The Pharmacology of TNF Inhibitors Clinical Investigator Amgen/Wyeth Centocor NIH (GAIT) LaJolla...
43
The Pharmacology of TNF The Pharmacology of TNF Inhibitors Inhibitors Clinical Investigator Amgen/Wyeth Centocor NIH (GAIT) LaJolla Pharmaceuticals ISIS Genentech/IDEC Aventis Consultant/Lecturer Aventis Centocor Amgen/Immunex Wyeth-Ayerst Pharmacia Abbott Astra Zeneca
-
Upload
thomasine-stewart -
Category
Documents
-
view
222 -
download
0
Transcript of The Pharmacology of TNF Inhibitors Clinical Investigator Amgen/Wyeth Centocor NIH (GAIT) LaJolla...

The Pharmacology of TNF The Pharmacology of TNF InhibitorsInhibitors
Clinical Investigator
Amgen/WyethCentocorNIH (GAIT)LaJolla
Pharmaceuticals ISISGenentech/IDECAventis
Consultant/LecturerAventisCentocorAmgen/ImmunexWyeth-AyerstPharmaciaAbbottAstra Zeneca
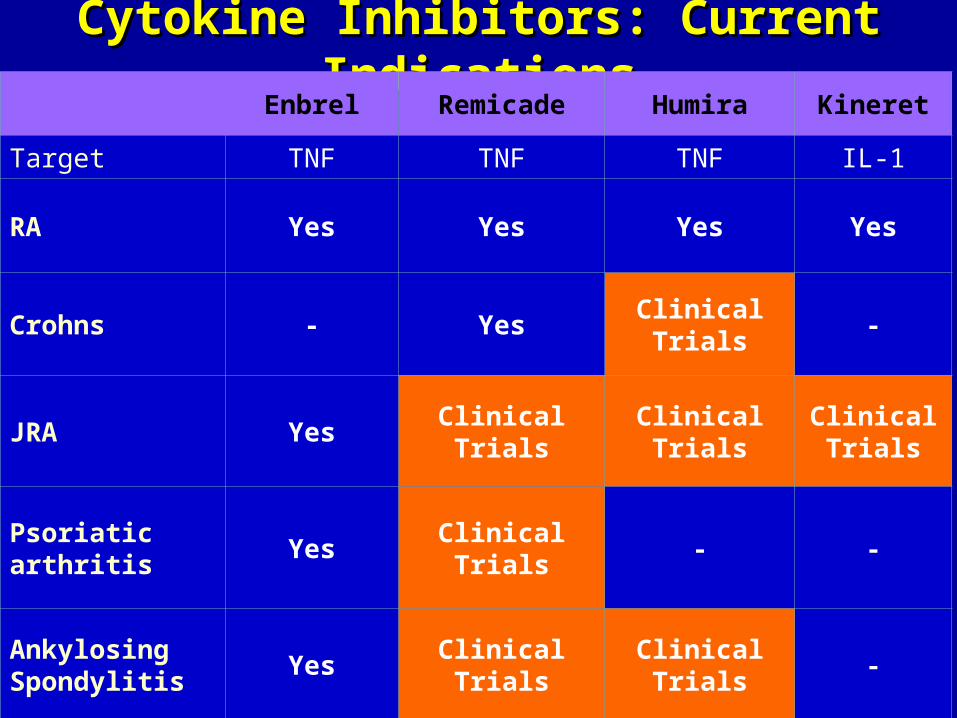
Cytokine Inhibitors: Current IndicationsCytokine Inhibitors: Current IndicationsEnbrel Remicade Humira Kineret
Target TNF TNF TNF IL-1
RA Yes Yes Yes Yes
Crohns - YesClinical Trials
-
JRA Yes Clinical TrialsClinical Trials
Clinical Trials
Psoriatic arthritis
Yes Clinical Trials - -
Ankylosing Spondylitis
Yes Clinical TrialsClinical Trials
-

Kavanaugh A, Cohen S, Cush J
Inhibitors of tumor necrosis factor (TNF) in Rheumatoid Arthritis: Will that dog hunt? J Rheumatol 1998;25:2049

