THE RENAL AND METABOLIC MORPHO … · ATHEROSCLEROTIC CORONARY ARTERY DISEASE 8 2.1. Generalities...
27
THE RENAL AND METABOLIC MORPHO-FUNCTIONAL PROFILE OF PATIENTS WITH ACUTE MIOCARDIAL INFARCTION REVASCULARIZED BY PRIMARY PERCUTANEOUS CORONARY ANGIOPLASTY PHD THESIS SUMMARY SCIENTIFIC COORDINATOR: Prof. Dr. COVIC Adrian PHD STUDENT: BURLACU Alexandru 2017
-
Upload
truongdieu -
Category
Documents
-
view
218 -
download
0
Transcript of THE RENAL AND METABOLIC MORPHO … · ATHEROSCLEROTIC CORONARY ARTERY DISEASE 8 2.1. Generalities...

THE RENAL AND METABOLIC MORPHO-FUNCTIONAL
PROFILE OF PATIENTS WITH ACUTE MIOCARDIAL
INFARCTION REVASCULARIZED BY PRIMARY
PERCUTANEOUS CORONARY ANGIOPLASTY
PHD THESIS SUMMARY
SCIENTIFIC COORDINATOR:
Prof. Dr. COVIC Adrian
PHD STUDENT:
BURLACU Alexandru
2017
i
CONTENTS
ABBREVIATIONS iii
GENERAL PART
CHAPTER 1. CHRONIC KIDNEY DISEASE 1
1.1. Definitions and classifications 1
1.2. Risk factors for chronic kidney disease 4
1.3. Modalities of evaluation of renal function 5
1.4. Chronic advanced kidney disease – “end-stage renal disease” 6
CHAPTER 2. ATHEROSCLEROTIC CORONARY ARTERY DISEASE 8
2.1. Generalities and classifications 8
2.2. Coronary atherosclerosis - localization of a systemic pathology 10
2.3. Heart Team Concept 12
2.4. Acute ST segment elevation myocardial infarction 13
2.4.1. Definition and prognosis in the short / long term 13
2.4.2. Treatment algorithms - the role of primary percutaneous coronary
intervention (PCI) 14
2.4.3. Current state of STEMI management in Romania - National Program
of Invasive Treatment of Acute Myocardial Infarction 15
CHAPTER 3. INTERRELATIONSHIPS – RENAL DYSFUNCTION AND
CORONARY ARTERY DISEASE 17
3.1. Cardio-renal syndromes - definitions and classifications 17
3.2. Chronic kidney disease - a cardiovascular risk factor 18
3.3. Atherosclerotic coronary artery disease - an independent risk factor for the
decline in renal function 21
CHAPTER 4. ACUTE KIDNEY INJURY – CONTRAST MEDIA INDUCED
22
4.1. Definitions, generalities and classifications 22
4.2. Epidemiology and pathophysiological mechanisms 24
4.3. Complications of acute kidney injury 25
4.4. Acute renal failure in patients with acute coronary syndrome 26
CHAPTER 5. RENAL ARTERY STENOSIS 27
5.1. Definition and classification 27
5.2. Consequences of renal artery stenosis 27
5.3. Established methods and modern diagnostic methods 29
5.4. Controversy regarding the treatment of renal artery stenosis 31
5.5. Pathogenic features: risk groups and screening 34
CHAPTER 6. ARTERIAL STIFFNESS 36
6.1. General and surrogate markers 36
ii
6.2. Dynamics of structural and functional modifications of the stiffened
arterial wall 36
6.3. Clinical implications and influence of vascular stiffness on cardiovascular
prognosis 38
6.4. Therapeutic features 39
CHAPTER 7. MULTI-SITE ATEROSCLEROTIC ARTERIAL DISEASE 41
7.1. Definition and utility 41
7.2. Prognostic and screening in different clinical scenarios 42
7.3. Coronary atherosclerosis and other peripheral determinations (carotid,
renal or lower limbs) - management problems 43
PERSONAL PART
CHAPTER 8. MOTIVATION, GENERAL OBJECTIVES AND STRUCTURE
OF DOCTORAL RESEARCH 45
CHAPTER 9. RENAL ARTERY STENOSIS IN STEMI PATIENTS INCLUDED
IN NATIONAL PRIMARY PERCUTANEOUS REVASCULARIZATION
PROGRAM: PREVALENCE AND CORRELATIONS 48
9.1. Introduction 48
9.2. Matherial and methods 49
9.2.1. The research protocol, the investigated population and the location of
the study 49
9.2.2. Ethical considerations 50
9.2.3. REN-ACS registry 51
9.2.4. Angiographic evaluation of renal and coronary arteries 56
9.2.5. Biological analyzes and cardiac ultrasound 64
9.2.6. Analysis of body composition 65
9.2.7. Measurements for the evaluation of arterial stiffness 66
9.2.8. Statistic analysis 68
9.2.9. CRUSADE score - method of assessing haemorrhagic risk 69
9.3. Results 69
9.3.1. Baseline features 69
9.3.2. Comparative view on patient group RAS + versus patient group RAS-
79
9.4. Discussions 85
9.4.1. Discussions on the general results of the REN-ACS registry 85
9.4.2. Discussions on RAS in REN-ACS 87
9.4.3. Discussions on ischemic and haemorrhagic risks in CKD and ACS
patients: a critical analysis of the Guidelines of the European Society of Cardiology
92
9.5. Conclusions 110

