The Purnell Model for Cultural Competence - Semantic Scholar · The Purnell Model for Cultural...
10
The Purnell Model for Cultural Competence Larry Purnell, PhD, RN, FAAN The twenty^-first centujy has ushered ir\ an era of mul- ticulturalisrn and diuersity in health care. Cultural compe- tence, an essential component within the multidisciplinary healthcare team, has become a major initiative. The Purnell Model of Cultural Competence is proposed as an organizing framework to guide cultural competence among mu/t/discip/inary members of the healthcare team in a variety? of primar\;, secondary/, and tertiary settings. First, essential definitions for understanding culture and cultural concepts are introduced. A brief overview of the Purneil Model for Cultural Competence including pur- poses, underlying assumptions, and major components of the Model are presented. The primary) and secondary} characteristics of culture that determine the degree to which people adhere to their dominant culture are also included. Cultural general knowledge and skills ensures thai providers have a process for "becoming" cuituraily com- petent. This manuscript presents definitions of essential terminology for understanding culture and the Purnell Model for Cultural Competence. KEY WORDS: Purnell Model; Primary character- istics; Secondary characteristics. H ealthcare professionals and healthcare organi- zations are avidly addressing multicultural diversity and racial and ethnic disparities in health. Almost every health journal now has articles addressing "cultural competence." Healthcare professional societies and organizations have some type of standards, initiative, or statement encouraging its mem- bers to become culturally sensitive and/or culturally com- petent. Moreover, one can now find workshops that address culturally sensitive and culturally competent care from a plethora of organizations and individuals. The stress on culture and diversity is good because cultural competence improves the health of the country's citizens. However, culture is an extremely demanding and complex concept, requiring providers to look at themselves, their patients, their communities, their colleagues, and their Larry Purnell, PhD, RN, FAAN, Professor, University of Delaware, College of Health and Nursing Sciences, Department of Nursing, McDowell Hall, Newark, Delaware. employment settings from multiple perspectives. Increasing one's consciousness of cultural diversity improves the possibilities for healthcare practitioners to provide culturally competent care, and therefore improved care. Cultural competence is a conscious process and not necessarily linear. To add to the com- plexity of learning culture, no standardization of terminol- ogy related to culture and ethnicity exists. The definition of cultural sensitivity presented by one person or group is the same definition that another person or group defines as cultural competence or awareness. In an attempt to reach consensus and standardize definitions of these and other terms commonly used in health care, the American Academy of Nursing Expert Panel on Cultural Competence has been developing over the last two years a White Paper that addresses this issue. This manuscript presents definitions of essential terminology as a starting point for understanding culture and the Purnell Model for Cultural Competence. DEFINITIONS Although anthropologists and sociologists have pro- posed many definitions of culture Purnell defines culture as THE JOURNAL OF MULTICULTURAL NURSING & HEALTH 11:2 Summer 2005
Transcript of The Purnell Model for Cultural Competence - Semantic Scholar · The Purnell Model for Cultural...

The Purnell Model for Cultural Competence
Larry Purnell, PhD, RN, FAAN
The twenty^-first centujy has ushered ir\ an era of mul-ticulturalisrn and diuersity in health care. Cultural compe-tence, an essential component within the multidisciplinaryhealthcare team, has become a major initiative. ThePurnell Model of Cultural Competence is proposed as anorganizing framework to guide cultural competenceamong mu/t/discip/inary members of the healthcare teamin a variety? of primar\;, secondary/, and tertiary settings.First, essential definitions for understanding culture andcultural concepts are introduced. A brief overview of thePurneil Model for Cultural Competence including pur-poses, underlying assumptions, and major components of
the Model are presented. The primary) and secondary}characteristics of culture that determine the degree towhich people adhere to their dominant culture are alsoincluded.
Cultural general knowledge and skills ensures thaiproviders have a process for "becoming" cuituraily com-petent. This manuscript presents definitions of essentialterminology for understanding culture and the PurnellModel for Cultural Competence.
KEY WORDS: Purnell Model; Primary character-istics; Secondary characteristics.
