
THE PATHOLOGICAL CHANGES IN CHRONIC BRONCHITIS … · REID: ThePathological Changesin Chronic...
6
THE PATHOLOGICAL CHANGES IN CHRONIC BRONCHITIS AND EMPHYSEMA By LYNNE REID, M.R.C.P., M.R.A.C.P. Research Fellow, Institute of Diseases of the Chest, Brompton Hospital Chronic bronchitis defies close definition, just as it has defied all attempts at prevention or cure. Its beginning is innocuous enough, being charac- terized by cough and clear mucoid sputum; yet this may lead to incapacitating breathlessness, heart failure and death. Pathologically the disease is disappointing in that there is no specific or diagnostic lesion, since in its early or mild stage the only disturbance may be hypersecretion of mucus (an accentuation of the normal function of the bronchial tree) while in the later stages damage to bronchioles and alveoli has serious and far- reaching functional effect but does not produce any specific pathological change. Bronchial Hypersecretion Hypersecretion of mucus not only holds the key to an understanding of the causes of chronic bronchitis, but its measurement is one of the main difficulties in detecting the onset of the disease and in studying its epidemiological aspects (Stuart- Harris, I954; Ogilvie, 1957; Oswald, 1957). Without being aware of it, the healthy individual normally forms about ioo c.c. of mucoid secretion in 24 hours (Policard and Galy, I945), but what increase is necessary before coughing causes secre- tion to present as sputum is not known, although it is probable that the increase may have to be large, and certain that it varies widely with dif- ferent individuals. Nor is it known, when there is excess, what proportion of the whole is coughed up as sputum. Clinical, epidemiological, bacterio- logical and pathological studies suggest no single cause of chronic bronchitis, but rather that responsibility is shared by many, acting either singly or in combination. Infection (May, 1952; Stuart-Harris, 1954), atmospheric pollution (Logan, I956; Pattle and Collumbine, I956; Ogilvie and Newell, I957) and conditions (Pem- berton and Goldberg, 1953), smoking (Doll and Hill, I956), exposure to industrial dusts (Logan, 1956) and familial variation (Oswald, Harold and Martin, 1953) may each contribute to the develop- ment of chronic bronchitis. Mucus is formed mainly in the trachea and larger bronchi. The mucous glands extend along the bronchial tree only as far as cartilage and, like the plates of cartilage, they reduce in number towards the periphery (Miller, I947). They are numerous in the trachea, in the main and lobar bronchi and in the large intra-segmental bronchi; while it is only at the bifurcations in the small ones that a gland is found adjacent to cartilage. Goblet cells also decrease toward the periphery, being numerous in large bronchi and sparse in bron- chioles. In a mild case of chronic bronchitis there may be little in the mucosa to reflect an increase in mucus production sufficient to cause sputum. In a well-established case, however, histological examination shows an increase in the cells dis- tended with mucus (Fig. I)-in the epithelium of the bronchi, the bronchioles and ducts of glands, and in the glands themselves (Florey, Carleton and Wells, I932; Reid, 1954). There is a close relation between the secretion of mucus and the cilia, the upward movement of mucus depending on an effective ciliary' escalator.' In the absence of acute infection the cilia are usually intact, but if many goblet cells are dis- charging the effective ciliary area may thereby be reduced. Acute infection not infrequently occurs and here the walls of bronchi are infiltrated with inflammatory cells; also there may be destruction of cilia which, however, re-form with healing. Peripheral Changes The name 'chronic bronchitis' suggests that the disease is mainly concerned with the large air- tubes, but its progress can be appreciated only if the perhaps more serious changes, those which develop further down the bronchial tree, in the bronchioles and alveoli, are understood (Gairdner, 1850; Amberson and Spain, 1947; Reid, I954, I957; Leopold and Gough, 1957). It is in the region of the secondary lobule, the respiratory part of the lung (Fig. 2), that the serious functional damage is done which "gives rise to dyspnoea. Recurrent infection, a clinical manifestation of the 24 copyright. on 9 April 2019 by guest. Protected by http://pmj.bmj.com/ Postgrad Med J: first published as 10.1136/pgmj.34.387.24 on 1 January 1958. Downloaded from
Transcript of THE PATHOLOGICAL CHANGES IN CHRONIC BRONCHITIS … · REID: ThePathological Changesin Chronic...