iii
CHAPTER 10. SYNTAX AND CLINICAL SYNTAX SCORES IN ACUTE
MIOCARDIAL INFARCTION PATIENTS WITH PRIMARY PCI:
CORRELATIONS AND PREDICTION OF RENAL ARTERY STENOSIS 111
10.1. Introduction 111
10.2. Materials and Methods 114
10.2.1. Study population, inclusion criteria and measurements 114
10.2.2. Stents types 114
10.2.3. SYNTAX score: calculation method 117
10.2.4. SYNTAX derived scores 126
10.2.5. Clinical SYNTAX score computation 127
10.2.6. Statistical analysis 128
10.3. Results 129
10.3.1. Descriptive statistics by SYNTAX score 130
10.3.2. Descriptive statistics by Clinical SYNTAX score 134
10.3.3. Correlative analyzes for the SYNTAX score and Clinical SYNTAX
score 137
10.3.4. Clinical SYNTAX score vs. SYNTAX score – as RAS + predictors
138
10.4. Discussions 139
10.5. Conclusions 141
CHAPTER 11. MAIN CONCLUSIONS 142
CHAPTER 12. ORIGINALITY AND PERSPECTIVES OF THESIS 143
REFERENCES 144
ANNEXES 168
Anex 1: Informed consent 168
The PhD thesis includes:
• The General part consists of 7 chapters totaling 45 pages
• The Personal part consists of 5 chapters totaling 100 pages
• Bibliographic references containing 448 bibliographical references
• Attachment section
• Iconography consisting of 77 tables and 66 figures
• List of articles published during the doctoral program: 3 ISI articles as first
author and 1 ISI article as second author.
The abstract selectively reproduces the iconography and bibliography in the text,
observing the numbering and the content of the thesis in extenso. The present
bibliographic references are identical to those existing in the PhD thesis.
Keywords, MeSH list: coronary artery disease, chronic kidney disease, renal artery
stenosis, acute miocardial infarction, SYNTAX score, arterial stiffness, dehidration,
prediction models, Guidelines, bleeding risk, thrombotic risk.
1
MOTIVATION, GENERAL OBJECTIVES AND STRUCTURE
OF DOCTORAL RESEARCH
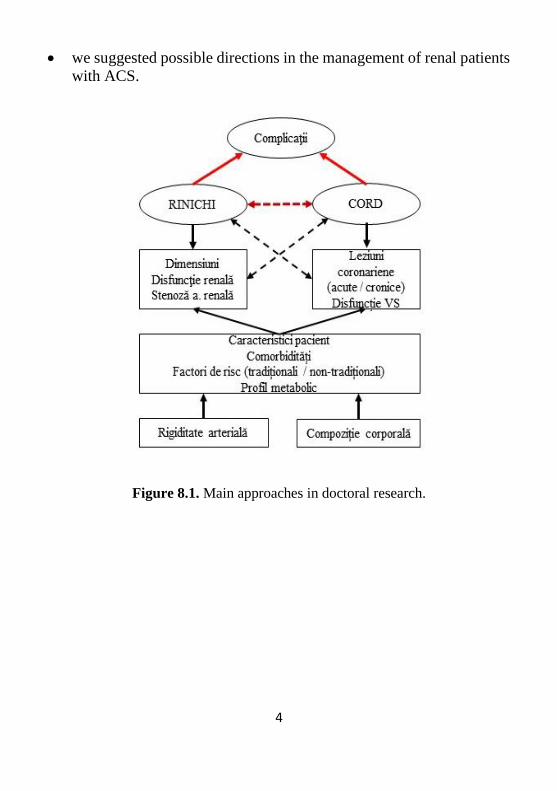
Our doctoral research mainly focuses on a complex analysis of
kidney-to-heart inter-relationships on several levels (kidney: structure,
function, renal artery, coronary epicardial arteries, myocardial systolic
function) in a particular clinical-metabolic context with acute myocardial
infarction, assessment of vascular rigidity, hydration composition)
(Figure 8.1).
The reasons why some study protocols have been developed and
numerous resources have been invested stem from the fundamental
premise that the number of patients with acute myocardial infarction or
with chronic kidney disease or both is extremely high. Both pathologies
frequently coexist and are generating numerous cardiovascular and renal
terminal complications, with extremely high morbidity and mortality.
To date, an increased volume of clinical trials and a very large
scientific community involved in the above mentioned pathology show
the major interest in both diseases and the financial resources invested
(both in research and in the implementation of new medications and
protocols). Newer measures and more effective protocols can simplify
the identification of those complex patients for whom complex and
expensive therapeutic resources are already invested. For example,
simple prediction of RAS presence in AMI patients may lead to the
development of screening protocols at the same time as the acute
coronary procedure.
In the argumentation of the doctoral motivation we took into
account that:
over 30% of patients with acute myocardial infarction have a chronic
renal dysfunction;
Chronic renal impairment influences the progression and short-term
prognosis of STEMI patients as well as the recurrence of coronary
events by one year;
medication given to patients with acute myocardial infarction is
sensitive (remittance) to renal function, and the latter is often severely
affected by AMI management (eg concomitant use may severely
2
aggravate renal dysfunction or the administration of inhibitors of
angiotensin converting enzyme may increase the degree of pre-
existing renal dysfunction);
the main cause of mortality in kidney patients is cardiovascular (of
which myocardial infarction is an important percentage);
the percentage of RAS in patients with CAD (non-acute) is important
(one in five chronic CAD patients also has significant RAS;
the RAS prevalence is still unknown in patients with AMI;
RAS predictors in patients with AMI are not evaluated in order to
develop a screening protocol simultaneously with the
coronarography time;
these patients with ACS have no morpho-functional characterization
of the kidney (kidney arteries, kidney size, glomerular filtration rate);
there is no data on the metabolic profile of patients with AMI and
RAS (serum lipids, glycemia);
no vascular rigidity measurements were performed in patients with
renal and coronary multi-site atherosclerotic lesions (especially in
patients with acute coronary syndromes);
there is no hydration status data in coronary patients (in acute
myocardial infarction) with or without RAS;
there are no data on the usefulness and correlations between
complexity scores of coronary lesions (SYNTAX, Clinical
SYNTAX) and other peripheral determinations (RAS);
there is no uniform assessment of hemorrhagic and ischemic risk in
ACS in renal patients;
management recommendations (stratification of ischemic and
hemorrhagic risk) in ESC guidelines in renal patients suffering from
acute coronary events are scattered and often devoid of evidence;
there are numerous "sensitive areas" in the context of ESC treatment
guidelines for patients with advanced CKD and coronary artery
disease (because randomized trials have excluded patients with renal
dysfunction in principle).
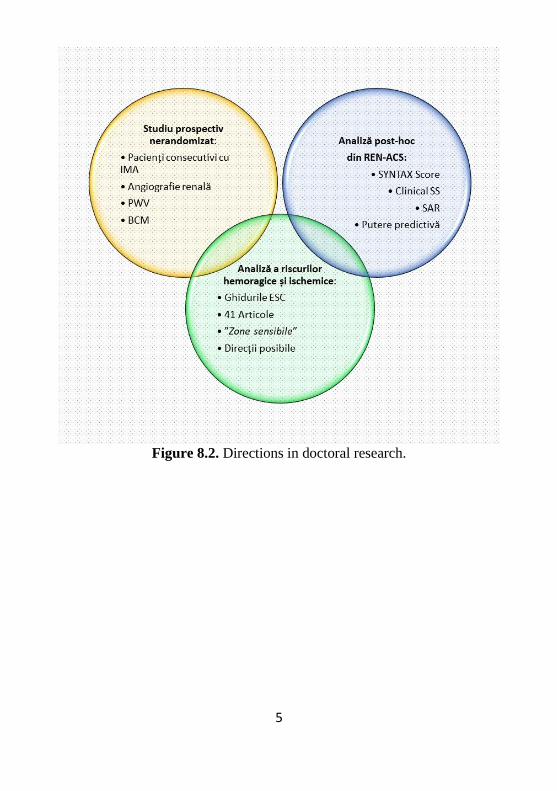
Our doctoral research aims to investigate and clarify the above-
mentioned aspects by going on three intersecting directions (Figure 8.2):

