The NHS Commissioning Environment, A Guide for ion in the Third Sector

of 44
-
Upload
garden-gorilla -
Category
Documents
-
view
220 -
download
0
Transcript of The NHS Commissioning Environment, A Guide for ion in the Third Sector
-
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
1/44
Th NHS cissiningnvinnt: A guid
ganisatins in ththid sct
-
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
2/44
DH INformATIoN reADer BoX
PolicyHR/WorkforceManagementPlanningClinical
EstatesCissiningIM & TFinanceSocial Care/Partnership Working
Dcunt pups For information
Gatway nc 13911
Titl The NHS commissioning environment: A guide fororganisations in the third sector
Auth The Department of Health; Third Sector Partnership Team
Publicatin dat March 2010
Tagt audinc National charities, third sector and social enterprise
volunteer-involving organisations; third sector and socialenterprise service providers; local community voluntarygroups, Voluntary Organisations/NDPBs, Trade Unions
Ciculatin list Voluntary Organisations/NDPBs Trade Unions
Dsciptin This guide aims to support third sector organisations andand social enterprises maximise their full potential incontributing to improved health and well-being servicesand outcomes for England, by describing key featuresof the NHS commissioning environment and highlightingthe potential roles and opportunities for the sector
Css nc N/A
Supsdd dcunts N/A
Actin quid N/A
Tiing N/A
Cntact dtails Howard ChapmanThird Sector Partnership TeamRoom 3E44, Quarry HouseQuarry Hill, LeedsLS2 7UE0113 254 5212
f rcipints us
Crown copyright 2010
First published March 2010
Produced by COI for the Department of Health
www.dh.gov.uk/publications
http://www.dh.gov.uk/publicationshttp://www.dh.gov.uk/publications -
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
3/44
fwd by thminist Stat
Ca Svics
As Minister of State for Care Services and with
responsibility for the third sector within health and social
care,I am well aware of the sectors substantial role in the delivery of high quality health and social care services.
Icontinue to be excited about the possibilities for thesectors contribution to tackling some of our biggest health challenges.
Third sector organisations have a strong track-record of
designing services based on strong insight into community and individual clients
needs, and are often better placed to respond flexibly to those needs. They are
often able to reach those vulnerable and hard to reach groups who may not be
in regular contact with statutory health and social care services.
Government reform recognises that by developing a broader range of service
providers, we can increase capacity, encourage innovation and improve userresponsiveness. However,Iappreciate there are challenges and barriers that canprevent the sector from achieving its full potential. In particular, if we are to
encourage third sector organisations to enter NHS markets, it is important that we
help the sector to better understand the developing commissioning environment,
which can seem complex and daunting.
Ihope that this guide will go some way to assist third sector organisations toachieve their potential by explaining, in a straightforward way, the NHS
commissioning environment including the commissioning cycles, and illustratingpotential roles and opportunities for the sector.
Phil Hope
1
-
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
4/44
-
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
5/44
Cntnts
1. Intductin...................................................................................................4 2. Undstanding th stuctu th NHS........................................................5
2.1 Introduction...........................................................................................52.2 The organisational structure of the NHS.................................................62.3 Roles of organisations ............................................................................ 7
3. What is Cissining? ............................................................................123.1 The commissioning cycle ..................................................................... 123.2 What is commissioning? ...................................................................... 123.3 Who are the commissioners for the NHS?............................................16 3.4 Patient Public Involvement...................................................................193.5 The Compact.......................................................................................20
4. Hw t ngag and wk with cissins ............................................214.1 An overview of healthcare planning processes .....................................214.2 Points of engagement for thirdsector organisations.............................254.3 Collaboration and partnership working opportunities...........................27
5. Bcing a svic pvid t th NHS......................................................28 5.1 Tendering process and awarding contracts ...........................................285.2 Procurement policy .............................................................................. 285.3 Choice, Cooperation and Competition.................................................295.4 Grants as a funding route.....................................................................305.5 The procurement process..................................................................... 325.6 NHS contracts...................................................................................... 35
6. Cnclusin.......................................................................................................38
3
-
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
6/44
1. Intductin
1.1 Thirdsectororganisationsand social enterprisesarekeypartnersindelivery
at everylevel andquarter acrossthehealth and social care system: contributingtothedevelopment andimplementationofpolicy and
services,helpingdriveinnovation andqualityimprovement; informingand contributingthroughthecycleof commissioningfor
healthand care services,helping understand users needs andexpectations; and
asprovidersofhealth and careservicesamongst anincreasinglydiverserangeformally commissionedbytheNHS andlocal authorities.
1.2 CommissioningofNHS servicesisincreasinglyfocusing onquality,greatercontrol,pathways of care,personalisation, andimprovingthe outcomesforindividuals.Thisisbeingachievedthroughgiving service users more choiceof services and
providers.
Two examples of
how
this
is
being achieved are:
thedevelopment ofpersonalhealthbudgetswhichgiveserviceusersthefreedomtodirectlychoose andpayfor care; and
theconcept of any willingproviderisbeing usedtocommissionpotentialproviderstogive service users choice andensurethatqualityisthe organisingprinciple ofhealthcaredelivery.
1.3 Thisguideaimstosupportthirdsectororganisationsand social enterprisesto makethe most ofthe opportunities available and maximisethe extenttowhichthey are ableto achievetheirfullpotentialin contributingtoimprovedhealthand wellbeing services and outcomesforthepopulation ofEngland.Itdoesthisbydescribingthekeyfeatures oftheNHScommissioning environment, along withkey stagesinthe commissioningcycles,highlightingthepotential roles and opportunitiesforthe sectorsetting outthekey stagesinbeing commissioned,inparticularfocusing on: understandinghowtheNHS commissioning environmentisstructured; howthirdsectororganisationsand social enterprisescanengagewith
NHScommissioners; and tenderingprocessesandfunding routesthattheNHS uses.
4
-
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
7/44
2. Undstanding th stuctu th NHS
2.1 Intductin2.1.1 If the third sector and social enterprises are to work successfully with the
NHS, and the NHS is to benefit from the opportunities and benefits offered
by the third sector service delivery, it is key that there is mutual
understanding between NHS commissioners and third sector organisations.
There are ongoing initiatives to improve commissioners capability andunderstanding of the third sector. The aim of this guide is to help
organisations in the third sector to understand how the NHS works and
where the key opportunities for partnership working exist. This section
explains the way the NHS is structured, the planning process, and how
priorities are set. Finally, it focuses upon how to engage with
commissioners and, where appropriate, tender and contract for NHS
funded services.
2.1.2 The English health care system has four main features: The Government sets out policy and key priorities.
The health system is funded by the state through taxation.
The Government appoints the key regulators of services.
The Government allocates funds to local commissioners to supportproviders of health care services.
2.1.3 One of the main reasons this guide is being produced is that the last of
these is changing. The ability of patients to choose means that the provider
market for health is diversifying. Other sectors are becoming approved
providers of services, contracted to provide services through an increasingly
sophisticated process of procurement by PCTs.