Global Safety and Efficacy of Etanercept in Global Safety and Efficacy of Etanercept in RARA
Klareskog, L, Moreland L, Cohen S. ACR 2002Klareskog, L, Moreland L, Cohen S. ACR 2002
Early RA (U.S.)Advanced RA (U.S.)Advanced RA (Europe)
Months
Reason: Loss of efficacy 8 %Adverse event 9 %Patient decision 5 %Protocol issues 2 %Lost to follow up 1 %Other 3 %Total 29%
0
20
40
60
80
100
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51
% R
em
ain
ing
on
Stu
dy
DiscontinuationsDiscontinuations~80%

DMARD Durability in RA DMARD Durability in RA PatientsPatients
DMARD Durability in RA DMARD Durability in RA PatientsPatients
Pincus T, et al. J Rheumatol. 1992;19:1885–1894.Pincus T, et al. J Rheumatol. 1992;19:1885–1894.
Azathioprine (n = 56)
Hydroxychloroquine(n = 228)
Methotrexate (n = 253)
Oral gold (n = 84)
Parenteral gold (n = 269)
Penicillamine (n = 193)
1.01.0
0.80.8
0.60.6
0.40.4
0.20.2
00
00 1010 2020 3030 4040 5050 6060
MonthsMonths
Est
imat
ed C
on
tin
uat
ion
Est
imat
ed C
on
tin
uat
ion

*paired-rank sum` test (n=68)
Withdrawal of Methotrexate and PrednisoneWithdrawal of Methotrexate and PrednisoneChange at 3 YearsChange at 3 Years
0
5
10
15
20
Mean
MTX
d
ose (
mg
/wk)
Baseline Year 3
17.6
9.3
p<0.001*
0
5
10
Baseline Year 3M
ean
Pre
din
son
e
dose (
mg
/d)
6.4
2.3
p<0.001
Methotrexate Prednisone
Increased 3% 3%
Decreased or D/C
68% 85%
Discontinued 39% 59%
MTX Prednisone

TNF Antagonists: TNF Antagonists: Other Indications and Clinical Other Indications and Clinical
InvestigationsInvestigations
TNF Antagonists: TNF Antagonists: Other Indications and Clinical Other Indications and Clinical
InvestigationsInvestigationsConfirmed Efficacy in
Trials► Crohn’s disease ► Spondyloarthropathies
Psoriatic arthritisPsoriasisAnkylosing spondylitis
► Juvenile rheumatoid arthritis
► Adult Still’s disease
Under Investigation► Vasculitis: Wegener’s, GCA, PAN► Scleroderma► Graft-versus-host disease► Inflammatory myositis► Interstitial lung disease► Sjögren’s syndrome► Inflammatory eye and ear disease► Asthma► Hepatitis C► Sarcoidosis► Behçet’s syndrome► Pyoderma gangrenosum

Psoriatic Arthritis: Improved Psoriatic Arthritis: Improved Skin LesionsSkin Lesions
12 Weeks12 WeeksBaselineBaseline
Elbow of patient 577; 50% improvement in target lesion.Elbow of patient 577; 50% improvement in target lesion.

Nail Responses with Etanercept
Baseline
Week 8 Week 12
Week 2

Cytokine Signaling Pathways Cytokine Signaling Pathways Involved in RAInvolved in RA
Cytokine Signaling Pathways Cytokine Signaling Pathways Involved in RAInvolved in RA
Choy EH, Panayi GS. N Engl J Med. 2001;344:907–916.Choy EH, Panayi GS. N Engl J Med. 2001;344:907–916.
TNFIL-1IL-6
IFNIL-12
IL-4IL-10
Macrophage
RF
IL-4IL-6
IL-10Plasmacell
B cell
Interferon
Th0
Th2
Synovium
OPGL
CD4 + T cell
CD69CD11
CD11CD69
Osteoclast FibroblastChondrocyte
Production of metalloproteinases andother effector molecules
Migration of polymorphonuclear cells
Erosion of bone and cartilage

ProinflammatoryTGF
MMPs
TIMPs
sTNFR, IL-4, IL-10IL-11, IL-13, IL-18 BP
Adapted from Arend WP. Arthritis Rheum. 2001;45:101–106.Adapted from Arend WP. Arthritis Rheum. 2001;45:101–106.
Autoimmune diseases
-Anti-inflammatory
IL-1RasIL-1RIIIL-1 RaMAb to IL-6RMAb to TNF
IL-1, TNFGM-CSF, IFNIL-6, IL-8IL-15, IL-16IL-17, IL-18

