
The Laboratory Medicine of Infectious Diseases
66
The Laboratory Medicine of Infectious Diseases Professor C W K Lam Department of Chemical Pathology The Chinese University of Hong Kong Prince of Wales Hospital Hong Kong
Transcript of The Laboratory Medicine of Infectious Diseases

The Laboratory Medicine of Infectious Diseases
Professor C W K LamDepartment of Chemical PathologyThe Chinese University of Hong KongPrince of Wales HospitalHong Kong

13 December 2004
15 May 2006

H1N1 Spanish flu 1918, H2N1 Asian flu 1957, H3N2 Hong Kong flu 1968
Courtesy Professor Paul K S Chan, Microbiology, CUHK-PWH

Palese P. Nature Medicine 2004; 10:S82-7

Mid 1990s : Receding infectious diseases
Late 1990s : > 30 emerging infections
Legionnaires HIV / AIDS
BSE / vCJD Nipah virus
SARS (2003) HPAI (since 2004)
Strep sius (2005) Chikungunya (2005-6)

Attack of HIV on T-Cells
High infectivity, long disease progression, high mortality
Drug-resistant pulmonary tuberculosis

TB: 1/3 world population is infected8.7 M new cases per year with 1.7 M deaths (40 M in 25 years)
HIV / AIDS Drive TB Epidemic∗ promotes progression of recently
acquired TB∗ reactivates latent TB∗ facilitates transmission in community∗ changes clinical and laboratory
presentations

HIV infection / Immunosuppression / Immunodeficiency:
T-helper (CD4+) lymphocyte deficiency ===> IFNγ ===> MØ activation ===> intracellular growth of Mycobacterium tuberculosis

14:00 h Infection in the Immunocompromised Child(Seminar Room 1, 2/F, PWH) SCID / post BMT



Emerging Infectious Diseases (2006), 12:894 – 899.
Severe Community-acquired Pneumonia Due to
Staphylococcus aureus, 2003-04 Influenza Season
Jeffrey C Hageman,* Timothy M. Uyeki,* John S. Francis,† Daniel B. Jernigan,* J. Gary Wheeler,‡ Carolyn B. Bridges, § Stephen J. Barenkamp,¶ Dawn M. Sievert,
Arjun Srinivasan,* Meg C. Doherty, ‡ Linda K. McDougal,* George E. Killgore,* Uri A. Lopatin,# Rebecca Coffman,** J. Kathryn MacDonald, †† Sigrid K. McAllister,*
Gregory E. Fosheim,* Jean B. Patel,* and L. Clifford McDonald*

H5N1 Avian Influenza in China, Indochina and Europe
Adapted from Assoc Prof David S C Hui, Respiratory Medicine, CUHK-PWH
2008: 63% of 383 WHO: 100M 2005: NEJM Dec


Courtesy Dr S F Lui
(October 2005)

M 31 yrs: exposure to dead chicken 5 days before illness (onset 3/1/04). Temp 400C, malaise, dry cough, SOB, headache for 2 days. His 2 sisters died of confirmed H5N1 2 weeks later. (Courtesy Dr David Hui, Respiratory Medicine, CUHK-PWH)
5/1/04
Died 9/1/04
WBC 2.5, L=0.6
Platelets 57
ALT 109, AST 322, CK
Sore throat, ± diarrhoeaARDSHaemophagocytic syndrome (clinical and laboratory)MOF, DIC
* Rapid lung destruction (Dr J Farrar, Oxford)* Reye’s syndrome (Dr D Hui, Hong Kong)

