
The in-house magazine for the IAS Private Members Club REVOLUTION! - Aging … · 2018-10-30 ·...
27
The in-house magazine for the IAS Private Members Club In this issue: No2, 2018 US $10 / EU €8 / GB £7 The peptide biomarker revolution The latest about gene switches Vitamin B17 and cancer Looking to a world without cancer Fighting Alzheimer’s disease How a snow-drop extract can help Why bother? Being concerned about preventing disease REVOLUTION! s ue e e u
Transcript of The in-house magazine for the IAS Private Members Club REVOLUTION! - Aging … · 2018-10-30 ·...

The in-house magazine for the IAS Private Members Club
In this issue:
No2, 2018US $10 / EU €8 / GB £7
The peptide biomarker revolution
The latest aboutgene switches
Vitamin B17 and cancer
Looking to a world without cancer
Fighting Alzheimer’s disease
How a snow-drop extract can help
Why bother?
Being concerned about preventing disease
REVOLUTION!
In this issue:In this issue:In this issue:In this issue:In this issue:In this issue:In this issue:
TESTIMONIALS CONTENTS
WELCOME
DR. AUBREY DE GREY
THIERRY HERTOGHE M.D.
NICHOLAS PERRICONE M.D.
JONATHAN WRIGHT M.D.
“IAS has shown great vision and leadership, as an organisation focused mainly on the provision of contemporary medical interventions against aging, in also supporting the SENS Foundation’s efforts to hasten the development of much more powerful future interventions.”
“IAS has a history of making throughout the world crucial, but difficultly accessible medications available to patients. IAS is one of the pioneering societies in anti-aging medicine that has helped this new medical specialty move forward.”
“IAS is an outstanding resource for the finest, most up-to-date news and information on healthy aging. They also offer products of the highest integrity and efficacy. In fact, IAS is the world’s greatest source (often the only source) for the most cutting edge and advanced nutrients to ensure optimum health span and maximum life span.”
“Every adult has the right to take care of his or her own personal health as he or she chooses. In the 20th and 21st centuries, this universal human right has been nearly obliterated by an ocean of nanny-state regulation and deliberate suppression of information by bureaucracies, with hidden and not-so-hidden agendas. International Anti-aging Systems is a beacon of useful health care information and a literal island of freedom of health care product choice in our otherwise un-free health care world.”
03Welcome To our second issue of 2018
04Forefront Interesting items in the news
10The peptide biomarker revolutionAn article by Marios Kyriazis, M.D.
FEATURED PRODUCTS
50Antiaging-Systems.comWhere to find what you need
02TestimonialsNice comments from nice people
48CouponsSave money with these vouchers
14The story of vitamin B17 Otherwise known as laetrile
24Alzheimer’s disease We’re delighted to have Will Block write for us
32Why bother? Mr. Richard Swift gives his considered opinion
Revolutions are rare, but nonetheless dramatic things, they tend to rapidly overturn orthodox thinking, and so in that context we have several stories in this issue that are a revolution for health.
The first is told by Dr. Marios Kyriazis and it describes the hot-topic of the decades of secret Soviet research; research that led to the discovery that short-chain peptides (found in food) are gene switches.
Dr. Kyriazis has a new book out that details the uses of this technology and it is the first to be written specifically for the public, it is called; ‘the peptide bioregulator revolution.’
Then there is vitamin B17, a natural component of many foods, particularly apricot kernels and apple seeds etc. It is also known by other names such as amygdalin and laetrile, in this super article its controversial role in cancer is highlighted.
We are also delighted that Will Block, the former owner of Life Enhancement Inc. and one of the world’s leading
health researchers has written his first piece for the Aging Matters™ magazine. Here, he informs us about how to cope with Alzheimer’s and highlights the positive aspects of the snow-drop extract known as galantamine.
Lastly, why should we bother? Taking care of one’s health is a constant fight, not only the application of what is right for us, but also the never-ending learning of new information as it comes to light. Mr. Richard Swift, a brilliant wordsmith and legal expert in the health field shares his opinions with us.
History teaches us that countless peoples have fought hard for their freedoms. Today we demand freedom in healthcare and our right to choose.
Vive la revolution!
Phil Micans, MS, PharmB Editor, Aging Matters™ Magazine
Ward Dean, M.D. Medical Director
www.aging-matters.com
1. Declaration: The IAS Aging Matters™ magazine is intended for IAS private club members (and therefore is not intended for the public). It focuses on the latest international nutritional, hor-monal and drug therapies to help combat the signs of aging. These signs include the physical, mental and internal changes consisting of the diseases and disorders such as cancer, arthritis and senile dementias etc. However, the main focus is upon the prevention of such aging diseases and disorders for the ‘healthy-aging’ individual.
2. Copyright 2018: All copyrights are acknowledged. Whilst every effort has been made to ensure accuracy, no responsibility can be accepted for illustrations, photographs, artwork or advertis-ing materials while in transmission or with the publisher or their agents.
3. Disclaimer: All educational information is offered under IAS terms and conditions. This information does not replace the advice of your physician and restrictions may apply in some coun-tries. The opinions expressed by the writers may not be those of IAS or the magazine. Any prices shown are in US Dollars and are for reference purposes only and they do not include taxes (where applicable), nor do they include shipping & handling fees. Prices, conditions and terms are subject to change without notice.
