The Present and Future of HIV Prevention Abridged Deck
57
description
Presentation slides of select panelists at the Jhpiego event, The Present and Future of HIV Prevention.
Transcript of The Present and Future of HIV Prevention Abridged Deck


Combination HIV Prevention: Now is the Time
April 25, 2013
Chris Beyrer MD, MPHJohns Hopkins Bloomberg School of Public Health

Combination HIV prevention
Strategic, simultaneous use of different classes of prevention: biomedical, behavioral, social/structural
Operates on multiple levels (individual, relationship, community, social), to respond to the specific needs of particular communities and modes of HIV transmission
Efficient use of resources through prioritizing, partnership, and engagement of affected communities

The CDC Continuum of HIV Care - 2011
80%
62%
41%36%
28%
Greenberg, CROI 2013

HIV treatment reduces incidence at community levels

Global HIV prevalence of HIV in MSM compared with regional adult prevalence in 2011
Source: Beyrer, Baral, van Griensven, Goodreau, Chariyalertsak, Wirtz, Brookmeyer, The Lancet, 2012

Map of HIV prevalence among female sex workers in low-income and middle-income countries, 2007-2011
Pooled OR for HIV infection among FSW compared to other reproductive age women: 13.49 (95% CI 10.04-18.12)

Map of HIV prevalence among transgender women, 2000-2011
Pooled OR for HIV infection among TGW compared to other reproductive people: 48.8 (95% CI 31.2-76.3)

Combinations for Key Populations
Strategic, simultaneous use of different classes of prevention: biomedical, behavioral, social/structural
Targeted to the drivers of HIV: granular, specific, acceptable, scalable
Implemented in partnership, with real engagement of affected communities

Effect of different intervention combinations and yearly recruitment rates on HIV incidence after 5 years
Degenhardt, et al. Prevention of HIV infection for people who inject drugs. Lancet 2010.

Scaling up Combination HIV Interventions when force of infection is great: Nairobi, Kenya IDUs. (Strathdee, et al,
Lancet 2010)

MP3: MODEL EVALUATED IMPACT OF COMBINATION HIV PREVENTION FOR MSM IN SOUTH AFRICA
KEY MODEL CHARACTERISTICS• Agent based stochastic model (micro-simulation)• Calibrated to peri-urban South Africa MSM• Sexual mixing networks of main, regular & casual partners• Accounts for increased transmission with UAIs• Accounts for heterogeneities in sexual behaviors (predominantly receptive, predominantly insertive, versatile) frequency of HIV testing (high, low, never testers)• Accounts for impact of ART on risk of acquisition and transmission• Accounts for variability in acceptance and adherence rates to PREP
MODEL OUTPUTCumulative incident infections over 5 years AIMS:• Reduce UAIs• Increase ART coverage for tested HIV infected persons (<350 CD4)• Provide PREP for high risk persons (># partners or in sero-discordant couples)• Increase HIV testing
The Sibanye MP3 Project (NIAID R01-AI094575) PI: Patrick Sullivan



Conclusions
• Combination prevention is already a reality
• Refinement needed—research will be key
• Combinations for key populations will need to be targeted, informed by epidemiology, specific to be effective


The Present and The Future of HIV Prevention:Voluntary Medical Male CircumcisionApril 25, 2013

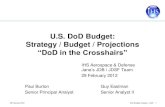
Three randomized control trials (RCTs) demonstrated that adult VMMC reduces men’s risk of HIV acquisition by 60 percent
Follow-up up to five or six years post-trial indicated that this protective effect was durable and even increased over time.
VMMC is a one-time, short procedure that confers a lifetime of reduced HIV infection risk for heterosexual men. VMMC also reduces the risk for human papillomavirus (HPV), cervical cancer and some STIs among men and female sexual partners of circumcised men
0.85
2.1
0.66
2.1
4.2
1.33
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
South Africa Kenya Uganda
Trial
HIV
In
cid
ence
/100
py
Intervention
Control
Efficacy60% (CI 30-77%)
Efficacy 53% (CI 22-72%)
Efficacy60% (CI 32-76%)