• F/6 yr, fever for 8 days, developed acute respiratory distress.• Adm WBC 2.4 x 109/L, L 0.5 x 109/L, plt 127 x 109/L, ALT 246 IU/L, AST 1379
IU/L, nasal swab H5 Ag +ve.• Given Methylpred 5 mg/kg/day and Tamiflu. Died 3 days after adm.
CXR on admission CXR 6 hours after admission
CXR on day 2 CXR on day 3
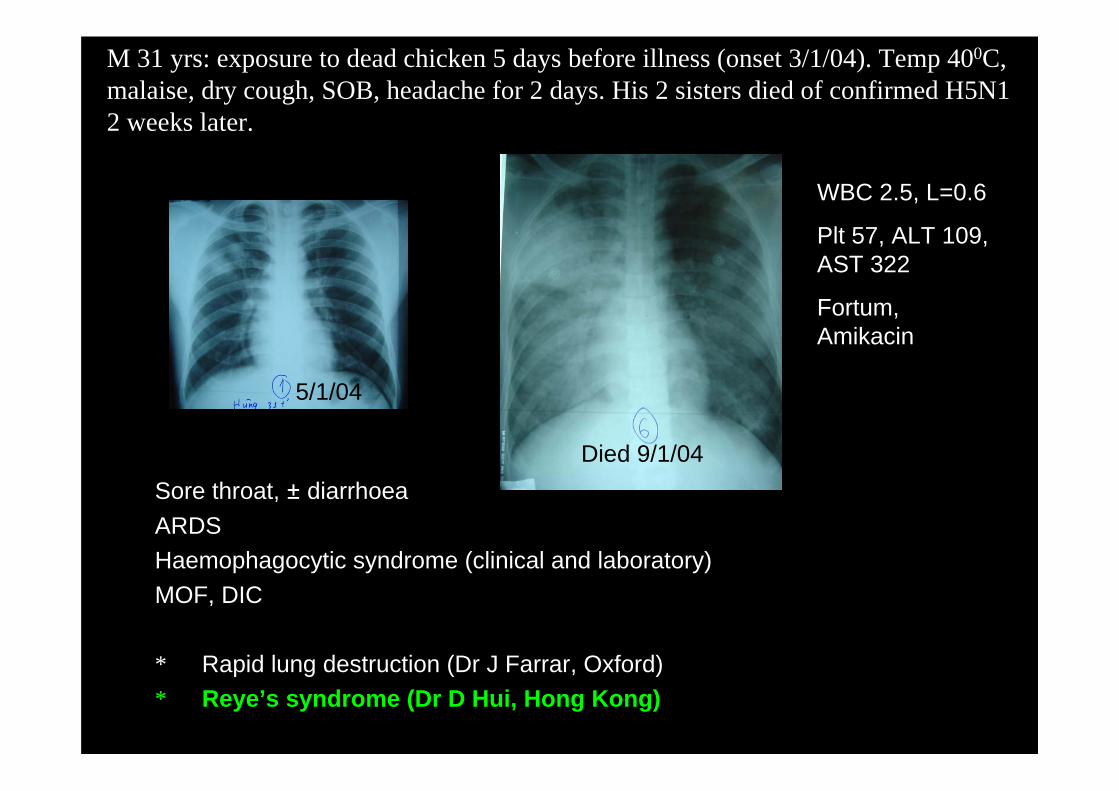
M 31 yrs: exposure to dead chicken 5 days before illness (onset 3/1/04). Temp 400C, malaise, dry cough, SOB, headache for 2 days. His 2 sisters died of confirmed H5N1 2 weeks later.
5/1/04
Died 9/1/04
WBC 2.5, L=0.6
Plt 57, ALT 109, AST 322
Fortum, Amikacin
Sore throat, ± diarrhoeaARDSHaemophagocytic syndrome (clinical and laboratory)MOF, DIC
* Rapid lung destruction (Dr J Farrar, Oxford)* Reye’s syndrome (Dr D Hui, Hong Kong)


