
THE PATHOLOGY OF EMPHYSEMA
9
POSTGRAD. MED. J. (1965), 41, 392 THE PATHOLOGY OF EMPHYSEMA J. GOUGH, M.D., F.C. Path. Welsh National School of Medicine, Cardiff. IN THIS Cardiff Symposium of the Postgraduate Medical Journal, I should first explain why the Pathology Department of the Welsh National School of Medicine became interested in emphysema as one of its main subjects for research. It arose out of a study of thousands of respiratory cripples in the coal mining industry. In the early part of this century coal miners were a healthy population apart from accidents, but by the third decade it was evident that respiratory disease of serious proportions was arising. At first it was thought that this was silicosis (Cummins and Sladden, 1930), affecting those miners who were exposed to rock dust as well as to coal. It soon became evident, however, that although there were cases of silicosis in those who worked especially on rock, there was a far higher incidence of respiratory troubles in miners who worked on the coal seams and in coal trimmers who load coal into ships. The name "coal worker's pneumoconiosis" was applied and is now accepted in law. A study of the lungs of miners showed that there are two quite separate forms of pneumoconiosis (Gough, 1947). The one is a massive fibrosis while the other consists of discrete nodules of coal with comparatively little fibrosis but which subsequently become surrounded by a characteristic emphysema now known as "focal dust emphysema". A tech- nique was evolved to demonstrate this emphysema more effectively. This is the whole lung paper section method devised by Gough and Wentworth (1957/58; 1960). It is carried out on lungs fixed in expansion. The large section method was next used for a study of respiratory diseases of the general population and it revealed (Gough, 1952) two fundamen- tally different forms of emphysema. In the one there was a selective involvement of the centres of the lung lobules. This is known as central or centrilobular emphysema. In the other form there was no selection of the kind of air spaces dilated and since this lesion was not based on the lobule but often affected the greater part of both lungs it was referred to as generalised but this name was not sufficiently precise and the condition is now known as "'panacinar" or "panlobular". In view of the common use of the terms lobule and acinus in the classification of emphysema, it is necessary to define them. Anatomy The Lobule (also called the secondary lobule of Miller) The lung lobule is the smallest component which is bounded by fibrous tissue septa. This is the definition given by the Basle Convention and is used by anatomists, and is an important anatomical structure for reference. The lobules are 1-2 cm. in diameter. Their outlines are not easily seen in some parts of the lungs but those of us who have studied coal miners' lungs are very familiar with the lobular structure because in many miners the fibrous tissue septa become impregnated with coal (Fig. 1). The lobules tend to be pyramidal with their apices directed towards the hilum. They have their own air and blood supply and lymphatic drainage. They are virtually miniature lungs, a feature which becomes important in the correlation of emphysema with disturbed function because uneven functional capacity in different units or parts of the lung is readily brought out by function tests and a study of the pathology shows that some lobules may be severely affected while neighbouring ones may be virtually normal. The Acinus It is much more difficult to define the acinus because different authors have used this term in. different ways. In classifying the different types of emphysema a Ciba Foundation Symposium (1959) used 'acinus' for the unit of respiratory tissue distal to the terminal bronchiole. All the components in the acinus so defined bear alveoli. This acinus consists of respiratory bronchioles, alveolar ducts, alveolar sacs and alveoli. The Ciba Symposium recommended that the classification of emphy-
Transcript of THE PATHOLOGY OF EMPHYSEMA

POSTGRAD. MED. J. (1965), 41, 392
THE PATHOLOGY OF EMPHYSEMA
J. GOUGH, M.D., F.C. Path.Welsh National School of Medicine, Cardiff.
IN THIS Cardiff Symposium of the PostgraduateMedical Journal, I should first explain why thePathology Department of the Welsh NationalSchool of Medicine became interested inemphysema as one of its main subjects forresearch. It arose out of a study of thousandsof respiratory cripples in the coal miningindustry. In the early part of this century coalminers were a healthy population apart fromaccidents, but by the third decade it wasevident that respiratory disease of seriousproportions was arising. At first it was thoughtthat this was silicosis (Cummins and Sladden,1930), affecting those miners who were exposedto rock dust as well as to coal. It soon becameevident, however, that although there werecases of silicosis in those who worked especiallyon rock, there was a far higher incidence ofrespiratory troubles in miners who worked onthe coal seams and in coal trimmers who loadcoal into ships. The name "coal worker'spneumoconiosis" was applied and is nowaccepted in law. A study of the lungs ofminers showed that there are two quite separateforms of pneumoconiosis (Gough, 1947). Theone is a massive fibrosis while the other consistsof discrete nodules of coal with comparativelylittle fibrosis but which subsequently becomesurrounded by a characteristic emphysema nowknown as "focal dust emphysema". A tech-nique was evolved to demonstrate thisemphysema more effectively. This is the wholelung paper section method devised by Goughand Wentworth (1957/58; 1960). It is carriedout on lungs fixed in expansion. The largesection method was next used for a study ofrespiratory diseases of the general populationand it revealed (Gough, 1952) two fundamen-tally different forms of emphysema. In theone there was a selective involvement of thecentres of the lung lobules. This is known ascentral or centrilobular emphysema. In theother form there was no selection of the kindof air spaces dilated and since this lesion wasnot based on the lobule but often affected thegreater part of both lungs it was referred to
as generalised but this name was not sufficientlyprecise and the condition is now known as"'panacinar" or "panlobular". In view of thecommon use of the terms lobule and acinus inthe classification of emphysema, it is necessaryto define them.