THE PATHOLOGICAL CHANGES INCHRONIC BRONCHITIS AND EMPHYSEMA
By LYNNE REID, M.R.C.P., M.R.A.C.P.Research Fellow, Institute of Diseases of the Chest, Brompton Hospital
Chronic bronchitis defies close definition, just asit has defied all attempts at prevention or cure.Its beginning is innocuous enough, being charac-terized by cough and clear mucoid sputum; yetthis may lead to incapacitating breathlessness,heart failure and death. Pathologically thedisease is disappointing in that there is no specificor diagnostic lesion, since in its early or mild stagethe only disturbance may be hypersecretion ofmucus (an accentuation of the normal function ofthe bronchial tree) while in the later stages damageto bronchioles and alveoli has serious and far-reaching functional effect but does not produceany specific pathological change.Bronchial Hypersecretion
Hypersecretion of mucus not only holds the keyto an understanding of the causes of chronicbronchitis, but its measurement is one of the maindifficulties in detecting the onset of the disease andin studying its epidemiological aspects (Stuart-Harris, I954; Ogilvie, 1957; Oswald, 1957).Without being aware of it, the healthy individualnormally forms about ioo c.c. of mucoid secretionin 24 hours (Policard and Galy, I945), but whatincrease is necessary before coughing causes secre-tion to present as sputum is not known, althoughit is probable that the increase may have to belarge, and certain that it varies widely with dif-ferent individuals. Nor is it known, when there isexcess, what proportion of the whole is coughed upas sputum. Clinical, epidemiological, bacterio-logical and pathological studies suggest no singlecause of chronic bronchitis, but rather thatresponsibility is shared by many, acting eithersingly or in combination. Infection (May, 1952;Stuart-Harris, 1954), atmospheric pollution(Logan, I956; Pattle and Collumbine, I956;Ogilvie and Newell, I957) and conditions (Pem-berton and Goldberg, 1953), smoking (Doll andHill, I956), exposure to industrial dusts (Logan,1956) and familial variation (Oswald, Harold andMartin, 1953) may each contribute to the develop-ment of chronic bronchitis.
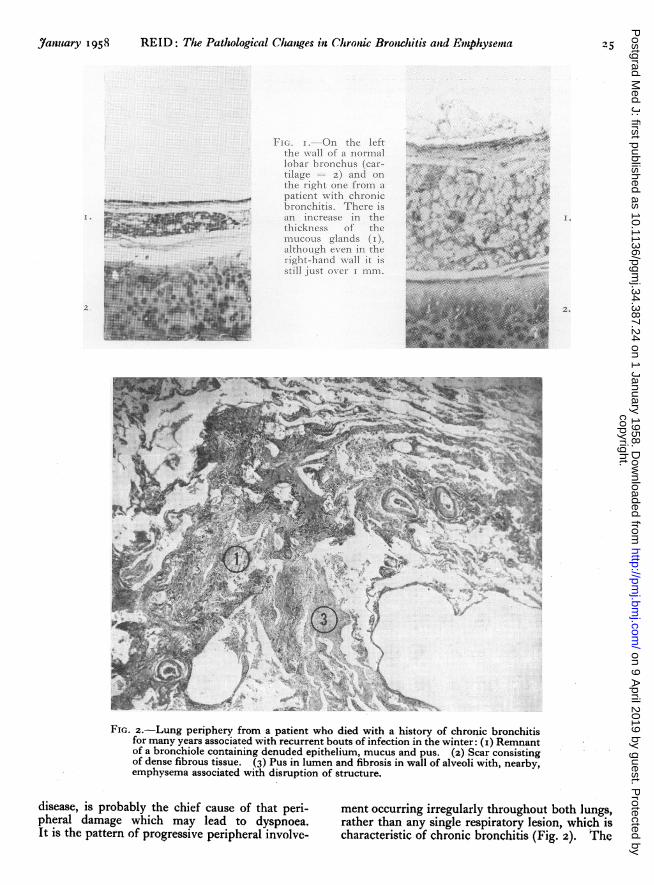
