significance (p = 0.06) as a predictor of future injury (see Fig. I).
A 75% specificity and 67% sensitivity of prediction can be achieved by using only the % hot spot. No other aspect of the implants had significant influence on the complica- tion rate. Using our data, the relationship between the percentage hot spot and the risk of future complications seems evident. For example, if the summed areas of the hot spot in three planes of the implant occupy 50% of the prescribed dose volume, the patient stands a 50% chance of developing a treatment-related complication. Some patients may, however, die of uncontrolled disease before such complications develop. In our series, a latent interval
0’ ’ ’ ’ ’ ’ ’ ’ ’ ’ .I .2 .3 .4 .5 .6 .7 .8 .9
% Hot Spot Fig. 1. Dosimetric analysis of complications with Syed-Neblett Template.
of seven months to two years was usually necessary before complications occurred.
The percentage hot spot in reality represents the degree of nonuniformity of dose rate across the implant volume. In the practice of brachytherapy, we would prefer that the dose rate within the treatment volume be absolutely uniform. In most instances, however, this cannot be achieved because of the physical contraints of the isotope used. In the case of the Syed-Neblett template, the iridium seeds represent point sources, arranged in linear arrays, within a rectangular volume. By manipulating seed strength and the number of seeds and ribbons used, the inhomogeneity of dose across the template can be changed dramatically. For example, if a template is loaded with 44 ribbons, 220 seeds at 0.33 milligram radium equivalent per seed, the reference isodose (85% of maximum) will be 81 rad per hour. The maximum dose rate will be 95 rad per hour and will only cover 19% of the treatment volume. If the central tandem is loaded with cesium-I 37 sources, as was the case in most of our implants, the inhomogeneity of dose will increase. Adding two 10 mgm cesium-137 sources to the central tandem, the maximum dose rate will nearly double (150 rad per hour) and would occupy 25% of the treatment volume. Such inhomogeneities are thought to be undesirable in interstitial implants. Fletcher and Stoval16 gave high priority to the avoidance of such regions of overdosage. They retrospectively reviewed 157 patients who had implants for oral cavity carcinomas at the M.D. Anderson Hospital and Tumor Institute and found that one-half of the instances of necrosis occurred in regions of over- dosage, as shown on the isodose contours. Their recom- mendation was that isodose contours should be routinely made through various planes of the implant and that dosage inhomogeneity should be sought and corrected during the time of treatment.
We recommend that when Syed-Neblett type implants are used, the central tandem not be loaded with cesium- 137 or radium-226 sources. Doing so only increases the dosage inhomogeneity in the treatment volume and places the patient at risk for late complications. A separate implant, using the tandem only, can be planned at a later time. When the radiotherapist knows the approximate volume of the implant, i.e., the number of ribbons and seeds to be used, the implant can be pre-planned using computerized dosimetry. Areas of overdosage or inhomo-

lYO2 Radiation Oncology 0 Biology 0 Physics December 1983, Volume 9, Number 12
geneity can be discovered on pre-planning dosimetry and corrected. Once the actual implant has been accom- plished, its dosimetry can be reviewed for the percentage hot spot. If the percentage hot spot is significant, i.e. 20% or above, the dose rate within the implant can be altered by replacing ribbons. Lower individual seed strength ribbons may be used in the interior of the implant to make the dose distribution more homogeneous. This differential loading technique has been previously described by the authors.3