3
1. A prospective non-randomized unicentric study, in which:
we enrolled a group of consecutive patients with acute myocardial
infarction;
we evaluated the presence of renal artery stenosis by renal
angiography simultaneously with the cardiac catheterization
procedure;
we have set up a register based on the European CARDS standards;
we have entered data on enrolled patients (demographics, co-
morbidities, blood tests, echocardiographic parameters);
we measured and recorded vascular rigidity parameters;
we measured and recorded hydric status and body composition by
bioimpedance;
we subsequently analyzed correlations between the presence of RAS
and the other characteristics of patients with AMI;
we have developed a multivariate RAS prediction model based on
previously identified variables;
we followed the development of a screening protocol based on the
results of the prediction models.
2. A post-hoc analysis of the population enrolled in the first study, in
which:
we stratified the patients included in the registry according to
SYNTAX and Clinical SYNTAX coronary complexity scores;
we analyzed the registry in order to identify the variables correlated
with the two scores;
we evaluated the predictive potential of the two scores for RAS.
3. A literature review of hemorrhagic and ischemic risks, in which:
we have identified the clinical, therapeutic and prognostic features of
patients with acute coronary syndromes and CKD;
we analyzed the guidelines in the latest ESC guides on the
management of these patients;
we identified and evaluated the main "sensitive areas" existing in
these Guidelines;
4
we suggested possible directions in the management of renal patients
with ACS.
Figure 8.1. Main approaches in doctoral research.
5
Figure 8.2. Directions in doctoral research.

6
RENAL ARTERY STENOSIS IN STEMI PATIENTS INCLUDED
IN NATIONAL PRIMARY PERCUTANEOUS
REVASCULARIZATION PROGRAM: PREVALENCE AND
CORRELATIONS
Materials and Methods
In our cohort, prospective, randomized, non-randomized (REN-
ACS) study, 250 consecutive patients with ST segment elevation acute
myocardial infarction were enrolled who were eligible for inclusion in
the National Percutaneous Treatment Program of Acute Myocardial
Infarction.
Of the 250 consecutive patients referred to primary angioplasty,
37 subjects were excluded from the study, with only 213 patients
performing coronary angiography and renal angiography. Subsequently,
a total of 181 people met the full inclusion criteria (32 patients were
excluded for incomplete data reasons).
This study was conducted between October 2014 and March 2015
at the "Prof. Dr. G.I.M. Georgescu "- Iaşi.
The research protocol was registered with NCT02388139 on
ClinicalTrials.gov, the most well-known American institution supported
by the National Library of Medicine (NLM) and the National Institutes
of Health (NIH).
All patients were admitted for percutaneous emergency coronary
intervention (through the National Percutaneous Treatment Program of
Acute Myocardial Infarction) and were treated (medically and
interventionally) in accordance with standard European protocols (1).
Coronary angiography was performed by a major arterial femoral
approach less than 12 hours after the onset of angina pectoris in AMI.
The detailed coronarographic aspect (by segments), the type of implanted
stent, the specific periprocedural complications, the TIMI flow at the end
(Figure 9.2) were noted.
Concomitantly, renal diagnostic angiography was performed in
the same procedure. Independent measurements were made by two
operators based on a predefined scale, measuring the size of the kidneys
(after the records during the procedure).

