The quandary of autoimmune pancreatitis and pancreatic ductal … · 2018. 12. 7. · The quandary...
9
www.ijhpd.com The quandary of autoimmune pancreatitis and pancreatic ductal adenocarcinoma: A case report and review of IgG4 immunostaining in a cohort of patients receiving neoadjuvant chemotherapy Ornela Dervishaj, Harish Lavu, Charles J Yeo, Agnieszka K Witkiewicz ABSTRACT Introduction: Autoimmune pancreatitis (AIP) is an inflammatory disease whose clinical presentation can mimic that of pancreatic ductal adenocarcinoma (PDA). AIP can appear on imaging as a bulky, sausagelike pancreatic mass with biliary and pancreatic ductal obstruction, resembling the classic “double duct sign” appearance of PDA. A definitive preoperative diagnosis of AIP can be difficult because the two diseases (AIP and PDA) are similar in clinical presentation. Recent advances in serum marker evaluation such as IgG4 serum levels and immunostaining techniques have shown some promise in the differentiation of AIP from PDA. Case Report: We report the case of a patient with a preoperative diagnosis of locally advanced PDA who was treated with neoadjuvant gemcitabine based chemotherapy followed by surgical resection, but whose post resection pathology was indicative of AIP and not PDA. To explore the possibility that the pre resection gemcitabinebased chemotherapy had generated a complete pathological response and an inflammatory reaction of IgG4positive plasma cells, we studied the histology features and IgG4 plasma cell immunostaining characteristics of the pathology specimens of 14 patients with a diagnosis of PDA who were treated with neoadjuvant chemotherapy and surgical resection at our institution. Conclusion: Our results indicate that none of the patients treated with neoadjuvant chemotherapy had increased IgG4positive plasma cell immunostaining post operatively, further supporting the diagnosis of AIP and not PDA in our patient. Keywords: Autoimmune pancreatitis, Pancreatic tumor, Adenocarcinoma ********* Dervishaj O, Lavu H, Yeo CJ, Witkiewiez AK. The quandary of autoimmune pancreatitis and pancreatic ductal adenocarcinoma: A case report and review of IgG4 immunostaining in a cohort of patients receiving neoadjuvant chemotherapy. International Journal of Hepatobiliary and Pancreatic Diseases 2013;3:1–9. Article ID: 100010IJHPDOD2013 ********* doi:10.5348/ijhpd201310CR1 INTRODUCTION Autoimmune pancreatitis (AIP) is a rare form of chronic pancreatitis characterized by a lymphoplasmacytic infiltrate rich in IgG4positive plasma cells. It was formally recognized in 1995 when Yoshida et al. published a case report of a patient with pancreatitis and the presence of hyperglobulinemia [1]. However, reports of autoimmune pancreatitis may date to as early as the 1960’s, when Sarles et al. described a group of patients suffering from “primary inflammatory pancreatitis or primary noncalcifying pancreatitis with
Transcript of The quandary of autoimmune pancreatitis and pancreatic ductal … · 2018. 12. 7. · The quandary...

IJHPD – International Journal of Hepatobil iary and Pancreatic Diseases, Vol. 3 , 201 3. ISSN – [2230–901 2]
IJHPD 201 3;3:1 –9.www.ijhpd.com
The quandary of autoimmune pancreatitis and pancreaticductal adenocarcinoma: A case report and review of IgG4immunostaining in a cohort of patients receivingneoadjuvant chemotherapyOrnela Dervishaj, Harish Lavu, Charles J Yeo, Agnieszka K Witkiewicz
ABSTRACTIntroduction: Autoimmune pancreatitis (AIP) isan inflammatory disease whose clinicalpresentation can mimic that of pancreatic ductaladenocarcinoma (PDA). AIP can appear onimaging as a bulky, sausagelike pancreatic masswith biliary and pancreatic ductal obstruction,resembling the classic “double duct sign”appearance of PDA. A definitive preoperativediagnosis of AIP can be difficult because the twodiseases (AIP and PDA) are similar in clinicalpresentation. Recent advances in serum markerevaluation such as IgG4 serum levels andimmunostaining techniques have shown somepromise in the differentiation of AIP from PDA.Case Report: We report the case of a patientwith a preoperative diagnosis of locallyadvanced PDA who was treated withneoadjuvant gemcitabine based chemotherapyfollowed by surgical resection, but whose postresection pathology was indicative of AIP andnot PDA. To explore the possibility that the preresection gemcitabinebased chemotherapy hadgenerated a complete pathological response andan inflammatory reaction of IgG4positiveplasma cells, we studied the histology featuresand IgG4 plasma cell immunostaining
