
The Strama model and successful improvement of antibiotic...
75
The Strama model and successful improvement of antibiotic prescription in Sweden There are no conflicts of interest Christina Åhrén and Lars Blad Strama Region Västra Götaland och Strama Västernorrland
Transcript of The Strama model and successful improvement of antibiotic...

The Strama model and successful improvement of antibiotic prescription in Sweden
There are no conflicts of interest
Christina Åhrén and Lars Blad
Strama Region Västra Götaland och Strama Västernorrland

The Swedish strategic programme against
antibiotic resistance
“ tighten things up”
National collaboration network
against antibiotic resistance
with the goal to preserve the effectiveness
of available antibiotics.

We can not stop but we hope
to halt antibiotic resistance development
- important steps!
Good hygiene
Use antibiotics
according to guidelinesReduce infection rates

.Sid
Outpatient use of Antibiotics in Europe 2009Packages per 1000 inhabitants per day (PID)
Adriaenssens N et al. J Antimicrob Chemother, 2011

goal: 250 prescriptions/inhabitants and year
Successful reduction in most age groups
and counties since 2010

www.lvn.se
Swedish STRAMA as an example of Successful Control of Antibiotic Use
Lars Blad
Dep Med Officer for Comm Disease Control,
Senior Consultant Infection Control,
Chairman STRAMA Committee,
Västernorrland County;
Member of Swedish Strama Nat:l Boards;
WHO EURO Consultant on work against AMR

Sweden has a comparatively favourable situation regarding antibiotic resistance
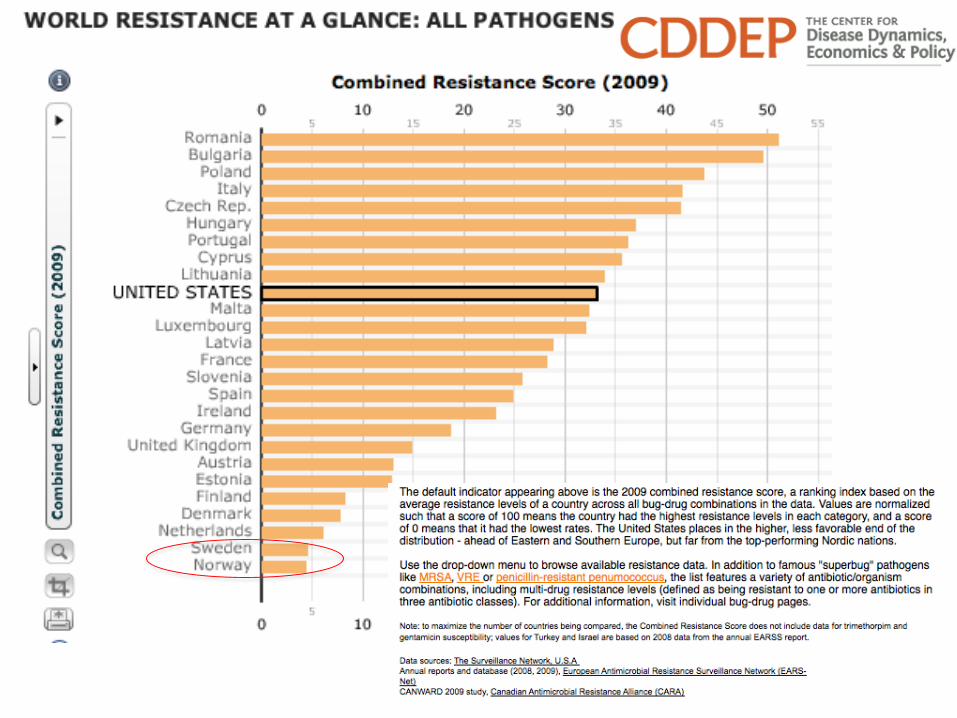

Peace >200 years..

