The Spleen and Splenomegaly
20
Clarissa Gurbani Year 3 Medical Student University of Manchester
-
Upload
meducationdotnet -
Category
Documents
-
view
314 -
download
5
Transcript of The Spleen and Splenomegaly
Clarissa GurbaniYear 3 Medical StudentUniversity of Manchester
Length – approx 12cm (5 inches) in adults Weight – approx 160 g Colour – deep red Position
◦ Between 9th to 11th ribs on left side
◦ Splenic artery From coeliac trunk (T12), a branch of the abdominal
aorta Branches into trabecular arteries Further branches surrounded by white pulp Capillaries discharge blood into red pulp
◦ Splenic vein Joins SMV to form hepatic portal vein
Gastrosplenic ligament◦ Broad band of mesentery◦ Attaches spleen to lateral border of stomach
Surfaces◦ Diaphragmatic – smooth and convex◦ Visceral – i.e. conforming to shape of:
Stomach (gastric area) Left kidney (renal area)
Hilum◦ Pt of communication of splenic vessels with spleen◦ Groove that marks border between gastric and
renal areas.
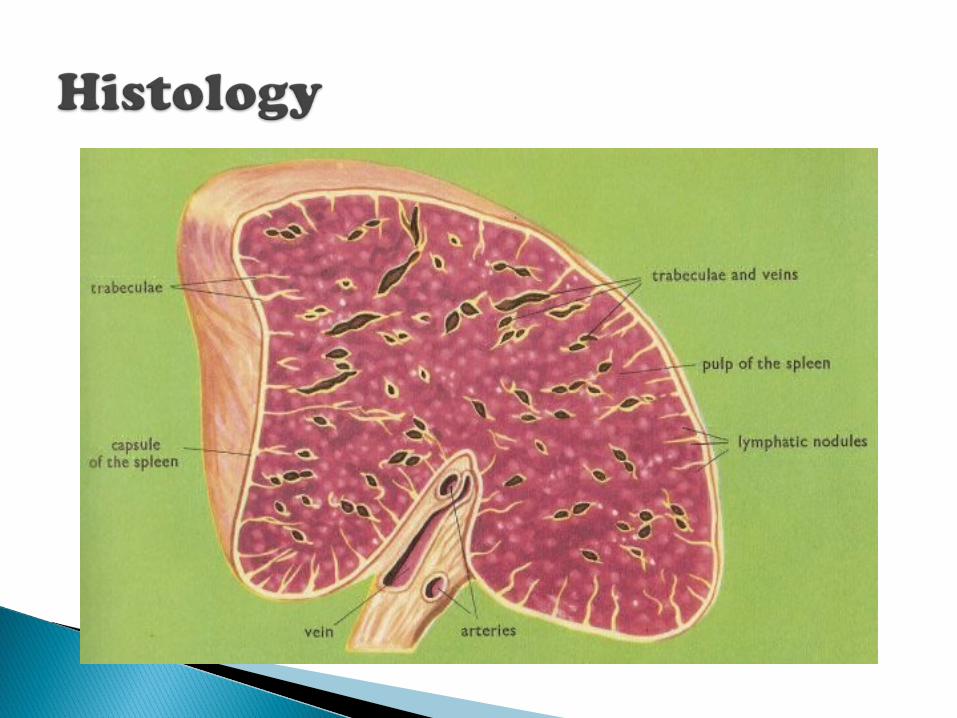
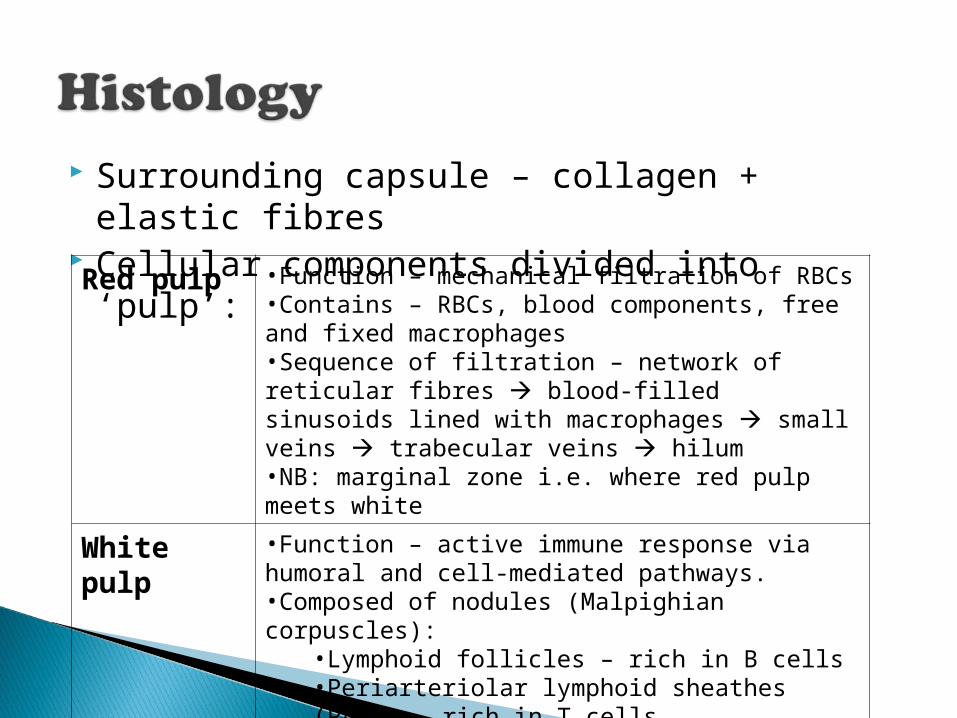
Surrounding capsule – collagen + elastic fibres
Cellular components divided into ‘pulp’:Red pulp •Function – mechanical filtration of RBCs•Contains – RBCs, blood components, free and fixed macrophages•Sequence of filtration – network of reticular fibres blood-filled sinusoids lined with macrophages small veins trabecular veins hilum•NB: marginal zone i.e. where red pulp meets white
White pulp
•Function – active immune response via humoral and cell-mediated pathways.•Composed of nodules (Malpighian corpuscles):
•Lymphoid follicles – rich in B cells•Periarteriolar lymphoid sheathes (PALS) – rich in T cells