characteristics of the pathology specimens of 14patients with a diagnosis of PDA who were treatedwith neoadjuvant chemotherapy and surgicalresection at our institution. Conclusion: Ourresults indicate that none of the patients treatedwith neoadjuvant chemotherapy had increasedIgG4positive plasma cell immunostaining postoperatively, further supporting the diagnosis ofAIP and not PDA in our patient.Keywords: Autoimmune pancreatitis,Pancreatic tumor, Adenocarcinoma
*********Dervishaj O, Lavu H, Yeo CJ, Witkiewiez AK. Thequandary of autoimmune pancreatitis and pancreaticductal adenocarcinoma: A case report and review ofIgG4 immunostaining in a cohort of patients receivingneoadjuvant chemotherapy. International Journal ofHepatobiliary and Pancreatic Diseases 2013;3:1–9.Article ID: 100010IJHPDOD2013
*********doi:10.5348/ijhpd201310CR1
INTRODUCTIONAutoimmune pancreatitis (AIP) is a rare form ofchronic pancreatitis characterized by alymphoplasmacytic infiltrate rich in IgG4positiveplasma cells. It was formally recognized in 1995 whenYoshida et al. published a case report of a patient withpancreatitis and the presence of hyperglobulinemia [1].However, reports of autoimmune pancreatitis may dateto as early as the 1960’s, when Sarles et al. described agroup of patients suffering from “primary inflammatorypancreatitis or primary noncalcifying pancreatitis with
CASE REPORT OPEN ACCESS
Ornela Dervishaj1 , Harish Lavu1 , Charles J Yeo1 ,Agnieszka K Witkiewicz2
Affi l iations: 1Department of Surgery, Thomas JeffersonUniversity, Jefferson Pancreas, Bil iary & Related CancerCenter, Philadelphia PA, USA; 2Department of Pathology,Thomas Jefferson University, Philadelphia, PA, USA.Corresponding Author: Agnieszka K Witkiewicz, MD, 1 32S. 1 0th Street Suite 285 D Philadelphia, PA 1 91 07, USA;Ph: (21 5) 955-3778; Fax: (21 5) 955-5058; Email :[email protected]
Received: 23 March 201 2Accepted: 29 March 201 2Published: 05 January 201 3
Dervishaj et al. 1

IJHPD – International Journal of Hepatobil iary and Pancreatic Diseases, Vol. 3 , 201 3. ISSN – [2230–901 2]
IJHPD 201 3;3:1 –9.www.ijhpd.com Dervishaj et al. 2
hypergammaglobulinemia” [1–3]. Other terms used todescribe autoimmune pancreatitis in the past haveincluded “lymphoplasmacytic sclerosing pancreatitis”[4], “nonalcoholic ductdestructive chronicpancreatitis” [2] and “chronic sclerosing pancreatitis”[5]. Autoimmune pancreatitis may be part of theautoimmune systemic disorder described as IgG4related disease as it is often associated with a IgG4positive plasma cell infiltrate in the biliary tree, lungs,lymph nodes, salivary glands and kidneys. UntreatedIgG4related disease often progresses fromlymphoplasmacytic inflammation to extensive fibrosis.Glucocorticoids are generally the first line of treatmentregardless of the organ involved [8, 39].The typical clinical presentation of AIP i.e. painlessjaundice with weight loss, often mimics that ofpancreatic ductal adenocarcinoma (PDA) and there canbe difficulty in distinguishing between the two diseases.In North America, nearly 2.5% ofpancreaticoduodenectomies have been performed forcases of AIP that were presumed to be PDA [6]. Due tothe difficulty in obtaining a definitive preoperativehistologic diagnosis, it is not uncommon in the clinicalsetting to have cases of PDA that are not confirmeduntil after surgical resection and postoperativepathologic examination of the resected specimen. Giventhe similarity in clinical presentation between AIP andPDA, a number of published studies have offeredcriteria to allow for a more accurate differentiationbetween the two diseases [6, 9] (Table 1). While some ofthese criteria have sensitivity as high as 97% [7], a basictenet for the workup of these patients calls for theexclusion of malignancy before the diagnosis of AIP canbe made. IgG4positive plasma cell immunostaining hasshown some promise in distinguishing between AIP andPDA, although interpretation of IgG4positive plasmacell immunostaining on preoperative fine needle or coreneedle biopsies can be challenging.In this paper, we report the case of a patient whounderwent neoadjuvant gemcitabine basedchemotherapy for suspected locally advanced PDA.After what was assumed to be a favorable clinicalresponse to preoperative treatment, the patientunderwent surgical resection viapancreaticoduodenectomy. However, pathologicevaluation of the resected specimen showed featuresmore consistent with AIP rather than PDA. In this studywe review the important facts related to this case anddescribe the findings of a retrospective analysis of thepathologic specimens of fourteen other patients whounderwent neoadjuvant chemotherapy and surgicalresection at our institution. We immunostained thetissues of these fourteen neoadjuvant patients with amarker for AIP, the IgG4 antibody. To our knowledgethis is the first such report in the English literature.
