The PHARLAP Study - Wellington Intensive Care Unitwellingtonicu.com/Data/Trials/PHARLAP.pdf · The...
39
The PHARLAP Study
Transcript of The PHARLAP Study - Wellington Intensive Care Unitwellingtonicu.com/Data/Trials/PHARLAP.pdf · The...
The PHARLAP Study
A Multi-centre RCT ofAn Open Lung Strategy including Permissive Hypercapnia, Alveolar
Recruitment and Low Airway Pressure in
The PHARLAP Study Investigators for the ANZICS Clinical Trials Group

PHARLAP Study Aim
To compare
• PHARLAP Open Lung Ventilation PH Permissive Hypercapnia AR Alveolar Recruitment (staircase RM) LAP Low Airway Pressures
With
• Standard mechanical ventilation (ARDSnet)

PEEP + Recruitment Trials ALVEOLI LOVS EXPRESS
Number 549 985 768
PEEP 8.3→13.2 9→14 7→14
Plateau press 24→27 24→28 21→28
Recruitment 35-40 for 30 (80 pt) 40 for 40 No RM
Mortality 28%→25% 40%→36% 39%→36%
P value not significant not significant not significant

Meta-analyses
ALI/Hi'PEEP' Number' Hosp'Mortality' P'value
! ALI!(all)! 2272! 35.2→32.9%! 0.25
! ARDS! 992! 39.1→34.1%! 0.05
! No!ARDS! 404! 19.2→27.2%! 0.07
! ! ! ! Briel JAMA 2010;303:865-83
Amato'2'unpublished'meta=analysis' Mortality'' P'value

Meta-analyses
' Amato'LOVS're=analysis' Mortality'' P'value'
' ' RM,!Hi!PEEP,!Compl!↑! ↓!! !<0.05!! RM,!Hi!PEEP,!Compl!↓!! ↑!!
' ALI'Recruitment' P/F' Mortality
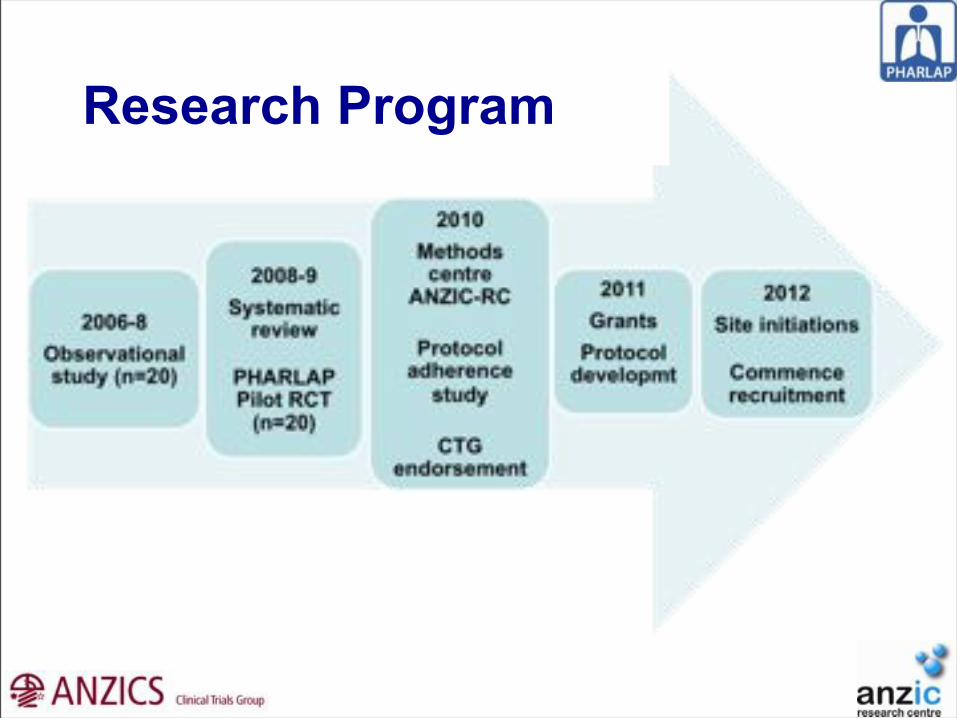
Research Program

PHARLAP Pilot Study

Pilot Study
Hodgson C, Nichol A, Tuxen D, Davies A, Cooper J, et al.
!PaO2/FIO2!!(P=0.005) !Compliance!!!!(P<0.001)

Pilot Study
PHARLAP
(10!pa>ents)
Control
(10!pa>ents)P!value
Hospital!mortality 3 2 0.61
ICU!LOS!(days) 9.9!(5.6814.8) 16.0!(8.1819.3) 0.19
Hospital!LOS!(days) 17.9!(13.7834.5) 24.7!(20.5839.8) 0.16
Dura>on!of!MV!(hrs) 180!(878298) 341!(1318351) 0.13
Rescue!Therapies 0 2 0.46
SOFA!(day!7) 8.6!±!0.3 8.4!±!0.6 0.27
Barotrauma 0 0 1.0
Hodgson C, Nichol A, Tuxen D, Davies A, Cooper J, et al.

