The Role of DHMC as an ST Elevation Myocardial Infarction ...The Role of DHMC as an ST Elevation...
46
The Role of DHMC as an ST The Role of DHMC as an ST Elevation Myocardial Infarction Elevation Myocardial Infarction Receiving Center in a Regional Receiving Center in a Regional STEMI Care Network: STEMI Care Network: Nathaniel Niles, MD Nathaniel Niles, MD CREST Symposium CREST Symposium November 7th, 2008 November 7th, 2008
Transcript of The Role of DHMC as an ST Elevation Myocardial Infarction ...The Role of DHMC as an ST Elevation...
The Role of DHMC as an ST The Role of DHMC as an ST Elevation Myocardial Infarction Elevation Myocardial Infarction Receiving Center in a Regional Receiving Center in a Regional
STEMI Care Network:STEMI Care Network:
Nathaniel Niles, MDNathaniel Niles, MDCREST SymposiumCREST SymposiumNovember 7th, 2008November 7th, 2008
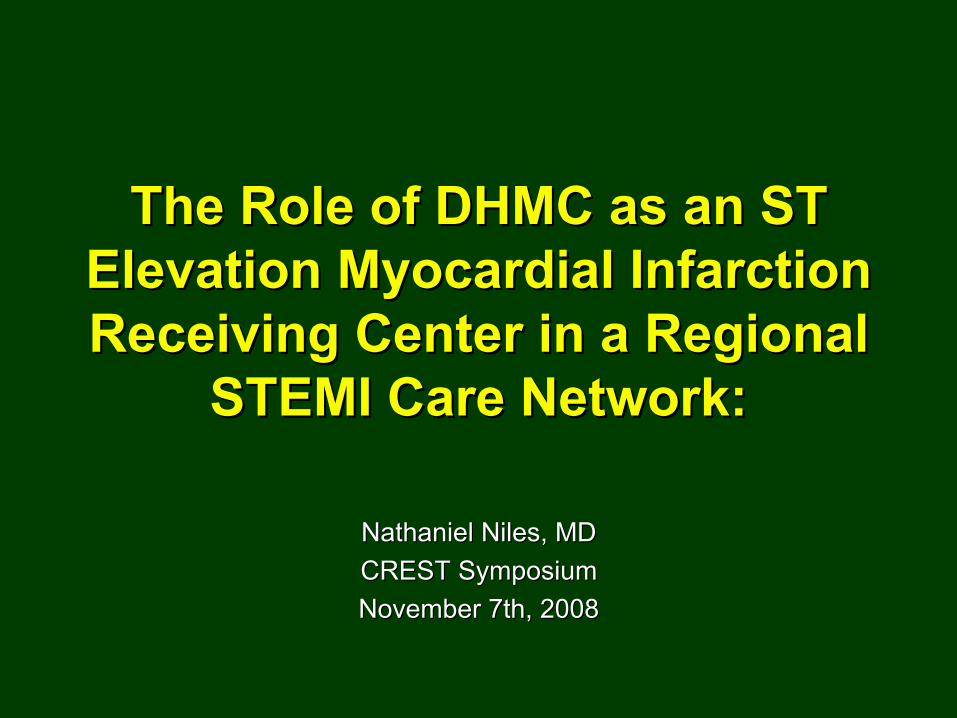
STEMI = Acute Coronary ThrombosisSTEMI = Acute Coronary Thrombosis

STEMI STEMI (ST elevation Myocardial Infarction)(ST elevation Myocardial Infarction)
•• Relatively commonRelatively common•• Multiple treatment Multiple treatment
strategy optionsstrategy options•• Requires coordinationRequires coordination
•• MultidisciplinaryMultidisciplinary•• EMSEMS•• Emergency MedicineEmergency Medicine•• CardiologyCardiology
•• InterhospitalInterhospital•• Must be managed Must be managed
quicklyquicklyTime Time ~ Muscle~ Muscle
Presenter
Presentation Notes
The guidelines discuss in detail the decision to take the time from first medical contact or first door to balloon number to < 90 minutes. For the last decade the importance of time to treatment in PPCI has been debated. The next few studies support the argument “time does matter in PPCI”.

Boersma E. et al. Lancet. 1996:348:771Boersma E. et al. Lancet. 1996:348:771
PrePre--Hospital DelayHospital Delay The Golden early hours:The Golden early hours:
MetaMeta--analysis on 50,246 patients in thrombolytic analysis on 50,246 patients in thrombolytic trialstrials

7
31
68
97
2
21
14
0
10
20
30
Death Non-fatalreinfarction
Total stroke Recurrentischemia
Death,reinfarction,
stroke
Primary PCI
ThrombolyticTherapy
p=0.0002p=0.0002
p=0.0003p=0.0003
p=0.0004p=0.0004
p=0.0001p=0.0001
p=0.0001p=0.0001
Freq
uenc
y (%
)Fr
eque
ncy
(%)
Thrombolytic Therapy is Inferior to PCI for Thrombolytic Therapy is Inferior to PCI for Treating STEMITreating STEMI
23 study systematic review: short23 study systematic review: short--term outcomesterm outcomes
Lancet 2003;361:13Lancet 2003;361:13--2020

7
21.3
0
89
6.9
2.5 2.45
15
0
5
10
15
20
Death Non-fatalreinfarction
Total stroke ICH Death,reinfarction,
stroke
1 PCI (n=1466) TTx (n=1443)
p=0.057p=0.057
p=0.0001p=0.0001
p=0.049p=0.049
p=0.0001p=0.0001
Freq
uenc
y (%
)Fr
eque
ncy
(%)
Transfer for PCI Transfer for PCI vsvs
OnOn--site Thrombolyticsite Thrombolytic5 study systematic review:5 study systematic review:
Lancet 2003;361:13Lancet 2003;361:13--2020
p=0.25p=0.25
Average Transfer Time Average Transfer Time 39 minutes39 minutes
oo
11oo
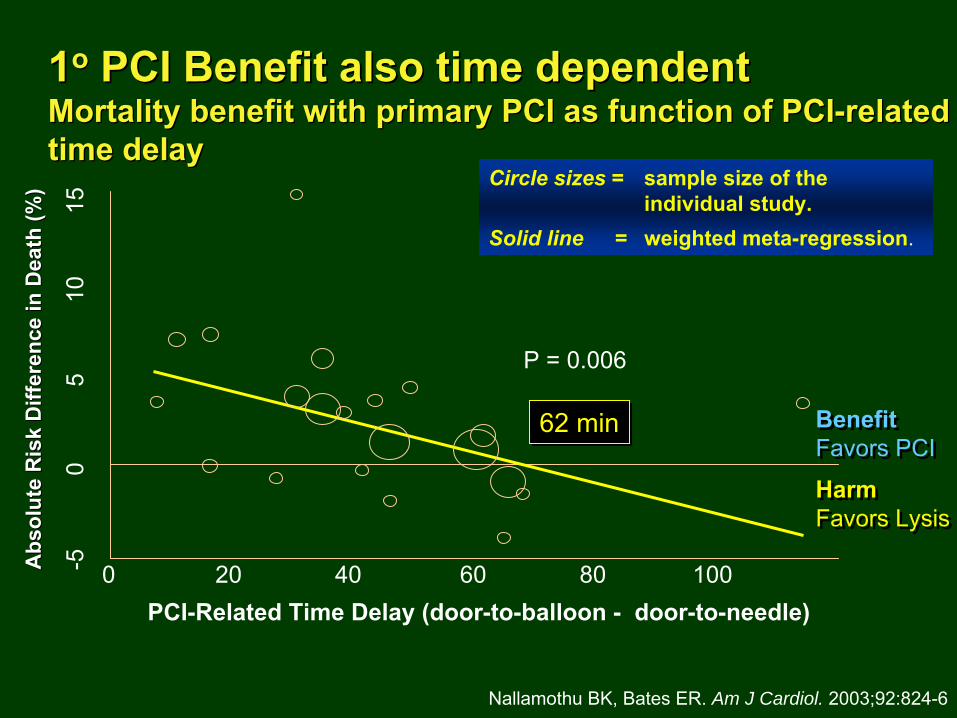
PCI Benefit also time dependentPCI Benefit also time dependent Mortality benefit with primary PCI as function of PCIMortality benefit with primary PCI as function of PCI--relatedrelated
time delaytime delay
P = 0.006
0 20 40 60 80 100PCI-Related Time Delay (door-to-balloon -
door-to-needle)
Abs
olut
e R
isk
Diff
eren
ce in
Dea
th (%
)A
bsol
ute
Ris
k D
iffer
ence
in D
eath
(%)
-50
510
15
Circle
sizes
=
sample size of the individual study.
Solid line
=
weighted meta-regression.
Nallamothu BK, Bates ER.