Key Actions Attributed to TNFKey Actions Attributed to TNF
TNFTNF(VEGF)

Adapted with permission from Choy EH, Panayi GS. N Engl J Med. 2001;344:907–916.
Inhibition of CytokinesInhibition of Cytokines
Activation ofanti-inflammatory pathways
Anti-inflammatorycytokineSuppression ofinflammatorycytokines
Neutralization of cytokines
Soluble receptor
Monoclonal antibody
No signal
Receptor blockade
Monoclonal antibody
Receptor antagonist
No signal
Inflammatory cytokine
Normal interaction
Cytokine receptorInflammatory signal


TNF AntagonistsTNF Antagonists
infliximabetanercept
adalimumab
Murine sequences
Human sequences
nerelimomabCDP-571
afelimomabCDP-870
PEG

Evolution of TNF Blocking TherapiesEvolution of TNF Blocking Therapies
*Some patients not taking concomitant MTX may derive additional benefit fromincreasing the dosing frequency of adalimumab to 40 mg every week*Some patients not taking concomitant MTX may derive additional benefit fromincreasing the dosing frequency of adalimumab to 40 mg every week
Etanercept Infliximab Adalimumab
Characteristic (ENBREL) (REMICADE) (HUMIRA™)
Class sTNFR TNF MAb TNF MAb
Construct Recombinant Chimeric MAb Recombinant
fusion protein human MAb
Half-life 4 days 8–10 days 10–20 days
Binding target TNF/LT TNF TNF
Administration 25 mg 3–10 mg/kg 40 mg
SC IV with MTX SC
Twice weekly Every 4–8 weeks Every other week*
Etanercept Infliximab Adalimumab
Characteristic (ENBREL) (REMICADE) (HUMIRA™)
Class sTNFR TNF MAb TNF MAb
Construct Recombinant Chimeric MAb Recombinant
fusion protein human MAb
Half-life 4 days 8–10 days 10–20 days
Binding target TNF/LT TNF TNF
Administration 25 mg 3–10 mg/kg 40 mg
SC IV with MTX SC
Twice weekly Every 4–8 weeks Every other week*

Synthesis and Actions of TNFSynthesis and Actions of TNF

Human (IgG)
Mouse(Binding Site for TNF)
Knight DM, et al. Mol Immunol. 1993; 30(16):1443-53.
Chimeric (mouse/human) IgG1 monoclonal antibody
Binds to TNF with high affinity and specificity
Chimeric A2 (cA2) Monoclonal AntibodyChimeric A2 (cA2) Monoclonal Antibody
InfliximabInfliximab

Mechanisms for Antibody Neutralization of TNFMechanisms for Antibody Neutralization of TNF

Effect of Anti-TNF Antibody on Established Collagen-Induced Arthritis in Mice
Effect of Anti-TNF Antibody on Established Collagen-Induced Arthritis in Mice
* p < 0.05 vs. control Indicates injections
Adapted from Williams RO, et al. Proc Natl Acad Sci. 1992; 89:9784-88.
Effect on Clinical ProgressionEffect on Clinical Progression

Inhibitory Effect of Infliximab on Synovial Cell IL-1 Production
Inhibitory Effect of Infliximab on Synovial Cell IL-1 Production
Brennan FM, et al. Lancet. 1989; ii:244-47. Haworth C, et al. Eur J Immunol. 1991; 21:2575-79.Butler D, et al. Eur Cytokine Network. 1995; 6:225-30.