TESTIMONIALS CONTENTS
2 AGINGMATTERS AGINGMATTERS 3

Researchers have rejuvenated mice by reversing age-related wrinkles and hair loss. It is possible that humans could get a similar make-over in the future.
Scientists at the University of Alabama at Birmingham asked, “Wrinkled skin and hair loss are hallmarks of aging, what if they could be reversed?”
They introduced a specific gene mutation on a test mouse- this prompted a drastic change in appearance. Within a four week period, the mouse had developed wrinkles and extensive hair loss. Researchers turned off the culprit mutation and regular function was restored in the gene, the mouse returned to its youthful appearance with smooth skin and thick fur only two months later.
Keshav Singh, a professor of genetics who led the study stated “To our knowledge, this observation is unprecedented.”
The professor said in a statement, “This mouse model should provide an unprecedented opportunity for development of preventive and therapeutic drug development strategies to augment the mitochondrial functions for the treatment of aging-associated skin and hair pathology and other human diseases in which mitochondrial dysfunction plays a significant role.”
During the study, the test mice were given an antibiotic which prompted the change within the gene. All of the mice showed grey hair, hair loss and thinning hair- the females has more severe wrinkles than the males.
The study said “Dramatically, this hair loss and wrinkled skin could be reversed by turning off the mutation, the wrinkled skin showed changes similar to those seen in both intrinsic and extrinsic aging- intrinsic aging is the natural process of aging, and extrinsic aging is the effect of external factors that influence aging, such as skin wrinkles that develop from excess sun or long-term smoking.”
Further Reading
Veronica Jimenez, et al. 2018 ‘ FGF21 gene therapy as treatment for obesity and insulin resistance’. DOI 10.15252/emmm.201708791| Published online 09.07.2018 EMBO Molecular Medicine (2018) e8791
DNA STRUCTURE GENETIC RESEARCHERS REVERSE WRINKLES, GREY HAIR AND BALDING IN MICE
FOREFRONT
AGINGMATTERS 54

HUMAN IMMUNE SYSTEM FIGHTING INFECTIONS
Middle aged adults could benefit from a short term treatment to revitalise the immune system and organs that deteriorate with age. Scientists have hailed the success of a clinical trial which found that experimental anti-aging drugs may protect older people from potentially fatal respiratory infections by rejuvenating their immune systems.
The trial consisted of people aged 65 and over, the participants who received the anti-aging drug combination reported nearly half the number of infections over the following year as a control group who received only placebos.
The experimental drugs used in this trial are known as mTOR inhibitors, and also appeared to boost candidate’s responses to the flu vaccine, with tests presenting 20% more flu-fighting antibodies found in the blood up to a month after the vaccine was administered.
This study’s findings are a milestone for researchers who believe that the best way to combat diseases of old age may be to design new drugs that fight the aging process itself.
Matt Kaeberlein the director of the healthy aging and longevity research institute at the University of Washington who was not involved in the study stated, “ this is an extremely important and exciting study” he added “ I think this study raises the real possibility that most middle-aged adults could benefit from short-term treatments with mTOR inhibitors.”
The drugs work by blocking events in the body that starts with the so-called ‘mechanistic target of rapamycin’, or mTOR. This is part of a group of proteins involved in the course of aging. Tests in mice have presented that experimental mTOR inhibitors can extend lifespan and rejuvenate the immune system and organs which deteriorate in old age.
The next step in the research process will be to investigate into whether the drugs work better in some groups of older people than others, an example being over 85’s or those with health conditions such as diabetes or heart failure.
Mannick the chief medical officer at a Boston-based company called resTORbio, found that the drugs boosted the immune system responses that specifically target viruses. Mannick stated, “We hope we can keep everybody healthier and with a better quality of life as they grow older.”
Further Reading
Joan B. Mannick, Et, al: 2018 ‘ TORC1 inhibition enhances immune function and reduces infections in the elderly.’ Science Translational Medicine 11 Jul 2018: Vol. 10, Issue 449, eaaq1564
DOI: 10.1126/scitranslmed.aaq1564
TRIAL OF ANTI-AGING DRUGS THAT REJUVENATE IMMUNE SYSTEM HAILED A SUCCESS
FOREFRONT
7 6 AGINGMATTERS
New research demonstrations that gene therapy can completely reverse markers of type 2 diabetes and obesity in rodents.
According to recent estimates over 30 million U.S. adults had diabetes in the year 2015 and the rates of newly diagnosed children and teenagers have greatly increased. Worldwide, the number of people diagnosed with diabetes has almost quadrupled between 1980 and 2014, according to the World Health Organization.
This new research could bring hope in curing this disorder. Fatima Bosch and her team of scientists at the Universitat Autonoma de Barcelona (UAB) in Catalunya Spain, have successfully reversed the disorder in rodents.
They achieved this using gene therapy, a method that introduces new genetic material into cells to create beneficial proteins or to counterbalance the effects of malfunctioning genes.
Researchers designed two mouse models of type 2 diabetes and obesity. One was diet induces and the other was genetically modified.