Am J Cardiol. 2003;92:824-6
62 min62 min Benefit
Favors PCI
Benefit
Favors PCI
Harm
Favors Lysis
Harm
Favors Lysis
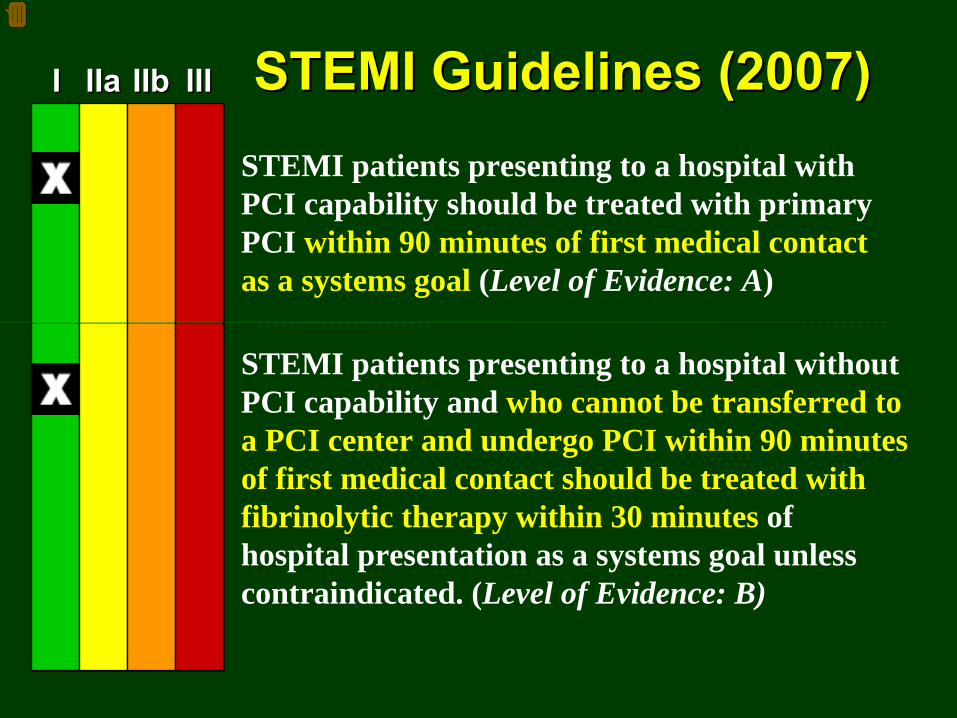
II IIaIIa IIbIIb IIIIII
STEMI patients presenting to a hospital with PCI capability should be treated with primary PCI within 90 minutes of first medical contact as a systems goal (Level of Evidence: A)
STEMI patients presenting to a hospital without PCI capability and who cannot be transferred to a PCI center and undergo PCI within 90 minutes of first medical contact should be treated with fibrinolytic therapy within 30 minutes of hospital presentation as a systems goal unless contraindicated. (Level of Evidence: B)
STEMI Guidelines (2007)STEMI Guidelines (2007)
Presenter
Presentation Notes
The weight of effidence is applied to a particular area and a Class of Recommendations is formulated. The classes range from I – III, and Class II is subdivided into a and b. Class I-the intervention is useful and effective Class IIa-suggests the evidence conflicts or there is a difference of opinions but leans toward efficacy Class IIb-suggests the evidence conflicts or there is a difference of opinions but leans against efficacy Class III-suggests the intervention is not useful/effective and may be harmful Most physicians would suggest that: Class I and IIa should be practiced Class IIb should be given careful consideration for an individual patient. Class III should not be practiced
Regional STEMI Care NetworkRegional STEMI Care Network RationaleRationale
•• PCI is > thrombolytic therapyPCI is > thrombolytic therapy•• Transfer for PCI > onTransfer for PCI > on--site site fibrinolyticfibrinolytic
therapytherapy•• Death during transfer rare Death during transfer rare
•• US Guidelines: D2B US Guidelines: D2B ≤≤90 minutes90 minutes•• Only ~ 25% acute care hospitals in the US are PCI capable and evOnly ~ 25% acute care hospitals in the US are PCI capable and even en
fewer have 24/7 fewer have 24/7 cathcath
labslabs•• Hospital Hospital ““specializationspecialization””
on primary PCI on primary PCI →→
faster treatment and lower faster treatment and lower mortalitymortality
SoSo……What once could be treated locally (What once could be treated locally (TtxTtx
can be given at any hospital) now can be given at any hospital) now requires a regional network around a PCI Center to diagnose STEMrequires a regional network around a PCI Center to diagnose STEMI I get the patient rapidly to PCIget the patient rapidly to PCI
MoreoverMoreover……•• Trauma center systems have been successfulTrauma center systems have been successful•• Formalization of regional networks will better enable payers to Formalization of regional networks will better enable payers to track track
quality (treatment times) and structure incentivesquality (treatment times) and structure incentives
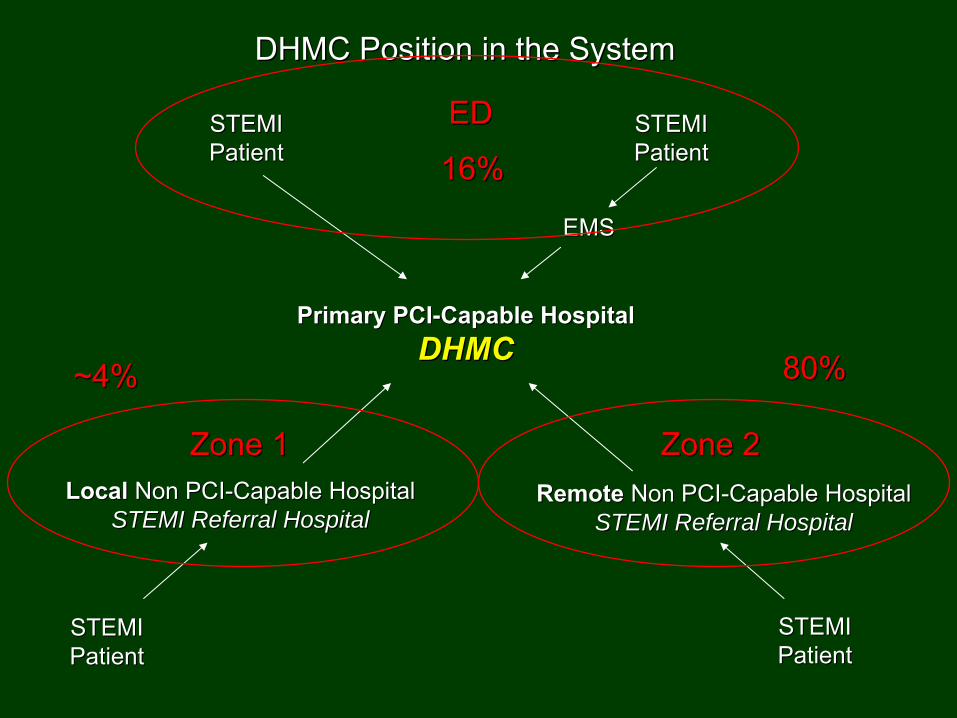
DHMC Position in the SystemDHMC Position in the System
STEMISTEMIPatientPatient
STEMISTEMIPatientPatient
STEMISTEMIPatientPatient
STEMISTEMIPatientPatient
EMSEMS
Primary PCIPrimary PCI--Capable HospitalCapable HospitalDHMCDHMC
LocalLocal
Non PCINon PCI--Capable HospitalCapable HospitalSTEMI Referral HospitalSTEMI Referral Hospital
RemoteRemote
Non PCINon PCI--Capable HospitalCapable HospitalSTEMI Referral HospitalSTEMI Referral Hospital
Zone 1Zone 1 Zone 2Zone 2
EDED
16%16%
~4%~4% 80%80%
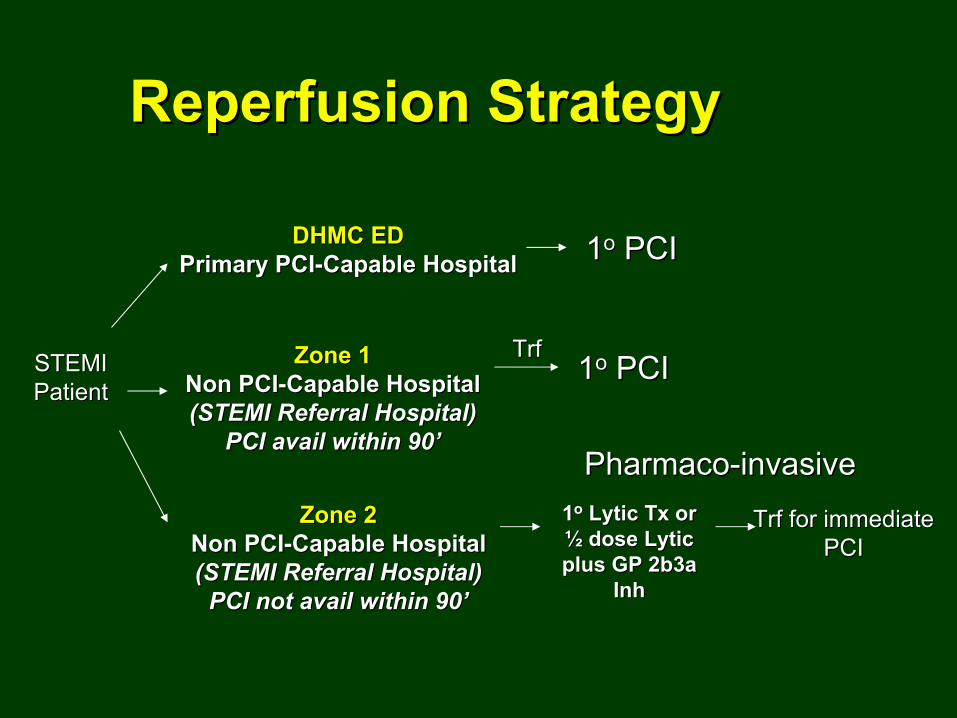
DHMC EDDHMC EDPrimary PCIPrimary PCI--Capable HospitalCapable Hospital
STEMISTEMIPatientPatient
11oo
PCIPCI
Zone 1Zone 1Non PCINon PCI--Capable HospitalCapable Hospital(STEMI Referral Hospital)(STEMI Referral Hospital)
PCI avail within 90PCI avail within 90’’
11oo
PCIPCI
Reperfusion StrategyReperfusion Strategy
Zone 2Zone 2Non PCINon PCI--Capable HospitalCapable Hospital(STEMI Referral Hospital)(STEMI Referral Hospital)
PCI not avail within 90PCI not avail within 90’’
11oo
LyticLytic
TxTx
or or ½½
dose dose LyticLytic
plus GP 2b3a plus GP 2b3a
InhInh
TrfTrf
for immediate for immediate PCIPCI
TrfTrf
PharmacoPharmaco--invasiveinvasive
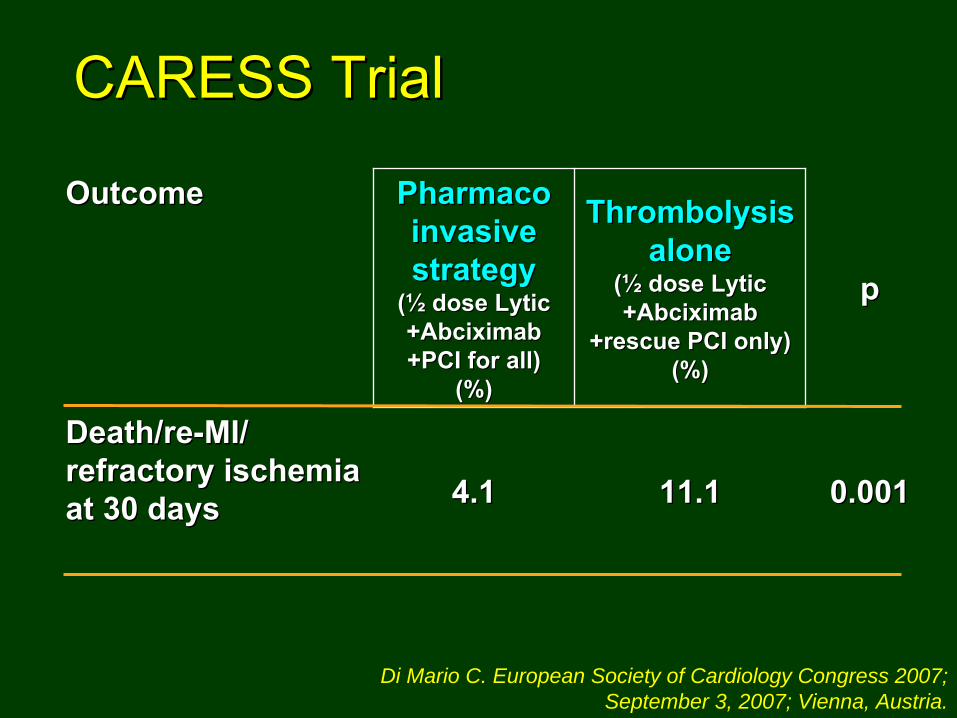
OutcomeOutcome PharmacoPharmaco invasive invasive
strategystrategy((½½
dose dose LyticLytic++AbciximabAbciximab+PCI for all) +PCI for all)
(%)(%)
ThrombolysisThrombolysis alonealone
((½½
dose dose LyticLytic++AbciximabAbciximab
+rescue PCI only) +rescue PCI only) (%)(%)
pp
Death/reDeath/re--MI/ MI/ refractory ischemia refractory ischemia at 30 daysat 30 days 4.14.1 11.111.1 0.0010.001
Di Mario C. European Society of Cardiology Congress 2007; September 3, 2007; Vienna, Austria.
