The influence of psychological factors on postpartum...
16
DRO Deakin Research Online, Deakin University’s Research Repository Deakin University CRICOS Provider Code: 00113B The influence of psychological factors on postpartum weight retention 12 months post-birth Citation: Collings, Rhian, Hill, Briony and Skouteris, Helen 2018, The influence of psychological factors on postpartum weight retention 12 months post-birth, Journal of reproductive and infant psychology, vol. 36, no. 2, pp. 177-191. DOI: http://www.dx.doi.org/10.1080/02646838.2018.1424323 © 2018, The Authors Reproduced by Deakin University under the terms of the Creative Commons Attribution Non- Commercial No-Derivatives Licence Downloaded from DRO: http://hdl.handle.net/10536/DRO/DU:30110320
Transcript of The influence of psychological factors on postpartum...

DRO Deakin Research Online, Deakin University’s Research Repository Deakin University CRICOS Provider Code: 00113B
The influence of psychological factors on postpartum weight retention 12 months post-birth
Citation: Collings, Rhian, Hill, Briony and Skouteris, Helen 2018, The influence of psychological factors on postpartum weight retention 12 months post-birth, Journal of reproductive and infant psychology, vol. 36, no. 2, pp. 177-191. DOI: http://www.dx.doi.org/10.1080/02646838.2018.1424323
© 2018, The Authors
Reproduced by Deakin University under the terms of the Creative Commons Attribution Non-Commercial No-Derivatives Licence
Downloaded from DRO: http://hdl.handle.net/10536/DRO/DU:30110320

Journal of reproductive and infant psychology, 2018vol. 36, no. 2, 177–191https://doi.org/10.1080/02646838.2018.1424323
The influence of psychological factors on postpartum weight retention 12 months post-birth
Rhian Collings, Briony Hill and Helen Skouteris
school of psychology, deakin university, geelong, australia
ABSTRACTBackground: During the first postpartum year 20% of women retain excessive weight from pregnancy (postpartum weight retention; PPWR), which predicts long-term overweight/obesity.Objective: The aim of this study was to explore the associations between psychological factors (depression, anxiety and stress symptoms and body attitudes) in late gestation and at 12-months postpartum with PPWR one-year post-birth.Methods: Pregnant women (N = 176) completed questionnaires in early–mid pregnancy (Time 1; mean (SD) = 16.97 (1.35) weeks), late pregnancy (Time 2; mean (SD) = 33.33 (2.05) weeks), and one year postpartum (Time 3; mean (SD) = 53.12 (3.34) weeks). Women provided demographic characteristics, height and pre-pregnancy weight at Time 1. At Times 2 and 3, weight, depressive, anxiety and stress symptoms and body attitudes (salience of weight and shape, attractiveness, feeling fat, and strength and fitness) were assessed in addition to physiological, socio-contextual and lifestyle factors. Gestational weight gain and PPWR were calculated. Hierarchical linear regression models were conducted to explore variance in 12-month PPWR.Results: Overall, models explained 26–39% variance in PPWR. Gestational weight gain in late pregnancy and low attractiveness at 12 months postpartum were the only variables associated significantly with 12-month PPWR.Conclusion: While psychological factors did not appear to be important direct contributors to PPWR at 12 months, the overall contribution of all variables suggests that such factors may be implicated in a small and incremental way. Exploration of the interactions between variables will help unpack potential mechanisms of the development of PPWR at 12 months post-birth.
Introduction
Weight gain in women of reproductive age contributes to obesity in child-bearing women (Lan-Pidhainy, Nohr, & Rasmussen, 2013; Melzer & Schutz, 2010). Postpartum weight reten-tion (PPWR) contributes to this health issue (Holland, Groth, & Kitzman, 2015; Montpetit, Plourde, Cohen, & Koski, 2012). One in five women experience substantial PPWR (Althuizen,
© 2018 the author(s). published by informa uK limited, trading as taylor & francis group.this is an open access article distributed under the terms of the creative commons attribution-noncommercial-noderivatives license (http://creativecommons.org/licenses/by-nc-nd/4.0/), which permits non-commercial re-use, distribution, and reproduction in any medium, provided the original work is properly cited, and is not altered, transformed, or built upon in any way.
KEYWORDSpostpartum weight retention; gestational weight gain; depressive symptoms; body dissatisfaction
ARTICLE HISTORYreceived 13 december 2016 accepted 11 november 2017
CONTACT Briony hill [email protected]
OPEN ACCESS