CASE REPORTThe patient was a 62yearold AfricanAmericanwoman of blood type O Rh+, with a past medical history
significant for diabetes, who presented to her primarycare physician with abdominal pain and about 12 kgweight loss. The patient had also been experiencingsymptoms of belching and acid reflux for one year andhad recently developed dark urine and pale stools. Atpresentation her total and direct bilirubin levels were10.6 mg/dl and 5 mg/dl, respectively. She was a nonsmoker, social drinker and denied illicit drug use. Herfamily history was significant for sarcoidosis in a sisterand systemic lupus erythematosus in her daughter andanother sister. There was no family history of pancreaticor other malignancy.A computerized tomography (CT) scan revealed afour centimeter pancreatic head mass with intrahepaticand extrahepatic biliary and pancreatic duct dilatation,as well as encasement of the superior mesenteric vein(SMV) (Figure 1). The CA199 (21 U/ml) and CEA (1.6ng/ml) levels were within normal limits. Endoscopicretrograde cholangiopancreatography (ERCP) was doneand showed a stricture within the distal common bileduct (CBD) with marked proximal biliary ductaldilatation. The bile duct brushings performed at thetime were negative for neoplastic cells and a metalbiliary endoprosthesis was placed within the CBD. Thepatient then underwent an endoscopic ultrasound(EUS) which demonstrated the mass in the head ofpancreas measuring 3.8x3 cm invading the splenoportalconfluence, SMV and partially encasing the hepaticartery. Enlarged hypoechoic lymph nodes adjacent tothe pancreas were also noted. A fine needle aspiration ofthe mass was nondiagnostic and revealed a few atypicalcells in a background of benign glandular cells,inflammatory cells and debris. A subsequent positronemission tomography (PET) scan showed ahypermetabolic mass in the head of the pancreas withan SUV of 7.14 and no metabolically activelymphadenopathy. The patient underwent a repeatEUSFNA in an attempt to obtain a definitive tissuediagnosis, but this also revealed benign glandular andinflammatory cells with debris.Despite failure to obtain a confirmatory pathologicdiagnosis, given the clinical picture, the patient wasgiven the presumptive diagnosis of PDA. The mass wasinitially deemed unresectable due to vascularencasement and the patient was referred forneoadjuvant chemotherapy with gemcitabine at a doseof 1000 mg/m2. She tolerated the neoadjuvanttreatment well, except for early myelosuppression thatrequired a dose reduction of gemcitabine after hersecond infusion. The patient completed three cycles oftreatment, with a total of nine infusions. Postchemotherapy restaging CT scan (Figure 2) showed areduction in the size of the pancreatic mass and foundthe SMV and portal vein to be free of tumorencasement. However, there still remained an area ofabnormality within the uncinate process of thepancreas. At this point, the mass was judged amenableto surgical resection and the patient underwent apyloruspreserving pancreaticoduodenectomy. Thepatient tolerated the surgery well and had an uneventfulpostoperative course on our clinical pathway [37]. She

IJHPD – International Journal of Hepatobil iary and Pancreatic Diseases, Vol. 3 , 201 3. ISSN – [2230–901 2]
IJHPD 201 3;3:1 –9.www.ijhpd.com Dervishaj et al. 3
was discharged to home six days after surgery. At eightmonths post surgery, the patient was symptom anddisease free with no signs of recurrent AIP and norequirement for steroid treatment.On pathologic examination of the patient’s resectedpancreas specimen no PDA was identified. However,there was a marked ductocentric lymphoplasmocyticinfiltrate consistent with AIP. Plasma cells present in
the inflammatory infiltrate had expression of CD138(plasma cell marker) and 90% of them were IgG4positive (43 IgG4positive plasma cells/HPF). Venulitiswas present and granulocytic epithelial lesions wereabsent. The entire pancreas specimen was submitted formicroscopic evaluation and there was no tumor presentand no evidence of metastasis in the 15 harvested lymphnodes (figure 3).
Table 1: Current Criteria for the diagnosis of AIP.