CARESS TrialCARESS Trial

How has DHMC really performed How has DHMC really performed as a STEMI Receiving Center?as a STEMI Receiving Center?

The RegionThe Region•• Upper CT Valley, Upper CT Valley,
~60 m N and 45 m ~60 m N and 45 m S on I91 and 30S on I91 and 30--40 40 m NW or SE on m NW or SE on I89.I89.
•• 20 Referral 20 Referral HospitalsHospitals
•• Zone 1 = the local Zone 1 = the local area, APD and area, APD and VAMCVAMC
•• Zone 2 = Zone 2 = everything elseeverything else
•• ~40 Ambulance ~40 Ambulance servicesservices
•• 2 Helicopters 2 Helicopters based at DHMCbased at DHMC

904 total registry patients from 2001904 total registry patients from 2001→→mid 2007mid 2007
891 STEMI patients891 STEMI patients
13 NSTEMI patients13 NSTEMI patients
742742Presented to regional referral hospitalsPresented to regional referral hospitals
3434Zone 1 Zone 1
(VAMC or APD)(VAMC or APD)11
Admitted to initial Admitted to initial hospital or hospital or
initially initially tfxdtfxd
elsewhereelsewhere
33 33 transferred transferred
emergently to emergently to DHMC with DHMC with
STEMISTEMI
1 1 Managed Managed
conservativelyconservatively
149149Presented Presented to DHMCto DHMC
44DHMC DHMC
inpatientsinpatients145 145 admitted with admitted with STEMI from STEMI from DHMC ERDHMC ER
9 9 Managed Managed
conservativelyconservatively
708708Zone 2Zone 2
(Other referral hospitals)(Other referral hospitals)5353
Admitted to Admitted to initial hospital initial hospital or initially or initially tfxdtfxd
elsewhereelsewhere
655 655 transferred transferred
emergently to emergently to DHMC with DHMC with
STEMISTEMI
12 12 Managed Managed
conservativelyconservatively
136 136 to to cathcath
lab lab emergentlyemergently
5 post 5 post lyticlytic131 no 131 no lyticlytic
0 0 to to cathcath
lab lab latelate
post post lyticlytic
32 32 to to cathcath
lab lab emergentlyemergently
3 post 3 post lyticlytic29 no 29 no lyticlytic
0 0 to to cathcath
lab lab latelate
post post lyticlytic
596 596 to to cathcath
lab lab emergentlyemergently
470 post 470 post lyticlytic124 no 124 no lyticlytic
47 47 to to cathcath
lab lab latelate
post post lyticlytic
DHMC STEMI RegistryDHMC STEMI Registry
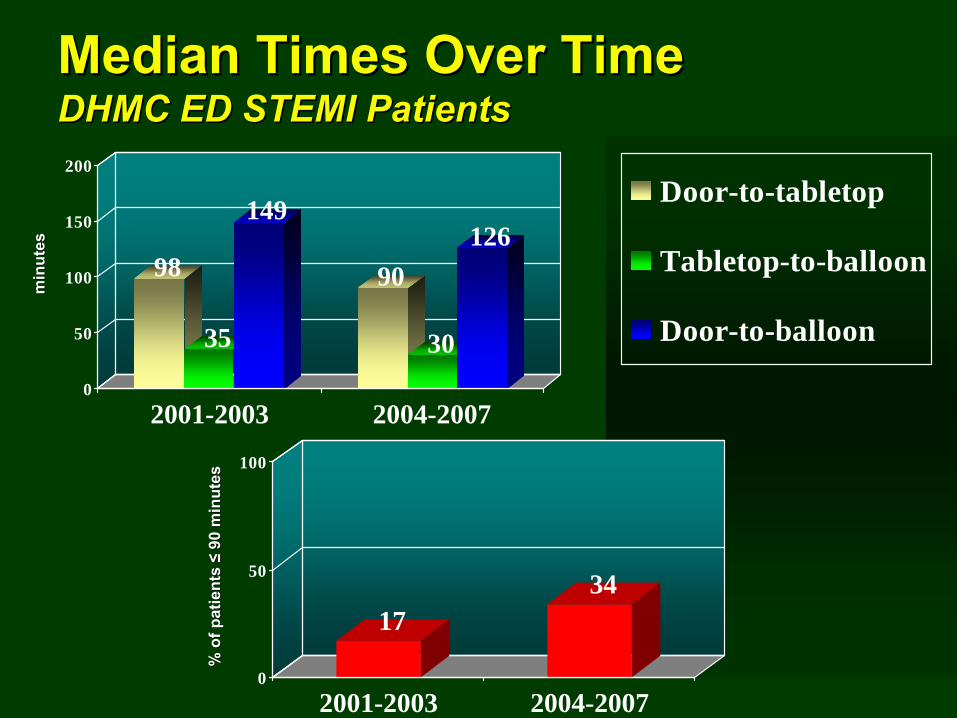
Median Times Over TimeMedian Times Over Time DHMC ED STEMI PatientsDHMC ED STEMI Patients
1734
0
50
100
2001-2003 2004-2007
% o
f pat
ient
s %
of p
atie
nts ≤≤
90 m
inut
es90
min
utes
98
35
149
90
30
126
0
50
100
150
200
