
The Kentucky Pharmacist Vol. 9, No. 6
40
Vol. 9, No. 6 November 2014 T T T HE HE HE K K K ENTUCKY ENTUCKY ENTUCKY P P P HARMACIST HARMACIST HARMACIST News & Information for Members of the Kentucky Pharmacists Association Get Involved - Stay Involved Membership Matters in YOUR KPhA KPhA Rebuilding for the Future – Work on YOUR KPhA Building
-
Upload
kentucky-pharmacists-association -
Category
Documents
-
view
233 -
download
10
description
November 2014 issue of the peer reviewed journal of the Kentucky Pharmacists Association
Transcript of The Kentucky Pharmacist Vol. 9, No. 6

Vol. 9, No. 6 November 2014
TTTHEHEHE KKKENTUCKYENTUCKYENTUCKY
PPPHARMACISTHARMACISTHARMACIST
News & Information for Members of the Kentucky Pharmacists Association
Get Involved -
Stay Involved
Membership Matters
in YOUR KPhA
KPhA Rebuilding for the Future –
Work on YOUR KPhA Building

November 2014
THE KENTUCKY PHARMACIST 2
Table of Contents
Table of Contents
Table of Contents— Oath— Mission Statement 2 President’s Perspective 3 KPhA Mid-Year Conference on Legislative Priorities 4 From your Executive Director 6 APSC 8 2014 Oral Chemo Therapy Bill 9 Technician Review 10 Nov. 2014 CE — Evaluation of Abdomen, Musculoskeletal, and Nervous System 11 November Pharmacist/Pharmacy Tech Quiz 16
KPhA Emergency Preparedness 17 Continuing Education Article Submission Guidelines 18 Dec. 2014 CE — Preventing Errors in the Pharmacy 19 December Pharmacist/Pharmacy Tech Quiz 26 Kentucky Renaissance Pharmacy Museum 27 KPhA New and Returning Members 28 Pharmacy Law Brief 32 Pharmacy Policy Issues 34 Pharmacists Mutual 36 Cardinal Health 37 KPhA Board of Directors 38 50 Years Ago/Frequently Called and Contacted 39
Oath of a Pharmacist
At this time, I vow to devote my professional life to the service of all humankind through the profession of
pharmacy.
I will consider the welfare of humanity and relief of human suffering my primary concerns.
I will apply my knowledge, experience, and skills to the best of my ability to assure optimal drug therapy
outcomes for the patients I serve.
I will keep abreast of developments and maintain professional competency in my profession of pharmacy.
I will embrace and advocate change in the profession of pharmacy that improves patient care.
I take these vows voluntarily with the full realization of the responsibility with which I am entrusted by the public.
Kentucky Pharmacists Association
The mission of the Kentucky Pharmacists
Association is to promote the profession of
pharmacy, enhance the practice standards of the
profession, and demonstrate the value of pharmacist
services within the health care system.
Editorial Office:
© Copyright 2014 to the Kentucky Pharmacists Association. The Kentucky Pharmacist is the official journal of the Kentucky Pharmacists Association published bi-monthly. The Kentucky Pharmacist is distributed to KPhA members, paid through allocations of membership dues. All views expressed in articles are those of the writer, and not necessarily the official position of the Kentucky Pharmacists Association.
Editorial, advertising and executive offices at 1228 US 127 South, Frankfort, KY 40601. Phone 502.227.2303 Fax 502.227.2258. Email [email protected]. Website http://www.kphanet.org.
The Kentucky Pharmacy Education and Research
Foundation (KPERF), established in 1980 as a non-profit
subsidiary corporation of the Kentucky Pharmacists
Association (KPhA), fosters educational activities and
research projects in the field of pharmacy including career
counseling, student assistance, post-graduate education,
continuing and professional development and public health
education and assistance.
It is the goal of KPERF to ensure that pharmacy in Kentucky
and throughout the nation may sustain the continuing need
for sufficient and adequately trained pharmacists. KPERF will
provide a minimum of 15 continuing pharmacy education
hours. In addition, KPERF will provide at least three
educational interventions through other mediums — such as
webinars — to continuously improve healthcare for all.
Programming will be determined by assessing the gaps
between actual practice and ideal practice, with activities
designed to narrow those gaps using interaction, learning
assessment, and evaluation. Additionally, feedback from
learners will be used to improve the overall programming
designed by KPERF.

November 2014
THE KENTUCKY PHARMACIST 3
In 2017, KPhA will celebrate
the 50th anniversary of the
start of construction of
YOUR KPhA building. As
with any 50 year old, it is
beginning to show its age. Over the last few years, there
have been a number of “emergency” repairs that needed to
be made that were not in the KPhA budget. As we dis-
cussed the need for these repairs and the methods of fund-
ing them, it occurred to me that this might be a recurring
concern in future Board meetings. What will go wrong next,
and how will we pay for it? I began to think that we need to
start planning for future building needs and emergencies.
KPhA is very fortunate to own our own building, but as eve-
ry homeowner knows, there will always be problems to fix.
In order to plan for the future, I thought it would be best to
look back at the KPhA pioneers who had the vision to build
an office for KPhA. Scott Sisco and UK PY-4 student War-
ren Finlinson were kind enough to dig through the archives
of The Kentucky Pharmacist to uncover some of the history
of the building. Many pharmacists may not realize it, but up
until 1995 KPhA and the Board of Pharmacy shared offic-
es. From 1939 – 1965, E. M. Josey served as both the Ex-
ecutive Director of KPhA and the Executive Secretary of
the Kentucky Board of Pharmacy. At the time of his death,
KPhA and the Board shared office space in downtown
Frankfort. Following his death, separate appointments were
made for the Executive Director of KPhA (Bob Lichtefeld)
and Board of Pharmacy (C.O. Ducker as acting director).
They discovered then that there was office space for only
one director! Also during this time, many KPhA members
came to the offices for the first time after his passing. As
quoted in the minutes of the KPhA House of Delegates
meeting July 27, 1966, Mary Frances Feiler was quoted as
saying “what are we doing in a dump like this?” Bob
Lichtefeld was kinder in his comments; he recalled that it
was “not a nice place.” There was much discussion in the
convention minutes as to what should be done about the
current KPhA and Board offices. This discussion led to the
initial planning for the building.
Initially, when Mr. Josey had passed away, a group of phar-
macists raised money for a scholarship fund in his honor;
however, once discussion began of the construction of a
KPhA building, the scholarship changed into a building fund
campaign to honor Mr. Josey (the current KPhA building is
named the E. Murphy Josey Memorial Building). The Board
agreed to continue to lease office space in what would be
called a “pharmaceutical building.” Through the hard work
of many pharmacists, a building campaign co-chaired by
Ben Koby and Earl P. Slone, was started. On the cover of
the March 1967 cover of The Kentucky Pharmacist is a pic-
ture of the proposed building and a slogan to describe it. It
reads: “Dedicated to those who have served Kentucky
pharmacy in the past and to those who will serve in the fu-
ture.” I could not agree more! Another great quote comes
from past KPhA president, Ralph J. Schwartz, who wrote in
the October 1967, issue “The future home of Kentucky
pharmacy shows that we are on the move again, that we
are not tired and content, that we want to build upon the
solid foundation of service laid down by our past members
and leaders. It also symbolizes our new spirit of independ-
ence.” The ground breaking for the new building was at
noon Oct. 2, 1967. To quote past-president Schwartz
again, “So – a comment became an idea. The idea became
a dream.”
In late July 1968, employees of KPhA (Mrs. Margaret Du-
vall and Robert J. Lichtefeld) and the Kentucky Board of
Pharmacy (John H. Voige, Richard Ross and Earl Becknell)
moved into the new building. It was a great moment in the
history of pharmacy in Kentucky and of YOUR KPhA. The
building was possible because of the donations of over 500
pharmacists, pharmacies, wholesalers, local associations
and other individuals and businesses. Approximately
$100,000 was raised during the building campaign.
Let’s now fast forward 48 years. Our building is beginning
PRESIDENT’S
PERSPECTIVE
Robert Oakley
KPhA President
2014-2015
President’s Perspective
Continued on Page 5
KPhA Rebuilding for the Future –
Work on YOUR KPhA Building

November 2014
THE KENTUCKY PHARMACIST 4
2014 Mid-Year Conference on Legislative Priorities
Stacie Maass, APhA Senior VP, Pharmacy Practice and Government Affairs, presents on Federal Provider Status at the
2014 KPhA Mid-Year Conference on Legislative Priorities. (Below, left) Maass met with the Provider Status Workgroup
and the Government Affairs Committee.
KPhA Member Jill Rhodes explains the Oral
Chemo Therapy Parity bill passed in the 2014
Legislative Session. (For more on the bill, see
page 9.)
Featuring the
KPhA Student
Legislative Day in partnership with
Sullivan University College of Pharmacy
and
University of Kentucky College of Pharmacy

November 2014
THE KENTUCKY PHARMACIST 5
2014 Mid-Year Conference on Legislative Priorities
to show its age. There are many items in current need of
repair or replacement and the appearance is worn looking.
There has been little work done on the outside to improve
appearances. For example, how many of you have visited
the offices lately and noticed the “leaning wall of KPhA” at
the front of our building? How it is still standing, I don’t
know. The KPhA building is no longer the show place it was
when it first opened.
I believe that the KPhA members in 1966 were visionary
and forward thinking in their decision to build the current
KPhA office. I also believe that the current members of
KPhA need to be equally forward thinking to protect and
maintain their legacy. Therefore, I would like to announce
the start of a campaign to raise funds for the maintenance
and to upgrade YOUR KPhA building. It will be called
“Rebuilding for the Future.” KPhA will establish a separate
fund, entirely through donations, to use for building im-
provements. We will be seeking donations from individuals,
pharmacies, organizations and corporations. I recognize
that we will be competing with many other organizations for
your donations just as it was in 1966-67 when over 500
individuals, companies and organizations made the initial
donations to build the KPhA building.
We are in the very early stages of our campaign. I will be
working closely with our Executive Director, Bob McFalls, to
finalize the details of our campaign. We will be launching it
soon, and we will be sending more information on the de-
tails. I also would like to hear from you, the members. If you
have ideas or suggestions on the rebuilding fund campaign,
please let me know. If you have stories you would like to
share about the history of the building or the original build-
ing fund campaign, please let us know. We can share these
stories with the members of YOUR KPhA.
Have a happy and joyous holiday season. Remember, it is
the season for sharing and giving.
Continued from Page 3
Show your Pharmacist Pride with a KPhA
Roamey Window Cling!
$5 — All proceeds benefit
the KPhA Building Fund
Available at the KPhA Online Store
www.kphanet.org, click on About Tab, Online Store
CAPT Doug Thoroughman, PhD, MS, CDC Career Epide-
miology Field Officer, presents on the Ebola Crisis in West
Africa.
KPhA Thanks our 2014 Mid-Year Conference
Sponsors
Unanimous Consent Majority Vote
($2,000 and up)
American Pharmacy
Cooperative Inc.
American Pharmacy
Services Corp.
Kentucky Customers of
Cardinal Health
Pfizer
Sullivan University College
of Pharmacy
Richard and Zena Slone
Center for the
Advancement of Pharmacy
Practice at UKCOP
Celgene
Passport Health Plan
Pharmacists Mutual

November 2014
THE KENTUCKY PHARMACIST 6
From Your Executive Director
MESSAGE FROM YOUR
EXECUTIVE DIRECTOR
Robert “Bob” McFalls
Technically, I am not sure if it is truly Fall or a pseudo Win-
ter that has returned to Kentucky, but one thing is for sure
— it is basketball season once again throughout the Com-
monwealth. And that can only mean one thing to a state full
of people in love with the sport of basketball, from Paducah
to Pikeville, from northern Kentucky to Albany, from Lexing-
ton to Louisville and all points in between. We love our bas-
ketball team of choice, and we hunger to see them win. We
are a people steeped in rich tradition and in love with our
championships, even as we hunger for more. And for the
mini fans that are learning the history and the rules, we
strive to pass on our heritage, to help them to claim the leg-
acy that is ours as dedicated fans. It is quite an exciting re-
sponsibility to undertake and to share together.
As a member of YOUR KPhA, you share a similar, rich his-
tory of an Association dating back to 1877 as the 14th state
association to be formed nationally. Our legacy is rich, and
the words of the past continue to speak to the present while
outlining the future in advancing the profession. In this re-
spect, I would like to offer a few brief observations about
the legacy of E.M. Josey, R.Ph., former Executive Secre-
tary both of the Kentucky Pharmacists Association and of
the Kentucky Board of Pharmacy. Following his untimely
death, Mr. Josey’s contributions were honored by action of
the 89th Annual Convention of the Kentucky Pharmacists
(then Pharmaceutical) Association meeting in Covington,
which memorialized him at the KPhA Headquarters Building
in Frankfort by designating that KPhA (and at the time, the
Board of Pharmacy) would be housed in the new Josey Me-
morial Building. In reading Mr. Josey’s detailed reports from
the 1960s in The Kentucky Pharmacist, one quickly realizes
how engaged he was in making a difference for others and
for pharmacists as a whole. Mr. Josey literally died “on the
job” when he passed away suddenly on June 17, 1965, not
far from where YOUR KPhA headquarters now stands.
And, just as he led the way in his professional life, commit-
ment and service, Mr. Josey and his legacy continue to rep-
resent you and your professional colleagues today. YOUR
KPhA’s records document how the voluntary action and
commitment of another individual, C.O. Ducker, Inspector
for the Board of Pharmacy, offered the first pledge of
$200.00 at a meeting in July 1966 that immediately led to
six matching pledges at the same meeting to establish the
initial building fund. The Kentucky Pharmacist (October
1967) goes on to report, “Thus with the assurance of this
initial $1,400.00 the ball was ready to roll. “A comment be-
came an idea. The idea became a dream.” And with a lot of
sweat, determination, efforts, leadership and participation of
the pharmacy family, the dream became reality. Later, in
October 1967, YOUR KPhA declared in its dedication of the
“Home of Pharmacy in Kentucky” the ultimate acknowl-
edgement of service — recognizing not only Mr. Josey and
his commitment but extending that level of service to each
and every one who would walk beside him and follow in his
professional footsteps — by dedicating the new headquar-
ters: “To Those Who Have Served Kentucky Pharmacy in
the Past and To Those Who Will Serve in the Future.”
Indeed, YOUR KPhA Headquarters is a living memorial to
the sacrifice and commitment of those who have gone be-
fore us to those who now carry the torch forward today and
to those who will lead in the future. At the luncheon ceremo-
ny following the official ground-breaking in October 1967,
George Grider spoke eloquently as APhA President to the
profession, stating in part: “…State pharmaceutical associa-
tions, as in our own case, have alternately thrived and with-
ered over the years, depending upon their membership
number and vigor. State associations have, for the most
part, been ill-housed and ill-fed, with never enough space,
enough equipment, enough staff and, of course, enough
money. Today’s action marks the end of such inadequacy
for Kentucky pharmacy, as we join the ever growing list of
state associations that are erecting permanent homes for
themselves. The future home of Kentucky pharmacy shows
that we are on the move again, that we are not tired and
content, that we want to build upon the solid foundation of
service laid down by our past members and leaders. It also
symbolizes our new spirit of independence…. Under the
aggressive and intelligent leadership of President (Ralph)
Swartz, our officers and of our Executive Director Bob
Lichtefeld, Kentucky pharmacy is advancing swiftly into the
mainstream of American pharmacy. We are showing new
vigor, new enthusiasm.”