The Syed-Neblett template is unique in that it allows us to treat larger pelvic volumes than are possible using either the Fletcher or Manchester systems. It is certain that inhomogeneities in this large volume can have delete- rious effects, and possibly, that high dose rates may contribute indirectly to the incidence of complications. In contrast to other implants used in our institution, the Syed-Neblett template was usually loaded so as to deliver a dose rate of 100 cGy per hour or more to the treatment volume (Table 6). The median dose rate used at UNMH for tongue implants using iridium-192 was 40 rad per hour; the median dose rate used in breast implants was the same. In our patients with cervical carcinoma treated with the Fletcher system applicators, the range of dose to Tod’s point A was only 30 to 60 cGy per hour (Table 7). Our complication rates for these implants are signifi- cantly lower than those found in our template series. With our method of analysis, we did not see a direct correlation between the dose rates and subsequent complications. However, it is customary in the practice of brachytherapy to maintain a dose rate of 30 to 50 cGy per hour in large volume implants. In the period studied our institutional bias was toward the use of high dose rates in templates. In spite of the lack of association between complications and dose rates, we do not now use or recommend high dose rates in gynecological implants. We did not find any
Table 6. Characteristics of implant dosimetry
cGy per hour in No. of Seed strength mgms. No. of treatment volume patients radium equivalent patients
40 50 60 70 80 85 90
100 105 II0 120 150
1 1 1 I 2 1 2
I2 1 1 4 1
Total 28
.27 1
.32 2
.33 2
.35 I
.37 2
.38 I
.40 4
.4l 2
.42 I
.43 2
.44 4
.45 1
.46 2
.47 I
.52 I
.57 I
Total 28
Table 7. Comparison of prescribed dose rate using Fletcher-Suit tandem and ovoids with Syed-Neblett implants
Dose rates in cGy/hr. Fletcher-Suit Syed-Neblett
40 48 1 50 32 I 60 3 I 70 1 80 2 85 I 90 2
100 - 12 I05 I II0 1 120 4 I50 1
83 28
(I 9/28,68%, 2 100 cGy/hr)
significant influence of the total dose from external irradiation on the complication rate in patients who received a Syed-Neblett template (Table 8).
Pitts and Waterman reported a similar interstitial technique of using radium needles for the irradiation of both the cervix and parametrium, in the late 1930’~.~ These authors treated Stage I through Stage IIB (modern FIG0 staging) cervical cancer by freehand implantation of radium needles into the paracervical and parametrial tissues. This was combined withthe concurrent use of a radium capsule in the cervical canal-so as to deliver a dosage of 3300 mg hours in the cervical canal and 6000 mg hours in the parametrium. By the use of this tech- nique, they were able to increase five year survivals for Stage IIB patients from 14.0% in the 1921-1925 cohort to 33% in the 1931-1933 group. Out of a total of 480 patients (1926-I 938) 38, or 7.9’%, developed fistula. They were able to reduce their fistula incidence by the use of lower intensity needles, longer treatment times (144 to 168 hours) and lower dose rates. They added little, if any, external irradiation. These authors felt that too close an interval between the internal and external irradiation could result in fistula formation and that “overtreatment can spoil good results as easily as undertreatment.”
Table 8. Logistical analysis of complications
Variables analyzed
Dose from iridium- 192 implant(s) Dose Rate in prescribed volume of template Number of seeds in implant Radium equivalent (total of Ir’92 + Cs”‘) Individual iridium seed strength Template volume % area of “Hot Spot” in template External XRT dose (total of cGy) Iridium- 192 in obturator ring trochars Tandem loaded with Cesium- 137 Number of seeds per ribbon
P
0.73 0.61 0.95 0.80 0.89 0.65 0.06 0.87 0.23 0.98 0.19

The results of our analysis have led us to use cautious selection of patients for template. We prefer to use the template in patients with central, moderate volume dis- ease. Pre-planning computerized dosimetry is a must for the selection of optimal iridium seed strength and ribbon number. Dose inhomogeneity, or hot spots, should be corrected after viewing the dosimetry from the actual implant. The concept of the Syed-Neblett template is a logical extension of techniques developed in an older and larger series using radium, and it appears to standardize and make reproducible a volume implant of the cervix and parametria.