178 R. COLLINGS ET AL.
van Poppel, de Vries, Seidell, & van Mechelen, 2011), classified as the retention of 5 kg or more above pre-pregnancy weight at 6 months and one year after delivery (Gunderson et al., 2008; Phillips, King, & Skouteris, 2014). Excessive PPWR contributes to the development of several chronic lifestyle diseases (Kac, Benicio, Velasquez-Melendez, & Valente, 2004; Rooney, Shauberger, & Mathiasen, 2005), increases the risk of mental illness including post-partum mood disorders (Astrachan-Fletcher, Veldhuis, Lively, Fowler, & Marcks, 2008) and is implicated in higher weight status in both the short (Zilko, Rehkopf & Abrams, 2010) and long term (Linné, Dye, Barkeling, & Rossner, 2004). In order to implement effective interven-tion and prevention strategies to reduce the associated health outcomes of long-term obe-sity, it is important to understand the aetiology and perpetuating factors for PPWR within the first year post-birth.
Various physiological, sociocultural, medical and behavioural factors have been associated with PPWR. The most salient of these is excessive gestational weight gain (GWG), which is defined as weight gain above the recommended range for each BMI category according to the Institute of Medicines (IOM) guidelines (2009; Amorim, Rossner, Neovius, Lourenco, & Linné, 2007; Martin, Hure, Macdonald-Wicks, Smith, & Collins, 2014). Additional factors include high pre-pregnancy body mass index (BMI; Davis, Zyzanski, Olson, Stange, & Horwitz, 2009), poor sleep quality at 6 months postpartum (Gunderson et al., 2008), poor socioeco-nomic status (Shrewsbury, Robb, Power, & Wardle, 2009), reduced social support (Sterling et al., 2009), low maternal education (Siega-Riz et al., 2010), older age (Kac et al., 2004), multiparity (Gunderson & Abrams, 1999), low levels of breastfeeding (Kac et al., 2004) and decreased physical activity during both pregnancy and postpartum (Althuizen et al., 2011).
In contrast to research on physiological, sociocultural, medical and behavioural factors, the contribution and importance of psychological factors measured during pregnancy and in the late postpartum period to PPWR one year post-birth is comparatively less understood (Siega-Riz et al., 2010). Symptoms of depression, stress and anxiety during pregnancy and the early postpartum (up to 6 months) are associated with PPWR (Herring et al., 2008; Pederson et al., 2011; Phillips, King, & Skouteris, 2013; Phillips et al., 2014; Whitaker, Young-Hyman, Vernon, & Wilcox, 2014). Moreover, body image concerns among postpartum women are reportedly associated with depression, stress and anxiety (Walker, 1998). It has been argued that postpartum women may experience psychological distress due to an inability to return to their pre-pregnancy weight quickly (Walker, Timmerman, Kim, & Sterling, 2002), and when the perception of their weight is no longer attributed to pregnancy, body dissat-isfaction ensues (Clark, Skouteris, Wertheim, Paxton, & Milgrom, 2009b; Gjerdingen et al., 2009; Rallis, Skouteris, Wertheim, & Paxton, 2007). Among investigations of psychological correlates of PPWR at 12 months postpartum, research has been limited to observing only depressive symptoms (Siega-Riz et al., 2010), only depressive and stress symptoms (Whitaker et al., 2014), or excluding psychological factors altogether (He, Hu, Chen, Wang, & Qin, 2014).
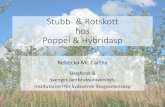
In order to deepen our understanding of the role psychological factors have with PPWR, Phillips, King, and Skouteris (2012) proposed a conceptual, multifactorial model to outline the contribution of maternal physiological and physical, socio-contextual and lifestyle, psy-chological and behavioural factors to PPWR (Figure 1). The model asserts that psychological constructs such as depressive, anxiety and stress symptoms and body dissatisfaction are implicated in women’s ability to partake in healthful behaviours, which directly impact PPWR. Phillips et al. (2013, 2014) have evaluated the contribution of these factors to PPWR at 3, 6 and 9 months postpartum, reporting that stress at 3 months postpartum was positively

JOURNAL OF REPRODUCTIVE AND INFANT PSYCHOLOGY 179
correlated with excessive PPWR at the same time point, and higher body dissatisfaction at both 3 and 6 months postpartum was associated with greater PPWR at 9 months. Evaluations of the model include exploration of the association between psychological factors experi-enced both during pregnancy and the postpartum period and their impact on PPWR because pregnancy represents a transition period where body changes occur rapidly (Park, Senior, & Stein, 2003) and persist into the postpartum (Herring et al., 2008).
Given that past studies have not simultaneously explored the contribution of psycholog-ical factors (depression, stress, anxiety, and body image) to postpartum weight retention at 12 months, the overall aim of this study was to evaluate the contribution of psychological factors to PPWR at 12 months as proposed in the model by Phillips et al. (2012). Specifically, we aimed to: (1) explore the relationship between psychological factors (depressive, anxiety and stress symptoms and body image) during late gestation with PPWR at 12 months, after controlling for the influences of socio-contextual, maternal lifestyle, physiological and phys-ical weight factors; and (2) investigate the concurrent associations between psychological factors and PPWR at 12 months, after controlling for the above variables.
Method
Participants and procedure
Pregnant women between 16 and 18 weeks gestation were recruited via advertisements in the media, parenting magazines, online forums and an antenatal clinic in the Western area of metropolitan Melbourne, Australia to take part in a postal questionnaire study exploring maternal psychosocial well-being during pregnancy and the first 12 months post-birth. Data were collected early on in pregnancy (Time 1; T1; M (SD) = 16.97 (1.35) weeks gestation), late pregnancy (Time 2; T2; M (SD) = 33.33 (2.05) weeks gestation) and at 12 months post-birth (Time 3; T3; M (SD) = 53.12 (3.34) weeks postpartum). Of 467 women recruited, 386 (83%) provided data at 32 weeks pregnant, and 246 (53%) provided data at 12 months postpartum. Participants were excluded due to no height and weight data (n = 7), substantial missing data (n = 34) and univariate/multivariate outliers (n = 27). Thus, 178 women were included
Figure 1. a conceptual model of psychosocial predictors of postpartum weight retention.

180 R. COLLINGS ET AL.
in the current analyses. There were no significant differences with respect to demographics and weight variables between the final sample and those excluded. Ethics approval was obtained from the relevant Human Research Ethics committees.
Measures
Pre-pregnancy BMI and demographics were recorded at T1 (early gestation), GWG at T2 (approximately 33 weeks gestation) and PPWR at T3 (12 months post-partum). The additional predictor variables including anxiety and distress, depression, body dissatisfaction, physical activity, social support and sleep quality were assessed at both T2 and T3. Measures are presented in the categories indicated in Phillips et al.’s (2012) model.
Outcome variable
PPWR at 12 monthsPPWR was calculated by subtracting weight at T1 (baseline) from weight at T3 (12 months post-birth). Postpartum weight retention was defined as the difference in weight of at least 5 kg compared to pre-pregnancy weight (Pederson et al., 2011).
Predictor variables
Psychological variablesPsychological distress. The Edinburgh Postnatal Depression Scale (EPDS; Cox, Holden, & Sagovsky, 1987) was used to assess depressive symptoms over the past month. The EPDS has been validated for use in the gestational and postpartum periods (Thorpe, 1993). Items were summed to achieve a global score. Cronbach’s alphas in the current study were .82 for T2 and .65 for T3.
The Depression, Anxiety, and Stress scale – Short form (DASS-21; Lovibond & Lovibond, 1995) subscales were used to assess symptoms of anxiety and stress. Symptoms were eval-uated over the past month, with higher scores signifying greater severity. Relevant items for each subscale were summed to create total subscale scores. Cronbach’s alpha for anxiety were .71 (T2) and .75 (T3), and for stress were.76 (T2) and .83 (T3).
Body attitudes. The Ben-Tovim Walker Body Attitudes Questionnaire (BAQ) was used to assess body image constructs (Ben-Tovim & Walker, 1991). Four subscales appropriate for pregnant and postpartum women were used: attractiveness, salience of weight and shape, strength and fitness and feeling fat. Scores were summed to compute a subscale score for each construct with higher scores representing greater support for each component. Cronbach’s alphas for each scale in the current study were: feeling fat .85 (T2) and .90 (T3); attractiveness .65 (T2) and .80 (T3); salience of weight and shape .71 (T2) and .85 (T3); strength and fitness .78 (T2) and .83 (T3).
CovariatesCovariates in the model were based on the factors considered to contribute to psychological distress in Phillips et al.’s (2012) conceptual model, and were classified as maternal physio-logical and physical weight factors, socio-contextual and lifestyle factors, and behaviours.