2001-2003 2004-2007
Door-to-tabletop
Tabletop-to-balloon
Door-to-balloon
min
utes
min
utes
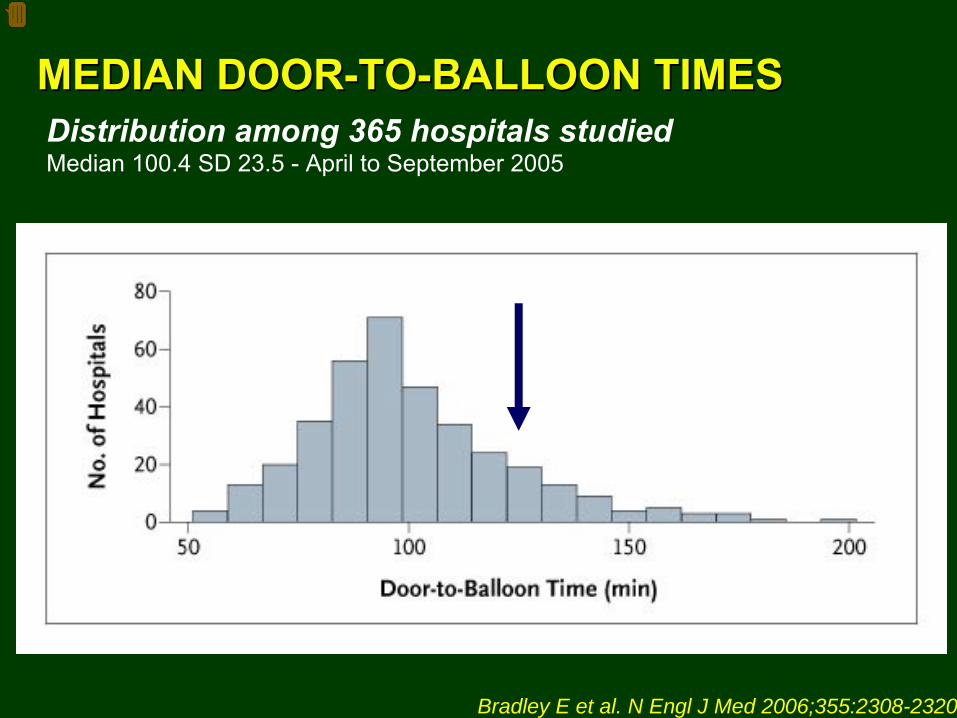
Distribution among 365 hospitals studiedMedian 100.4 SD 23.5 -
April to September 2005
Bradley E et al. N Engl J Med 2006;355:2308-2320
MEDIAN DOORMEDIAN DOOR--TOTO--BALLOON TIMESBALLOON TIMES
Presenter
Presentation Notes
Figure 1. Frequency Distribution for Median Door-to-Balloon Times among Study Hospitals. The median door-to-balloon time was calculated for each hospital in the study. The mean ({+/-}SD) of these median times was 100.4{+/-}23.5 minutes, which is considerably longer than the 90-minute interval recommended in the 2004 guidelines of the American Heart Association and the American College of Cardiology. DHMC: 2006 Median 107 min STDEV 58 min DHMC: 2007 YTD Median 117 min STDEV 42 min DHMC: Combinded Median 110 min STDEV
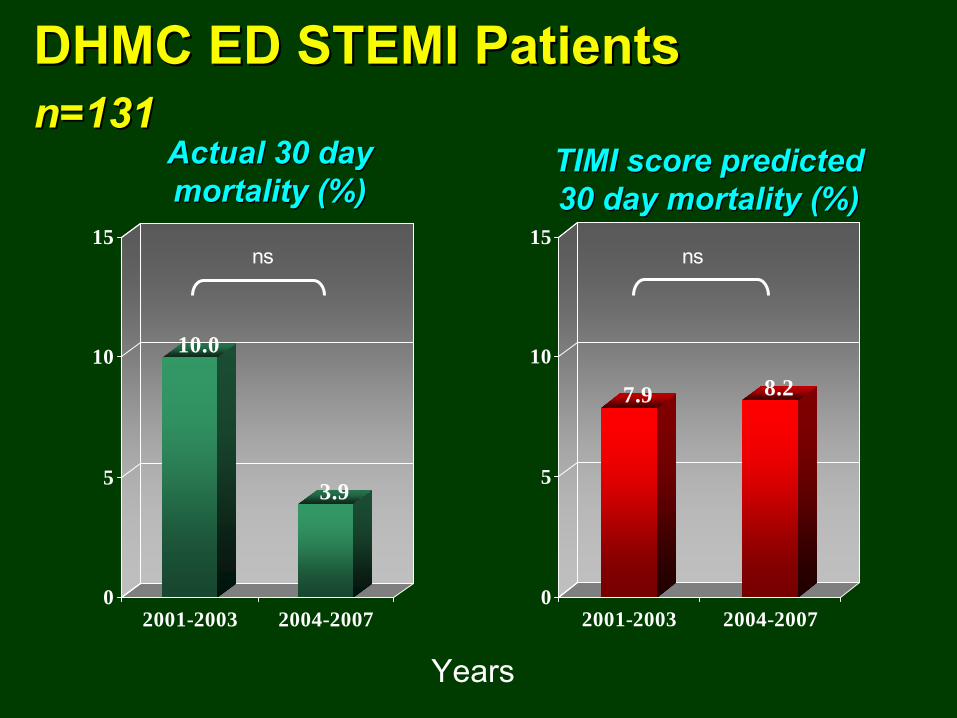
DHMC ED STEMI PatientsDHMC ED STEMI Patients n=131n=131
10.0
3.9
0
5
10
15
2001-2003 2004-2007
ns
Years
7.9 8.2
0
5
10
15
2001-2003 2004-2007
ns
Actual 30 day Actual 30 day mortality (%)mortality (%)
TIMI score predicted TIMI score predicted 30 day mortality (%)30 day mortality (%)
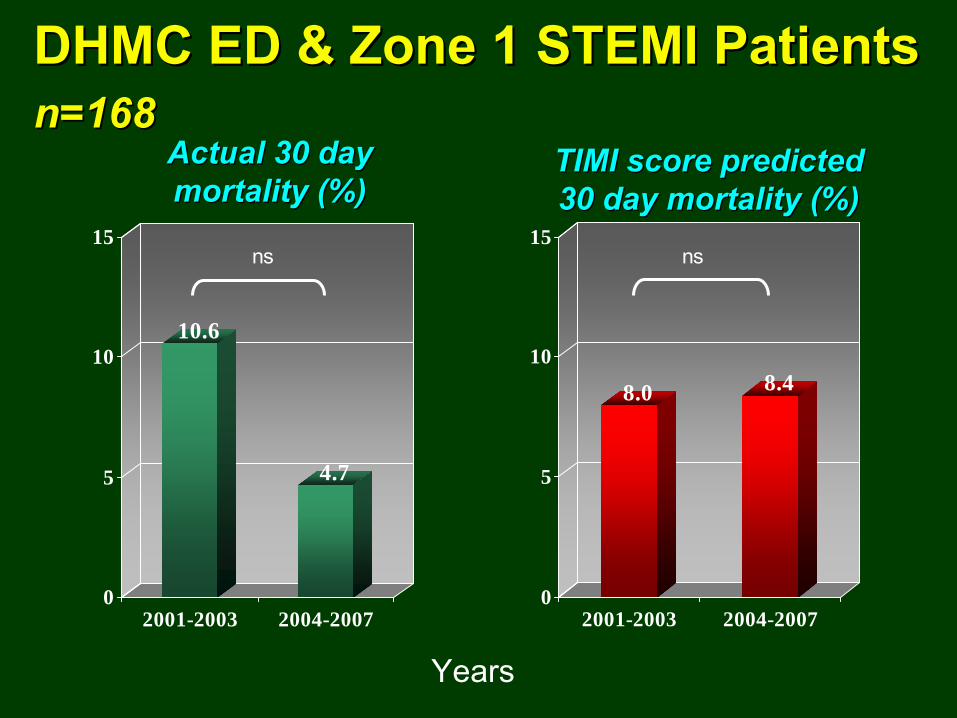
DHMC ED & Zone 1 STEMI PatientsDHMC ED & Zone 1 STEMI Patients n=168n=168
10.6
4.7
0
5
10
15
2001-2003 2004-2007
ns
Years
8.0 8.4
0
5
10
15
2001-2003 2004-2007
ns
Actual 30 day Actual 30 day mortality (%)mortality (%)
TIMI score predicted TIMI score predicted 30 day mortality (%)30 day mortality (%)
Zone 2 PatientsZone 2 Patients
(STEMI Patients Transferred from (STEMI Patients Transferred from Remote Referral Hospitals)Remote Referral Hospitals)
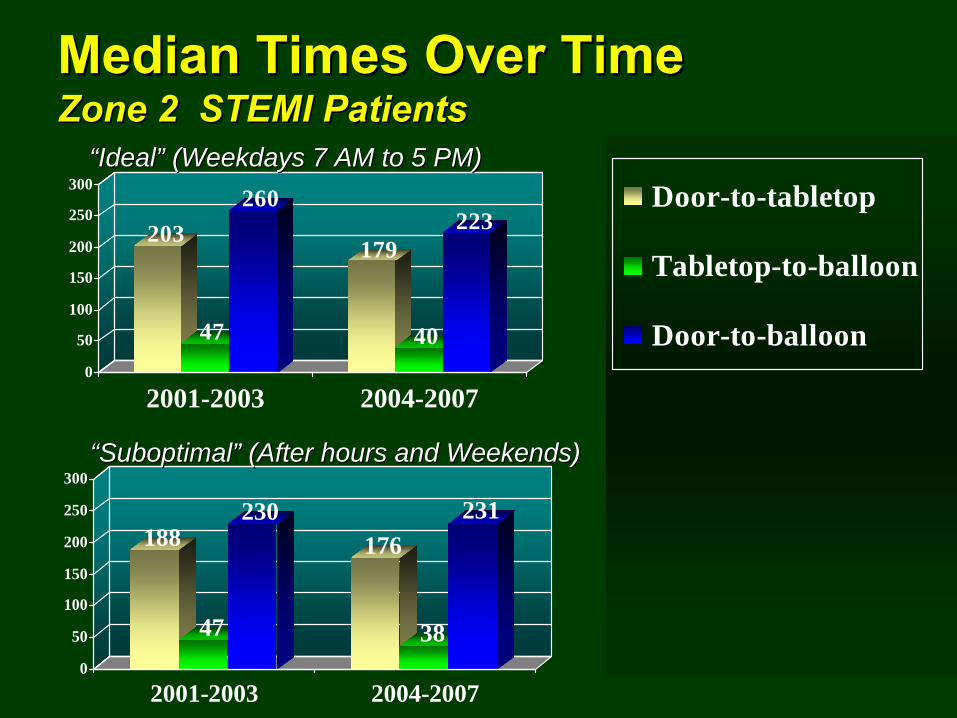
Median Times Over TimeMedian Times Over Time Zone 2 STEMI PatientsZone 2 STEMI Patients
188
47
230176
38
231
0
50
100
150
200
250
300
2001-2003 2004-2007
Door-to-tabletopTabletop-to-balloonDoor-to-balloon)
203
47
260
179
40
223
0
50
100
150
200
250
300
2001-2003 2004-2007
Door-to-tabletop
Tabletop-to-balloon
Door-to-balloon
““IdealIdeal”” (Weekdays 7 AM to 5 PM)(Weekdays 7 AM to 5 PM)
““SuboptimalSuboptimal”” (After hours and Weekends)(After hours and Weekends)
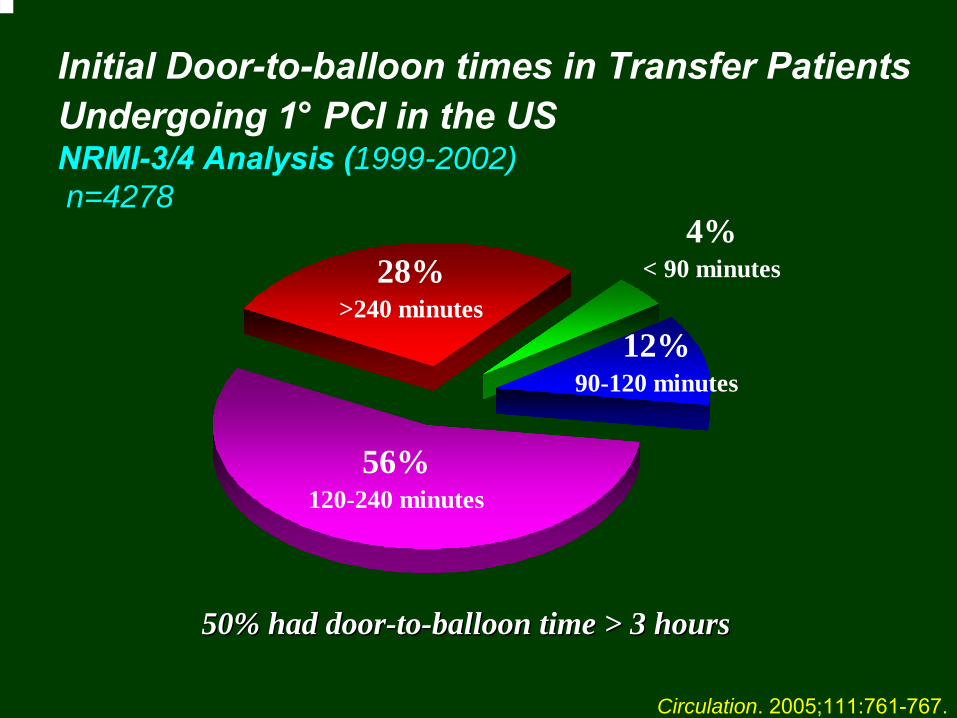
Initial Door-to-balloon times in Transfer Patients Undergoing 1°
PCI in the US
NRMI-3/4 Analysis (1999-2002) n=4278
12%90-120 minutes
56%120-240 minutes
4% < 90 minutes 28%
>240 minutes
Circulation. 2005;111:761-767.