November 2014
THE KENTUCKY PHARMACIST 7
From Your Executive Director
On behalf of YOUR KPhA staff, I want to say how exciting
it is to be a part of a winning team, as we seek the next
opportunity to advance the ball down the court, to block
the opposition, to score by getting the ball to and in the
basket and to win endless championships for our pharma-
cy team. Let us be thankful for those who have given so
much, as we also acknowledge those who are faithfully
serving the association NOW. And, as we reflect during
the holiday season that is upon us, let’s take time to exam-
ine the key elements of our individual legacy as well. For
what is it that you seek to be remembered, and what do
you intend to pass on as your legacy to the profession of
pharmacy? Thank you Mr. Josey. And thank you, KPhA
Member!
Reminder: CE deadline for 2014 is December 31 To maintain your Kentucky Pharmacist li-
cense, you must complete 15 hours of con-
tinuing education each year between Janu-
ary 1 and December 31. These hours can be
live or home based activities. But they must
be COMPLETED between those dates.
In April 2014, ACPE released a few updates on CPE Moni-
tor. Beginning May 1, ACPE enabled a 60-day submission
rule for activities. What does this mean for you? Probably
not much for live activities. YOUR KPERF Administrator
(that would be Scott Sisco, KPhA Director of Communica-
tions and Continuing Education) must have activities up-
loaded to CPE Monitor within 60 days of the completion of
the activity.
On home activities (the CE articles in these pages each
issue), activities must be uploaded within 60 days of the
completion date. So make sure you send in your quizzes
soon after you complete them. Beginning Jan. 1, 2015,
CPE Monitor will not accept activities completed more
than 60 days prior to submission. If you
submit home based activities to KPERF
after the 60 day deadline, they will be re-
turned to you.
In regards to the completion date for home
activities, which is next to your signature on
the answer sheets for the CE quizzes, ACPE considers
this date to determine when the credit for the activity is val-
id. So, if you put a completion date on a quiz in Decem-
ber 2014, but mail it to KPhA for credit in January 2015,
it will count toward your total for 2014.
The expiration date for home-based CE programs remains
the same as it always has. Programs are valid for three
years after the release date. KPERF lists the expiration
date at the top of the page of answer sheets. You can still
complete CE activities from past years for current year
credit, as long as the program hasn’t expired. All KPERF
CE articles are available online for KPhA members under
the Education tab on www.kphanet.org.
Watch eNews and
subsequent editions
of The Kentucky
Pharmacist for more
information on ways
YOU can help
rebuild YOUR KPhA
Headquarters!

November 2014
THE KENTUCKY PHARMACIST 8
APSC

November 2014
THE KENTUCKY PHARMACIST 9
2014 Oral Chemo Parity Bill
KPhA Government Affairs Contribution Name: _______________________________Pharmacy: _____________________________
Email: ______________________________________________________________
Address: _____________________________________________________________
City: ___________________________________________ State: _________ Zip: ____________
Phone: ________________ Fax: _________________ E-Mail: ______________________________
Contribution Amount: $_________ Check ____ (make checks payable to KPhA Government Affairs)
Mail to: Kentucky Pharmacists Association, 1228 US Highway 127 South, Frankfort, KY 40601
New Law in Effect January 2015: Oral Chemo Parity Bill to expand access
to effective cancer therapies As of Jan. 1, 2015, many Kentucky cancer patients will
benefit from the state’s new Oral Cheomtherapy Parity Bill,
which passed in the 2014 Kentucky Legislative session as
part of House Bill 126.
Intravenous (IV)/infused anticancer medications are typical-
ly covered under a health plan's medical benefit, with pa-
tients responsible for a nominal copayment, per treatment.
Orally-administered anticancer medications, however, are
usually covered under a health plan's pharmacy benefit.
Under the pharmacy benefit, oral anticancer medications
are often included in the highest tier of a health plan’s drug
benefit and come with the highest out-of-pocket cost, re-
quiring patients to pay a coinsurance – or a percentage of
the overall total cost of the drug. This percentage coinsur-
ance can often equal thousands of dollars each month; a
price tag that restricts access to life-saving oral anticancer
therapies for untold numbers of cancer patients.
Come Jan. 1, 2015, this will change for cancer patients in
Kentucky, when HB 126 goes into effect, giving them great-
er access to the latest and most effective anticancer treat-
ments. The bill, which passed at the end of the 2014 legis-
lative session after a hard fought battle by YOUR KPhA
patients, patient advocacy organizations and Senator Tom
Buford, requires health insurance companies to charge
patients no more than $100 out-of-pocket for a 30-day sup-
ply of orally administered anticancer medications. The orig-
inal bill was sponsored by Sen. Buford and overwhelmingly
passed both houses of the state legislature. HB 126 was
signed into law by Governor Steve Beshear in April.
“We are proud to have been a part of the successful out-
come of this important legislation needed by cancer pa-
tients”, stated KPhA President Bob Oakley. “Improving ac-
cess to one’s medication therapy by controlling out of pock-
et costs will increase adherence and be positive for the
patient overall.”
The law does not require health plans to cover a new ser-
vice and only impacts those that currently list chemothera-
py as a covered benefit. The state law impacts residents
covered by a private commercial health plan. The law does
not impact the federal Medicare program. Kentucky joins
33 other states and the District of Columbia, including Mis-
souri, Wisconsin and Ohio, in enacting similar legislation.
For more information about KAR Chapter 304/HB126,
please visit: www.kphanet.org.

November 2014
THE KENTUCKY PHARMACIST 10
Technician Review
KPhA Technician members are eligible for Free CE modeled on PTCB standards by becoming a member of the KPhA Pharmacy Technician Academy. All KPhA Technician Members are eligible for Academy Membership at no additional cost.
FREE
CE
KPhA Member Pharmacy Technicians
The mission of the KPhA Academy of Pharmacy Technicians is:
To unite the pharmacy technicians throughout the Commonwealth to have one
voice toward the advancement of our profession.
To follow what is currently happening with your profession please read our
newsletter articles and become involved.
For more information contact Don Carpenter via email at [email protected]
Technician Review From the KPhA Academy of Technicians
Your KPhA Pharmacy Technician Academy continues to
grow in numbers and support. We are 40 members strong
and hope to see more growth in the coming New Year.
Currently, we are in discussion with the Board of Pharma-
cy’s Advisory Council concerning future recommendations
to the Board of Pharmacy. We have addressed the KPhA
Professional Affairs Committee’s concerns about our pro-
posals and look forward to gaining their support.
The Academy would like to remind all certified pharmacy
technicians that beginning in 2015 all continuing education
must be technician specific. As a member of the KPhA
Pharmacy Technician Academy, you are eligible to receive
up to 10 hours of free online technician-specific continuing
education from the Collaborative Education Institute. If you
are already of member of KPhA you may go to the KPhA
website at http://www.kphanet.org/ and join the Academy or
contact Don Carpenter at [email protected]. If you
are not a member of KPhA yet and wish to join the associa-
tion you can join via the website.
The members of the Pharmacy Technician Academy would
like to wish everyone a Merry Christmas and Happy New
Year.

November 2014
THE KENTUCKY PHARMACIST 11
Nov. 2014 CE — Abdomen, Musculoskeletal, and Nervous Systems
Pharmacist Patient Assessment Skills for Optimizing Self-Care, Part 4 of 4: Evaluation of the Abdomen, Musculoskeletal, and Nervous Systems By: Kimberly A. Messerschmidt, PharmD; Professor of Pharmacy Practice, SDSU College of Pharmacy. Clinical
Pharmacist, Sanford USD Medical Center and Kelley J. Oehlke, PharmD; Residency Program Director, Clinical
Pharmacy Specialist, Ambulatory Care, Sioux Falls VA Health Care System
Reprinted with permission of the authors and the South Dakota Pharmacists Association where this article originally ap-
peared. This activity may appear in other state pharmacy association journals. There are no financial relationships that
could be perceived as real or apparent conflicts of interest.
Universal Activity # 0143-9999-14-011-H01-P&T
2.0 Contact Hours (0.2 CEU)
Goal: To enhance pharmacists’ knowledge regarding patient assessment.
Objectives
At the conclusion of this article, the reader should be able to:
1. Properly evaluate common gastrointestinal complaints and recognize when to refer patients to their physicians. 2. Identify medications that commonly cause diarrhea and constipation. 3. Describe risk factors and symptoms associated with GERD. 4. Evaluate the characteristics and common causes of leg pain . 5. Recognize typical symptoms associated with various types of headaches, transient ischemic attack (TIA) and cerebrovascular accident (CVA).
KPERF offers all CE
articles to members
online at
www.kphanet.org
Introduction
Each and every day, thousands of people seek guidance
from their pharmacist regarding the appropriate use of their
medications. Pharmacists must rely upon not only their
pharmaceutical knowledge base, but also upon effective
communication and patient assessment skills in order to
meet the needs of these individuals.
In this final section of our four part series, we continue to
explore opportunities for utilizing basic patient assessment
skills, with a focus on assessment of the abdomen, muscu-
loskeletal system and nervous system. By understanding
these vital concepts, pharmacists can confidently make an
early impact on patient care.
Abdomen
The pharmacist’s role in assessment of the abdomen nor-
mally does not entail performing a physical examination.
However, the pharmacist should be able to interpret the
information from an exam or a patient interview in order to
make sound, medication related recommendations. In most
cases, patients who present to the pharmacy with ab-
dominal pain should be referred to their physician.
Patients with other common gastrointestinal complaints
such as nausea and vomiting, diarrhea, constipation, peptic
ulcer disease (PUD) and gastroesophageal reflux disease
(GERD) may or may not need to be referred; in these cas-
es, a thorough patient history will help the pharmacist to
determine the best course of action.
Nausea is generally nonspecific and may be associated
with a number of conditions including viral illness, pregnan-
cy, motion sickness, liver or pancreatic disease or malig-
nancy. Nausea also is a very common side effect of many
medications. Vomiting may occur with more specific illness-
es such as gastroenteritis, bile duct obstruction, intestinal
obstruction or it may be the result of head trauma or inges-
tion of a toxic substance. Since nausea and vomiting can
be caused by such a variety of benign to serious condi-
tions, one of the major goals of treatment should be to
identify and resolve the underlying disorder. Assessment of
the situation includes identifying how long the patient has
been experiencing the nausea or vomiting, when it began,
what it was associated with (e.g., food, new medication),
what the vomitus looks and smells like (e.g., vomited mate-
rial with a fecal smell indicates intestinal obstruction and