Healthcare professionals and healthcare organi-zations are avidly addressing multiculturaldiversity and racial and ethnic disparities inhealth. Almost every health journal now has
articles addressing "cultural competence." Healthcareprofessional societies and organizations have some typeof standards, initiative, or statement encouraging its mem-bers to become culturally sensitive and/or culturally com-petent. Moreover, one can now find workshops thataddress culturally sensitive and culturally competent carefrom a plethora of organizations and individuals. Thestress on culture and diversity is good because culturalcompetence improves the health of the country's citizens.However, culture is an extremely demanding and complexconcept, requiring providers to look at themselves, theirpatients, their communities, their colleagues, and their
Larry Purnell, PhD, RN, FAAN, Professor,University of Delaware, College of Health andNursing Sciences , Department of Nursing,McDowell Hall, Newark, Delaware.
employment settings from multiple perspectives.Increasing one's consciousness of cultural diversity
improves the possibilities for healthcare practitioners toprovide culturally competent care, and thereforeimproved care. Cultural competence is a consciousprocess and not necessarily linear. To add to the com-plexity of learning culture, no standardization of terminol-ogy related to culture and ethnicity exists. The definitionof cultural sensitivity presented by one person or group isthe same definition that another person or group definesas cultural competence or awareness. In an attempt toreach consensus and standardize definitions of these andother terms commonly used in health care, the AmericanAcademy of Nursing Expert Panel on CulturalCompetence has been developing over the last two yearsa White Paper that addresses this issue. This manuscriptpresents definitions of essential terminology as a startingpoint for understanding culture and the Purnell Model forCultural Competence.
DEFINITIONS
Although anthropologists and sociologists have pro-posed many definitions of culture Purnell defines culture as
THE JOURNAL OF MULTICULTURAL NURSING & HEALTH 11:2 Summer 2005

...the totality of socially transmitted behavioral pat-terns, arts, beliefs, values, customs, lifeways, and allother products of human work and thought charac-teristics of a population of people that guide theirworldview and decision making. These patterns maybe explicit or implicit, are primarily learned and trans-mitted within the family, are shared by most membersof the culture, and are emergent phenomena thatchange in response to global phenomena. Culture islearned first in the family, then in school, then in thecommunity and other social organizations such as thechurch. (Purnell, 2003,p.3) .
Within all cultures are subcultures, ethnic groups, orethnocultural populations, groups who have experiencesdifferent from those of the dominant culture with whichthey identify; they may be linked by nationality, language,socioeconomic status, education, sexual orientation, orother factors that functionally unify the group and act col-lectively on each member with a conscious awareness ofthese differences (Purnell, 2003). Additionally, subculturesdiffer from the dominant cultural group and share beliefsaccording to the primary and secondary characteristics ofculture (defined later in this manuscript). A specific exam-ple of how two people from the dominant American cul-ture may vary follows;
Susan Jones, age 62, is an uninsured, single,white Catholic lesbian who makes $20,000 ayear and practices aromatherapy. WilliamJames, age 28, is an insured, heterosexual, mar-ried, white male with 4 children and makes$200,000 per year and believes strongly in high-technology health care.
While these two people both come from the "domi-nant American culture," their worldview is probably verydifferent due to their subcultures and primary and sec-ondary characteristics of culture such as age, gender, sex-ual orientation, marital status, parental status, and socioe-conomic and insurance status.
Culture is largely unconscious and has powerful influ-ences on health and illness. Healthcare providers mustrecognize, respect, and integrate clients' cultural beliefsand practices into health prescriptions. Thus, the providermust be culturally aware, culturally sensitive, and havesome degree of cultural competence to be effective inintegrating health beliefs and practices into plans andinterventions. Cultural awareriess, essentially the objec-tive material culture, has more to do with an appreciationof the external signs of diversity, such as arts, music, dress,and physical characteristics. Cultural sensitivify has moreto do with personal attitudes and not saying things thatmight be offensive to someone from a cultural or ethnicbackground different from the healthcare provider's.Moreover, culturally sensitive, politically correct languagechanges over time, within ethnic groups, and within the
broader cultural group, creating uncertainties for health-care providers. For example, what is the politically correctterm: Hispanic or Latino? According to the Office ofMinority Health (2004), both terms are acceptable.However, some individuals prefer the term Hispanic, oth-ers prefer the term Latino, and for others, neither term isapporpriate and the person self-identifies with anotherterm more appropriate to the country of origin or ethnici-ty. Many times it is not necessary to label a person; how-ever, when it is necessary, simply ask the person howhe/she wishes to be identified.
Cultural competence has several characteristics andincludes knowledge and skills as well as the following:
• Developing an awareness of one's own culture,existence, sensations, thoughts, and environmentwithout letting them have an undue influence onthose from other backgrounds;
• Demonstrating knowledge and understanding ofthe client's culture, health-related needs, andmeanings of health and illness;
• Accepting and respecting cultural differences;• Not assuming that the healthcare provider's
beliefs and values are the same as the client's;• Resisting judgmental attitudes such as "different
is not as good;" and• Being open to cultural encounters;• Being comfortable with cultural encounters;• Adapting care to be congruent with the client's
culture;• Cultural competence is an individualized plan of
care that begins with performing an assessmentthrough a cultural lens.
