The Science Behind The LSE ® Noise Barrier System Sound-Absorptive Performance.

PP-GIP-GBR-2692 Date of preparation: October 2017 1
The science behind ACRODAT®
ACRODAT® is an interactive software medical device that can help physicians evaluate disease activity in patients with acromegaly. These pages provide an overview of the concepts and scientific basis behind ACRODAT®.
1. What are the challenges in the treatment of acromegaly? Despite the availability of multimodal treatment options for acromegaly, achievement of long-term disease control is suboptimal in a significant number of patients.1 Furthermore, disease control as defined by biochemical normalisation may not always show concordance with disease-related symptoms or the patient’s perceived quality of life.2–4 Recently, several treatment guidelines have addressed the criteria for assessment of disease activity.5,6 The consensus on criteria for cure defines active disease as 1) a random GH >1 μg/L and nadir GH after OGTT ≥0.4 μg/L, 2) elevated IGF-I and 3) clinically active. A definition of the term “clinically active” is not provided.7 GH and IGF-I are key biochemical parameters to assess disease activity in acromegaly, but the variability in assay performance and broad normal ranges may limit their predictive value of disease control. Even when achieving biochemical control, patients may still experience disease-specific symptoms such as soft tissue swelling, perspiration, and a generally reduced health status and quality of life.2–4 The patients’ own perspective of their health status may, therefore, be an important additional measure to assess the level of disease activity and for clinical decision making.
2. Development of ACRODAT®: Acromegaly Disease Activity Tool ACRODAT® uses five disease-specific parameters to assess disease activity in acromegaly: IGF-I, tumour size, comorbidities, symptoms and quality of life (see Section 3). These parameters were identified by a panel of 10 experts in the field of endocrinology, neurosurgery and acromegaly management following a rigorous selection process. Each parameter was defined by the panel at three levels of severity (see Table 1):
Level 1 = The patient is adequately controlled;
Level 2 = The patient shows mild disease activity, further evaluation of the patient’s condition is needed;
Level 3 = The patient shows significant disease activity requiring clinical action. Table 1: Five selected parameters and their level of severity
Health Status Parameter Parameter Levels
IGF-I
1 = The patient’s IGF-I is within normal limits 2 = The patient’s IGF-I exceeds the upper limit of normal but not more than 1.2X the upper limit of normal, or is below the lower limit of normal 3 = The patient’s IGF-I is significantly elevated, more than 1.2X the upper limit of normal

PP-GIP-GBR-2692 Date of preparation: October 2017 2
Health Status Parameter Parameter Levels
Tumour status
1 = Based on the most current MRI, the tumour is not visible or has not changed since the prior MRI 2 = Based on the most current MRI, a slight increase in tumour size (≤ 20%) has been observed 3 = Based on the most current MRI, a clinically significant increase in tumour size (>20%) and/or invasiveness has been observed over the prior MRI and/or a worsening in vision is observed
Comorbidities
1 = The patient does not have a diagnosis of diabetes, complaints of sleep apnoea are absent and cardiac disease (if present) is well controlled 2 = The patient has diabetes that is controlled by therapy with no concomitant complaints of sleep apnoea, and cardiac disease (if present) is controlled with therapy OR, the patient does not have diabetes but has complaints of sleep apnoea and/or cardiac disease that is not well controlled with therapy 3 = The patient has diabetes that is not well controlled by therapy OR the patient has diabetes that is well controlled, with complaints of moderate to severe sleep apnoea and/or uncontrolled cardiac disease
Symptoms
1 = Mild: The patient reports no or only mild symptoms on the Signs and Symptoms score (SSS), all symptoms rated ≤ 2 2 = Moderate: The patient reports the presence of some symptoms on the SSS but no single symptom exceeds a score of 6 (mild to moderate) and the mean score is ≤ 4 overall 3 = Severe: The patient reports significant symptoms on the SSS with the mean score > 4 OR one or more symptoms rated > 6
Health-related quality of life impairment*
1 = The patient reports no or minimal impairment in quality of life (total score ≥ 60) 2 = The patient reports mild to moderate impairment in quality of life (40 ≤ total score < 60) 3 = The patient reports significant impairment in quality of life (total score < 40)
*The experts selected ACROQoL as the most suitable currently available tool to address disease specific QoL assessment. In order to avoid bias, the term ‘Health-related quality of life’ was used in the validation study.
The five parameters and three levels within each parameter produced a total of 243 (35) possible patient profiles or scenarios. These patient scenarios were then used to evaluate their predictive validity in a separate cohort of endocrinologists routinely managing patients with acromegaly in their clinical practice (validation study). A total of 21 endocrinologists from Canada, France, Germany, Italy, Spain, and the United Kingdom evaluated a total of 1,091 patient scenarios. For each scenario, the endocrinologists were asked whether the patient (an adult patient with a confirmed diagnosis of acromegaly) described by the hypothetical profile was:
Stable (the patient is adequately controlled);
Had mild disease activity (the patient shows mild disease activity, further evaluation of the patient’s condition is needed;
Had significant disease activity (the patient shows significant disease activity requiring clinical action).
For algorithm development to predict disease activity categorisation based on values of the five health status parameters, both Classification And Regression Tree (CART) methods and multivariable logistic regression methods were implemented.