• PREPAREDNESS* Cultural and Socio-economic* Public Health* Laboratory Response
December 2004
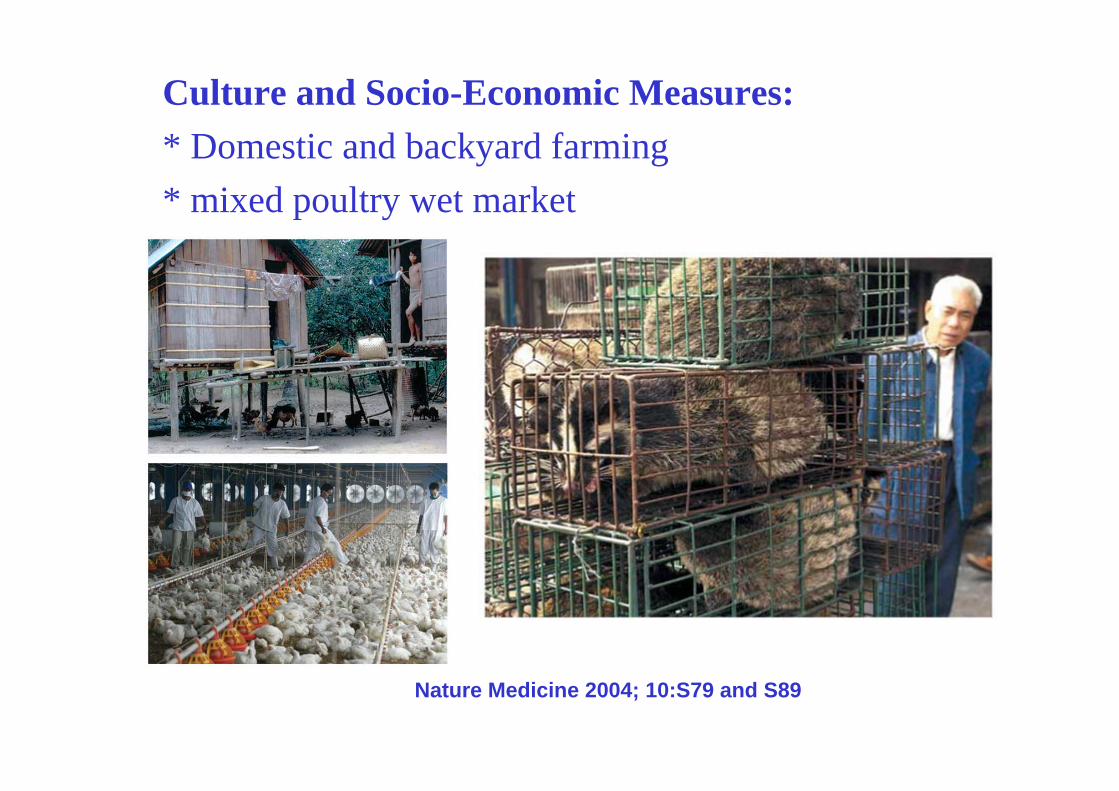
Culture and Socio-Economic Measures:* Domestic and backyard farming* mixed poultry wet market
Nature Medicine 2004; 10:S79 and S89

Public Health MeasuresAnti-influenza Drugs : (1) M2 channel blocker
(2) NA inhibitor
Palese P. Nature Medicine 2004; 10:S82-6

Public Health Measures : Vaccines
* Antigenic Variation (drift and shift)
(1) A / New Caledonia H1N1(2) A / Fujian H3N2 (Wisconsin H3N2)(3) B / Shanghai (Malaysia)
(N) A / California H3N2
* Reverse Genetics (transfection of plasmids)(1) Construct actual vaccine candidate(2) Improve attenuation

H5N1 Avian Influenza in China, Indochina and Europe
Adapted from Assoc Prof David S C Hui, Respiratory Medicine, CUHK-PWH
2008: 63% of 383 WHO: 100M 2005: NEJM Dec

THE CHINESE UNIVERSITY OF HONG KONGDEPARTMENT OF MEDICINE & THERAPEUTICS
Medical Grand Round
Molecular and Immunological Aspects of SARS
by
Dr Rossa Chiu (Molecular Epidemiology)DLo
Dr Michael Chan (Chemical Pathology)CL
Dr C K Wong (Clinical Immunology)CL
Dr Allen Chan (Molecular Diagnostics)DLo
DEPARTMENT OF CHEMICAL PATHOLOGY
Moderator: Dr C W K Lam