AnatomyThe Lobule (also called the secondary lobuleof Miller)The lung lobule is the smallest component
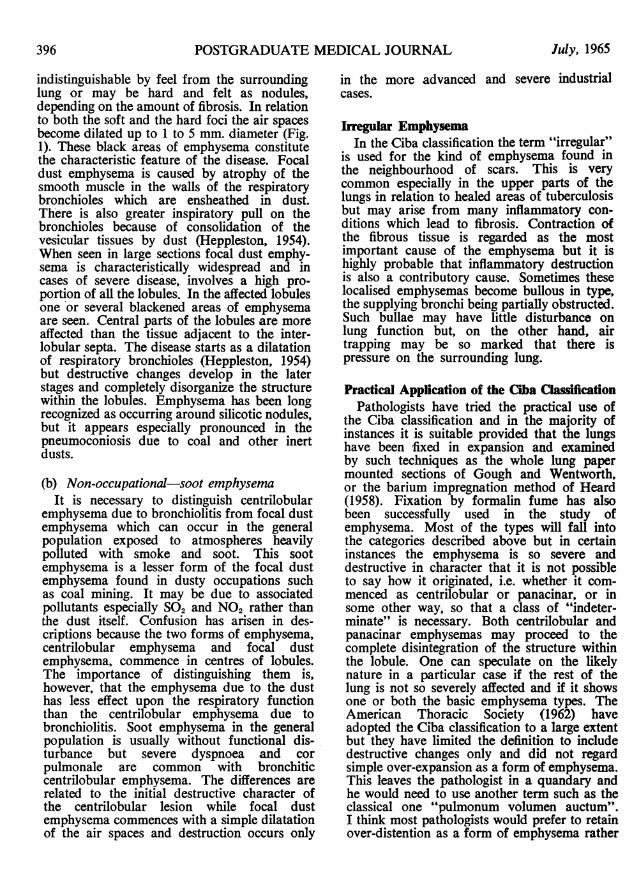
which is bounded by fibrous tissue septa. Thisis the definition given by the Basle Conventionand is used by anatomists, and is an importantanatomical structure for reference. The lobulesare 1-2 cm. in diameter. Their outlines are noteasily seen in some parts of the lungs but thoseof us who have studied coal miners' lungs arevery familiar with the lobular structure becausein many miners the fibrous tissue septa becomeimpregnated with coal (Fig. 1). The lobulestend to be pyramidal with their apices directedtowards the hilum. They have their own airand blood supply and lymphatic drainage. Theyare virtually miniature lungs, a feature whichbecomes important in the correlation ofemphysema with disturbed function becauseuneven functional capacity in different units orparts of the lung is readily brought out byfunction tests and a study of the pathologyshows that some lobules may be severelyaffected while neighbouring ones may bevirtually normal.
The AcinusIt is much more difficult to define the acinus
because different authors have used this termin. different ways. In classifying the differenttypes of emphysema a Ciba FoundationSymposium (1959) used 'acinus' for the unitof respiratory tissue distal to the terminalbronchiole. All the components in the acinusso defined bear alveoli. This acinus consistsof respiratory bronchioles, alveolar ducts,alveolar sacs and alveoli. The Ciba Symposiumrecommended that the classification of emphy-

July, 1965 GOUGH: Pathology of Emphysema 393
I
.:t
ij!
i.."·.:b...·.·i,·
·:·:
r
ir··:
:'%:·.i.·_.ilE...;.i.PPc.P.#a.':."-.;,e..b
·,.·
FIG. 1.-Lobules outlined by dust in the connectivetissue septa. In the centres of the lobules is anearly stage of focal dust emphysema. Air spacesat the periphery of the lobules are intact. x2.3.
sema should be based on pathological anatomybecause respiratory function tests and radiologyare not sufficiently reliable to warrant a preciseclassification at the present time. Function testsdo not distinguish the different varieties ofchronic non-specific obstructive lung diseases,emphysema, bronchitis and asthma withsufficient precision: improvements in this res-pect, however, are developing and combinedradiological, functional and anatomical classi-fications are appearing. It will be necessary,however, to study large series of cases wherethere is correlation of functional disturbancein life with the pathological anatomy beforethese classifications are acceptable. Limitingthe definition and classification, therefore,strictly to pathology, the Ciba Symposiumproposed the following: -"Emphysema is a condition of the lung
characterized by increase beyond the normalin the size of air spaces distal to the terminalbronchiole either from dilatation or fromdestruction of their walls."Emphysema can be diagnosed and classified
consistently only on preparations from lungsdistended and fixed before they are cut. Thesimplest technique is intrabronchial infusion offixative. In some cases identification of theanatomical origin of enlarged spaces mayrequire such techniques as the study of serialsections, or stereoscopic microscopy of lungslices.The term emphysema is restricted to dilata-
tion of air spaces distal to the terminalbronchiole in order to differentiate emphysemafrom dilatations which include structuresproximal to the terminal bronchiole, as invarious forms of honeycomb lung.