Antibiotic
pressure
Survival and spread of
antibiotic resistant bacteria
Poor Hygiene &Infection Control
The two main factors we can influence
to reduce ABR in human health care:
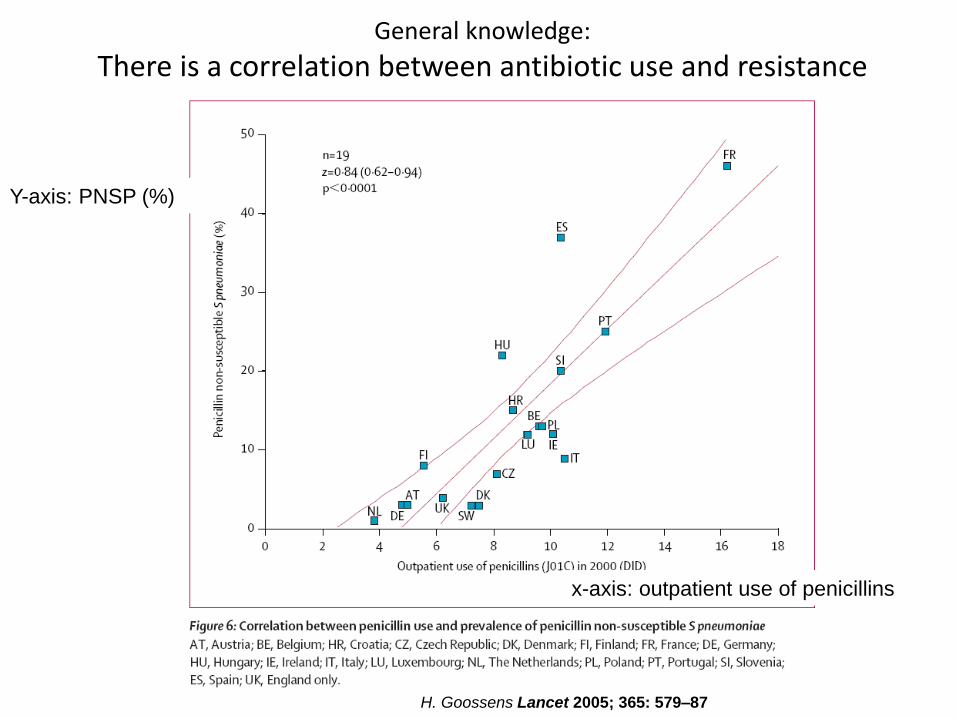
General knowledge:
There is a correlation between antibiotic use and resistance
Y-axis: PNSP (%)
x-axis: outpatient use of penicillins
H. Goossens Lancet 2005; 365: 579–87

All age groups
0-4 year
Prescriptions/1000 inhabitants and year
1987-2014


Antibiotics (J01 excl. methenamine) in the Nordic countries1978-2013total sales, DDD/1000 inhabitants and day

The Swedish Experience
The Swedish Strategic Programme
Against Antibiotic Resistance
http:// www.strama.se
Founded in 1995. The remit from the Government
is to collaborate interdisciplinary on issues
aiming to preserve the effectiveness of antibiotics.

•
•
•
Sigvard Mölstad, Professor
and PHC clinician
”Champions”..

Strama AdvisoryCouncil -
experts
SwedishMedical
Association
National Board of Health and Welfare
SwedishVeterinaryInstitute
SwedishAssociation of
Local Authoritiesand Regions
MedicalProducts Agency
The Dental and PharmaceuticalBenefits Agency
European Centre for Disease
Prevention and Control
Network of local Strama groups
Swedish Institutefor CommunicableDisease Control
Political level
Professional organizations
Stramacoordination and feedback
Exchange ideas - What
works?
- Web page
- Larger yearly meetings

Early demand-driven development
of surveillance systems
ABR:
• ResNet (1994/2002)
• EARSS/EARS-Net
• SmiNet (notifiables)
• SveBar
AB use:
•PHC: ”Week 47” (2000)
– PRIS/RAVE
– ”PV-quality”
•Hospital: PPS (2003)
– SAI/Anti-Infection Tool
•/ESAC, ESAC-Net/
•Individual drs data
feedback (2012)

www.lvn.se
What has Strama done/contributed to?• Monitored and analyzed ABR and AB use
• Updated guidelines
• Implemented guidelines
• Set goals: pcV, quinolones, 250..
• Education campaigns: childrens day care, child health, LTCF/care for the elderly..
• Monitoring of complications
• System for diagnosis related AB prescription, hospitals..
• Information to media, public, politicians
• Broadening to multiple sectors of society
• Bacteria have no borders..
19