Mucus is formed mainly in the trachea andlarger bronchi. The mucous glands extend alongthe bronchial tree only as far as cartilage and, likethe plates of cartilage, they reduce in numbertowards the periphery (Miller, I947). They arenumerous in the trachea, in the main and lobarbronchi and in the large intra-segmental bronchi;while it is only at the bifurcations in the small onesthat a gland is found adjacent to cartilage. Gobletcells also decrease toward the periphery, beingnumerous in large bronchi and sparse in bron-chioles. In a mild case of chronic bronchitis theremay be little in the mucosa to reflect an increase inmucus production sufficient to cause sputum.In a well-established case, however, histologicalexamination shows an increase in the cells dis-tended with mucus (Fig. I)-in the epithelium ofthe bronchi, the bronchioles and ducts of glands,and in the glands themselves (Florey, Carleton andWells, I932; Reid, 1954).There is a close relation between the secretion of
mucus and the cilia, the upward movement ofmucus depending on an effective ciliary' escalator.'In the absence of acute infection the cilia areusually intact, but if many goblet cells are dis-charging the effective ciliary area may thereby bereduced. Acute infection not infrequently occursand here the walls of bronchi are infiltrated withinflammatory cells; also there may be destructionof cilia which, however, re-form with healing.Peripheral ChangesThe name 'chronic bronchitis' suggests that
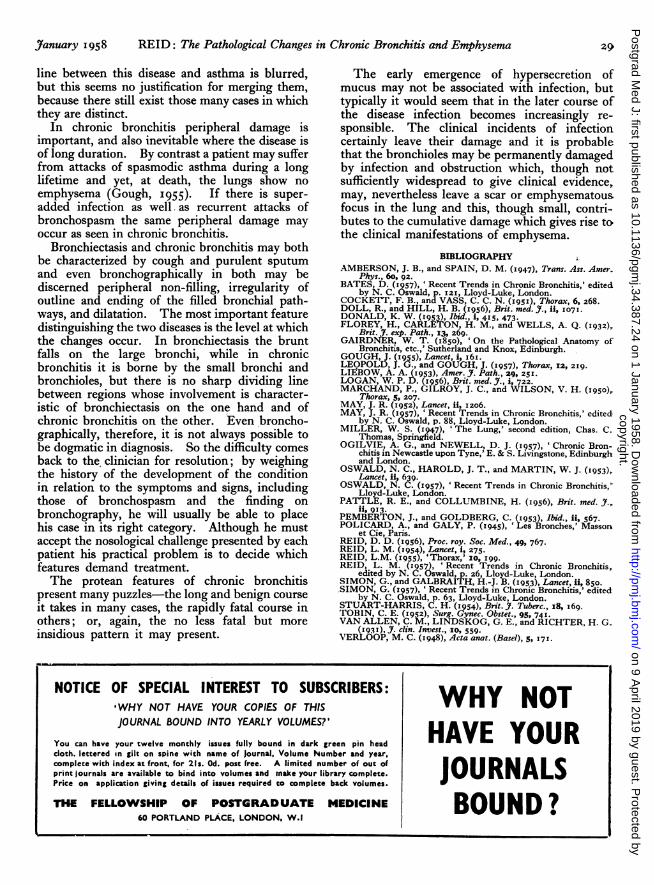
the disease is mainly concerned with the large air-tubes, but its progress can be appreciated onlyif the perhaps more serious changes, those whichdevelop further down the bronchial tree, in thebronchioles and alveoli, are understood (Gairdner,1850; Amberson and Spain, 1947; Reid, I954,I957; Leopold and Gough, 1957). It is in theregion of the secondary lobule, the respiratory partof the lung (Fig. 2), that the serious functionaldamage is done which "gives rise to dyspnoea.Recurrent infection, a clinical manifestation of the
24copyright.
on 9 April 2019 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.34.387.24 on 1 January 1958. Dow
nloaded from
January 1958 REID: The Pathological Changes in Chronic Bronchitis and Emlphysema 25
~i ;:
;...~..E,.:;.i.:.~;,;;:8.:_. i,,: :---- ......,. ...:
:i;;....F:::d"!
:. ...; :
!':ii.,i ii ..;iij. I .......,;j li:..i:
......;....;.