1. Unselective distribution beyond the terminalbronchiole (panacinar emphysema)(a) Dilatation alone (e.g. compensatory
emphysema and emphysema due topartial main bronchus obstruction).
(b) Destruction of the walls of air spaces(panacinar destructive emphysema).
2. Selective distribution beyond the terminalbronchiole.(i) Predominantly affecting respiratorybronchioles.(a) Dilatation alone (e.g. focal emphysema
due to dust).(b) Destruction of the walls of air spaces
(centrilobular emphysema).(ii) Predominantly affecting alveolar ductsand sacs.(a) dilatation alone.(b) destruction.
3. Irregular distribution beyond the terminalbronchiole (irregular emphysema).Of the five pathologists who took part in the
symposium one, Dr. L. McA. Reid, proposedan alternative arrangement of the various typesof emphysema but all the pathologists wereagreed what the types are. The difference ofopinion was whether the precise anatomicallocation should be the primary basis of theclassification, or whether destruction should bethe primary criterion. The following alternativearrangement of the classification was proposed: -1. Dilatation alone.
(a) Unselective distribution (compensatoryemphysema and emphysema due topartial main bronchus obstruction).
(b) Selective distribution predominantlyaffecting respiratory bronchioles (e.g.focal emphysema due to dust).
2. Destruction of the walls of air spaces.(a) Unselective distribution (panacinar des-
tructive emphysema).(b) Selective distribution predominantly
affecting respiratory bronchioles (cen-trilobular emphysema).
(c) Irregular distribution (irregular emphy-sema).
Centrilobular Emphysema (Gough, 1952;Leopold and Gough, 1957)
This is a common condition in the generalpopulation. The centrilobular origin of emphy-sematous spaces is best observed in lobuleswhich are not severely diseased. The changesare destructive even in the smallest lesions, andthe ragged air spaces at the centre contrastwith the normal pattern of lung tissue. A

394 POSTGRADUATE MEDICAL JOURNAL July, 1965
at:>
-
\ - a s S
. THK-W"Cj .~!./:._1:DU
- -'
..:
..
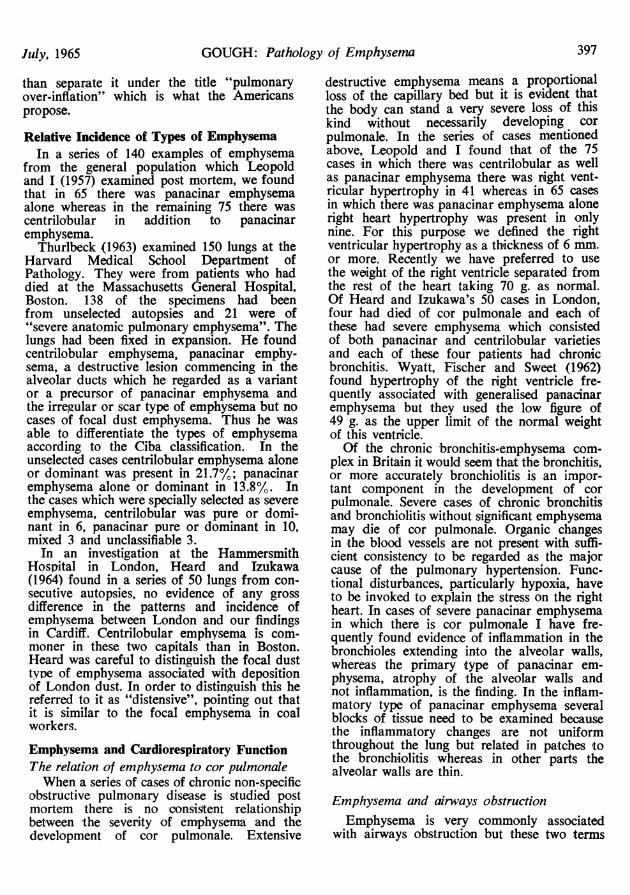
FIG. 2.-Diagram of a lobule showing the characteris-tics of centrilobular emphysema.T.B.-Terminal bronchiole.R.B. 1, 2 & 3-Three orders of respiratorybronchioles. x3.5 approximately.
mulberry-like cluster of emphysematous spacesdevelops (Fig. 2). The spaces become confluentas they enlarge. Carbon in amounts commonin the lungs of town-dwellers is collected aroundthe spaces and in their partitions, thus helpingto delineate the lesion but dust is not anessential component. The emphysematousciuster is marked off into loculi by partitionswhich do not, however, form completeseparations. These partitions radiate from onebronchiole which provides the airway to thecluster. This bronchiole is called the "sup-plying" bronchiole. Patent communicationsbetween the bronchioles and the emphysematousspaces are traceable in all lesions although thecalibre of these passages varies. The "sup-plying" bronchioles show histological changesof chronic inflammation and the inflammationhaving extended peripherally, centrilobularemphysema is one of the results due to breakageof the walls of respiratory bronchioles. Suchperipheral extension of inflammation may occurvery irregularly in the lung so that unaffected
lobules are contiguous with lobules showingcentrilobular emphysema. Spread of inflam-mation also leads to breakage of the partitionsradiating from respiratory bronchioles. In thenormal lung these partitions help keep openthe bronchioles to which they are attached.Rupture of the partitions causes the bronchiolesto collapse during expiration thus producingair trapping.Panacinar (syn. panlobular emphysema.Generalized emphysema)The panacinar type is conveniently classified
into sub-groups. One appears to be an atrophicprocess of unknown cause and this is calledprimary. The other is commonly associatedwith chronic bronchitis. Centrilobular andpanacinar emphysema often occur together inlungs showing chronic bronchitis.