PP-GIP-GBR-2692 Date of preparation: October 2017 3
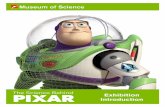
A summary of the development path for ACRODAT® is shown in Figure 1: Figure 1: ACRODAT® development path The validation study outcome was a confirmation of the current status of acromegaly management which demonstrated a main focus on tumour status and IGF-I value. In the CART decision tree model, only IGF-I and tumour status had any influence in the ultimate disease activity rating. Results from the CART and multivariable logistic regression models were combined to compute an overall ACRODAT® score, which ranged from 0 to 1 (0 indicating a purely “stable” rating, and 1 indicating a purely “significant disease activity” rating). Ultimately, IGF-I and tumour status taken together exhibited non-compensatory decision-making properties: if either was indicated as level 3, the patient scenario would be classified as “significant disease activity” regardless of the level of the other three clinical parameters. However, if neither of these two health status parameters were indicated as level 3, then the other three health status parameters (comorbidities, symptoms and quality of life) along with the remaining levels of IGF-I and tumour status appeared to operate in a compensatory manner. The results have been used to build ACRODAT®, a tool supporting objective measures as well as patient-reported indicators of health status. The value of ACRODAT® is in its potential ability to provide a holistic view of disease activity at any stage of the disease, independent of the therapeutic interventions received. In addition to supporting clinical decision making, this tool may enable the treating endocrinologists to further optimise a patient-centred approach to acromegaly disease management. A more detailed description of the methodology used to develop ACRODAT® is available on demand (please contact Roy Gomez at [email protected])
3. Indicators of disease activity IGF-I Considering both GH and IGF-I, elevated IGF-I levels were considered by the expert panel to be the single best currently available predictor for biochemical disease activity in acromegaly. IGF-I levels are less fluctuating than GH levels and reflect actual GH action in the body. Recently, more reliable age-related normative data is also available for IGF-I assays.8 For patients on pegvisomant treatment, normalization of IGF-I is the only reliable marker of disease control, as pegvisomant interferes with most commercially available GH assays.9 Over the years, consensus statements have recommended varying levels of GH to represent control whereas IGF-I guidance has remained the same, stating that the age-adjusted levels should be in the normalised range.5 ACRODAT® uses the cut-off range of 1.2x the upper limit of normal in order to differentiate between mild and significant disease activity. This value of 1.2 is in line with research in the field where this cut-off value has been used to signify uncontrolled and active disease in various cohorts and studies.10,11
Tumour status Pituitary MRI is recommended to ascertain tumour size, location and invasiveness.5 A patient is considered stable when the pituitary tumour mass effect is clinically insignificant and the lesion is