By delivering this gene, the researchers stimulated the production of protein, this caused the rodents to lose weight and lowered their insulin resistance- a crucial risk factor in type 2 diabetes. The mice also lost weight and the treatment reduced the fat and inflammation in their adipose tissue.
Using gene therapy is free of side effects, and a single dose is enough to make the mice produce the protein naturally for several years.
First study author Veronica Jimenez, a UAB researcher stated, “This is the first time that long-term reversion of obesity and insulin resistance have been achieved upon a one-time administration of a gene therapy, in an animal model that resembles obesity and type 2 diabetes in humans.“
Further Reading
Veronica Jimenez, et al. 2018 ‘ FGF21 gene therapy as treatment for obesity and insulin resistance’. DOI 10.15252/emmm.201708791| Published online 09.07.2018 EMBO Molecular Medicine (2018) e8791
GENETIC ENGINEERING OF DNA STRUCTURE TYPE 2 DIABETES, OBESITY MAY SOON BE REVERSED WITH GENE THERAPY
FOREFRONT
AGINGMATTERS 98

THE PEPTIDEBIOREGULATOR REVOLUTIONBy Marios Kyriazis MD
This summer, my new book; ‘The Peptide Bioregulator Revolution’ is being released. The book subtitled; ‘The use of bioactive peptides for aging and health’, is a review of available scientifi c evidence regarding the role of bio-active peptides (i.e. short or long sequences of amino acids), which can be used in several health conditions, and in aging itself. There exist quite a few
peptides, both natural and synthetic, which have a regulatory action on many parts of the metabolism. Many details of this action have been studied by Prof. Vladimir Khavinson, Director of the Saint-Petersburg Institute of Bioregulation and Gerontology, who, together with his team, is the main proponent of the use of bio-active peptides.
In this book there are sections on research regarding the function of peptides as bio-regulators, as well as detailed information on the benefi ts of peptides in several health conditions. Examples include bone disease, circulation and cardiac problems, muscle weakness, kidney and liver
conditions, and several other age-related degenerative diseases. The aim is to give a comprehensive introduction and analysis of this important subject, not only from a fi rm scientifi c perspective but also from a practical point of view.
MECHANISM OF PEPTIDE BIOREGULATORS EFFECT
STROMALCELL
DNA
CELL PROLIFERATIONMITOSIS
CELLULARHOMEOSTASIS
CELL DIFFERENTIATIONPROTEIN SYNTHESIS
G2 G1
DNA mRNA
PEPTIDEBIOREGULATORS
DR. KYRIAZIS LATEST BOOK ABOUT THE RUSSIAN PEPTIDE BIOREGULATORS
THE PEPTIDE BIOMARKER REVOLUTIONA 60-page booklet by Dr. Marios Kyriazis. Save $5.00 normally $14.99 just $9.99
VALID UNTIL 31/01/2019 WITH CODE REVOLUTION5
AVAILABLE AT THE LONGEVITY.STORE
THE PEPTIDE BIOREGULATOR REVOLUTION
10 AGINGMATTERS AGINGMATTERS 11

CASE STUDY
Whilst I was writing the book, I decided to try one such bio-regulator peptide, on one of my patients to see for myself if any of the claims made have some relevance in everyday medical practice. So, here, I am going to mention a case study, not as solid scientific evidence, but as food for thought and for further discussion.
The case is with regards to one male patient aged 48 years, with diagnosed and established end-stage renal failure, of unknown etiology. Creatinine was 6 to 7 times the normal levels, and blood urea was consistently over 10 times the normal levels, together with proteinuria and anaemia. The patient was due to be admitted starting peritoneal dialysis and was on the waiting list
for renal transplant. He agreed to try the renal bio-peptide Pielotax™ twice a day for 4 weeks, and the course repeated after 4 weeks, at one capsule a day for 8 weeks. His condition was stabilised and had no significant kidney-related symptoms. Peritoneal dialysis was postponed, and all blood values remain stable. This, in the absence of any other changes in his treatment, suggests that the peptides may have played a role, although this is not presented here as a firm scientific case. Nevertheless, if taken is association with other such anecdotal cases, it points at the possibility that there is indeed something positive here, something that it is endorsed by the previous positive studies of bio-peptides in the laboratory.
have found epigenetically active peptides in a long-lived species of rat. This means that the peptides can influence the DNA of the animal, depending on stimuli originating from the environment. In other words, these long-lived animals have a mechanism by which they respond positively to adverse or beneficial external challenges and are thus able to live longer. This mechanism was found to be absent in the proteins of other short-lived species of rats or mice, which suggests that it is the action of the specific peptides, operating in accordance with the given environment, that leads to increased lifespan 3. Another specific experiment gives some more details into this life-prolonging mechanism. Using a neuro-regulator peptide (called EDR) lead to an improvement of the structure of mouse neurons in culture by 71%, while a similar peptide (KED) increased it by 20%. The authors concluded that4:
“Tripeptide EDR can be recommended for further experimental study as a candidate neuroprotective agent for prevention and treatment of Alzheimer’s disease”.
Along the same lines, administration of the kidney-specific peptide (EDL) (not to be confused with the EDR above), in laboratory rats had protective effects on kidney function, and it improved protein excretion and energy supply to the kidneys5.