FIG. I.-On the leftthe wall of a normallobar bronchus (car-tilage = 2) and onthe right one from apatient with. chronicbronchitis. There isan increase in thethickness of themucous glands (I),although even in theright-hand wall it isstill just over i mm.
I"'B
.t."..a i;r" C:.;"" .c.ja.·;nF.%' C;""; .mr a.a..; cF "
..i.u.
.j.g.C.%rPu.i.;.$....i.i.
a .e.i.t.i .e..-aaa.a.a.
I,
2.
- w ih* *
lP*E'
*· *i .t'.·
Y 11 'RO.....;4
FIG. z.-Lung periphery from a patient who died with a history of chronic bronchitisfor many years associated with recurrent bouts of infection in the winter: (i) Remnantof a bronchiole containing denuded epithelium, mucus and pus. (2) Scar consistingof dense fibrous tissue. (3) Pus in lumen and fibrosis in wall of alveoli with, nearby,emphysema associated with disruption of structure.
disease, is probably the chief cause of that peri-pheral damage which may lead to dyspnoea.It is the pattern of progressive peripheral involve-
ment occurring irregularly throughout both lungs,rather than any single respiratory lesion, which ischaracteristic of chronic bronchitis (Fig. 2). The
copyright. on 9 A
pril 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.34.387.24 on 1 January 1958. D
ownloaded from

26 POSTGRADUATE MEDICAL JOURNAL January 1958
types of lesion are many. In the bronchioles theremay be hypertrophy of goblet cells or purulentbronchiolitis. This may produce ulceration ofbronchioles and alveoli, and give rise to micro-abscess cavities; stenosis of the bronchiole may alsooccur or even obliteration of its lumen. Alveolarinflammation may give rise to patchy pneumonicconsolidation, oedema, mucus and pus in the al-veoli, while more permanent damage such asorganization of inflammatory exudate, emphysemaand collapse may also result. Although the lesionsare varied they fall generally into two groupsaccording as they are the direct result of infectionor obstruction, though it is often hard to determinethe respective role these play in any sequence ofchanges, particularly since infection may act byobstruction as well as by destruction or consolida-tion, while obstruction arising from hypersecretionalone probably predisposes to infection.Some of the changes listed are acute and may
resolve, while others represent permanent damageeither directly from initial destruction or because,failing to resolve, they proceed to fibrosis. In-directly damage may also be the result of distortionof lung architecture, distension of air spaces orvascular adjustment in adjacent lung. The patho-logical changes vary not only in their nature andage but also in their extent. Damage often occursirregularly within a secondary lobule (Fig. 3) sothat within a single unit most of the changes maypresent, but the disease may involve a lobule orgroup of lobules uniformly. Scars may, therefore,represent either a considerable volume of lung orrather less than one acinus.Although bronchioles and alveoli are functionally
closely related their changes are not alwaysparallel in severity, and here collateral ventilationis important. Van Allen, Lindskog and Richter(193 ) have shown that obstruction of a segmentalbronchus may not result in collapse, since air canpass from lobule to lobule by drift across alveolarwalls and the change in alveoli may, therefore, beless than would be expected from the associatedlesion in the bronchial wall.
EmphysemaWhere there is shortness of breath the clinician
often couples the diagnosis of emphysema withthat of bronchitis. At once a new field of diag-nostic uncertainty is opened up. Emphysema hasa different diagnostic meaning for the clinician,radiologist, physiologist and pathologist, since thedifferent techniques they use measure differentaspects of the disease. In order to reconcile theseeming contradictions, it is probably most usefulto consider first the pathological diagnosis andthen to correlate this with the results of othermethods of enquiry. The technique of the
t.b·iji·· .:· :*IL
") !I3· *i··:
2. .jiF
j
·· Bi
rl*_..sre.- -- .. 41.i.· ·.*lc.;-ul--~-.:·*:i..
I.