MPD Main pancreatic duct; US Ultrasonography; CT Computed tomography, MRI Magnetic resonance imaging, ERCP Endoscopic retrograde cholangiopancreatography, MRCP Magnetic resonance cholangiopancreatography, HPF High powerfield, ANA Antinen trophil antibody, RF Rheumatoid factorNUD Criteria/parameter not used for diagnosis

IJHPD – International Journal of Hepatobil iary and Pancreatic Diseases, Vol. 3 , 201 3. ISSN – [2230–901 2]
IJHPD 201 3;3:1 –9.www.ijhpd.com Dervishaj et al. 4
To study the possibility that neoadjuvantchemotherapy elicited a complete tumor response witha IgG4positive plasma cell infiltrate, weimmunostained with IgG4 antibody fourteen other casesof PDA that were treated preoperatively with eithergemcitabine alone or another chemotherapeutic agentand were surgically resected at our institution. Informedpatient consent was obtained preoperatively via an IRBapproved protocol for the use of resected tissues forscholarly activity. The clinicopathologic characteristicsof each case and the results of IgG4 staining are shownin Table 2. The age range for the PDA patients treatedwith neoadjuvant chemotherapy was 49–69 years with amedian age of 57 years. All patients except one weretreated with gemcitabine based neoadjuvantchemotherapy and ten patients were also treated withradiation preoperatively. All patients had proven PDAon pathology after surgery, and no patient had acomplete pathologic response. None of the patients hadhistologic features of AIP or a high number of IgG4positive plasma cells on analysis of their resectionspecimens (figure 4).
DISCUSSIONWe present the case of a patient who had apresumptive diagnosis of locally advanced pancreaticductal adenocarcinoma (PDA) and received neoadjuvantgemcitabine based chemotherapy and subsequentsurgical resection. However, postoperative pathologicexamination of the pancreas revealed evidence ofautoimmune pancreatitis (AIP) and no sign of PDA. AIPand PDA can be difficult to distinguish clinically. Theaverage age of AIP patients is 68 years with a rangenoted in the literature between 51–87 years, whichcoincides with the typical age range for PDA [6, 9, 12,13]. The symptom cluster of AIP coincides with that ofPDA, including obstructive jaundice, abdominal painand elevated liver enzymes [9, 12, 15]. More than 50%AIP patients present with weight loss [9, 12] and somemay also report new onset diabetes or worseningglycemic control, all of which are also common findingsin patients with PDA [12]. Despite the similarities inpresentation between these two diseases, it is essentialto differentiate between them in order to devise aproper treatment strategy.Although the pathogenesis of AIP is still uncertain,our understanding of this disease entity has increased inthe recent years. Two forms of AIP are recognized: type1 and type 2. Type 1 AIP is histologically characterizedby lymphoplasmacytic inflammation in a storiformpattern around medium sized and large pancreatic ductsand is associated with acinar atrophy, obliterativevenulitis and a mildtomoderate eosinophil infiltrate[2, 4, 5, 8, 15]. The periductal nature of theinflammatory infiltrate is particularly distinctive andhelps separate AIP from other types of pancreatitis. Thisform of AIP is more likely to be systemic and ischaracterized by IgG4positive plasma cell infiltrates
and elevated serum levels of IgG4. Associated systemicor extrapancreatic manifestations of type 1 AIP caninclude lymphoplasmacytic sclerosing cholecystitis, aswell as lymphoplasmacytic infiltrates in the lungs,salivary glands and kidneys [2, 4, 8]. The inflammatorylesion frequently forms a tumefactive mass that maydestroy the involved organ [8]. Interestingly, all of theextrapancreatic lesions in patients with type 1 AIP willshow an infiltration of abundant IgG4positive plasmacells, but such an infiltration is not detected in patientswith PDA [16]. Based upon this observation someauthors have recommended IgG4immunostaining ofextrapancreatic lesions (salivary glands, gallbladderetc.) in addition to Japanese criteria to diagnose AIP [6](Table 1).
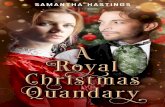
Figure 1: Preneoadjuvant chemotherapy abdominal CT scandemonstrating tumor mass (m). The superior mesenteric vein(SMV, black arrow) appears to be completely encased by thetumor at this crosssectional level.
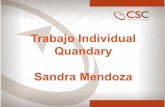
Figure 2: Postneoadjuvant chemotherapy CT scan illustratingmarked decrease in pancreatic mass. The metallic biliaryendoprosthesis is seen (white arrowhead) and the Superiormesenteric vein (SMV, black arrow) is no longer encased bytumor.