These new and positive experiments, give an overall optimistic picture with regards to the use of bio-active peptides which work on specific organs and in specific ways. Of course, experiments in laboratory animals do not always translate into effective clinical therapies for humans, but nevertheless, the research shows that the mechanism is there, it is effective, and this encourages further research.
I quote from my overall Conclusion in the book: “…Based on existing scientific evidence (which may or may not be strong), it appears that the use of these
regulatory bio-peptides may be worthwhile in some cases. The specific preparation may help in some respects, the side effects are negligible, and it may be better to try the preparation rather than not try it. In other words, if there is no valid reason not to use it, then use it, unless your physician specifically has a different opinion. The issue with any newly available treatment is that it may give hope for treatment, or it may need time for the researchers to optimise the preparation, dose, and formulation. So, ultimately, it is a matter of personal choice, reflecting the character of the user. An open minded, well informed user will act differently from a pessimist, poorly informed one.”
Therefore, my recommendation is to read the book, get the information you need, and discuss a positive course of action with your physician, with a therapy that is tailored specifically to your own needs.
NEW RESEARCH
Let me now mention some additional research, the latest scientific findings that come to support the overall thrust of the book.
A single course of treatment using a peptide that regulates the microcirculation in the brain, resulted in an improved density of the blood vessels in the pia mater (the innermost sheet of the membranes surrounding the brain). Further courses of treatment improved the blood flow to the brain by about 15%, compared to animals which were not treated. In addition, the treated animals were resistant to a subsequent interruption of oxygen to the brain 1. Although this experiment was performed on laboratory animals, it just indicates in general terms the clinical effectiveness of the bio-peptide used.
A synthetic peptide, which mirrored the structure of the natural peptide complex present in the epiphysis, was found to have similar biological effects as those of the natural one. For example, it normalised melatonin synthesis, and overall improved the retina, the vascular and immune systems. This shows that even synthetic peptides, when constructed in accordance with other naturally occurring ones, may have similar biological effects. Therefore, it may not be necessary to rely too much on extracting natural peptides from different live tissues, but we can use synthetic ones which are cheaper and easier to create2.
One new piece of research gives an interesting glimpse into the action of bio-active peptides. Researchers
References1. Sokolova IB, Ryzhak GA, Khavinson VK. Functional cumulation of influence of vascular pep-
tide bioregulator on microcirculation in the brain cortex of spontaneously hypertensive rats. Adv Gerontol. 2017;30(5):671-675
2. Khavinson VK, Kopylov AT, Vaskovsky BV, Ryzhak GA, Lin’kova NS. Identification of Peptide AEDG in the Polypeptide Complex of the Pineal Gland. Bull Exp Biol Med. 2017 Nov;164(1):41-43
3. Khavinson VK, Kormilets DY, Mar’yanovich AT. Peptides (Epigenetic Regulators) in the Struc-ture of Rodents with a Long and Short Lifespan. Bull Exp Biol Med. 2017 Sep;163(5):671-676
4. Kraskovskaya NA et al. Tripeptides Restore the Number of Neuronal Spines under Condi-tions of In Vitro Modeled Alzheimer’s Disease. Bull Exp Biol Med. 2017 Aug;163(4):550-553
5. Zamorskii I et al. Nephroprotective Effect of EDL Peptide at Acute Injury of Kidneys of Differ-ent Genesis. Bull Exp Biol Med. 2017 Jul;163(3):389-393
Mouse neuron
THE PEPTIDEBIOREGULATOR REVOLUTION
THE PEPTIDE BIOREGULATOR REVOLUTIONTHE PEPTIDE BIOREGULATOR REVOLUTION
12 AGINGMATTERS AGINGMATTERS 13

VITAMIN B17: AN ALTERNATIVE CANCER TREATMENTBy Leslie J. Farer
If you’re a baby boomer or older, you may remember hearing about Laetrile, the highly publicized cancer drug that provoked an unprecedented medical and political controversy that peaked in the 1970’s. Proponents considered Laetrile, a synthetic form of the naturally occurring plant compound amygdalin (derived from apricot kernels), a safe and “natural” alternative to conventional toxic chemotherapy, but the medical establishment called it a “fraud,” dismissing it as an ineffective and toxic drug that should be prohibited from use. A series of mostly negative animal studies from the 1970’s and a clinical trial in the early 1980’s that came up empty put the lid − perhaps too soon − on further human testing of this substance which never gained FDA approval. But interest in amygdalin has been revived in recent years, with new studies on cell cultures revealing previously unknown mechanisms of action against a variety of cancers.
Up until now, those wishing to take advantage of amygdalin’s purported benefits could only do so by consuming apricot kernels or similar pills of unknown purity and potency. But now, IAS offers a superior alternative: B17-Pro™ which is purified amygdalin in 100 mg tablets. In this article, we’ll cover the chemistry and properties of amygdalin, its eventful history, the contentious relationship between the medical establishment and amygdalin (Laetrile) proponents, the pros and cons of its use, new discoveries and potential applications, and its use today.