50% had door50% had door--toto--balloon time > 3 hoursballoon time > 3 hours
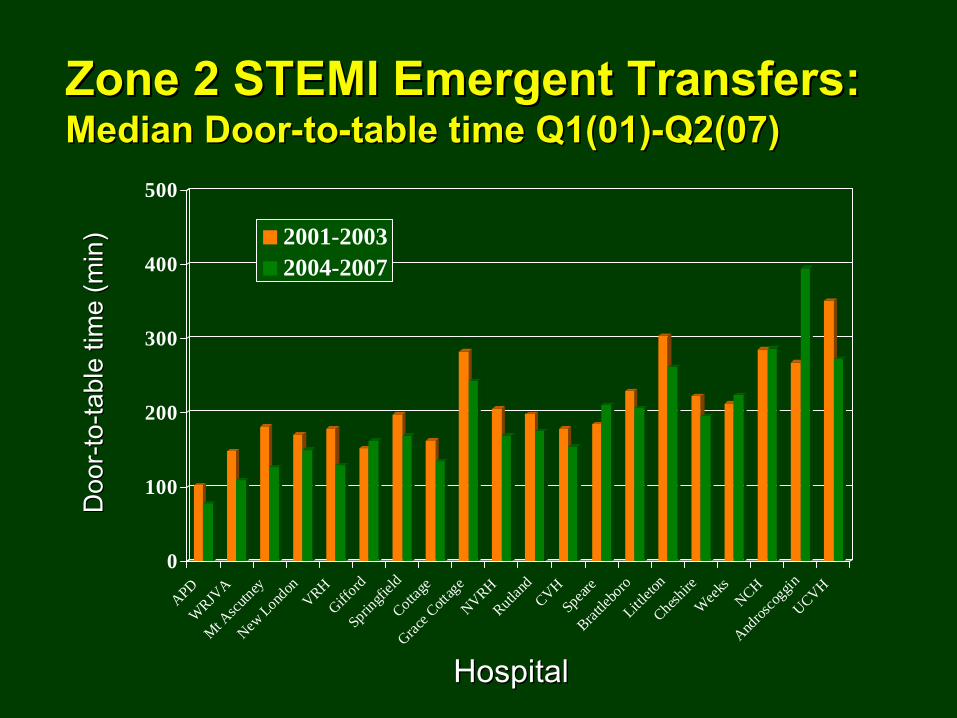
Zone 2 STEMI Emergent Transfers: Zone 2 STEMI Emergent Transfers: Median DoorMedian Door--toto--table time Q1(01)table time Q1(01)--Q2(07)Q2(07)
0
100
200
300
400
500
APDW
RJVA
Mt Ascu
tneyNew
London
VRHGiff
ordSprin
gfield
Cottage
Grace C
ottag
eNVRHRutla
ndCVHSpear
eBrat
tlebo
roLittl
eton
Cheshire
Wee
ksNCH
Andros
coggin
UCVH
2001-20032004-2007
Doo
rD
oor -- t
oto-- ta
ble
time
(min
)ta
ble
time
(min
)
HospitalHospital
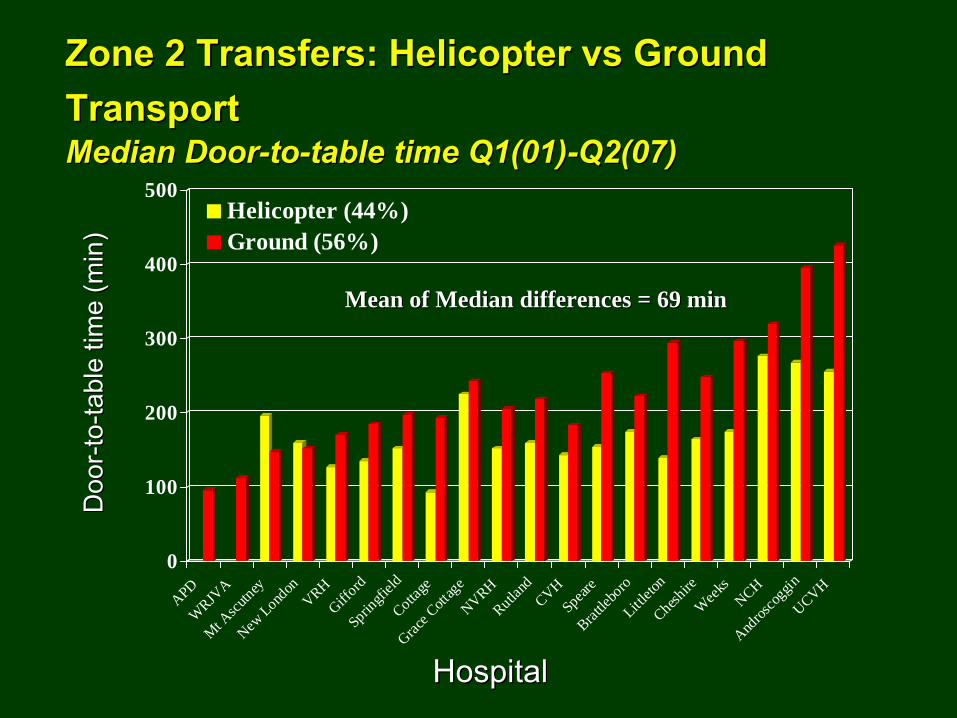
Zone 2 Transfers: Helicopter Zone 2 Transfers: Helicopter vsvs
Ground Ground TransportTransport
Median DoorMedian Door--toto--table time Q1(01)table time Q1(01)--Q2(07)Q2(07)
0
100
200
300
400
500
APDW
RJVA
Mt Ascu
tneyNew
London
VRHGiff
ordSprin
gfield
Cottage
Grace C
ottag
eNVRHRutla
ndCVHSpear
eBrat
tlebo
roLittl
eton
Cheshire
Wee
ksNCH
Andros
coggin
UCVH
Helicopter (44%)Ground (56%)
Doo
rD
oor -- t
oto-- ta
ble
time
(min
)ta
ble
time
(min
)
HospitalHospital
Mean of Median differences = 69 minMean of Median differences = 69 min

STEMI Emergent Transfer Volumes STEMI Emergent Transfer Volumes Q1(01)Q1(01)--Q2(07)Q2(07)
0
10
20
30
40
50
60
70
80
90
100
Q1(01)
Q2(01)
Q3(01)
Q4(01)
Q1(02)
Q2(02)
Q3(02)
Q4(02)
Q1(03)
Q2(03)
Q3(03)
Q4(03)
Q1(04)
Q2(04)
Q3(04)
Q4(04)
Q1(05)
Q2(05)
Q3(05)
Q4(05)
Q1(06)
Q2(06)
Q3(06)
Q4(06)
Q1(07)
Q2(07)
Half Dose
Full Dose
No Lytic Given
Ukn
Per
cent
of S
TEM
I Pat
ient
sP
erce
nt o
f STE
MI P
atie
nts

Zone 2 STEMI Emergent Transfer Patients: Zone 2 STEMI Emergent Transfer Patients: By Intended DoseBy Intended Dose
30 Day Mortality30 Day Mortality
11.8
7
3.5
02468
101214161820
None Given Full Dose Half Dose
% M
orta
lity
Lytic Dose Strategy
nsp<0.0006
p=0.08
N=136N=136 N=171N=171 N=339N=339
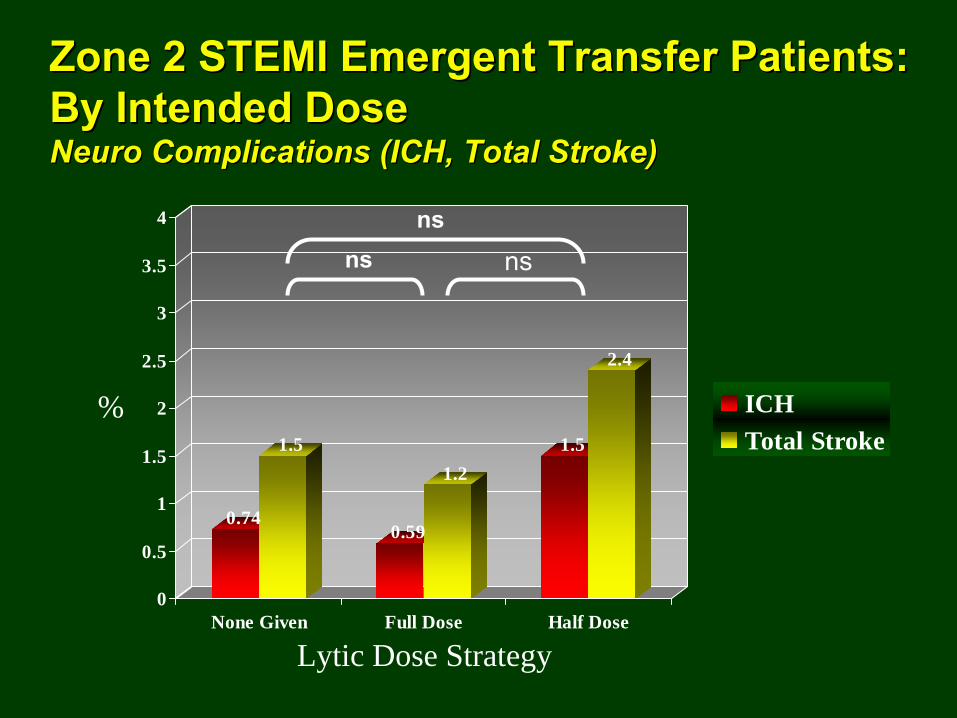
Zone 2 STEMI Emergent Transfer Patients: Zone 2 STEMI Emergent Transfer Patients: By Intended DoseBy Intended Dose
NeuroNeuro
Complications (ICH, Total Stroke)Complications (ICH, Total Stroke)
0.74
1.5
0.59
1.21.5
2.4
0
0.5
1
1.5
2
2.5
3
3.5
4
None Given Full Dose Half Dose
ICHTotal Stroke
%
Lytic Dose Strategy
nsns
ns

Zone 2 Transfer PatientsZone 2 Transfer Patients n=641n=641
8.1
5.1
0
5
10
15
2001-2003 2004-2007
ns