JOURNAL OF REPRODUCTIVE AND INFANT PSYCHOLOGY 181
Maternal physiological and physical weight factorsPre-pregnancy weight was assessed via self-report at T1. Weight at T2 was assessed via self-re-port. At T3, 10.7% of weight measures were collected objectively by a researcher during a home visit and the remaining were self-reported.
Pre-pregnancy BMI. Pre-pregnancy BMI was computed as kg/m2. Pre-pregnancy BMI was classified in accordance with World Health Organisation (World Health Organisation (WHO), 2000) guidelines.
Gestational weight gain. Gestational weight gain was calculated by subtracting pre-pregnancy weight (T1) from T2 weight (32 weeks gestation). Women were classified according to IOM (2009) recommendations for total GWG.
Sleep quality. Sleep quality was assessed at T2 and T3 with the Pittsburgh Sleep Quality Index (PSQI; Buysee, Reynolds, Monk, & Berman, 1989). The PSQI quantifies patterns and quality of sleep over the past month with a total indicating overall sleep quality. The scale has been validated in both pregnancy and the postpartum (Jomeen & Martin, 2007).
Socio-contextual and lifestyle factorsSocial support. Social support was assessed at T2 and T3 using the Multidimensional Scale of Perceived Social Support (MSPSS; Zimet, Dahlem, & Farley, 1988). The MSPSS measures perceived social support from family, friends and significant others. Items were summed to obtain a total score of perceived social support. Construct validity and test–retest reliability have been supported (Zimet et al., 1988). Cronbach’s alphas for the current study were .92 (T2) and .92 (T3).
Demographics. Demographic information included maternal age, ethnicity, educational attainment, household income and parity.
BehavioursAt T2 and T3, participants reported duration (in minutes) of physical activity (low to high intensity exercise) over the past week, based on one self-reported item. Exclusive breast-feeding was not included in the current study given recommendations do not exceed 6 months (WHO, 2016). As per Phillips et al.’s (2014) study at 9 months postpartum, fruit and vegetable intake was not included.
Statistical analyses and power calculation
Data were analysed using IBM SPSS Version 23.0. A total of 262 cases with substantial missing data, including incomplete time points, were removed. Data were not missing completely at random; recruitment from the general population (vs. antenatal clinic) was associated with missingness (>5%). Missing data (<5%) were found for physical activity at 12 months and GWG, which was replaced with expectation maximisation. Regression assumptions and preliminary analyses were conducted to ensure no violation of normality, linearity, multi-collinearity and homoscedasticity. Transformations did not address skew or kurtosis issues, hence multivariate and univariate outliers (according to Mahalanobis’ distance) were removed (27 cases) to improve skew/kurtosis. The final sample size was 178.

182 R. COLLINGS ET AL.
As per the approach by Phillips et al. (2014) at 3 months postpartum, two hierarchical regressions were conducted. In the first model, 12-month PPWR was regressed on 14 vari-ables from gestation (T2). In the second model, 12-month PPWR was regressed on 14 vari-ables at 12 months post-birth (T3). Recruitment source (antenatal clinic or general population) was entered at step 1 to account for missingness. In each model, GWG, pre-pregnancy BMI and sleep quality were entered at step 2 due to GWG’s strong relationship with PPWR. At step 3, demographic variables were entered, followed by maternal behavioural factors at step 4. Stress, anxiety and depressive symptoms were entered at step 5, and body attitudes at step 6.
The sample size (N = 178) gave sufficient power based on an alpha level of .05, a moderate effect size of 0.15 and 97.7% power to identify an association between psychological vari-ables and PPWR (G*Power (Version 3.1.9.2); Faul, Erdfelder, Lang, & Buchner, 2007). Furthermore, according to Green (1991), 50 + 8 k where k is the number of predictors is the minimum acceptable sample size for the regression model to be a total fit. Fourteen pre-dictor variables were included in each model, thus a minimum of 162 participants were required.
Results
Demographic characteristics of the current sample are shown in Table 1. Participants were largely Caucasian, married, educated sample, in paid employment and an average household income greater than AUD$105,000 (average yearly income in Australia in 2016–17 was approximately $80,278; Australian Bureau of Statistics, 2017). Mean age was 31.4 years (SD = 4.64; range 19–43). Pre-pregnancy BMI, GWG and PPWR are displayed in Table 1. Approximately half the women were classified as overweight/obese (n = 94; 52.8%) and 54 (30.3%) exceeded GWG recommendations. Thirty-six women (20.2%) retained greater than 5 kg at 12 months postpartum (M = 0.5 kg; SD = 6.49).
Intercorrelations for PPWR and study variables at T2 and T3 are shown in Tables 2 and 3 and results of the hierarchical linear regressions are presented in Table 5. The first regression model explored statistical predictors at T2 (late gestation) of PPWR (Table 4). At step 1, entry of recruitment source contributed no significant variance (p = .81). At step 2, physiological facets including GWG, pre-pregnancy BMI and sleep quality explained 17.7% of the variance in PPWR (∆R2 = .20, F(3, 153) = 12.54, p < .001), with GWG the only unique predictor (β = .46, p < .001). Social support, age and education (step 3), contributed no significant additional variance (p = .70). Similarly, physical activity duration at step 4 (p = .47), depression, anxiety and stress symptoms at step 5 (p = .50) and body attitude constructs at step 6 (p = .16) offered no additional significant contribution to variance in PPWR. Overall, this model explained 25.6% of the total variance of PPWR at 12 months postpartum.
A second hierarchical regression was conducted to explore predictors at T3 (postpartum) of PPWR at 12 months post-birth (Table 5). Recruitment source (step 1) was not associated with 12-month PPWR (p = .83). At step 2, GWG, pre-pregnancy BMI and sleep quality accounted for 21.7% of the variance in PPWR (∆R2 = .21, F(3,153) = 14.15, p < .001). At step 3, social support, age, and education offered no additional unique variance (p = .72). Entry of physical activity (step 4) along with depression (p = .65), anxiety and stress symptoms (p = .86; step 5), explained no further variance in PPWR. At step 6, feeling fat, attractiveness, salience of weight and shape and feelings of strength and fitness added 15.7% variance

