The Neurobiology of Drug Addiction The Neurobiology of Drug Addiction Glen R. Hanson, Ph.D., D.D.S....
70
The Neurobiology of Drug Addiction Glen R. Hanson, Ph.D., D.D.S. Director, Utah Addiction Center Professor of Pharmacology and Toxicology, U of U Senior Advisor, NIDA
-
date post
20-Dec-2015 -
Category
Documents
-
view
228 -
download
4
Transcript of The Neurobiology of Drug Addiction The Neurobiology of Drug Addiction Glen R. Hanson, Ph.D., D.D.S....

The Neurobiology of Drug Addiction
The Neurobiology of Drug Addiction
Glen R. Hanson, Ph.D., D.D.S.Director, Utah Addiction Center
Professor of Pharmacology and Toxicology, U of USenior Advisor, NIDA
Glen R. Hanson, Ph.D., D.D.S.Director, Utah Addiction Center
Professor of Pharmacology and Toxicology, U of USenior Advisor, NIDA

Drug Abuse and Addiction are Among the Most Serious
Public HealthProblems Facing Our Society
Drug Abuse and Addiction are Among the Most Serious
Public HealthProblems Facing Our Society
• and Frequently Coexist with Other Mental and Physical Disorders
• and Frequently Coexist with Other Mental and Physical Disorders

Americans’ Views of the Seriousnessof Health Problems(Top Ten of Thirty-Six Problems)
Americans’ Views of the Seriousnessof Health Problems(Top Ten of Thirty-Six Problems)
65%
65%
68%
69%
71%
73%
74%
75%
78%
82%
StressStress
Alcohol abuseAlcohol abuse
SmokingSmoking
Child abuseChild abuse
ViolenceViolence
HIV/AIDSHIV/AIDS
Heart diseaseHeart disease
Drunk drivingDrunk driving
CancerCancer
Drug abuseDrug abuse
% s
ayin
g “v
ery
seri
ous
pro
ble
m”
% s
ayin
g “v
ery
seri
ous
pro
ble
m”
Harvard School of Public Health/Robert Wood Johnson Foundation/ICR, August 2000Harvard School of Public Health/Robert Wood Johnson Foundation/ICR, August 2000
Drug abuseDrug abuse
SmokingSmoking
HIV/AIDSHIV/AIDS
Child abuseChild abuse
ViolenceViolence
StressStress
CancerCancer
Drunk drivingDrunk driving
Heart diseaseHeart disease
Alcohol abuseAlcohol abuse

Two Decades of NeurobiologicalResearch Have
Brought Us A New Understanding of Drug Abuse and Addiction, Their
Complexity and their Solutions
Two Decades of NeurobiologicalResearch Have
Brought Us A New Understanding of Drug Abuse and Addiction, Their
Complexity and their Solutions

We Know That DespiteTheir Many Differences, VirtuallyAll Abused Substances Enhance
Dopamine (neurotransmitter) Activity(particularly related to pleasure,
motor, and cognitive function
We Know That DespiteTheir Many Differences, VirtuallyAll Abused Substances Enhance
Dopamine (neurotransmitter) Activity(particularly related to pleasure,
motor, and cognitive function
For Example…For Example…
• Other pathways also involved!• Other pathways also involved!