IJHPD – International Journal of Hepatobil iary and Pancreatic Diseases, Vol. 3 , 201 3. ISSN – [2230–901 2]
IJHPD 201 3;3:1 –9.www.ijhpd.com Dervishaj et al. 5
Type 2 AIP differs from type 1 in that it is notassociated with infiltrates of IgG4positive plasma cellsin the pancreas or other organs nor increased serumlevels of IgG4. Histopathologically, type 2 AIP ischaracterized by granulocytic epithelial lesions inassociation with destruction and obliteration of thepancreatic duct, which are absent in type 1 AIP.Clinically, the disease tends to be confined to thepancreas, though a few studies have linked type 2 AIP toulcerative colitis. It has been suggested that type 2 AIPmay have a higher likelihood of recurrence [16]. AIP issometimes referred to as lymphoplasmacytic sclerosingpancreatitis (LPSP) for type 1 AIP and idiopathic ductcentric pancreatitis (IDCP) for type 2 AIP. Given thatour patient had an IgG4 inflammatory infiltrate with
venulitis and absent granulocytic epithelial lesions, sheappears to be best classified as type 1 AIP.A number of serum diagnostic markers for AIP havebeen studied. Given the inflammatory nature of thedisease, antinuclear antibody (ANA) and rheumatoidfactor (RF) have been examined and found to bepositive in 43% to 75% of AIP patients. Neither of thesepossess adequate sensitivity or specificity to be deemedreliable clinical diagnostic tests [3, 6, 14, 18]. To date,serum IgG4 levels have shown the most promise as adiagnostic marker for AIP with 80% patients havingelevated serum levels (above 140 mg/dL) [6, 18]. Incomparison, PDA patients rarely have elevated values ofserum IgG4. Ghazale et al. found that 10% of PDApatients had serum IgG4 values above 140 mg/dL, ascompared with 76% of AIP patients. If a higher level(greater than 280 mg/dL) of serum IgG4 is used as acutoff only 1% of PDA patients will have values abovethis threshold, compared to 53% AIP patients [7, 18]. Toincrease the diagnostic value of serum IgG4 in AIP,some authors have recommended combining serumIgG4 with ANA and RF. The combined sensitivity ofthese three tests may be as high as 97% [6, 7, 14].On crosssectional imaging, AIP has thecharacteristic appearance of diffuse enlargement of thepancreas with a capsulelike rim and without ductaldilatation or cutoff [17], though Manfredi et al. foundthat on review of CT scan imaging, 67% of their patientswith AIP had focal enlargement of the pancreas while33% patients had diffuse enlargement [21]. A capsulelike rim of contrast enhancement was seen in 46%patients where delayed phase scanning was performedand the main pancreatic duct (MPD) was dilatedupstream in 57% patients with focal enlargement of thepancreas. Recently it has been suggested that a 2weektrial of steroids may help to distinguish AIP from PDAas there can be a dramatic imaging response in cases ofAIP and typically no response in the setting ofmalignancy [16, 39]. AIP patients do not have elevatedvalues of serum tumor marker CA199, which areusually elevated in cases of PDA. A diagnosis of AIP isone of exclusion and can only be concluded when theworkup for malignancy is negative and there is strongclinical evidence for AIP. As a cautionary note, ourgroup recently reported on the case of a patient withsimultaneous AIP and PDA [32], an unusual andproblematic event.Though focal aggregates of IgG4positive plasma cellinfiltrates have been reported in chronic pancreatitisassociated with PDA, the mean number of IgG4positiveplasma cells per high power field (HPF) is much higherin the diffuse infiltrates of AIP (62.1/HPF in AIP versus9.9/HPF in chronic pancreatitis associated with PDA)[15]. Dhall et al. found that in 84% of their AIP casesthere were more than 50 IgG4positive plasmacells/HPF, while there were no PDA cases above thisvalue. These findings have been confirmed by others [2,38] and it was found that when using a cutoff value of50 IgG4positive cells/HPF, the sensitivity of IgG4staining for AIP increases to 84% and the specificity to100% with a significant p value (p < 0.0001).
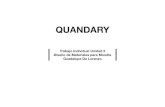
Figure 3: Histology and immunohistochemical stains. A)Lymphoplasmacytic infiltrate centered on a large intralobarduct (H&E, ×50), B) Venulitis (H&E, ×50, arrow), C)Immunohistochemical labeling with an antibody to CD138highlights numerous plasma cells present in the inflammatoryinfiltrate (CD138, ×100), D) Immunohistochemical labelingwith an antibody to IgG4 highlights numerous IgG4positiveplasma cells (IgG4, ×100).
Figure 4: Immunohistochemical staining for IgG4 inpancreatic ductal adenocarcinoma (PDA) cases treated withneoadjuvant chemotherapy. A) Well differentiated PDA and B)Poorly differentiated PDA showing only rare IgG4positiveplasma cells (arrows) (IgG4, x100).