If eight of 10 adult men are circumcised within five years in 14 priority countries in eastern and southern Africa, approximately 3.5 million new HIV infections may be prevented within 15 years, averting as much as $16.5 billion in HIV care and treatment costs.
Almost half of the infections averted are among women


VMMC is provided as a minimum package of services that and is in addition to existing and new HIV prevention interventions
VMMC programs offer unprecedented opportunities to engage men in health education and counseling, notably HTC services
Men who are identified as living with HIV by VMMC programs are referred to the continuum of care, including ART (further decreasing their HIV transmission risk)
Education and Counseling
Screening and treatment for
STIs
Provision of male and female condoms
Safe circumcision procedure
Post op follow up and linkage
to care

Annual number of VMMCs funded through PEPFAR in 14 priority countries
According to WHO and PEPFAR estimates achievement towards the 20 m
• End of 2010 ~3%
• By October 2011 ~5%
• By December 2012 ~ 12% Total=2,352,780
2007-2009 2010 2011 2012
Series1 73200 218900 574200 1486480
100,000
300,000
500,000
700,000
900,000
1,100,000
1,300,000
1,500,000
Chart Title
Nu
mb
er o
f M
Cs

Jhpiego’s Support to Four Countries
2008 2009 2010 2011 20120
50000
100000
150000
200000
250000
300000
350000
400000
16325595
99195
244628
380235
Mozambique, Tanzania, Kenya, Zambia (15-20% of global VMMC)
Commulative

As VMMC is scaled up, challenges faced have differed from country to country
In many populations acceptability is high but demand for services, particularly among ‘older men’ remains low
There is a need for continued innovation both in how VMMC is expanded and in the products and tools that support such expansion, e.g. private sector, increased efficiency and quality of services, new circumcision devices being evaluated by WHO
There is also a need to innovate in the areas of communication, “marketing” and demand generation to maximize the benefits of VMMC for men, women and their families
Sustainability through introduction of Early Infant Male Circumcision
Shang Ring


The Present and Future of the Prevention of Mother-to-Child
Transmission of HIV in Resource-Limited Settings
Rene Ekpini, MD, MPH
JHPIEGO’s PANEL
Washington DC,
April 25, 2013

1.The present: the Global plan for the Elimination of New HIV Infections among Children by 2015 and Keeping their Alive
2.The Need to Sharpen our Response: why we still need more effective PMTCT programmes
3.The future of PMTCT: reshaping PMTCT programmes and the global agenda
Outline

The present
the Global plan for the Elimination of New HIV
Infections among Children by 2015 and Keeping their
Alive

Global Sub-Saharan Africa
Number of women 15+ living with HIV
15.0 million 8.7 million 58%
Number of pregnant women living with HIV
1.47 million 1.36 million 92%
Number of children <15 years living with HIV
3.3 million 3.1 million 94%
Number of children <15 years newly infected with HIV
330,000 300,000 91%
Number of children <15 years dying of AIDS related causes
230,000 210,000 91%
Global summary of HIV epidemic in women and children, UNAIDS 2011
UNAIDS, Global Report on AIDS, 2012

Global Plan Towards the Elimination of New HIV Infections Among Children by 2015 and Keeping
Their Mothers Alive (EMTCT)
Source: P.39 of the Global Plan towards the elimination of new HIV infections among children by 2015 and keeping their mothers alive

Prevention of Mother-to-Transmission of HIV (PMTCT): the four-pronged
approach
Childbearing
women
Women
living
with HIV Pregnant
women
living with
HIV HIV-infected
children
Prevent new
infections Avoid unintended
pregnancies
Prevent
MTCT
Care, treatment and support for mothers & their
children
1
2
3
4