*c·.
i:·;··: :X
FIG. 3.-On the lower left is a scar (I) including fibroustissue and elastic fibres (black) showing the patternof condensed alveoli. Adjacent emphysema (2)means that certain intact alveoli (3) are no longersupported by normal lung. A septum is evident atthe lower left-hand corner forming a boundary ofthis secondary lobule within which a variety ofchanges are seen.
pathologist is sensitive in that he can examine thelung directly and minutely. Thus he mayjustifiably diagnose emphysema where the clinicianand the physiologist would not, since the disease istoo limited in extent to give rise to such degree offunctional disturbance as they would considersignificant. The same may apply to the radio-logist if the lesion is not extensive enough to giverise to localized hypertranslucency.The essential feature of the pathological
diagnosis of emphysema is an increase in thequantity of air beyond the terminal bronchioles ina given volume of lung and, obversely, a decreasein the amount of alveolar capillary blood (Reid,1957; Simon, 1957). By emphasising a reductionin the amount of blood as well as an increase in airthe pathologist relates the basis of his diagnosismore closely to those features which are significantto other techniques. For example, the hyper-translucency seen by the radiologist results from arelative increase in air, while the decrease incarbon monoxide uptake detected by the physio-logist is the result of loss of capillary bed. Within
copyright. on 9 A
pril 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.34.387.24 on 1 January 1958. D
ownloaded from

REID: The Pathological Changes in Chronic Bronchitis and Emphysema
the above definition two different pathologicaltypes of emphysema can be recognized-in thefirst the structure of the lung is still intact, eventhough it is distended; while in the second thereis destruction or disruption of alveolar walls(Fig. 3). The second includes many differentmorphological types, ranging from mild to severedisease, from the localized to the diffuse, fromthe air-containing space of only a centimetre indiameter to one as large as a grapefruit. But toall of these disruption of lung is the commoncrucial feature.The overdistension type of emphysema is the
less well understood of the two, and in chronicbronchitis it is overshadowed in importance by thesecond type to which inflammatory damage sooften gives rise. Sometimes on opening the chesta whole lobe may appear emphysematous, beingfluffy, dry to the touch, failing to collapse andshowing evidence of poor elasticity after com-pression; and yet, throughout the lobe, thehoneycomb structure of the lung is still intact evenif a little coarser. Overdistension also contributesto the development of emphysema when it occursunevenly in lung adjacent to scars (Fig. 3) repre-senting considerable condensation of tissue. Insome patients with chronic bronchitis fibroticnodules are frequent, while the total resting volumeis normal, or, more often, increased, indicating arelative dilatation of some parts of the lung.Although ulceration or destruction of pulmonary
structure may occur anywhere along the bron-chioles or in the alveoli, the region of the bron-chiolo-alveolarjunction is a frequent site of damage,but unless many are involved the damage will notbe clinically apparent. With loss of integrity ofthis part of the lung the normal volume change onrespiration is impaired since this is dependent onthe structure being intact.
Destruction of part of the wall of the bronchioleand of alveoli may bring about an increase involume, loss of the capillary bed and conversion ofthe bronchiolar wall to the structure of a flap-valve(Reid, 1957). Such pulmonary destruction maybe followed by interference with blood supply tointact alveoli and by trapping of air resulting fromthe flap-valve action of a distorted bronchiolar wall.The area of such a focus of emphysema may be nomore than a few square millimetres.
Large bullae, easily visible to the naked eye, mayresult if the initial destruction is greater, or ifsecondary changes are superimposed on smallinitial lesions. The distension of the smallerspace behind the flap-valve of the bronchiolar wallmay occur gradually with ordinary respiration,with coughing, because of collapse or fibrosis inneighbouring lobules or by reason of impairmentof blood supply to the part beyond.
Although, externally, bullae may appear tocontain only air, when cut there may be tags orflimsy strands of lung passing through them.Sometimes a whole lobe or a large part of its volumemay be represented only by these shreds, whichconsist of connective tissue septa, bronchi andblood vessels. Remnants of alveoli may persist asreddish brown tags or they may be compressedagainst septum or pleura until ultimately, to thenaked eye, they appear as fibrous thickening.Changes in Blood VesselsThe significant disturbance in the vascular
system is usually secondary to bronchial damage.Destruction of capillary bed (Fig. 3), arterioles andeven larger vessels may be found with emphysemaand endarteritis obliterans is frequently seen inarteries supplying fibrotic scars. But histologicalstudy is only a preliminary to the more difficulttask of interpreting the functional derangement.