IJHPD – International Journal of Hepatobil iary and Pancreatic Diseases, Vol. 3 , 201 3. ISSN – [2230–901 2]
IJHPD 201 3;3:1 –9.www.ijhpd.com Dervishaj et al. 6
Table 2: PDA patients treated with neoadjuvant chemotherapy, radiation and resection (n=14).
PDA Pancreatic Ductal Adenocarcinoma, SMA Superior Mesenteric Artery, SMV Superior Mesenteric Vein, HPF High PowerField, Radiation Administration of radiation postchemotherapy and preresection

IJHPD – International Journal of Hepatobil iary and Pancreatic Diseases, Vol. 3 , 201 3. ISSN – [2230–901 2]
IJHPD 201 3;3:1 –9.www.ijhpd.com Dervishaj et al. 7
Histopathologic examination of our 14 neoadjuvanttreated PDA patients did not reveal any of the previouslymentioned histologic features of AIP(lymphoplasmacytic inflammation, obliterativevenulitis, or elevated IgG4positive plasma cells). Onlyone of our 14 patients had more than 10 IgG4positiveplasma cells/HPF (Table 2), which is still much lowerthan the typical cutoff value of 50 cells/HPF seen onhistologic examination of AIP patients. Based uponthese results it appears that neoadjuvant chemotherapydoes not result in an AIPlike IgG4positive plasma cellinflammatory reaction within the pancreaticparenchyma.The only curative treatment for PDA involvessurgical resection. Hence, the recommended practice forlocalized disease is surgery followed by adjuvantchemotherapy with or without radiation [28].Neoadjuvant chemotherapy is used to downstagepatients who present with locally advanced unresectabledisease or, in some centers, as an upfront treatment inpatients with operable PDA. Although there are studiesdemonstrating decreased margin positivity and localfailure, as well as increased survival in the subset ofpatients who undergo neoadjuvant therapy followed bysurgical resection for operable PDA, much of theexisting evidence is in the form of singleinstitutionexperience. Although gemcitabine [25] or gemcitabinebased combination chemotherapy [26–27] is consideredthe standard of care, only 30% of patients treated in theneoadjuvant setting will exhibit conversion to resectabledisease [19, 20], and to date no pathologic completeresponses to gemcitabine neoadjuvant therapy has beenreported.
CONCLUSIONIn conclusion, we report the case of AIP in a patientwho was originally considered to have PDA andunderwent neoadjuvant chemotherapy and subsequentsurgical resection. Postoperative pathologicexamination of the specimen revealed the presence ofabundant IgG4positive plasma cells and ductocentricinflammation, characteristic of AIP. Neither a completepathologic response, nor histologic features of AIP, noran increased number of IgG4positive plasma cells wereseen in any of the other 14 specimens from PDA patientstreated with neoadjuvant chemotherapy examined inthis study. To the best of our knowledge this is the firsttime that these results are being reported in the Englishliterature. We conclude that neoadjuvant chemotherapydoes not result in an IgG4positive plasma cell infiltratein the pancreas, and we additionally have concluded thatour patient had an initial diagnosis of AIP and not PDA.
*********
Author ContributionsOrnela Dervishaj – Substantial contributions toconception and design, Acquisition of data, Analysis and
interpretation of data, Drafting the article, Revising itcritically for important intellectual content, Finalapproval of the version to be publishedHarish Lavu – Substantial contributions to conceptionand design, Acquisition of data, Analysis andinterpretation of data, Drafting the article, Revising itcritically for important intellectual content, Finalapproval of the version to be publishedCharles J Yeo – Substantial contributions to conceptionand design, Acquisition of data, Analysis andinterpretation of data, Drafting the article, Revising itcritically for important intellectual content, Finalapproval of the version to be publishedAgnieszka K Witkiewicz – Substantial contributions toconception and design, Acquisition of data, Analysis andinterpretation of data, Drafting the article, Revising itcritically for important intellectual content, Finalapproval of the version to be publishedGuarantorThe corresponding author is the guarantor ofsubmission.Conflict of InterestAuthors declare no conflict of interest.Copyright© Ornela Dervishaj et al. 2013; This article isdistributed under the terms of Creative CommonsAttribution 3.0 License which permits unrestricted use,distribution and reproduction in any means providedthe original authors and original publisher are properlycredited. (Please see www.ijhpd.com/copyrightpolicy.php for more information.)