5
-
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
8/44
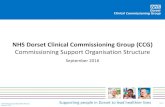
Structure of the NHS today
Department of Health
Funding
Accountability
Referrals
Contracts
10 Strategic HealthAuthorities
152 primary care trusts
Specialistservices
Hospitalservices
Out of hospitalservices
Communityservices
Primary careservices
GPs
Providers
The NHS commissioning environment: a guide for organisations in the third sector
2.2 Th ganisatinal stuctu th NHS2.2.1 In very simple terms the NHS is structured to plan and deliver services as
set out below:
6
-
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
9/44
Understanding the structure of the NHS
2.2.2 To fully explain the main structures, the diagram below illustrates the
nature of the relationships between the various elements of the NHS
system, including regulators:
2.3 rls ganisatinsThis next section explains in detail the roles of each type of organisation
in this structure.
Dpatnt Halth (DH)
2.3.1 The DH has the overall responsibility for health and social care policy
for England. The role of the DH is to set overall policy, guidance and
frameworks designed to create the conditions for improvement and
innovation in the delivery of health and social care, to benefit staff,
patients and the public by:
setting national standards;
shaping the direction of health and social care services;
promoting health and wellbeing; and reducing health inequalities.
7
-
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
10/44
DH Third Sector Partner Induction 5 May 2009
The NHS commissioning environment: a guide for organisations in the third sector
2.3.2. The DH does not deliver health and social care services to the public
directly. Instead it works with a variety of delivery partners, principally
within the health and social care system, which includes the NHS, local
government, DHs arms length bodies, and independent private and third
sector organisations. More information about the DH can be found at
www.dh.gov.uk
Statgic Halth Authitis (SHAs)
2.3.3 Strategic Health Authorities provide the key link between the DH and
the local NHS. The role of the 10 SHAs is to provide strategic leadership
for a large geographical area at regional level and monitor the performanceof local PCT areas, including local NHS Trusts, to ensure that local health
systems operate effectively and collaboratively. Of particular relevance
to this guide, SHAs have a lead role in assuring PCTs commissioning
competencies and are responsible for PCT commissioning development
programmes.
rginal planning
SHAs are mainly coterminous, and work closely with the Government
Offices for the Regions. At a regional level the SHAs need to be aware ofthe other demands on government and work with several regional
partners. These are set out below:
Regional landscapeRegional Association Public Healthof Directors of Adult ObservatoriesDH Regional
Social ServicesTeam
StrategicCommission Health AuthorityCare Quality
Regional SelectImprovement and
Regionaland Grand
Efficiency CommitteesPartnership
RegionalGovernment Assembly
Office (replacement organisation in allregions except London)
Regional DevelopmentLocal
Government Agency UniversitiesAssociation
Regional Ministersregional body
8
http://www.dh.gov.uk/http://www.dh.gov.uk/ -
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
11/44
Understanding the structure of the NHS
SHAs work with the Regional Improvement and Efficiency Partnerships
on issues of joint concern, with the Government Offices and the Joint
Improvement Partnerships (JIPs) whose membership include key regional
figures from the DH social care team and Directors of Adult and Childrens
services as well as key third sector representation.
Some joint commissioning may take place at a regional level where the
people needing services are small in number and have relatively specialist
requirements. This regional commissioning level can provide focus on
common outcomes and give greater efficiency to provision. Regional
structures do vary.
Piay ca tusts
2.3.4 Most primary care trusts (PCTs) have the same geographic boundaries as
local authorities. PCTs have three main functions:
to engage with their local population to improve health and wellbeing;
to commission a comprehensive and equitable range of high quality,responsive and efficient services, within allocated resources, across all
health service sectors; and
to directly provide services, for example many PCTs currently providedistrict nursing and health visiting services and some also provide some
specialist services such as community dentistry.
PCTs must have in place separate internal management arrangements
for their provider arms, ensuring that they are treated in the same
manner as any other provider. In February 2010 the Department of
Health issued guidance (Transforming Community Services: The
assurance and approvals process for PCT-provided community
services), which required PCTs to develop, agree and implementproposals for the future organisational structure of their current PCT-
provided community services. Options include integration with other
community-based providers, which could include third sector providers,
as well as setting up new social enterprises under the Right to Request
scheme (see below).
Pvids
2.3.5 There are a number of types of organisations that provide NHS-funded
care. Traditionally, most services have been delivered by PCTs themselves,
and NHS Trusts which are accountable to SHAs and usually provide either
acute hospital, mental health or ambulance services. Increasingly, NHS
9
-
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
12/44
The NHS commissioning environment: a guide for organisations in the third sector
Trusts are becoming NHS Foundation Trusts; these have a greater degree
of autonomy than NHS Trusts and and are regulated by Monitor (see
below).
2.3.6 Most primary care services have traditionally been delivered by General
Practitioners, either as independent practitioners or working in partnership
with other GPs within a practice. GPs also have a role in commissioning
services as practice based commissioners; this is explained in more detail in
the section focusing on Strategic Commissioning.
2.3.7 The diversity of providers is expanding. Already some services in some
areas are delivered by non-NHS providers, and also by local authorities.NHS staff working in PCT-provided community services have also been
given the Right to Request to develop a business case for the transfer of
the services they provide into a social enterprise which will diversify future
supply further. Any services which are transferred under this arrangement
will be market tested after the expiry of the initial contract.
rgulatsCa Quality Cissin
2.3.8 Until recently the quality of NHS services was monitored by the Health
Care Commission (HCC), the Commission for Social Care Inspection (CSCI)
and the Mental Health Act Commission. From April 2009 they merged into
one organisation, the Care Quality Commission (CQC), which regulates
the quality of both health and adult social care. Health and social care
providers including, for the first time, NHS providers are required to
register with the new regulator in order to provide services that fall under
the scope of regulated activity. The registration requirements that all
providers, including the third sector, must meet are consistent across both
health and adult social care. Regulation is focused on essential levels of
safety and quality of services to ensure that patients, users and vulnerable
groups are protected.
In addition, the CQC carry out a periodic review of PCTs, NHS providers
and local authorities (previously known as the Annual Health Check) and
Performance assessment of Local Authorities. For more information go to
www.cqc.org.uk.
mnit2.3.9 NHS foundation trusts provide over half of all NHS hospital and mental
health services. Foundation Trusts are monitored by an independent
10
http://www.cqc.org.uk/http://www.cqc.org.uk/ -
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
13/44
Understanding the structure of the NHS
regulator Monitor to ensure that they are well managed and financially
strong. There are three main strands to Monitors work:
determining whether NHS trusts are ready to become NHS FoundationTrusts;
ensuring that NHS Foundation Trusts comply with the conditions theyhave signed up to that they are well-led and financially robust; and
supporting NHS Foundation Trust development.
Audit Cissin
2.3.10 The Audit Commission audits NHS trusts, PCTs and strategic healthauthorities to review the quality of their financial management systems.
They also publish independent reports which highlight risks and good
practice to improve the quality of financial management in the health
service and encourage continual improvement in public services including
in the field of public health and health inequalities.
Cphnsiv Aa Assssnts (CAA)
2.3.11 The Audit Commission has developed tailored frameworks for CAA for
council areas, which will include the role and contribution of PCTs. The
frameworks pull together a range of information in an objective and
comparable way to reach an overall judgement on a councils performance.