(a) Primary typeIn this type the various air-containing spaces
in the acini enlarge, i.e. it is unselective andaffects respiratory bronchioles, alveolar ducts,alveolar sacs and alveoli. Not only does thelesion appear uniformly in the individual lobulesbut it is a condition which often affects alarge part of both lungs. Commonly the wholeof both lungs show the condition. It is for thisreason that I preferred originally to call it"generalized". It is a common disease in thegeneral population; not infrequently it is anincidental finding and may be an exaggerationof the ageing process, because from childhoodup to adult life the air spaces show a naturalincrease in size. One suspects, however, thatit may not be a simple ageing process becausemany old people, especially older women, showno sign of it. This difference in the sex incidencewould seem to suggest that the emphysematouschanges seen in old people's lungs are moreassociated with wear and tear and the effectsof disease rather than the mere passage of time.It should be pointed out, however, that thereare senile changes in the lungs which lead toreduced respiratory capacity but which are notemphysema. These changes are thought to berelated to the physico-chemical changes in theconnective tissues. (See Ageinp of the Lung,Ed. Cander, L., and Moyer, J. H., 1964).(b) Panacinar emphysema associated withchronic bronchitisSome of the most severe cases of chronic
non-specific obstructive lung disease consist ofchronic bronchitis and panacinar emphysema(Fig. 3). In these cases the inflammatorychanges extend to the smallest bronchioles and
July, 1965 GOUGH: Pathology of Emphysema 395
#i B .F' I'::.a.·. j,.·..aa.·..t.F . t··.FnS.W."s·".b* i;`.F.:"' :,·i1.41 ;u C:: :1 1:··9*·
:. )ii: ·.· r
1'7*·blii
ii I-a:
·::r;·..q·q $
f.P.;'
z.
I.ea;.. ..d..R.SSP'.31. TI.Ri. :IT
:r'··.g.q.,.t..,.E.:.C..lj.j·gg.·1., .j&· ....'9.;.i.s.B.!··g6id...E....;.i..·..%?'P'
%·i·.F.31.`p r .a.i
i:a::-.
t i
:·-
:.I
:*.·
:a:l
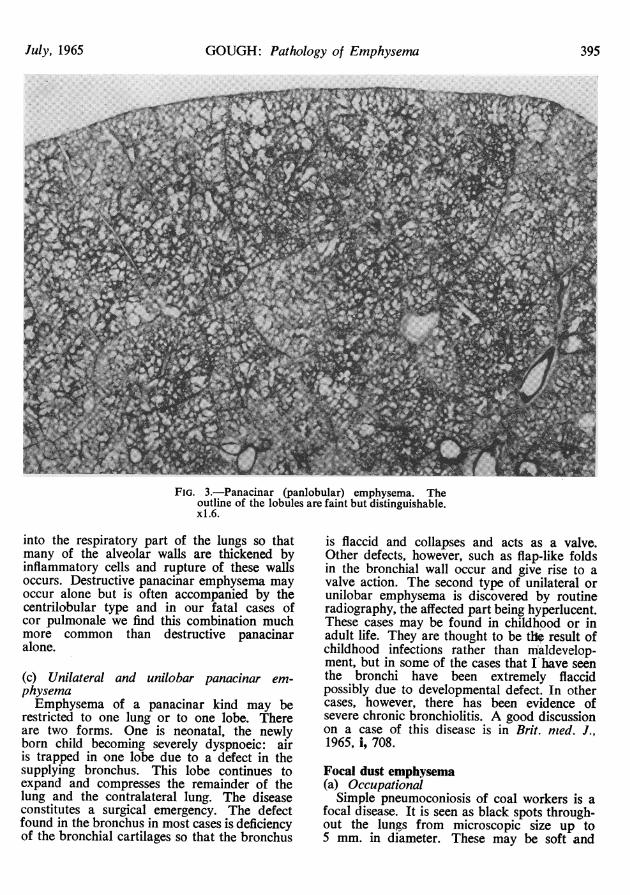
FIG. 3.-Panacinar (panlobular) emphysema. Theoutline of the lobules are faint but distinguishable.xl.6.
into the respiratory part of the lungs so thatmany of the alveolar walls are thickened byinflammatory cells and rupture of these wallsoccurs. Destructive panacinar emphysema mayoccur alone but is often accompanied by thecentrilobular type and in our fatal cases ofcor pulmonale we find this combination muchmore common than destructive panacinaralone.