Organizational cultural competence is also importantand essential for healthcare educational and serviceorganizations. At a minimum, for an organization to beculturally competent, the following should be in place.
• The mission and philosophy must address diver-sity initiatives;
• Culture must be included in the orientation pro-gram of all new employees;
• Diversity workshops must be provided on an ongoing basis;
• Interpretation and translation services must exist,especially in the languages of the population theyserve;
• Cultural brokers must include mentors foremployees unfamiliar with the culture of thepatients;
• Directional signs must be posted in languages ofthe populations who use the facility;
• Culturally congruent meals are provided forpatients;
• An array of culturally diverse artwork and otherobjective signs of culture are displayed;
8 THE JOURNAL OF MULTICULTURAL NURSING & HEALTH 11:2 Summer 2005

• The ethics committee has representation from thecommunity and from the ethnocultural groupsserved;
• A concerted effort is made to recruit employeesrepresentative of the populations they serve; and
• Any number of culturally specific services: e.g. ahospital that serves the orthodox Jewish commu-nity programs elevator doors to open automati-cally and on each floor on the Sabbath and toprovide kosher meals.
The word race has become a very controversial word,at least in the United States. The Human Genome Project(2004) demonstrates that all human beings share a genet-ic code that is over 99 percent identical. Some peopleminimize or dispute the concept of race and others stressits importance given the major initiatives addressing racialand ethnic dispartiies in health care. However, the con-troversial term race must still be addressed. Race is genet-ic in origin and includes physical characteristics that aresimilar among members of the group, such as skin color,blood type, hair and eye color. Difference among races issignificant when conducting health assessments, investi-gating hereditary and genetic diseases, and prescribingmedication. People from a given racial group may, but donot necessarily, share a common culture or subculture:e.g., most African Americans have black skin but a personwith white skin and no ancestry with people with blackskin may self-identity with the African American culture.
Healthcare providers must assess the patient's andfamily's beliefs for effective health maintenance and well-ness, illness and disease prevention, and health restora-tion. A belief is something that is accepted as true, espe-cially as a tenet or a body of tenets accepted by an indi-vidual or group. A common belief among cultures is thathealth, either good health or bad health, is ''God's Will."Beliefs do not have to be proven; they are consciously orunconsciously accepted as truths and must be included inthe client's individualized plan of care, regardless of whatthe provider thinks about them.
All groups have similar or the same values but theyvary in the degree and the intensity by which they areheld by the group and by the individual. Values are prin-ciples and standards that have meaning and worth to anindividual, family, group, or community. Major culturalvalues include individualism versus collectivism, beingversus doing, hierarchial versus egalitarian status, youthversus elders, cooperation versus competetion, ascribedversus achieved status, change versus tradition, and for-mality versus informailty, to name a few. The more one'svalues are internalized, the more difficult it is to avoid thetendency toward ethnocentrism. Ethnocentrism, the uni-versal tendency of human beings to think that their waysof thinking, acting, and believing are the only right, prop-er, and natural ways, can be a major barrier to providingculturally competent care. Ethnocentrism perpetuates anattitude in which beliefs that differ greatly from one's own
are strange, bizarre, or unenlightened, and thereforewrong (Purnell, 2003). Most of the literature in nursingaddresses only the negative aspects of ethnocentrism.However, there is a positive aspect of ethnocentrism fromthe patient's, family's, and community perspetives.Ethnocentrism is responsible for cultural self-survival andhelps people maintain self-worth and self-survival. Thesepositive attributes can be negative when one uses his/herown worth in relation to others who are perceived to beinferior (Walker & Avant, 1995).
Culture as a Process
Cultural competence is a process, not an endpoint(See figure 1). One progresses (a) from unconsciousincompetence (not being aware that one is lacking knowl-edge about another culture), (b) to conscious incompe-tence (being aware that one is lacking knowledge aboutanother culture), (c) to conscious competence (learningabout the client's culture, verifying generalizations aboutthe client's culture, and providing culturally specific inter-ventions), and finally (d) to unconscious competence(automatically providing culturally congruent care toclients of diverse cultures). Unconscious competence isdifficult to accomplish and potentially dangerous becauseindividual differences exist within specific cultural groups.To be even minimally effective, culturally competent care(really an individualized plan of care) must have the assur-ance of continuation after the original impetus is with-drawn; it must be integrated into and valued by the cul-ture that is to benefit from the interventions.