Table 1. Summary of SARS cases with onset of illness from 1 November 2002 to 31 July 2003. WHO
Area Number of Cases
Median Age (range)
Number of Deaths (%)
Number of HCW* Infected (%)
Date of First & Last Cases
Australia 6 15 (1-45) 0 (0) 1 (16) 26/2/03 – 1/4/03 Canada 251 49 (1-98) 43 (17) 109 (43) 23/2/03 – 12/6/03 China 5281 Pending 349 (6.6) 1002 (19) 16/11/03 – 3/6/03 Hong Kong 1755 40 (0-100) 299 (17) 386 (22) 15/2/03 – 31/5/03 Singapore 238 35 (1-90) 33 (14) 97 (41) 25/2/03 – 5/5/03 Taiwan 346 42 (0-93) 37 (11) 68 (20) 25/2/03 – 15/6/03 Others 221 13 (5.9) 44 (17)
29 8098 774 (9.6) 1707 (21)
* HCW = healthcare workers
SARS-CoV (32 kB): Droplet Transmission
Lam CWK, Chan MHM, Wong CK. Clin Biochem Rev 2004; 25: 121-32.

Table 2. Clinical and general laboratory manifestations of SARS in adult patients.
The Chinese University of Hong Kong27
Patient population 66 men, 72 women 69 healthcare workers, mean ± SD age = 39. ± 17 years
Incubation period 2-16 days (median 6 days) Clinical presentations Fever (100%)
Chills ± rigor (73.2%) Myalgia (60.9%) Cough (57.3%) Headache (55.8%) Dizziness (42.8%) Sputum production (29.0)%) Sore throat (23.2%) Coryza (22.5%) Nausea and vomiting (19.6%) Diarrhoea (19.6%)
Radiological findings At the onset of fever, 78.3% had abnormal CXR (air-space consolidation) 54.6% unilateral focal involvement, 45.4% either unilateral multifocal or bilateral
General Laboratory findings
Lymphopenia (69.6%) Thrombocytopenia (44.8%) Prolonged APTT (42.8%) ↑D-dimer (45.0%) ↑ALT (23.4%) ↑LDH (71.0%) ↑CK (32.1%) Hyponatremia (20.3%) Hypokalemia (25.2%)
(1) Active Viral Infection
(2) Hyperactive Immune Response
(3) Recovery or pulmonary destruction
Tx: Antibiotics, ribavirin, oral/iv ± pulse steroid, TCM; Pentaglobin, Kaletra, convalescent serum.

Hotel MHotel M
Hong KongHong Kong


13 April
15 April
16 April



Prince of Wales Hospital
Department of Chemical Pathology

The Chinese University of Hong Kong
Department of Chemical Pathology



NT East Cluster
The Chinese University of Hong
Kong (CUHK) - Main Campus
Alice Ho Miu Ling Nethersole Hospital -
600-bed Acute General Hospital
North District Hospital -600-bed Acute General
Hospital nearest to China border
Prince of Wales Hospital -
1400-bed CUHK Teaching Hospital

Medical Year 1 End-of-Year Exam 2003-2004 Scenario and MCQ on PHOM1: Acid-Base and Electrolyte Homeostasis (Jan 2004 from C W K Lam) During the Lunar New Year holidays, a 63-old lady visited her relatives in Guangzhou for a week and developed watery diarrhea for two days before her return to Hong Kong. At the Lo Wu border she was found to run a fever of 38.50C and admitted to the Isolation & Triage Ward of Prince of Wales Hospital for suspected SARS. On admission she looked very tiredwith dry lips and sunken eyes. Laboratory tests on admission showed the following: Arterial blood and venous plasma Reference Interval ________________________________________________________________ Na 145 mmol/L 134 - 145 : pH 7.31 7.35 - 7.45 : SARS Corona Virus RNA = negative

