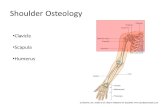
The Scapula Counts Too!

of 12
description
Shoulder
Transcript of The Scapula Counts Too!
-
1The Scapula Counts Too! Incorporating Scapular Exercises
into Shoulder Rehabilitation
Brady L. Tripp PhD, ATCFlorida International University
Mini-course Goals
We willz Review the role of scapula in shoulder function and dysfunctionz Demonstrate and practice clinical assessment techniques and special
tests to evaluate scapular functionz Identify and discuss components of scapular rehabilitationz Demonstrate and practice methods to integrate scapular stability
exercises into shoulder rehabilitation
This course is designed for clinicians who wish to enhance theirability to assess and rehabilitate shoulder dysfunction. We willdiscuss and practice advanced clinical techniques to assess scapular function and integrate scapula control exercises into shoulder rehabilitation. We will review material using brief PowerPoint presentations followed by demonstrations and hands-on experience applying the assessment and rehabilitation techniques.
Agenda1. Clinical Exam2. Shoulder Foundation Understanding Function of the ScapulaComponents of Scapular Control3. Posture / Postural Awareness 4. Flexibility, Neuromuscular Control, Strength and EnduranceDeveloping Stability5. Continuum of Stability6. Engraining Functional StabilityIntegrating Scapular Control into Rehabilitation7. Progressive VariationTake Home PointsQuestions
Dr. Tripps Tips for Shoulder Rehabilitation
1. Clinical exam is VITAL! 2. Proximal stability is the foundation for distal stability, mobility
and function3. Poor posture / postural awareness and pain inhibit progress4. Stability requires flexibility, neuromuscular control, strength
and endurance5. Stability is a continuum, develop it as a continuum
static dynamic functional 1-joint multi-joint functional
6. Engrain motor patterns that begin with scapular setting7. Use progressive variation to increase demands of exercises;
follow established progression sequence
-
2Primary Functions of the Scapula
The Scapula a Mobile and Stable Base
Scapula must move consistently with humerus
Clinical Exam and Scapular FunctionGoal: Identify issues, eliminate concerns and develop goals Adequate visualization of landmarks Multiple repetitions of flexion and scaption Adding 1-5 lb weights may help identify deficits Classify scapular motion as NORMALNORMAL
or
ABNORMALABNORMAL
Clinical Exam is VITAL! How would you describe what is going on here?
Scapular Motion
Goal = Identify issuesNORMAL and ABNORMAL Scapular Motion Rotations about 3 axes, in 3 planes
Upward / Downward Rotation Internal / External Rotation Anterior / Posterior Tilt
Superior / Inferior Translation (shrug)
Scapular Upward Rotation
50 5Normal Range
2 5Resting Position
FrontalPlane of Motion
SagittalAxis of Rotation
Scapular Upward Rotation
50 5Normal Range2 5Resting Position
Scapular Upward Rotation
50 5Normal Range2 5Resting Position
-
3Scapular External Rotation
25 10Normal Range
-30 15Resting Position
TransversePlane of Motion
VerticalAxis of Rotation25 10Normal Range
-30 15Resting Position
Scapular External Rotation
Scapular External Rotation
25 10Normal Range
-30 15Resting Position
Scapular Posterior Tilt
30 15Normal Range
-8 5Resting Position
SagittalPlane of Motion
HorizontalAxis of Rotation
Scapular Posterior Tilt
30 15Normal Range-8 5Resting Position
Scapular Posterior Tilt
30 15Normal Range-8 5Resting Position
-
4Clinical Exam Classify scapular motion as normal or abnormal
Abnormal compared to what?Different compared to: 1) ideal = abnormal
2) the other side = asymmetric3) other reps = inconsistent
Ideal scapular motion as the arm elevates :smooth increases in UR, ER and PT
as the arm is loweredsmooth decreases in UR, ER and PT
The humerus is elevating smoothly, the scapula should follow The scapula must maintain a stable alignment with the humerus,
if not we lose dynamic stability
Clinical ExamNormal or Abnormal Scapular Motion?