CANCER CELLS
VITAMIN B17: AN ALTERNATIVE CANCER TREATMENT
14 AGINGMATTERS AGINGMATTERS 15

AN AMYGDALIN (LAETRILE) PRIMER
Amygdalin, derived from the Greek word meaning “almond,” is a naturally occurring substance found in the pits, seeds, and kernels of hundreds of fruits and plants such as apricots (the richest source), bitter almonds, apples, peaches, plums and berries. Amygdalin belongs to a class of compounds known as cyanogenic glycosides, (containing one or more simple sugar molecules and a nitrile (−C N) group that can potentially be metabolized in the body to hydrogen cyanide (HC N)).
Natural amygdalin is an optically active isomer with the chemical name D-mandelonitrile-beta-D-gentiobioside, also referred to as D-amygdalin, (see figure 1). US-patented Laetrile (a synthetic derivative of amygdalin known as L-mandelonitrile-beta-D-glucuronide), is structurally and pharmacologically like amygdalin (see figure 2) and technically also a cyanogenic glycoside. Both compounds are also called nitrilosides.
Amygdalin and its synthetic derivative have been promoted as alternative cancer treatments since the early 1950s.
It’s impossible to discuss one without the other, since they are related substances whose names are used interchangeably in the medical literature and elsewhere,
but technically they are not identical. But at some point, after it gained patent in the US in 1961, the term “Laetrile” became synonymous with “amygdalin.” This merging of terms, as one author put it; “confuses an already complicated story.”1 A research paper from the 1970’s went on to say that; “amygdalin at various concentrations and with numerous impurities is the most common cyanogenic glycoside found in Laetrile
samples.”2 Considering that US-patented Laetrile was probably never manufactured on a large scale, and that Mexican-produced Laetrile is D-mandelonitrile-beta-D-gentiobioside, i.e. amygdalin, made from crushed apricot pits,3 it seems safe to assume that the chemical identity of the substance used by “Laetrile” practitioners and studied in animal and human trials was and currently is amygdalin. To add to the nomenclature confusion, “Vitamin B17” has also been applied to both Laetrile and amygdalin (we’ll see more on B17 later).
[Note: In this article, as much as possible, especially when discussing the scientific studies, we’ll refer to the substance D-mandelonitrile-beta-D-gentiobioside as “amygdalin.” When discussing its historical significance, as in the next section, and its use by medical practioners, we’ll use the term “Laetrile,” since this was the designation commonly applied to this therapy starting in the 1960’s.]
The main proposed anti-cancer mechanism is localized delivery of cyanide to cancer cells, destroying them. When amygdalin interacts with the enzyme beta-glucosidase and water, it degrades to produce hydrogen cyanide, benzaldehyde, and glucose.2,4,5 Cyanide release was originally thought to be the main cancer-fighting mechanism,4,6 but benzaldehyde and prunasin (another breakdown product of amygdalin) may also inhibit cancer cells.4,6,7 In fact, benzaldehyde has been shown to be effective as a primary cancer therapy in humans.7
The usual course of Laetrile treatment involves intravenous (IV) administration by a physician for a period (several weeks or months, according to response) followed by oral maintenance therapy (tablets), usually as part of a comprehensive “metabolic” program consisting of a specialized plant-based diet, high-dose vitamins and pancreatic enzymes.
The main risk of Laetrile therapy (and a major aspect of its controversial use) is cyanide toxicity, especially when administered orally. Intestinal bacteria and some
commonly consumed plants contain enzymes, (beta-glucosidases) that initiate the breakdown of amygdalin and cleave the nitrile group, releasing cyanide into the bloodstream. 4 Oral amygdalin is estimated to be 40 times more potent than the IV form due to its enzymatic conversion to cyanide in the GI tract.8 In contrast, IV administration bypasses the GI tract, limiting rates of conversion to cyanide.9
Proponents consider amygdalin (Laetrile) an effective and natural alternative to conventional side-effect-ridden chemotherapy, with decades of safe use if administered by an experienced practitioner, while the conventional medical establishment has, over the past five decades, predominantly labeled it a “fraud,” a “cancer quackery,” ineffective, and potentially toxic.
Laetrile has been banned in the US and the EU for decades, but amygdalin-rich apricot kernels and apricot-based pills are available. However, amygdalin tablets (B17-Pro™), consisting of the isolated active ingredient, must be purchased online. Amygdalin and Laetrile are still permitted to be manufactured and administered in clinics in certain countries, such as Mexico.