November 2014
THE KENTUCKY PHARMACIST 12
Nov. 2014 CE — Abdomen, Musculoskeletal, and Nervous Systems
mandates immediate referral), whether associated symp-
toms such as pain or fever are present, and whether the
patient has any underlying medical conditions.
Because it is impossible to discuss all of the clinical situa-
tions in which nausea and vomiting might be a pertinent
finding, clinical judgment is needed to determine which pa-
tients are not candidates for self-care. Table 1 lists some
examples of patients that should typically be referred to
their physician for further evaluation. Additionally, any pa-
tient who experiences nausea and vomiting for more than
one or two days, or who has a complicated medical history
or a continued worsening of their condition should be re-
ferred.1
Dehydration may result from excessive vomiting and is es-
pecially important with infants and young children. Warning
signs of dehydration in children include excessive thirst,
decreased urine output, dry mucous membranes, fever
without sweating, unusual listlessness or decreased alert-
ness, a sunken fontanelle and crying with little tear produc-
tion.1 Additionally, patients may experience dizziness and
lightheadedness, fainting or low blood pressure. Any pa-
tient exhibiting symptoms of dehydration should be referred
to their physician.
Diarrhea and constipation also are frequent complaints of
patients, especially in the elderly population. Diarrhea is the
abnormal passage of watery stools, and constipation is in-
frequency of, and/or difficulty in passing hard stools. Com-
mon finding of patients with diarrhea include sudden onset
of abnormally frequent stools, which also may be accompa-
nied by abdominal cramping, weakness, fatigue, abdominal
bloating and flatulence, nausea, vomiting and fever. Signs
of dehydration and electrolyte/metabolic abnormalities may
be found on physical exam. Low back pain, abdominal dis-
tention, vague discomfort, anorexia and headache may be
found in patients
with constipation.
Similar assess-
ment questions
apply to diarrhea
and constipation
as for nausea and
vomiting.
Drug-induced
causes of diar-
rhea and consti-
pation may be found in Table 2. Patients should be warned
of the potential side effects of medications and what to do if
they occur. Lack of exercise and inadequate intake of fluids
and fiber also may cause constipation; each of these fac-
tors should be addressed when treating this common com-
plaint. As with vomiting, rehydration should always be
stressed to patients who experience severe and/or pro-
longed episodes of diarrhea. In general, if the diarrhea or
constipation has been present for one week or more, or if
there is evidence of bleeding, the patient should be re-
ferred. Other exclusions for self-treatment are listed in Ta-
ble 3.
Common causes of peptic ulcer disease (PUD) include Hel-
icobacter pylori and NSAIDs. A patient may present with
melena (dark, sticky stools), hematochezia (bright red
blood in stool), epigastric pain, pain that awakens the pa-
tient at night, weight loss, nausea and vomiting, belching or
bloating. Pain that is relieved by eating, or that occurs 1 to
3 hours after eating is more typically associated with a duo-
denal ulcer, while pain that is exacerbated by eating is
more suggestive of a gastric ulcer. Encourage the patient
to remove aggravating factors such as cigarette smoking,
NSAID or aspirin use and alcohol. Avoiding foods that
cause dyspepsia also will aid in healing. Any patient with
Table 1. Exclusions to self-treatment of nausea and vomiting1
Suspected food poisoning that has lasted for more than 12 hours
Accompanying symptoms such as: severe abdominal pain, fever and diarrhea,
blood in the vomitus, signs of liver dysfunction (e.g., yellow skin or eyes, dark
urine, pale stools) or stiff neck and headache with light sensitivity
History of a recent head injury
Underlying chronic medical condition such as glaucoma, BPH, gastrointestinal
disease or diabetes
Suspected medication side-effect or sign of toxicity (e.g,, digoxin, theophyl-
line, lithium)
Suspected eating disorder
Pregnancy
DIARRHEA
Antibiotics
Antacids (containing magnesium)
Acarbose
Bethanecol
Colchicine
Metformin
Metoclopramide
Quinidine
CONSTIPATION
Opiate analgesics
Antacids (containing aluminum or
calcium)
Anticholinergics
Antihypertensives
Diuretics
Iron supplements
Neuroleptics
Vincristine
Table 2. Medications that commonly
cause diarrhea and constipation

November 2014
THE KENTUCKY PHARMACIST 13
Nov. 2014 CE — Abdomen, Musculoskeletal, and Nervous Systems
suspected PUD should be referred to a physician for further
evaluation.
GERD is a disorder in which gastric contents are refluxed
into the esophagus. Risk factors for this disorder may in-
clude:
Large meals and eating before bedtime
Dietary fat
Chocolate, peppermint, alcohol and caffeine
Medications (e.g.,alpha blockers, beta blockers, calci-
um channel blockers, anticholinergics, theophylline,
benzodiazepines, barbiturates)
Pregnancy and obesity
The patient may present with heartburn (retrosternal burn-
ing and discomfort), water brash (hypersalivation), belch-
ing, dysphagia or respiratory symptoms (e.g., morning
hoarseness, pneumonitis, cough, wheezing and chest tight-
ness).
Generally, GERD is a chronic condition that is character-
ized by recurrent symptoms and may require long-term or
maintenance therapy. Self treatment may include nonphar-
macologic therapy such as changing the diet, elevating the
head of the bed and avoiding medications that affect the
lower esophageal sphincter. Patients presenting with warn-
ing symptoms (e.g., dysphagia, choking, bleeding, weight
loss) or atypical symptoms (e.g., chest pain, pulmonary
symptoms, chronic hoarseness, chronic cough or pharyngi-
tis) should be evaluated by a physician. Patients who do
not respond to self-care, including lifestyle modifications
and OTC treatment, after two weeks also should be re-
ferred for a complete evaluation.2
MUSCULOSKELETAL
Leg pain is a frequent complaint relating to the peripheral
vascular system. Leg pain, cramping or weakness that oc-
curs with walking and is relieved with rest is termed inter-
mittent claudication, and is a primary symptom associated
with peripheral vascular disease (PVD). It is caused by hy-
poxia, or lack of oxygen to the leg muscles. Leg pain also
can result from musculoskeletal problems, trauma and vari-
ous other causes (e.g., deep vein thrombosis or DVT).
Edema in the extremities, manifested as a change in the
usual contour of the leg, also may be a common complaint
of patients. When assessing a patient’s peripheral edema,
press your index finger on the extremity and hold for sever-
al seconds. A depression that does not rapidly refill and
resume its original contour indicates pitting edema. This
finding is not usually accompanied by a thickening or
change in pigmentation of the overlying skin, which may be
more indicative of venous stasis. Peripheral edema may be
secondary to heart failure, PVD, DVT, trauma or renal fail-
ure.
If a patient presents with unilateral leg swelling, warmth,
erythema and tenderness, a DVT may be suspected. A
DVT is defined as the presence of a thrombus, or clot in a
deep vein and is accompanied by an inflammatory process
in the vessel wall. Blood flow stasis, vascular damage and
hypercoagulability are all factors which may predispose the
patient to thrombus formation. Major veins that are com-
monly affected include the iliac, femoral and popliteal. Risk
factors associated with DVT include:
Orthopedic surgical procedures
Cancer
Fractures of the spine, pelvis, femur and tibia
Immobilization
Pregnancy
Estrogen use
Hypercoagulable disease states
Exclusions for self-treatment of diarrhea
Patients less than 6 months of age
Significant dehydration
Persistent fever or vomiting, or abdominal pain
Significant medical comorbidities (e.g., uncontrolled dia-
betes, immunosuppression)
Pregnancy
Chronic or persistent diarrhea (e.g, symptoms not re-
solved after 48 hours)
Poor response to self-treatment
Blood, mucus, or pus in the stool
Exclusions for self-treatment of constipation
Significant abdominal pain or distention
Accompanying fever, nausea, and/or vomiting
Unexplained changes in bowel habits or significant weight
loss
Dark, tarry, bloody, or pencil thin stools
Persistent (i.e., two weeks or more) or recurrent (i.e., over
3 months or more) symptoms
History of inflammatory bowel disease
Table 3. Exclusions for self-treatment of diarrhea
and constipation1
November 2014
THE KENTUCKY PHARMACIST 14
Nov. 2014 CE — Abdomen, Musculoskeletal, and Nervous Systems
Occasionally, a cord-like obstruction
may be felt on palpation of the affect-
ed leg, but patients also may be
asymptomatic. Skin color may vary
between erythema (redness), pallor
(paleness) or cyanosis (a dusky blue
hue). The major concern of a DVT is
the risk of a thrombus detaching and
moving to the lung, which is termed
pulmonary embolism (PE). Any suspi-
cion of a DVT or PE should be re-
ferred for emergency attention.
NERVOUS SYSTEM
The nervous system is divided into
two parts, the central nervous system
(CNS) and the peripheral nervous
system (PNS). The brain and spinal
cord are included in the CNS, while the PNS includes the
12 pairs of cranial nerves, the 31 pairs of spinal nerves and
the corresponding branches. The PNS carries messages to
the CNS from sensory receptors and from the CNS out to
the muscles, organs and glands. The evaluation of motor,
sensory, autonomic, cognitive and behavioral elements
makes neurologic assessment one of the most complex
portions of the physical examination.
Many neurologic and systemic medical illnesses result in
specific abnormalities in cranial nerve function. Some of the
most common conditions that elicit questions from patients
concerning neurologic diseases include headaches, transi-
ent ischemic attack (TIA) and cerebrovascular accident
(CVA), or stroke.
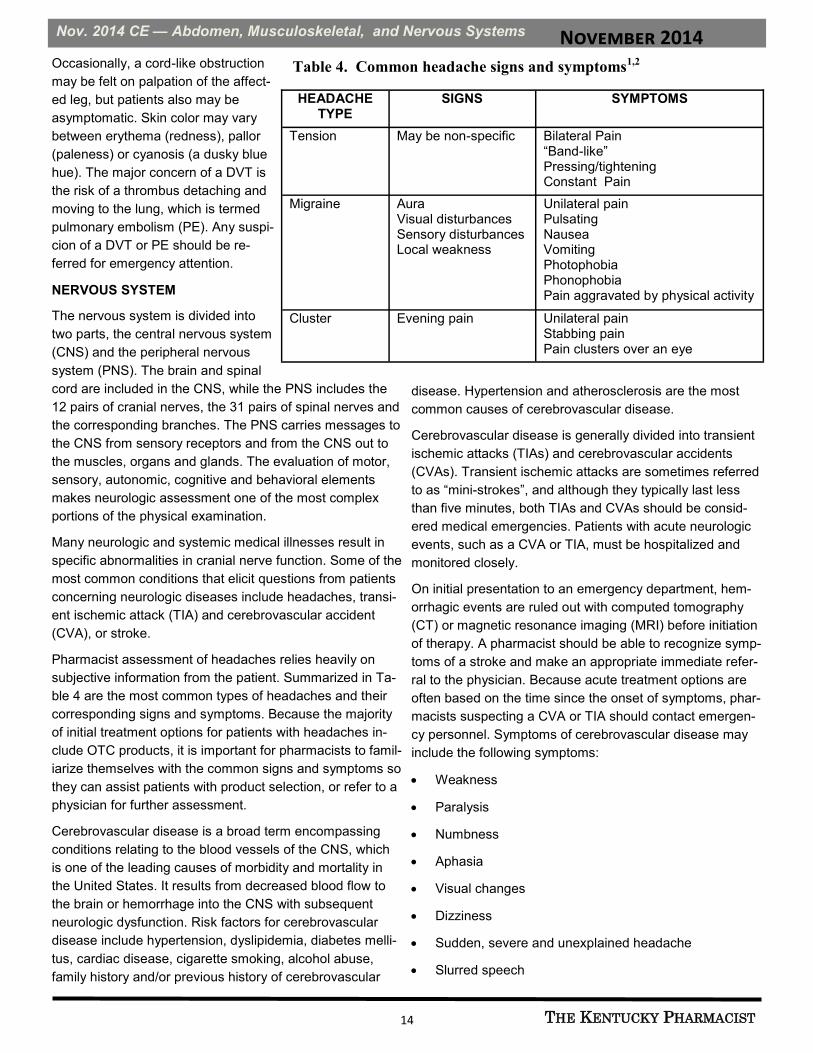
Pharmacist assessment of headaches relies heavily on
subjective information from the patient. Summarized in Ta-
ble 4 are the most common types of headaches and their
corresponding signs and symptoms. Because the majority
of initial treatment options for patients with headaches in-
clude OTC products, it is important for pharmacists to famil-
iarize themselves with the common signs and symptoms so
they can assist patients with product selection, or refer to a
physician for further assessment.
Cerebrovascular disease is a broad term encompassing
conditions relating to the blood vessels of the CNS, which
is one of the leading causes of morbidity and mortality in
the United States. It results from decreased blood flow to
the brain or hemorrhage into the CNS with subsequent
neurologic dysfunction. Risk factors for cerebrovascular
disease include hypertension, dyslipidemia, diabetes melli-
tus, cardiac disease, cigarette smoking, alcohol abuse,
family history and/or previous history of cerebrovascular
disease. Hypertension and atherosclerosis are the most
common causes of cerebrovascular disease.
Cerebrovascular disease is generally divided into transient
ischemic attacks (TIAs) and cerebrovascular accidents
(CVAs). Transient ischemic attacks are sometimes referred
to as “mini-strokes”, and although they typically last less
than five minutes, both TIAs and CVAs should be consid-
ered medical emergencies. Patients with acute neurologic
events, such as a CVA or TIA, must be hospitalized and
monitored closely.
On initial presentation to an emergency department, hem-
orrhagic events are ruled out with computed tomography
(CT) or magnetic resonance imaging (MRI) before initiation
of therapy. A pharmacist should be able to recognize symp-
toms of a stroke and make an appropriate immediate refer-
ral to the physician. Because acute treatment options are
often based on the time since the onset of symptoms, phar-
macists suspecting a CVA or TIA should contact emergen-
cy personnel. Symptoms of cerebrovascular disease may
include the following symptoms:
Weakness
Paralysis
Numbness
Aphasia
Visual changes
Dizziness
Sudden, severe and unexplained headache
Slurred speech
HEADACHE TYPE
SIGNS SYMPTOMS
Tension May be non-specific
Bilateral Pain “Band-like” Pressing/tightening Constant Pain
Migraine Aura Visual disturbances Sensory disturbances Local weakness
Unilateral pain Pulsating Nausea Vomiting Photophobia Phonophobia Pain aggravated by physical activity
Cluster Evening pain Unilateral pain Stabbing pain Pain clusters over an eye
Table 4. Common headache signs and symptoms1,2