Dilatation of the main pulmonary arteries inemphysema is often seen radiographically; at thesame time their branches may be abnormallynarrow right from their point of origin (Simon,I957). This dilatation has been confirmed bymeasurement of the arteries at autopsy, whileexamination of the wall has confirmed that thechange is not due to any associated organic disease.Dilatation suggests that the proximal part of thearterial system behaves like a reservoir, while theintra-pulmonary narrowing points to an alterationin amount or rate of flow through the lung.The capillary bed in the wall of the bronchial
tree is supplied by bronchial artery, that in the wallof the respiratory bronchioles by both bronchialand pulmonary artery, that of the respiratorytissue beyond from pulmonary artery alone. The.capillary bed at each of these levels may be reducedby destruction or by scarring of respiratory tissue.The bronchioles seen passing in the flimsy strandsof emphysematous lung often have no pulmonaryarteriole accompanying them, these having beenlost along with the supporting lung. The lumenof pulmonary arteries supplying emphysematousareas is often reduced, perhaps with some degree ofendarteritis obliterans. This change may also beseen in vessels supplying scars. In respiratoryand terminal bronchioles where the wall is stillintact the capillaries are often grossly dilated.The two pathways of venous drainage from the
lung do not correspond topographically to thedouble arterial supply. Normally the truebronchial veins drain only the proximal largebronchi and pleura, pass to the azygos veins andthe right side of the heart, while the more peri-pheral part of the bronchial tree, like the respira-tory tissue, drains to the pulmonary veins and theleft side of the heart. Marchand and his colleagues
January I958 27
copyright. on 9 A
pril 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.34.387.24 on 1 January 1958. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
(I950) have shown dilatation of the true bronchialveins in emphysema, while Liebow (1953) and co-workers have demonstrated that there is easiercommunication between them and the peripheralpulmonary venous system, with an increase in theblood returning from the lungs through thebronchial veins to the right side of the heart.
This is but one feature of the abnormal vasculardynamics in emphysema which gives rise to theclinical features of cor pulmonale. The arterialand venous systems not only communicate witheach other through a capillary bed, but pre-capillary anastomoses exist between bronchial andpulmonary artery and between pulmonary arteryand veins (Verloop, 1948; Cockett and Vass, '951;Tobin, 1952). This complexity of the normalvascular arrangements makes the interpretationof changes in disease extremely difficult. Inchronic bronchitis the changes are lobular notlobar. The latter may be produced experi-mentally and their effect on bronchial and pul-monary artery flow determined, but these effectsare not necessarily applicable to the conditionsfound with intralobular disease.
Correlation of Pathological Changes withRadiological and BronchographicAppearancesThe correlation of these changes with those seen
in radiographs and bronchograms (Simon andGalbraith, I953; Simon, I957) and with thefindings of respiratory function tests explainssomething of the variation in the results obtainedby these different methods of investigation whichcontributes to the difficulties of diagnosis.A patient may be short of breath and yet,
because individual lesions may be small, the lungmay radiographically appear normal, althoughsmall scars, either singly or in a cluster, may bevisible. Hypertranslucency, either localized orgeneralized, may be evident and it may be de-marcated by a line shadow suggesting the wall of abulla. While individual lesions may not bevisible on a radiograph they may yet be sonumerous and so serious as to cause secondarychanges to the heart, great blood vessels anddiaphragm, detectable by radiography.Bronchography usually reveals more damage
than a plain radiograph. The dilated ducts ofmucous glands may fill with radio-opaque materialand give rise to the linear projections from theoutline of main, lobar and segmental bronchi.
In the peripheral part of a bronchogram threechanges have been described as characteristic ofchronic bronchitis-the absence of peripheralfilling, irregular endings of those pathways whichdo fill, and the presence of pools of radio-opaquematerial. Although technical inadequacies as the
cause of these irregularities must be excluded, theyfrequently reflect damage in the periphery.Scarring of bronchial pathways and condensationof lung tissue in fibrotic nodules result in loss ofperipheral pattern, while delayed filling may resultfrom emphysema because of impaired ventilation.