Pilot Study
PHARLAP
(10!pa>ents)
Control
(10!pa>ents)P!value
Hospital!mortality 3 2 0.61
ICU!LOS!(days) 9.9!(5.6814.8) 16.0!(8.1819.3) 0.19
Hospital!LOS!(days) 17.9!(13.7834.5) 24.7!(20.5839.8) 0.16
Dura>on!of!MV!(hrs) 180!(878298) 341!(1318351) 0.13
Rescue!Therapies 0 2 0.46
SOFA!(day!7) 8.6!±!0.3 8.4!±!0.6 0.27
Barotrauma 0 0 1.0
Hodgson C, Nichol A, Tuxen D, Davies A, Cooper J, et al.

'Research Question
In ARDS patients, Does the Open Lung Strategy Increase ventilator free days (VFDs) at day 28 When compared with standard mechanical ventilation?

Methods
• Phase II RCT
• 340 patients
• ARDS < 48 hrs (but < 5 days of MV)

SitesAlbury WodongaAlfredAustinBendigoBlacktownBox HillCanberraEpworth RichmondFlindersGeelongGold CoastJohn HunterLyell McEwinNambour
NorthernPrince CharlesRoyal DarwinSir Charles GairdnerSt GeorgeSt Vincent’s SydneyWesternWoolongong
Christchurch CVICU AucklandDCCM AucklandMiddlemoreWellington

Study Leadership
Project Manager Victoria Bennett
Management Committee
Andrew Davies (Co-Chair) Alistair Nichol (Co-Chair) Michael Bailey Andrew Bersten Jamie Cooper John Fraser Lisa Higgins Carol Hodgson Shay McGuinness Lynne Murray Rachael Parke David Tuxen

Outcome Measures
Primary – VFD at day 28
Secondary Physiological/inflammatory
- Oxygenation, lung compliance- IL-6/IL-8 in blood/tracheal aspirates
Clinical- Safety, LOS (ICU, hospital), mortality,- Use of rescue therapies- HRQoL 6mths
Economic

Mechanical Ventilation:• VCV assist control ventilation (or SIMV if required)• Tidal volumes ≤ 6 mls/kg PBW• Plateau pressures ≤ 30 cmH2O • RR < 35 breaths/min• Early spontaneous breathing using PSV allowed (careful tidal volumes)• Neuromuscular blockers if required
Oxygenation: • Target oxygenation SpO2 90-95% PaO2 60-80 mmHg• Oxygenation maintainenance using the PEEP/FiO2 Chart
Management of Acidosis and Hypercapnia: • pH goal for control patients: pH 7.30-7.45
FiO2 0.3 0.4 0.4 0.5 0.5 0.6 0.7 0.7 0.7 0.8 0.9 0.9 0.9 1.0
PEEP 5 5 8 8 10 10 10 12 14 14 14 16 18 18V24
Control Group Strategy

Combined Open Lung Procedure (up to 5 days):• PCV• Staircase recruitment manoeuvre• PEEP titration manoeuvre• Brief recruitment manoeuvre
Ongoing PHARLAP mechanical ventilation:• Tidal volume: 4-6 ml/kg PBW • Total pressure (ie. inspiratory pressure + PEEP): 25-28 cmH2O• Breath rate: ≤ 35 breaths/minute• Leave PEEP on optimal setting unless weaning or a problem• Target oxygenation SaO2 90-95% (daily precise target) PaO2 60-80 mmHg• Brief recruitment manoeuvre if SaO2 ≤ 2% below the target
Permissive hypercapnia: • Breath rate aiming for a low pH in the range of 7.15-7.30• Tidal volume can be reduced• Hypercapnia should be tolerated if pH ≥ 7.15
PHARLAP Group Strategy






Control Group:If PaO2 < 60 mmHg or SaO2 < 90% on 4 end columns
PHARLAP Group:If PaO2 < 60 mmHg or SaO2 < 90% and brief recruit man done/contra-indicated
Hypoxaemic rescue therapy:• Inhaled NO• Inhaled prostacyclin• Prone positioning• High frequency oscillation• ECMO
• Choice depends on local practice, availability, feasibility• No recruitment manoeuvres in control group unless no feasible alternative
Severe Hypoxaemia

• MAP < 60 mmHg despite attempts to augment (vasopressor/fluid)
• Active air leak through intercostal catheter
• Pneumatoceles, subpleural cysts, pericardial/mediastinal emphysema on CXR
• Subcutaneous emphysema not related to trauma, surgery or ICU procedures
• SVT with MAP < 70 mmHg or Any VT
Recruitment Manoeuvre Contra-indications
• Day 1 fluid balance aim is what best suits patient’s clinical state
• From Day 2 on, ignore Day 1 and aim to avoid cumulative positive fluid balance
• Correct unplanned positive fluid balance with fluid restriction +/- diuretics
• Monitor renal function carefully
• For hypotension during COLP, preference is vasopressors, then IV fluid
Fluid Management