(c) Unilateral and unilobar panacinar em-physemaEmphysema of a panacinar kind may be
restricted to one lung or to one lobe. Thereare two forms. One is neonatal, the newlyborn child becoming severely dyspnoeic: airis trapped in one lobe due to a defect in thesupplying bronchus. This lobe continues toexpand and compresses the remainder of thelung and the contralateral lung. The diseaseconstitutes a surgical emergency. The defectfound in the bronchus in most cases is deficiencyof the bronchial cartilages so that the bronchus
is flaccid and collapses and acts as a valve.Other defects, however, such as flap-like foldsin the bronchial wall occur and give rise to avalve action. The second type of unilateral orunilobar emphysema is discovered by routineradiography, the affected part being hyperlucent.These cases may be found in childhood or inadult life. They are thought to be the result ofchildhood infections rather than maldevelop-ment, but in some of the cases that I have seenthe bronchi have been extremely flaccidpossibly due to developmental defect. In othercases, however, there has been evidence ofsevere chronic bronchiolitis. A good discussionon a case of this disease is in Brit. med. J.,1965, i, 708.
Focal dust emphysema(a) Occupational
Simple pneumoconiosis of coal workers is afocal disease. It is seen as black spots through-out the lungs from microscopic size up to5 mm. in diameter. These may be soft and
POSTGRADUATE MEDICAL JOURNAL
indistinguishable by feel from the surroundinglung or may be hard and felt as nodules,depending on the amount of fibrosis. In relationto both the soft and the hard foci the air spacesbecome dilated up to 1 to 5 mm. diameter (Fig.1). These black areas of emphysema constitutethe characteristic feature of the disease. Focaldust emphysema is caused by atrophy of thesmooth muscle in the walls of the respiratorybronchioles which are ensheathed in dust.There is also greater inspiratory pull on thebronchioles because of consolidation of thevesicular tissues by dust (Heppleston, 1954).When seen in large sections focal dust emphy-sema is characteristically widespread and incases of severe disease, involves a high pro-portion of all the lobules. In the affected lobulesone or several blackened areas of emphysemaare seen. Central parts of the lobules are moreaffected than the tissue adjacent to the inter-lobular septa. The disease starts as a dilatationof respiratory bronchioles (Heppleston, 1954)but destructive changes develop in the laterstages and completely disorganize the structurewithin the lobules. Emphysema has been longrecognized as occurring around silicotic nodules,but it appears especially pronounced in thepneumoconiosis due to coal and other inertdusts.
(b) Non-occupational-soot emphysemaIt is necessary to distinguish centrilobular
emphysema due to bronchiolitis from focal dustemphysema which can occur in the generalpopulation exposed to atmospheres heavilypolluted with smoke and soot. This sootemphysema is a lesser form of the focal dustemphysema found in dusty occupations suchas coal mining. It may be due to associatedpollutants especially SO2 and NO2 rather thanthe dust itself. Confusion has arisen in des-criptions because the two forms of emphysema,centrilobular emphysema and focal dustemphysema, commence in centres of lobules.The importance of distinguishing them is,however, that the emphysema due to the dusthas less effect upon the respiratory functionthan the centrilobular emphysema due tobronchiolitis. Soot emphysema in the generalpopulation is usually without functional dis-turbance but severe dyspnoea and corpulmonale are common with bronchiticcentrilobular emphysema. The differences arerelated to the initial destructive character ofthe centrilobular lesion while focal dustemphysema commences with a simple dilatationof the air spaces and destruction occurs only
in the more advanced and severe industrialcases.
Irregular EmphysemaIn the Ciba classification the term "irregular"
is used for the kind of emphysema found inthe neighbourhood of scars. This is verycommon especially in the upper parts of thelungs in relation to healed areas of tuberculosisbut may arise from many inflammatory con-ditions which lead to fibrosis. Contraction ofthe fibrous tissue is regarded as the mostimportant cause of the emphysema but it ishighly probable that inflammatory destructionis also a contributory cause. Sometimes theselocalised emphysemas become bullous in type,the supplying bronchi being partially obstructed.Such bullae may have little disturbance onlung function but, on the other hand, airtrapping may be so marked that there ispressure on the surrounding lung.
Practical Application of the Ciba ClassificationPathologists have tried the practical use of
the Ciba classification and in the majority ofinstances it is suitable provided that the lungshave been fixed in expansion and examinedby such techniques as the whole lung papermounted sections of Gough and Wentworth,or the barium impregnation method of Heard(1958). Fixation by formalin fume has alsobeen successfully used in the study ofemphysema. Most of the types will fall intothe categories described above but in certaininstances the emphysema is so severe anddestructive in character that it is not possibleto say how it originated, i.e. whether it com-menced as centrilobular or panacinar, or insome other way, so that a class of "indeter-minate" is necessary. Both centrilobular andpanacinar emphysemas may proceed to thecomplete disintegration of the structure withinthe lobule. One can speculate on the likelynature in a particular case if the rest of thelung is not so severely affected and if it showsone or both the basic emphysema types. TheAmerican Thoracic Society (1962) haveadopted the Ciba classification to a large extentbut they have limited the definition to includedestructive changes only and did not regardsimple over-expansion as a form of emphysema.This leaves the pathologist in a quandary andhe would need to use another term such as theclassical one "pulmonum volumen auctum".I think most pathologists would prefer to retainover-distention as a form of emphysema rather
396 July, 1965
GOUGH: Pathology of Emphysemathan separate it under the title "pulmonaryover-inflation" which is what the Americanspropose.
Relative Incidence of Types of EmphysemaIn a series of 140 examples of emphysema
from the general population which Leopoldand I (1957) examined post mortem, we foundthat in 65 there was panacinar emphysemaalone whereas in the remaining 75 there wascentrilobular in addition to panacinaremphysema.