Dopamine Pathways
Functions•reward (motivation)•pleasure,euphoria•motor function (fine tuning)•compulsion•perserveration•decision making
Serotonin Pathways
Functions•mood•memory processing•sleep•cognition
nucleusaccumbens
hippocampus
striatum
frontalcortex
substantianigra/VTA
raphe
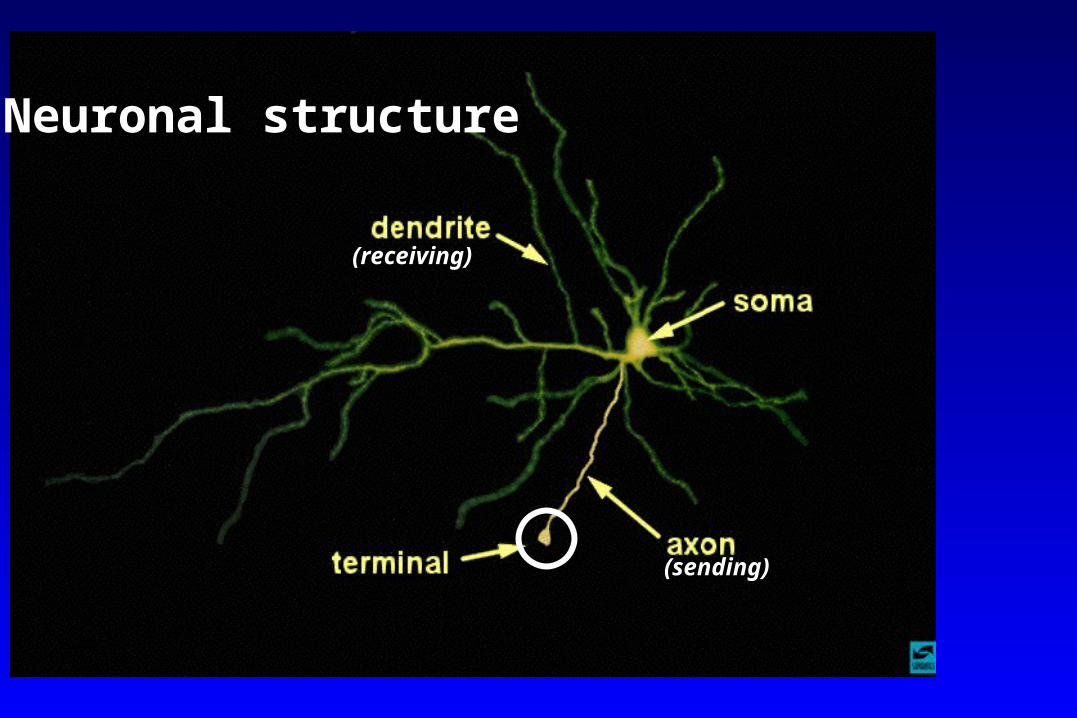
Neuronal structure
(receiving)
(sending)

/serotonin/serotonin
Vmat
transporterstimulationstimulation
DA/5HT DA/5HT
How some drugs of abuse cause dopamine release:• opioids narcotics (activate opioid receptors)• nicotine (activate nicotine receptors)• marijuana (activate cannabinoid receptors)• caffeine• alcohol (activate GABA receptors; an inhibitory transmitter)
How some drugs of abuse cause dopamine release:• opioids narcotics (activate opioid receptors)• nicotine (activate nicotine receptors)• marijuana (activate cannabinoid receptors)• caffeine• alcohol (activate GABA receptors; an inhibitory transmitter)
Drug :• cocaine• ritalin
vesicle Neuronal terminal

• Release DA from vesicles and reverse transporter
Drug Types:• Amphetamines -methamphetamine -MDMA (Ecstasy)
Vmat
transporter
serotonin/serotonin/
DA/5HT DA/5HT