Irregularities in the outline of the bronchial wallmay be caused by narrowing from fibrosis ordilatation from ulceration. Pools of lipiodolseveral millimetres in diameter represent dilatedbronchioles or small bronchi (Reid, 1955). Some-times a pool has a spiked or irregular outline,resembling normal filling save that it is rathercoarser, and here also there is dilatation andobliteration of the bronchioles in the secondarylobule.
Correlation with Respiratory Function StudiesIn the mild stages of chronic bronchitis there
may be no impairment of respiratory function(Bates, 1957), but all too frequently the disease isprogressive and in severe cases the patterncharacteristic of emphysema is seen (Donald,1953). There is an increase in total lung volumeand in the relative amount of residual air because,with expiration, the lung empties incompletely,air being trapped before the normal level ofdeflation is reached. Contributing to this phe-nomenon is blockage of the lumen by sputum,stenosis of the wall of the bronchial tree anddestruction of lung tissue converting the walls ofbronchioles into flap-valves.
Because of the operation of collateral ventilation(van Allen, Lindskog and Richter, 1931) the lesionsin alveoli need not parallel in severity those inbronchioles, so that diffusion of gas may beimpaired even where perfusion by blood is normal,and vice versa. Factors which impair ventilationwill adversely affect the intrapulmonary mixingof gases. Although there may be free com-munication between neighbouring bullous areas,allowing for rapid equalization of gas betweenthem, there may still be evidence of poor mixing,because large volumes are uniformly poorlyventilated from the bronchi.
Loss of capillary bed will be associated withreduction in carbon monoxide uptake, but theresults of this test must be interpreted in thelight of ventilation. Where perfusion of blood isseriously affected there will be decrease in arterialoxygen levels, while impairment of gas diffusionwill give rise to retention of carbon dioxide-oxygen desaturation and retention of carbondioxide are not always proportional.To conclude, the presence of bronchospasm and
the relief given by bronchodilators in certaincases of chronic bronchitis suggest that the dividing
28 January 1958copyright.
on 9 April 2019 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.34.387.24 on 1 January 1958. Dow
nloaded from
January 1958 REID: The Pathological Changes in Chronic Bronchitis and Emphysema 2
line between this disease and asthma is blurred,but this seems no justification for merging them,because there still exist those many cases in whichthey are distinct.
In chronic bronchitis peripheral damage isimportant, and also inevitable where the disease isof long duration. By contrast a patient may sufferfrom attacks of spasmodic asthma during a longlifetime and yet, at death, the lungs show noemphysema (Gough, I955). If there is super-added infection as well as recurrent attacks ofbronchospasm the same peripheral damage mayoccur as seen in chronic bronchitis.
Bronchiectasis and chronic bronchitis may bothbe characterized by cough and purulent sputumand even bronchographically in both may bediscerned peripheral non-filling, irregularity ofoutline and ending of the filled bronchial path-ways, and dilatation. The most important featuredistinguishing the two diseases is the level at whichthe changes occur. In bronchiectasis the bruntfalls on the large bronchi, while in chronicbronchitis it is borne by the small bronchi andbronchioles, but there is no sharp dividing linebetween regions whose involvement is character-istic of bronchiectasis on the one hand and ofchronic bronchitis on the other. Even broncho-graphically, therefore, it is not always possible tobe dogmatic in diagnosis. So the difficulty comesback to the clinician for resolution; by weighingthe history of the development of the conditionin relation to the symptoms and signs, includingthose of bronchospasm and the finding onbronchography, he will usually be able to placehis case in its right category. Although he mustaccept the nosological challenge presented by eachpatient his practical problem is to decide whichfeatures demand treatment.The protean features of chronic bronchitis
present many puzzles-the long and benign courseit takes in many cases, the rapidly fatal course inothers; or, again, the no less fatal but moreinsidious pattern it may present.
The early emergence of hypersecretion ofmucus may not be associated with infection, buttypically it would seem that in the later course ofthe disease infection becomes increasingly re-sponsible. The clinical incidents of infectioncertainly leave their damage and it is probablethat the bronchioles may be permanently damagedby infection and obstruction which, though notsufficiently widespread to give clinical evidence,may, nevertheless leave a scar or emphysematousfocus in the lung and this, though small, contri-butes to the cumulative damage which gives rise tothe clinical manifestations of emphysema.