November 2014
THE KENTUCKY PHARMACIST 15
Nov. 2014 CE — Abdomen, Musculoskeletal, and Nervous Systems
Conclusion
With the rising cost of health care, more and more patients
find themselves looking for opportunities to self treat a vari-
ety of medical ailments. While some conditions are amena-
ble to self-treatment, others call for prompt medical evalua-
tion. By using effective communication and patient assess-
ment skills, pharmacists are in an ideal position to help
guide patients towards the best course of care.
References
1. Berardi RR, Ferreri SP, Hume AL, Kroon LA, Newton
GD, Popovich NG et al, editors. Handbook of Nonpre-
scription Drugs: An Interactive Approach to Self-Care.
16th ed. Washington DC: The American Pharmaceuti-
cal Association; 2009.
2. Dipiro JT, et al (eds): Pharmacotherapy: A Pathophysi-
ologic Approach. 7th ed. McGraw Hill; 2008.
Suggested Readings
1. Jones RM and Rospond RM. Patient Assessment in
Pharmacy Practice. 2nd ed. Baltimore (MD): Lippincott
Williams & Wilkins; 2006.
2. Longe RL and Calvert JC. Physical Assessment: A
Guide for Evaluating Drug Therapy.1st ed. Vancouver:
Applied Therapeutics, Inc; 1994.
November 2014 — Pharmacist Patient Assessment Skills for Optimizing Self-Care, Part 4 of 4:
Evaluation of the Abdomen, Musculoskeletal, and Nervous Systems
1. Nausea may be associated with a number of conditions including: A. Viral illness. B. Pregnancy. C. Motion sickness. D. All of the above. 2. Excessive thirst, decreased urine output, dry mucous membranes and fever without sweating are all signs of: A. Peptic ulcer disease. B. Gastroesophageal reflux disease. C. Dehydration. D. Constipation. 3. A disorder in which gastric contents are refluxed into the esophagus is termed: A. Dysphagia. B. Pneumonitis. C. GERD. D. Pharyngitis. 4. Weakness, numbness, visual changes, slurred speech and aphasia are all symptoms associated with: A. Tension headache. B. Cerebrovascular accident. C. Cluster headache. D. Intermittent claudication. 5. Bilateral, "band-like", pressing/tightening and constant pain are symptoms of which type of headache? A. Tension B. Migraine C. Cluster D. Withdrawal 6. Risk factors that are associated with a DVT include all of the following EXCEPT: A. Orthopedic surgical procedures. B. Regular exercise. C. Pregnancy. D. Estrogen use.
7. Constipation may be caused by all of the following EXCEPT: A. Opiate analgesics. B. Lack of exercise. C. Iron supplements. D. Antacids containing magnesium. 8. Which of the following medications may cause diarrhea? A. Opiate analgesics B. Antacid (containing magnesium) C. Vincristine D. Anticholinergics 9. Self treatment for GERD may include all of the following EXCEPT: A. Consuming a large glass of caffeine prior to bedtime. B. Changing the diet. C. Elevating the head of the bed. D. Avoiding medications that affect the lower esophageal
sphincter. 10. Pharmacists suspecting a CVA or TIA should: A. Wait until 3 symptoms are present. B. Contact emergency personnel immediately. C. Consider changing the patient’s medications. D. Wait 1 day to see if symptoms persist. 11. If a patient presents with unilateral leg swelling, warmth, erythema and tenderness, a _________ may be suspected. A. DVT B. Tension headache C. TIA D. PE 12. Which of the following would exclude a patient from self-treatment of constipation? A. Significant abdominal pain or distention B. Dark, tarry, bloody or pencil thin stools C. History of inflammatory bowel disease D. All of the above are exclusions to self-treatment

November 2014
THE KENTUCKY PHARMACIST 16
Nov. 2014 CE — Abdomen, Musculoskeletal, and Nervous Systems
This activity is a FREE service to members of the Kentucky Pharmacists Association. The
fee for non-members is $30. Mail completed forms to: KPERF, 1228 US 127 South,
Frankfort, KY 40601. Credit will be applied to your CPE Monitor Profile.
The Kentucky Pharmacy Education & Research Foundation is
accredited by The Accreditation Council for Pharmacy
Education as a provider of continuing Pharmacy education.
Quizzes submitted without NABP eProfile
ID # and Birthdate cannot be accepted.
PHARMACISTS ANSWER SHEET November 2014 — Pharmacist Patient Assessment Skills for Optimizing Self-Care, Part 4 of 4: Evaluation of the Abdomen, Musculoskeletal, and Nervous Systems (2.0 contact hours) Universal Activity # 0143-9999-14-011-H01-P Name ________________________________________________ KY Lic. # __________________________________ Address ______________________________________________Email_____________________________________ PLEASE CIRCLE THE APPROPRIATE ANSWERS: 1. A B C D 3. A B C D 5. A B C D 7. A B C D 9. A B C D 11. A B C D 2. A B C D 4. A B C D 6. A B C D 8. A B C D 10. A B C D 12. A B C D Information presented in the activity: Met my educational needs ___Yes ___No Figures and tables were useful ___Yes ___No Achieve the stated objectives ___Yes ___No Posttest was appropriate ___Yes ___No Was well written ___Yes ___No Commercial bias was present ___Yes ___No Is relevant to my practice ___Yes ___No Unmet Objectives:______________________________________________________________________________ I hereby certify that I completed this self-study program independently and without assistance from any other party. Signature ______________________________________________Completion Date __________________________
Personal
NABP eProfile ID #_____________________________ Birthdate ___________________(MM/DD)
Expiration Date: December 2, 2017 Successful Completion: Score of 80% will result in 2.0 contact hour or 0.2 CEU.
Participants who score less than 80% will be notified and permitted one re-examination.
TECHNICIANS ANSWER SHEET. November 2014 — Pharmacist Patient Assessment Skills for Optimizing Self-Care, Part 4 of 4: Evaluation of the Abdomen, Musculoskeletal, and Nervous Systems (2.0 contact hours) Universal Activity # 0143-9999-14-011-H01-T Name _______________________________________________KY Cert. # __________________________________ Address ______________________________________________Email_____________________________________ PLEASE CIRCLE THE APPROPRIATE ANSWERS: 1. A B C D 3. A B C D 5. A B C D 7. A B C D 9. A B C D 11. A B C D 2. A B C D 4. A B C D 6. A B C D 8. A B C D 10. A B C D 12. A B C D Met my educational needs ___Yes ___No Figures and tables were useful ___Yes ___No Achieve the stated objectives ___Yes ___No Posttest was appropriate ___Yes ___No Was well written ___Yes ___No Commercial bias was present ___Yes ___No Is relevant to my practice ___Yes ___No I hereby certify that I completed this self-study program independently and without assistance from any other party. Signature ______________________________________________Completion Date __________________________
Personal
NABP eProfile ID #_____________________________ Birthdate ___________________(MM/DD)

November 2014
THE KENTUCKY PHARMACIST 17
KPhA Pharmacy Emergency Preparedness
KPhA Pharmacy Emergency Preparedness Initiative Interest Form
Name: ______________________ Status (Pharmacist, Technician, Other): ___________________
Email: ______________________________ Phone: ___________________________
For Pharmacists: Interest in serving as a volunteer: Yes____ No _____
You also may join the Medical Reserve Corps by following the KHELPS link on KPhA Website to register
(www.kphanet.org under Resources)
Please send this information to Leah Tolliver, KPhA Director of Pharmacy Emergency Preparedness via email at
[email protected], fax to 502-227-2258 or mail at KPhA, 1228 US 127 South, Frankfort, KY 40601.
For more Emergency
Preparedness Resources, visit
www.kphanet.org, click on
Resources and Emergency
Preparedness.
Coming Soon!
Emergency Preparedness Training YOUR KPhA has developed two emergency preparedness
training programs for the KPhA Pharmacy Volunteers that
will be available online in the next few weeks. Watch
eNews for more information on these programs.
Also, KPhA Director of Pharmacy Emergency Prepared-
ness, Leah Tolliver, is developing a new CE program that
will roll out this winter and spring at our local organizations
about preparing your pharmacy in the event of a disaster.
These tips and procedures will be relevant to all pharma-
cies including retail, hospital, long term care and com-
pounding. If you are interested in seeing this program at
your local organization meeting, contact your local leader
or KPhA!
This program also will be offered at the 137th KPhA Annual
Meeting and Convention June 25-28, 2015 in Bowling
Green!

November 2014
THE KENTUCKY PHARMACIST 18
The following broad guidelines should guide an au-
thor to completing a continuing education article for
publication in The Kentucky Pharmacist.
Average length is 4-10 typed pages in a word pro-
cessing document (Microsoft Word is preferred).
Articles are generally written so that they are per-
tinent to both pharmacists and pharmacy techni-
cians. If the subject matter absolutely is not perti-
nent to technicians, that needs to be stated clearly
at the beginning of the article.
Article should begin with the goal or goals of the
overall program – usually a few sentences.
Include 3 to 5 objectives using SMART and meas-
urable verbs.
Feel free to include graphs or charts, but please
submit them separately, not embedded in the text
of the article.
Include a quiz over the material. Usually between
10 to 12 multiple choice questions.
Articles are reviewed for commercial bias, etc. by
at least one (normally two) pharmacist reviewers.
When submitting the article, you also will be
asked to fill out a financial disclosure statement to
identify any financial considerations connected to
your article.
Articles should address topics designed to narrow
gaps between actual practice and ideal practice in
pharmacy. Please see the KPhA website
(www.kphanet.org) under the Education link to see
previously published articles.
Articles must be submitted electronically to the KPhA
director of communications and continuing education
([email protected]) by the first of the month pre-
ceding publication.
YOUR KPhA Needs YOU! Have an idea for a continuing education article? WRITE IT!
Continuing Education Article Guidelines
Kentucky Pharmacists Political Advocacy Contribution Form
Name: _________________________________ Pharmacy: ___________________________
Address: _______________________ City: ________________ State: _____ Zip: ________
Phone: ________________ Fax: _________________ E-Mail: __________________________________
Contribution Amount: $_________ Check ____ (make checks payable to KPPAC)
Mail to: Kentucky Pharmacists Political Advocacy Council, 1228 US Highway 127 South, Frankfort, KY 40601
CONTRIBUTION LIMITS
The primary, runoff primary and general elections are separate elections. The maximum contribution from a PAC to a candidate or slate of candidates is $1,000 per election.
Individuals may contribute no more than $1,500 per year to all PACs in the aggregate.
In-kind contributions are subject to the same limits as monetary contributions.
Cash Contributions: $50 per contributor, per election. Con-tributions by cashier’s check or money order are lim-ited to $50 per election unless the instrument identi-fies the payor and payee. KRS 121.150(4)
Anonymous Contributions: $50 per contributor, per elec-tion, maximum total of $1,000 per election.
(This information is in accordance with KRS 121. 150)
CE Article Guidelines