Years
7.6 7.5
0
5
10
15
2001-2003 2004-2007
ns
Actual 30 day Actual 30 day mortality (%)mortality (%)
TIMI Score predicted TIMI Score predicted 30 day mortality (%)30 day mortality (%)
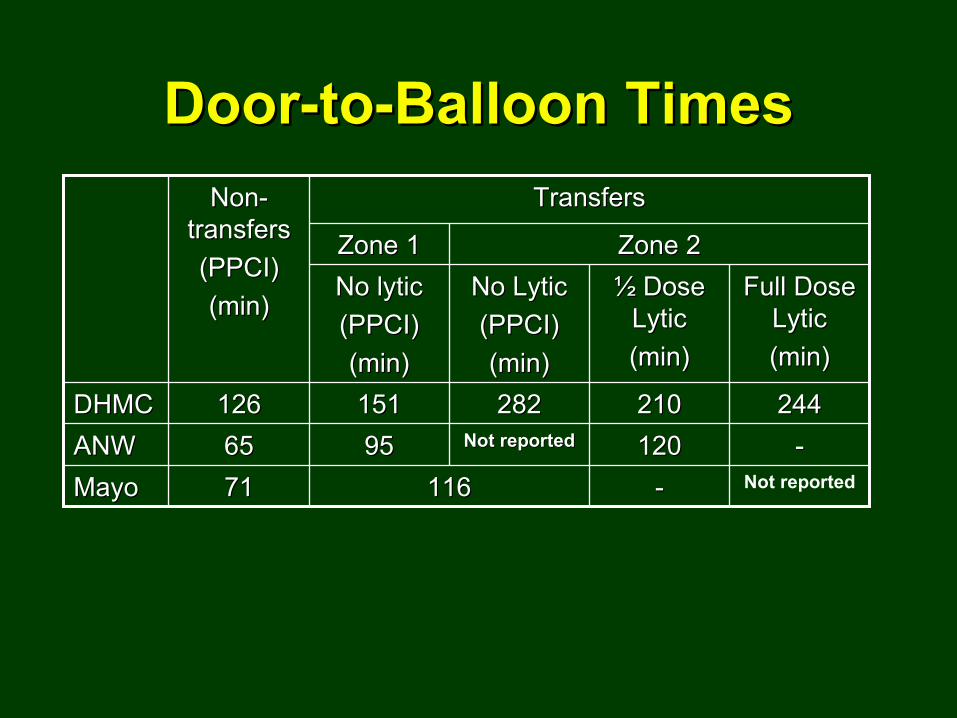
DoorDoor--toto--Balloon TimesBalloon TimesNonNon--
transferstransfers(PPCI)(PPCI)(min)(min)
TransfersTransfers
Zone 1Zone 1 Zone 2Zone 2No lyticNo lytic(PPCI)(PPCI)(min)(min)
No No LyticLytic(PPCI)(PPCI)(min)(min)
½½
Dose Dose LyticLytic(min)(min)
Full Dose Full Dose LyticLytic(min)(min)
DHMCDHMC 126126 151151 282282 210210 244244ANWANW 6565 9595 Not reportedNot reported 120120 --MayoMayo 7171 116116 -- Not reported
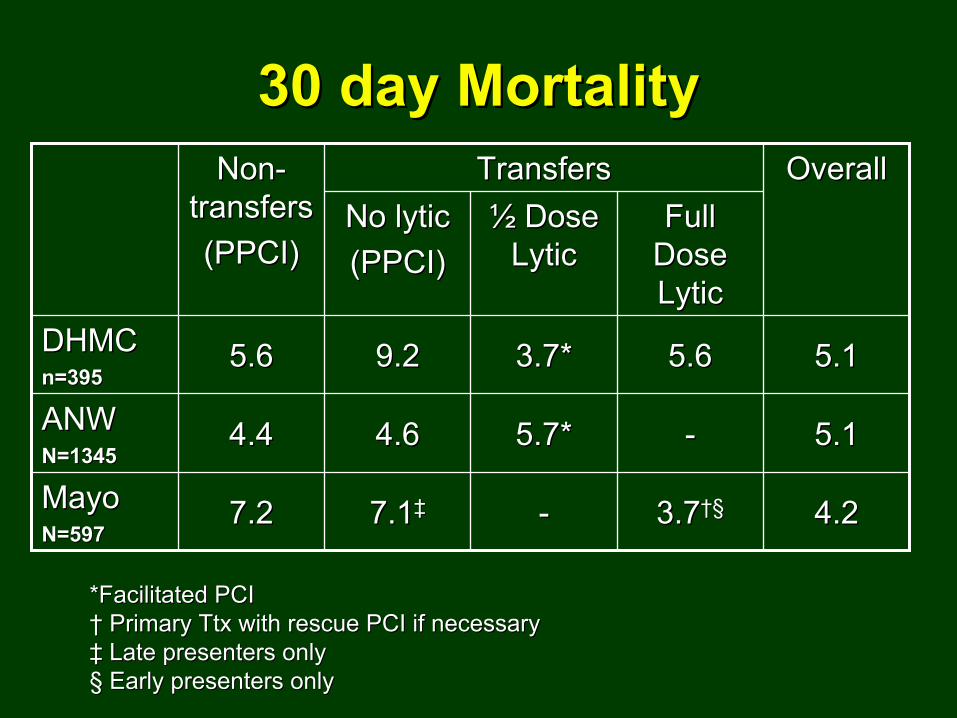
30 day Mortality30 day MortalityNonNon--
transferstransfers(PPCI)(PPCI)
TransfersTransfers OverallOverallNo lyticNo lytic(PPCI)(PPCI)
½½
Dose Dose LyticLytic
Full Full Dose Dose LyticLytic
DHMCDHMCn=395n=395
5.65.6 9.29.2 3.7*3.7* 5.65.6 5.15.1
ANWANWN=1345N=1345
4.44.4 4.64.6 5.7*5.7* -- 5.15.1
MayoMayoN=597N=597
7.27.2 7.17.1‡‡ -- 3.73.7††§§ 4.24.2
*Facilitated PCI *Facilitated PCI ††
Primary Ttx with rescue PCI if necessaryPrimary Ttx with rescue PCI if necessary‡‡
Late presenters onlyLate presenters only§§
Early presenters onlyEarly presenters only
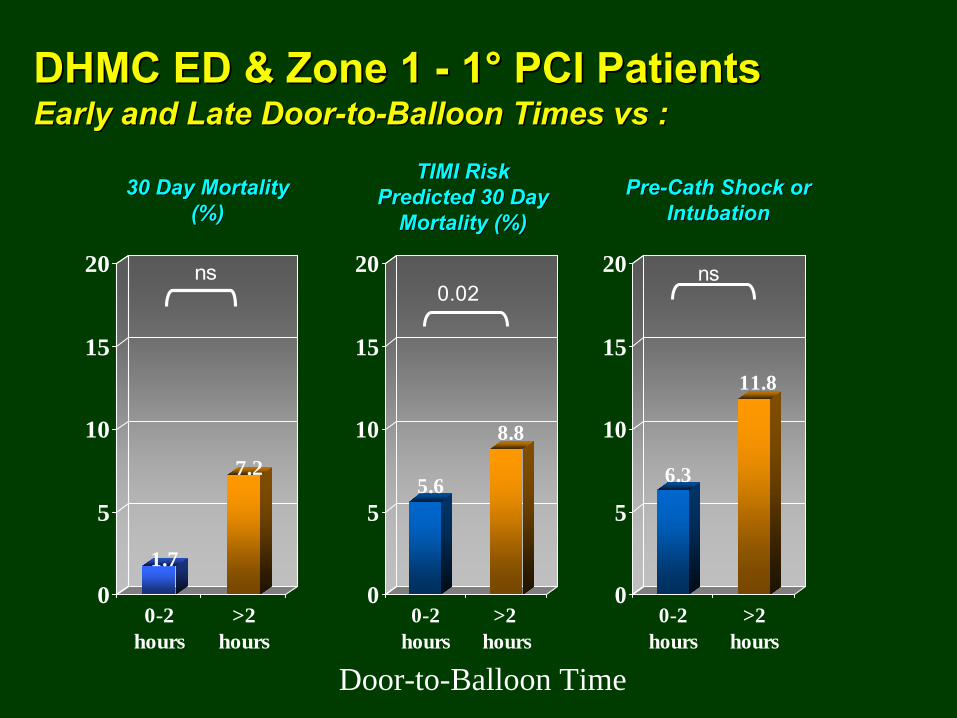
DHMC ED & Zone 1 DHMC ED & Zone 1 --
11°°
PCI PatientsPCI Patients Early and Late DoorEarly and Late Door--toto--Balloon Times Balloon Times vsvs
::
1.7
7.2
0
5
10
15
20
0-2hours
>2hours
ns
Door-to-Balloon Time
5.6
8.8
0
5
10
15
20
0-2hours
>2 hours
0.02
30 Day Mortality 30 Day Mortality (%)(%)
TIMI Risk TIMI Risk Predicted 30 Day Predicted 30 Day
Mortality (%)Mortality (%)PrePre--CathCath
Shock or Shock or IntubationIntubation
6.3
11.8
0
5
10
15
20
0-2hours
>2hours
ns
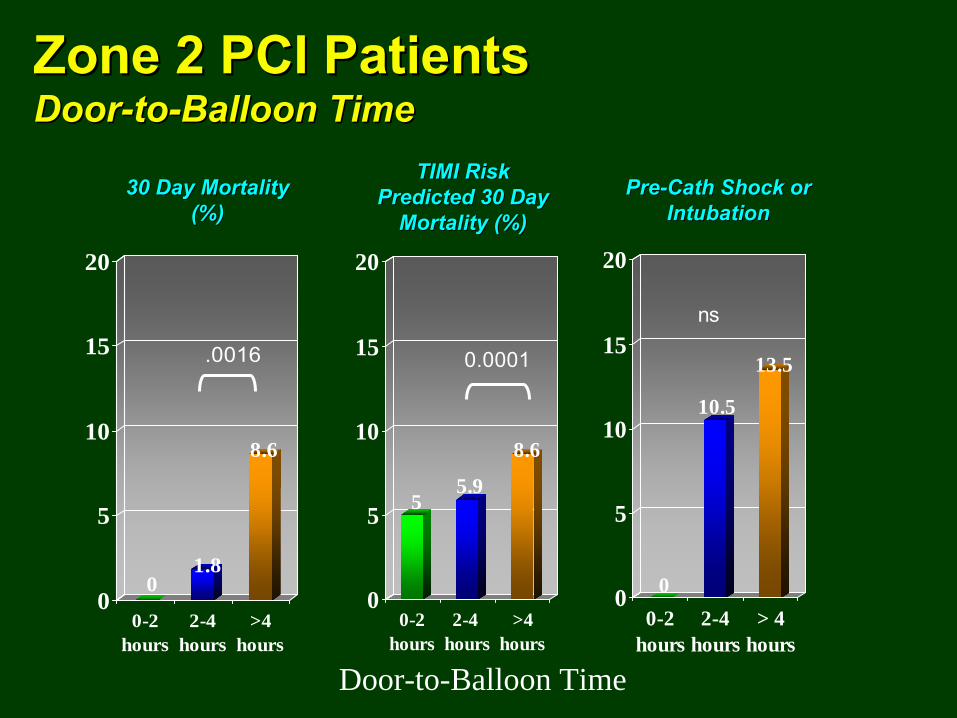
Zone 2 PCI PatientsZone 2 PCI Patients DoorDoor--toto--Balloon TimeBalloon Time
01.8
8.6
0
5
10
15
20
0-2hours
2-4hours
>4hours
.0016
Door-to-Balloon Time
55.9
8.6
0
5
10
15
20
0-2hours
2-4 hours
>4hours
0.0001
30 Day Mortality 30 Day Mortality (%)(%)
TIMI Risk TIMI Risk Predicted 30 Day Predicted 30 Day
Mortality (%)Mortality (%)PrePre--CathCath
Shock or Shock or IntubationIntubation
0
10.5
13.5
0
5
10
15
20
0-2hours
2-4hours
> 4hours
ns
Can we be satisfiedCan we be satisfied…… No!No!