PP-GIP-GBR-2692 Date of preparation: October 2017 4
considered to be stable, i.e. has not changed in size or invasiveness over time. ACRODAT® uses a 20% increase in tumour volume to show a change in patient status – this value has been previously utilised in clinical trials to note a significant change in tumour volume and is widely accepted by the community.12,13
Co-morbidities A wealth of co-morbidities exist in patients with acromegaly, including skin, joint and cardiovascular complications, as well as sleep apnoea.14 ACRODAT® uses three co-morbidities known to be directly related to acromegaly that can also be modified AND managed by appropriate modification of available treatment options – sleep apnoea, diabetes and cardiac disease (including hypertension, hyperlipidaemia or other cardiac abnormalities) – as part of the assessment. Cardiovascular disease is considered a key factor because of the heightened risk for cardiovascular complications and consequent need for early identification and treatment. Having diabetes, even if it was adequately controlled with anti-diabetic medication, was considered by the expert panel as an independent risk factor requiring further evaluation. Sleep apnoea is a comorbidity that occurs in 60–80% of patients, and may contribute to hypertension and cardiovascular disease.14 Sleep indexes may improve during effective treatment of acromegaly.15,16 Biochemical control through surgical or pharmacological means has been demonstrated to provide improvements in clinical parameters for sleep apnoea, diabetes and cardiovascular events.17 It has been surmised that the use of more stringent criteria to define cure, together with aggressive treatment of co-morbidities, has and will continue to significantly improve the prognosis for patients with acromegaly.14 It is to this end that ACRODAT® includes these three key co-morbidities alongside the more clinical metrics of tumour size and IGF-I. In the study by Gurel et al. both patients and physicians shared the dealing of co-morbidities as their key goals for the treatment of acromegaly.18
Symptoms Acromegaly can cause a variety of symptoms, such as headache, sweating (especially at night), carpal tunnel syndrome, joint pain; a gradual deepening of the voice is also observed.19 The Patient-assessed Acromegaly Symptom Questionnaire (PASQ) score has been developed in order to assess the symptoms of acromegaly and the patient’s perceived health on a 0–8-point scale, ranging from “Absent” (0) to “Severe, incapacitating”(8).20 In a 1-year study assessing the IGF-I status of the patient and their PASQ score, it was found that patients’ symptoms and perceived health do not merely reflect IGF-I status or biochemical control.20 An abbreviated version of the PASQ score (Signs and Symptoms Score) is used in ACRODAT®. In a recent patient study, participants wished to feel as free from the disease as they could and for many, this meant feeling less symptomatic with no headaches, joint pain, less fatigue and a reduction in the swelling of soft tissue.18 This underlines the need for careful evaluation of signs and symptoms when the patient is presenting at the clinic.
Health-related quality of life Acromegaly has been associated with substantial impairment in quality of life, which has been attributed to the symptoms of the disease, co-morbidities and to the burden of treatment.18 Assessment of the quality of life that the patient with acromegaly is experiencing is an important outcome to be measured in clinical practice.21 Not only does this information provide the treating physician with the patient’s perspective regarding issues often not addressed by healthcare professionals, but also their expectations of treatment goals and the impact the disease has on their daily life.21 Generic QoL questionnaires that can be utilised across many disease areas exist, but the ACROQoL, which is used in ACRODAT®, is specific to patients with acromegaly and is more likely to identify the impairments due to the underlying disease, as well as the benefits of treatment.21

PP-GIP-GBR-2692 Date of preparation: October 2017 5
The ACROQoL questionnaire was originally published in 2002 and contains 22 statements for which patients have to rate their level of agreement, or provide the treating physician with an overarching view of the frequency of these events.22 The statements assess the overall mental and physical well-being of the patient. In a study in Korean patients receiving treatment for acromegaly utilising the ACROQoL questionnaire, the psychological appearance subdomain showed a significant increase during the entire 24-week study and demonstrated a weak negative correlation with change in IGF-I levels.23
Sub-group analyses of controlled versus uncontrolled patients were carried out with no difference in ACROQoL scores, thus demonstrating that biochemical control may not reflect the quality of life.23 Since the health-related quality of life reflects patient‐related parameters, it is a complementary technique in monitoring the patient alongside the biochemical, radiological and other usual objective parameters used in every day clinical practice.21
4. Future management of patients with acromegaly According to a recent survey, patient perceptions regarding the healthcare community appear to be strongly influenced by their experiences during the diagnostic process, which in acromegaly can be a contracted process.18 These perceptions may influence attitudes toward subsequent treatment, including the extent to which patients discuss lifestyle issues with their physicians.18 It is important that patients are asked more about how acromegaly impacts them in terms of their day-to-day activities. The survey found that patients with a good partnership with their physicians were more willing to discuss the disease’s impact on their lives.18 Regular monitoring of a patient with acromegaly is important in maintaining follow-up of care and continued assessment of their disease.24,25 While the recommendations highlight assessment of biochemical measures and tumour size5 with ‘cure’ or ‘control’ defined by GH and IGF-I control, the optimal management of acromegaly goes beyond this to include the comprehensive management of the symptoms and co-morbidities typically associated with the disease.17,24 Taking the patient as a whole into consideration may help define management pathways that better reflect the personalised and predictive approach that patients expect as standard of care.26 It is hoped that with its carefully chosen balance of clinical and patient-focussed parameters (IGF-I, tumour size, co-morbidities, symptoms and quality of life), ACRODAT® can support a more holistic approach to acromegaly disease management, encouraging both physicians and patients in monitoring acromegaly more closely and facilitating the important discussions with the ultimate aim of improved patient outcomes.