November 2014
THE KENTUCKY PHARMACIST 19
Dec. 2014 CE — Preventing Errors
Preventing Errors in the Pharmacy
to Improve Patient Safety By: Lauren E. Glaze, PharmD, Julie N. Burris, PharmD, Sullivan University College of Pharmacy
There are no financial relationships that could be perceived as real or apparent conflicts of interest.
Universal Activity # 0143-0000-14-012-H05-P&T
1.5 Contact Hours (0.15 CEU)
Objectives
At the conclusion of this article, the reader should be able to:
1. Define medication errors and identify the most common errors made in the community pharmacy setting.
2. Describe at what point(s) medication errors may occur in the chain of pharmaceutical patient care.
3. Recognize the common causes of medication errors. 4. Identify methods for pharmacy clerks, technicians and pharmacists to prevent medication errors.
KPERF offers all CE
articles to members
online at
www.kphanet.org
Medication Errors
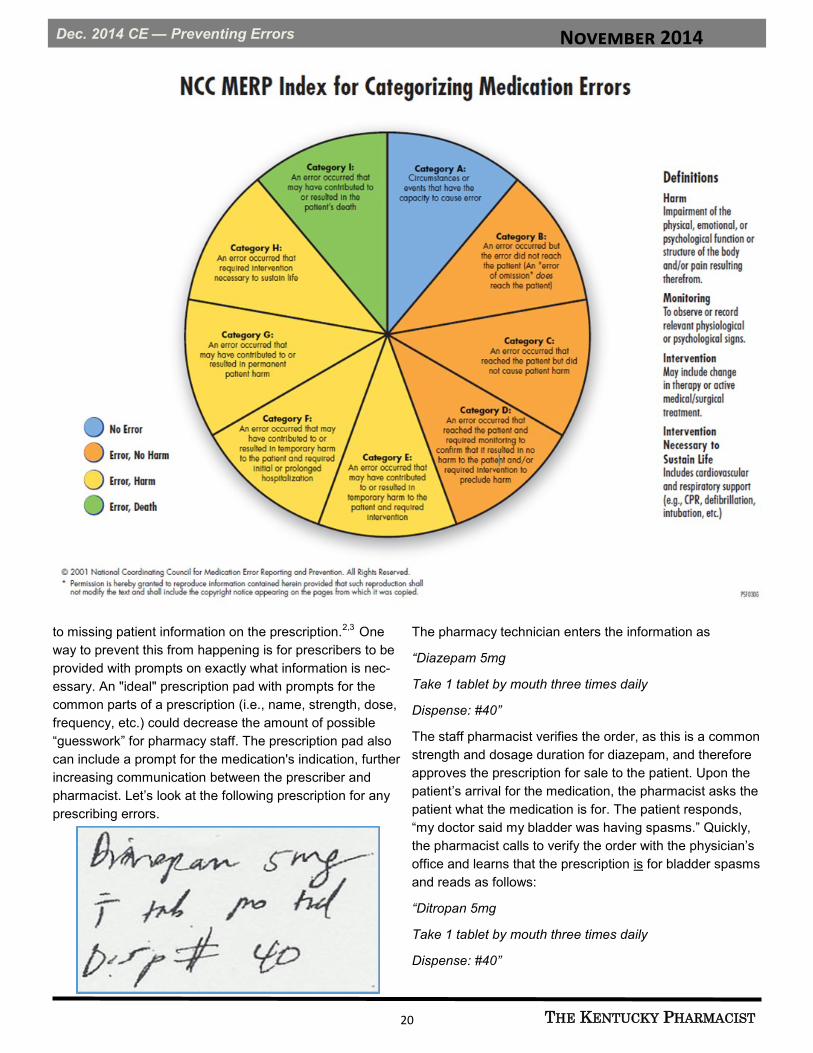
The National Coordinating Council for Medication Error
Reporting and Prevention (NCC MERP) defines a medica-
tion error as "… any preventable event that may cause or
lead to inappropriate medication use or patient harm while
the medication is in the control of the health care profes-
sional, patient, or consumer. Such events may be related to
professional practice, health care products, procedures and
systems, including prescribing; order communication; prod-
uct labeling, packaging and nomenclature; compounding;
dispensing; distribution; administration; education; monitor-
ing; and use."1 To define medication errors, the Council
also classifies medication errors by whether the error
reached the patient, if the patient was harmed and the se-
verity of the outcome (if applicable). The classification of
medication errors are listed in the chart on the next page.
Another way to consider medication errors is to classify
them by type instead of outcome. For example, common
errors that occur in the community pharmacy setting are
Errors of Omission, Errors of Commission and System Er-
rors (see chart below).
How do pharmacists and pharmacy staff prevent these er-
rors?
The first step in preventing errors is gathering information
on what leads to errors. Recognizing that a medication er-
ror has occurred is the beginning of the quality improve-
ment cycle. Finding out why it occurred is the next step.
The next section will focus on the causes of medication
errors and the most common scenarios for the errors to
take place.
Where do Medication Errors Occur?
Prescribing Step:
A medication error may take place at any step of the pro-
cess. The first and most common errors occur during the
prescribing step, with the vast majority of these errors due
TYPE DEFINITION EXAMPLE(S)
Errors of omission Failing to do something correctly Failing to include strength of a medication on a prescription
Failing to administer a dose of medication
Errors of commission Doing something incorrectly Prescribing the wrong antibiotic Dispensing an incorrect dose of an
appropriate drug Bypassing a drug interaction alert
System error An error that is not the result of an individu-al's actions but the predictable outcome of a series of actions and factors that com-
prise a diagnostic or treatment process
Poor lighting Inadequate staffing Handwritten orders Ambiguous drug labels
November 2014
THE KENTUCKY PHARMACIST 20
Dec. 2014 CE — Preventing Errors
to missing patient information on the prescription.2,3
One
way to prevent this from happening is for prescribers to be
provided with prompts on exactly what information is nec-
essary. An "ideal" prescription pad with prompts for the
common parts of a prescription (i.e., name, strength, dose,
frequency, etc.) could decrease the amount of possible
“guesswork” for pharmacy staff. The prescription pad also
can include a prompt for the medication's indication, further
increasing communication between the prescriber and
pharmacist. Let’s look at the following prescription for any
prescribing errors.
The pharmacy technician enters the information as
“Diazepam 5mg
Take 1 tablet by mouth three times daily
Dispense: #40”
The staff pharmacist verifies the order, as this is a common
strength and dosage duration for diazepam, and therefore
approves the prescription for sale to the patient. Upon the
patient’s arrival for the medication, the pharmacist asks the
patient what the medication is for. The patient responds,
“my doctor said my bladder was having spasms.” Quickly,
the pharmacist calls to verify the order with the physician’s
office and learns that the prescription is for bladder spasms
and reads as follows:
“Ditropan 5mg
Take 1 tablet by mouth three times daily
Dispense: #40”