7
Laboratory blood tests (standard set - blood count, biochemistry,
lipid profile) were recorded and noted in the database.
Based on the clinical examination and the interview defined
previously (2) (adapted to the European CARDS data recording
standards), information was obtained on:
medical history - data relevant to coronary artery disease and
RASc - previous interventions, chronic kidney disease, chronic
heart failure, peripheral arterial disease;
cardiovascular risk factors - age, weight, height, abdominal
perimeter, body mass index, smoking, sedentary disease, diabetes
mellitus, hypertension, dyslipidemia;
Killip-Forrester classification of post-infarct cardiac
insufficiency;
According to the management protocol of patients with AMI,
cardiac ultrasound was performed before angiography (measurement and
recording of the left ventricular ejection fraction) immediately after the
patient's admission to the Coronary Intensive Care Unit.
Twenty-four hours after percutaneous intervention the parameters
derived from electrical bioimpedance and arterial stiffness were
evaluated and recorded.
The Research Ethics Committee of the University of Medicine
and Pharmacy "Gr. T. Popa "University of Iasi approved the study
protocol. This protocol was based on international ethical principles of
scientific research, to which Romania also joined (3). All patients were
invited to sign an informed consent (approved by the Ethics Commission
- Annex 1).
To perform body composition analysis, we used Portable Body
Composition Monitoring (BCM®, Fresenius Medical Care, Germany).
The results were recorded in two minutes on a dedicated card and then
transferred to our REN-ACS database through the Fluid Management
Tool® software.
We used the SphygmoCor® device (AtCor, Australia) to acquire
carotid-femoral and carotid-radial PWV and aortic augmentation index.

8
Figure 9.2. Flow-chart in REN-ACS
Results
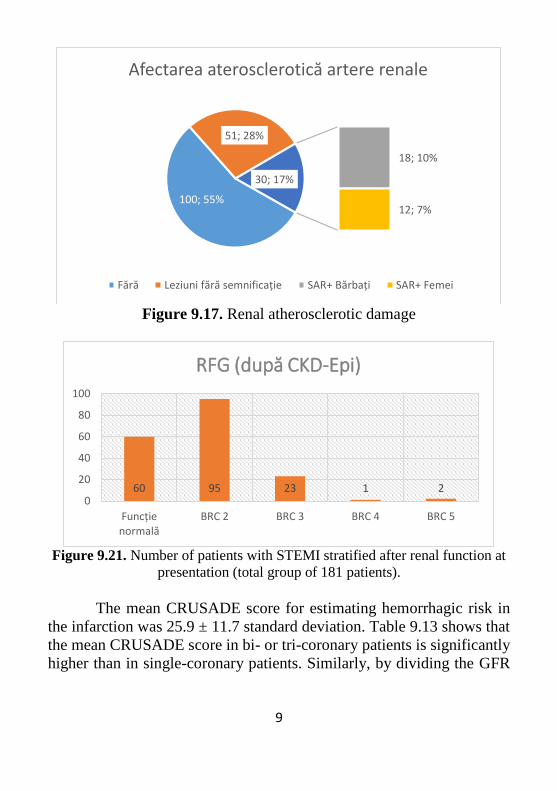
Renal atherosclerotic lesions (both significant and insignificant)
were found in 81 patients (45% of the total): 59 of them had unilateral
determinations (representing 32.6%) and 22 patients showed bilateral
injuries (equivalent to 12.2%) (Figure 9.17). The distribution of patients
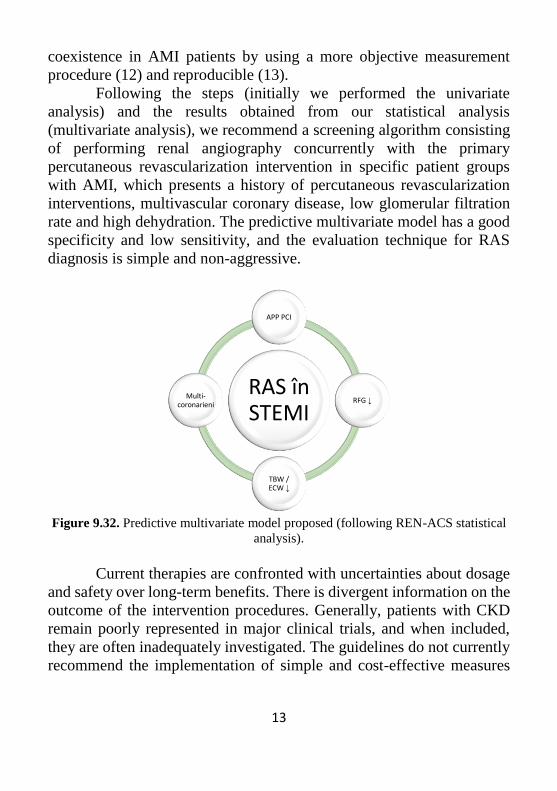
in the batch according to eGFR at admission is shown in Figure 9.21.
9
Figure 9.17. Renal atherosclerotic damage
Figure 9.21. Number of patients with STEMI stratified after renal function at
presentation (total group of 181 patients).
The mean CRUSADE score for estimating hemorrhagic risk in
the infarction was 25.9 ± 11.7 standard deviation. Table 9.13 shows that
the mean CRUSADE score in bi- or tri-coronary patients is significantly
higher than in single-coronary patients. Similarly, by dividing the GFR
100; 55%
51; 28%
18; 10%
12; 7%
30; 17%
Afectarea aterosclerotică artere renale
Fără Leziuni fără semnificație SAR+ Bărbați SAR+ Femei
60 95 23 1 20
20
40
60
80
100
Funcție normală
BRC 2 BRC 3 BRC 4 BRC 5
RFG (după CKD-Epi)

10
on the two subgroups mentioned, there is a strong statistical significance
of decreased renal function in multi-coronaries.
Table 9.13. Distribution of the CRUSADE hemorrhagic risk score depending
on the number of affected coronary arteries.
Total group
(n=181)
Unicoronary
(n=79)
Bi- or tri-
coronary
(n=102)
P value
CRUSADE
score
25,9 ± 11,7 23,8 ± 10,6 27,5 ± 12,2 0,03
eGFR 79,5 ± 20,0 84,8 ± 18,2 75,4 ± 20,5 0,001
Table 9.16 describes PWV-cf and PWV-cr averages based on the
number of coronary arteries involved. It is noted that in the multi-
coronary patients, the carotid-femoral pulse wave velocity is significantly
higher than in the unicoronary patients.
Table 9.16. Pulse wave velocities (carotid-femoral and carotid-radial) in
unicoronarian and multi-coronary patients.
Total group
(n=181)
Unicoronary
(n=79)
Bi- or tri- coronary
(n=102) P
PWV-cf 9,39 ± 2,54 8,94 ± 2,0 9,73 ± 2,8 0,04
PWV-cr 7,00 ± 1,15 7,1 ± 1,1 6,93 ± 1,2 0,41
Results of body composition records by BCM depending on the
presence or absence of CKD (GFR less than 90 mL / min / m2). It is noted
that TBW, ECW and ICW values are significantly lower (dehydration)
in patients with renal dysfunction than those with normal renal function.
RAS + (defined as significant stenosis - over 50% - renal artery)
was identified in 30 patients, representing 16.6% of the study group.
The univariate logistic regression analysis evaluated the
association of each of the variables with the presence of RAS + (Table
9.28).
In multivariate models, variables that remained independently
associated with RAS+ were the antecedents of PCI, GFR, multivascular
BCI, TBW or ECW (Table 9.29 and 9.30).