Figure 1: Amygdalin (D-mandelonitrile-beta-D-gentiobioside) Figure 2: US-Patented Laetrile (L-mandelonitrile-beta-D-glucuronide)
OO
OO
OH
OH
OH
HOHO
HOHO
CN
HOOCHO
HOOH
OO
ON
Figure 1 Figure 2
VITAMIN B17: AN ALTERNATIVE CANCER TREATMENT
VITAMIN B17: AN ALTERNATIVE CANCER TREATMENTVITAMIN B17: AN ALTERNATIVE CANCER TREATMENT
16 AGINGMATTERS AGINGMATTERS 17
HISTORY, CONTROVERSY, AND POLITICS
Amygdalin, in the form of bitter almonds, has been used for centuries. It was first isolated in France in 1830, and was later used to treat cancer in Russia in 1845 and in the US in the 1920’s. In the 1950’s, an IV form was synthesized and patented as Laetrile in 1961. In the years following, the public’s quest for a “natural” alternative to harsh chemotherapies caused Laetrile’s popularity to soar − it’s estimated that by 1978, more than 70,000 Americans had undergone treatment with it.9,10
But the 1970’s was a decade characterized by an unprecedented medical, political, and even ethical controversy as Laetrile’s availability to the public became threatened when an Investigational New Drug (IND) application was rejected by the FDA based on lack of efficacy in animal studies. (In the US, an IND application must be filed with the FDA prior to clinical studies in humans as part of the drug approval process.) Even though the FDA is charged with ensuring that any drug on the market is both safe and effective, the agency’s thumbs down on Laetrile was seen by many as a
violation of one’s “freedom of choice” in determining his or her choice of cancer treatment. Laetrile supporters believed that the FDA, the pharmaceutical industry, and the medical establishment (including the American Medical Association and the American Cancer Society) were intentionally conspiring to restrict access to a potentially life-saving drug. One of the top centers of cancer research in the US, the Memorial Sloan-Kettering Cancer Center in New York, was even suspected of covering up positive results in animal studies (we’ll see more on this later).
Legal proceedings in Oklahoma, Massachusetts, New Jersey, and California challenged the FDA’s authority, which led to the legalization of Laetrile in 27 states in the 1970’s. But in 1980, the US Supreme Court upheld a Federal ban on interstate shipment of Laetrile, which effectively put an end to its use in the US. Laetrile never gained approval by either the FDA or the European Commission. However, as mentioned, it is still manufactured and administered in clinics, predominantly in Mexico, but also elsewhere around the globe.
RATIONALE FOR AMYGDALIN (LAETRILE) USE
Supporters of amygdalin (Laetrile) base their claim on its anti-cancer properties largely on epidemiological data, citing indigenous peoples such as the Hunzakut tribe of the Karakoram Mountains of northern Pakistan who routinely consume nitrilosides and typically live to 100 years old with very low rates of cancer. (The assumption here is that nitriloside intake, including amygdalin, is directly responsible for longevity and low-cancer incidence, but other factors such as a healthy diet, ample exercise, and a rich social network also contribute to these peoples’ health.) And as far as epidemiological observations, though they are informative, they are not proof of efficacy.
One of the main early promoters of amygdalin (Laetrile), biochemist E.T. Krebs Jr., labeled it “vitamin B17,” and believed it to be a natural cancer-fighting food component, that if regularly consumed, as in the Hunzakut diet, would prevent various types of cancer. According to Krebs, cancer is a vitamin B17 deficiency disease. However, “vitamin B17” does not meet the definition of “vitamin,” is not required for normal metabolism, and is not an approved designation.
Besides epidemiological data, Laetrile proponents also point to case reports from doctors who have apparently administered it safely, effectively, and without toxicity for decades. But case reports are difficult to interpret due to lack of uniform documentation, use of conventional chemotherapies in combination with Laetrile, and variations in the dose and duration of treatment.3
As mentioned, cyanide is thought to be the main anti-cancer agent formed from amygdalin metabolism, and the rationale among Laetrile practitioners is to maintain cyanide blood levels high enough, but still below the toxic threshold to ward off cancer and boost the
immune system. According to one doctor with a long history of using Laetrile in his practice, Dr. Philip E. Binzel, Jr., “Laetrile is nothing more than a concentrated form of nitrilosides. When ingested, nitriloside has merited recognition by maintaining non-toxic cyanide levels and acting as a potential threat to the immune surveillance, thereby lessening the frequency of cancerous tumors.”11
Various mechanisms have been proposed to explain amygdalin’s purported anti-cancer activity. One is that it is preferentially toxic to malignant cells, since they exhibit higher activity of beta-glucosidase than normal cells and lower levels of another enzyme, rhodanese (thiosulfate sulfurtransferase).2,3 Beta-glucosidase initiates the breakdown of amygdalin, producing cyanide, and rhodanese converts cyanide to the non-toxic substance thiocyanate.3 A higher ratio of beta-glucosidase to rhodanese in cancer cells favors increased cyanide production with lower rates of conversion to thiocyanate, making the drug much more lethal to cancer cells than normal cells. Another proposed mechanism involves another altered enzyme ratio, this time between beta-glucuronidase (not to be confused with beta-glucosidase) and rhodanese, which also leads to higher localized cyanide concentrations in cancerous cells.3 Some studies do demonstrate the difference in concentrations of the enzymes rhodanese,12 beta-glucosidase,13 and beta-glucuronidase14 in normal versus malignant tissues. However, other studies have found that cyanide is also released in normal cells,15 and highly elevated oral doses have led to cases of deaths and toxicity.2
One cancer-inhibiting mechanism less often proposed by Laetrile proponents − but positively demonstrated in studies − is the amygdalin breakdown product benzaldehyde, which has shown efficacy in humans against tumors.7
T-cells attacking cancer cell
VITAMIN B17: AN ALTERNATIVE CANCER TREATMENT VITAMIN B17: AN ALTERNATIVE CANCER TREATMENT
18 AGINGMATTERS AGINGMATTERS 19

DOES IT WORK? WHAT THE STUDIES SHOW
As mentioned, the conventional medical establishment has flatly rejected amygdalin (Laetrile) as a potential chemotherapeutic agent and most studies from the 1970’s and early 1980’s found it ineffective against a variety of cancers, in animals and humans, and potentially dangerous due to cyanide toxicity. Upon reviewing the medical literature, it’s common to find conclusions such as this one, from a panel of independent reviewers: “Laetrile has shown little anti-cancer activity in animal studies and no anti-cancer
activity in human clinical trials.”3 And this one, from a Cochrane review: “The risk-benefit balance of laetrile or amygdalin as a treatment for cancer is therefore unambiguously negative.” 8
But it should be mentioned that the studies − animal and human − are laced with inconsistencies and ambiguities, and often present conflicting data, of which we’ll see numerous examples below.