Thurlbeck (1963) examined 150 lungs at theHarvard Medical School Department ofPathology. They were from patients who haddied at the Massachusetts General Hospital,Boston. 138 of the specimens had beenfrom unselected autopsies and 21 were of"severe anatomic pulmonary emphysema". Thelungs had been fixed in expansion. He foundcentrilobular emphysema, panacinar emphy-sema, a destructive lesion commencing in thealveolar ducts which he regarded as a variantor a precursor of panacinar emphysema andthe irregular or scar type of emphysema but nocases of focal dust emphysema. Thus he wasable to differentiate the types of emphysemaaccording to the Ciba classification. In theunselected cases centrilobular emphysema aloneor dominant was present in 21.7%; panacinaremphysema alone or dominant in 13.8%. Inthe cases which were specially selected as severeemphysema, centrilobular was pure or domi-nant in 6, panacinar pure or dominant in 10,mixed 3 and unclassifiable 3.
In an investigation at the HammersmithHospital in London, Heard and Izukawa(1964) found in a series of 50 lungs from con-secutive autopsies, no evidence of any grossdifference in the patterns and incidence ofemphysema between London and our findingsin Cardiff. Centrilobular emphysema is com-moner in these two capitals than in Boston.Heard was careful to distinguish the focal dusttype of emphysema associated with depositionof London dust. In order to distinguish this hereferred to it as "distensive", pointing out thatit is similar to the focal emphysema in coalworkers.
Emphysema and Cardiorespiratory FunctionThe relation of emphysema to cor pulmonaleWhen a series of cases of chronic non-specific
obstructive pulmonary disease is studied postmortem there is no consistent relationshipbetween the severity of emphysema and thedevelopment of cor pulmonale. Extensive
destructive emphysema means a proportionalloss of the capillary bed but it is evident thatthe body can stand a very severe loss of thiskind without necessarily developing corpulmonale. In the series of cases mentionedabove, Leopold and I found that of the 75cases in which there was centrilobular as wellas panacinar emphysema there was right vent-ricular hypertrophy in 41 whereas in 65 casesin which there was panacinar emphysema aloneright heart hypertrophy was present in onlynine. For this purpose we defined the rightventricular hypertrophy as a thickness of 6 mm.or more. Recently we have preferred to usethe weight of the right ventricle separated fromthe rest of the heart taking 70 g. as normal.Of Heard and Izukawa's 50 cases in London,four had died of cor pulmonale and each ofthese had severe emphysema which consistedof both panacinar and centrilobular varietiesand each of these four patients had chronicbronchitis. Wyatt, Fischer and Sweet (1962)found hypertrophy of the right ventricle fre-quently associated with generalised panacinaremphysema but they used the low figure of49 g. as the upper limit of the normal weightof this ventricle.Of the chronic bronchitis-emphysema com-
plex in Britain it would seem that the bronchitis,or more accurately bronchiolitis is an impor-tant component in the development of corpulmonale. Severe cases of chronic bronchitisand bronchiolitis without significant emphysemamay die of cor pulmonale. Organic changesin the blood vessels are not present with suffi-cient consistency to be regarded as the majorcause of the pulmonary hypertension. Func-tional disturbances, particularly hypoxia, haveto be invoked to explain the stress on the rightheart. In cases of severe panacinar emphysemain which there is cor pulmonale I have fre-quently found evidence of inflammation in thebronchioles extending into the alveolar walls,whereas the primary type of panacinar em-physema, atrophy of the alveolar walls andnot inflammation, is the finding. In the inflam-matory type of panacinar emphysema severalblocks of tissue need to be examined becausethe inflammatory changes are not uniformthroughout the lung but related in patches tothe bronchiolitis whereas in other parts thealveolar walls are thin.
Emphysema and airways obstruction
Emphysema is very commonly associatedwith airways obstruction but these two terms
397July, 1965
POSTGRADUATE MEDICAL JOURNAL
should not be taken as synonyms. There isnow considerable evidence that airwaysobstruction can occur with little or no em-physema. This conclusion is based upon thefinding of instances of severe chronic bronchitiswith only very little destructive emphysema(Gough and Leopold, 1962). Such individualsmay have been called emphysematous duringlife because they had marked airways obstruc-tion. Simpson, Heard and Laws (1963)described three patients showing clinical andphysiological features of chronic obstructivelung disease, though none showed radiologicalevidence of emphysema by established criteria.There was gross impairment of ventilatoryfunction but an insignificant degree of em-physema was found at necropsy using specialmethods of examination. These observationswere based on Heard's method of examiningthe lungs post mortem and they agree withmy findings with paper mounted sections.McNab, Grove and Nariman (1961) suggest
that study of the effects of exercise on arterialoxygen saturation and on ventilation equivalentfor oxygen may show whether anatomicalemphysema is present or not. They found thatcentrilobular emphysema was associated withgross physiological defects. Bates and Christie(1964) conclude that in the correlation ofstructure and function in emphysema it is un-fortunately true that the simplest ventilatorytests are of little value in this regard, but theyfeel that, in the majority of these patients, thecombination of careful history-taking, detailedradiography and a complete assessment offunction enables the physician to build up afairly accurate picture of the probable morpho-logical changes in the lungs.The Lungs in Fatal Status AsthmaticusAmong the cases I studied of chronic lungdisease in the general population there were
some who had been diagnosed as asthma andhad died in status asthmaticus. These had beenseen by Dr. D. A. Williams during life anddiagnosed by him as typical asthma. In mostinstances their lungs at autopsy did not showdestructive emphysema. The lungs from theasthmatics were distended as is seen in drown-ing and they showed the classical appearancesof plugging of the bronchi with dense mucus.Histologically there was infiltration with eosino-philes but, whereas in bronchitics there wasmuch destruction of the walls of the air spaces,in the asthmatics the emphysema was mainlysimple over-expansion.