00100100200200300300400400500500600600700700800800900900
1000100011001100
00 11 22 33 44 5 hr5 hr
Time After AmphetamineTime After Amphetamine
% o
f B
as
al
Re
lea
se
% o
f B
as
al
Re
lea
se
DADADOPACDOPACHVAHVA
AccumbensAccumbens AMPHETAMINEAMPHETAMINE
00
100100
200200
300300
400400
00 11 22 33 44 5 hr5 hrTime After CocaineTime After Cocaine
% o
f B
as
al
Re
lea
se
% o
f B
as
al
Re
lea
se
DADADOPACDOPACHVAHVA
AccumbensAccumbensCOCAINECOCAINE
00
100100
150150
200200
250250
00 11 22 3 hr3 hr
Time After NicotineTime After Nicotine
% o
f B
as
al
Re
lea
se
% o
f B
as
al
Re
lea
se
AccumbensAccumbensCaudateCaudate
NICOTINENICOTINE
Source: Di Chiara and ImperatoSource: Di Chiara and Imperato
Effects of Drugs on Dopamine ReleaseEffects of Drugs on Dopamine ReleaseEffects of Drugs on Dopamine ReleaseEffects of Drugs on Dopamine Release
100100
150150
200200
250250
00 11 22 33 4hr4hrTime After EthanolTime After Ethanol
% o
f B
as
al
Re
lea
se
% o
f B
as
al
Re
lea
se
0.250.250.50.5112.52.5
AccumbensAccumbens
00
Dose (g/kg ip)Dose (g/kg ip)
ETHANOLETHANOLETHANOLETHANOL
Much greaterActivity than anyOther drug of abuse -causes neurotoxicity

00
5050
100100
150150
200200
00 6060 120120 180180
Time (min)Time (min)
% o
f B
asal
DA
Ou
tpu
t%
of
Bas
al D
A O
utp
ut
NAc shellNAc shell
EmptyEmpty
BoxBox FeedingFeeding
Source: Di Chiara et al.Source: Di Chiara et al.
FOODFOOD
100100
150150
200200
DA
Co
nce
ntr
ati
on
(%
Bas
elin
e)D
A C
on
cen
tra
tio
n (
% B
asel
ine)
MountsMountsIntromissionsIntromissionsEjaculationsEjaculations
1515
00
55
1010
Co
pu
latio
n F
req
ue
nc
yC
op
ula
tion
Fre
qu
en
cy
SampleNumberSampleNumber
11 22 33 44 55 66 77 88 99 1010 1111 1212 1313 1414 1515 1616 1717
ScrScrScrScrBasBasFemale 1 PresentFemale 1 Present
ScrScrFemale 2 PresentFemale 2 Present
ScrScr
Source: Fiorino and PhillipsSource: Fiorino and Phillips
SEXSEX
Natural Rewards Elevate Dopamine LevelsNatural Rewards Elevate Dopamine LevelsNatural Rewards Elevate Dopamine LevelsNatural Rewards Elevate Dopamine Levels

Implication:Implication:
Elucidation of the mechanism of drug addiction will help to
understand other addictive andmotivational behaviors/disorders
Elucidation of the mechanism of drug addiction will help to
understand other addictive andmotivational behaviors/disorders

OFCOFCSCC
NAccNAccVPVP
REWARDREWARD
PFCPFC
ACGACG
INHIBITORY CONTROL
INHIBITORY CONTROL
MOTIVATION/DRIVE
(saliency)
MOTIVATION/DRIVE
(saliency)
Brain Circuits Involved in Drug Addiction
Brain Circuits Involved in Drug Addiction
HippHipp
AmygAmyg MEMORY/LEARNING MEMORY/
LEARNING

HOW DOES ADDICTION OCCUR? HOW DOES ADDICTION OCCUR?

• Principles of Behavior Dynamics
Behavior Tracts Compete for ExpressionBehavior Tracts Compete for Expression
Expression is Determined by (i) Dominance of Tracts, (ii) Strength of Prefrontal Cortex to Select, (iii) Relevance or saliency (orbitofrontal cortex)
Expression is Determined by (i) Dominance of Tracts, (ii) Strength of Prefrontal Cortex to Select, (iii) Relevance or saliency (orbitofrontal cortex)
AA
BC
PrefrontalCortex CCbehavior
expressedbehaviorexpressed BBbehaviorexpressed
Activation of Dopamine reward pathway initiates a behavior track
Activation of Dopamine reward pathway initiates a behavior track
dopamine initiated
(Miller & Cohen, Annu. Rev. Neurosci. 24 [2001] 167)
Orbito-frontal cortex