Anti-virus antibody testing in blood
Peiris JS, Chu CM, Cheng VC, et al. Lancet 2003; 361: 1767

Why a blood test?
Early viraemic phaseCirculates through all affected organsSafe to collectEasy to handleAllows quantification
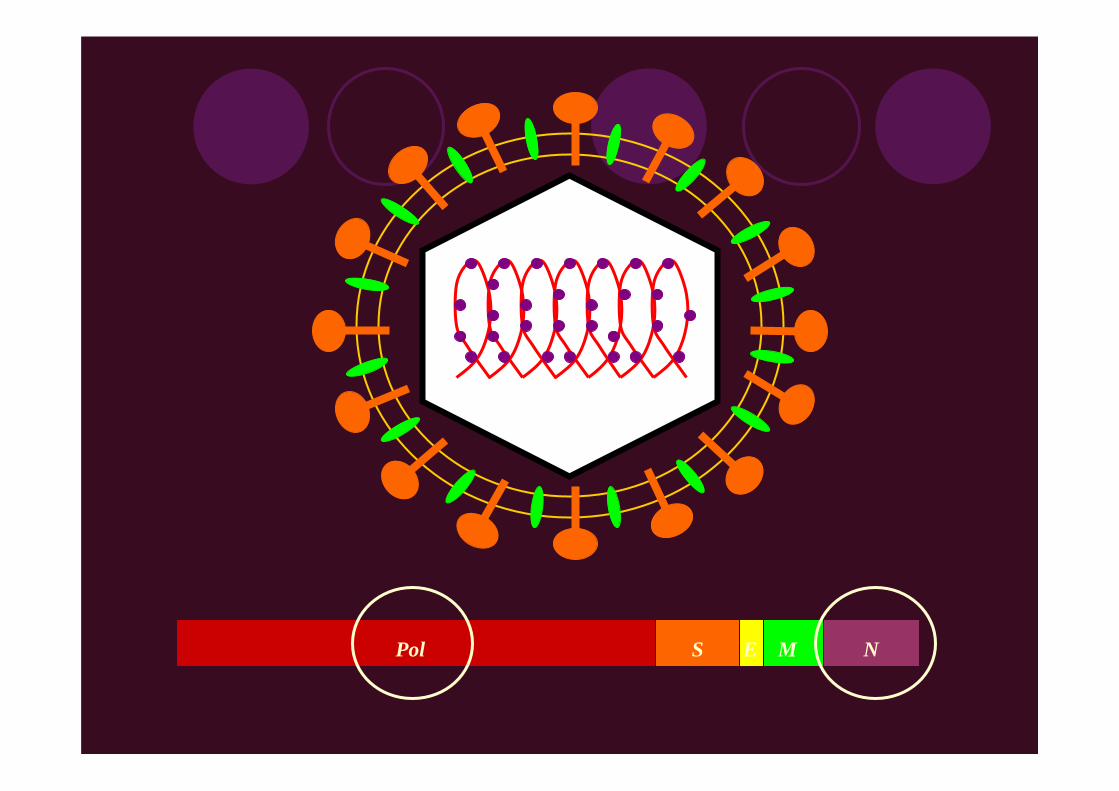
Pol S E M N

SARS-CoV RNA in Serum / Plasma
Archived serum samples23 SARS patientsAdmission mean 2.6 days after fever onset (range: 1 to 6 days)Pol RT-PCRAdmission samples: 78%30 non-SARS patients: 0%Good correlation with N RT-PCR
Ng EK, Hui DS, Chan KCA, et al. Clin Chem 2003; 326:850.