Progress toward MTCT elimination goals in 22 priority countries, 2009-2011
UNAIDS, A progress report on the Global Plan towards the elimination of new HIV infections among children by 2015 and keeping their mothers alive, 2012

Treatment simplification and optimization for MTCT elimination
1 pill a day for All HIV+ pregnant women
Increasing access for 1000s of women (Coverage & Uptake)
Low transmission rate: Saving life of 1000s of children
Simplification Optimization High impact on maternal
&child health
No CD4 for initiation

TUNISIA
MOROCCO
SAHARA
ALGERIA
MAURITANIA
MALI NIGE
R
LIBYA
CHAD
Mediterranean Sea
Sea
EGYPT
SUDAN
ETHIOPIA
DJIBOUTI
ERITREA
SOMALIAKENYA
TANZANIA
DEMOCRATIC
CENTRAL
RWANDA
GABON
EQUATORIAL
ANGOLA
CONGO
NIGERIA
BENIN
DTVOIRE
SIERRA
SENEGAL
GHANA
THE
GUINEA
LIBERIA
CAMEROON
SOUTH AFRICA
MALAWI
ZAMBIA
MOZAMBIQUE MADAGASCARZIMBABWE
BOTSWANA
SWAZILAND
Indian
Ocean
LESOTHO
NAMIBIA
ANGOLA
Atlantic
Ocean
WESTERN
Red
UGANDA
OF THE CONGO
REPUBLIC
BURUNDI
GUINEAREP. OF
TOGOCOTE
BURKINA
GUINEA
LEONE
GAMBIA
BISSAU
Walvis Bay
SOUTH
REPUBLIC
AFRICAN
THE
AFRICA
Legend Actively implementing or phased roll- out underway
MOH endorsed; preparing for roll-out
Operational planning, piloting, or costing underway
Considering B+
No immediate plans to implement B+
SOUTHSUDAN
Source: PEPFAR PMTCT/Pediatrics TWG - Updated February 28, 2013
Many countries transitioning to lifelong triple ARV regimen for PMTCT (Option
B+)
Note: Haiti is actively implementing Option B+; India is implementing Option B+ in two states

The Need to Sharpen our Response
Why we still need more effective PMTCT
programmes

The performance of the MNCH platform is critical: modalities of MTCT elimination in the US vs
Low- and middle-income countries
Timing of ANC
1st Trim 2nd Trim 3rd Trim
US 73% 21% 5%
LMIC 28% 40% 28%
Pe
rcen
t

Elimination of MTCT requires more than just effective ARV regimens
• Continuing new HIV infections in women of childbearing age in sub-Saharan Africa- HIV prevalence is higher among young women than
young men
- In 2010, 71% of people 15-24 years old living with HIV were women
• HIV incidence in pregnancy in low-resource countries ranges between 1.3-10.7 with an increased risk of HIV transmission to infants during pregnancy and in the postnatal
• High rates of unmet needs for family planning in most countries: women living with HIV have similar or lower rates compared to HIV-uninfected women

Remaining issues with ARV-based interventions
• Even with maternal triple drug regimens, there is still residual postnatal transmission, particularly for infants of women presenting late in pregnancy or in labor
• Actual impact depends on adherence to maternal antiretroviral therapy (ART) especially in the postnatal period
• Even with maternal ART, residual breast milk infection (1-4% at 6 months, 2-6% at 12 months) still exists

The Future of PMTCT
Reshaping PMTCT
programmes and the global agenda

Conceptual framework for a strategic shift for optimal impact
Novel PMTCT-related prevention strategies VACCINES (Pregnant women-Neonates); MICROBICIDES
Targeted interventions for ADOLESCENT GIRLS
Lifelong ART for HIV+ pregnant women
Curing HIV infected
newborns
Integrating HIV testing in FP clinics
Test and Trea
t (ART)
Primary prevention &
ART for sexual partners
1
3
Integrating Family planning in:
ANC & PNC
ART centers/ clinics
Prevention of
unintended
pregnancies
(FAMILY PLANNING
)