• Principles of Behavior Dynamics
AAC
B
PrefrontalCortex
How does a behavior become an addiction?
BBB BAddictionbehaviorexpressed
dopamine
Orbito-frontal cortex

Prolonged Drug Use Prolonged Drug Use ChangesChangesthe Brain and the Brain and
In FundamentalIn Fundamentaland Long-Lasting Waysand Long-Lasting Ways
Prolonged Drug Use Prolonged Drug Use ChangesChangesthe Brain and the Brain and
In FundamentalIn Fundamentaland Long-Lasting Waysand Long-Lasting Ways
We Have Generated A Lot of Evidence Showing That… We Have Generated A Lot of Evidence Showing That…

We Have Evidence That These Changes Can Be Both
Structural and Functional
We Have Evidence That These Changes Can Be Both
Structural and Functional
AND…AND…

Positron Emission TomographyPositron Emission Tomography
BRAIN IMAGINGBRAIN IMAGING
Magnetic Resonance ImagingMagnetic Resonance Imaging

control cocaine abuser
Decreases in Metabolism in Orbito Frontal Cortex (OFC)
Decreases in Metabolism in Orbito Frontal Cortex (OFC)
Volkow et al. Am. J. Psychiatry 148, 621Volkow et al. Am. J. Psychiatry 148, 621
Compromise assigning appropriate ValueCompromise assigning appropriate Value

Source: McCann U.D. et al., The Journal of Neuroscience, 18(20), pp. 8417-8422, October 15, 1998.Source: McCann U.D. et al., The Journal of Neuroscience, 18(20), pp. 8417-8422, October 15, 1998.
METH Suppresses Expression of DAT
(note: duration of use/3-20 yrs; abstinent/ 1-4 yrs)

Comparison Subject METH AbuserComparison Subject METH Abuser
Dopamine Transporter Loss AfterHeavy Methamphetamine Use
(PET analysis)
Source: Volkow, N.D. et al., Am J. Psychiatry, 158(3), pp. 377-382, 2001. Source: Volkow, N.D. et al., Am J. Psychiatry, 158(3), pp. 377-382, 2001.

Dependence of Verbal Memory on Striatal Dependence of Verbal Memory on Striatal DATDAT
Dependence of Verbal Memory on Striatal Dependence of Verbal Memory on Striatal DATDAT
0
3
6
9
12
15
1 1.2 1.4 1.6 1.8 2
Dopamine transporter (Bmax/Kd)
Num
ber
of w
ords
0
3
6
9
12
15
1 1.2 1.4 1.6 1.8 2
Dopamine transporter (Bmax/Kd)
Num
ber
of w
ords
0
3
6
9
12
15
1 1.2 1.4 1.6 1.8 2
Dopamine transporter (Bmax/Kd)
Num
ber
of w
ords
0
3
6
9
12
15
1 1.2 1.4 1.6 1.8 2
Dopamine transporter (Bmax/Kd)
Num
ber
of w
ords
R = 0.70R = 0.70p < 0.005p < 0.005R = 0.70R = 0.70p < 0.005p < 0.005
R = 0.64R = 0.64p < 0.01p < 0.01R = 0.64R = 0.64p < 0.01p < 0.01
Interference recallInterference recallInterference recallInterference recall Delayed recallDelayed recallDelayed recallDelayed recall
Source: Volkow, N.D. et al., Am J. Psychiatry, 158(3), pp. 377-382, 2001. Source: Volkow, N.D. et al., Am J. Psychiatry, 158(3), pp. 377-382, 2001.
Compromises Cognitive FunctionsCompromises Cognitive Functions

MOTOR FUNCTIONMOTOR FUNCTION
• Slowed gait• Slowed gait
•Impaired balance•Impaired balance
• Impairment correlates with damage to dopamine system• Impairment correlates with damage to dopamine system

Implication:Implication:
Brain changes resulting from prolonged use of psychostimulants,
such as methamphetamine may be reflected in compromised cognitive and motor functioning
Brain changes resulting from prolonged use of psychostimulants,
such as methamphetamine may be reflected in compromised cognitive and motor functioning

Is There Recovery?Is There Recovery?
• Good News: After 2 years some of the dopamine deficits are recovering
• Good News: After 2 years some of the dopamine deficits are recovering
• Bad News: Functional deficits persist• Bad News: Functional deficits persist
• What does this mean???• What does this mean???