The treatment of bulky, locally advanced cervical or vaginal cancer still represents a formidable therapeutic problem, not only because local control is suboptimal, but also, because of the high incidence of distant failures. In our experience, the Syed-Neblett interstitial volume implant has not improved our results and we no longer use it in the treatment of large bulky gynecologic malignan- cies. However, this therapeutic modality may have a place in the treatment of small to moderate volume disease
confined to the central pelvis, for example Stage IVA central carcinoma of the cervix or vagina. The volume implant may also be of benefit to the patient with small to moderate volume disease and a distorted vaginal anato-
my. If the Syed-Neblett interstitial implant is to be used,
careful attention should be placed in the analysis of the different factors involved in this modality of treatment. The dose from iridium-l 92 implant, dose rate in pre- scribed volume of template, number of seeds in implant, radium equivalent (total of lr19* + CS’~‘), individual iridium seed strength, template volume, percent area of “hot spot” in template, external XRT dose (total of cGy), iridium-l 92 in obturator ring trochars, tandem loaded with cesium- 137, and number of seeds per ribbon must be taken into consideration in the treatment planning of patients treated with the Syed-Neblett interstitial tem- plate.
Guidelines for the use of the Syed-Neblett volume interstitial implant in gynecologic malignancies will be the subject of an upcoming paper from our institution.
Syed template in gynecology 0 F. AMPUERO et al. I903
REFERENCES I. Cox, D.R.: The Analysis of Binary Data. London,
Methuen, 1970. 2. Delcos, L., Fletcher, G.H., Moore, E.B., Sampiere, V.A.:
Minicolpostats, dome cylinders, other additions and improvements of the Fletcher-Suit Afterloading System: Indications and limitations of their use. Int. J. Radiat. Oncol. Biof. Phys. 6: I 195-l 206, 1980.
3. Doss, L.L., Lake, D.: Dosimetry in Syed Implants. Abstracts of papers for the Winter Meeting of the Ameri- can Endocurietherapy Society, Wailea Beach, Maui, Hawaii, December 9-1 I, I98 1, p. 14.
4. Feder, B.H., Syed, A.M.N., Neblett, D.: Treatment of extensive carcinoma of the cervix with the “transperineal parametrial butterfly.” Int. J. Radiat. Oncol. Biol. Phys. 4: 735-742, 1978.
5. Fleming, P., Syed, A.M.N., Neblett, D., Puthawala, A., George, F.W., III, Townsend, D.: Description of an after- loading ?r interstitial-intercavitary technique in the treat- ment of carcinoma of the vagina. Obstet. Gynecol. 55: Z-530, 1980.
6. Fletcher, G.H., Stovall, M.: A study of the explicit distribu- tion of radiation in interstitial implantations. Radiology 78: 766-782, 1962.
7. Hiilesmaa, V.K., Vesterinen, E., Nieminen, U., Grohn, P.: Carcinoma of the uterine cervix Stage 111: A report of 3 1 I cases. Gynecol. Oncol. 12: 99-106, 198 I.
8. Kagan, A.R., Nussbaum, H., Gilbert, H., Chan, P.Y.M., Rao, A., Saltz, A., Tawa, K., Wollins, M.D.: A new staging for irradiation injuries following treatment for cancer of the cervix uteri. Gynecol. Oncol. 7: 166-l 75, 1975.
9. Pitts, H.C., Watterman, G.W.: Report of results of radium treatment of carcinoma of cervix. Am. J. Obstet. Gynecol. 20: 607-611, 1930.
IO. Piver, M.S., Chung, W.S.: Prognostic significance of cervi- cal lesion size and pelvic node metastases in cervical carci- noma. Obstet. Gynecol. 45: 507-5 IO, 1975.
I I. Rosen, I.I., Lane, R.D., Kelsey, C.A.: Computation of dose distribution for radioactive seed implants. Acta. Radiol. Oncol. 19: 41-44, 1979.
12. Watterman, G.W., DiLeone, R., Tracy, E.: The use of long interstitial radium needles in the treatment of cancer of the cervix. Am. J. Roentgenol. 57: 67 l-678, 1947.
13. Wharton, J.T., Jones, H.W., III, Day, T.G., Jr., Rutledge, F.N., Fletcher, G.H.: Preirradiation celiotomy and extended field irradiation for invasive carcinoma of the cervix. Obstet. Gynecol. 49: 333-338, 1977.