JOURNAL OF REPRODUCTIVE AND INFANT PSYCHOLOGY 183
(∆R2 = .04, F(4,142) = 9.12, p < .001), with attractiveness contributing uniquely to the model (β = –.32, p < .001). Overall, the model explained 38.7% of the total variance of PPWR at 12 months postpartum.
Table 1. demographic characteristics of sample (N = 178).
n % Mean SDage 19–25 18 9.9 26–29 48 26.9 30–34 70 39.5 35–39 37 20.5 40–43 5 2.5Marital status Married 140 78.7 de facto 33 18.5 never married/single 5 2.8Birth location australia 143 80.3 new Zealand 5 2.8 europe (incl. united Kingdom) 14 7.8 north america 4 2.2 asia 12 6.7education tertiary level (post high school) 159 89.4 high school or less 19 10.6employment in paid employment 145 81.5 full-time carer 33 18.5household income <aud$65,000 33 18.6 aud$65,000–aud$105,000 43 24.2 >aud$105,000 100 56.9 Missing 2 1.1parity primiparous 83 46.6 Multiparous 95 53.4substance use during pregnancy smoking 1 0.6 alcohol (2 glasses or more at one time) 119 66.9psychiatric history none 131 73.6 Minor depression 21 11.8 anxiety disorder 19 10.7 Major depression 7 3.9 antenatal or postnatal depression 6 3.3 Bipolar disorder 2 1.1 receiving current treatment 7 3.9 family history of mental illness 94 52.8pre-pregnancy BMi, kg/m2 26.5 5.94 healthy (18.5–24.9) 43.8 78 overweight (25–29.9) 33.1 59 obese (>30) 19.7 35 underweight (<18.5) 2.8 5 Missing values .6 1gWg, kg (t2) 10.66 4.93 Within 31.5 56 above 30.3 54 Below 37.6 67 Missing values .6 1ppWr, kg (t3) .54 6.49 <5 kg 75.8 138 >5 kg 20.2 36 Missing values 3.9 7

184 R. COLLINGS ET AL.
Tabl
e 2.
cor
rela
tions
of t
2 (g
esta
tiona
l) va
riabl
es (N
= 1
78).
*p <
.01.
; **p
< .0
5.
12
34
56
78
910
11
1213
14M
(ran
ge) S
D1
ppW
r–
−.0
1.4
2**
.10
.07
.00
−.1
5*.0
7.0
6−
.02
−.0
7−
.02
−.0
8.0
1.5
4 (-
20, 2
8.5)
6.3
22
pre-
preg
nanc
y BM
i–
−.2
1**
.115
.04
.16*
−.0
9.2
7**
.14
−.0
6.0
2−
.08
.11
−.0
726
.50
(15.
51, 5
0.88
) 5.2
23
gW
g–
.06
.16*
.14
−.0
0.0
0−
.13
.08
−.1
0.1
1−
.08
.04
10.6
6 (.8
, 23.
60) 4
.91
4 d
epre
ssio
n –
−.1
8*−
.28*
*.1
4−
.24*
*−
.27*
*−
.02
.05
−.2
9**
.05
−.0
418
.45
(10,
24)
2.3
15
anxi
ety
–.6
3**
.04
.07
.10
.06
.01
−.0
7−
.06
.03
2.75
(0, 9
) 2.3
16
stre
ss
–−
.06
.25*
*.2
6**
.06
−.0
6−
.05
−.0
1.0
53.
13 (0
, 10)
2.4
67
attr
activ
enes
s –
−.5
1**
−.3
4**
.47*
*.0
1.1
9*.0
0.0
113
.03
(8,1
7) 1
.93
8 fe
elin
g fa
t –
.71*
*−
.33*
*−
.09
−.2
0**
−.0
8−
.05
28.1
7 (1
3, 4
8) 8
.02
9 sa
lienc
e of
wei
ght a
nd
shap
e –
−.2
5**
−.0
9−
.11
.02
.13
12.6
1 (5
, 18)
1.9
2
10 s
tren
gth
and
fitne
ss
–.1
2.1
9*−
.11
.16*
17.4
9 (1
0, 2
4) 2
.67
11 p
hysi
cal a
ctiv
ity–
−.1
4−
.11
.14
113.
64 (0
, 525
) 116
.54
12 p
erce
ived
soci
al
supp
ort
–.1
2.2
5**
73.7
9 (3
6, 8
4) 9
.16
13 a
ge
–.0
231
(19,
43) 4
.65
14 e
duca
tion
–6.
15 (2
, 8) 1
.69