Infliximab (Anti-TNF mAb) in Patients with Active RA
Infliximab (Anti-TNF mAb) in Patients with Active RA
Paleolog EM, et al. Arthritis Rheum. 1995; 38 (suppl.):Abstract S757.
Serum VEGF and Serum E-selectinSerum VEGF and Serum E-selectin

Binding Characteristics: TNF Inhibitors
Etanercept Infliximab Adalimumab
Association Rate (Ka)
7.9 x 106 M-1 Sec-1 1.4 x 106 M-1 Sec-1 1.9 x 105 M-1 Sec-1
Dissociation Rate (Kd)
2.4 x 10-4 Sec-1 2.7 x 10-4 Sec-1 8.8 x 10-5 Sec-1
Affinity Constants (Ka)
33.9 x 109 M-1 5.8 x 109 M-1 2.2 x 109 M-1

Infliximab IV: 9.5 Day Half-Infliximab IV: 9.5 Day Half-LifeLife
Percent of Maximum Serum Concentration Percent of Maximum Serum Concentration at Steady Stateat Steady State
002020404060608080
100100120120
00 6060 120120 180180 240240
DaysDays
Dosed every 8 weeksDosed every 8 weeks
55-fold Variation55-fold Variation
1.81%1.81%
%%

Adalimumab SQ: 14 Day Adalimumab SQ: 14 Day Half-LifeHalf-Life
Percent of Maximum Serum Concentration atPercent of Maximum Serum Concentration at Steady StateSteady State
00
5050
100100
150150
00 2828 5656
DaysDays
Dosed every 2 weeksDosed every 2 weeks
1.5-fold Variation1.5-fold Variation
%%
1414 4242

Etanercept SQ: 4.8 Day Half-Etanercept SQ: 4.8 Day Half-LifeLife
Percent of Maximum Serum Concentration atPercent of Maximum Serum Concentration at Steady StateSteady State
00
5050
100100
150150
00 3030 6060
DaysDays
Dosed twice a weekDosed twice a week
1.5-fold Variation1.5-fold Variation
%%

Safety Considerations With Safety Considerations With BiologicsBiologics
Safety Considerations With Safety Considerations With BiologicsBiologics
► Serious infections
► Opportunistic infections (TB)
► Malignancies
► Demyelination
► Hematologic abnormalities
► Administration reactions
► Congestive heart failure
► Autoantibodies and lupus

TOTAL Opportunistic InfectionsTOTAL Opportunistic InfectionsEtanercept Infliximab Adalimuma
b
# Exposed 130,000 365,000 2468
M. Tuberculosis 38 277 13
(%US/%EU) (32/68) (31/69) (23/77)
Extrapulmonary/miliary
52% 30-45% 40%
Pneumocystis carnii 4 38 -
Histoplasmosis* 1 30 3
Listeriosis 2 28 -
Atypical mycobacteria
10 26 1
Aspergillus 5 24 2
Cytomegalovirus 5 16 -
Systemic Candidiasis
7 13 -
Others Crypto3, sporo1
Cocci 13 Nocardia 1

TNF and Mycobacterial TNF and Mycobacterial InfectionInfection► Active TB arises in 10% of patients infected
► 1/3 of world infected with m.Tbc► Many patients develop latent Tb harboring dormant by
viable tubercle bacilli► Nitric oxide & TNF (less so IL-1) play an essential role:
activation of macrophages and granuloma formation resulting in containment of persistent Tb infection
► Animal models, TNF inhibition fatal reactivation of latent Tb
► TNF deficient mice: resistant to endotoxin, succeptable to Candida albicans, Listeria monocytogenes, M. TB
► Anti-TNF therapy is anti-granulomatous therapy! (Tbc cases, Sarcoid, Wegeners, pyoderma gangr., etc)

Tbc – Differences between TNF Tbc – Differences between TNF inhibitorsinhibitors
Infliximab Etanercept
Pharmacokinetic(1/2 life)
210 hrs 102 hrs
Off Rate Slow Fast
Lymphotoxin inhibition
None Yes
Apoptosis Yes No
Cell Lysis in vitro Yes No
Age > 65 yrs 42 % <25%
Dose escalation 1/3 dose>90% 1.6 vials per
week

Tuberculosis & TNF Tuberculosis & TNF AntagonistsAntagonists
►Patients should be evaluated for latent TB infection with a tuberculin skin test prior to initiation of TNF antagonist therapy1
►Obtain CXR? Not Routinely advocated in USA If PPD positive If Signs/Sxs presentRecent/known TB Contact
►If latent TB: initiate INH prior to or with TNF inhibitor therapy
►If active TB infection, treat 4 drugs, delay intiation of TNF inhibitor therapy1Furst, et al, Ann Rheum Dis, 2002;61:(Suppl II):ii-ii7