Example 1: pneumococci
• Signal/starting point: 90’s, alarming
increase of R in Southern Sweden
• Action necessary, broad measures:
– Decrease ab pressure!
• Strama network is formed 1995
– Reduce spread!
• PRP: mandatory reporting, tracing, containment
measures
• ”Anti-infection prophylaxis” for pre-school children

Fluoroquinolone-Resistant E.coli in Europe, 2001-2006
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
NO
(1
11
7)
EE
(1
16
)
SE
(2
90
4)
FI
(15
43
)
IS (
99
)
NL
(2
14
0)
FR
(4
61
0)
GR
(9
50
)
SI
(52
6)
HR
(5
27
)
BE
(1
11
8)
LU
(1
91
)
UK
(1
87
9)
PL
(1
53
)
IE (
11
84
)
AT
(1
33
6)
CZ
(1
80
9)
BG
(1
55
)
HU
(7
23
)
IT (
82
6)
IL (
86
2)
PT
(7
54
)
ES
(2
81
6)
DE
(1
04
0)
MT
(8
4)
CY
(5
7)
RO
(4
7)
TR
(7
82
)
Country code (average number of isolates reported per year)
% f
luo
ro
qu
ino
lon
e r
esi
sta
nce
2001
2002
2003
2004
2005
2006
Example 2: fluoroquinolone resistance in E. coli

ResNet 2007: E.coli
27
1,22,7
1,1
12
17,5
0
5
10
15
20
25
30
Ampicillin Mecillinam Cefadroxil Nitrofurantoin Quinolone * Trimethoprim
% R
1996
1997
1999
2001
2002
2003
2004
2005
2006
2007

The continuous work of the Strama group
Hospitals, Clinics,
PHC C:s
Pharmacy,Bact. lab,
Strama group
Prescription
of AB:s /changed/
Local data
on ABR, and
AB use
Feed back of data;
interventions
Resistance
is influenced
Cultures are
taken
Gathering of
data
Analysis
Epid.Int.
Lars Blad, 2009

Figure by Ulf Lindahl, Strama Västernorrland
Kirurgkliniken, Sundsvall, antibiotika på recept
0
500
1000
1500
2000
2500
3000
2006-
KV1
2006-
KV2
2006-
KV3
2006-
KV4
2007-
KV1
2007-
KV2
2007-
KV3
2007-
KV4
2008-
KV1
2008-
KV2
2008-
KV3
2008-
KV4
DDD (definierade dygnsdoser)
J01MA02 - ciprofloxacin
J01CF05 - flukloxacillin
J01FF01 - klindamycin
J01AA02 - doxycyklin
J01CE02 - fenoximetylpenicillin(pcV)
J01CA04 - amoxicillin
J01AA04 - lymecyklin
J01EE01 - sulfametoxazol +trimetoprim
J01MA06 - norfloxacin
J01CA08 - pivmecillinam
J01AA07 - tetracyklin
J01EA01 - trimetoprim
Surgical clinic, Sundsvall hospital, antibiotic prescriptions
2006 - 2008D
DD
, D
efined D
aily
Doses

Kinoloner (J01M), totalt (recept och rekvisitioner)
0,0
0,2
0,4
0,6
0,8
1,0
1,2
1,4
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 (jan-
aug)
DDD / 1000 inv / dag
Riket
Västernorrland
Figure by Ulf Lindahl, Strama Västernorrland
Fluoroquinolone use (J01M), total (prescriptions and requisitions) D
DD
/1000 inhabitants
/day
Sweden
Västernorrland

Sales of antibiotics commonly used to treat lower urinary
tract infections in women (sales on prescriptions), age 18-79 years,
2000-2013, prescriptions/1000 women and year; Sweden
New recommendations from
MPA and Strama