BIBLIOGRAPHYAMBERSON, J. B., and SPAIN, D. M. (1947), Trans. Ass. Amer.
Phys., 60, 92.BATES, D. (1957), 'Recent Trends in Chronic Bronchitis,' edited
by N. C. Oswald, p. 121, Lloyd-Luke, London.COCKETT, F. B., and VASS, C. C. N. (I951), Thorax, 6, 268.DOLL, R., and HILL, H. B. (x956), Brit. med. J., ii, 0o71.DONALD, K. W. (1953), Ibid., i, 415, 473.FLOREY, H., CARLETON, H. M., and WELLS, A. Q. (1932),Brit. J. exp. Path., 13, 269.GAIRDNER, W. T. (1850), 'On the Pathological Anatomy of
Bronchitis, etc.,' Sutherland and Knox, Edinburgh.GOUGH, J. (x955), Lancet i,i6I.LEOPOLD, J. G., and GOUGH, J. (1957), Thorax, 12, 219.LIEBOW, A. A. (1953), Amer. J. Path., 29, 251.LOGAN, W. P. D. (1956), Brit. med. J., i, 722.MARCHAND, P., GILROY, J. C., and WILSON, V. H. (1950),
Thorax, 5, 207.MAY, J. R. (1952), Lancet, ii, 1206.MAY, J. R. (I957), ' Recent Trends in Chronic Bronchitis,' edited,
by N. C. Oswald, p. 88, Lloyd-Luke, London.MILLER, W. S. (I947), 'The Lung,' second edition, Chas. C.
Thomas, Springfield.OGILVIE, A. G., and NEWELL, D. J. (I957), 'Chronic Bron-
chitis in Newcastle upon Tyne,' E. & S. Livingstone, Edinburghand London.OSWALD, N. C., HAROLD, J. T., and MARTIN, W. J. (1953),Lancet, ii, 639.OSWALD, N. C. (I957), 'Recent Trends in Chronic Bronchitis,'
Lloyd-Luke, London.PATTLE, R. E., and COLLUMBINE, H. (1956), Brit. med. J.,
ii, 913.PEMBERTON, J., and GOLDBERG, C. (1953), Ibid., ii, 567.POLICARD, A., and GALY, P. (1945), 'Les Bronches,' Masson
et Cie, Paris.REID, D. D. (I956), Proc. roy. Soc. Med., 49, 767.REID, L. M. (1954), Lancet, i, 275.REID, L.M. (I955), 'Thorax,' 0o, I99.REID, L. M. (x957), 'Recent Trends in Chronic Bronchitis,edited by N. C. Oswald, p. 26, Lloyd-Luke, London.SIMON, G., and GALBRAITH, H.-J. B. (1953), Lancet, ii, 850.SIMON, G. (I957), 'Recent Trends in Chronic Bronchitis,' edited
by N. C. Oswald, p. 63, Lloyd-Luke, London.STUART-HARRIS, C. H. (1954), Brit. J. Tuberc., I8, I69.TOBIN, C. E. (1952), Surg. Gynec. Obstet., 95, 741.VAN ALLEN, C. M., LINDSKOG, G. E., and RICHTER, H. G.
(I93I), . clin. Invest., Io, 559.VERLOOP, M. C. (1948), Acta anat. (Basel), 5, 171.
NOTICE OF SPECIAL INTEREST TO SUBSCRIBERS: WHY N
,WHY NOT HAVE YOUR COPIES OF THISJOURNAL BOUND INTO YEARLY VOLUMES?' HAVE
You can have your twelve monthly issues fully bound in dark green pin head *cloth, lettered in gilt on spine with name of Journal, Volume Number and year,complete with index at front, for 21s. Od. post free. A limited number of out ofprint journals are available to bind into volumes and make your library complete.Price on application giving details of issues required to complete back volumes. w
THE FELLOWSHIP OF POSTGRADUATE MEDICINE BOUN60 PORTLAND PLACE, LONDON, W.I
copyright. on 9 A
pril 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.34.387.24 on 1 January 1958. D
ownloaded from


