11
Table 9.28. Univariate RAS+ associations.
Parameters Odds Ratio 95% CI
Sex
(1=Male, 2=Female) 2,294 1,006-5,231
Age, yrs 1,039 1,003-1,078
PCI (0=Nu, 1=Da) 11,462 1,996-65,808
CAD (0=Nu, 1=Da) 2,404 1,008-5,731
GFR 0,971 0,952-0,989
Fibrinogen 1,003 1,000-1,005
No of diseased vessels
(0=1 vas, 1=≥2 vase) 3,374 1,448-9,678
PWV-cf 1,202 1,039-1,391
TBW 0,915 0,861-0,973
ECW 0,822 0,703-0,961
ICW 0,882 0,805-0,966
Table 9.29. Multivariate associations of RAS (model with TBW).
Parameters Odds Ratio 95% CI
PCI (0=Nu, 1=Da) 8,590 1,319-55,928
GFR 0,978 0,958-0,999
Number of diseased vessels
(0 = 1 vas, 1 = ≥2 vase) 3,113 1,127-8,593
TBW 0,933 0,875-0,995
Table 9.30. Multivariate associations of RAS (model with ECW).
Parametri Odds Ratio 95% CI
PCI (0=Nu, 1=Da) 8,097 1,178-55,646
GFR 0,974 0,954-0,995
No of diseased vessels
(0 = 1 vas, 1 = ≥2 vase) 3,143 1,143-8,646
ECW 0,845 0,716-0,997
Both models showed accuracy (84.5%), specificity (98.7%),
sensitivity (13.3%), and identical positive (66.7%) and negative (83.4%)
predictive values.

12
Discussions
In the literature, only a few trials and a single systematic review
(4) discussing the incidence of RAS in stable coronary artery disease,
while there is no study evaluating a cohort of patients with AMI. In fact,
all previous studies excluded this category of patients. The systematic
evaluation of existing literature has identified eight studies in which renal
screening angiography was performed in patients with stable coronary
artery disease in elective settings.
Our results show consistent values for the prevalence of RAS in
AMI (16.6%) than those reported for recognized risk groups (suspicion
of renovascular hypertension (4, 5) - 14.1%, hypertension and diabetes
mellitus (6) – 17,1%, chronic coronary disease (4, 7, 8) – 9,1% to 10,8%).
Our doctoral research is the first published trial evaluating the
arterial stiffness (via PWV) and the hydric status (via BCM) in
consecutive AMI patients.
Our results suggest that increased blood rigidity is associated with
an increased prevalence of RAS in the AMI patients group. We believe
that in-depth research is needed to refine the predictive power of the
interactive relationship between increased arterial stiffness and the RAS
+ phenotype.
One of the strongest predictors of RAS + in our study was the
decline in renal function. Patients in the RAS + trial group had a
significantly lower glomerular filtration rate than those in the RAS-
group, reflecting a more severe and wider coronary disease(9) (9),
correlating with a higher risk of major cardiac events even after an AMI
(10). The decrease in glomerular filtration rate may be due to the
development of RAS, namely chronic ischemic nephropathy following
atheromatous stenosis and / or the coexistence of multiple risk factors.
Furthermore, the CRUSADE score was significantly higher in the
RAS + study group. This means that patients with STEMI and RAS +
have a significantly higher risk of bleeding than patients without RAS.
thus leading to even greater risk of major cardiac events (11).
The present PhD research is the first to suggest the importance of
bioimpedance and water status assessment in conjunction with RAS
13
coexistence in AMI patients by using a more objective measurement
procedure (12) and reproducible (13).
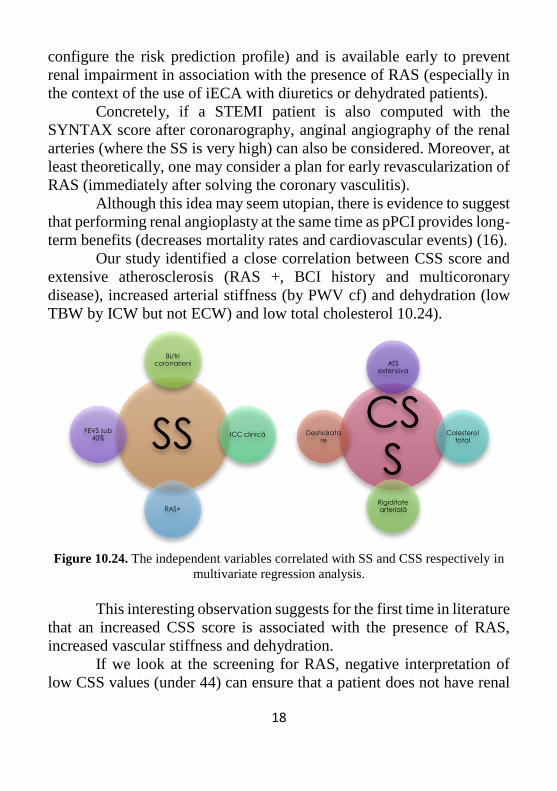
Following the steps (initially we performed the univariate
analysis) and the results obtained from our statistical analysis
(multivariate analysis), we recommend a screening algorithm consisting
of performing renal angiography concurrently with the primary
percutaneous revascularization intervention in specific patient groups
with AMI, which presents a history of percutaneous revascularization
interventions, multivascular coronary disease, low glomerular filtration
rate and high dehydration. The predictive multivariate model has a good
specificity and low sensitivity, and the evaluation technique for RAS
diagnosis is simple and non-aggressive.
Figure 9.32. Predictive multivariate model proposed (following REN-ACS statistical
analysis).
Current therapies are confronted with uncertainties about dosage
and safety over long-term benefits. There is divergent information on the
outcome of the intervention procedures. Generally, patients with CKD
remain poorly represented in major clinical trials, and when included,
they are often inadequately investigated. The guidelines do not currently
recommend the implementation of simple and cost-effective measures
RAS în STEMI
APP PCI
RFG ↓
TBW / ECW ↓
Multi-coronarieni