The CAA framework document, published on 10 February 2009, set out
how CAA will be delivered from April 2009. CAA reflects the new era of
public sector partnership working. This new assessment framework will
provide a snapshot of how effectively local partnerships are working
together to deliver local peoples priorities.
CAA has been developed and will be delivered jointly by the main public
sector inspectorates. The partner inspectorates are:
Audit Commission
CQC
HM Inspectorate of Constabulary
HM Inspectorate of Prisons
HM Inspectorate of Probation, and
Ofsted.
11
-
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
14/44
3. What is cissining?
3.1 Th cissining cycl
3.2 What is cissining?
3.2.1 There are many definitions but the four main components are:
Identifying need What do we need?
Identifying demand How much do we need?
Shaping the market Who can do it and how?
Holding the market to account Monitor, adjust and review
3.2.2 The key principles for commissioning as set out by the Office of the Third
Sector are:
Understand the needs of those using the service.
12
-
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
15/44
What is commissioning?
Consult provider organisations when setting priorities.
Put outcomes for users at the heart of the process.
Map the fullest practical range of providers.
Consider investing in the provider base.
Ensure contract processes are transparent and fair.
Ensure long-term contracts and risk sharing.
Seek feedback to review effectiveness of the commissioning process.
3.2.3 The processes and broad timetables for commissioning within the NHS are: Strategic Commissioning:
needs assessment (spring and summer);
decommissioning decisions (summer and early autumn);
priority setting (autumn);
defining the service programmes required (on-going).
Funding/Procurement and Contracting (see the PCT ProcurementGuide, www.dh.gov.uk/en/Publicationsandstatistics/Publications/
PublicationsPolicyAndGuidance/DH_113745):
shape the structure of supply (ongoing)
grant funding awards (winter and spring)
procurement and contracting (winter)
Monitoring, Performance Management Review
contract settlement and review (monthly)
performance assessment (monthly)
Wld Class Cissining
3.2.4 The Department of Health has developed a vision for NHS commissioning
which outlines what it means to be world class commissioners within the NHS
at a local level, and how world class commissioning will impact population
health and wellbeing. See www.dh.gov.uk/en/managingyourorganisation/
commissioning/worldclasscommissioning/index.htm
13
http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/http://www.dh.gov.uk/en/managingyourorganisation/http://www.dh.gov.uk/en/managingyourorganisation/http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/ -
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
16/44
The NHS commissioning environment: a guide for organisations in the third sector
In suay:3.2.5 World class commissioning aims to
deliver better health and wellbeing for all, so that:
people will live healthier and longer lives; and
health inequalities will be dramatically reduced.
deliver better care for all:
services will be evidence-based and of the best quality; and
people will have choice and control over the services that they use,so services become more personalised.
deliver better value for all:
investment decisions will be made in an informed and consideredway, ensuring that improvements are delivered within available
resources; and
PCTs will work with others to optimise effective care.
WCC assuanc syst3.2.6 The world class commissioning assurance system gives appropriate
frameworks for assessing a PCTs current capability and identifying future
development requirements for world class commissioning, and to ensure
that health outcomes are improving. Therefore, it also gives the third sector
a useful understanding of what they can expect from local commissioners.
Cptncis
3.2.7 World class commissioning competencies describe the knowledge, skills,
behaviours, and characteristics that commissioners will need to reach world
class status.
3.2.8 In summary, world class commissioners will:
locally lead the NHS;
work with community partners;
engage with public and patients;
collaborate with clinicians;
manage knowledge and assess needs;
14
-
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
17/44
What is commissioning?
prioritise investment of all spend;
stimulate the market;
promote improvement and innovation;
secure procurement skills;
manage the local health system; and
efficiency and effectiveness of spend.
3.2.9 The full vision and other information is available at www.dh.gov.uk/en/
Managingyourorganisation/Commissioning/Worldclasscommissioning/index.htm
3.2.10 Third sector organisations can help commissioners to achieve these
competencies, particularly in relation to working with community partners,
engaging the public and patients, assessing need, stimulating the market
and promoting improvement and innovation.
Suppt and dvlpnt awk
3.2.11 A support and development framework exists to give commissioners accessto the tools they need to drive improvements in commissioning practice,
either by sharing services and good practice, developing internal resources,
or buying in external expertise, for example through the Framework for
procuring External Support for Commissioners (FESC). FESC provides PCTs
with easy access to a framework of expert suppliers who can support them
in undertaking their commissioning functions. FESC assists commissioners
by:
providing easy access to a framework of organisations, offering a range
of skills and experience, that have been through a robust pre-qualification process by the Department;
saving time in undertaking procurement activities with easy access tooptimum value for money solutions;
minimising the range of organisations offering resources, which willreduce the legal and cost implications that can be encountered when
seeking to procure external support; and
adopting more innovative and efficient approaches to commissioning.
There is the potential for third sector organisations to become involved in
supporting PCTs as commissioners (for example, in contributing to needs
15
http://www.dh.gov.uk/en/http://www.dh.gov.uk/en/ -
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
18/44
The NHS commissioning environment: a guide for organisations in the third sector
assessment or service design and specification), helping them to become
world class commissioners either directly or in partnership with a FESC
provider.
3.3 Wh a th cissins th NHS?3.3.1. The commissioners of NHS services are principally practice based
commissioners and PCTs. This section sets out their roles in more detail
and also the roles of other key commissioning organisations.
Pactic basd cissining
3.3.2 A practised based commissioning (PBC) group often comprises GPs, but it
can also include other primary care professionals such as nurses,
pharmacists and optometrists, amongst others. Individual practices may
become a PBC, they may also form an alliance/consortium or a cluster with
other practices in their local area.
3.3.3 PBCs develop commissioning plans for their communities and patients, and
working closely with PCTs and secondary care clinicians, decide how best
to meet the needs of their patients to achieve the best clinical, health and
wellbeing outcomes. They also play a key supporting role to PCTs byproviding valuable feedback on provider performance.
3.3.4 PCTs are the budget holders, and therefore take the lead in actually buying
services including tendering and placing contracts. They have overall
accountability for healthcare commissioning; however, practice based
commissioning is crucial at all stages of the commissioning process, to
inform each PCTs purchasing decisions.
3.3.5 More information can be found at: www.dh.gov.uk/en/Managingyourorganisation/Commissioning/Practice-basedcommissioning
Piay ca tusts
3.3.6 PCTs are responsible for working with PBCs and local authorities to engage
with their local population to assess needs, commissioning health care
services to meet those needs, and improve health and wellbeing outcomes.
3.3.7 They normally take the lead in procuring and placing contracts with
providers to reflect those commissioning needs. PCTs can enter intopartnerships with local authorities who may take the lead in procurement
and contracting for services (see below for joint commissioning).
16
http://www.dh.gov.uk/en/http://www.dh.gov.uk/en/ -
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
19/44
What is commissioning?
3.3.8 PCTs may also work together and collaborate to commission services via
Specialist Commissioning Groups (SPGs) to agree strategic commissioning
approaches for specialist services that are organised across larger
geographical areas. Local cancer networks are an example of this. A single
PCT may then take the lead in contracting for services on behalf of the
SPG to meet the aims of the joint commissioning plan.
Lcal authitis
3.3.9 Local authorities are responsible for commissioning social care for their
population.