•• InIn--
house D2B times are too slowhouse D2B times are too slow•• We can see a relationship between D2B time and We can see a relationship between D2B time and
30 day outcome in our overall data30 day outcome in our overall data•• Less than 20% of our patients are offered 1Less than 20% of our patients are offered 1ºº
PCI PCI
•• ICH risk of ICH risk of ½½
dose dose lyticlytic
protocol (1.5%protocol (1.5%--
in our in our hands too high?)hands too high?)
•• A STEMI Center Certification Program is in the A STEMI Center Certification Program is in the works (Criteria for eligibility will likely be based on works (Criteria for eligibility will likely be based on treatment times and volumes as well as quality treatment times and volumes as well as quality outcomes)outcomes)
•• PayPay--forfor--performance reimbursement strategies performance reimbursement strategies are here or comingare here or coming
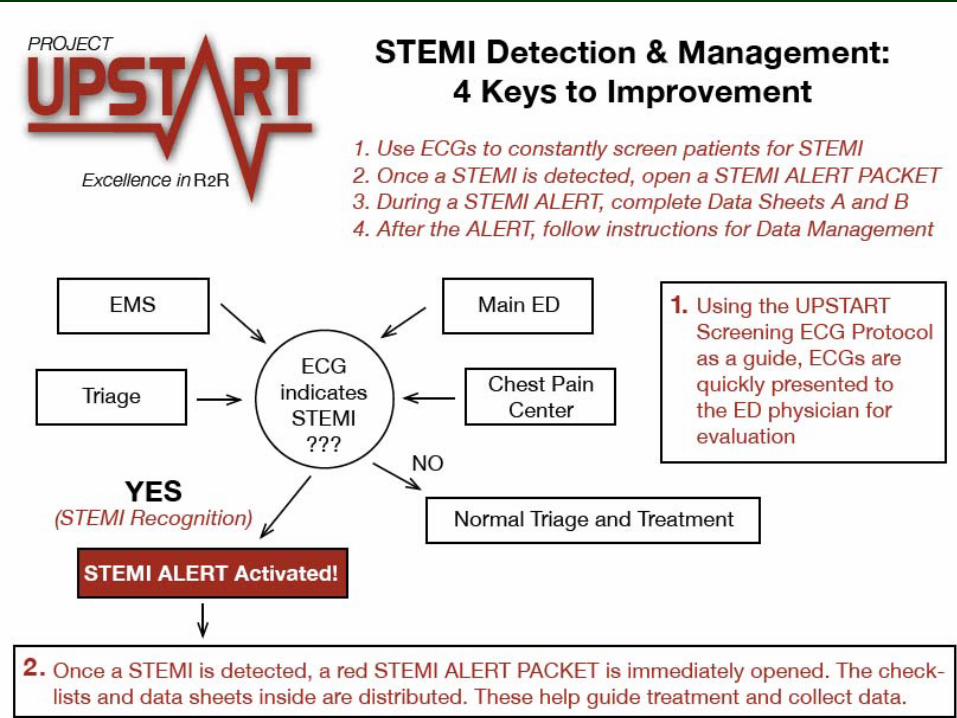
ST
Elevation MI Process UpgradeSTEP UP Project
Obtain commitment of DHMC Senior managementForm a multidisciplinary group with members from Cardiology, Emergency medicine, EMS, Communications, CCU, Cardiac Cath Lab, DHMC administration and Quality managementIdentify/develop and implement strategies which improve the process of care, treatment times and outcomes of STEMI patients within our hospital and within our region
STEP 1 STEP 1 --
Get OrganizedGet Organized
STEP UP
Project: Goals1.
Implement proven strategies for reducing Door-
to-balloon time to < 90 min in > 75% of STEMI patients
2.
Design a STEMI pre-hospital triage network for the purpose of providing timely primary angioplasty to STEMI patients from an enlarged geographic area around DHMC
3.
Critically assess our current inter-hospital transfer system including the current facilitated PCI program in order to identify process/protocol improvements
D2B: An Alliance for Quality D2B: An Alliance for Quality EvidenceEvidence--based Strategies based Strategies for reducing Door-
to-balloon time to < 90 min in > 75% of STEMI patients
1.1.
ED physician activates the cath labED physician activates the cath lab2.2.
One call activates the cath labOne call activates the cath lab
3.3.
CathCath
lab team ready in 20lab team ready in 20--30 minutes30 minutes4.4.
Prompt data feedbackPrompt data feedback
5.5.
TeamTeam--based approachbased approach6.6.
PrePre--hospital ECG to activate the hospital ECG to activate the cathcath
lab*lab*
STEP 2 STEP 2 --
Improve InImprove In--house D2Bhouse D2B
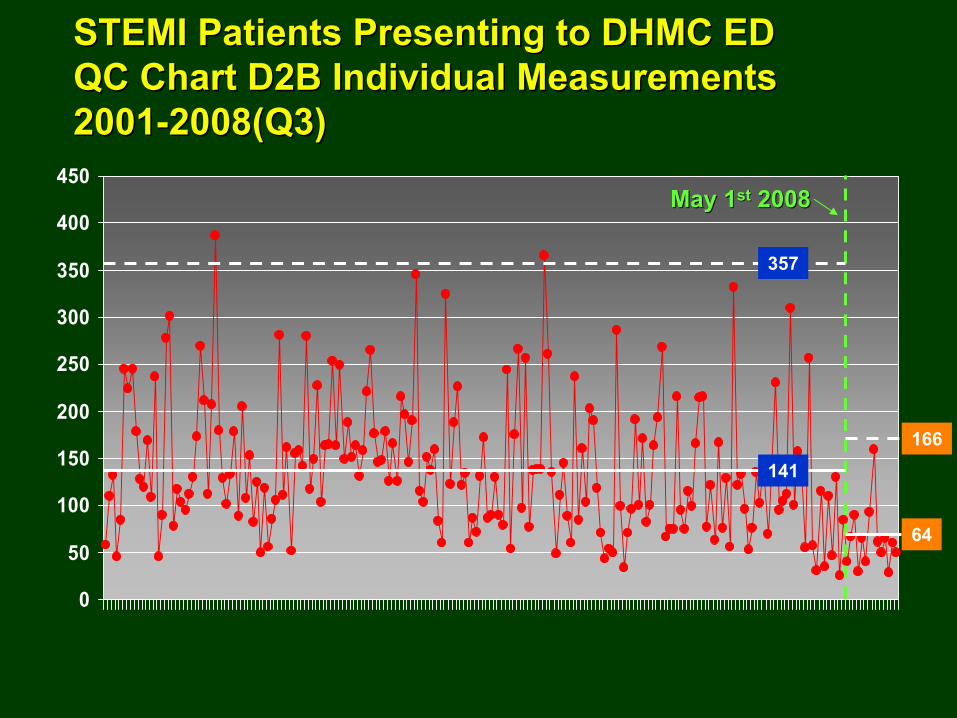
STEMI Patients Presenting to DHMC EDSTEMI Patients Presenting to DHMC ED QC Chart D2B Individual MeasurementsQC Chart D2B Individual Measurements 20012001--2008(Q3)2008(Q3)
0
50
100
150
200
250
300
350
400
450
141
64
May 1May 1stst
20082008
357
166
0
25
50
75
100
1stQtr'01
2ndQtr'01
3rdQtr'01
4thQtr'01
1stQtr'02
2ndQtr'02
3rdQtr'02
4thQtr'02
1stQtr'03
2ndQtr'03
3rdQtr'03
4thQtr'03
1stQtr'04
2ndQtr'04
3rdQtr'04
4thQtr'04
1stQtr'05
2ndQtr'05
3rdQtr'05
4thQtr'05
1stQtr'06
2ndQtr'06
3rdQtr'06
4thQtr'06
1stQtr'07
2ndQtr'07
3rdQtr'07
4thQtr'07
1stQtr'08
2ndQtr'08
3rdQtr'08
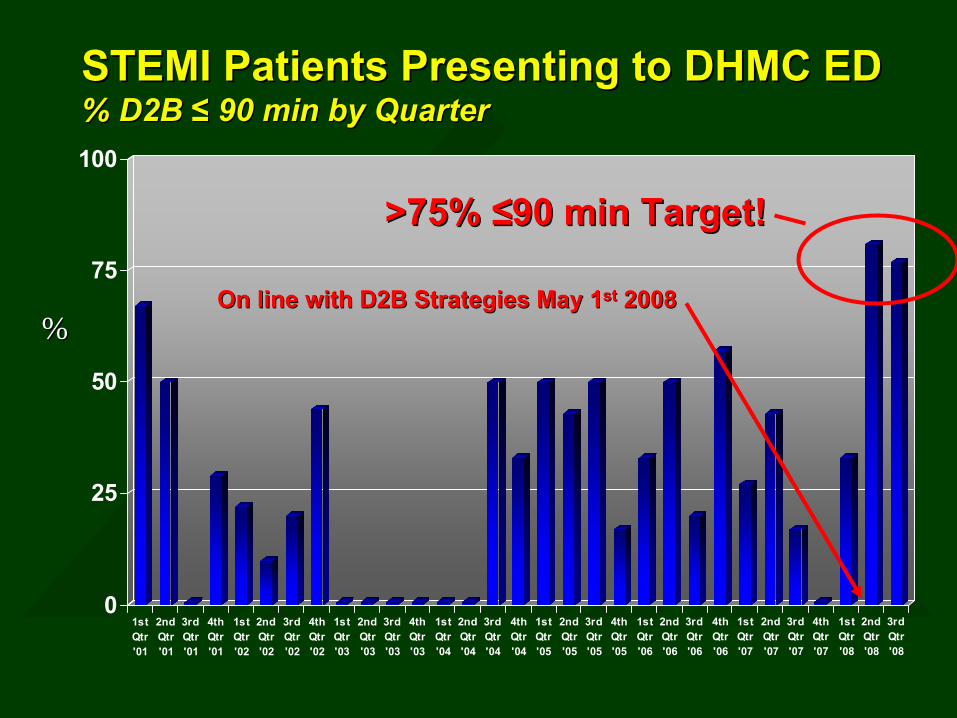
STEMI Patients Presenting to DHMC EDSTEMI Patients Presenting to DHMC ED % D2B % D2B ≤≤
90 min by Quarter90 min by Quarter
On line with D2B Strategies May 1On line with D2B Strategies May 1stst
20082008
>75% >75% ≤≤90 min Target!90 min Target!