14
that could be protective measures for these patients, such as creatinine
clearance clearance or eGFR recommendations.
We believe that the lack of clinical trials must not discourage the
common sense of clinical practice, and that clearer decision-making
algorithms with better ends are feasible and necessary. Furthermore, in
our opinion urgent randomized robust studies are urgently needed to
explore and cover the large gaps in the information framework covering
this patient population. They also require specific assessment procedures,
and we believe that it is imperative to design a strategy with specific
measures translated by effectively reducing the incidence of
haemorrhages.
SYNTAX AND CLINICAL SYNTAX SCORES IN ACUTE
MIOCARDIAL INFARCTION PATIENTS WITH PRIMARY PCI:
CORRELATIONS AND PREDICTION OF RENAL ARTERY
STENOSIS
Materials and Methods
The research group of this post-hoc registry analysis is part of the
previous REN-ACS study.
The SYNTAX score (SS) is a tool for calculating the severity of
coronary atherosclerotic disease. It's based on a complex computational
algorithm that uses 11 elements of severity (14). Currently, the
calculation is done online at www.syntaxscore.com. If the initial score
was developed for patients with left coronary artery lesion or severe
tricoronary lesions to guide the revascularization method (between
percutaneous coronary angioplasty and aortic coronary bypass surgery),
further studies have shown that it can be used as a predictor of major
cardiovascular events and in the acute context (acute coronary
syndromes) or in patients with single or bi-coronary lesions.
The SYNTAX Clinical Score was calculated retrospectively for
each patient in the REN-ACS after the SS calculation (described in
CHAPTER 10.2.3). The formula used was CSS = [SS] × [modified
ACEF score] (15).
Results

15
The calculations behind the current analysis were based on SS
and CSS assessments. Thus, SYNTAX scores varied between 1 and 46.5
with a mean ± standard offset of 16.95 ± 8.45 and a median of 17.5.
Clinical SYNTAX scores were in the range of 1.22 and 255.15 with a
mean ± standard offset of 39.3 ± 41.3 and a median of 28.
The study group was divided by SS into tertiles as follows: tertile
1 SS ≤ 11 (n = 59). Tertile 2 SS 11.1 = 19.9 (n = 61 patients), tertile 3 SS
≥ 20 (n = 61). After the descriptive and correlative analysis of SS, the
patient group was divided by tertiles CSS: tertile 1 CSS ≤ 19.2 (n = 60
patients), tertile 2 CSS 19.3 - 38.8 (n = 61 patients) and tertile 3 CSS ≥
38.9 (n = 60 patients).
The results of coronary angiography and renal angiography are
shown in Table 10.11. Both multi-coronary patients and those with RAS
+ are significantly more numerous in the upper tertile of the SS.
Table 10.11. Results of coronary angiography and renal angiography after the SS.
Variabile
Tertile 1
SS ≤ 11
(n = 59)
Tertile 2
SS 11,1–
19,9 (n =
61)
Tertile 3
SS ≥ 20
(n = 61)
p1
(I–II)
p2
(II-
III)
p3
(I-III)
Bi- or tri-
coronary, n (%)
15 (25,4) 40 (65,5) 47 (77) 0,001 0,16 0,001
RAS+, n (%) 5 (8,5) 8 (13,1) 17 (27,8) 0,41 0,043 0,006
The stratification of renal angiography results after CSS (Figure
10.22) showed that the prevalence of RAS + was higher in the upper
third.
The SS-related independent variables were: FEVS <40%, RAS +,
ICC history and multivascular BCI (Table 10.20).

16
Figure 10.22. RAS by CSS tertiles (p 1 = 0.77, p 2 = 0.003 and p 3 = 0.001).
Similarly, CSS-related independent variables in the multivariate
linear regression analysis were: RAS +, PWV-cf, BCI history,
multivascular CAD, total serum cholesterol and TBW (by ICW, but not
ECW) (Table 10.21).
Table 10.20. Independent variables associated with SS in multivariate analysis.
Variable B value CI 95% P Value
RAS+ 3,31 0,40 – 6,23 0,026
CHD 3,53 0,80 – 6,27 0,012
LVEF lower 40% 3,33 1,2 – 5,46 0,002
Multivessel 6,21 3,99 – 8,42 0,001
Table 10.21. Independent variables associated with CSS in multivariate analysis.
Variable B value CI 95% P value
RAS+ 26,46 12,43 – 40,48 0,001
CAD 17,69 6,48 – 28,9 0,002
Multivessel 16,75 6,45 – 27,04 0,002
PWV – cf 3,18 1,14 – 5,21 0,002
TBW -0,81 -1,46 – -0,153 0,016
Total colesterol -0,12 -0,22 – -0,018 0,022
5 619
0%
20%
40%
60%
80%
100%
Terțila I a CSS Terțila II a CSS Terțila III a CSS
Stenoza de arteră renală
SAR+ Fără SAR