HUMAN STUDIES
Amygdalin (Laetrile) is an unusual case; it never gained IND approval from the FDA (based on negative findings in animal studies), a preliminary step to proceed with clinical trials, yet the NCI agreed to sponsor (and the FDA approved) phase I and II clinical trials nonetheless, bypassing this regulation and most likely responding to public pressure. Prior to the clinical trials, the NCI
attempted to compare the efficacy of Laetrile versus conventional chemotherapy by reviewing case reports of patients treated with each method. The problem was, the review panel couldn’t obtain sufficient data on Laetrile − after sending out close to half a million requests to doctors for information on their patients who had benefitted from the drug, the NCI received
ANIMAL STUDIES
Animal studies from the 1970’s evaluating the potential cancer-inhibiting activity of amygdalin reported predominantly negative findings, including two from 1975 sponsored by the National Cancer Institute (NCI). In these studies, various cancers were transplanted into mice and rats (osteogenic sarcoma, melanoma, carcinosarcoma, lung carcinoma, and leukemia). The rodents were then administered either amygdalin alone or in combination with beta-glucosidase (presumably to enhance the degradation of amygdalin to cyanide). Neither study found any significant cancer-inhibiting activity in any of the tumor types or leukemias studied with either the single or combination treatment, and both showed that co-administration with beta-glucosidase led to increased toxicity,16,17 an expected result due to the higher rate of conversion to cyanide. Although other animal studies from the 1970’s using transplanted tumors corroborated these negative findings,18,19 one study did report success in treating
breast cancer in mice with combination therapy (amygdalin, vitamin A and enzymes).20
Other positive results were the originally hushed-up and later publicized set of unpublished animal experiments performed at Memorial Sloan-Kettering Cancer Center in the 1970’s in which amygdalin was shown to reduce the spread of cancer. These studies were performed by respected researcher Dr. Kanematsu Sugiura on mice bred to spontaneously develop tumors (not transplanted tumors as in the NCI studies). Sugiura found that amygdalin was 80% effective in preventing the spread of lung cancer in treated mice compared to a control group. 21 Apparently, Sloan-Kettering covered-up these results (for various reasons, perhaps political or economic) until they were leaked to the press by a principled and forthright employee − the subject of a documentary film; “Second Opinion: Laetrile at Sloan Kettering.”21
a meager 93 responses, and many case reports had to be thrown out due to insufficient documentation. In the end, the panel of 12 oncologists, blinded to the actual treatments, evaluated 160 cases (68 Laetrile, 68 chemotherapy, 24 controls). Of the 68 Laetrile cases, the panel found only two complete and four partial responses to the drug, precluding any definite determination as to its efficacy.10 Yet, the NCI agreed to sponsor clinical trials.
The 1981 phase I trial was a very small study on only six patients that evaluated the safety of oral and IV administration in doses like those commonly used by Laetrile practitioners. Neither the IV nor the oral dose (500 mg tablet, three times daily) produced any toxic reaction, though the tablets did raise blood cyanide levels and led to symptoms of toxicity in one patient who also consumed a large helping of raw almonds. The researchers concluded that; “amygdalin in the doses employed produces few clinical side effects,” i.e., minimal toxicity.22
Since amygdalin was shown to be reasonably safe in the phase I trial, a larger phase II efficacy trial was conducted
at the Mayo Clinic in 1982. 178 patients with various types of cancer received amygdalin intravenously for 21 days, followed by oral tablets (500 mg, three times daily), using doses and schedules “representative of current Laetrile practice.” The IV vials used in the study contained DL-amygdalin, a racemic mixture, which is a combination of both natural D-amygdalin (the biologically active isomer) and L-amygdalin (an artificial, inactive form) “so that the preparations would correspond with the products distributed by the major supplier.” The oral tablets contained only D-amygdalin. In keeping with the comprehensive metabolic therapy program used by Laetrile practitioners, patients also received vitamins and pancreatic enzymes, and followed a specialized diet. Of 178 patients, only one responded to treatment. And even though amygdalin produced minimal side effects in the previous safety study, several patients in this trial experienced symptoms of cyanide toxicity (granted, this was a much larger study). The researchers concluded that “amygdalin (Laetrile) is a toxic drug that is not effective as a cancer treatment and does not warrant further study”23. It conformed to the overriding view of the medical establishment at the time and ended the prospect of any further human testing some 35 years ago.
