Safety and Effectiveness of Transarterial Embolization for ...

S L I D E 1
The Role of Transarterial Radioembolization (TARE) in the Management of Hepatocelllar Carcinoma
Raj Ayyagari M.D.Assistant Professor of RadiologySection of Interventional RadiologyYale University School of [email protected]

S L I D E 2
Disclosures
• I do not have any financial interest or other relationship with the manufacturers of any products or providers of services I intend to discuss.

S L I D E 3
Overview
• TARE Treatment Rationale
• Patient selection
• Technique
• Dosimetry
• Side Effects, Complications
• Clinical OutcomesWang EA, Broadwell SR, Bellavia RJ, Stein JP. J Gastrointest Oncol. 2017;8(2):266-278.

S L I D E 4
TARE Treatment Rationale
• Transarterial radioembolization (TARE) is the hepatic intra-arterial injection of the radioisotope Yttrium-90to treat unresectable HCC.
• Yttrium-90 , a β-emitter with a ½-life of 64.2h and tissue penetration of 2.5-11 mm, is incorporated into glass (TheraSphere) or resin (SIR-Spheres) microspheres 20-60µm in diameter.
• By delivering an internal radiation source, TARE is a form of brachytherapy. Allows safe administration of therapeutically high radiation doses (up to 150 Gy) with lower risk of radiation-induced liver damage than external beam radiation (at 35-40 Gy).

S L I D E 5
TARE Treatment Rationale
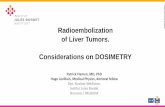
• High tumoricidal doses achieved by preferential deposit of particles in tumor due to differential perfusion.
• Treatments can be…– Whole liver (higher risk)– Lobar– Segmental (“Radiation
Segmentectomy”)– Sequential– Repeated?
SIRTex, Incorporated

S L I D E 6
Patient Selection for TARE• Multifactoral assessment involving disease burden,
biochemical profile, and performance status.
• Unresectable, with large majority of tumor burden (if not all of it) in the liver, with <70% of the liver involved.
• Adequate functional liver reserve needed: total bilirubin <2 mg/dL, albumin >3 g/dL, and a normal INR.
• ECOG performance status score of 0-1, maybe 2.
• Extreme caution when treating patients with ampulla of Vater manipulations due to increased risk of liver abscess.
• Portal vein patency not required, and in fact tumoralportal thrombus cannot be treated any other way.

S L I D E 7
TARE Technique

S L I D E 8
TARE Technique
• Outpatient procedure involving an initial mapping mesenteric angiogram combined with a liver-lung shunt scan, followed by dose planning and a subsequent angiographic treatment procedure.
• If radioactive particles embolize anywhere but the targeted liver (via shunts, collaterals, reflux)…– Lungs: Radiation pneumonitis– Stomach/Bowel: Ulcers,
bleeding, perforation– Can be DEVASTATING.

S L I D E 9
TARE Technique
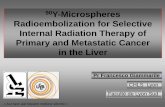
• Mapping mesenteric angiogram goals:
– embolize collaterals (GDA, right gastric artery)…hepatic arterial variants are common!
– evaluate arterial anatomy to plan catheter placement
– obtain liver lobar/segmental/tumoral volumes…needed for dosimetry.
– inject ~4 mCi technetium-99m MAA test dose…arteriovenous shunting can be extensive!

S L I D E 10
TARE Technique

S L I D E 11
TARE Technique

S L I D E 12
TARE Dosimetry
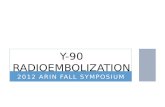
• Lobar or segmental liver volumes are calculated using diagnostic MRI/CT, axial SPECT-CT, or even better, cone-beam CTA images.
• Liver tumor volumes are calculated using a diagnostic MRI/CT.
• BSA is calculated using patient height and weight.• Lung shunt fraction is calculated by a nuclear medicine
scan that measures the amount of 99mTc-MAA that gets to the lungs.
• Treatment Dose calculation method differs based on whether glass TheraSpheres (2500 Bq/sphere) or resin SIR-Spheres (50 Bq/sphere) are being used.

S L I D E 13
TARE Dosimetry
• TheraSpheres:
Activity = Absorbed Dose (Gy) x Mass of Liver50 x (1-%LSF/100) x (1-%R/100)
Target delivered activity is typically 80-150 Gy
• SIR-Spheres:
Activity = BSA – 0.2 + %Tumor Involvement100
LSF <10% = no dose reduction; LSF 10-15% = 20% reduction; LSF 15-20% = 40% reduction

S L I D E 14
TARE Side Effects, Complications
SIDE EFFECTS:• Fatigue – 50-60% patients in first 1-2 weeks after.• Low grade abdominal pain, nausea/vomiting – 20%.
COMPLICATIONS:• Radiation-induced GI ulcers often refractory to
conservative management.• Biliary complications (10%): dyskinesia, cholecystitis
(2.7%), stricture (2.4%), necrosis (3.9%), biloma (1%).• Radiation-induced liver disease – sinusoidal congestion,
venous occlusion, hepatic fibrosis; 4-8 weeks after; 4-7%, but in a series including liver metastatic lesions previously treated with chemotherapy; no predictive model for RILD.