17
We performed the ROC curves (and AUC for each) for both SS
and CSS. The objective was to evaluate the predictive accuracy of the
two RAS + scores. Both curves are shown in Figure 10.23. The area
under the curve for SS was 0.69 (CI 95% 0.58 - 0.79) and for CSS was
0.74 (CI 95% 0.63 - 0.84) (p <0, 05 for both analyzes, DeLong method).
Figura 10.23. Comparația între AUC pentru ROC SS și CSS.
Discussions
Our approach is the first investigation to calculate and compare
SS and CSS in consecutive STEMI patients for pPCI. Moreover, the two
scores were first evaluated as RAS + predictors (at least until now, the
scores were only used for the assessment of cardiovascular prognosis).
Another novelty of the present study is that PWV and post-procedural
body bioimpedance (BCM) parameters are now analyzed in correlation
with the two SS and CSS scores.
Thus, we can clearly state that patients with RAS + have an
increased SYNTAX score, or in other words, a high SS score correlates
with multi-site atherosclerosis. This information is extremely useful (to
18
configure the risk prediction profile) and is available early to prevent
renal impairment in association with the presence of RAS (especially in
the context of the use of iECA with diuretics or dehydrated patients).
Concretely, if a STEMI patient is also computed with the
SYNTAX score after coronarography, anginal angiography of the renal
arteries (where the SS is very high) can also be considered. Moreover, at
least theoretically, one may consider a plan for early revascularization of
RAS (immediately after solving the coronary vasculitis).
Although this idea may seem utopian, there is evidence to suggest
that performing renal angioplasty at the same time as pPCI provides long-
term benefits (decreases mortality rates and cardiovascular events) (16).
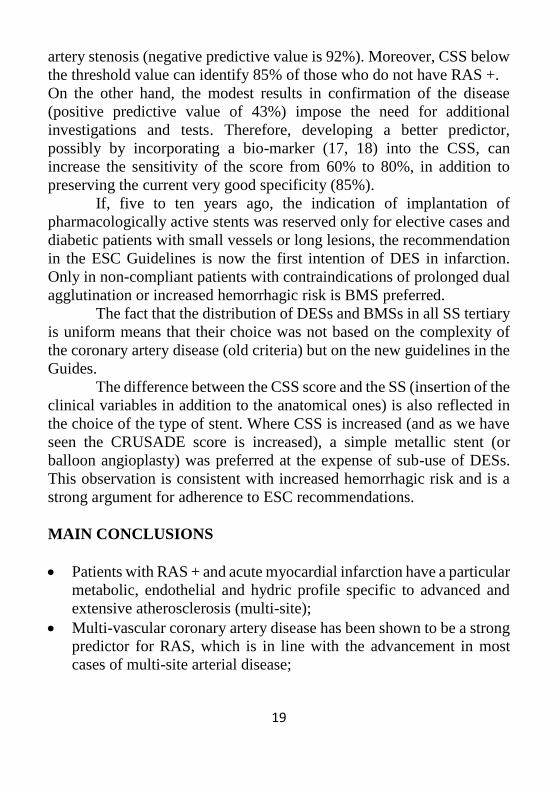
Our study identified a close correlation between CSS score and
extensive atherosclerosis (RAS +, BCI history and multicoronary
disease), increased arterial stiffness (by PWV cf) and dehydration (low
TBW by ICW but not ECW) and low total cholesterol 10.24).
Figure 10.24. The independent variables correlated with SS and CSS respectively in
multivariate regression analysis.
This interesting observation suggests for the first time in literature
that an increased CSS score is associated with the presence of RAS,
increased vascular stiffness and dehydration.
If we look at the screening for RAS, negative interpretation of
low CSS values (under 44) can ensure that a patient does not have renal
SS
Bi/tri coronarieni
ICC clinică
RAS+
FEVS sub 40%
CSS
ATS extensiva
Colesterol total
Rigiditate arterială
Deshidratare
19
artery stenosis (negative predictive value is 92%). Moreover, CSS below
the threshold value can identify 85% of those who do not have RAS +.
On the other hand, the modest results in confirmation of the disease
(positive predictive value of 43%) impose the need for additional
investigations and tests. Therefore, developing a better predictor,
possibly by incorporating a bio-marker (17, 18) into the CSS, can
increase the sensitivity of the score from 60% to 80%, in addition to
preserving the current very good specificity (85%).
If, five to ten years ago, the indication of implantation of
pharmacologically active stents was reserved only for elective cases and
diabetic patients with small vessels or long lesions, the recommendation
in the ESC Guidelines is now the first intention of DES in infarction.
Only in non-compliant patients with contraindications of prolonged dual
agglutination or increased hemorrhagic risk is BMS preferred.
The fact that the distribution of DESs and BMSs in all SS tertiary
is uniform means that their choice was not based on the complexity of
the coronary artery disease (old criteria) but on the new guidelines in the
Guides.
The difference between the CSS score and the SS (insertion of the
clinical variables in addition to the anatomical ones) is also reflected in
the choice of the type of stent. Where CSS is increased (and as we have
seen the CRUSADE score is increased), a simple metallic stent (or
balloon angioplasty) was preferred at the expense of sub-use of DESs.
This observation is consistent with increased hemorrhagic risk and is a
strong argument for adherence to ESC recommendations.
MAIN CONCLUSIONS
Patients with RAS + and acute myocardial infarction have a particular
metabolic, endothelial and hydric profile specific to advanced and
extensive atherosclerosis (multi-site);
Multi-vascular coronary artery disease has been shown to be a strong
predictor for RAS, which is in line with the advancement in most
cases of multi-site arterial disease;
20
For the same reasons, vascular stiffness is more pronounced in
patients with RAS +;
All patients with STEMI were relatively dehydrated (mild subclinical
dehydration), which can be interpreted either as a consequence of the
particular hormonal and metabolic environment in AMI context or as
an independent and unknown risk factor;
Moreover, patients with RAS + and STEMI were significantly
dehydrated than those without RAS, dehydration may have origins
associated with RAS + induced renal dysfunction;
A low GFR in STEMI correlates with the presence of RAS +;
The predictive model of RAS + (which includes the history of PCI,
low GFR, multi-coronary damage and dehydration) has a very good
accuracy and specificity and can be integrated into screening
algorithms;
SYNTAX and Clinical SYNTAX Coronary Complexity scores can
also be used as a predictor of RAS (not only for prognostic
assessment);
Patients with STEMI and CKD have an increased risk of major
bleeding;
Current treatment algorithms include unclear dosages and safety over
long-term benefits. There is divergent information on the outcome of
the intervention procedures (it seems that patients with advanced
CKD have low benefits from PCI in terms of mortality and
complications);
Patients with CKD remain poorly represented in major clinical trials,
and when included, they are often inadequately investigated. The
guidelines do not currently recommend the implementation of simple
and cost-effective measures that could be protective measures for
these patients, such as, for example, obtaining emergency GFR (early
blood tests and updated calculation formulas that would allows early
adjustment of medication and early stratification of ischemic and
haemorrhagic risks);
21
SELECTIVE BIBLIOGRAPHY
1. Steg PG, James SK, Atar D, Badano LP, Blomstrom-Lundqvist C,
Borger MA, et al. ESC Guidelines for the management of acute myocardial
infarction in patients presenting with ST-segment elevation. Eur Heart J 2012;
33:2569-2619.
2. Flynn MR, Barrett C, Cosio FG, Gitt AK, Wallentin L, Kearney P, et
al. The Cardiology Audit and Registration Data Standards (CARDS), European
data standards for clinical cardiology practice. Eur Heart J 2005; 26:308-313.
3. World Medical Association Declaration of Helsinki: ethical principles
for medical research involving human subjects. Jama 2013; 310:2191-2194.
4. de Mast Q, Beutler JJ. The prevalence of atherosclerotic renal artery
stenosis in risk groups: a systematic literature review. Journal of Hypertension
2009; 27:1333-1340.
5. Vasbinder GB, Nelemans PJ, Kessels AG, Kroon AA, Maki JH, Leiner
T, et al. Accuracy of computed tomographic angiography and magnetic
resonance angiography for diagnosing renal artery stenosis. Ann Intern Med
2004; 141:674-682; discussion 682.
6. Valabhji J, Robinson S, Poulter C, Robinson AC, Kong C, Henzen C,
et al. Prevalence of renal artery stenosis in subjects with type 2 diabetes and
coexistent hypertension. Diabetes Care 2000; 23:539-543.
7. Park S, Jung JH, Seo HS, Ko YG, Choi D, Jang Y, et al. The prevalence
and clinical predictors of atherosclerotic renal artery stenosis in patients
undergoing coronary angiography. Heart Vessels 2004; 19:275-279.
8. Conlon PJ, Little MA, Pieper K, Mark DB. Severity of renal vascular
disease predicts mortality in patients undergoing coronary angiography. Kidney
Int 2001; 60:1490-1497.
9. Kim IY, Hwang IH, Lee KN, Lee DW, Lee SB, Shin MJ, et al.
Decreased renal function is an independent predictor of severity of coronary
artery disease: an application of Gensini score. J Korean Med Sci 2013;
28:1615-1621.
10. Fischer MJ, Ho PM, McDermott K, Lowy E, Parikh CR. Chronic
kidney disease is associated with adverse outcomes among elderly patients
taking clopidogrel after hospitalization for acute coronary syndrome. BMC
Nephrol 2013; 14:107.
11. Abu-Assi E, Raposeiras-Roubin S, Garcia-Acuna JM, Gonzalez-
Juanatey JR. Bleeding risk stratification in an era of aggressive management of
acute coronary syndromes. World J Cardiol 2014; 6:1140-1148.