• Directional tip for R or L lung samples
• Can be performed bedside in minutes
• Maintains PEEP
• Features a soft, cushioned tip

Two sizes of KimVent BAL Caths
•13F is recommended for a size 7cm ETT and smaller
•16F is recommended for a size 7.5cm ETT and larger

Preparation
• Pre-oxygenate: FiO2 1.0 for 2 minutes
• Leave PEEP on current setting
• Draw up 60 ml of 0.9% saline (usually three 20 ml syringes)
• Prepare clean environment as per usual site practice for similar interventions
• Connect 0.9% saline syringe to upper port on 3 way tap and point off arrow to other port
• Ensure the blue locking device is open
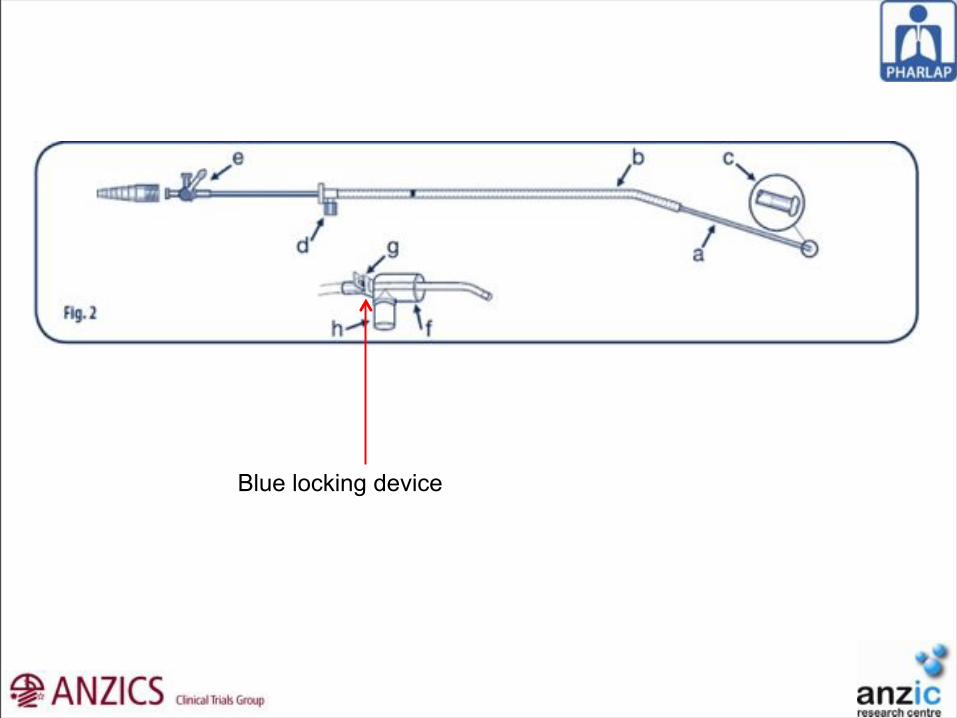
Blue locking device

Introduce the BAL catheter by forwarding the catheter through connector B so that the catheter tip protrudes through the connector before connecting to the endotracheal tube
Disconnect the in-line suction and ventilator and attach connector B to the endotracheal tube (Fig. 1) – the catheter should be 2 cm into the endotracheal tube.
Reconnect the ventilator tubing to connector B.

Advance catheter until the numbers on the catheter match the numbers on the endotracheal tube
At this point the catheter is located exactly at the distal point of the endotracheal tube

Ensure the white oxygen port on the catheter is orientated to the right.
This means that the internal catheter will be angled towards the right main bronchus.
Forward the entire catheter another 5 cm and check that the white oxygen port remains orientated to the right side
Flush the catheter with 5 ml 0.9% saline. Lock the blue locking device
Gently advance the inner catheter until a spongy resistance is noted (ie. the catheter is appropriately wedged in a distal bronchus)

• Inject first syringe of 0.9% saline, followed by 5 ml air
• With same syringe, gently hand aspirate BAL, then do same with subsequent syringes
via the 3 way port until a minimum volume of 10 ml is obtained
• Withdraw inner suction catheter until solid black mark outside connector to ETT
• Unlock blue locking device. Withdraw entire catheter
• Reconnect in-line suction catheter and original connectors
BAL Sample Collection
• Combine collected BAL fluid from each syringe into sterile container
• Label as BAL for PHARLAP study
• If patient in PHARLAP group, followed with combined open lung
procedure or a brief recruitment manoeuvre as appropriate
BAL Sample Collection


Something to think about

474 pts with severe and persistent ARDS 27 ICUs
Prone (16 hrs/day)
Vs
Supine
PROSEVA Study
Guerin C, et al. ESICM 2012

474 pts with severe and persistent ARDS 27 ICUs
Prone (16 hrs/day)
Vs
Supine
PROSEVA Study
0
12.5
25.0
37.5
50.0
28 day mortality 90 day mortalityProneSupine
Guerin C, et al. ESICM 2012