%%
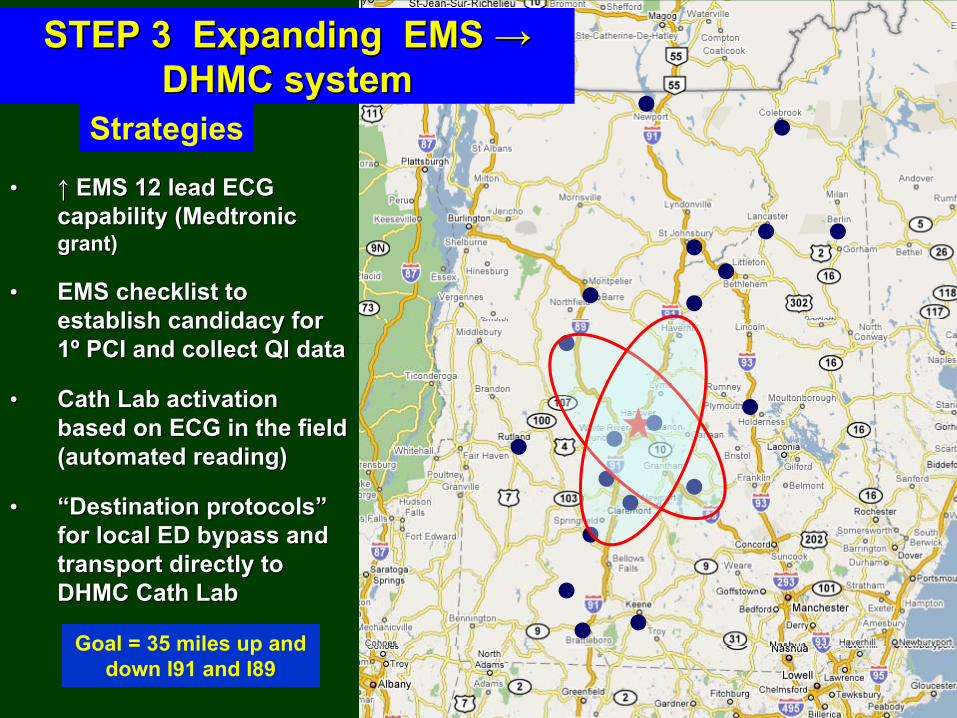
STEP 3 Expanding EMS STEP 3 Expanding EMS →→ DHMC systemDHMC system
•• ↑↑
EMS 12 lead ECG EMS 12 lead ECG capability (Medtronic capability (Medtronic grant)grant)
•• EMS checklist to EMS checklist to establish candidacy for establish candidacy for 11ºº
PCI and collect QI dataPCI and collect QI data
•• CathCath
Lab activation Lab activation based on ECG in the field based on ECG in the field (automated reading)(automated reading)
•• ““Destination protocolsDestination protocols””
for local ED bypass and for local ED bypass and transport directly to transport directly to DHMC DHMC CathCath
LabLab
Goal = 35 miles up and down I91 and I89
Strategies
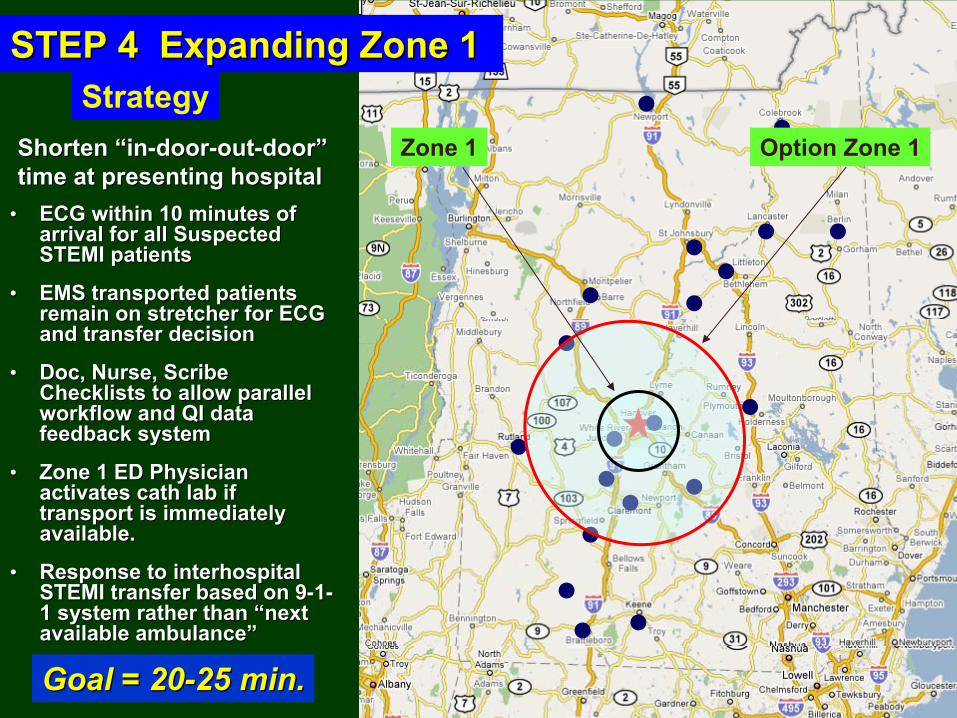
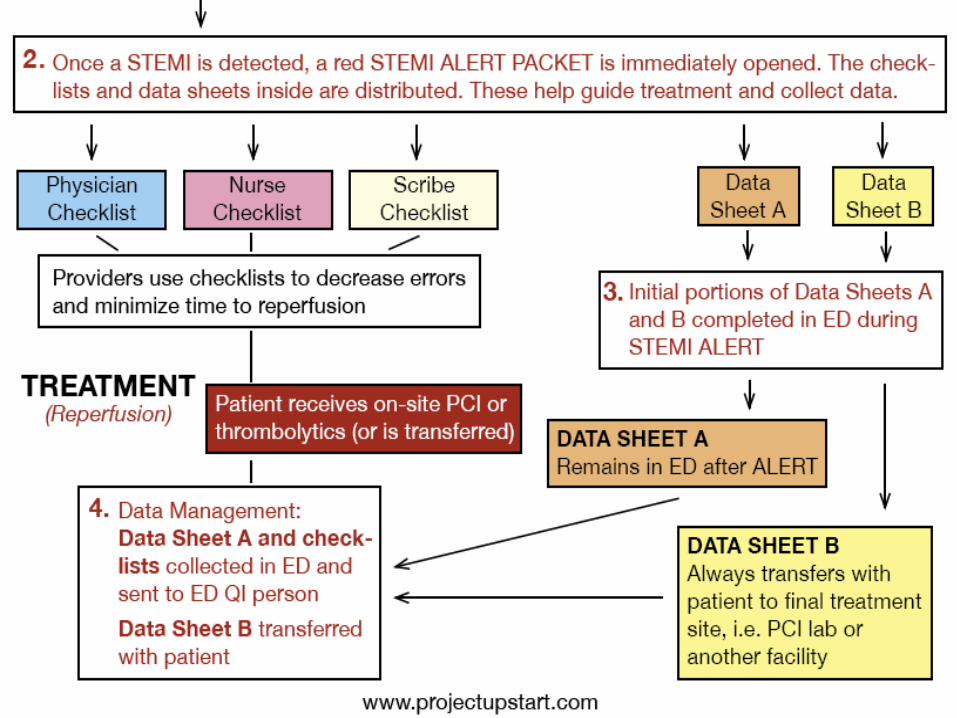
•• ECG within 10 minutes of ECG within 10 minutes of arrival for all Suspected arrival for all Suspected STEMI patientsSTEMI patients
•• EMS transported patients EMS transported patients remain on stretcher for ECG remain on stretcher for ECG and transfer decisionand transfer decision
•• Doc, Nurse, Scribe Doc, Nurse, Scribe Checklists to allow parallel Checklists to allow parallel workflow and QI data workflow and QI data feedback systemfeedback system
•• Zone 1 ED Physician Zone 1 ED Physician activates activates cathcath
lab if lab if transport is immediately transport is immediately available. available.
•• Response to Response to interhospitalinterhospital
STEMI transfer based on 9STEMI transfer based on 9--11--
1 system rather than 1 system rather than ““next next available ambulanceavailable ambulance””
STEP 4 Expanding Zone 1STEP 4 Expanding Zone 1
Shorten Shorten ““inin--doordoor--outout--doordoor””
time at presenting hospitaltime at presenting hospital
Zone 1 Option Zone 1
Goal = 20Goal = 20--25 min.25 min.
Strategy


Rethink the Zone 2 StrategyRethink the Zone 2 Strategy
•• Continue the Facilitated PCI option?Continue the Facilitated PCI option?•• Selected patients only?Selected patients only?•• Change Change lyticlytic
regimen?regimen?
STEP 5STEP 5
√√
YesYes
√√
NoNo
√√
YesYes

The The PharmacoPharmaco--invasive Option for Zone 2 Patientsinvasive Option for Zone 2 Patients Alternative RegimensAlternative Regimens
½½
dose dose LyticLytic
plus GP plus GP 2b3a inhibitor plus low 2b3a inhibitor plus low dose heparin infusion dose heparin infusion followed by PCI ASAPfollowed by PCI ASAP
ProsPros ProsProsSuperior to Superior to ““StandStand--alonealone””
lyticlytic
TxTx
in in CARESS TrialCARESS Trial
Superior to Superior to ““StandStand--alonealone””
lyticlytic
TxTx
in in TRANSFER AMI and CAPITAL AMI TRANSFER AMI and CAPITAL AMI TrialsTrials
Benefits early presentersBenefits early presenters Benefits early presentersBenefits early presentersWe have good mortality track recordWe have good mortality track record Simpler / QuickerSimpler / Quicker
ConsCons ConsConsIncreased bleeding/ICH in our handsIncreased bleeding/ICH in our hands More Bleeding / ICH riskMore Bleeding / ICH risk
Not guideline compliantNot guideline compliantComplex and time consumingComplex and time consuming
Full dose Full dose lyticlytic
and and clopidogrelclopidogrel
plus low plus low
dose heparin bolus dose heparin bolus followed by PCI ASAPfollowed by PCI ASAP
Questions?Questions?