Transforming MNCH services for effective delivery of an integrated
model of care
Early ANC booking during 1st trimester
Focused ANC
(at least 4 visits)
Institutional delivery
Postnatal care
Triple ARVs for PMTCT
Infant feeding counselling and support
Facility and community level interventions
Removing supply and demand side bottlenecks
Retention in care and treatment

Challenges ahead -1
•Scaling up “test and treat” approach in low prevalence and concentrated epidemic settings: what approaches for HIV testing and counseling?
•Rethinking the public health and clinical purpose of CD4 counts (vs low cost point of care viral load) and Early Infant Diagnosis (DBS/PCR) in a well performing programme
At the programmatic level

Challenges ahead -2
• Mainstreaming MTCT elimination in the global health agenda and national development strategies for a broader impact beyond HIV
• Do not forget HIV-infected children: influencing the global agenda and national responses for paediatric HIV treatment and care in the context of MTCT elimination
• Creating a social movement to improve accountability: establishing durable community accountability mechanisms that involve women and men living with HIV
At the policy level

Two Worlds, Two Realities, One Hope: addressing inequity for social justice
Special thanks to: Lynne Mofenson


The Present & Future of HIV Prevention
An Advocate’s Perspective
Mitchell WarrenExecutive Director, AVAC25 April 2013

“Few could have imagined that we’d be talking about the real possibility of an AIDS-free generation. But that’s what we’re talking about.”
December 1, 2011

“An AIDS free generation is within our reach.” February 12, 2013

AIDS-free generation
Cure
Ending AIDS
Ending the epidemic
Functional cure
Preventive vaccine
Treatment as prevention
Therapeutic vaccine
“Epidemic” is occurrence of more cases of disease than would normally be expected in a specific place or community over a period of time. “Ending” would lower rate of new infections, and even eliminate new cases in some populations. See also “beginning to end…”
Sometimes used in reference to the specific goal of eliminating new pediatric infections by 2015, allowing a generation of children to be born without HIV.
Strategy to eliminate HIV from a person’s body. A cure would be a revolutionary breakthrough, but is not a requisite for ending the epidemic.
HIV is the virus that causes the syndrome of diseases known as AIDS. A goal of “ending AIDS” can be understood as effectively treating all people with HIV and ensuring them long, healthy lives.
Strategy to suppress HIV viral load keeping it below the level of detection without the use of ART. The virus would not be eliminated from the body but would be effectively controlled.
Vaccine used in HIV-negative individuals to prevent or dramatically reduce the risk of infection. Many believe that the long-term goal of ending the epidemic—and preventing a surge of new infections—depends on a vaccine.
Vaccine designed to stimulate the immune response to HIV in a person already infected with the virus, in order to control the infection. Also referred to as an immunotherapeutic vaccine.
Systemtic use of ART to reduce sexual transmission risk in HIV-positive people. Also known as TasP, T4P, TisP and TLC+ (testing, linkage to care plus tx).
Mind the Language

Prevention Paradigm 2013 and beyondDifferent Strokes for Different Folks
Method Contraception HIV Prevention
Behaviour ✓ ✓
Barrier Methods ✓ ✓
Gels ✓
Rings ✓
Oral pill ✓ ✓
Injectables ✓
Implants ✓
Surgical procedures ✓ ✓
Treatment ✓