November 2014
THE KENTUCKY PHARMACIST 21
Dec. 2014 CE — Preventing Errors
This scenario is an example of the risks of missing infor-
mation on a prescription and encourages the use of pre-
scription pad templates with a prompt for the medication’s
indication.
Electronic prescriptions are legible, neat and a faster option
for prescriptions, but they are not without error.
Over half of all prescriptions in the U.S. are transmitted
electronically. These electronic prescribing systems still
require human intervention. It's estimated that a pharmacist
intervenes in one out of every 10 e-prescriptions.4 With
electronic prescriptions, errors have occurred such as the
prescriber choosing the wrong product, selecting a liquid
form or more expensive tablet when a cheaper capsule is
available, selecting the wrong patient or inconsistent direc-
tions and/or quantities.5 For example, the following pre-
scription is easily read, but the instructions for use leave
the pharmacist to question what the physician actually in-
tended.
The electronic prescription contains two different directions,
leaving the pharmacist to call and clarify with the physician.
Dispensing Step:
Another area where the majority of medication errors may
occur is during the dispensing step. This also is where the
most legal claims are filed against the pharmacist, so it is
important to avoid these errors. According to the NCC
MERP, the following rules for best pharmacy practice
should be implemented to the pharmacy staff to avoid dis-
pensing medication error:
Patient profiles should be current and contain enough
information for pharmacists to assess appropriateness.
Work areas should be well designed to help prevent
errors with adequate lighting, low noise and few dis-
tractions.
Drugs should be organized to reduce confusion be-
tween similar names, labels or strengths.
Pharmacists should counsel patients when dispensing
medications. This is an important safety check for dis-
pensing and patient comprehension.
Pharmacies should have and follow dispensing policies
and procedures. This creates a standard of practice for
all to follow. These can also be reviewed if an error
occurs; procedures can then be improved to prevent
future errors.6
What are the Causes of Medication Errors?
Abbreviations:
While it is important to know where medication errors may
occur, it is equally important to recognize the most common
causes of medication errors. Many factors along the way
can contribute to the failure of the medication use system
and result in medication errors. Organizations like The In-
stitute for Safe Medication Practices (ISMP) and the Joint
Commission collect data on medication errors, analyze the
data to reveal the causes of errors and then alert pharma-
cists and prescribers so that errors can be prevented.
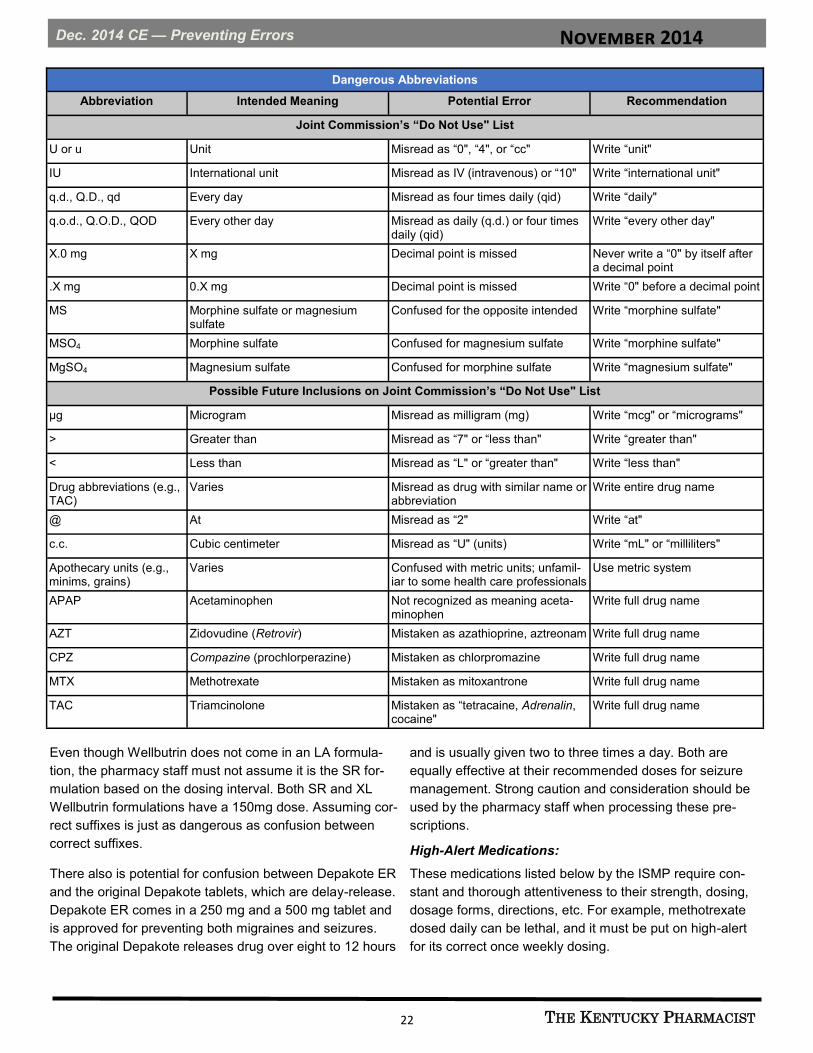
Abbreviations, though useful, have proven to be danger-
ous. The Joint Commission released its “Do Not Use” List
to prevent these errors. The table on pages 24 and 25 in-
cludes other common errors with abbreviations.7
Sound-Alike, Look-Alike Drugs:
Another common cause of medication errors is the mix-up
of “Sound-Alike, Look-Alike Drugs.” The FDA requires
TALL MAN lettering for at least 33 of these potentially con-
fused generic medications. For example, glipizide is printed
as glipiZIDE to avoid confusion with glyBURIDE, or predni-
sone and prednisoLONE.
Drug Name Suffixes:
Suffixes at the end of drug names such as CD, LA, ER, XR,
SR, and XL can lead to errors. Errors that result from the
use of suffixes may happen because of confusion about the
suffix, not knowing what the suffix means and lack of stand-
ardized meanings of suffixes. This can lead to product mix-
ups, prescriptions written with incorrect dosing intervals or
frequencies, omission of a suffix, incorrect suffix, etc.8
Wellbutrin SR and Wellbutrin XL are commonly confused
suffixes. Both Wellbutrin SR and Wellbutrin XL formulations
of bupropion are expected to have similar efficacy for treat-
ing depression. The difference is that Wellbutrin XL is given
once a day instead of twice a day. For example, Wellbutrin
XL 300 mg once a day is equivalent to Wellbutrin SR 150
mg twice a day. It is important to note also what the incor-
rect suffix is, as seen below:
November 2014
THE KENTUCKY PHARMACIST 22
Dec. 2014 CE — Preventing Errors
Dangerous Abbreviations
Abbreviation Intended Meaning Potential Error Recommendation
Joint Commission’s “Do Not Use" List
U or u Unit Misread as “0", “4", or “cc" Write “unit"
IU International unit Misread as IV (intravenous) or “10" Write “international unit"
q.d., Q.D., qd Every day Misread as four times daily (qid) Write “daily"
q.o.d., Q.O.D., QOD Every other day Misread as daily (q.d.) or four times daily (qid)
Write “every other day"
X.0 mg X mg Decimal point is missed Never write a “0" by itself after a decimal point
.X mg 0.X mg Decimal point is missed Write “0" before a decimal point
MS Morphine sulfate or magnesium sulfate
Confused for the opposite intended Write “morphine sulfate"
MSO4 Morphine sulfate Confused for magnesium sulfate Write “morphine sulfate"
MgSO4 Magnesium sulfate Confused for morphine sulfate Write “magnesium sulfate"
Possible Future Inclusions on Joint Commission’s “Do Not Use" List
µg Microgram Misread as milligram (mg) Write “mcg" or “micrograms"
> Greater than Misread as “7" or “less than" Write “greater than"
< Less than Misread as “L" or “greater than" Write “less than"
Drug abbreviations (e.g., TAC)
Varies Misread as drug with similar name or abbreviation
Write entire drug name
@ At Misread as “2" Write “at"
c.c. Cubic centimeter Misread as “U" (units) Write “mL" or “milliliters"
Apothecary units (e.g., minims, grains)
Varies Confused with metric units; unfamil-iar to some health care professionals
Use metric system
APAP Acetaminophen Not recognized as meaning aceta-minophen
Write full drug name
AZT Zidovudine (Retrovir) Mistaken as azathioprine, aztreonam Write full drug name
CPZ Compazine (prochlorperazine) Mistaken as chlorpromazine Write full drug name
MTX Methotrexate Mistaken as mitoxantrone Write full drug name
TAC Triamcinolone Mistaken as “tetracaine, Adrenalin, cocaine"
Write full drug name
Even though Wellbutrin does not come in an LA formula-
tion, the pharmacy staff must not assume it is the SR for-
mulation based on the dosing interval. Both SR and XL
Wellbutrin formulations have a 150mg dose. Assuming cor-
rect suffixes is just as dangerous as confusion between
correct suffixes.
There also is potential for confusion between Depakote ER
and the original Depakote tablets, which are delay-release.
Depakote ER comes in a 250 mg and a 500 mg tablet and
is approved for preventing both migraines and seizures.
The original Depakote releases drug over eight to 12 hours
and is usually given two to three times a day. Both are
equally effective at their recommended doses for seizure
management. Strong caution and consideration should be
used by the pharmacy staff when processing these pre-
scriptions.
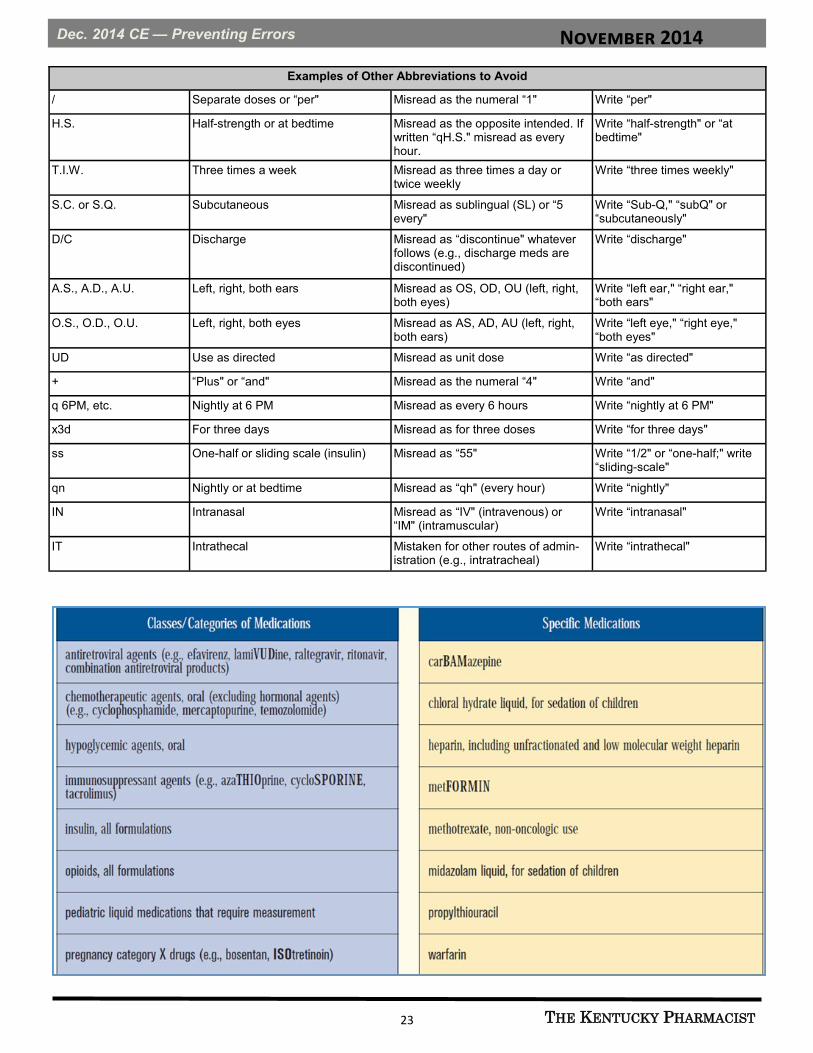
High-Alert Medications:
These medications listed below by the ISMP require con-
stant and thorough attentiveness to their strength, dosing,
dosage forms, directions, etc. For example, methotrexate
dosed daily can be lethal, and it must be put on high-alert
for its correct once weekly dosing.
November 2014
THE KENTUCKY PHARMACIST 23
Dec. 2014 CE — Preventing Errors
Examples of Other Abbreviations to Avoid
/ Separate doses or “per" Misread as the numeral “1" Write “per"
H.S. Half-strength or at bedtime Misread as the opposite intended. If written “qH.S." misread as every hour.
Write “half-strength" or “at bedtime"
T.I.W. Three times a week Misread as three times a day or twice weekly
Write “three times weekly"
S.C. or S.Q. Subcutaneous Misread as sublingual (SL) or “5 every"
Write “Sub-Q," “subQ" or “subcutaneously"
D/C Discharge Misread as “discontinue" whatever follows (e.g., discharge meds are discontinued)
Write “discharge"
A.S., A.D., A.U. Left, right, both ears Misread as OS, OD, OU (left, right, both eyes)
Write “left ear," “right ear," “both ears"
O.S., O.D., O.U. Left, right, both eyes Misread as AS, AD, AU (left, right, both ears)
Write “left eye," “right eye," “both eyes"
UD Use as directed Misread as unit dose Write “as directed"
+ “Plus" or “and" Misread as the numeral “4" Write “and"
q 6PM, etc. Nightly at 6 PM Misread as every 6 hours Write “nightly at 6 PM"
x3d For three days Misread as for three doses Write “for three days"
ss One-half or sliding scale (insulin) Misread as “55" Write “1/2" or “one-half;" write “sliding-scale"
qn Nightly or at bedtime Misread as “qh" (every hour) Write “nightly"
IN Intranasal Misread as “IV" (intravenous) or “IM" (intramuscular)
Write “intranasal"
IT Intrathecal Mistaken for other routes of admin-istration (e.g., intratracheal)
Write “intrathecal"
November 2014
THE KENTUCKY PHARMACIST 24
Dec. 2014 CE — Preventing Errors
Patient Counseling:
Not enough can be said about the importance of patient
education. Patients are the final step in preventing a medi-
cation error. When counseling patients, be sure to use lan-
guage that is simple and clear, free from "medical jargon"
that patients may not understand. Furthermore, patient in-
formation is meant to help patients understand and proper-
ly use their medications. This information is often distribut-
ed through medication leaflets, commonly known as patient
information sheets. Patient information sheets should sup-
ply sufficiently specific information, including directions for
use and/or adverse reactions. They also should be easy for
patients to read and understand by using patient-friendly
language and having proper print size and spacing.9
Even more so, by simply counseling a patient, one could
find out that the medication prescribed was Ditropan, in-
stead of Diazepam, as mentioned in our previous example.
If the pharmacist had not counseled the patient, a medica-
tion error would have occurred and possibly caused harm
to the patient.
How Can Medication Errors be Prevented?
Individual Responsibilities:
Individual responsibility for each pharmacy clerk, technician
and pharmacist should be based on the Five “RIGHTS”, i.e.
RIGHT PATIENT
RIGHT DRUG
RIGHT DOSE
RIGHT TIME
RIGHT ROUTE
Taking a moment to verify this information could mean the
difference between Mr. Rodger’s and Mr. Roger’s prescrip-
tion being incorrectly filled, a 2 year old child receiving Om-
nicef Suspension QD vs. QID or using Ciprodex Otic in the
eye compared to the ear. Looking over the Five “RIGHTS”
is imperative to preventing medication errors.
Organizational Responsibilities:
The best way to prevent medication errors is to design a
system that includes adequate safety nets with checks and
balances. When errors do slip through, documenting and
evaluating the cause of the error will help improve the en-
tire system. Individual members of organizations must be
motivated and rewarded for using safe practices. Shortcuts
for the sake of speed or impatient customers should be
discouraged, as problems must be identified and replaced
with behaviors and practices that keep patients safe.
Technology is a huge benefit to the community pharmacy,
whether by automating prescriptions, electronic prescribing,
computer data entry or barcoding medications. However, it
cannot be overstated that technology is not flawless. Com-
puterized pharmacy programs still require human interven-
tion and checking by all staff in the pharmacy.
References
1. National Coordinating Council for Medication Error Re-
porting and Prevention. About Medication Errors.
www.nccmerp.org/aboutMedErrors.html. (Accessed
September 29, 2014).
2. Malone PM, Mosdell KW, Kier KL, et al. Drug Infor-
mation: A Guide for Pharmacists. 2nd ed. New York,
NY: McGraw-Hill Publishing, 2001.
3. Kennedy AG, Littenberg B. A modified outpatient pre-
scription form to reduce prescription errors. Jt Comm J
Qual Saf 2004;30:480-487.
4. Gilligan AM, Miller K, Mohney A, et al. Analysis of phar-
macists’ interventions on electronic versus traditional
prescriptions in two community pharmacies. Res So-
cial Adm Pharm 2012;8:523-532.
5. Grossman JM, Cross DA, Boukus ER, Cohen GR.
Transmitting and processing electronic prescriptions:
experiences of physician practices and pharmacies. J
Am Med Inform Assoc 2012;19:353-359.
6. National Coordinating Council for Medication Error Re-
porting and Prevention. About Medication Errors.
www.nccmerp.org/aboutMedErrors.html. (Accessed
September 29, 2014).
7. Institute for Safe Medication Practices. Special Issue -
Do Not Use These Dangerous Abbreviations or Dose
Designations. www.ismp.org/Newsletters/acutecare/
articles/20030220_2.asp. (Accessed September 29,
2014).
8. National Coordinating Council for Medication Error Re-
porting and Prevention. Council recommendations.
Promoting the safe use of suffixes in prescription drug
names. http://www.nccmerp.org/council/council2008-08
-01.html. (September 29, 2014).
9. Svarstad BL, Mount JK, Tabak ER. Expert and con-
sumer evaluation of patient medication leaflets provid-
ed in U.S. pharmacies. J Am Pharm Assoc (2003)
2005;45:443-451.
November 2014
THE KENTUCKY PHARMACIST 25
Dec. 2014 CE — Preventing Errors
December 2014 — Preventing Errors in the Pharmacy to Improve Patient Safety
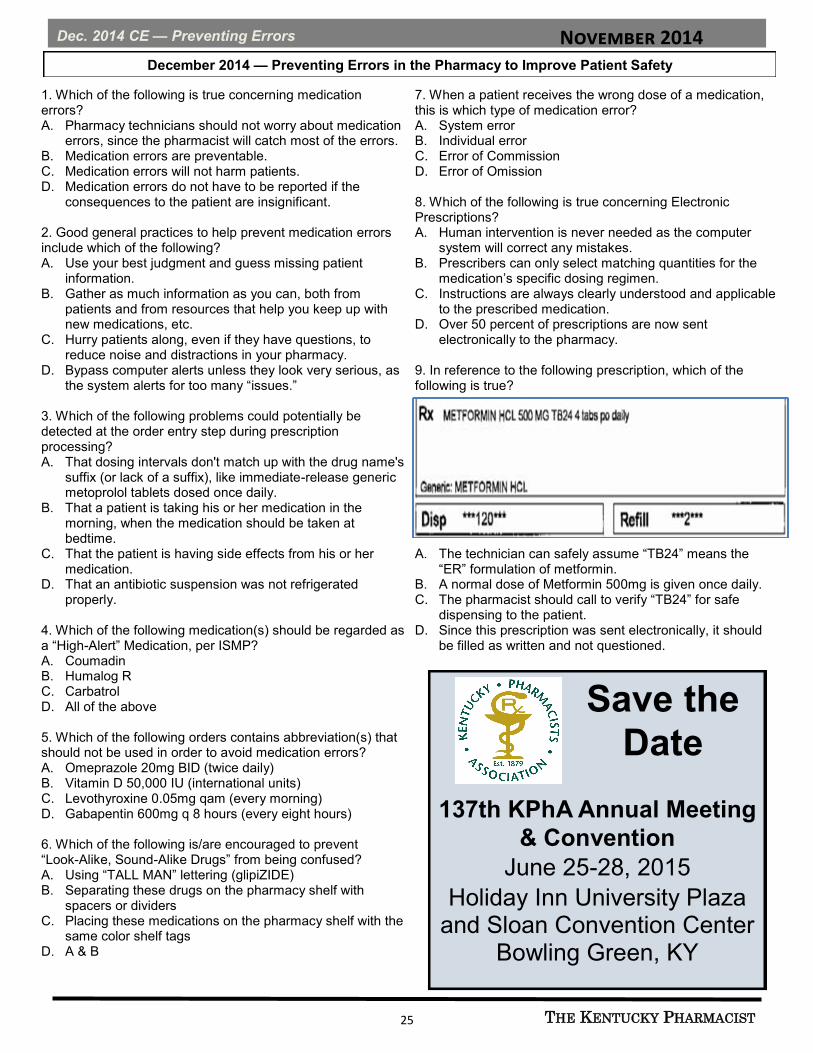
1. Which of the following is true concerning medication errors? A. Pharmacy technicians should not worry about medication
errors, since the pharmacist will catch most of the errors. B. Medication errors are preventable. C. Medication errors will not harm patients. D. Medication errors do not have to be reported if the
consequences to the patient are insignificant. 2. Good general practices to help prevent medication errors include which of the following? A. Use your best judgment and guess missing patient
information. B. Gather as much information as you can, both from
patients and from resources that help you keep up with new medications, etc.
C. Hurry patients along, even if they have questions, to reduce noise and distractions in your pharmacy.
D. Bypass computer alerts unless they look very serious, as the system alerts for too many “issues.”
3. Which of the following problems could potentially be detected at the order entry step during prescription processing? A. That dosing intervals don't match up with the drug name's
suffix (or lack of a suffix), like immediate-release generic metoprolol tablets dosed once daily.
B. That a patient is taking his or her medication in the morning, when the medication should be taken at bedtime.
C. That the patient is having side effects from his or her medication.
D. That an antibiotic suspension was not refrigerated properly.
4. Which of the following medication(s) should be regarded as a “High-Alert” Medication, per ISMP? A. Coumadin B. Humalog R C. Carbatrol D. All of the above 5. Which of the following orders contains abbreviation(s) that should not be used in order to avoid medication errors? A. Omeprazole 20mg BID (twice daily) B. Vitamin D 50,000 IU (international units) C. Levothyroxine 0.05mg qam (every morning) D. Gabapentin 600mg q 8 hours (every eight hours) 6. Which of the following is/are encouraged to prevent “Look-Alike, Sound-Alike Drugs” from being confused? A. Using “TALL MAN” lettering (glipiZIDE) B. Separating these drugs on the pharmacy shelf with
spacers or dividers C. Placing these medications on the pharmacy shelf with the
same color shelf tags D. A & B
7. When a patient receives the wrong dose of a medication, this is which type of medication error? A. System error B. Individual error C. Error of Commission D. Error of Omission 8. Which of the following is true concerning Electronic Prescriptions? A. Human intervention is never needed as the computer
system will correct any mistakes. B. Prescribers can only select matching quantities for the
medication’s specific dosing regimen. C. Instructions are always clearly understood and applicable
to the prescribed medication. D. Over 50 percent of prescriptions are now sent
electronically to the pharmacy. 9. In reference to the following prescription, which of the following is true?
A. The technician can safely assume “TB24” means the “ER” formulation of metformin.
B. A normal dose of Metformin 500mg is given once daily. C. The pharmacist should call to verify “TB24” for safe
dispensing to the patient. D. Since this prescription was sent electronically, it should
be filled as written and not questioned.
Save the
Date
137th KPhA Annual Meeting
& Convention
June 25-28, 2015
Holiday Inn University Plaza and Sloan Convention Center
Bowling Green, KY