National Guidelines”common infections in out patients”
bySwedish Medical Product Agency
StramaSwedish CDC (today Public Health Agency)
AOM, 2000, updated 2010
Tonsillitis 2001, updated 2012
Sinusitis, 2003
Lower UTI, 2007
Lower RTI, 2008
Skin infections, 2009
Early warning signs of serious infections in children, 2011 Acne, kol……
Slide: courtesy Prof. S Mölstad


Hospital admissions for acute mastoiditis, quinsy, and acute rhinosinusitis in children were stable or decreased 1987-2004
Data from the national registry of diagnosis in hospital care (National Board of Health and Welfare)Lancet Infect Dis 2008; 8: 125–32
Strama campaign Strama campaign
Strama campaign Strama campaign

www.lvn.se
Important success factors:
• Local engagement – energy from patient contacts
• Multidisciplinary composition of groups; at local and national levels
• Media exposure – public and decisionmakers informed
• Network – bottoms-up, top-down, and LATERAL sharing
• Regularly updated, evidence-based national guidelines, concentrated and brought to the prescriber in and end-user friendly format; including peer-to-peer discussions in small groups

.Sid
Mandatory notification of AMR of particular concern according to communicable diseases act
Lab + clinical notification within 48 hours
14/04/201632
0
1000
2000
3000
4000
5000
6000
7000
8000
MRSA ESBL VRE PNSP
To
tala
an
tale
t a
nm
äld
a f
all
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012

www.lvn.se

Hip replacement
Organ transplants
Cancer chemotherapy
Intensive care
Care of preterm babies
Modern medicine is not possible without effective antibiotics

www.folkhalsomyndigheten.se/ www.reactgroup.org/
www.strama.se
THANK YOU FOR YOUR ATTENTION – find out more at:

Local experience
Strama
Region Västra Götaland
Christina ÅhrénMD, PhD
[email protected] www.vgregion.se/strama

300 km
• 1,6 million inhabitants
• < 1 million Gothenburg area
• 49 counties
• 4 major hospitals
• 200 PHCC
• 50 % private
• 50 % Gothenburg area
Region Västra Götaland

Strama Region Västra Götaland
Part of the Regional Patient Safety Unit
• General practioner (GP)
• Infectious diseases
• Medical officer
• Infection control
• Clin. Microbiology
• Pharmacists
+ local network
7 persons, part time

Strama - ”network”
Local
Strama
Local
Strama
Local
Strama
Local
Strama
local
pharmaceutical
committee
pharmacists
Various
specialist within
Infectious
diseases
Public, Patients, Media
Prescribers
• Primary care• Hospital care
• Dental care
• Veterinarians
Management
Politicians
Regional
Strama

We can not stop but hope
to halt antibiotic resistance development
- important steps!
Good hygiene
Enhance
compliance to
guidelinesReduce infection rates

Unaltered prescription rates in most counties
until start of national patient safety initiative 2011

Others
Prescription in hospitals, dentists etc
Total prescription
Prescription in primary care
Antibiotic prescription in different settings
in Region Västra Götaland 2011-2015 prescription/1000 inhabitants, last 12 months

405 31123 %
23 % reduction in prescriptions rate 2012-2015prescription/1000 inhabitants and year

Perscription/1000 inhabitants and yearseptember 2012
(range: 492 – 315)
Perscription/1000 inhabitants and yeardecember 2015
(range: 385 – 248)

Antibiotic prescription in different counties
in Region Västra Götaland 2012 and 2015 prescription/1000 inhabitants and year

Over prescription for respiratory tract infections,
mostly in primary care
Primary care
65%
RTI
UTI
SSTI

Increase awareness about updated guidelines!
>2000 down-loads + webbversion!
Increase
compliance!Common infections
in PHC