CO
MB
IN
E
Demonstrate proven tools for immediate impact
• Daily oral TDF/FTC as PrEP• 1% tenofovir gel
Develop long-term solutions to end the epidemic• AIDS vaccines• Cure• Multi-purpose prevention technologies• Next generation ARV-based prevention• Non-ARV-based microbicides• Rectal microbicides
Years to Impact Zero to 5 5 to 10 10 to End
GOAL: A sustained d e c l i n e i n H I V infections (now at 2.5 million/year)
• Define and initiate the “core package” of PrEP demonstration projects
• Safeguard HIV Prevention Research Funding
• End confusion about “combination prevention”
• Narrow gaps in treatment cascade• Prepare for new non-surgical male
circumcision devices
• Testing• Treatment• Voluntary Medical Male Circumcision • Female and male condoms• Prevention of pediatric infection• Syringe exchange programs
Deliver proven tools for immediate impact
AVAC Report 2012: Achieving the End – One year and counting. www.avac.org/report2012.
Three-Part Agenda for Ending AIDS

DNA/
Ad5
2010 2011 2012 2013 2014 2015 2016
1 2 3 4 1 2 3 4 1 2 3 4 1 2 3 4 1 2 3 4 1 2 3 4 1 2 3 4
Positive efficacy result
No effect
Regulatory submission/filing
Planned
Final results pending
DPV ring
Oral TDF/FTC
Oral TDF
Rectal TFV gel
TFV gel
TMC278 LA Injectable
DNA/Ad5
TIMELINE LEGEND
Pox-Protein
HIV Prevention Options Timeline * **
* Trial end-dates are estimates; due to the nature of clinical trials the actual dates may change. For full trial details, see www.avac.org/pxrd. ** Not all trials included are effectiveness trials. Trials included on this list are mainly phase II/IIb, III/IIIb and IV trials.
Bangkok Tenofovir Study/CDC 4370
Partners PrEP Partners PrEP (no placebo)2008
2005
2009 VOICE/MTN 003
Ora
l TDF
/FTC
Ora
l TDF
iPrEx2007 iPrEx Open-Label Extension (OLE)
2009 FEM-PrEP
US FDA approval
CAPRISA 0042007
2007 TDF2 Open-Label ExtensionTDF2/CDC 4940
TFV
gel
FACTS 001Earliest regulatory submission
VOICE/MTN 0032009
MTN 017 Rect
al
TFV
gel
DPV
Ring The Ring Study/IPM 027
ASPIRE/MTN 020
Earliest regulatory submission
Possible Long-Acting Injectable efficacy
TMC
278
LA In
ject
.Po
x-Pr
otei
n
Various Phase I/II preliminary and bridging studiesRV 1442004
South Africa Licensure
South Africa Research
Thai Licensure
2009 HVTN 505
Additional demonstration projects & intermittent PrEP studies
CAPRISA 008
FACTS 002 and other adolescent studies
Various Phases of Long-Acting Injectables (TMC278, GSK744)
AVAC Report 2012: Achieving the End – One year and counting. www.avac.org/report2012
AVAC, April 2013

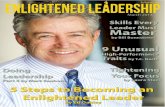
Who is actually in the trial?
Trial Median Age
Married/Stable partner Efficacy Adherence
(as per drug levels)
CAP 004 24 88% TFV gel: 39% [CI = 6-60%] 50.5%
iPrEx 27 Oral TDF/FTC: 42% [CI = 18-60%] 51%
Partners PrEP 36 98% Oral TDF: 67% [CI = 44-81%]
Oral TFD/FTC: 75% [CI = 55-87%] 83%81%
TDF-2 25 6% Oral TDF/FTC: 62% [CI = 22-83%] 80.5%
FEM-PrEP 24 31% Oral TDF/FTC: No Protection 24%
VOICE 25 21%TFV gel: No protectionOral TDF: No protectionOral TDF/FTC: No protection
23%28%29%
VOICE-SA 25 8% To come
VOICE-Ug 28 50% To come
VOICE-Zim 28 94% To come
FACTS 2015

The most recent bottom line(s)
Prevention research is hard – and unpredictable!We need to improve adherence
By improving adherence supportBy “improving” existing products through marketingBy developing other types of products
We need to better understand behaviours – sexual, product use, trial participation and personal reporting
…and the “pre-behaviours” – risk perception