ICU and non-ICU patientsDay 1 of Admission
ICU(n=11)
non-ICU(n=12)
Seru
m S
AR
S C
oV(c
opie
s/m
l)
0
10
100
1000
10000
100000
1000000
10000000p=0.002, Mann-Whitney test30 times

Electronic request
QuestionnaireFresh
specimenECPath registrationElectronic reporting
TAT – 1 to 1.5 daysManual extraction 3 hoursReal-time PCR 3 hours


MALDI-TOF-MS
Matrix-Assisted Lazer Desorption Ionization Time-of-Flight Mass Spectrometry

AccurateFast: 3000 samples/day

Chemical Pathology & Clinical Immunology
Biochemical Markers of Bone Metabolism -Steroid-Induced Osteonecrosis (1 paper)
Serum LDl and Lymphocyte Subsets -Prognostic Indicators (1 review + 3 papers)
Plasma Cytokines and Chemokines -Immunopathophysiology (4 papers)

Pathophysiology of SARS poorly understood
Age > 60 years and serum LD > 300 U/L ==> adverse outcomes (138, 227 and 151 patients)
Lymphocytes <1000/µL in 98% of 157 patients ==> disease severity
109 patients ==> daily blood samples for serum total LD and LD isoenzymes; CBP, WBC and DC, and lymphocyte subsets

Serum total LD : lactate-to-pyruvate assay
LD isoenzymes at peak LD : gel electrophoresis
Lymphocyte subsets : fluorescence flow cytometry
CD56B-Lymphocytes
CD16Natural Killer Cells
CD8T-Suppressor Lymphocytes
CD4T-Helper Lymphocytes
CD3Total T-lymphocytes
ImmunophenotypingSubpopulation

Multiple ROC curve comparison of age, serum total LDH activity, serum LD1 activity, serum LD1/LD2 ratio, blood total haemoglobinconcentration, and blood absolute lymphocyte count for the prediction of death

Tissue destruction in SARS-CoV infection ==> serum total LD
LD1 major contributor of total LD ==> LD1 also from tissue destruction
Chan MHM, Wong VWS, Wong CK, et al. J Int Med 2004; 255:512.
Ribavirin ==> 20 g/L decrease in Hb ===> LD1Wong RSM, Wu A, To KF, et al. BMJ 2003; 326:1358.
LD1 assay using same automation Onigbinde TA, Wu AH, Johnson M, et al. Clin Chem 1990; 36:1819.
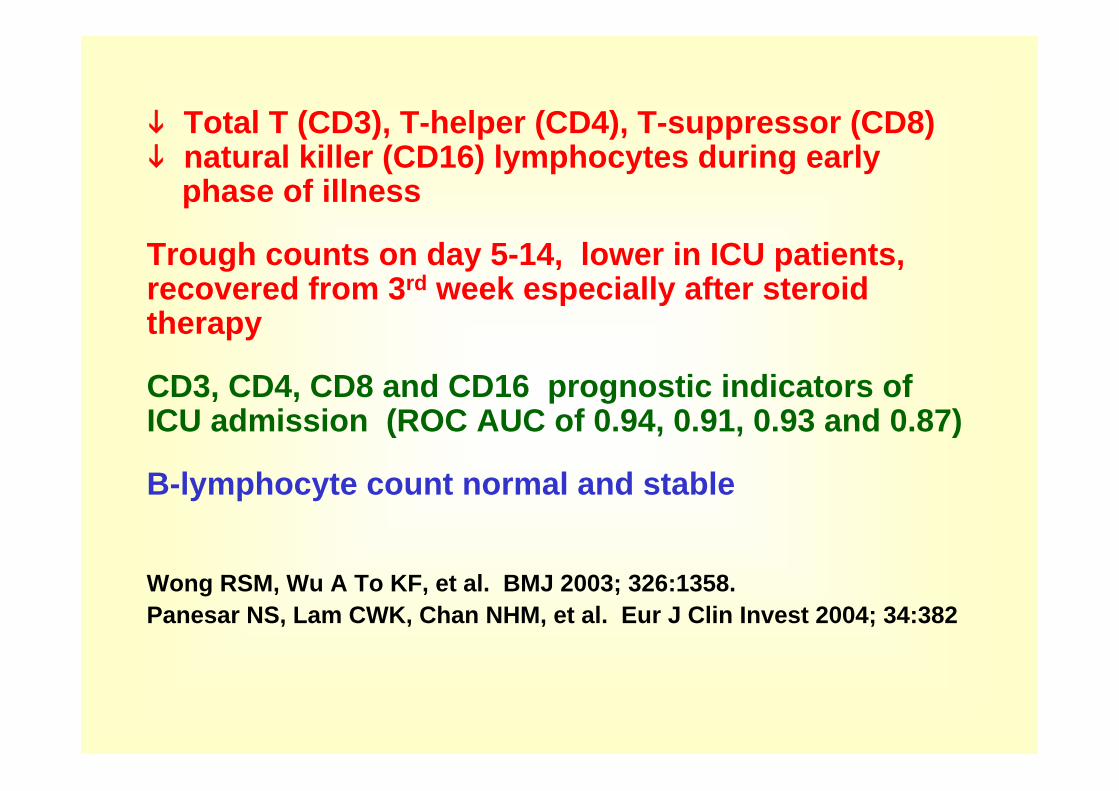
Total T (CD3), T-helper (CD4), T-suppressor (CD8)natural killer (CD16) lymphocytes during earlyphase of illness
Trough counts on day 5-14, lower in ICU patients, recovered from 3rd week especially after steroid therapy
CD3, CD4, CD8 and CD16 prognostic indicators of ICU admission (ROC AUC of 0.94, 0.91, 0.93 and 0.87)
B-lymphocyte count normal and stable
Wong RSM, Wu A To KF, et al. BMJ 2003; 326:1358.Panesar NS, Lam CWK, Chan NHM, et al. Eur J Clin Invest 2004; 34:382