Simplify guidelines, acute tonsillitis
Poster and pocket version

Lifesaving• Meningitis
• Sepsis
• Pneumonia
• Erysipelas
• Pyelonephritis
No effect• Common cold
• Tonsillitis, neg for GAS
•Acute bronchitis
Reduce symptoms• Lower UTI
• Tonsillitis (3/4 Centor)
+ pos Strep A
Minor/no effect?• Clinical maxillary sinusitis
• Sore throat (<3 Centor)
•Acute otis 1 - 12 years
Reduce complications• erytema migrans (borrelia)
• STI
•Acute otitis < 1 år
• some skin infections
How sick is the patient -
– will he/she benefit from antibiotics?
aim: cure – relieve – comfort – not harm

”Strama–GPs” visit
primary healthcare centres (PHCC)
Inform about:
• Threat of resistance
• Updated guidelines (RTI)
• Prescription at the PHCC
• All personnel
• All 200 PHCC
two years
“Strama – doctor”
GP

One Strama-doctor
on each PHCC
Responsibility for the local process
Strama´s extended arm
Strama has to facilitate their work!

Educated 1-2 times/year
• work-shops
• seminars
Fed 2-3 times yearly
• comparative prescription data
• educational material
Certain tasks
Yearly report:
• how do we perform
• suggestions fore
improvementsreimbursement
feedback
Strama-doctors

Participants
• all doctors and management
• < 30 min/session
Reflect on prescription patterns
• Their prescription in relation to other PHCC
• Individual prescription in relation to one`s colleagues
• antibiotics per se
• antibiotics in relation to infectious diagnoses
• Medical records reed by a colleagues
Educational group discussion with colleagues

• quarterly
• easily interpreted
• PHCC names given
Ten with the
highest and lowest
rates highlighted
Comparative prescription data

Factors affecting prescription
patterns
• Patient population: age, comorbidity
• Seasonal variation: flue tourist effect
• Drop – in
• Organization at the local PHCC
• Economic reimbursement systems
• Locums
• etc

D. Tell BMJOpen 2015
Prescription rates for acute bronchitis
in patients < 50 years
0%
10%
20%
30%
40%
50%
60%
AT-läkare ST-läkare Yngre DL Äldre DL Hyrläkare TotaltYoung doctors Old GP Locums Total

Case discussions
• new treatment guidelines
• include nurses
One of several optional alternatives• quiz
• e-learning about antibiotic resistance, cases
• education session fore other health care personnel
• inform temporary locums
Discussion!
Educational group discussion with colleagues

Case discussionsCases with questions and manuals
www.vgregion.se/strama

Power-points with manuals for education
www.vgregion.se/strama
Acute otitis media Acute tonsillitis