Reward System in AddictionReward System in Addiction
CocaineCocaine
FoodFood
Ac t
i vit
y o
f R
e war
d S
yst e
m
METHMETH
AlcoholAlcohol
Ability to Experience Rewards Is DamagedAbility to Experience Rewards Is Damaged
con
trol
s
trea
ted
More
Less

Get Rewired by Drug UseGet Rewired by Drug Use
Their Brains…Their Brains…

INHERITED FACTORS(genetic vulnerability-not inevitability)
INHERITED FACTORS(genetic vulnerability-not inevitability)
• Common strategy to investigate are Twin Studies• Common strategy to investigate are Twin Studies
In General: Inheritability for Drug Abuse Ranges From 40-60%In General: Inheritability for Drug Abuse Ranges From 40-60%
• Some Variability Between Drugs• Some Variability Between Drugs
• Some Gender Variability• Some Gender Variability

17172222
r-SA
r-candidate
r-SA
r-candidate
55 66 3 samples, > 2 labs4 samples, > 3 labs
>2 samples, >2 labs
3 samples, > 2 labs4 samples, > 3 labs
>2 samples, >2 labs
Chromosomal Locations for Substance Abuse Vulnerability Loci Chromosomal Locations for Substance Abuse Vulnerability Loci
Uhl et al Tr Genetics, updated June 03Uhl et al Tr Genetics, updated June 03

Complex geneticsComplex genetics
Complex phenotypes (expressions)Complex phenotypes (expressions)
(Relation to Risk Factors?)(Relation to Risk Factors?)

VULNERABILITY to What?VULNERABILITY to What?Starting Drug Use?
Liking Drugs More?
Continuing Drug Use?
Becoming Addicted?
Specific to A Particular Drug?
Starting Drug Use?
Liking Drugs More?
Continuing Drug Use?
Becoming Addicted?
Specific to A Particular Drug?

For Example-Contribution of Genetic Factors to:
Nicotine-Nicotine-
•Liability to initiate=56%•Liability to initiate=56%• Transition to dependence=70%• Transition to dependence=70%
• Smoking persistence= >50%• Smoking persistence= >50%
(Lerman & Berrettine, Amer. J. Med. Gen. 54 (2003) 48)(Lerman & Berrettine, Amer. J. Med. Gen. 54 (2003) 48)

Genetics May Influence HowNeurobiology Interacts With Environment
Genetics May Influence HowNeurobiology Interacts With Environment

GeneticsGeneticsGeneticsGenetics
EnvironmentEnvironmentEnvironmentEnvironment
Gene/Gene/EnvironmentEnvironmentInteractionInteraction
Gene/Gene/EnvironmentEnvironmentInteractionInteraction

PET Images:PET Images:Dopamine Receptor DensityDopamine Receptor Density
PET Images:PET Images:Dopamine Receptor DensityDopamine Receptor Density
MoreMore likelylikelyto self-to self-administeradministerCocaineCocaine
MoreMore likelylikelyto self-to self-administeradministerCocaineCocaine

Effect of Social Dominance on CocaineEffect of Social Dominance on CocaineSelf -AdministrationSelf -Administration
*
*
.003 .01 .03 .1
0.0
0.5
1.0
1.5
2.0 TOTAL INTAKE(mg/kg/session)
Cocaine (mg/kg/injection)
Subordinate
Dominant
Mea
n i
nta
ke/s
essi
on
(m
g/k
g)