Each healthcare provider adds a new and uniquedimension to the complexity of providing culturally com-petent care. The way healthcare providers perceive them-selves as competent providers is often refiected in the waythey communicate with clients. Thus, it is essential forhealthcare professionals to take time to think about them-selves, their behaviors, and their communication styles inrelation to their perceptions of culture. Cultural selfawareness is a deliberate and conscious cognitive andemotional process of getting to know yourself: your per-sonality, your values, your beliefs, your professionalknowledge standards, your ethics, and the impact of thesefactors on the various roles played when interacting withindividuals who are different from yourself. The ability tounderstand oneself sets the stage for integrating newknowledge related to cultural differences into the profes-sional's knowledge base and perceptions of health inter-ventions. Even then, traces of ethnocentrism may uncon-sciously pervade one's attitudes and behavior.
STEREOTYPING VERSUS GENERALIZATION
Stereotyping, an over simplified conception, opinion,or belief about some aspect of an individual or group ofpeople is a common occurrence among people, andoccurs at the intra-individual level, inter-individual level.
THE JOURNAL OF MULTICULTURAL NURSING & HEALTH 11:2 Summer 2005

and inter-group level (Stevens & Fiske, 1995).Stereotyping has both cognitive (categorization) andmotivational components, which bolsters self-esteem(Baumeister, Smart, & Boden. 1996; Fiske. 2000; Turner,1987). Stereotyping is a normal function and peopleaccentuate differences between categories and minimizedifferences within categories (Capozza & Nanni, 1986). Astereotype can be positive, "all Asians are good in math,"or negative, "all African American teenagers are sexuallypromiscuous." Obviously these statements are example ofsubjective essentialism and entitativity (Yzerbyt, Corneille,& Estrada, 2001) because not all Asians are good at mathand not all African American teenagers are promiscuous.However, stereotyping has advantages, including savingperceivers' mental resources to allow them to operateunder a cognitive load (Pendry, 1998). A stereotype is,however, an endpoint.
Given that stereotyping is a common occurrence,healthcare professionals must concentrate on impressionmanagement and validate cultural group generalizations.Generalization, rules that groups adopt about othergroups, is a point, and the healthcare provider must see ifthe individual fits the cultural pattern. Impression man-agement begins with self awareness and is a consciousprocess through which providers must cognitively engageto control stereotypical thinking (Pacquiao, 2000;Schneider, 1981). The value in making generalizationsabout cultural groups is that the healthcare providerknows what questions to ask. For example, in collectivistcultures, such as Korean, Chinese, Filipino, andVietnamese to name a few, ingroup harmony is essentialto ingroup loyalty and conformity to standards of behav-ior. If the provider automatically assumes that the previ-ous statement is tme, then that person is stereotyping theperson based on the characteristics of east Asian cultures.Adopting such a generalization is a beginning point fromwhich the provider must determine the extent to whichthe patient and/or family adheres to these cultural charac-teristics.
Some authorities believe that learning the charactris-tics of cultural groups and that research on cultural groupscan reinforce stereotyping (Dreher & MacNaughton,2002). These authorities maintain that the provider needsto only know a genera! cultural approach for assessmentsand may disregard cultural specific information. If theprovider does not know cultural specific characteristics,e.g. Mexican clients may use curanderos, masajistas, andsobadores (folk healers) for generic health care, theywould not know to specifically ask about them; and there-fore, essential information may be missed. Knowing boththe genera! and specific characteristics of the culturalgroup leads to an improved assessment allowing one tomake an individualized plan of care.
THE PURNELL MODEL EORCULTURAL COMPETENCE
The Purnell Mode! for Cultural Competence (SeeFigure 1) started as an organizing framework in 1991when the author was teaching undergraduate studentsand discovered the need for both students and staff tohave a framework for learning about their cultures andthe cultures of their patients and families. Comments fromstaff and students made it dear that ethnocentric behav-ior and tack of cultural awareness, cu!tural sensitivity, andcultural competence existed. The Purnell Model wasdesigned as a wholistic organizing framework with specif-ic questions and a format for assessing culture that couldbe used across disciplines and practice settings.