JOURNAL OF REPRODUCTIVE AND INFANT PSYCHOLOGY 185
Tabl
e 3.
cor
rela
tions
of t
3 (p
ostp
artu
m) v
aria
bles
(N =
178
).
*p <
.01.
; **p
< .0
5.
12
34
56
78
910
11
1213
14M
(ran
ge) S
D1
ppW
r–
−.0
1.4
2**
.09
.05
.03
−.3
1**
.28*
*.0
6−
.12
.11
−.1
1−
.08
.01
.54
(–20
, 28.
5) 6
.32
2 pr
e-pr
egna
ncy
BMi
–−
.21*
*.0
3.1
0.0
6−
.18*
.49*
*.1
4−
.09
.40*
*−
.06
.11
.07
26.5
0 (1
5.51
, 50.
88) 5
.22
3 g
Wg
–.0
6−
.05
−.0
2.1
3−
.04
.00
.23*
*−
.07
.00
−.0
8.0
410
.66
(.8,2
3.60
)4.9
14
dep
ress
ion
–−
.18*
−.2
8**
−.3
2**
.23*
*.2
0*−
.30*
*−
.04
−.1
7*.0
6.0
318
.82
(13,
24)
2.0
65
anxi
ety
–.6
3**
−.2
5**
.26*
*.1
4−
.33*
*.2
4**
−.1
1.0
7.0
42.
22 (0
, 10)
2.3
26
stre
ss
–−
.27*
*.1
8*.2
2**
−.2
1**
.17*
.27*
*.0
5−
.08
3.04
(0, 1
0) 2
.72
7 at
trac
tiven
ess
–−
.48*
*−
.31*
*.4
7**
−.0
9−
.18*
.07
.05
2 11
5.39
(8, 2
4) 2
.81
8 fe
elin
g fa
t –
.79*
*−
.33*
*.1
1−
.22*
*.1
3−
.03
33.7
8 (1
2, 5
5) 1
0.13
9 sa
lienc
e of
wei
ght a
nd
shap
e –
−.2
3**
.05
.19*
.03
−.0
113
.43
(8, 2
0) 2
.58
10 s
tren
gth
and
fitne
ss
–.0
5−
.09
.02
.13
16.4
4 (9
, 24)
2.7
611
phy
sica
l act
ivity
–.0
2−
.08
−.0
321
4.30
(0, 9
90) 1
75.9
112
per
ceiv
ed so
cial
supp
ort
–.0
8.0
273
.84
(45,
84)
8.5
713
age
–.0
231
(19,
43) 4
.65
14 e
duca
tion
–6.
15 (2
, 8) 1
.69

186 R. COLLINGS ET AL.
Discussion
The aim of this study was to explore the relationship between psychological factors (body image and symptoms of depression, anxiety and stress) during late gestation and concur-rently with PPWR at 12 months using Phillips et al.’s (2012) conceptual model as a guide. Consistent with past research, GWG at 32 weeks pregnant was found to be the strongest predictor of PPWR one year postpartum (Amorim et al., 2007; Linné et al., 2004; Pederson
Table 4. hierarchical regression of late pregnancy variables associated with 12-month ppWr (N = 178).
**p < .001.
Predictors ∆R2 p B SE B β
Step 1 .00 .81 recruitment source −.41 1.05 .02 Step 2 .20 .00 gWg .55 .09 .46** pre-pregnancy BMi .10 .09 .08 sleep quality −.47 .65 −.05 Step 3 .01 .70 social support −.03 .05 −.05 age −.08 .10 −.06 education .16 .27 .04 Step 4 .00 .47 exercise −.00 .01 −.06Step 5 .01 .50 depressive symptoms .19 .16 .10 anxiety symptoms .13 .27 .05 stress symptoms −.32 .26 −.13 Step 6 .04 .16 feeling fat −.10 .08 −.16 strength and fitness .029 .13 .02 salience of weight and shape .14 .22 .07 attractiveness −.48 .20 −.23
Table 5. hierarchical regression of variables associated with ppWr performed at t3 (N = 178).
**p < .001.
Predictors ∆R2 p B SE B β
Step 1 .00 .83 recruitment source .245 1.12 .02 Step 2 .22 .00 gWg .62 .10 6.23** pre-pregnancy BMi .17 .09 .13 sleep quality −.33 .67 −.04 Step 3 .01 .72 social support −.06 .05 −.08 age −.02 .10 −.02 education −.02 .25 −.04 Step 4 .00 .65 physical activity .00 .00 .05 Step 5 .00 .86 depressive symptoms .17 .24 .08 anxiety symptoms −.04 .33 −.02 stress symptoms −.01 .25 −.00 Step 6 .16 .00 feeling fat .12 .07 .23 strength and fitness −.15 .11 −.11 salience of weight and shape −.18 .18 −.12 attractiveness −.55 .15 −.32**

JOURNAL OF REPRODUCTIVE AND INFANT PSYCHOLOGY 187
et al., 2011; Siega-Riz et al., 2010). Of the psychological factors, feeling less attractive at 12 months postpartum was the only variable associated with 12-month PPWR. Only two previous studies (Clark et al., 2009b; Rallis et al., 2007) have explored the association between body image with PPWR at 12 months. Rallis et al. (2007) reported no association between body image and PPWR, whilst Clark et al. (2009b) reported feeling fat and salience of weight and shape to be associated with increased PPWR. Investigation of how body image is asso-ciated with PPWR throughout the first postpartum year is similarly contradictory. For instance, Phillips et al. (2014) reported that salience of weight and shape (but not strength and fitness, feeling fat or attractiveness) at 3 and 6 months was associated with 9-month PPWR. At 9 months postpartum, Gjerdingen et al. (2009) found global body dissatisfaction to be related to PPWR. Collectively, this body of research suggests that body dissatisfaction may contribute to PPWR in complex and unique ways across the reproductive life phase. For instance, women may experience dissatisfaction with their body due to changes associated with pregnancy and childbirth (Rallis et al., 2007), diminishing the resolve to return to a pre-pregnancy weight and contributing to PPWR (Amorim et al., 2007). In contrast, the lack of association between body image during gestation with weight retention at 12 months postpartum reported here corresponds with research suggesting a temporary reprieve from body image concerns during pregnancy as a result of acceptance of the change in functionality of the pregnant body (Rallis et al., 2007; Watson, Fuller-Tyszkiewicz, Broadbent, & Skouteris, 2015) and there-fore body image concerns in pregnancy are not directly related to PPWR. Additionally, the lower Cronbach’s alpha of attractiveness in the present study (α = 0.65) at the end of gesta-tion may indicate women’s varied experiences of attractiveness during pregnancy, whereby some women may feel unattractive in later stages of pregnancy and other women may embrace a new type of attractiveness associated with pregnancy. Consequently, the preg-nancy period where some women are more ‘accepting’ of their body could be an opportunity educate women about body image concerns that may be experienced in the postpartum, including elements surrounding realistic weight and emotional changes likely to occur (Clark, Skouteris, Wertheim, Paxton, & Milgrom, 2009a).
The lack of association between depressive and anxiety symptoms during gestation and at 12 months postpartum may indicate that the salience of psychological distress and its potential impact on weight retention reduces throughout the postpartum period. Phillips et al. (2013) found stress to contribute a significant amount of variance to 3-month PPWR. Previous studies have found women experience higher depression and anxiety symptoms at 3 and 6 months postpartum compared to 12 months (McCall-Hosenfeld, Phiri, Shaefer, Zhu, & Kjerulff, 2016).
Maternal physiological, socio-contextual and medical factors were proposed to influence PPWR in the model described by Phillips et al. (2012). Contrary to previous findings, we found no associations between these factors either during pregnancy or at 12 months postpartum with 12-month PPWR (Kac et al., 2004; Siega-Riz et al., 2010). Hence, it is possible that these factors are implicated in late PPWR indirectly (Riley, 2011; e.g. by influencing factors that are more closely related to PPWR such as physical activity or dietary behaviours) or that other factors not included in Phillips et al. (2012) model have stronger associations with PPWR. Maternal behaviour, specifically physical activity, proposed to directly influence PPWR was not found to be significantly associated with 12-month PPWR in this study. This could be due to the brevity of the measure used and its insensitivity in picking up small changes in activity levels (Australian Institute of Health and Wellbeing, 2003). Past research has indicated