S L I D E 15
TARE Clinical Outcomes
• 1-year survival rates of untreated HCC patients are ~50% among intermediate stage (BCLC-B) patients and ~25% among advanced stage (BCLC-C) patients.
• Salem et al reported TARE results in 291 intermediate and advanced stage patients. Response rates were 42% (WHO) and 57% (EASL). TTP was 7.9 mo. CP-A patients had median survival of 17.2 mo, CP-B 7.7 mo, and CP-B with PVT 5.6 mo.
• Hilgard et al validated these results in 108 patients, and showed outcomes equivalent to cTACE and DEB-TACE.
• A 325 patient study by Sangro et al showed TARE patients to have median survival of 24.4 mo (BCLC-A), 16.9 mo (BCLC-B), and 10.0 mo (BCLC-C).

S L I D E 16
TARE Clinical Outcomes
• As yet, no RCT comparing TARE and TACE in HCC.
• Salem et al’s “comparative effectiveness report” of a 245 patient cohort (123 TARE, 122 cTACE) described adverse events, toxicities, repsonse rates, and TTP to be improved in TARE, with no difference in overall survival.
• TARE has also been shown to superior favorable rate of down-staging HCC patients to transplantation.
• TARE also seems to cause less hepatotoxicity than TACE in patients with a TIPS in place, likely due to the minimal embolic effect of TARE.

S L I D E 17
REFERENCES• Matalon TS, Athanasoulis CA. Margolies MN. et al. Hemorrhage with pelvic fractures: efficacy of transcatheter embolization. AJR Am J
Roentgenol 1979; 133:859-864.• Hen-Menachem Y, Coldwell DM, Young JWR, Burgess AR. Hemorrhage associated with pelvic fractures: causes, diagnosis, and emergent
management. AJR Am J Roentgenol 1991; 157:1005-1014.• Panetta T, Sclafani SJA. Goldstein AS, et al. Percutaneous transcatheter embolization for massive bleeding from pelvic fractures. J Trauma
1985; 25:1021-1029.• Agolini SP, Shah K. Jaffe J, et al. Arterial embolization is a rapid and effective technique for controlling pelvic fracture hemorrhage.• J Trauma 1997; 43:395-399. DiGiacomo JC. Bonadies JA, Cole FJ, et al. Practice management guidelines for hemorrhage in pelvic fracture.
In Practice Management Guidelines for Trauma. The EAST Practice Management Guidelines Work Group: Eastern Association For theSurgery of Trauma, 2001. Available from http://www.east.org/tpg/pelvis.pdf.
• Aspelin P, Aubry P, Fransson SG, et al. for the NEPHRIC Study Investigators. Nephrotoxic effects in high-risk patients undergoing angiography. N Engl J Med 2003; 348:491-499.
• Obaro RO, Sniderman KW. Case report: avascular necrosis of the femoral head as a complication of complex embolization for severe pelvic haemorrhage. Br J Radiol 1995; 68:920-922.
• Takahira N, Shindo M, Tanaka K, et al. Gluteal muscle necrosis following transcatheter angiographic embolization for retroperitoneal haemorrhage associated with pelvic fracture. Injury2001; 32:27-32.
• Hawkins L, Pomerantz M, Eiseman B. Laparotomy at the time of pelvic fracture. J Trauma 1970; 10:619-623. • Velmahos GC, Chahwan S, Hanks SE, et al. Angiographic embolization of bilateral internal iliac arteries to control life-threatening
hemorrhage after blunt trauma to the pelvis. Am Surg 2000; 66: 858-862.• Velmahos GC, Chahwan S, Falabella A, et al. Angiographic embolization for intraperitoneal and retroperitoneal injuries. World J Surg
24(5):539-545.• Shanmuganathan K, Mirvis SE, Sover ER. Value of contrast-enhanced CT in detecting active hemorrhage in patients with blunt abdominal
or pelvic trauma. AJR Am J Roentgenol 1993; 161:65-69.• Stephen D, Kreder H, Day AC, et al. Early detection of arterial bleeding in acute pelvic trauma. J Trauma 1999; 47:638-642. • Sieber PR. Bladder necrosis secondary to pelvic artery embolization: case report and literature review. J Urol 1994; 151:422.• Hare WS, Holland CJ. Paresis following internal iliac embolization. Radiology 1983; 146:47-51. • Ramirez JI, Velmahos GC, Best CR, et al. Male sexual function after bilateral internal iliac artery embolization for pelvic fracture. J
Trauma 2004; 56:734-741.• Fahmy K. Internal iliac artery ligation and its efficiency in controlling pelvic hemorrhage. Int Surg 1969; 51:244-250.• Tajes RV. Ligation of the hypogastric arteries and its complications in resection of carcinoma of the rectum. Am J Gastroenterol 1956;
26:612-618.