Strama-Quiz
– Short case reports
– Follow up with discussion
– Check locums
– Include nurses
1 X 2
Fall A.
Anton som är 25 år och tidigare frisk söker vårdcentralen med halsont sedan två dagar tillbaka. Han har ingen
hosta eller snuva. Det gör ont när han sväljer men han kan äta och dricka. Han är helt opåverkad och har temp
38,1 °. Vid inspektion av mun och svalg ses rodnade tonsiller med beläggningar. Inga palpabla lymfkörtlar på
halsen.
1. Hur många Centorkriterier har Anton?
1. 2
X. 3
2. 4
2. Ska vi ta några prover?
1. Strep-A-test
X. Strep-A-test och CRP
2. Inga prover behövs
3. När rekommenderas antibiotikabehandling vid faryngotonsillit?
1. Vid 4 Centorkriterier
X. Vid positivt strep-A-test
2. Vid 3-4 Centorkriterier och positivt strep-A-test
Fall B.
Emma är 32 år och tidigare frisk. Hon söker vårdcentralen med hosta sedan två veckor. Hon röker inte. Hon har
gula upphostningar men är opåverkad och afebril. Ingen andningspåverkan. Hon har andningsfrekvens 18/minut,
spridda liksidiga biljud vid lungauskultation, i övrigt är status normalt.
4. Vad gör du?
1. Tar CRP för att bedöma behov av antibiotikabehandling
X. Exspektans
2. Ordinerar antibiotika eftersom hon har gula upphostningar och förloppet är långdraget
5. Hur länge pågår hostan i genomsnitt vid en akut bronkit?
1. Tre veckor
X. Två veckor
2. En vecka
6. När har antibiotika effekt vid en akut bronkit?
1. Om bronkiten orsakas av en bakterie
X. Om bronkiten orsakas av mycoplasma
2. Antibiotika har ingen effekt vid akut bronkit
Fall C.
Elias som är 2½ år gammal kommer till vårdcentralen pga värk i båda öronen sedan igår. Han är förkyld och
hostig sedan 3-4 dagar, idag temp 39,1°. Han har haft en akut mediaotit (AOM) för ett år sedan, för övrigt frisk.
Han leker i väntrummet. Status: Opåverkad. Båda trumhinnorna är ogenomskinliga, färgförändrade, buktande
och rör sig inte vid siegling.
7. Vad gör du?
1. Förskriver antibiotika
X. Exspektans, information
2. Exspektans, information, planerat återbesök om 2 dagar
8. Vad skulle du ha gjort om Elias varit 1½ år gammal?
1. Förskrivit antibiotika
X. Exspektans, information
2. Exspektans, information, planerat återbesök om 2 dagar
Fall D.
Martin 29 år har varit förkyld i en vecka och har gul, tjock snuva. Sedan igår har han fått värk över båda
kinderna. Han har temp 37,5° och har inte tagit någon analgetika. Värken ökar när han böjer sig framåt. Han är
frisk för övrigt och är på jobbet (kontorsarbete).
9. Vad gör du?
1. Remitterar patienten för radiologisk undersökning
X: Förskriver antibiotika i sinuitdos
2. Exspektans, symtomlindrande behandling
Fall E.
Sara är 42 år och söker med typiska cystitsymtom. Hon är i övrigt frisk, inte gravid och har inte feber,
flanksmärta eller genitala symtom.
10. Vilken är den avgörande faktorn för att erbjuda antibiotikabehandling?
1. Resultatet av urinstickan
X. Graden av besvär
2. Alla kvinnor med cystit bör antibiotikabehandlas

90 %
Become an antibiotic smart doctor !
(e-learning from Strama Stockholm + SALAR)

www.vgregion.se/strama
e-learning
Yearly summery
of all reports
from PHCCs
Important
knowledge
base
www.vgregion.se/strama

Reports 2013-2015
• 92-86 % (178-186/200) PHCC reported
• >1000 doctors/year participated in an educational group discussion
• two case discussions
• prescription patterns
• 2015: >700 doctors did the quiz

Report 2015
• Medical records exchanged, read and discussed
• voluntary
• 3 notes/doctor 15 minutes
• all should read
• 60% of PHCC chose this option
• >2000 visits for ID were read
• median: 15 ( 6-150) ID visits

Conclusions from reports
• There is still a need for increased
knowledge about updated guidelines
• Educational group discussions appreciated
• comparative data engage
• awareness of one`s (unknown) behavior
• reading records positive

Conclusions from reports
“It is not only about doctors”
• Everybody has to "talk the same language”
with the patients• receptionist doctor must be educated
• Structural factors at the PHCC are of great
importance
• ”do not see the doctor unless necessary”
• reduce patient drop-in, nurse triage
• local guidelines agreed upon
• continuity in staff employment
• management

Education – not only doctors!
> 2000 persons!
Nurses in LTCFNurses in PC
Dentists

Well informed patients are important!National patient information – several languages

Patient information material
www.antibiotikaellerinte
Child health care
Västerbotten HallandStockholm + SALAR
Elderly health care

www.vgregion.se/strama
Patient
informations,
Posters
to order for
free
Movie

Factors for success• Joint national initiative
• Local management back-up
• Top, including politicians PHCC
• Economic incentives
• Worked with the local PHCC/”Strama -
doctors”
• Facilitate the local process, keep it simple!
• Alert continuously
• Joint enemy, important to defeat

Upcoming challenges
• Keep the good work going in PHC
• Lack of time and staff
• Demand for high availability
• Follow complication rates
• Increase compliance in hospital care

Thank you for the attention!

Media campaign – no long-lasting effect !


