188 R. COLLINGS ET AL.
structured physical activity is associated with reduced 12-month PPWR (O’Toole, Sawicki, & Artal, 2004). It has been suggested that pregnant women disengage from healthy lifestyles (such as physical activity) and develop poor maternal behaviours, which may transfer into the postpartum, creating suboptimal behaviours, thus preventing successful weight loss (van der Pligt et al., 2016). Atkinson, Shaw, and French (2016) explored women’s decisions regarding behaviours throughout pregnancy and found women act upon bodily signals and perception of acceptable behaviour, which were often contrary to what health professionals advised and tended to follow a view of a temporary respite from a healthful lifestyle. While not possible in the current study due to the large number of predictor variables and restric-tive sample size, other analysis methods such as path analysis will allow this possibility to be tested and may provide insight into the mechanisms implicated in the development of 12-month PPWR.
One quarter of the variance in 12-month PPWR was explained by the variables in late pregnancy included in the model, and concurrently measured predictors explained almost 40% of the variance in 12-month PPWR. Whitaker et al. (2014) tested a model of stress, GWG and demographic factors on PPWR, finding that 23% of the variance in 12-month PPWR was explained by their model. Given the additional variables included in our model these findings appear consistent, but suggest that comprehensive models of determinants of PPWR have added value when variables are evaluated together rather than independently.
Limitations
Firstly, the study’s sample is relatively homogeneous; the majority of participants reported characteristics commensurate with a high socioeconomic status. As such, the findings cannot be generalised to more diverse populations given individuals with alternate ethnicities or lower socioeconomic status may experience different psychosocial concerns (Huang, Wang, & Dai, 2010) and PPWR (Shrewsbury et al., 2009). In addition to this, although it is possible that women who dropped out of the study differed from women who were retained (albeit this was not apparent when comparing included and excluded women), the high drop-out rate when going from pregnancy (T2) to postpartum (T3) is a limitation of the study. Secondly, the majority of weight data were reported subjectively. However, the accuracy of self-re-ported weight in perinatal populations has been found to be satisfactory (Herring et al., 2008; McPhie et al., 2011). Thirdly, dietary variables could not be included in our model due to substantial missing data. Consequently, the contribution of dietary behaviours to 12-month PPWR could not be ascertained. Past research has identified poor dietary intake with high levels of total energy intake is associated with increased weight retention (Oken, Taveras, Popoola, Rich-Edwards, & Gillman, 2007). Finally, early postpartum predictors of 12-month PPWR were not explored due to sample size restrictions.
Conclusion
While depression, anxiety and stress symptoms during late pregnancy or at 12 months post-partum were not associated with 12-month PPWR, feelings of attractiveness were signifi-cantly and concurrently related to 12-month PPWR. This was the first study to explore the concurrent associations at this time point. The value of comprehensive and multifactorial models understanding weight outcomes (e.g. Phillips et al., 2012) are important to consider