How do we quantify abnormal?
Clinical Exam
EXAMPLES
Abnormal Upward Rotation
Abnormal Upward Rotation Abnormal Upward Rotation
Lack of adequate UR or poor NMC-inconsistency Shrug initiates movement = superior translation during
elevation
Result: less subacromial space, greater tuberosity closer to coracoacromial arch
-
5Abnormal Upward Rotation Abnormal Scapular External Rotation
Abnormal Scapular External Rotation
Lack of ER or poor NMC-inconsistency Medial border becomes prominent, lifting off the
thoracic wallResult:
Increased scapulo-humeral angle (transverse plane)
Decreases space between supraspinatus and posterior superior glenoid (i.e. posterior impingement)
Lack of Scapular External Rotation
Abnormal Scapular External Rotation Abnormal Scapular External Rotation
-
6Abnormal Posterior Tilt Abnormal Posterior Tilt
Lack of adequate PT or poor NMC-inconsistency Inferior angle becomes prominent, lifting off the
thoracic wall posteriorly
Result: Decreases subacromial space, bring greater tuberosity closer to coracoacromial arch (i.e. subacromial impingement)
Abnormal Posterior Tilt Abnormal Posterior Tilt
Abnormal Scapular Motion :Research Findings
Three characteristics were quantified in patients classified as having abnormal kinematics andin pathologic subjects
1. less total IR/ER 2. less consistent IR/ER3. less consistent UR
Impingement Patients( Warner 1992, Lukasiewicz 1999, Ludwig 2000, Hebert 2002 ) Less UR, delayed UR or a more superior
position on thorax (2cm) Less ER Less PT (~9)
May anteriorly tilt as the arm elevates
Abnormal Scapular Motion :Research Findings
-
7Clinical Exam
PRACTICAL EXAMPLESGoal = Identify1. Normal Scapular Motion2. Abnormal Scapular Motion
Asymmetric? Inconsistent? Lack of: Upward Rotation (shrug)?
External Rot. (medial border prominent)Posterior Tilt (inferior angle prominent)
Dr. Tripps Tips for Shoulder Rehabilitation
1. Clinical exam is VITAL! Goal: Identify issues, eliminate concerns and develop goals
2. Proximal stability is the foundation for distal stability, mobility and functionGoal: Build the foundation early (scapular control) before progressing distally
Agenda1. Clinical Exam2. Shoulder Foundation Understanding Function of the ScapulaComponents of Scapular Control3. Posture / Postural Awareness 4. Flexibility, Neuromuscular Control, Strength and EnduranceDeveloping Stability5. Continuum of Stability6. Engraining Functional StabilityIntegrating Scapular Control into Rehabilitation7. Progressive VariationTake Home PointsQuestions
Result:Scapula: less PT (~4 less)
less UR (~5 less)a more superior position
on thoraxGH Joint: less shoulder abduction
(~24less)
Components of Scapular Control
Posture: Forward Head / Kyphosis / Slouching ( Ludwig 1996, Kebaetse 1998 )
Dr. Tripps Tips for Shoulder Rehabilitation
1. Clinical exam is VITAL! Goal: Identify issues, eliminate concerns and develop goals
2. Proximal stability is the foundation for distal stability, mobility and functionGoal: Build the foundation early (scapular control) before progressing distally
3. Poor posture / postural awareness and pain inhibit progressGoal: Address posture and pain first
Muscular Inflexibility
Pectoralis Minor or Biceps (short head)Pulls coracoid anterior/inferiorly Result: Decreased ER and PT,
fwd rounded shoulders
Rehab GoalsAddress Posture!
&Postural Awareness!
What does that mean for this guy?
-
8Components of Scapular Control
Fatigue Tsai, McClure 2003
PT,ER, UR McQuade, 1998
loss of scapular control McQuade, 1995
PT, UR
What does that mean for these guys?