Addictive Disorders Often Co-Exist Addictive Disorders Often Co-Exist with or Predispose to Mental Disorderswith or Predispose to Mental Disorders
DSM IV Manual: Devotes ~ 100 pages to describing addiction and dependence disorders
DSM IV Manual: Devotes ~ 100 pages to describing addiction and dependence disorders
Discusses substance abuse as a confound to diagnosis and Tx Discusses substance abuse as a confound to diagnosis and Tx
National ComorbidityNational ComorbiditySurvey (NCS)Survey (NCS)
Nearly halfNearly half of individuals with a of individuals with a past yearpast yearsubstance use disorder also had a mentalsubstance use disorder also had a mentaldisorderdisorder
Mental disorders found to be Mental disorders found to be most prevalentmost prevalentincluded included affectiveaffective disorders, disorders, anxietyanxiety disorders, disorders,personalitypersonality disorders, and disorders, and psychoticpsychotic disorders disorders
Nearly halfNearly half of individuals with a of individuals with a past yearpast yearsubstance use disorder also had a mentalsubstance use disorder also had a mentaldisorderdisorder
Mental disorders found to be Mental disorders found to be most prevalentmost prevalentincluded included affectiveaffective disorders, disorders, anxietyanxiety disorders, disorders,personalitypersonality disorders, and disorders, and psychoticpsychotic disorders disorders
(Note: can we have parity for mental health with- out considering drug abuse?)(Note: can we have parity for mental health with- out considering drug abuse?)

Common Underlying NeurobiologicalFactors Can Be:
Common Underlying NeurobiologicalFactors Can Be:
Structural/anatomical (same regions and pathways)Structural/anatomical (same regions and pathways)
Neurochemical (imbalance of neurotransmitters)Neurochemical (imbalance of neurotransmitters)
Genetic (inherited factors that compromise function) Genetic (inherited factors that compromise function)

Because of this overlap, drugs of abusecan cause symptoms that mimic
most forms of mental illness
Because of this overlap, drugs of abusecan cause symptoms that mimic
most forms of mental illness

Drug DisorderCocaine and MethamphetamineCocaine and Methamphetamine Schizophrenia, paranoia,
anhedonia, compulsivebehavior
Schizophrenia, paranoia,anhedonia, compulsivebehavior
StimulantsStimulants Anxiety, panic attacks, mania and sleep disordersAnxiety, panic attacks, mania and sleep disorders
LSD, Ecstasy & psychedelicsLSD, Ecstasy & psychedelics Delusions and hallucinationsDelusions and hallucinations
Alcohol, sedatives, sleepaids & narcoticsAlcohol, sedatives, sleepaids & narcotics
Depression and mood disturbancesDepression and mood disturbances
PCP & KetaminePCP & Ketamine Antisocial behaviorAntisocial behavior

Some drugs of abuse have a mechanism of action similar to
that of drugs used as psychotherapeutic agents
Some drugs of abuse have a mechanism of action similar to
that of drugs used as psychotherapeutic agents
Significance: rationale for
self-administrationSignificance: rationale for
self-administration

Serotonin/dopamine synaptic terminal
Synaptic vesicle
Postsynaptictarget
Activate transmitter receptors
Causes an effectCauses an effect
transporterProzac,Ritalin, &Cocaineblock

Chronic use of some of these drugs ofabuse may alter the way the brain
functions, making persons particularlysusceptible to mental illness
Chronic use of some of these drugs ofabuse may alter the way the brain
functions, making persons particularlysusceptible to mental illness

Double
People With Comorbid Mental and Addictive DisordersHave a Brain Disease
People With Comorbid Mental and Addictive DisordersHave a Brain DiseaseDoubleDouble
MentalDisorder
MentalDisorder
AddictiveDisorder
AddictiveDisorder
ComorbidDisordersComorbidDisorders