TNF Inhibitors & Antibody TNF Inhibitors & Antibody Formation Formation Infliximab Etanercept
► ANA 22,43,63% 11%► dsDNA 8,14,10,16 4,7,9,15%► Ab to Rx HACA 8.3,17,25,50% < 1%► Drug-induced lupus 4 pts (0.2%) 4 pts +► Etiology ? IL-10?► HACA: directed against murine component
Crohns; 13% HACA+ > more likely to have infusion rxn Lower HACA levels: MTX, 6MP, AZA; higher dose (10mg)Maini’99 1mg 3mg 10mg
-MTX 53% 21% 7%+MTX 15% 7% 0%
HACA
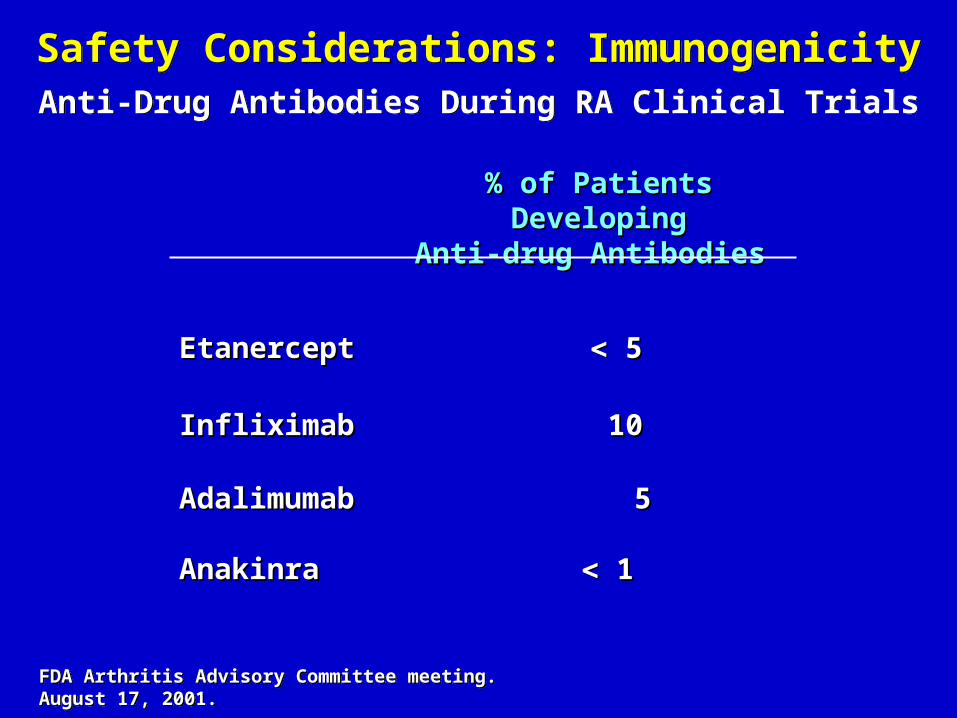
Safety Considerations: ImmunogenicityAnti-Drug Antibodies During RA Clinical Trials
Safety Considerations: ImmunogenicityAnti-Drug Antibodies During RA Clinical Trials
% of Patients Developing% of Patients DevelopingAnti-drug AntibodiesAnti-drug Antibodies
EtanerceptEtanercept 55
InfliximabInfliximab 1010
AdalimumabAdalimumab 55
AnakinraAnakinra 11
FDA Arthritis Advisory Committee meeting. August 17, 2001.FDA Arthritis Advisory Committee meeting. August 17, 2001.

Safety Issue:Safety Issue:Administration ReactionsAdministration Reactions
Injection-site reactions Etanercept 37% <2%
Anakinra 71% 7% Adalimumab 18.5% 0.3% Infliximab 22% 1.9%
Enbrel® (etanercept) [package insert]. 2002; Remicade® (infliximab) [package insert]. 2002; Kineret™ (anakinra) [package insert]. 2002; Keystone E et al. Ann Rheum Dis. 2001;60 (suppl 1):67. [Abstract]; van de Putte LBA et al. Ann Rheum Dis. 2002;61(suppl 1):168. [Abstract]; Schiff M et al. Ann Rheum Dis. 2002;61(suppl 1):169. [Abstract]
Incidence D/C
Infusion reactions