REFERENCES1. Yoshida K, Toki F, Takeuchi T, Watanabe S,Shiratori K, Hayashi N. Chronic pancreatitis causedby an autoimmune abnormality. Proposal of theconcept of autoimmune pancreatitis. Dig Dis Sci1995;40(7):1561–8.2. Zhang L, Notohara K, Levy MJ, Chari ST, Smyrk TC.IgG4positive plasma cell infiltration in thediagnosis of autoimmune pancreatitis. ModernPathology 2007;20(1):23–8.3. Deshpande V, Gupta R, Sainani N, et al.Subclassification of Autoimmune Pancreatitis: AHistologic Classification With Clinical Significance.Am J Surg Pathol 2011;35(1):26–35.4. Deshpande V, Chicano S, Finkelberg D, et al.Autoimmune pancreatitis: A systemic immunecomplex mediated disease. Am J Surg Pathol2006;30(12):1537–45.5. Kloppel G, Luttges J, Sipos B, Capelli P, Zamboni G.Autoimmune pancreatitis: pathological findings.JOP 2005;6(1 Suppl):97–101.6. Terumi Kamisawa. Diagnostic criteria forAutoimmune Pancreatitis. J Clin Gastroenterology2008;42(4):404–7.7. Naitoh I, Nakazawa T, Ohara H, et al. ComparativeEvaluation of the Japanese Diagnostic Criteria for

IJHPD – International Journal of Hepatobil iary and Pancreatic Diseases, Vol. 3 , 201 3. ISSN – [2230–901 2]
IJHPD 201 3;3:1 –9.www.ijhpd.com
Autoimmune Pancreatitis. Pancreas2010;39(8):1173–9.8. Stone JH, Zen Y, Deshpande V. IgG4related disease.The New England Journal of Medicine2012;366(6):539–51.9. Giday SA, Khashab MA, Buscaglia JM, et al.Autoimmune pancreatitis: current diagnostic criteriaare suboptimal. Journal of Gastroenterology andHepatology 2011;26(6):970–3.10. Rivera F, LopezTarruella S, VegaVillegas ME,Salcedo M. Treatment of advanced pancreaticcancer: from gemcitabine single agent tocombinations and targeted therapy. CancerTretament Reviews 2009;35(4):335–9.11. Louvet C, Labianca R, Hammel P, et al. Gemcitabinein combination with oxaliplatin compared withgemcitabine alone in locally advanced or metastaticpancreatic cancer: Results of a GERCOR andGISCAD Phase III trial. Journal of Clinical Oncology2005;23(15):3509–16.12. Raina A, Yadav D, Krasinskas AM, et al. Evaluationand management of autoimmune pancreatitis:experience at a large US center. Am J Gastroenterol2009;104(9):2295–306.13. Sah RP, Chari ST, Pannala R, et al. Differences inclinical profile and relapse rate in type 1 versus type2 autoimmune pancreatitis. Gastroenterology2010;139(1):140–8.14. Sah RP, Chari ST. Serologic issues in IgG4relatedsystemic disease and autoimmune pancreatitis.Current opinion in Rheumatology 2011;23(1):108–3.15. Dhall D, Suriawinata AA, Tang LH, Shia J, KlimstraDS. Use of immunohistochemistry for IgG4 indistinction of autoimmune pancreatitis fromperitumoral pancreatitis. Human Pathology2010;41(5):643–52.16. Asghari F, Fitzner B, Holzhüter SA, et al.Identification of quantitative trait loci for murineautoimmune pancreatitis. J Med Genet2011;48(8):557–62.17. Shimosegawa T, Chari ST, Frulloni L, et al.International Consensus Diagnostic Criteria forAutoimmune Pancreatitis Guidelines of theInternational Association of Pancreatology. Pancreas2011;40(3):352–8.18. Ghazale A, Chari ST, Smyrk TC, et al. Value of serumIgG4 in the diagnosis of autoimmune pancreatitisand in distinguishing it from pancreatic cancer.American College of Gastroenterology2007;102(8):1646–53.19. Palmer DH, Stocken DD, Hewitt H, et al. ARandomized Phase 2 Trial of NeoadjuvantChemotherapy in Resectable Pancreatic Cancer:Gemcitabine Alone Versus Gemcitabine Combinedwith Cisplatin. Annals of Surgical Oncology2007;14(7):2088–96.20. Landry J, Catalano PJ, Staley C, et al. Randomizedphase II study of gemcitabine plus radiotherapyversus gemcitabine, 5fluorouracil, and cisplatinfollowed by radiotherapy and 5fluorouracil forpatients with locally advanced, potentially resectablepancreatic adenocarcinoma. J Surg Oncol2010;101(7):587–92.21. Manfredi R, Graziani R, Cicero C, et al. AutoimmunePancreatitis: CT patterns and their changes aftersteroid treatment. Radiology 2008;247(2):435–43.22. Varadhachary GR, Wolff RA, Crane CH, et al.Preoperative gemcitabine and cisplatin followed by