Rehab GoalsBuild Endurance! Maintain Form!
Serratus Anterior Result: During arm elevation: less UR, less PT,
poor NMC of UR,PT,ERPlus Sign positive= medial border is
not held on thoracic wallScapular Flip Sign positive= medial
border is not held on thoracic wall Pathologic shoulders display decreased Serratus
Anterior activity during arm elevation (Ludwig, 2000)
Muscular Weakness / Neurological
Muscular Weakness / Neurological
Lower and Middle Trapezius Result: During arm elevation: less UR,
lack of PT (tilts anteriorly), lack of ER (internally rotates), poor NMC of UR,PT,ER
Plus Sign positive= medial border is not held on thoracic wall
Scapular Flip Sign positive= medial border is not held on thoracic wall
Overhead athletes with impingement display delayed activation of Lower and Middle Trap during arm elevation (Cools, 2003)
Muscular Dominance / Inflexibility
Upper TrapeziusShrug initiates movement =
superior translation during elevation
Result: During arm elevation: lack of adequate UR, poor NMC of UR
Pathologic shoulders displayed increased EMG during arm elevation with a load (Ludwig, 2000)
Effecting Scapular PositionTo increase upward rotation, external rotation,
posterior tilt:Strengthen:
Serratus AnteriorLower and Middle Traps
Increase Flexibility, Limit Dominance: Upper Trap and LevatorPec Minor
Who will rehab help?
Scapular Retraction TestDuring Active Flexion:Examiner: one hand supporting the
elbow/forearm, the other hand retracting and posteriorly tilting the scapula.
Positive Finding:Improved strengthReduction or elimination of symptoms
-
9Scapular Assistance TestDuring Active Flexion:Examiner: one hand stabilizing root of
scapular spine, assisting upward rotation; the other assisting posterior tilt at the inferior angle
Positive Finding:Improved strengthReduction or elimination of symptoms
Dr. Tripps Tips for Shoulder Rehabilitation
1. Clinical exam is VITAL! Goal: Identify issues, eliminate concerns and develop goals
2. Proximal stability is the foundation for distal stability, mobility and functionGoal: Build the foundation early (scapular control) before progressing distally
3. Poor posture / postural awareness and pain inhibit progressGoal: Address posture and pain first
4. Stability requires flexibility, neuromuscular control, strength and endurance
Goal: Develop each component of stability
Agenda1. Clinical Exam2. Shoulder Foundation Understanding Function of the ScapulaComponents of Scapular Control3. Posture / Postural Awareness 4. Flexibility, Neuromuscular Control, Strength and EnduranceDeveloping Stability5. Continuum of Stability6. Engraining Functional StabilityIntegrating Scapular Control into Rehabilitation7. Progressive VariationTake Home PointsQuestions
Developing StabilityStability is a continuum, develop it as a continuum
single multi-joint functionalstatic dynamic functional Examples?
Rhythmic Stabilization Scapular Clock
Create a StableStable Base! Create a MobileMobile Base!
Developing StabilityEngrain motor patterns that begin with scapular setting
Create a Stable Base!