1. Removal of abnormal RBCs and other blood components (via phagocytosis)
2. Fe storage (recycled from RBCs)3. Initiation of immune responses by
B and T cells in response to circulating antigens
Cannot get above it (ribs overlie the top) Dull to percussion (kidneys are resonant
due to underlying bowel) Moves more with inspiration towards RIF Medial notch
Causes can be divided into:◦ Infective◦ Haematological◦ Neoplastic
Also can be grouped with associated features◦ Fever◦ Lymphadenopathy◦ Purpura◦ Arthritis◦ Ascites◦ Murmurs◦ Anaemia◦ Weight loss and CNS signs◦ Massive
Infection ◦ Malaria◦ SBE/IE◦ Hepatitis◦ EBV◦ TB◦ CMV◦ HIV
Sarcoid Malignancy
Glandular fever (mono)◦ Aka infectious mononucleosis◦ Secondary to EBV infection
Leukaemias, lymphoma Sjogren’s syndrome
◦ Xerostomia (dry mouth), xerophthalmia (dry eyes)◦ Another cause of xerophthalmia? – Vit A
deficiency
Septicaemia Typhus DIC (Disseminated Intravascular
Coagulation) Amyloid Meningococcaemia
Sjogren’s syndrome RA and SLE Infection e.g. Lyme Vasculitis, Behcet’s
Carcinoma Portal HTN
SBE/IE Rheumatic fever Hypereosinophilia Amyloid
Sickle-cell Thalassaemia Leishmaniasis Leukaemia Pernicious anaemia
◦ Lack of secretion of intrinsic factor (IF) from gastric oxyntic cells, which is needed for B12 absorption
POEM (polyneuropathy, organomegaly, endocrinopathy, M-protein banding)
Cancer, lymphoma TB Arsenic poisoning Paraproteinaemia
Malaria Leishmaniasis Myelofibrosis Chronic myeloid leukaemia Gaucher’s syndrome
The Oxford Handbook of Clinical Medicine, 8th edition
Martini’s Fundamentals of Anatomy and Physiology, 8th edition
Macleod’s Clinical Examination, 12th edition
Thank you!