All healthcare discip!ines value communication andneed to know their client's ethnocultural beliefs. Althoughphysicians, nurses, nutritionists, therapists, technicians,morticians, home health aides, and other caregivers needsimilar culturally specific information, the manner inwhich the information is used may differ significantlybased on the discipline, individual experiences, and spe-cific circumstances of interacting with the client. Each dis-cipline has its own unique knowledge base to support itsways of knowing its clients as well as techniques, ro!es,norms, va!ues, ideo!ogies, attitudes, and beliefs, whichinterlock to make a reinforced and supportive systemwithin its defined practice. An understanding of ethnocu!-tural diversity improves the effectiveness of all healthcareproviders.
The Purnell Model has been classified by three well-known nurse theorists as holographic and complexity the-ory because it includes a model and organizing frame-work that can be used by all healthcare providers in vari-ous disciplines and settings. Additionally, these nurse the-orists early in 1998 confirmed that the Purne!! Model wasnot a conceptua! framework, but rather a grand theory.Although the professiona! community recognizes thatscholarly controversy exists in distinguishing between aconceptual framework and grand theory, the va!ue andutility of the Purnell Model has been documented indeveloping cultural competence across disciplines and instimulating further inquiry and knowledge quest.
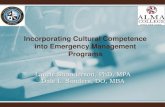
The Model is a circle, with an outlying rim represent-ing globa! society, a second rim representing community,a third rim representing family, and an inner rim repre-senting the person. The interior ofthe circle is divided into12 pie-shaped wedges depicting cu!tural domains andtheir concepts. The dark center of the circ!e representsunknown phenomena. Along the bottom of the mode! isa jagged line representing the nonlinear concept of cultur-al consciousness. The 12 cultural domains (constructs)provide the organizing framework of the mode!.
10 THE JOURNAL OF MULTICULTURAL NURSING & HEALTH 11:2 Summer 2005

Figure 1 - The Purnell Model for Cultural Competence
§ S ^ G ^.§
Unconsciously Incompetent - Consciously incompetent - Consciously competent - Unconsciously competent
Primary characteristics of culture: age, generation, nationality, race, color, gender, religion
Secondary characteristics of culture: educational status, socioeconomic status, occupation, military status, political beliefs, urban versusrural residence, enclave identity, marital status, parental status, physical characteristics, sexual orientation, gender issues, and reason formigration (sojourner, immigrant, undocumented status)
THE JOURNAL OF MULTIOULTURAL NURSING & HEALTH 11:2 Summer 2005 11

Healthcare providers can use this same process to under-stand their own cultural beliefs, attitudes, values, prac-tices, and behaviors.
The purposes of the Purnell Model are to
• Provide a framework for all healthcare providersto learn concepts and characteristics of culture;
• Define circumstances that affect a person's cul-tural worldview in the context of historical per-spectives;
• Provide a nnodel that links the most central rela-tionships of culture;
• Interrelate characteristics of culture to promotecongruence and to facilitate the delivery of con-sciously sensitive and competent health care;
• Provide a framework that rcfiects human charac-teristics such as motivation, intentional ity, andmeaning;
• Provide a structure for analyzing cultural data;and
• View the individual, family, or group within theirunique ethnocultural environment.
The explicit assumptions upon which the Model isbased are
• All healthcare professions need similar informa-tion about cultural diversity.
• All healthcare professions share the metapara-digm concepts of global society, family, person,and health.
• One culture is not better than another culture;they are just different.
• Core similarities are shared by all cultures.• Differences exist within, between, and among
cultures.• Cultures change slowly over time.• The primary and secondary characteristics of cul-
ture determine the degree to which one variesfrom the dominant culture.
• If clients are coparticipants in their care and havea choice in health-related goals, plans, and inter-ventions, their compliance and health outcomeswill be improved.
• Culture has a powerful influence on one's inter-pretation of and responses to health care.
• Individuals and families belong to several cultur-al groups.
• Each individual has the right to be respected forhis or her uniqueness and cultural heritage.
• Caregivers need both cultural-general and cultur-al-specific information in order to provide cultur-ally sensitive and culturally competent care.
• Caregivers who can assess, plan, intervene, andevaluate in a culturally competent manner willimprove the care of clients for whom they care.
• Learning culture is an ongoing process thatdevelops in a variety of ways, but primarilythrough cultural encounters (Campinha-Bacote,2004).
• Prejudices and biases can be minimized with cul-tural understanding.
• To be effective, health care must reflect theunique understanding of the values, beliefs, atti-tudes, lifeways, and worldview of diverse popu-lations and individual acculturation patterns.
• Differences in race and culture often requireadaptations to standard interventions.