3.3.10 Local authorities and PCTs work as key partners in Local Strategic
Partnerships (LSPs). LSPs are non-statutory, multi-agency partnerships that
match local authority boundaries. They are charged with bringing together
different sectors of the community public, private, community and the
third sector to work together more effectively in instigating and
developing new initiatives that improve the main areas of performance laid
out in the PSAs and the Local Area Agreement targets (see below). Most
LSP structures deal with the local issues relating to earning, learning,
community safety and health. Each Local Authority should have a
dedicated structure for its LSP and a website detailing its local structure
and targets. In most areas, third sector organisations are already involved
in the LSP, which reflects the local Compact agreement. Individual
organisations may wish to consider their own links with the LSPs and
how they can influence them effectively.
3.3.11 Some services may form legal partnerships with PCTs to commission and/
or provide services jointly. The framework provided by the National Health
Service Act 2006 means money can be pooled between health bodies and
health-related local authority services, functions can be delegated andresources and management structures can be integrated.
The arrangements allow commissioning for existing or new services, as wellas the development of provider arrangements, to be joined up. They were
previously referred to as Section 31 Health Act flexibilities, and cover:
lead commissioning (where a commissioner takes the lead on behalf ofthe other);
integrated provision (where health and social care staff work together,sometimes this is via a Care Trust); and
17
-
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
20/44
The NHS commissioning environment: a guide for organisations in the third sector
pooled budgets (where budgets are merged for specific issues, e.g.learning disability services).
3.3.12 In England, Section 31 of the Health Act 1999 has been replaced by
Section 75 of the National Health Service Act 2006, which has consolidated
NHS legislation. The new provision is in exactly the same terms, and
existing Section 31 arrangements will continue as if made under the new
powers.
Any new partnership arrangements should refer to the new powers underSection 75, rather than to Section 31. Similarly, previous grant
arrangements known as Section 28A
and Section 28 BB have changed asresult of the NHS Act 2006, and are now known as Section 256 and 76
respectively.
3.3.13 Further information can be found at www.dh.gov.uk/en/Healthcare/
IntegratedCare/Healthact1999partnershiparrangements/index.htm
Childns Tusts
3.3.24 Childrens Trusts bring together all local services for children and young
people, to focus on improving outcomes. They do not necessarily manageservices directly, but focus on ensuring that services are commissioned and
organised in a cohesive and coherent manner. Their commissioning plans
are normally procured and contracted by both PCTs and local authorities.
3.3.25 Arrangements which allow local authorities and primary care trusts to pool
childrens budgets or integrate the provision of childrens services are
known as Section 10 agreements.
Lad pvids3.3.26 PCTs may choose to contract with a lead provider to deliver certain types
of care; the lead provider may then sub-contract elements of this care to
other providers. Both NHS trusts and NHS foundation trusts could be lead
providers of care. Equally, third sector or independent sector providers
could also undertake this role. Where this arrangement is in place, lead
providers are responsible for ensuring that the main requirements of their
contract with the commissioner in relation to quality and governance are
reflected in any sub-contract.
18
http://www.dh.gov.uk/en/Healthcare/http://www.dh.gov.uk/en/Healthcare/ -
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
21/44
What is commissioning?
3.4 Patint Public InvlvntLcal Invlvnt Ntwks (LINks)
3.4.1 The Local Government and Public Involvement in Health Act 2007 placed
a duty on local authorities with social services responsibilities to arrange for
a LINk to be established in their area (from 1 April 2008). This same
legislation abolished the previous system of Patient Forums.
3.4.2 Local authorities contract with a Host organisation that is then responsible
for setting up and supporting the LINk. LINks are independent networks of
individuals, organisations, groups and associations, and have been set up
to:
cover all publicly funded health and adult social care services in thelocal authority area;
promote and support the involvement of people in the commissioning,provision and scrutiny of local services, thereby providing communities
with a mechanism to monitor and review local health and social care;
actively canvass every section of the community for their views andexperiences of local care services;
make those views known to those responsible for commissioning,providing, managing and scrutinising services.
3.4.3 Under the legislation LINks can:
make recommendations for improvements and expect a response withina specific timescale;
enter certain premises and view the care being provided; and
refer matters to the local Overview and Scrutiny Committee and expecta response within a specific timescale.
3.4.4 Anyone can get involved in a LINk from individuals (e.g. carers, service
users, community leaders) to groups and organisations (e.g. charities,
faith groups, Black and Minority Ethnic (BME) organisations, user-led
organisations, tenant groups and youth councils) in a variety of ways
to suit their needs.
ovviw and Scutiny Citts3.4.5 Each local authority has a Health Overview and Scrutiny Committee; these
were established by the Health and Social Care Act in 2001 to monitor
19
-
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
22/44
The NHS commissioning environment: a guide for organisations in the third sector
local health services and it must be consulted on major local service
changes.
3.5 Th Cpact3.5.1 Established in 1998, the Compact is an agreement between Government
and the voluntary and community sector in England. It recognises the vital
role that the sector has in society, working alongside the state and the
private sector, and the values, principles and commitments it shares with
Government. The Compact provides the framework for how both parties
should work together, with overarching principles and commitments that
each side will undertake in order to ensure productive partnership working.It is built on trust, mutual goodwill and the belief that working together
will produce better outcomes than working in isolation.
3.5.2 The Compact is not statutory guidance, its authority derives from the fact
that it is signed up to by government and the sector. The Compact applies
to central government departments, including Government Offices for the
Regions, and executive non-departmental public bodies that have a
relationship with the third sector organisations.
3.5.3 A national level, the Compact Partnership consists of the Office of the
Third Sector, based in the Cabinet Office, which represents the interests of
government, and Compact Voice, which represents the interests of the
third sector. The Commission for the Compact is an independent body
responsible for overseeing the Compact.
3.5.4 All English local authority areas are covered by a Local Compact. These
compacts, along with regional compacts that support them, provide a
jointly agreed framework of principles to guide the working relationship
between local authorities, primary care trusts and other public bodies andthe third sector in the area, with the aim of deriving mutual, purposeful
and positive benefit. Local Compacts cover all aspects of relations across
the whole range of third sector organisations in the local area. They are
based on the national Compact, but are tailored to take into account
differences between areas.
3.5.5 A key Compact principle, especially at local level, is that service delivery
and voluntary and community activity are equally important. Therefore,
contracts and grants (and other support) should be kept in balance.
20
-
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
23/44
4. Hw t ngag and wkwith cissins
4.1 An vviw halthca planning pcsss4.1.1 In many ways the heart of the commissioning cycle is what used to be
called a planning process. The planning process starts with the
determination of key goals, and aims to make the best use of available
resources. All budgets are finite and therefore it is essential to know the
limit of resources available to the planning organisations of the NHS andthen determine the priorities for investment. The process for setting out
the national priorities and the financial resources available to the NHS is
the responsibility of government. The local NHS responds to national
priorities by developing a plan to deliver improvement. Increasingly the
focus is for the local NHS to establish and address priorities at a local level
within its geographic boundary. Central to this is the Joint Strategic Needs
Assessment (JSNA) which is led by primary care trusts (PCTs) and local
authorities.