Most of our fatal cases of asthma havebeen in women. In 101 deaths from statusasthmaticus analysed by Dr. D. A. Williams,two-thirds were females and this distributionwas found in all age groups. It might be arguedthat the absence of destructive emphysema wasmainly due to the fact that most of the patientswere women but the same is true of some menwho died in status asthmaticus. Williams andLeopold (1959) reported the autopsy findingsof 25 adults, 19 females and six male, all ofwhom had died in status asthmaticus. Thelungs were examined in my department. Theaverage age of death was 56 years and tenwere over 60 years. The average duration ofasthma was 21 years, three were over 40 years,yet in none of the female cases nor in fourout of six of the male cases was there anydestructive emphysema. Williams (1964) con-siders that cigarette smoking accounts for thehigher incidence of destructive emphysema inmale asthmatics.Of course, individuals who started with
asthma in childhood or later and subsequentlydeveloped bronchitis had the pathological find-ings of bronchitis. In localities where bronchitisis very common, as in London with its pollutedatmosphere, cases of uncomplicated asthmamay be rarer. With the clean air in Cardiff wedo not have such difficulty in separating"asthma" from chronic bronchitis. We can,however, only be sure of the post mortem diag-nosis of asthma if death is due to statusasthmaticus. If an asthmatic dies of a causeother than asthma there may be no evidenceof asthmatic changes in the lungs.
Experimental EmphysemaMany attempts have been made to produce
emphysema in experimental animals. Becauseof the view held for many years that the primecause of emphysema is obstruction to the airflow most experiments have been based uponthis.view. Attempts at producing emphysemaby partial obstruction have, however, hadvarying success. A summary of the earlier workis given by Rasmussen and Adams (1942). Theythemselves failed to produce emphysema indogs by over-distention simulating repeatedasthmatic attacks extending over severalmonths. It is significant, however, that one oftheir dogs developed a spontaneous infectionof the lungs and in it emphysema developedand the authors remarked that "It is mostsuggestive that the factor of infectionwhen added to repeated over-distention
July, 1965398
July, 1965 GOUGH: Pathology of Emphysema 399
is significant in the production of pulmonaryemphysema". Likewise Anderson andcolleagues (1964) failed to produce emphysemain dogs by means of a Venturi valve inthe trachea but when they combined thisobstruction with the destructive effect of dilutenitric acid, they produced emphysema. In-cidentally they found that "retired" grey-hounds had a significant degree of naturalemphysema. Wright and Kleinerman (1963)produced experimental centrilobular emphy-sema by exposing guinea pigs to nitrogendioxide. a common constituent in pollutedatmospheres. This same gas adsorbed on tocarbon also had a focal destructive effect onthe lungs of mice, (Boren, 1964). Centrilobularemphysema has been produced in rats byGross, Babyak, Tolker, and Kaschak (1964)by the action of papain. These various investi-gations confirm our observation of thevulnerability of the respiratory bronchiolesemphasizing the relationship of centrilobularemphysema to external agents which wouldinclude atmospheric pollutants as well as in-fections. Anderson and colleagues (1964) usingpaper-mounted sections, have found a closecorrelation between centrilobular emphysemaand cigarette smoking but found no suchrelationship between panacinar emphysemaand smoking.
SummaryFor satisfactory post mortem study of em-
physema the lungs should be expanded to asize approximating that present during life.This is best done by formalin either in solutionor as a fume. The study is greatly enhancedif whole lung sections mounted on paper bythe Gough and Wentworth technique, or im-pregnated with barium sulphate, by Heard'stechnique, is used. Two fundamentally differ-ent anatomical forms of emphysema are seen,centrilobular, a destructive lesion affectingprimarily the respiratory bronchioles andpanacinar (panlobular) in which all varietiesof air spaces in the lobule expand. One formof the panacinar type consists of simple dilata-tion while the other is destructive. Focal dustemphysema is a specific variety seen mostfrequently in coal workers. It is also centrilobu-lar in position and commences with dilatationof respiratory bronchioles but later may leadto destruction of the walls of the air spaces.A minor form of this disease occurs in thegeneral population in the form of soot emphy-sema from polluted atmospheres.
The prevalent chronic non-specific obstructivepulmonary disease in Britain frequently causescor pulmonale. The commonest finding in suchinstances is a combination of chronic bronchitis(including bronchiolitis) and centrilobular andpanacinar emphysema. In some instances thebronchitis is accompanied by only panacinaremphysema and in fewer instances bronchitisis present with insignificant emphysema. Thisemphasizes the importance of the bronchiticcomponent as a cause of pulmonary hyper-tension in the bronchitis-emphysema complex.The cor pulmonale is apparently not solely dueto reduction of the vascular bed and thethickening of blood vessels, although theseundoubtedly contribute, but also to functionaldisturbance, probably hypoxia. Preliminaryexperimental work in animals confirms thevulnerability to damage of the respiratorybronchioles which has been observed in man.Long standing primary spasmodic asthma, ifnot complicated by bronchitis, does not usuallylead to destructive emphysema in non-smokers.