• Cultural awareness improves the caregiver's self-awareness.
• When individuals of dissimilar cultural orienta-tions meet in a work or therapeutic environment,the likelihood for developing a mutually satisfy-ing relationship is improved if both parties in therelationship attempt to learn about each other'sculture.
• Culture is not border bound. Fteople bring theirculture with then when they migrate.
• Professions, organizations, and associations havetheir own culture, which can be analyzed using agrand theory of culture.
METAPARADIGM CONCEPTS
The macro aspects of this Model include the tradi-tional nursing metaparadigm concepts of global society,community, family, and person. Although not all nursetheorists support the nursing metaparadigm concepts(Leininger, 1997}, this author has found them to beimmensely valuable because they provide a wholistic andglobal perspective. The theory and model are conceptu-alized from biology, anthropology, sociology, economics,geography, history, ecology, physiology, psychology,political science, pharmacology, and nutrition as well astheories from communication, family development, andsocial support. The Model can be used in clinical practice,in formal and continuing education education, inresearch, and in the administration and management ofhealthcare services.
Phenomena related to a global society include worldcommunication and politics; conflicts and warfare; natu-ral disasters and famines; international exchanges in edu-cation, business, commerce, and information technology;advances in the health sciences; space exploration; andthe expanded opportunities for people to travel aroundthe world cind interact with diverse societies. Globalevents that are widely disseminated by television, radio,satellite transmission, newsprint, and information technol-ogy affect all societies, either directly or indirectly. Suchevents create chaos while consciously and unconsciouslyforcing people to alter their lifeways, worldviews, andacculturation patterns.
12 THE JOURNAL OF MULTICULTURAL NURSING & HEALTH 11:2 Summer 2005

In its broadest definition, community is a group ofpeople having a common interest or identity and living ina specified locality. Community includes the physical,social, and symbolic characteristics that cause people toconnect. Bodies of water, mountains, rural versus urbanliving, and even railroad tracks help people define theirphysical concept of community. Today, however, technol-ogy and the Internet allow people to expand their com-munity beyond physical boundaries. Economics, religion,politics, age, generation, and marital status delineate thesocial concepts of community. Sharing a specific languageor dialect, lifestyle, history, dress, art, or musical interestare symbolic characteristics of a community. Peopleactively and passively interact with the community, neces-sitating adaptation and assimilation for equilibrium andhomeostasis in their worldview. Individuals may willinglychange their physical, social, and symbolic communitywhen it no longer meets their needs.
A family; is two or more people who are emotionallyconnected. They may, but do not necessarily, live in closeproximity to each other. Family may include physicallyand emotionally close and distant consanguineous rela-tives as well as physically and emotionally connected anddistant non-blood-related significant others. Family struc-ture and roles change according to age, generation, mar-ital status, relocation or immigration, and socioeconomicstatus, requiring each person to rethink individual beliefsand lifeways.
A person is a biopsychosociocultural being who isconstantly adapting to his or her environment. Humanbeings adapt biologically and physiologically with theaging process; psychologically in the context of social rela-tionships, stress, and relaxation; socially as they interactwith the changing community; and ethnoculturally withinthe broader global society. In highly individualisticWestern cultures, a person is a separate physical andunique psychological being and a singular member ofsociety. The self is separate from others. However, in high-ly collectivist Asian cultures, the individual is defined inrelation to the family, including ancestors, or anothergroup rather than a basic unit of nature.
Health, as used in this article, is a state of wellness asdefined by people within their ethnocultural group.Health generally includes physical, mental, and spiritualstates. The concept of health, which permeates all meta-paradigm concepts of culture, is defined globally, nation-ally, regionally, locally, and individually. People can speakabout their personal health status or the health status ofthe nation or community. Health can also be subjective orobjective in nature.
In the center of the Purnell Model Is an empty circle.This circle represents unknown phenomena, practices, andcharacteristics of the individual or the group. In the case ofhealthcare providers, this circle can expand or contractdepending upon the providers cultural self awareness andthe knowldege and skills they possess for working with cul-tually diverse clients, families, and communities.
CONSTRUCTS AND CONCEPTS
On a micro level, the Model has an organizing frame-work consisting of 12 domains, constructs, and their con-cepts, which are cotnmon to all cultures, subcultures, andethnic groups. These 12 domains are interconnected andhave implications for health. The utility of this organizingframework comes from its concise structure, which can beused in any setting and applied to a broad range of empir-ical experiences and can foster inductive and deductivereasoning in the assessment of cultural domains. They canbe used to formulate questions and statements for con-ducting research. Once cultural data are analyzed, thepractitioner can fully adopt, modify, or reject healthcareinterventions and treatment regimens in a manner thatrespects the client's cultural differences. Such adaptationsimprove the quality of the client's healthcare experiencesand personal existence.