Cphnsiv Spnding rviw (CSr)
4.1.2 The CSR is a process which started in 1997, under the current Government,
and covers a three-year period which sets out fixed expenditure limits for
each government department, including Health. The CSR process also sets
out the key improvements in public services to be made in the three-year
period for which the expenditure limit has been set. The Governments
priorities are set out in Public Service Agreements (PSAs). The PSAs for
the current period are set out at www.hm-treasury.gov.uk/pbr_csr07_
psaindex.htm. The current PSAs are reflected in the Operating Frameworkof the NHS.
4.1.3 The NHS is funded through general taxation. Funding for government
departments is determined through Spending Reviews. The Treasury
announced three years of funding for the NHS as part of the last
Comprehensive Spending Review (CSR) in October 2007. The CSR also
sets out the key priorities for the funding as part of the Departments
Public Service Agreements (PSAs). The current CSR period runs from
2008/09 to 2010/11. A key aim of the Spending Review process, has beento allow organisations to develop longer term financial plans. This includes
21
http://www.hm-treasury.gov.uk/pbr_csr07_http://www.hm-treasury.gov.uk/pbr_csr07_ -
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
24/44
The NHS commissioning environment: a guide for organisations in the third sector
the ability to award longer term contracts to providers and grants to third
sector organisations.
4.1.4 The Government priorities are set out in the PSAs. Where appropriate the
Department cascades these to the NHS though the priorities set out in the
NHS Operating Framework and its Vital Signs indicators. The indicators
clearly distinguish the national must dos from those areas where local
organisations need to set their priorities based on local needs. The
operating framework for the NHS in England 2010/11, which sets out
current priorities for the NHS along with performance management
arrangements, is available at: www.dh.gov.uk/en/Publicationsandstatistics/
Publications/PublicationsPolicyAndGuidance/DH_110107. This keypublication sets out the issues which PCTs are required to address and is
therefore ssntial ading cunt and ptntial pvids.
4.1.5 Along with the Operating Framework, the DH issues financial allocations
to PCTs to fund local services.
Natinal plicy
4.1.6 National policy is set out by the DH at various times of the year and
includes major strategies or statements about organisational changes and
technical guidance on a variety of NHS issues. The DH website provides
information about new documents and new consultations (www.dh.gov.
uk). Organisations such as the National Institute for Health and Clinical
Excellence (www.NICE.org.uk), the Kings Fund (www.kingsfund.org.uk)
and the NHS Confederation (www.nhsconfed.org) produce useful analyses
of the papers issued.
Piitis and planning
4.1.7 The following annual planning processes and documents are key
to understanding the priorities at both national and local levels. Their
development also gives the potential for third sector organisations to
influence commissioning priorities and receive early notice of tendering
opportunities.
Lcal iplntatin
4.1.8 In most places the detailed plan for each PCT is worked on during the
summer and autumn. During that period there should be openengagement with users and user groups in order to review current services
and to help produce the plans for future service configuration. A Joint
22
http://www.dh.gov.uk/http://www.nice.org.uk/http://www.dh.gov.uk/en/Publicationsandstatistics/http://www.dh.gov.uk/http://www.dh.gov.uk/http://www.nice.org.uk/http://www.kingsfund.org.uk/http://www.nhsconfed.org/http://www.nhsconfed.org/http://www.kingsfund.org.uk/http://www.nice.org.uk/http://www.dh.gov.uk/http://www.dh.gov.uk/http://www.dh.gov.uk/en/Publicationsandstatistics/ -
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
25/44
How to engage and work with commissioners
Strategic Needs Assessment (JSNA) is now required for each local authority
and PCT area to frame its commissioning plans; this is described in more
detail below. Between October and December most PCTs prioritise their
planned spending for the year to come, and start to consider how to work
with the providers across all sectors. The period between January and
March is when contracts and other forms of agreement with providers are
finalised. A final plan is agreed by the board of each PCT either in March
of every year or as soon as possible in the new financial year.
PCTs are required to produce five-year Strategic Commissioning plans
which should also be aligned with information from the JSNA (see 4.1.17).
Lcal Aa Agnts (LAAs)
4.1.9 LAAs set out the priorities for each Local Strategic Partnership (LSP) area to
achieve. They are agreed between central government and each LSP
through the Government Offices for the Regions. There are 188 National
Indicators in total, on which progress in each LSP area is reported. Many of
these relate to health and social care, but others relate to community
safety, education and other matters that contribute to improved
communities. Of these 188 national indicators, each LSP will have agreed
35 as key priorities for action (LAA targets), although progress against any
of the 188 could contribute to the Comprehensive Area Assessment (CAA)
by the Audit Commission, Care Quality Commission (CQC) and other
inspectorates of how well the LSP is improving outcomes for local people
in the area. New initiatives and proposals developed by any organisation
should ideally show how the services on offer will contribute to the
achievement of LAA targets.
4.1.10 The NHS has two sets of indicators against which performance is managed
and monitored. These are set out in the NHS Operating Framework asExisting Commitments and Vital Signs. Some of these are specific to the
NHS, while other health and wellbeing indicators require working in
partnership with local authorities. These indicators can help potential
providers to frame discussions and proposals in ways that assist
commissioners to achieve their priorities.
Dict Public Halth pt
4.1.11 Each PCT has a Director of Public Health (DPH). Some are shared with
other NHS organisations but all should be appointments agreed with the
local authority.
23
-
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
26/44
The NHS commissioning environment: a guide for organisations in the third sector
4.1.12 Each DPH produces a report on an annual basis. The report sets out an
assessment of the health of the population for a specific geographic area
and makes recommendations as to how health can be improved in that
area.
4.1.13 It is important to note that the report is independent, in as much as the
report does not have to be formally sanctioned by a local authority or a
PCT board. It is a statement of the independent professional view of the
DPH.
4.1.14 The report should provide health planners with a good basis for producing
local action plans and should be taken account of within the JSNA. It istherefore also useful for the third sector to understand the key priorities of
the Director of Public Health, as this will have an influence upon
commissioning decisions.
Jint Statgic Nds Assssnt (JSNA)
4.1.15 The Local Government and Public Involvement in Health Act 2007 requires
local authorities and health bodies to produce a JSNA of the health and
wellbeing of their local community. This became a duty in April 2008.
JSNA guidance is available at: www.dh.gov.uk/en/Publicationsandstatistics/
Publications/PublicationsPolicyAndGuidance/dh_081097.
4.1.16 The JSNA has been referred to as the story of the community and uses
data regarding population, health, housing, social care and other
prominent areas of possible concern to help paint a picture of both current
and future needs. It may also describe the historical context for the
assessment. It will help communities to understand themselves and
contribute to the setting of priorities through the various planning
mechanisms described here. It is expected that the priorities described in
the JSNA will reflect the outcomes that communities wish for and shape
the final commissioning plans of PCTs and local authorities.
4.1.17 The JSNA should provide the basis for framing key commissioning decisions
to ensure that they meet the identified needs of local people. Third sector
organisations can offer a vital role in engaging and representing the needs
of the population as part of this assessment process.