November 2014
THE KENTUCKY PHARMACIST 26
This activity is a FREE service to members of the Kentucky Pharmacists Association. The
fee for non-members is $30. Mail completed forms to: KPERF, 1228 US 127 South,
Frankfort, KY 40601. Credit will be applied to your CPE Monitor Profile.
The Kentucky Pharmacy Education & Research Foundation is
accredited by The Accreditation Council for Pharmacy
Education as a provider of continuing Pharmacy education.
Quizzes submitted without NABP eProfile
ID # and Birthdate cannot be accepted.
Dec. 2014 CE — Preventing Errors
PHARMACISTS ANSWER SHEET December 2014 — Preventing Errors in the Pharmacy to Improve Patient Safety (1.5 contact hours) Universal Activity # 0143-0000-14-012-H05-P Name ________________________________________________ KY Lic. # __________________________________ Address ______________________________________________Email_____________________________________ PLEASE CIRCLE THE APPROPRIATE ANSWERS: 1. A B C D 3. A B C D 5. A B C D 7. A B C D 9. A B C D 2. A B C D 4. A B C D 6. A B C D 8. A B C D Information presented in the activity: Met my educational needs ___Yes ___No Figures and tables were useful ___Yes ___No Achieve the stated objectives ___Yes ___No Posttest was appropriate ___Yes ___No Was well written ___Yes ___No Commercial bias was present ___Yes ___No Is relevant to my practice ___Yes ___No Unmet Objectives:______________________________________________________________________________ I hereby certify that I completed this self-study program independently and without assistance from any other party. Signature ____________________________________________Completion Date___________________________
Personal
NABP eProfile ID #_____________________________ Birthdate ___________________(MM/DD)
Expiration Date: November 6, 2017 Successful Completion: Score of 80% will result in 1.5 contact hour or 1.5 CEU.
Participants who score less than 80% will be notified and permitted one re-examination.
TECHNICIANS ANSWER SHEET. December 2014 — Preventing Errors in the Pharmacy to Improve Patient Safety (1.5 contact hours) Universal Activity # 0143-0000-14-012-H05-T Name _______________________________________________KY Cert. # __________________________________ Address ______________________________________________Email_____________________________________ PLEASE CIRCLE THE APPROPRIATE ANSWERS: 1. A B C D 3. A B C D 5. A B C D 7. A B C D 9. A B C D 2. A B C D 4. A B C D 6. A B C D 8. A B C D Met my educational needs ___Yes ___No Figures and tables were useful ___Yes ___No Achieve the stated objectives ___Yes ___No Posttest was appropriate ___Yes ___No Was well written ___Yes ___No Commercial bias was present ___Yes ___No Is relevant to my practice ___Yes ___No I hereby certify that I completed this self-study program independently and without assistance from any other party. Signature ____________________________________________Completion Date___________________________
Personal
NABP eProfile ID #_____________________________ Birthdate ___________________(MM/DD)

November 2014
THE KENTUCKY PHARMACIST 27
In 2009 the Centers for Medicare and Medicaid Services
(CMS) implemented Surety Bond Requirements for sup-
pliers of Durable Medical Equipment, Prosthetics and
Supplies (CMS-6006-F). This ruling requires that each
existing supplier must have a $50,000 surety bond to
CMS.
Pharmacists Mutual Insurance Company, through its
subsidiary PMC Advantage Insurance Services, Inc. d/b/
a Pharmacists Insurance Agency (in California), led the
way to meet this requirement by negotiating the price of
the bond from $1,500 down to $250 for qualifying risks.
To see if you qualify for a $250 Medicare Surety Bond,
or would like information regarding our other products,
please contact us:
Call 800.247.5930 Extension 4260
E-mail [email protected]
Contact a Pharmacists Mutual Field Representative or Sales Associate http://www.phmic.com/phmc/services/ibs/Pages/Home.aspx
In Kentucky, contact Bruce Lafferre at 800.247.5930 ext. 7132 or 502.551.4815 or Tracy Curtis at 800.247.5930 ext. 7103 or 270.799.8756.
Pharmacists Mutual Insurance offers Medicare Surety Bond
Donate online to the Kentucky Pharmacists Political Advocacy Council!
Go to www.kphanet.org and click on the Advocacy tab for more information about
KPPAC and the donation form.
Kentucky Renaissance Pharmacy Museum
The Kentucky Renaissance Pharmacy Museum offers several ways way to show support of the Museum, our state's
leading preservation organization for pharmacy.
While contributions of any size are greatly appreciated, the following levels of annual giving have been established
for your consideration.
Friend of the Museum $100 Proctor Society $250
Damien Society $500 Galen Society $1,000
Name______________________________________ Specify gift amount________________________
Address ____________________________________ City____________________Zip______________
Phone H____________________W________________ Email___________________________________
Employer name_____________________________________________________for possible matching gift.
Tributes in honor or memory of_____________________________________________________
Mail to: Kentucky Renaissance Pharmacy Museum, P.O.Box 910502, Lexington, KY 40591-0502 The Kentucky Renaissance Pharmacy Museum is a non-profit 501(c)(3) business entity and as such donations are tax deductible. A notice of your tax
deductible contributions will be mailed to you annually.
Questions: Contact Lynn Harrelson @ 502-425-8642 or [email protected]
For more information on the museum, see
www.pharmacymuseumky.org or contact Gloria Doughty at
[email protected] or Lynn Harrelson at [email protected].

November 2014
THE KENTUCKY PHARMACIST 28
KPhA New and Returning Members
KPhA Welcomes New and Renewing Members
September-October 2014
Michael Akers
Grayson
Cynthia Akers
Grayson
Jennifer Anderson
Morehead
Sandra Anderson
Monticello
Charla Applegate
Nicholasville
Robin Applegate
Nicholasville
Thomas Arnold
Nicholasville
John Ausenbaugh
Dawson Springs
Nancy Barker
Winchester
Kerri Barman
Scottsville
Ronald Barned
Glasgow
Justin Bell
Lexington
Jim Bell
Sebree
Victoria Bell
Burkesville
Christopher Betz
Louisville
Joseph Bickett
Louisville
Kaleb Blair
Whitesburg
Lanny Branstetter
Horse Cave
James Brown
Bowling Green
Johnny Burke
Prestonsburg
Wendell Butler
Burkesville
Kenneth Calvert
Glasgow
Marietta Campoy
Pikeville
Don Carpenter
Olive Hill
Joseph Carr
Owensboro
Michelle Casto-Litton
Zionsville, Ind.
Vickie Chaudry
Corbin
Donald Clark
Rockfield
Charles Clifton
Fort Thomas
Rhonda Cochran
Liberty
Elizabeth Cole
Louisville
Kimberly Corley
Owensboro
Randy Crawford
Franklin
Robert Cull
Owenton
Marcelle Curtis
Shelbyville
Rachel Damaske
Saint Joseph, Mich.
Kimberly Daugherty
Louisville
Michelle DeLuca Fraley
Lexington
Brittany Downing
Pine Knot
Derek Downing
Alexandria
David Dubrock
Arlington
Michael Durbin
McKee
Jennifer Dyer
Albany
Cathy Edwards
Richmond
Mark Edwards
Richmond
Rita Etter
Williamson, W.Virg.
Brian Fingerson
Louisville
Jennifer Fitch
Lexington
Laura Fleener
Leitchfield
William Fleming
Prospect
Charles Fletcher
Monticello
Shane Fogle
Central City
Timothy Ford
Campbellsville
Milton Frizzell
Murray
Barry Frost
Columbia
Keith Fuller
Kimper
Kelli Funk
Louisville
Judy Gallagher
Madisonville
MEMBERSHIP MATTERS:
To YOU, To YOUR Patients To YOUR
Profession!

November 2014
THE KENTUCKY PHARMACIST 29
KPhA New and Returning Members
Timothy Gallagher
Madisonville
Joyce Gardner
Hodgenville
Linda Gormley
Villa Hills
John Gorrell
Morehead
Daniel Gray
London
Marsha Greer-Arnold
Louisville
Richard Griffieth
Lexington
Jack Gross
Louisville
Erik Grove
Madison, IN
Philip Hamilton
Ludlow
Gary Hamm
Elizabethtown
Kyle Harris
London
Jeffrey Harrison
Tompkinsville
Emily Henderson
Shelbyville
Clara Herrell
Lexington
Amanda Holder
Bowling Green
Michael Horne
Georgetown
Jerry Horwitz
Cincinnati, OH
Marylou Hoskins
Hawesville
Marylou Hoskins
Owensboro
H. Harper Housman
Paducah
James Howze
St. Augustine, Fla.
Patrick James
Louisville
Phillip Johnson
Georgetown
Constance Jones
Russell Springs
Karen Jones
Gilbertsville
Megan Kappes
Fort Mitchell
Leigh Keeton
Flatwoods
Erin Kingrey
Austin
Jerry Knifley
Columbia
Kerry Knochenmus
Louisville
Robert Knott
Paducah
Dhaval Kotak
Radcliff
Kevin Lamping
Lexington
Judith Lawson
Monticello
Jill Lee
Frankfort
Robert Lester
Elkhorn City
Donna Lile
Campbellsville
Douglas Linger
Georgetown
Leslie Little
Berea
Jimmie Lockhart
Lexington
Aaron Lohnes
Stanville
Kathy Long
Benton
Robert Long
Louisville
Carolyn Mallory
Russellville
Terry Manley
Mount Sterling
Nicholas Maroudas
Williamson, W.Virg.
John Marshall
Henderson
Charles Martin
Crestwood
Aleshea Martin
Crestwood
William Mattingly
Lebanon
Ronald McClish
Simpsonville
Thomas McConnell
Kuttawa
Charlene McCown
Grayson
Jennifer Mccreary
Louisa
Sheldon Mccreary
Louisa
Leeann McDonald
Dunnville
Christopher McGlone
Vanceburg
William McMakin
La Grange
John McMeans
Ashland
Nicole McNamee
Forest Hills
Jesica Mills
Louisville
Boyd Minnich
Mount Sterling
Mickey Monroe
Frankfort
Emily Morton
Hardinsburg
Amy Mueller
Louisville
Steven Mueller
Petersburg
Lance Murphy
Louisville

November 2014
THE KENTUCKY PHARMACIST 30
Daniel Nall
Louisville
David Nation
Owensboro
Troy Neagle
Glasgow
James Neat
Louisville
William Nebel
Kuttawa
Clarinda Newell
Greenup
Jamie Norman
Russellville
Kenneth Norwood
Louisville
Fred Nowak
Independence
Robert Oakley
Louisville
Jeff O'Connor
Frankfort
Jennifer O'Hearn
Louisville
Jennifer Parker
Florence
Willie Patton
Grayson
Vincent Peak
Louisville
Robert Perkins
Clinton
Bernard Poe
Owenton
Andrea Potter-Adams
Isom
Walter Powell
Louisville
John Prine
Bowling Green
Nicholas Rawe
WIlder
James Ray
Hopkinsville
Levi Rice
Beaver Dam
Eugene Riley
Russellville
Stewart Riley
Elkton
Kristie Roark
Whitesburg
Elizabeth Routh
Louisville
Ashley Saling
Mammoth Cave
Gregory Sanders
Lexington
Angela Sandlin
Louisville
Phillip Sandlin
Louisville
Stanley Scates
Lexington
Ellen Schueler
Franklin
Aron Schwartz
Louisville
Benjamin Scott
Lexington
Joseph Serafini
Frankfort
Susanna Sexton
Cornettsville
Charles Shannon
Louisville
Michael Sheets
Fisherville
Nancy Shepherd
Paducah
Kelli Shirley
Glasgow
Jarrod Shirley
Glasgow
Thomas Shively
Owensboro
Angela Shoulders
Bowling Green
JD Shoulders
Bowling Green
Joe Simmons
Glasgow
Angela Slaughter
Covington
Lois Smith
Blackey
Francis Southall
Lebanon
Glenn Stark
Frankfort
Sandra Staton
Albany
Cheryl Steiner
Hopkinsville
Laura Stone
Louisville
Jack Stone
Mayfield
Larry Stovall
Scottsville
Brittany Taylor
Lancaster
Gloria Taylor
Louisville
Deborah Thorn
Bowling Green
Sandra Thornbury
Pikeville
Joel Thornbury
Pikeville
David Triplett
Louisville
Brenda Turner
Jackson
John Vaal
Edgewood
Lorne Virgin
Grayson
Kelly Walker
Philpot
Robert Wallace
Dry Ridge
Todd Walters
Pineville
Jeffrey Warner
Jamestown
KPhA New and Returning Members

November 2014
THE KENTUCKY PHARMACIST 31
Know someone who
should be on this list?
Ask them to join YOU in
supporting YOUR KPhA!
Julie Warren
Gamaliel
Kim Wheatley
Bardstown
David Whitley
Russellville
Ronald Whitmore
Alvaton
Denis Wiggins
Louisville
Lisa Williamson
Nicholasville
Brenda Wilson
Danville
Jacob Wishnia
Louisville
Carol Wishnia
Louisville
Simon Wolf
Louisville
William Wooden
Leitchfield
Glenn Wooden
Leitchfield
Leland Wright
Lexington
Arnold Zegart
Prospect
KPhA Honorary
Life Members
Ralph Bouvette
Leon Claywell
Gloria Doughty
Ann Amerson Stewart
KPhA New and Returning Members