Role of Stress and TraumaRole of Stress and Trauma

The Stress Hormone CycleThe Stress Hormone Cycle
HypothalamusHypothalamus
PituitaryGland
PituitaryGland
AdrenalGlands
AdrenalGlands
KidneysKidneys
CRFCRF
ACTHACTHCORTISOLCORTISOL
Stress ResponsesStress ResponsesStress ResponsesStress ResponsesStress ResponsesStress ResponsesStress ResponsesStress Responses
CRF:Corticotropin ReleasingFactor
CRF:Corticotropin ReleasingFactor

DRUG USEDRUG USE(Self-Medication)(Self-Medication)DRUG USEDRUG USE
(Self-Medication)(Self-Medication)
STRESSSTRESSSTRESSSTRESS
CRFCRFCRFCRF
AnxietyAnxietyAnxietyAnxiety
CRFCRFCRFCRF
AnxietyAnxietyAnxietyAnxiety
What Role Does Stress Play In Initiating Drug Use?
What Role Does Stress Play In Initiating Drug Use?

ProlongedProlongedDRUGDRUGUSEUSE
ProlongedProlongedDRUGDRUGUSEUSE
AbstinenceAbstinenceAbstinenceAbstinence
RELAPSERELAPSERELAPSERELAPSE
CRFCRFCRFCRF
AnxietyAnxietyAnxietyAnxiety
What Happens When A Person Stops Taking A Drug?
What Happens When A Person Stops Taking A Drug?

Stress Reliably Reinstates Drug Seeking in RatsStress Reliably Reinstates Drug Seeking in Rats
SalineSaline NicotineNicotine
Nicotine-trained ratsNicotine-trained rats
FootshockFootshock
SalineSaline CocaineCocaine FootshockFootshock WaterWater AlcoholAlcohol FootshockFootshock
Cocaine-trained ratsCocaine-trained rats Alcohol-trained ratsAlcohol-trained rats
00
2020
40406060
8080100100
Res
pon
ses
Res
pon
ses Inactive LeverInactive Lever
Active LeverActive Lever
SalineSaline HeroinHeroin FootshockFootshock
Heroin-trained ratsHeroin-trained rats
**
*
*
* **
*
00
2020
40406060
8080100100
Res
pon
ses
Res
pon
ses
From: Psychopharmacology, 1996, 1998, 1999 ; J. Neurosci. 1996From: Psychopharmacology, 1996, 1998, 1999 ; J. Neurosci. 1996

CRF1 Receptor Antagonist AttenuatesStress-Induced Reinstatement
of Drug Seeking
CRF1 Receptor Antagonist AttenuatesStress-Induced Reinstatement
of Drug SeekingAlcohol-trained ratsAlcohol-trained rats
From: Shaham et al. Psychopharmacology 1998; Le et al. Psychopharmacology, 2000From: Shaham et al. Psychopharmacology 1998; Le et al. Psychopharmacology, 2000
CP-154,526 Dose (mg/kg, SC)CP-154,526 Dose (mg/kg, SC)
Intermittent Footshock Intermittent Footshock No stressNo stress
Heroin-trained ratsHeroin-trained rats Cocaine-trained ratsCocaine-trained rats
00 1515
*
3030
*
00
1515
3030
4545
6060
Res
pon
ses
(3 h
r)R
esp
onse
s (3
hr)
*
*
00 1515 3030
*
00
1515
3030
4545
6060
Res
pon
ses
(1 h
r)R
esp
onse
s (1
hr)
00 1515 3030

Use the Science Use the Science

We Are Capitalizing onBasic Science Discoveries in the Design
Of Behavior Therapies andMedications
To Treat Addiction
We Are Capitalizing onBasic Science Discoveries in the Design
Of Behavior Therapies andMedications
To Treat Addiction

Objectives of Intervention:
• Rearrange dominance of behavior tracks• Rearrange dominance of behavior tracks contingency management (vouchers) contingency management (vouchers)
motivational enhancement motivational enhancement
therapeutic communities therapeutic communities

• Principles of Behavior Dynamics
AA
BC
PrefrontalCortex CCbehavior
expressedbehaviorexpressed BBbehaviorexpressed
dopamine initiated
Orbito-frontal cortex