Pactic basd cissining plans
4.1.18 Each practice based commissioner (PBC) will have a developed process to
produce a commissioning plan for its registered population. This gives PBCs
24
http://www.dh.gov.uk/en/Publicationsandstatistics/http://www.dh.gov.uk/en/Publicationsandstatistics/ -
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
27/44
How to engage and work with commissioners
the opportunity to suggest alterations to the PCTs current plans in respect
of the services which the PCT purchases. Through these plans there are
opportunities to deliver new, innovative and local improvements. Practice
based commissioning does not mean that practices themselves purchase
healthcare; this is a duty of the PCT.
4.1.19 Plans at a PBC level could give smaller providers an opportunity to work in
a particular area of PCT commissioning and often provides opportunities
for small-scale innovative approaches.
Pvid tust businss plans
4.1.20 NHS trusts and foundation trusts may provide an opportunity for a range
of providers to work in partnership. Trusts produce an annual business plan
setting out their priorities and the key actions they want to take in order to
achieve those plans. In developing these plans, trusts may well be willing
to work with a range of providers in the development and implementation
of their plans. There is no fixed national timetable for the production of the
plans, but mainly they will be expected to be complete before the end of
each calendar year.
4.2 Pints ngagnt thid sct ganisatinsGt t knw yu lcal cissins
4.2.1 For third sector organisations looking to engage and work with NHS
commissioners as a partner or provider, the same tips apply as with any
sector. The key to successful supply is to know your partner and the
market, and understand your partners or potential customers needs and
priorities. Developing a relationship with commissioners can help
organisations shape their potential services and identify future
opportunities for joint working.
4.2.2 It is important to remember that there is a distinct difference between
collaboration and cooperation with commissioners and others to shape the
commissioning plans for services, and competition when a formal tendering
process commences. Third sector organisations will have a legitimate
interest in both stages, but they are distinct. All parties need to ensure that
the first stage provides equal opportunities for all appropriate interests to
play a part. Involvement in this initial stage should not then lead to an
assumption that a competitive tender process is not required, or that thecompetitive tender process is different for any potential legitimate bidder.
25
-
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
28/44
The NHS commissioning environment: a guide for organisations in the third sector
4.2.3 It may also be important for third sector organisations to acknowledge the
differences there may be between their campaigning and advocacy roles
and their roles as potential providers of services. A clear distinction
between these roles will need to be made when working with
commissioners, unless specifically contracted to undertake a particular role,
for instance in an advocacy capacity.
4.2.4 There is already a clear duty, provided by legislation, requiring PCTs to
involve third sector organisations in developing the JSNA. If this is not
happening, organisations should establish how they can participate and
add value to the process.
4.2.5 All PCTs, trusts and local authorities have websites which give information
about their structures, their local plans and how to contact them. In
particular, it is worth looking at board agendas and papers to identify their
priorities in relation to commissioning; this may also identify the lead
individuals within key statutory organisations.
4.2.6 The most appropriate contact for any issue will depend upon specific
circumstances and may vary slightly at a local level, as commissioners do
not necessarily have exactly the same organisational structures.
4.2.7 If the proposed service is basd aund a paticula and sall cunity,
it may be most appropriate and beneficial to discuss it firstly with practice
based commissioners (GP practices). PCTs will have the information about
local PBCs.
4.2.8 If the service is of a spcialist natu a paticula clint gup, enquire
who in the PCT leads for commissioning specialist services.
4.2.9 If the service is focusing on gnal halth ptin, advic suppt it
may be most appropriate to contact the Public Health Directorate.
establish th nd
4.2.10 Is the proposed service one that the NHS currently buys? If it is an existing
service, are there plans to go to competitive tender? If so, when will this
happen?
Ds th ppsal t th cissins nds?4.2.11 Proposals should fit with the identified strategic needs assessment,
priorities and commissioning plan of the commissioner. In addition, your
26
-
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
29/44
How to engage and work with commissioners
proposal should be adabl, vidncd basd and where possible
demonstrate asuabl utcs. Successful proposals will probably
recognise the key partners in care delivery and linkages to other services to
ensure that svic uss a supptd and ca dlivy is salss.
Can th vidnc bas and cptnc th ppsd svicb dnstatd bustly?
4.2.12 Commissioners are held to account for spending public money, and while
they will be interested in new and innovative services, commissioning a
new, untested service without a strong evidence base represents a higher
degree of risk. Equally a new provider will need to give assurance that it isa safe and competent organisation. Providers therefore need to supply
robust evidence on a regular basis that they are fit for purpose, and as far
as possible demonstrate that their proposal will deliver a safe, effective and
value for money service which meets the identified needs.
4.3 Cllabatin and patnship wking pptunitis4.3.1 It may be useful to link up with other organisations with similar interests to
consider collaboration, and to participate in Strategic Commissioning
processes and/or service provision opportunities. Being a member of a localnetwork or providers forum may also provide a channel for regular
communication with commissioners. The local infrastructure organisations
can provide information about local networks and forums, and may also
offer opportunities to engage with local commissioners.
4.3.2 Consortia or partnership arrangements when tendering for services may
increase the potential opportunities for third sector organisations. Further
information and advice can be found in Working in a consortium, available
at: www.cabinetoffice.gov.uk/media/107235/consortium%20guide%20final.pdf
27
http://www.cabinetoffice.gov.uk/media/107235/consortium%20guide%20http://www.cabinetoffice.gov.uk/media/107235/consortium%20guide%20 -
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
30/44
5. Bcing a svic pvidt th NHS
5.1 Tnding pcss and awading cntacts5.1.1 This section gives an outline of the principles of procurement and how
providers of health care are selected where competitive tendering is used.
It then goes on to explain the different forms of contracts which the NHS
may use.
5.2 Pcunt plicy5.2.1 The PCT Procurement Guide for Health Services supports NHS
commissioners in deciding whether and how to procure health services
through formal tendering and market-testing exercises. The Guide is
intended to complement and build upon wider system management
initiatives and the world class commissioning programme. It is one of
several system management tools and guidance documents announced in
Annex C of The operating framework for the NHS in England 2008/09.
The Principles and Rules for Cooperation and Competition (PRCC) (Annex
D) set out the expected behaviours and processes for procurement, and for
cooperation and competition between providers. Principle 3 of the PRCC
requires PCTs to follow the guidelines set out in the PCT Procurement
Guide.
5.2.2 It is wth nting that NHS cissins d nt ncssaily hav t us
al xtnal pcunt pcsss all svics. Halth ca is
usually classiid as Pat B und eU pcunt law, which ans that
a cptitiv tnd aangnt is nt quid t awad a cntact halth ca. The Guide and the Principles will therefore be applied and
considered by commissioners in each individual circumstance, both when
procuring services, and working with existing providers, to give them the
opportunity to improve or redesign services.
5.2.3 The full guide can be found at www.dh.gov.uk/en/
Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/
DH_113745
28
http://www.dh.gov.uk/en/http://www.dh.gov.uk/en/ -
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
31/44
Becoming a service provider to the NHS
5.3 Chic, Cpatin and Cptitin5.3.1 Good procurement systems within the NHS will be characterised by the
proactive and effective use of:
chic on the part of patients between providers of clinical services,settings and models of care;
cptitin between providers for, and in, the healthcare market;
gvnanc arrangements in place in contracting organisations;
cntacts between NHS contracting organisations and providers;
statgic patnships; and
inatin for patients and referrers to enable them to make informedchoices.