JOURNAL OF REPRODUCTIVE AND INFANT PSYCHOLOGY 189
in future research due to the collective value of variables associated with PPWR. Furthermore, unpacking and exploring the changes of body image throughout pregnancy and postpartum is essential; support and education regarding acceptance of the bodily changes occurring during the reproductive life phase may assist in curbing weight gain associated with childbearing.
Disclosure statement
No potential conflict of interest was reported by the authors.
Funding
Briony Hill is funded by an Alfred Deakin Postdoctoral Research Fellowship.
ORCID
Helen Skouteris http://orcid.org/0000-0001-9959-5750
References
Althuizen, E., van Poppel, M., de Vries, J. H., Seidell, J. C., & van Mechelen, W. (2011). Postpartum behaviour as a predictor of weight change from before pregnancy to one year postpartum. BMC Public Health, 11(1), 149–149171. doi:10.1186/1471-2458-11-165
Amorim, A. R., Rossner, S., Neovius, M., Lourenco, P. M., & Linné, Y. (2007). Does excess pregnancy weight gain constitute a major risk for increasing long-term BMI?* Obesity, 15(5), 1278–1286.
Astrachan-Fletcher, E., Veldhuis, C., Lively, N., Fowler, C., & Marcks, B. (2008). The reciprocal effects of eating disorders and the postpartum period: A review of the literature and recommendations for clinical care. Journal of Women’s Health, 17(2), 227–239. doi:10.1089/jwh.2007.0550
Atkinson, L., Shaw, R. L., & French, D. P. (2016). Is pregnancy a teachable moment for diet and physical activity behaviour change? An interpretative phenomenological analysis of the experiences of women during their first pregnancy. British Journal of Health Psychology, 21(4), 842–858. doi:10.1111/bjhp.12200
Australian Bureau of Statistics (ABA). (2017). May key figures. Canberra, Australia: ABA.Australian Institute of Health and Wellbeing (AIHW). (2003). The active Australia survey: A guide and
manual for implementation, analysis and reporting. Canberra, Australia: AIHW.Ben-Tovim, D. I., & Walker, M. K. (1991). The development of the Ben-Tovim Walker Body Attitudes
Questionnaire (BAQ), a new measure of women's attitudes towards their own bodies. Psychological Medicine, 21(3), 775–784. doi:10.1017/S003329170002240
Buysee, D. J., Reynolds, C. F., Monk, T. H., & Berman, S. R. (1989). The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Journal of Psychiatric Research, 28(2), 193–213. doi:10.1016/0165-1781(89)90047-4
Clark, A., Skouteris, H., Wertheim, E. H., Paxton, S. J., & Milgrom, J. (2009a). My baby body: A qualitative insight into women’s body-related experiences and mood during pregnancy and the postpartum. Journal of Reproductive & Infant Psychology, 27(4), 330–345. doi:10.1080/02646830903190904
Clark, A., Skouteris, H., Wertheim, E. H., Paxton, S. J., & Milgrom, J. (2009b). The relationship between depression and body dissatisfaction across pregnancy and the postpartum: A prospective study. Journal of Health Psychology, 14(1), 27–35.
Cox, J. L., Holden, J. M., & Sagovsky, R. (1987). Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. British Journal of Psychiatry, 150(6), 782–786.
Davis, E. M., Zyzanski, S. J., Olson, C. M., Stange, K. C., & Horwitz, R. I. (2009). Racial, ethnic, and socioeconomic differences in the incidence of obesity related to childbirth. American Journal of Public Health, 99(2), 294–299. doi:10.2105/AJPH.2007

190 R. COLLINGS ET AL.
Faul, F., Erdfelder, E., Lang, A., & Buchner, A. (2007). G*Power 3: A flexible statistical power analysis program for the social, behavioural, and biomedical sciences. Behavioral Research Methods, 39(2), 175–191. doi:10.3758/BF03193146
Gjerdingen, D., Fontaine, P., Crow, S., McGovern, P., Center, B., & Miner, M. (2009). Predictors of mothers' postpartum body dissatisfaction. Women and Health, 49(6–7), 491–504.
Green, S. B. (1991). How many subjects does it take to do a regression analysis? Multivariate Behavioral Research, 26(3), 499–510. doi:10.1207/s15327906mbr2603_7
Gunderson, E. P., & Abrams, B. (1999). Epidemiology of gestational weight gain and body weight changes after pregnancy. Epidemiology Review, 21(2), 261–275. doi:10.1093/oxfordjournals.epirev.a018001
Gunderson, E. P., Rifas-Shiman, S. L., Oken, E., Rich-Edwards, J. W., Kleinmann, K. P., Taveras, E. M., & Gillman, M. W. (2008). Association of fewer hours of sleep at 6 months postpartum with substantial weight retention at 1 year postpartum. American Journal of Epidemiology, 167, 178–187.
He, X., Hu, C., Chen, L., Wang, Q., & Qin, F. (2014). The association between gestational weight gain and weight retention 1-year postpartum. Archives of Gynecology and Obstetrics, 290(3), 493–499.
Herring, S. J., Rich-Edwards, J. W., Oken, E., Rifas-Shiman, S. L., Kleinman, K. P., & Gillman, M. W. (2008). Association of postpartum depression with weight retention one year after childbirth. Obesity, 16(6), 1296–1301. doi:10.1038/oby.2008.71
Holland, M. L., Groth, S. W., & Kitzman, H. J. (2015). Gestatational weight gain and health outcomes 18 years later. Maternal and Child Health Journal, 19(10), 2261–2271. doi:10.1007/s10995-015-1745-7
Huang, T., Wang, H., & Dai, F. (2010). Effect of pre-pregnancy body size on postpartum weight retention. Midwifery, 26(2), 222–231. doi:10.1016/jmidw.2008.05.001
Institute of Medicine (IOM). (2009). Weight gain during pregnancy: Reexamining the guidelines - Report Brief. Washington, DC: National Academy Press.
Jomeen, J., & Martin, C. R. (2007). Assessment and relationship of sleep quality to depression in early pregnancy. Journal of Reproductive & Infant Psychology, 25(1), 87–99. doi:10.1080/02646830601117308
Kac, G., Benicio, M. H., Velasquez-Melendez, G., & Valente, J. G. (2004). Gestational weight gain and prepregnancy weight influence postpartum weight retention in a cohort of Brazilian women. The Journal of Nutrition, 134, 661–666.
Lan-Pidhainy, X., Nohr, E. A., & Rasmussen, K. M. (2013). Comparison of gestational weight gain-related pregnancy outcomes in American primiparous and multiparous women. American Journal of Clinical Nutrition, 97(5), 1100–1106. doi:10.3945/ajcn.112.052258
Linné, Y., Dye, L., Barkeling, B., & Rossner, S. (2004). Long-term weight development in women: A 15-year follow-up of the effects of pregnancy. Obesity Research, 12(7), 1166–1178. doi:10.1038/oby.2004.146
Lovibond, S. H., & Lovibond, P. F. (1995). Manual for the depression anxiety stress scales. Sydney, Australia: Psychology Foundation.
Martin, J. E., Hure, A. J., Macdonald-Wicks, L., Smith, R., & Collins, C. E. (2014). Predictors of post-partum weight retention in a prospective longitudinal study. Maternal and Child Nutrition, 10(4), 496–509.
McCall-Hosenfeld, J. S., Phiri, K., Shaefer, E., Zhu, J., & Kjerulff, K. (2016). Trajectories of depressive symptoms throughout the peri and postpartum period: Results from the first baby study. Journal of Womens Health, 25(11), 1112–1121. doi:10.1089/jwh.2015.5310
McPhie, S., Skouteris, H., McCabe, M., Ricciardelli, L. A., Milgrom, J., Baur, L. A., & Dell’aquila, D. (2011). Maternal correlates of preschool child eating behaviours and body mass index: A cross-sectional study. International Journal of Pediatric Obesity, 6(5–6), 476–480.
Melzer, K., & Schutz, Y. (2010). Pre-pregnancy and pregnancy predictors of Obesity. International Journal of obesity, 34, 2–44.
Montpetit, A. E., Plourde, H., Cohen, T. R., & Koski, K. G. (2012). Modeling the impact of pre pregnancy BMI, physical activity, and energy intake on gestational weight gain, infant birth weight, and postpartum weight retention. Journal of Physical Activity & Health, 9(7), 1020–1029.
O’Toole, M. L., Sawicki, M. A., & Artal, R. (2004). Structured diet and physical activity prevent postpartum weight retention. Journal of Women’s Health, 12, 10. doi:10.1089/154099903322643910
Oken, E., Taveras, E. M., Popoola, F. A., Rich-Edwards, J. W., & Gillman, M. W. (2007). Television, walking, and diet: Associations with postpartum weight retention. American Journal of Preventative Medicine, 32(4), 305–311. doi:10.1016/j.amepre.2006.11.012