• Strengthen prefrontal cortex influence (change thinking process)• Strengthen prefrontal cortex influence (change thinking process)
cognitive and cognitive behavioral tx (unlearn old habits-suppress; learn new skills)
cognitive and cognitive behavioral tx (unlearn old habits-suppress; learn new skills) assertiveness training (suppress and express)
assertiveness training (suppress and express)

• Principles of Behavior Dynamics
AA
BC
PrefrontalCortex CCbehavior
expressedbehaviorexpressed BBbehaviorexpressed
dopamine initiated
Orbito-frontal cortex

•Alter function of orbitofrontal (saliency) cortex•Alter function of orbitofrontal (saliency) cortex
motivational therapy motivational therapy
family therapies family therapies

• Principles of Behavior Dynamics
AA
BC
PrefrontalCortex CCbehavior
expressedbehaviorexpressed BBbehaviorexpressed
dopamine initiated
Orbito-frontal cortex

• Recovery of function (frontal and obito- frontal cortex)• Recovery of function (frontal and obito- frontal cortex)
all treatments that keep brain away from drugs for extended time
all treatments that keep brain away from drugs for extended time

• Principles of Behavior Dynamics
AA
BC
PrefrontalCortex CCbehavior
expressedbehaviorexpressed BBbehaviorexpressed
dopamine initiated
Orbito-frontal cortex

• Alleviate underlying psychiatric disorder• Alleviate underlying psychiatric disorder
administer: Antidepressants for depression
Ritalin for ADHD
Sedatives for anxiety
administer: Antidepressants for depression
Ritalin for ADHD
Sedatives for anxiety

Targets of MedicationTargets of Medication
• Methadone, LAAM and Buprenorphine• Methadone, LAAM and Buprenorphine
Activate opioid receptorsActivate opioid receptors
• Nicotine gum/patch• Nicotine gum/patch
Activate nicotinic receptorsActivate nicotinic receptors
• Naloxone• NaloxoneBlock opioid receptorsBlock opioid receptors

Vmat
transporterstimulationstimulation
DA DA
How some drugs of abuse cause dopamine release:• opioids narcotics (activate opioid receptors)• nicotine (activate nicotine receptors)
How some drugs of abuse cause dopamine release:• opioids narcotics (activate opioid receptors)• nicotine (activate nicotine receptors)
vesicle Neuronal terminal

• Psychostimulants• PsychostimulantsEnhancing GABA-ergic inhibition (baclofen-muscle relaxant; anti-seizure- Tiagabine)
Enhancing GABA-ergic inhibition (baclofen-muscle relaxant; anti-seizure- Tiagabine)
Cannabinoid antagonist (rimonabant)Cannabinoid antagonist (rimonabant)

• Principles of Behavior Dynamics
AA
BC
PrefrontalCortex CCbehavior
expressedbehaviorexpressed BBbehaviorexpressed
dopamine initiated
Orbito-frontal cortex
GABA and cannabinoidsystems critical forfunction
GABA and cannabinoidsystems critical forfunction

• Relieve stress-related drug abuse• Relieve stress-related drug abuse
CRF antagonistCRF antagonist
ProlongedProlongedDRUGDRUGUSEUSE
ProlongedProlongedDRUGDRUGUSEUSE
AbstinenceAbstinenceAbstinenceAbstinence
RELAPSERELAPSERELAPSERELAPSE
CRFCRFCRFCRF
AnxietyAnxietyAnxietyAnxiety

Science is helping to improve our strategies and successesScience is helping to improve our strategies and successes
To be successful, treatment is a Lifetime ProcessTo be successful, treatment is a Lifetime Process
Consequence: There is no
“cure”…
Consequence: There is no
“cure”…











![Neurobiology of Addiction presentation [Autosaved]](https://static.fdocuments.net/doc/165x107/61df190bd25d6301594124e7/neurobiology-of-addiction-presentation-autosaved.jpg)