Dr. Tripps Tips for Shoulder Rehabilitation
1. Clinical exam is VITAL! Goal: Identify issues, eliminate concerns and develop goals
2. Proximal stability is the foundation for distal stability, mobility and functionGoal: Build the foundation early (scapular control) before progressing distally
3. Poor posture / postural awareness and pain inhibit progressGoal: Address posture and pain first
4. Stability requires flexibility, neuromuscular control, strength and endurance
Goal: Develop each component of stability5. Stability is a continuum, develop it as a continuum
static dynamic functional; single multi-joint functionalGoal: Develop stability as a continuum progressing to functional
6. Engrain motor patterns that begin with scapular settingGoal: Emphasize beginning movement with a stable base
-
10
Agenda1. Clinical Exam2. Shoulder Foundation Understanding Function of the ScapulaComponents of Scapular Control3. Posture / Postural Awareness 4. Flexibility, Neuromuscular Control, Strength and EnduranceDeveloping Stability5. Continuum of Stability6. Engraining Functional StabilityIntegrating Scapular Control into Rehabilitation7. Progressive VariationTake Home PointsQuestions
Integrating Scapular Control into Rehabilitation
Use Progressive VariationProgressive Variation to modify exercises to achieve Goals
Clinical Exam Identifies Goals Build the foundation early (scapular control) before
progressing distally Address posture and pain first Develop each component of stability Develop stability as a continuum progressing to functional Emphasize beginning movement with a stable base
Progressive VariationExercise Variables Clinicians Can Manipulate to AdvanceDemands and Address Goals of Rehabilitation
Integrating Scapular Control into Rehabilitation
EXAMPLES
Examples
Progressive Variation
Examples
Progressive Variation
-
11
Examples
Progressive Variation
Video
ExercisesInferior Glide
Robbery
ExercisesLow Row
Lawnmower
ExercisesScapular Clocks
Rhythmic Stabilization
ExercisesProgression
Downward Rows
ExercisesForward Punch
Push-ups with +
-
12
Examples
Internal Rotation and Posterior Capsule (GIRD)Sleeper Stretch
Address Posture / Increase Flexibility
Anterior Shoulder Flexibility Muscles attaching to the coracoid
Pectoralis minor Short head of the biceps Coracobrachialis
Agenda1. Clinical Exam2. Shoulder Foundation Understanding Function of the ScapulaComponents of Scapular Control3. Posture / Postural Awareness 4. Flexibility, Neuromuscular Control, Strength and EnduranceDeveloping Stability5. Continuum of Stability6. Engraining Functional StabilityIntegrating Scapular Control into Rehabilitation7. Progressive VariationTake Home PointsQuestions
Take Home Points1. Clinical exam is VITAL! 2. Proximal stability is the foundation for distal stability, mobility
and function3. Poor posture / postural awareness and pain inhibit progress4. Stability requires flexibility, neuromuscular control, strength
and endurance5. Stability is a continuum, develop it as a continuum
static dynamic functional; single multi-joint functional6. Engrain motor patterns that begin with scapular setting7. Use progressive variation to increase demands of exercises;
follow established progression sequence
Thank You
Questions?
/ColorImageDict > /JPEG2000ColorACSImageDict > /JPEG2000ColorImageDict > /AntiAliasGrayImages false /DownsampleGrayImages true /GrayImageDownsampleType /Bicubic /GrayImageResolution 300 /GrayImageDepth -1 /GrayImageDownsampleThreshold 1.50000 /EncodeGrayImages true /GrayImageFilter /DCTEncode /AutoFilterGrayImages true /GrayImageAutoFilterStrategy /JPEG /GrayACSImageDict > /GrayImageDict > /JPEG2000GrayACSImageDict > /JPEG2000GrayImageDict > /AntiAliasMonoImages false /DownsampleMonoImages true /MonoImageDownsampleType /Bicubic /MonoImageResolution 1200 /MonoImageDepth -1 /MonoImageDownsampleThreshold 1.50000 /EncodeMonoImages true /MonoImageFilter /CCITTFaxEncode /MonoImageDict > /AllowPSXObjects false /PDFX1aCheck false /PDFX3Check false /PDFXCompliantPDFOnly false /PDFXNoTrimBoxError true /PDFXTrimBoxToMediaBoxOffset [ 0.00000 0.00000 0.00000 0.00000 ] /PDFXSetBleedBoxToMediaBox true /PDFXBleedBoxToTrimBoxOffset [ 0.00000 0.00000 0.00000 0.00000 ] /PDFXOutputIntentProfile () /PDFXOutputCondition () /PDFXRegistryName (http://www.color.org) /PDFXTrapped /Unknown
/Description >>> setdistillerparams> setpagedevice