REFERENCES
ANDERSON, A. E., AZUCY, A., BATCHELDER, T. L., andFORAKER, A. G. (1964): Experimental Analysis inDogs of the Relationship between PulmonaryEmphysema Alveolitis and Hyperinflation, Thorax,19, 420.
ANDERSON, A. E., HERNANDEZ, J. A., ECKERT, P., andFORAKER, A. G. (1964): Emphysema in LungMacrosections Correlated with Smoking Habits,Science, 144, 1025.
BATES, D. V., and CHRISTIE, R. V. (1964):Respiratory Function in Disease, p. 219, Phila-delphia and London: W. B. Saunders.
BOREN, H. G. (1964): Carbon as a Carrier Mechanismfor Irritant Gases, Arch. environm. Hlth., 8, 119.
CANDER, L., and MOYER, J. H. (1964): Ageing of theLung. The Tenth Hahnemann Symposium, NewYork and London: Grune & Stratton.
CUMMINS, S. L., and SLADDEN, A. F. (1930): CoalMiner's Lung: an Investigation into the Anthra-cotic Lungs of Coal Miners in South Wales,J. Path. Bact., 33, 1095.
AMERICAN THORACIC SOCIETY (1962): Definitions andClassification of Chronic Bronchitis, Asthma andPulmonary Emphysema. A Statement by theAmerican Thoracic Society, Amer. Rev. resp. Dis.,85, 762.
GOUGH, J. (1947): Pneumoconiosis in Coal Workersin Wales, Occup. Med., 4, 86.
GOUGH, J. (1952): Discussion on the Diagnosis ofPulmonary Emphysema, Proc. roy. Soc. Med.,45, 576.
GOUGH, J., and WENTWORTH, J. E. (1959): Correlationof Roentgenological and Pathological Changes inSome Diseases of the Lung. Harvey Lectures1957/58. Series 53, 171. New York: AcademicPress.
GOUGH, J., and WENTWORTH, J. E. (1960): RecentAdvances in Pathology, 7th Edition, London:J. & A. Churchill.
400 POSTGRADUATE MEDICAL JOURNAL July, 1965
GOUGH, J., and LEOPOLD, J. G. (1962): Techniquesused in the Study of Lung Pathology: TheAnatomy of Emphysema. Ciba Foundation Sym-posium on Pulmonary Structure and Function,p. 280, London: J. & A. Churchill.
GROSS, P., BABYAK, M. A., TOLKER, E., and KASCHAK,M. (1964): Enzymatically Produced PulmonaryEmphysema, J. occup. Med., 6, 481.
HEARD, B. E. (1958): A Pathological Study ofEmphysema of the Lungs with Chronic Bronchitis,Thorax, 13, 136
HEARD, B. E., and IZUKAWA, T. (1964): PulmonaryEmphysema in 50 Consecutive Male Necropsies inLondon, J. Path. Bact., 88, 423.
HEPPLESTON, A. G. (1954): The Pathogenesis ofSimple Pneumokoniosis in Coal Workers, J. Path.Bact., 67, 51.
LEOPOLD, J. G., and GOUGH, J. (1957): The Centri-lobular Form of Hypertrophic Emphysema and itsRelation to Chronic Bronchitis, Thorax, 12, 219.
MCNAB, G. R., GROVE, W. S., and NARIMAN, S.(1961): A Comparison of Physiological andPathological Findings in Chronic Bronchitis andEmphysema with Special Reference to Responseto Exercise, Thorax, 16, 56.
RASMUSSEN, R. A., and ADAMS, W. E. (1942):
Experimental Production of Emphysema, Arch.intern. Med., 70, 379.
SIMPSON, T., HEARD, B., and LAWS, J. W. (1963):Severe Irreversible Airways Obstruction withoutEmphysema, Thorax, 18, 361.
CIBA GUEST SYMPOSIUM (1959): Terminology,Definitions and Classification of Chronic PulmonaryEmphysema and Related Conditions. A Report ofthe Conclusions of a Ciba Guest Symposium,Thorax, 14, 286.
THURLBECK, W. M. (1963): The Incidence ofPulmonary Emphysema, Amer. Rev. resp. Dis.,87, 206.
WILLIAMS, D. A., and LEOPOLD, J. G. (1959): Deathfrom Bronchial Asthma, Acta allerg. (Kbh.), 14,83.
WILLIAMS, D. A. (1964): The Natural History ofAsthma, 5th International Congress of Allergology,p. 186, Madrid.
WRIGHT, G. W., and KLEINERMAN, J. (1963): TheJ. Burs Amberson Lecture. A Consideration ofthe Etiology of Emphysema in Terms of Contem-porary Knowledge, Amer. Rev. resp. Dis., 88, 605.
WYATT, J. P., FISCHER, V. W., and SWEET, H. C.(1962): Panlobular Emphysema: Anatomy andPathodynamics, Dis. Chest, 41, 239.


