gemcitabinebased chemoradiation for resectableadenocarcinoma of the pancreatic head. J Clin Oncol2008;26(21):3487–95.23. White RR, Tyler DS. Neoadjuvant therapy forpancreatic cancer: the Duke experience. Surg OncolClin N Am 2004;13(4):675–84.24. Katz MH, Pisters PW, Evans DB, et al. Borderlineresectable pancreatic cancer: the importance of thisemerging stage of disease. J Am Coll Surg2008;206(5):833–46.25. Burris HA 3rd, Moore MJ, Andersen J, et al.Improvements in survival and clinical benefit withgemcitabine as firstline therapy for patients withadvanced pancreas cancer: A randomized trial. J ClinOncol 1997;15(6):2403–13.26. Moore MJ, Goldstein D, Hamm J, et al. Erlotinib plusgemcitabine compared with gemcitabine alone inpatients with advanced pancreatic cancer: A phaseIII trial of the National Cancer Institute of CanadaClinical Trials Group. J Clin Oncol2007;25(15):1960–6.27. Heinemann V, Boeck S, Hinke A, Labianca R, LouvetC. Metaanalysis of randomized trials: Evaluation ofbenefit from gemcitabinebased combinationchemotherapy applied in advanced pancreaticcancer. BMC Cancer 2008;8:82.28. National Comprehensive Cancer Network. NCCNclinical practice guidelines in oncology: pancreaticadenocarcinoma. Available at:http://www.nccn.org/professionals/physician_gls/f_guidelines.asp#site Accessed April 9 2010.29. Gillen S, Schuster T, Meyer Zum Buschenfelde C,Friess H, Kleeff J. Preoperative/ neoadjuvant therapyin pancreatic cancer: a systematic review and metaanalysis of response and resection percentages. PLoSMed 2010;7(4):e1000267.30. Artinyan A, Anaya DA, McKenzie S, Ellenhorn JD,Kim J. Neoadjuvant therapy is associated withimproved survival in resectable pancreaticadenocarcinoma. Cancer 2011;117(10):2044–9.31. Van Toorenenbergen AW, Van Heerde MJ, VanBuuren HR. Potential value of serum total IgE fordifferentiation between autoimmune pancreatitisand pancreatic cancer. Scandal J Immunol2010;72(5):444–8.32. Witkiewicz A, Kennedy E, Kenyon L, Yeo CJ, HrubanRH. Synchronous autoimmune pancreatitis andinfliltrating pancreatic ductal adenocarcinoma: casereport and review of the literature. Human Pathology2008;39(10):1548–51.33. Stathopoulos GP, Syrigos K, Aravantinos G, et al. Amulticenter Phase III trial comparing irinotecangemcitabine (IG) with gemcitabine (G) monotherapyas firstline treatment in patients with locallyadvanced or metastatic pancreatic cancer. BritishJournal of Cancer 2006;95(5):587–92.34. AbouAlfa GK, Letourneau R, Harker G, et al.Randomized Phase III study of exatecan andgemcitabine compared with gemcitabine alone inuntreated advanced pancreatic cancer. Journal ofClinical Oncology 2006;24(27):4441–7.35. Moon SH, Kim MH, Park DH, et al. Is a 2weeksteroid trial after initial negative investigation formalignancy useful in differentiating autoimmunepancreatitis from pancreatic cancer? A prospectiveoutcome study. Gut 2008;57(12):1704–12.36. Evans DB, Varadhachary GR, Crane CH, et al.Preoperative gemcitabinebased chemoradiation for
Dervishaj et al. 8

IJHPD – International Journal of Hepatobil iary and Pancreatic Diseases, Vol. 3 , 201 3. ISSN – [2230–901 2]
IJHPD 201 3;3:1 –9.www.ijhpd.com
patients with resectable adenocarcinoma of thepancreatic head. J Clin Oncol2008;26(21):3496–502.37. Kennedy EP, Rosato EL, Sauter PK, et al. Initiationof a critical pathway for pancreaticoduodenectomyat an academic institutionthe first step inmultidisciplinary team building. J Am Coll Surg2007;204(5):917–23.38. Deheragoda MG, Church NI, RodriguezJusto M, etal. The use of immunoglobulin g4 immunostainingin diagnosing pancreatic and extrapancreaticinvolvement in autoimmune pancreatitis. ClinGastroenterol Hepatol 2007;5(10):1229–34.39. Sahani DV, Kalva SP, Farrell J, et al. AutoimmunePancreatitis: Imaging Features. Radiology2004;233(2):345–2.
Dervishaj et al. 9