Severe acute infections ===> cytokines and chemokines in circulation and tissues, e.g. CAP, RSV, swine influenza
Cytokine and chemokine storm ===> accelerates viral clearance, but may also cause exaggerate inflammation especially in response to a high viral load
20 adult SARS patients ===> daily plasma inflammatory cytokines and chemokines for ≤ 19 consecutive days upon admission

Cytokines in plasma
+PE
conjugated anti-
cytokine antibodies
6 different capture beads for cytokines with same size but different FL-3 intensities
3 hrs
Capture beads with specific cytokines and PE detector Ab
IL-6IL-2
TNF-αIFN-γ
IL-4IL-10
Analysis by Flow Cytometer
+
Cytometric Bead Array Analysis of 6 Cytokines Simultaneously using Flow Cytometry

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 250
150
300
450
600
750 *
*
*
*
* *
**
*
*
*
*
*
Day after Disease Onset
ng/L
Changes in plasma inflammatory cytokines in 20 SARS patients
Inflammatory cytokineIL-1β
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 250
25
50
75
100
125
150
175
* *
*
* *
*
Day after Disease Onset
ng/LInflammatory cytokine
IL-6
1 2 3 4 5 6 7 8 9 1011121314151617180
50
100
150
200
**
*
Day after Disease Onset
ng/LTh1 cytokine
IFN-γ
increase
increase
increase
*P < 0.05 Comparing with normal reference values

Th1 cytokine IFNγ, inflammatory cytokines IL-1β, IL-6 and IL-12 for 2 weeks
No increase in TNFα, IL-10 and IL-4
neutrophil chemokine IL-8, monocytechemoattractant protein-1 (MCP-1), and Th1 chemokine IFNγ-inducible protein-10 (IP-10)
Similar but milder changes in paediatricpatients
Wong CK, Lam CWK, Wu AKL, et al. Clin Exp Immunol 2004; 136:95Ng PC, Lam CWK, Li AM, et al. Paediatrics 2004; 113-e7Ng PC, Lam CWK, Li AM, et al. Arch Dis Child 2005; 90:422