22
12. Machek P, Jirka T, Moissl U, Chamney P, Wabel P. Guided
optimization of fluid status in haemodialysis patients. Nephrol Dial Transplant
2010; 25:538-544.
13. Kyle UG, Bosaeus I, De Lorenzo AD, Deurenberg P, Elia M, Gomez
JM, et al. Bioelectrical impedance analysis--part I: review of principles and
methods. Clin Nutr 2004; 23:1226-1243.
14. Sianos G, Morel MA, Kappetein AP, Morice MC, Colombo A,
Dawkins K, et al. The SYNTAX Score: an angiographic tool grading the
complexity of coronary artery disease. EuroIntervention 2005; 1:219-227.
15. Garg S, RASno G, Garcia-Garcia HM, Girasis C, Wykrzykowska J,
Dawkins KD, et al. A new tool for the risk stratification of patients with
complex coronary artery disease: the Clinical SYNTAX Score. Circ Cardiovasc
Interv 2010; 3:317-326.
16. Su CS, Liu TJ, Tsau CR, Liang KW, Chang WC, Ting CT, et al. The
feasibility, safety, and mid-term outcomes of concomitant percutaneous
transluminal renal artery stenting in acute coronary syndrome patients at high
clinical risk of renal artery stenosis. J Invasive Cardiol 2013; 25:212-217.
17. Gluba-Brzozka A, Michalska-Kasiczak M, Franczyk B, Nocun M, Toth
P, Banach M, et al. Markers of increased atherosclerotic risk in patients with
chronic kidney disease: a preliminary study. Lipids Health Dis 2016; 15:22.
18. American Diabetes Association Clinical Practice Recommendations
2001. Diabetes Care 2001; 24 Suppl 1:S1-133.





![Characteristics of coronary artery calcium and its ... · oronary artery calcium (CAC) is a specic marker of coronary atherosclerosis [1], its extent reects the burden of atherosclerotic](https://static.fdocuments.net/doc/165x107/5fc3069a0498e3155071621f/characteristics-of-coronary-artery-calcium-and-its-oronary-artery-calcium-cac.jpg)