THE 12 DOMAINS OF CULTURE
The 12 domains and their concepts essential forassessing the cultural attributes of an individual, family, orgroup are as follows:
• Overview, inhabited localities, and topographyincludes concepts related to the country of origin,current residence, the effects of the topography ofthe country of origin and current residence, eco-nomics, politics, reasons for emigration, andvalue places on education.
• Communication includes concepts related to thedominant language and dialects; contextual useof the language; and paralanguage variationssuch as voice volume, tone, intonations, reflec-tions, and willingness to share thoughts and feel-ings. Nonverbal communications such as the useof eye contact, facial expressions, touch, bodylanguage, spatial distancing practices, andacceptable greetings; temporality in terms of past,present, or future worldview; clock versus socialtime; and the use of names are also importantcommunication variables.
• Family roles and organization includes conceptsrelated to the head of the household and genderroles; family roles, priorities, and developmentaltasks of children and adolescents; childrearingpractices and roles of the aged and extendedfamily members. Individual and family social sta-tus in the community; and views toward alterna-tive life styles such as single parenting, sexual ori-entation, childless marriages, and divorce arealso included in this domain.
• Workforce issues include concepts related to
THE JOURNAL OF MULTICULTURAL NURSING & HEALTH 11:2 Summer 2005 13

autonomy, acculturation, assimilation, genderroles, ethnic communication styles, and health-care practices from the country of origin.
• Biocultura! ecology includes variations in specificethnic and racial origins such as skin colorationand physical differences in body stature; genet-ic, hereditary, endemic, and topographical dis-eases; and the differences in the way drugs aremetabolized by the body.
• High-risk behaviors includes the use of tobacco,cilcohol, and recreational drugs; lack of physicalactivity; increased calorie consumption; nonuseof safety measures such as seatbelts, and hel-mets; and engaging in risky sexual practices.
• Nutrition includes having adequate food for sat-isfying hunger; the meaning of food; food choic-es, rituals, and taboos; enzyme deficiencies; andhow food and food substances are used forhealth promotion and wellness and during illness
• Pregnancy and childbearing practices includesfertility practices; culturally sanctioned andunsanctioned methods for birth control: viewstoward pregnancy; and prescriptive, restrictive,and taboo practices related to pregnancy,birthing, and postpartum.
• Death rituals includes how the individual and theculture view death, rituals, and behaviors to pre-pare for death, and burial practices. Bereavementbehaviors are also included in this domain.
• Spirituality includes religious practices and theuse of prayer, behaviors that give meaning to life,and individual sources of strength.
• Healthcare practices includes the focus of healthcare such as acute or preventive; traditional,magicoreligious, and biomedical beliefs; individ-ual responsibility for health; self-medicatingpractices; and views toward mental illness,chronicity, rehabilitation, and organ donationand transplantation. Additionally, one's responseto pain and the sick role are shaped by culture.Barriers to health care are included in thisdomain.
• Healthcare practitioners concepts include the sta-tus, use, and perceptions of traditional, magi-coreligious, and Western biomediccil healthcareproviders. Additionally, the gender of the health-care provider may have significance in some cul-tural groups.
PRIMARY AND SECONDARY OF CULTURE
Major influences that shape peoples' worldview andthe degree to which they identify with and adhere to theircultural group of origin are called the primary and sec-ondary characteristics of culture. The primary characteris-tics are nationality, race, color, gender, age, and religiousaffiliation. Primary characteristics cannot easily bechanged. If these characteristics such as religion or genderare changed, a significant stigma may attach to the indi-vidual from society.
The secondary characteristics include educational sta-tus, socioeconomic status, occupation, military experi-ence, political beliefs, urban versus rural residence,enclave identity, marital status, parental status, physicalcharacteristics, sexual orientation, gender issues, reasonfor migration (sojourner, immigrant, or undocumentedstatus}, and length of time away from the country of ori-gin. People who live in ethnic enclaves and get their work,shopping, and business needs met without learning thelanguage and customs of their host country may be moretraditional than people in their home country.Immigration status influences a person's worldview. Forexample, people who voluntarily immigrate generallyacculturate more willingly; i.e., they modify their own cul-ture as a result of contact with another culture. Moreover,acculturation has different degrees in different contexts.For example, a person my acculturate in the workforce interms of language and practices, but speak their nativelanguage and adhere to traditional practices when athome. Similarly, they assimilate, that is, gradually adoptand incorporate the characteristics of the prevailing cul-ture more easily than people who immigrate unwillingly oras sojourners. Sojourners, who immigrate with the inten-tion of remaining in their new homeland only a shorttime, or refugees, who think they may return to theirhome country, may not perceive the need to acculturateor assimilate. Additionally, undocumented individuals(illegal aliens) may have a different worldview from thosewho have arrived with work visas as "legal immigrants."