Such systems will enable commissioners to secure the best services for the
people they serve, and supply benchmarks against which providers and
clinicians can measure themselves.
5.3.2 The Framework for Managing Choice, Cooperation and Competition
supports these outcomes by:
providing a statement of the bnits ctivly anaging chicand cptitin;
stating the c pincipls by which choice and competition should bemanaged;
ensuring that patints a d gnuin chics and have theinformation to make informed decisions;
defining ls and spnsibilitis anaging chic andcptitin;
outlining the role and development of the independent C-patinand Cptitin Panl; and
setting out how we propose to build the capability t anag chicand cptitin and hold organisations to account through appropriate
assuanc chaniss.
5.3.3 The full framework can be found at www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/
DH_084779
29
http://www.dh.gov.uk/en/http://www.dh.gov.uk/en/ -
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
32/44
The NHS commissioning environment: a guide for organisations in the third sector
C-patin and Cptitin Panl (CCP)
5.3.4 An independent national Co-operation and Competition Panel has been setup to advise the DH and consider complaints about alleged breaches of the
principles and rules, for example, from potential providers or bidders who
are dissatisfied with procurement processes. The CCP may consider four
types of cases:
merger inquiries
conduct inquiries
procurement dispute appeals
advertising and misleading information dispute panels
Merger inquiries and conduct inquiries may be considered directly by the
CCP. However, procurement and advertising disputes will only be
considered on appeal from a strategic health authority. The CCP may also
investigate and report on non-case specific competition issues referred to it
by the DH or by Monitor. More information about the referral process can
be found at www.ccpanel.org.uk/referrals-to-ccp/index.html
5.4 Gants as a unding ut5.4.1 PCTs may consider the use of grant funding to support or contribute to
some third sector activities. This is distinguished from services which are
purchased, where a full contract will be more appropriate.
5.4.2 There is a recognised need for both grant funding and contracts to support
a sustainable third sector, including social enterprises. Funding can have
different purposes, and there may be a benefit to maintaining a mix of
grant funding (such as to support the Joint Strategic Needs Assessment)alongside the increasing opportunities to contract for the delivery of public
services. Where third sector and social enterprise providers are acting as
publicly funded service providers on behalf of the NHS, it is appropriate to
have a legal contractual agreement in place, which shares risk and provides
a framework for performance.
5.4.3 The main determinants of the form of the financial relationship are the
purpose of funding and the nature of the intended outcomes. The decision
on which funding mechanism to use should be based on a combination of
these factors:
30
http://www.ccpanel.org.uk/referrals-to-ccp/index.htmlhttp://www.ccpanel.org.uk/referrals-to-ccp/index.html -
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
33/44
Becoming a service provider to the NHS
Purpose:
Pcunt: used to acquire goods, works or services in line with theGovernments policy of value for money the optimum combination
of whole-life cost and quality (or fitness for purpose) to meet the users
requirement normally achieved through competition; or
Gant: used to fund an activity of a recipient because that activity is inbroad alignment with the Governments objectives. There is a
continuum of uses of grant, although grants in general are subject to a
more detailed level of control than grant-in-aid. At one end of the
continuum, commissioners may wish to give money to a third sector
organisation because it wishes to offer financial support for specifiedaspects of the organisations expenditure. At the other, a commissioner
may wish to give a grant return for which the organisation must deliver
services as specified by the commissioner.
Other issues include:
what level of control is appropriate;
the state of the market; and
the specificity of the outcomes which the funder intends and theindicators available for qualitative and quantitative measurement of
these intended outcomes.
5.4.4 There is, however, an ongoing role for strategic or capacity building
funding, including general grants to assist with the costs of developing and
running an organisation where the objectives of the organisation align with
and contribute to the PCT or local authority responsibilities for health and
social care.
5.4.5 There is also a role for specific grants to enable an organisation to carry
out a particular project. Specific grants are also appropriate for financial
support in an area of work, designed and proposed by the third sector
organisation, that supports activities aligned with the Governments wider
objectives, for example hospice care.
5.4.6 Th Natinal Audit oics Successful Commissioning Guideshuld b
usd by cissins and thid sct pvids t assist in th
dtinatin th st apppiat unding ut. This can b undat www.na.g.uk/succssulcissining
31
http://www.nao.org.uk/successfulcommissioninghttp://www.nao.org.uk/successfulcommissioning -
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
34/44
The NHS commissioning environment: a guide for organisations in the third sector
It should be noted that the awarding of grants may still be on a
competitive basis. In addition, both funders and third sector organisations
need to be mindful of state aid issues when awarding grants.
5.5 Th pcunt pcssAdvtising NHS pcunts
5.5.1 It is now mandatory for all commissioners in the NHS to use the
Supply2Health portal for all healthcare service procurements. NHS
Supply2Health is an online resource that advertises opportunities to
provide Part B clinical services commissioned by the NHS in England.
The website also has details of contracts that have been awarded.
5.5.2 Supply2Health can be found at: www.supply2health.nhs.uk
Ky stags a al pcunt pcss
5.5.3 Competitive procurement approaches can vary and may be via an
invitation to tender, an invitation to negotiate or an any willing provider
route. If a service does go through a formal procurement process, the
key stages may include:
planning
affordability modelling
service specifications
key programme milestones
business case
Official Journal of the European Union (OJEU) advert
bidder expressions of interest (EOIs)
memorandum of information (MOI) and pre-qualification questionnaire(PQQ) issued
bidder information events
PQQ responses
bidder long list agreed and approved
invitation to tender (ITT) award of contract mobilisation
contract management.
32
http://www.supply2health.nhs.uk/http://www.supply2health.nhs.uk/ -
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
35/44
Becoming a service provider to the NHS
5.5.4 A procurement roadmap for community services has been developed to
support both commissioners and providers in explaining the potential
options when undertaking a competitive tender, and provides model
templates for each stage. This can be found at: www.pasa.nhs.uk/NR/
exeres/EE4ED689-03B5-4564-8070-B72E91B8376E.htm
Intnal itnss pups
5.5.5 Any organisation which is seeking to tender for the delivery of public
services must first of all ensure that it has a robust internal structure and
management arrangements which make it fit for purpose to do business
with the NHS. There are a number of resources which are available tosupport organisations in assessing their fitness for purpose. This guide is
intended to sit alongside these; however, there are two issues which an
organisation planning to provide NHS care may wish to take into account:
any relevant potential requirements of the pre-qualifying questionnaire(PQQ) within a tendering process; if an organisation does not meet
these, the tender cannot proceed beyond this stage of the process; and
the potential requirement to register with a regulator.
extnal quality assuanc gistatin
5.5.6 Many of the activities which are commissioned by the NHS are required to
be registered with a regulator. The role of the regulators and the
development of the Care Quality Commission is explained earlier in this
guide; the transitional arrangements for providers are summarised below.
5.5.7 All providers who are already registered under the Care Standards Act
2000 will be transferred across to a full registration system under the
Health and Social Care Act 2008 in 2010/11. Providers who set up new
services that fall within the scope of current registration systems will be
able to continue to apply under the current system in the run up to the
introduction of the new system. Any new providers making an application
from 1 July 2010 will do so against the requirements set under the Health
and Social Care Act 2008.