JOURNAL OF REPRODUCTIVE AND INFANT PSYCHOLOGY 191
Park, R. J., Senior, R., & Stein, A. (2003). The offspring of mothers with eating disorders. European Child & Adolescent Psychiatry, 12, 110. doi:10.1007/s00787-003-1114-8
Pederson, P., Baker, J. L., Henriksen, T. B., Lissner, L., Heitmann, B. L., Sorenson, T. I., & Nohr, E. A. (2011). Influence of psychosocial actors on postpartum weight retention. Obesity, 19(3), 639–646.
Phillips, J., King, R., & Skouteris, H. (2012). A conceptual model of psychological predictors of postpartum weight retention. Journal of Reproductive and Infant Psychology, 30(3), 278–288.
Phillips, J., King, R., & Skouteris, H. (2013). The influence of psychological distress during pregnancy on early postpartum weight retention. Journal of Reproductive and Infant Psychology, 32, 25–40.
Phillips, J., King, R., & Skouteris, H. (2014). The influence of psychological factors on postpartum weight retention at 9 months. British Journal of Health Psychology, 19(4), 751–766.
van der Pligt, P., Olander, E. K., Ball, K., Crawford, D., Hesketh, K. D., Teychenne, M., & Campbell, K. (2016). Maternal dietary intake and physical activity habits during the postpartum period: Associations with clinical advice in a sample of Australian first time mothers. BMC Pregnancy and Chilbirth, 16(1), 278. doi:10.1186/s12884-016-0812-4
Rallis, S., Skouteris, H., Wertheim, E. H., & Paxton, S. J. (2007). Predictors of body image during the first year postpartum: A prospective study. Women and Health, 45(1), 87–104.
Riley, H. (2011). Weight management before, during and after pregnancy – what are the “rules”? Nutrition Bulletin, 36(2), 212–215. doi:10.1111/j.1467-3010.2011.01891.x
Rooney, B. L., Shauberger, C. W., & Mathiasen, M. A. (2005). Impact of perinatal weight change on long-term obesity and obesity-related illness. Obstretrics & Gynecology, 106(6), 1349–1356. doi:10.1097/01.AOG.0000185480.09068.4a
Shrewsbury, V. A., Robb, K. A., Power, C., & Wardle, J. (2009). Socioeconomic differences in weight retention, weight-related attitudes and practices in postpartum women. Journal of Maternal & Child Health, 13(2), 231–240.
Siega-Riz, A. M., Herring, A. H., Carrier, K., Evenson, K. R., Dole, N., & Deierlein, A. (2010). Sociodemographic, perinatal, behavioural, and psychosocial predictors of weight retention at 3 and 12 months postpartum. Obesity, 18(10), 1996–2003.
Sterling, B. S., Fowles, E. R., Garcia, A. A., Jenkins, S. K., Wilkinson, S., Kim, M., & Walker, L. O. (2009). Altered perceptions of personal control about retained weight and depressive symptoms in low-income postpartum women. Journal of Community Health Nursing, 26(3), 143–157.
Thorpe, K. (1993). A study of the Edinburgh Postnatal Depression Scale for use with parent groups outside of the postpartum period. Journal of Reproductive & Infant Psychology, 11(2), 119–125. doi:10.1080/02646839308403204
Walker, L. O. (1998). Weight-related distress in the early months after childbirth. Western Journal of Nursing Research, 20(1), 30–44.
Walker, L., Timmerman, G. M., Kim, M., & Sterling, B. (2002). Relationships between body image and depressive symptoms during postpartum in ethnically diverse, low income women. Women & Health, 26(3), 101–121.
Watson, B., Fuller-Tyszkiewicz, M., Broadbent, J., & Skouteris, H. (2015). The meaning of body image experiences during the perinatal period: A systematic view of the qualitative literature. Body Image, 14, 102–113. doi:10.1016/j.bodyim.2015.04.005
Whitaker, K., Young-Hyman, D., Vernon, M., & Wilcox, S. (2014). Maternal stress predicts postpartum weight retention. Maternal Child Health Journal, 18(9), 2209–2217.
World Health Organisation (WHO). (2000). Obesity: Preventing & managing the global epidemic. Geneva, Switzerland: WHO.
World Health Organisation (WHO). (2016). Breastfeeding. Geneva, Switzerland: WHO.Zilko, C. E. M., Rehkopf, D., & Abrams, B. (2010). Association of maternal gestational weight gain with
short- and long-term maternal and child health outcomes. American Journal of Obstetrics and Gynecology, 202(6), 574. doi:10.1016/j.ajog.2009.12.007
Zimet, G. D., Dahlem, S. G., & Farley, G. K. (1988). The multi-dimensional scale of perceived social support. Journal of Personality Assessment, 52(1), 30–41. doi:10.1207/s15327752jpa5201_2