CONCLUSION
Today, each subgroup has the right to be respectedfor its unique individuality. Most health-related education-al programs and service providers have statementsaddressing multicultural diversity. Organizations and indi-viduals who understand their clients' cultural values,beliefs, and practices are in a better position to be co-par-ticipants with their clients and provide culturally accept-able care. Accordingly, multidisciplinary healthcare pro-fessionals can use the Purnetl Model as a guide for assess-ing, planning, implementing, and evaluating interven-tions. Through a systematic appraisal for each client andindividualizing care, improved opportunities for healthpromotion, illness and disease prevention, and healthrestoration occurs. To this end, healthcare providers need
14 THE JOURNAL OF MULTICULTURAL NURSING & HEALTH 11:2 Summer 2005

both general and specific cultural knowledge. One cannotpossibly know all the diverse world cultures and theircharacteristics. Cultural general knowledge and skills
ensures that providers have a process for "becoming" cul-turally competent.
REFERENCES
Baumeister, R., Smart, L, & Boden, J. (1996). Relation ofthreatened egoism to violence and aggression: Thedark side of self-esteem. Ps\^chological Reuiew, 105,5-33.
Campinha-Bacote. J. (2004). A Culturally CompetentModel of Care. Retrieved October 7, 2004 fromhttp://www.transculturalcare.net/
Capozza, D., & Nanni, R. (1986). Differentiation processfor social stimuli with different degrees of categoryrepresentativeness. European Journal of SocialPsychology, 16, 399-412.
Dreher, M., & MacNaughton, A. (2002). Cultural compe-tence in nursing: Foundation or fallacy. NursingOutlook, 50, 181-186.
Fiske, S. (2000). Stereotyping, prejudice, and discrimina-tion at the seam between centuries: Evolution, cul-ture, mind, and brain. European Journal of SocialPsi;chotog];, 30, 299-322.
Human Genome Project. (2004). Retrieved October 7,2004 fromhttp://www.ornl.gov/sci/techresources/Human_Genome/home.shtml
Joint Commission on Accreditation of HealthcareOrganizations: Standards (2004). Retrieved July 18,2004 fromhtfp://www.jcaho.org/accredited-I-organizations/ambulatory+care/standards/field -I- reviews/repl_fr.htm
Leininger, M. (1997). Overview of the Theory of CultureCare with fhe ethnonursing research method.Journal of Transcultural Nursing, (8)2, 32-52.
Office of Minority Health. (2004). Retrieved October2004 from http://www.ohmrc.gov
Pacquiao, D. (2000). Impression management: An alter-native to assertiveness in intercultural communica-tion. Journal of Transcultural Nursing, 11(1), 5-6.
Pendry, L. (1998). When the mind is otherwise engaged:Resource depletion and social stereotyping.EuropeanJournal of Social Psychology, 28, 293-299.
Purnell, L. (2003). Transcultural diversity and health care.In L. Purnel! and B. F^ulanka (Eds.), Transculturalhealth care: A culturally; competent approach, (2 ed.,pp. 1-7). Philadelphia: F A. Davis.
Schneider, D. (1981). Tactical self-presentation: Towardsa broader conception. In J. T. Tedecshi (Ed.),Impression management theory and social psijcholog-ical research (pp. 23-40). NY: Academic Press.
Stevens, L, & Fiske, S. (1995). Motivation and cognitionin social life: A social survival perspective. SocialCognition, 13, 189-214.
Walker, L, & Avant, K. (1995). Strategies for theory con-struction in nursing (3 ed) . Norwalk, CT: Appleton &Lange.
Yzerbyt, V, Corneille, O., & Estrada, C. (2001). The inter-play of subjective essentialism and entitativity in theformation of stereotypes. Personality and SocialPsychology Reuiew, (5)2, 141-155.
THE JOURNAL OF MULTICULTURAL NURSING & HEALTH 11:2 Summer 2005 15