Picing
5.5.8 The flexibility in how much providers can charge will depend on which
services they are providing and the tendering process. It is important toremember that price alone will not determine the outcome of a tendering
process, and that other factors are also taken into account when assessing
33
http://www.pasa.nhs.uk/NR/http://www.pasa.nhs.uk/NR/ -
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
36/44
The NHS commissioning environment: a guide for organisations in the third sector
each bid for the value for money it offers. The three main factors are
efficiency, economy and effectiveness.
Natinal tai
5.5.9 A national tariff for mainly acute based care is in place for the NHS under
the principles of Payment by Results (PbR). The main aim of PbR is to
ensure that competition is based upon quality and not price. Key objectives
are to:
support patient choice and encourage hospitals to respond to patientpreferences;
encourage commissioners to arrange provision of effective care in themost appropriate settings;
reward hospitals for the work they do;
increase transparency of hospital funding; and
impose a sharper budget discipline on hospitals.
5.5.10 The national prices are based upon health resource groups, which group
together similar treatments and costs in relation to each patient spell. Thereare separate tariffs for elective and emergency care, and a market forces
factor to compensate for unavoidable regional cost differences. A national
tariff ensures that there is a fair playing field in pricing for providers,
regardless of sector, and will be extended in the future to include mental
health services. Pilots are under way to explore the potential of developing
a good practice structure for setting a local tariff for community health
services.
Nn-tai pics5.5.11 All other prices are determined locally via procurement and contracting to
reflect the direct and indirect costs of providing services, including the
potential to agree a reasonable margin for the provider.
full Cst rcvy
5.5.12 DH policy requires PCTs to adopt procurement practices that are fair and
open. This means that they must be neutral between different types of
providers and transparent with regard to pricing. This should minimise
transaction costs, and allow providers to frame realistic economic tenders.
34
-
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
37/44
Becoming a service provider to the NHS
Such an approach therefore reflects the need to ensure that there is the
potential for full cost recovery. It reflects the principles of full cost recovery
as set out by the National Audit Office, which can be found at:
www.nao.org.uk/publications/0607/full_cost_recovery.aspx
5.5.13 Organisations seeking to tender need to ensure that they calculate their
full cost recovery proportionate to the size of contract being tendered for,
and may include a contribution to surplus. They should then decide the
extent to which they wish to include these elements in any proposed price
in the context of a competitive tender.
5.5.14 Tenders will have a value for money assessment. This can includeconsideration of the social value added through the design of the service,
such as employing local people, contributing to community infrastructure,
access to additional services not funded through statutory sources and
reinvestment of surplus for community benefit.
Any Willing Pvid dls
5.5.15 The Any Willing Provider procurement option allows PCT to procure one
or more potential providers for the same service, at a consistent price. This
is a framework approach where level of income which each provider
receives will be directly related to the number of referrals or episode of
care, with patient choice driving competition to improve quality.
5.6 NHS cntacts5.6.1 There are different standard contracts which PCTs may use to contract for
services; a summary of the options and their key features is set out below.
It is mandatory for PCTs to use these standard national contracts for all
NHS contracted activities:
Acut, ntal halth and cunity halth ca svics
5.6.2 The contract is for use with all sectors; it provides a fair playing field
between all providers, and aims to encourage innovation and increase the
efficiency and quality of services. The contract has been written to ensure
that, regardless of the financial value, the standards and requirements for
any provider supplying NHS-funded care are the same.
35
http://www.nao.org.uk/publications/0607/full_cost_recovery.aspxhttp://www.nao.org.uk/publications/0607/full_cost_recovery.aspx -
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
38/44
The NHS commissioning environment: a guide for organisations in the third sector
5.6.3 The contract also places responsibilities upon commissioners to ensure
that there are appropriate market management behaviours regardless
of contract size. There are four types of contract, for
acute/secondary care
mental health, including learning disabilities
community services
ambulance services.
5.6.4 These contracts are all structured with various sections. One section
contains the standard legal components and nationally set standards.Another identifies standard issues where locally determined targets should
be agreed, and the third section is for local determination between the
PCT and service provider. The standardised approach is intended to reduce
the administrative burden for providers and commissioners. The contract
can be used for more than one service and if the range of services
increases, these can be added to the existing contract rather than requiring
another separate agreement. Commissioners also have the option to use
coordinated commissioning arrangements, which means that a single
contract canbe agreedfor servicesthat areprovidedto morethan onePCT.5.6.5 The normal duration of a contract should be three years; however, the
contract can be agreed for either a longer or shorter period if appropriate,
with agreement from the relevant SHA. This acknowledges the
Governments commitment to longer term funding for the third sector.
5.6.6 Payment is normally monthly. However, to reflect the principles of the
Compact (see Chapter 3) for smaller organisations where the contract value
is less than 130,000 per annumand
the provider organisation has fewerthan 50 whole time equivalent staff, prepayment can be agreed at a
local level.
Copies of the NHS standard contracts and further information,
including an email helpline, can be found at: www.dh.gov.uk/en/
Managingyourorganisation/Commissioning/Systemmanagement/
DH_085048
Piay dical svics cntacts
5.6.7 The majority of primary medical services contracts require the provisionof the full range of essential services to a registered list of patients. It is
important to note that while GPs are the only professionals qualified to
36
http://www.dh.gov.uk/en/http://www.dh.gov.uk/en/ -
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
39/44
Becoming a service provider to the NHS
deliver the full range of essential services to patients, the use of skill mix
will play an important part in effective service delivery.
5.6.8 Essential services form the core level of service that patients would expect
their GP to provide. These services are described in legislation to secure a
uniform basis across all primary medical services contracting routes. These
legal requirements are not subject to local negotiation (although there may
be some matters of local interpretation), thus ensuring that all patients
receive a consistent level of provision.
5.6.9. Where a potential primary medical services contractor is required to hold a
registered list of patients, and consequently to provide the full range ofessential services, there are three possible contracting routes which will be
determined by the commissioner. These are:
general medical services (GMS) contract;
personal medical services (PMS) agreement; or
alternative provider medical services (APMS) contract.
5.6.10 A single contractor may hold a variety of contract types with a variety of
commissioners. For example, an existing GMS contractor might also holdan APMS contract with a second PCT.
5.6.11 For more information about primary care contracts see
www.primarycarecontracting.nhs.uk/uploads/medical/pcc_provider_
guide__nov_06_final.pdf
37
http://www.primarycarecontracting.nhs.uk/uploads/medical/pcc_provider_http://www.primarycarecontracting.nhs.uk/uploads/medical/pcc_provider_ -
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
40/44
6. Cnclusin
6.1 We hope that this guide is helpful to third sector organisations. While it is
intended to give an overview rather than a detailed compendium of policy,
the key aim is to improve understanding of NHS commissioning, and how
to work with commissioners. This is a live document which we will review
from time to time to take account of policy developments. We would
therefore welcome feedback on areas which could be improved or where
additional information would be helpful in future editions.
If you have any comments please email us [email protected]
38
mailto:[email protected]:[email protected]:[email protected] -
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
41/44
-
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
42/44
-
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
43/44
-
8/9/2019 The NHS Commissioning Environment, A Guide for ion in the Third Sector
44/44
Crown copyright 2010


