(a) Needed pulse steroid (b) Not needed pulse steroid
1 2 3 4 5 6 7 8 9 101112131415161718192021222324250
5
10
15
20
25
30
Day after Disease Onset
ng/L
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 250
5
10
15
20
25
30
Day after Disease Onset
ng/L
1 2 3 4 5 6 7 8 9 101112131415161718192021222324250
2000
4000
6000
8000
10000
12000
Day after Disease Onset
ng/L
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 250
2000
4000
6000
8000
10000
12000
Day after Disease Onset
ng/L
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 250
50
100
150
200
250
300
Day after Disease Onset
ng/L
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 250
50
100
150
200
250
300
Day after Disease Onset
ng/L
IL-8 IL-8
IP-10 IP-10
MCP-1 MCP-1
>
>
>

Changes in Plasma Chemokines of SARS PatientsBefore and After Corticosteroid Treatment
Chemokine Immediately before 1-2 days after 5-8 days after(ng/L) steroid treatment steroid treatment steroid treatment
IL-8 8.7 5.9 2.2*ψ(4.8 - 14.1) (2.8 – 19.8) (1.7 – 6.1)
IP-10 5553 4826 894*ψ(4864-7557) (2725 – 6098) (574 – 3117)
MCP-1 84.0 68.5 23.0*ψ(36.5 – 198) (26.0 – 118.5) (14.0 – 37.0)
Results as median (interquartile range)* p < 0.005 compared with concentrations before steroid treatmentψ p < 0.05 compared with concentrations 1-2 days after steroid treatment

Th1
Th2
Th1 predominanceActivation of cellular immunityInflammation and cytotoxicity
IL-1IL-6
* Fever* Lymphocyte activation* Macrophage stimulation* ↑ Leucocyte/endothelial adhesion* Acute phase proteins
Chemokines
corticosteroid
IL-8 Neutrophil infiltration &accumulation
MCP-1Alveolar macrophage infiltration & accumulation
IP-10Th1 cellInfiltration &accumulation
Dis
ease
sev
erity
Possible immunotherapy:Cytokine or chemokine antibody or antagonist (e.g. anti-IL-8)Possible marker and prognostic Indicator of disease severity:(e.g. plasma IL-1βand IP-10)
IFN-γ

Immune Reaction = Double-edged Sword
Communicable Disease ===> Cytokine and Chemokine Storm ===>Communication Disease ===> Messenger and Message Pathology ===>Morbidity and Mortality
Academic Pursuit ==> Philosophy of NatureApplied Science ==> Monitoring Disease Activity
Developing Therapy

3.5 Scholarships Commemorating Dr Tse Yuen ManIn the Spring of 2003, SARS broke out in Hong Kong without any alert. Dr Joanna Tse Yuen Man, a 1992 graduate of the Faculty of Medicine, the Chinese University of Hong Kong, was then a lung and chest specialist at the TuenMun Hospital. Dr Tse immediately volunteered to work in the Intensive Care Unit , where many SARS patients had already been in critical conditions. She was very devoted to her duty of caring for the SARS patients. Unfortunately, she herself succumbed to SARS in May, 2003.
Monitoring Disease ActivityGuiding / Developing Therapy* IL-6 MAb for CAP
Eur Respir J 2002; 20:990
* Anti-TNFα for RA and HPAIInfliximab™, Etenercept™
* Anti-TNFα not for SARS

The Laboratory Medicine of Infectious Diseases
Professor C W K LamDepartment of Chemical PathologyThe Chinese University of Hong KongPrince of Wales HospitalHong Kong


Professor Poul Astrup

Steroid-induced osteonecrosis in severe acute respiratory syndrome: a retrospective analysis of biochemical markers of bone metabolism and corticosteroid therapy
From the Departments of Chemical Pathology(MHMC, IHSC, LCWL, CKW, CWKL), Microbiology(PKSC), Diagnostic Radiology & Organ Imaging(JFG, GEA, ATA), and Medicine & Therapeutics(DSCH, JJYS), The Chinese University of Hong Kong, Prince of Wales Hospital, Shatin, NT, Hong Kong; and Department of Pathology (MWMS), Alice Ho Miu Ling Nethersole Hospital, Tai Po, NT, Hong Kong. Pathology June 2006; 38: 229-35


