Autoantibodies and TNF InhibitorsAutoantibodies and TNF Inhibitors
ANA (+)
dsDNA(+)
Drug-induced lupus
RA 30-40% 0-4% 0
Etanercept 11% 15% 4
Infliximab 62% 15% 6
Adalimumab
12.9% 5.6% 1
►PreScreen/Monitoring ANA & dsDNA Not Necessary!►Safe to use TNF inhibitors in ANA+ RA patients►Caution with lupus like patients (Thalidomide used in LE)
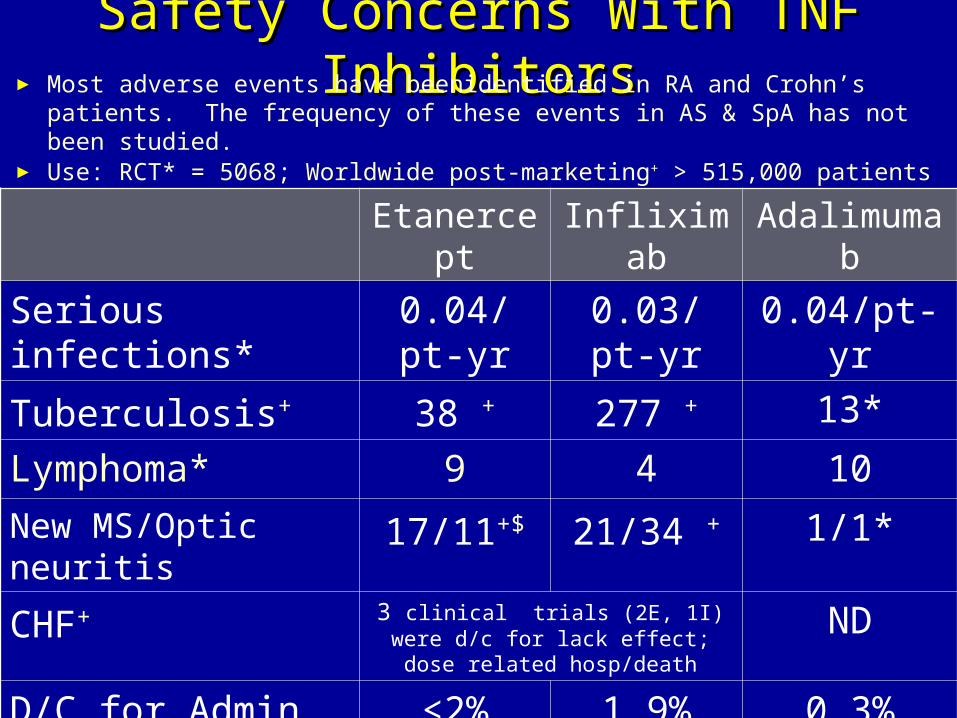
Safety Concerns With TNF Safety Concerns With TNF InhibitorsInhibitors► Most adverse events have beenidentified in RA and Crohn’s patients.
The frequency of these events in AS & SpA has not been studied.► Use: RCT* = 5068; Worldwide post-marketing+ > 515,000 patients
Etanercept
Infliximab Adalimumab
Serious infections*
0.04/pt-yr
0.03/pt-yr
0.04/pt-yr
Tuberculosis+ 38 + 277 + 13*
Lymphoma* 9 4 10New MS/Optic neuritis
17/11+$ 21/34 + 1/1*
CHF+ 3 clinical trials (2E, 1I) were d/c for lack effect; dose related
hosp/death
ND
D/C for Admin. Rxn*
<2% 1.9% 0.3%
(+)dsDNA* 15% 15% 5.7%
Drug induced Lupus
4 pts + 4 pts+ 1 pt.*

The TNF MarketThe TNF Market
►Estimates are that 10-20% of patients are on TNF inhibitors
►Infliximab Sales grew by >316% from 1999 to 2000
►Feb 2002 15% of etanercept Rxs by PCP ►2003 TNF inhibitors on the market in 2003
Infliximab, etanercept, adalimumab►Potential Market = $21 Billion►Current Market ~ $2 Billion►2004 Market Estimated @ $4 billion in sales