November 2014
THE KENTUCKY PHARMACIST 32
Pharmacy Law Brief
Pharmacy Law Brief: Alternative Dispute Resolution
Author: Joseph L. Fink III, B.S.Pharm., J.D., Professor of Pharmacy Law and Policy and Kentucky Pharmacists Association Professor of Leadership, Department of Pharmacy Practice and Science, UK College of Pharmacy
Question: I was speaking with a local attorney recent-
ly at a social function who indicated that mediation is occur-
ring with increasing frequency and in some fields reducing
the number of cases going to court, especially cases involv-
ing allegations of professional malpractice. Is this a local
trend or something of wider impact?
Response: Mediation is one form of what is known as
alternative dispute resolution, with the word “alternative”
indicating that this is an option which avoids the courtroom
and most legal processes attendant to a court proceeding.
The two principal approaches are arbitration and mediation.
Arbitration involves the two parties voluntarily agreeing to
have a third party, known as the arbitrator, decide the mat-
ter. The arbitrator meets with both sides to hear their per-
spectives and then issues a decision which is binding. One
will frequently hear of arbitration being used with salary dis-
putes in the world of professional athletics. That imposition
of a resolution differentiates arbitration from mediation. In
mediation there is a third party known as the mediator, or
sometimes called the “neutral,” who talks with the parties
and then proposes a solution to the dispute. The mediator
has no authority to impose the proposed outcome on the
parties; they must both agree to the solution of their free
will. Often a contract will then be used to formalize the
agreed upon outcome. One description of mediation I’ve
heard is that it represents presenting a “choice among a
limited number of unwanted options.”
Sometimes mediation is seen in conjunction with a court
proceeding. For example, if one were to go to Small Claims
Court in Fayette County for resolution of a dispute involving
less than $2,500, the jurisdictional limit of such a court, the
judge will direct the parties to meet with one of a cadre of
mediators standing by in an adjacent room to attempt to
resolve the matter without occupying the court’s time.
Mandatory arbitration clauses are being included in a wide
variety of contracts as the means of handing disputes, e.g.,
credit card agreements, insurer-participating provider
agreements, etc. In some cases this provision is buried
near the end of a lengthy document and the parties are not
both aware of its existence until a dispute arises.
These approaches have gained in popularity in recent
years for a number of reasons: (1) often less costly than
going to court; (2) ability with mediation to continue to have
a role in deciding the final outcome rather than having it
imposed by a judge, jury or arbitrator; (3) dispute may well
be resolved more quickly; (4) ADR is a private affair thereby
avoiding the public exposure of a court proceeding; and on
and on.
The Kentucky Court of Justice has adopted Mediation
Rules. To be placed on the Kentucky Roster of Approved
Mediators one must complete a 40 hour training program
and 15 hours of hands-on experience. One can then apply
to be placed on the Roster of Mediators that is maintained
by the Kentucky Administrative Office of the Courts. Like
many professional fields, there is a mandatory continuing
mediation education expectation for mediators of four hours
every two years. A common misconception is that one must
be an attorney to be a mediator; that is not at all the case.
Many mediators are social workers who mediate family dis-
putes.
Referring back to the original question or comment, I was
speaking with an attorney friend from Louisville who is ac-
tive in the field of medical malpractice litigation who indicat-
ed that he knows several attorneys in the field who’ve not
had a case go to trial in three years because mediation has
become so popular as a way to resolve those disputes out
of the public eye. In an area where one’s professional repu-
tation is so very important that argument is not hard to buy.
Finally, it is noteworthy for pharmacists that alternative dis-
pute resolution is sometimes referred to as “ADR”, an ab-
breviation that in our field sometimes has a different mean-
ing – adverse drug reaction! The two should not be con-
fused.
Submit Questions: [email protected]
Disclaimer: The information in this column is intended for
educational use and to stimulate professional discussion among
colleagues. It should not be construed as legal advice. There is
no way such a brief discussion of an issue or topic for education-
al or discussion purposes can adequately and fully address the
multifaceted and often complex issues that arise in the course of
professional practice. It is always the best advice for a pharma-
cist to seek counsel from an attorney who can become thorough-
ly familiar with the intricacies of a specific situation, and render
advice in accordance with the full information.
November 2014
THE KENTUCKY PHARMACIST 33
KPhA Save the Date/Connect/ EPIC
@KyPharmAssoc
@KPhAGrassroots
Facebook.com/KyPharmAssoc
KPhA Company Page
Are you connected
to YOUR KPhA?
Join us online!
Save the Date 137th KPhA Annual Meeting & Convention
June 25-28, 2015
Holiday Inn University Plaza and Sloan Convention Center Bowling Green, KY

November 2014
THE KENTUCKY PHARMACIST 34
Pharmacy Policy Issues
PHARMACY POLICY ISSUES:
New Federal Legislation Targets International Counterfeiting of Pharmaceuticals Author: Claire A. Hafner is a second professional year student at the University of Kentucky College of Pharmacy. A
native of St. Charles, Ill., she completed her pre-professional preparation at UK.
Issue: I’m a hospital pharmacist and I’ve had patients approach me with questions related to obtaining prescription
pharmaceuticals from Internet pharmacies. I guess they ask me because they don’t want to ask their community phar-
macist this question. Anyway, I’ve read in the professional literature about a major problem with counterfeiting of phar-
maceuticals, some of which is very well done so the product really looks like the real thing. Can you provide an update
on this issue?
Discussion: A counterfeit drug is defined as a drug
“made by someone other than the genuine manufacturer,
or by copying or imitating an original product without au-
thority or right, and then marketing the forged drug as the
original.”1 Unfortunately, the illegal and counterfeit medi-
cines market has expanded greatly in the past five years,
enough so that the U.S. Food and Drug Administration was
thrown into a worldwide crackdown this past May.
According to the FDA, more than 19,600 packages contain-
ing counterfeit medicines
were sequestered in the
action, involving authori-
ties from 111 countries.
Many of the unapproved,
fake drugs originated
from countries in South-
east Asia, including Chi-
na, India, Laos, Malay-
sia, Singapore and Tai-
wan. In addition, counter-
feit medicine packages
were found in Australia, New Zealand, Great Britain and
the United States. All in all, law enforcement agents arrest-
ed a total of 237 individuals in May as a part of the world-
wide crackdown, which resulted in the seizure of counter-
feit and illegal medicines worth $31.4 million.2
Some of the counterfeit drugs that U.S. consumers ordered
included medications such as pain relievers, hormone
medications (estrogen and human chorionic gonadotropin),
insulin and medication for erectile dysfunction. In fact, 583
packages, many of which included the medications listed
above, were seized from international mail facilities in the
United States. Many of these packages contained illegal
and counterfeit prescription medicines that had been or-
dered from Internet pharmacies online.
With today’s technology, a package of sophisticated coun-
terfeit dosage units can look identical to the real product.
Unfortunately, there is no way to tell if a tablet or capsule is
real or fake, which is why online pharmacies are so dan-
gerous to consumers. When individuals purchase prescrip-
tion medications from outside the direct supply chain, there
is no way to ensure that the medicines they are receiving
contain the correct active ingredient and proper dosages.
Customers of online pharmacies face many possible risks,
the most serious being
health risks — patients
may experience a reac-
tion to the counterfeit
medication, or may re-
ceive no therapeutic ben-
efit at all. In addition, con-
sumers can face other
risks, such as credit card
fraud, identity theft or
computer viruses.3
The FDA has been work-
ing to target the counterfeit medicines market, and this
worldwide operation worked to do just that. The FDA not
only seized almost 20,000 counterfeit medicine packages,
but also notified Internet service providers and domain
name registrars of the 10,603 websites that were guilty of
selling illegal prescription medications.
In conclusion, the Food and Drug Administration stated that
it will continue to reinforce its national as well as interna-
tional affiliations to “shed light on these Internet-based
fraudulent activities,” indicated Philip Walsky, acting direc-
tor of the FDA’s Office of Criminal Investigations. Hopefully
the FDA also will continue to uphold the stringent drug
manufacturing standards and regulations that are present
in our country, to help protect our people.
Have an Idea?: This column is designed to address timely and practical
issues of interest to pharmacists, pharmacy interns and
pharmacy technicians with the goal being to encourage
thought, reflection and exchange among practitioners.
Suggestions regarding topics for consideration are wel-
come. Please send them to [email protected].

November 2014
THE KENTUCKY PHARMACIST 35
Pharmacy Policy Issues
The Kentucky Pharmacist is online!
Go to www.kphanet.org, click on Communications
and then on The Kentucky Pharmacist link.
Would you rather receive the journal electronically?
Email [email protected] to be placed on the Green list for electronic delivery.
Once the journal is published, you will receive an email
with a link to the online version.
References:
1. "General Information on Counterfeit Medicines." WHO.
World Health Organization, n.d. Web. 07 July 2014.
<http://www.who.int/medicines/services/counterfeit/
overview/en/>.
2. Hirschler, Ben. "Fake Medicines worth $31 Million
Seized in Global Crackdown." Reuters. Thomson Reu-
ters, 22 May 2014. Web. 07 July 2014. <http://
www.reuters.com/article/2014/05/22/us-
pharmaceuticals-counterfeit-
idUSKBN0E21DG20140522>.
3. Preidt, Robert. "Illegal Online Meds Targeted in World-
wide Crackdown, FDA Says." Consumer HealthDay.
Food and Drug Administration, 22 May 2014. Web. 07
July 2014. <http://consumer.healthday.com/health-
technology-information-18/computers-internet-144/
breaking-brief-5-22-illegal-online-pharmacies-fda-
release-688137.html>.

November 2014
THE KENTUCKY PHARMACIST 36
Pharmacists Mutual

November 2014
THE KENTUCKY PHARMACIST 37
Cardinal Health
November 2014
THE KENTUCKY PHARMACIST 38
KPhA BOARD OF DIRECTORS
Duane Parsons, Richmond Chair
[email protected] 502.553.0312
Bob Oakley, Louisville President
Chris Clifton, Villa Hills President-Elect
Brooke Hudspeth, Lexington Secretary
Glenn Stark, Frankfort Treasurer
Raymond J. Bishop Past President
[email protected] Representative
Directors
Matt Carrico, Louisville*
Tony Esterly, Louisville
Matt Foltz, Villa Hills
Chris Killmeier, Louisville
Mallory Megee, Nicholasville University of Kentucky
[email protected] Student Representative
Jeff Mills, Louisville
Chris Palutis, Lexington
Christian Polen Sullivan University
[email protected] Student Representative
Richard Slone, Hindman
Mary Thacker, Louisville
Sam Willett, Mayfield
* At-Large Member to Executive Committee
HOUSE OF DELEGATES
Ethan Klein, Louisville Speaker of the House
Chris Harlow, Louisville Vice Speaker of the House
KPERF ADVISORY COUNCIL
Kim Croley, Corbin
Kimberly Daugherty, Louisville
Mary Thacker, Louisville
Matt Carrico, Louisville
KPhA/KPERF HEADQUARTERS
1228 US 127 South, Frankfort, KY 40601
502.227.2303 (Phone) 502.227.2258 (Fax)
www.kphanet.org
www.facebook.com/KyPharmAssoc
www.twitter.com/KyPharmAssoc
www.twitter.com/KPhAGrassroots
www.youtube.com/KyPharmAssoc
Robert McFalls, M.Div.
Executive Director
Scott Sisco, MA
Director of Communications & Continuing Education
Angela Gibson
Director of Membership & Administrative Services
Leah Tolliver, PharmD
Director of Pharmacy Emergency Preparedness
Elizabeth Ramey
Receptionist/Office Assistant
KPhA Board of Directors/Staff
KPhA sends email announcements weekly. If you aren’t receiving: eNews, Legislative
Updates, Grassroots Alerts and other important announcements, send your email address to
[email protected] to get on the list.
November 2014
THE KENTUCKY PHARMACIST 39
Kentucky Pharmacists Association 1228 US 127 South Frankfort, KY 40601 (502) 227-2303 www.kphanet.org Kentucky Board of Pharmacy State Office Building Annex, Ste. 300 125 Holmes Street Frankfort, KY 40601 (502) 564-7910 www.pharmacy.ky.gov Pharmacy Technician Certification Board (PTCB) 2215 Constitution Avenue Washington, DC 20037-2985 (800) 363-8012 www.ptcb.org
Kentucky Society of Health-System Pharmacists P.O. Box 4961 Louisville, KY 40204 (502) 456-1851 x2 (502) 456-1821 (fax) www.kshp.org [email protected]
American Pharmacists Association (APhA) 2215 Constitution Avenue NW Washington, DC 20037-2985 (800) 237-2742 www.aphanet.org
National Community Pharmacists Association (NCPA) 100 Daingerfield Road Alexandria, VA 22314 (703) 683-8200 [email protected]
Drug Information Center Sullivan University College of Pharmacy 2100 Gardiner Lane Louisville, KY 40205 (502) 413-8638 www.sullivan.edu Kentucky Regional Poison Center (800) 222-1222
Frequently Called and Contacted
50 Years Ago/Frequently Called and Contacted
KPhA Remembers KPhA desires to honor members who are no longer with us. Please keep KPhA
informed by sending this information to [email protected].
Deceased members for each year will be honored permanently at the KPhA office.
50 Years Ago at KPhA FROM E.M. JOSEY’S SCOOPS ‘N’ SCRAPS
First District Auxiliary
The Auxiliary to the First District of the Kentucky Pharmaceutical Association has made a
right generous contribution to the Kentucky Council on Pharmaceutical Education Scholar-
ship Fund. First, we want to thank the girls in West Kentucky for their interest in Pharmacy
and for their help, and second, we want to extend a most cordial invitation to anyone else
who would like to contribute.
- From The Kentucky Pharmacist, December 1964, Volume XXVII, Number 12.

November 2014
THE KENTUCKY PHARMACIST 40
THE
Kentucky PHARMACIST
1228 US 127 South
Frankfort, KY 40601
For more upcoming events, visit www.kphanet.org.
Save the Date
137th KPhA Annual
Meeting & Convention
June 25-28, 2015
Holiday Inn University Plaza and Sloan Convention Center
Bowling Green, KY
Come see Liz and Angela!


