PP-GIP-GBR-2692 Date of preparation: October 2017 6
References 1. Schöfl C, et al. Failure to achieve disease control in acromegaly: cause analysis by a registry-based survey. Eur J Endocrinol 2015;172:351–356. 2. Lansang C, et al. Serum IGF-I in treated acromegaly – how normal is “normal”? Pituitary. 2005;8:135-138. 3. Neggers SJCMM, et al. Quality of life in acromegalic patients during long-term somatostatin analog treatment with and without pegvisomant. J Clin Endocrinol Metab. 2008;93:3853-3859. 4. Rubeck KZ, et al. Conventional and novel biomarkers of treatment outcome in patients with acromegaly: discordant results after somatostatin analog treatment compared with surgery. Eur J Endocrinol. 2010;163:717-726. 5. Katznelson L, et al. Acromegaly: an endocrine society clinical practice guideline. J Clin Endocrinol Metab 2014;99:3933–3951. 6. Giustina A, et al. Expert consensus document. A consensus on the medical treatment of acromegaly. Nat Rev Endocrinol 2014;10:243–248. 7. Giustina A, et al. A consensus on criteria for cure of acromegaly. J Clin Endocrinol Metab 2010;95:3141-3148. 8. Bidlingmaier M, et al. Reference intervals for Insulin-like Growth Factor-1 (IGF-1) from birth to senescence: results from a multicentre study using a new automated chemiluminescence IGF-1 immunoassay conforming to recent international recommendations. J Clin Endocrinol Metab 2014;99:1712-1721. 9. Trainer PJ, et al. Treatment of acromegaly with the growth hormone-receptor antagonist pegvisomant. N Engl J Med 2000;342:1171–1177. 10. Freda PU, et al. Long-term treatment with pegvisomant as monotherapy in patients with acromegaly: experience from ACROSTUDY. Endocr Pract 2015;21:264–274. 11. Ramirez C, et al. Discontinuation of octreotide LAR after long term, successful treatment of patients with acromegaly: is it worth trying? Eur J Endocrinol 2012;166:21–26. 12. Petersenn S, et al. Pasireotide (SOM230) demonstrates efficacy and safety in patients with acromegaly: a randomized, multicenter, Phase II Trial. J Clin Endocrinol Metab 2010;95:2781–2789. 13. Lundin P, Pedersen F. Volume of pituitary macroadenomas: assessment by MRI. J Comput Assist Tomogr 1992:16;519-528. 14. Chanson P, Salenave S. Acromegaly. Orphanet J Rare Dis 2008;3:17. 15. Herrmann BL, et al. Effects of octreotide on sleep apnoea and tongue volume (magnetic resonance imaging) in patients with acromegaly. Eur J Endocrinol. 2004;151:309-315. 16. Berg C, et al. Influence of disease control with pegvisomant on sleep apnoea and tongue volume in patients with active acromegaly. Eur J Endocrinol. 2009; 161: 829–835. 17. Vilar L, et al. Multiple facets in the control of acromegaly. Pituitary 2014;17(Suppl 1):S11–S17. 18. Gurel MH, et al. Patient perspectives on the impact of acromegaly: results from individual and group interviews. Patient Prefer Adherence 2014;8:53–62. 19. Chanson P, et al. Acromegaly. Handb Clin Neurol 2014;124:197–219. 20. Sievers C, et al. Change of symptoms and perceived health in acromegalic patients on pegvisomant therapy: a retrospective cohort study within the German Pegvisomant Observational Study (GPOS). Clin Endocrinol (Oxf) 2010;73:89–94. 21. Webb SM, Badia X. Quality of life in acromegaly. Neuroendocrinology 2016;103:106–111. 22. Webb SM, et al. Acromegaly Quality of Life Questionnaire (ACROQOL) a new health-related quality of life questionnaire for patients with acromegaly: development and psychometric properties. Clin Endocrinol (Oxf) 2002;57:251–258. 23. Chin SO, et al. Change in quality of life in patients with acromegaly after treatment with octreotide LAR: first application of AcroQoL in Korea. BMJ Open 2015;5:e006898. 24. Silverstein JM. Need for improved monitoring in patients with acromegaly. Endocr Connect 2015;4:R59–R67.

PP-GIP-GBR-2692 Date of preparation: October 2017 7
25. Delemer B, et al. Patients lost to follow-up in acromegaly: results of the ACROSPECT study. Eur J Endocrinol 2014;170:791–797. 26. Puig Domingo M. Treatment of acromegaly in the era of personalized and predictive medicine. Clin Endocrinol (Oxf) 2015;83:3–14.

Non-Promotional Certificate UK
Pfizer Sponsor Eloise Musgrove
Name UK-PIH-ENDOCRINE ACRODAT Science Behind
Document Number PP-GIP-GBR-2692
NON-PROMOTIONAL ITEM CERTIFIED FOR USEThe below signatories have examined the electronic final form of this material and in their belief it complieswith the Code.
Other Final Country SignatoryName: STEVEN YULESignature Date: 15-Nov-2017 08:51:31 GMT+0000Reason: Non-Promotional item certified for use