Safety EfficacyQOL
Less Data More Data
ComfortDiscomfort
Decision Making and Newly Released Drugs
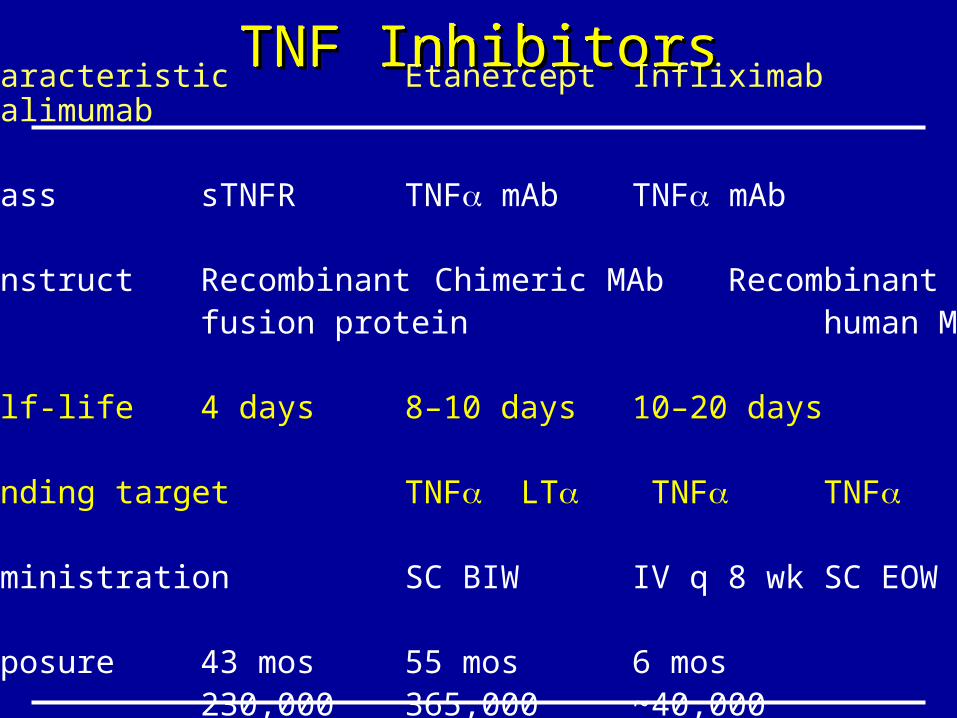
TNF InhibitorsTNF InhibitorsTNF InhibitorsTNF InhibitorsCharacteristic Etanercept Infliximab Adalimumab
Class sTNFR TNF mAb TNF mAb
Construct Recombinant Chimeric MAb Recombinantfusion protein human MAb
Half-life 4 days 8–10 days 10–20 days
Binding target TNF LT TNF TNF
Administration SC BIW IV q 8 wk SC EOW
Exposure 43 mos 55 mos 6 mos230,000 365,000 ~40,000

Comparison of New AgentsComparison of New AgentsEtanerceptEtanercept InfliximabInfliximab AnakinraAnakinra AravaArava
AdministrationAdministration BIW, SCBIW, SC q4-8 wk IVq4-8 wk IV QD, SCQD, SC POPOwith MTXwith MTX
Half-lifeHalf-life 102 hrs102 hrs 210 hrs210 hrs 5.9 hr 5.9 hr 15-18d15-18d
IndicationsIndications RA, JRA, ERARA, JRA, ERA RA, CrohnsRA, Crohns RARA RARA
ACR20ACR20 60-73%60-73% 42-80%42-80% 38-49%38-49% 50-52%50-52%
ACR70ACR70 10-15%10-15% 10%10% 10%10% 15%15%
*Practice20*Practice20 >90%>90% >90%>90% ???? 60*60*
*Born Again RA?*Born Again RA? 60-75%60-75% 60-75%60-75% (5%)(5%) 5%5%
CostsCosts $15,436$15,436 $13940-30287$13940-30287 $12,800$12,800 $2938$2938

TNF Antagonists: Relative TNF Antagonists: Relative ContraindicationsContraindications
TNF Antagonists: Relative TNF Antagonists: Relative ContraindicationsContraindications
►SLE
►Multiple sclerosis, optic neuritis
►Current active serious infections
►Chronic/recurrent infections
► Immunosuppression
►History of TB or positive PPD (untreated)
►Congestive heart failure