PROBLEMS WITH THE PHASE II STUDY
This last study has been criticized by Laetrile supporters and there are several points of contention, one of which is the type of amygdalin used for IV administration. As mentioned, D-amygdalin is the biologically active isomer, and this was the substance used in the oral tablets. But the IV vials contained a racemic mixture, a combination of the D and L isomers (one active, one inactive), which would have significantly lowered the potency (by approximately 50 percent). The authors, as stated above, attempted to simulate the product characteristic of the Mexican supplier at the time, but it’s impossible to know decades later if this was an accurate simulation. It makes sense that the active isomer, D-amygdalin, was used in the oral tablets, but why was the racemic mixture used in the IV vials?
Another criticism is the “one size fits all” schedule of IV and oral doses used in the study. All patients were
automatically switched from IV therapy to oral tablets after three weeks, regardless of response. Although the study authors stated that “the dosage and schedule were representative of past and present Laetrile practice,” 23
many practitioners generally advocate an individualized protocol, with the IV portion performed until a positive response is seen, often from four to 10 months, or even longer. 24 Patients are then put on oral maintenance (tablets) only when their cancer is in check and put back on IV if the cancer re-appears or grows. Some practioners even administer oral tablets while tapering off IV.
Perhaps the correct conclusion to be drawn from this study isn’t that “amygdalin (Laetrile) is ineffective as a cancer treatment,”23 but rather, that administering a drug of questionable potency on a truncated schedule to advanced cancer patients doesn’t work.
VITAMIN B17: AN ALTERNATIVE CANCER TREATMENTVITAMIN B17: AN ALTERNATIVE CANCER TREATMENT
20 AGINGMATTERS AGINGMATTERS 21
RECENT STUDIES
Although the conclusion of this last 1982 study precluded any further human trials, leaving the question of amygdalin’s efficacy in humans unanswered, the passage of a few decades − and some distance from the various political and scientific disputes − has led to renewed interest in recent years, and studies using cell cultures have resulted in promising findings.
Amygdalin has been shown to induce apoptosis (programmed cell death), 15,25 among other important mechanisms, and inhibit various types of cancer in breast, lung, bladder, colon, prostate, liver, kidney, and cervical cell lines. 15, 25-32 All of these studies draw a
favorable assessment of amygdalin’s cancer-inhibiting potential. For example, a 2018 study concludes: “This compound might be applicable in the treatment of various cancer cell types,” 15 quite the opposite determination from the majority of studies from the 1970’s and early 1980’s. So, the door has not been closed on amygdalin after all, as new research is uncovering potential applications and previously unknown mechanisms of action.
AMYGDALIN’S USE TODAY AND HOW TO USE B17-PRO™
As mentioned earlier, amygdalin (Laetrile) can be legally administered in clinics only in certain countries. Dr. Antonio Jimenez, chief medical officer and founder of Hope4Cancer Institute in Mexico is one of the doctors who uses it in his practice. Besides its role as a chemotherapeutic agent, Dr. Jimenez has observed that amygdalin provides pain relief and well-being enhancement in his patients. He doesn’t use it as a single therapy or “magic bullet,” though, but as part of a comprehensive treatment program to slow the progression of cancer (Dr. Jimenez has a realistic expectation, acknowledging amygdalin’s potential to inhibit cancer, but also realizing that it alone is not a cure, but an integral part of a multi-pronged approach to treatment.)
Outside of Mexico, those in the US and most European countries don’t have access to clinics such as the Hope4Cancer Institute, but instead resort to consuming apricot kernels or apricot-based pills (with unknown amounts of amygdalin of unknown purity). A superior alternative is B17-Pro™, containing 100 mg amygdalin per tablet, plus pancreatic enzymes and zinc. The recommended dose is one tablet per day with water
before a meal, or as directed. Consult your health care professional before using. Remember not to take amygdalin tablets shortly before eating raw almonds or crushed fruit pits, or with fruits or vegetables that contain beta-glucosidase or beta-glucuronidase (i.e., celery, peaches, bean sprouts, carrots, etc.).
Dr. Jimenez apparently has never seen a toxic reaction with the IV and oral doses he uses in his clinic, and that observation is shared by other Laetrile practitioners. But, as we saw earlier in the studies, cyanide toxicity is a concern. Symptoms include liver damage, difficulty walking, fever, coma, lethargy, convulsions, nausea, vomiting, and dizziness. Seek medical attention immediately if you develop any side effects. But B17-Pro™ is a low-dose product, and it is highly unlikely those symptoms will develop if taken as directed (one tablet per day, or as recommended by your physician, avoiding the foods listed above).
We have just covered a lot of territory about amygdalin, from its history steeped in controversy and politics, to its various mechanisms of action, to an overview of the
References1. Petersen JC, Markle GE. Politics and science in the Laetrile controversy. Soc Stud Sci. 1979
May;9(2):139-66.
2. Dorr RT, Paxinos J. The current status of laetrile. Ann Intern Med. 1978 Sep;89(3):389-97.
3. PDQ Integrative, Alternative, and Complementary Therapies Editorial Board. Laetrile/Amygdalin (PDQ®): Health Professional Version. 2017 Mar 15. In: PDQ Cancer Information Summaries. National Cancer Institute (US); 2002-.
4. Newmark J, Brady RO, Grimley PM, Gal AE, Waller SG, Thistlethwaite JR. Amygdalin (Laetrile) and prunasin beta-glucosidases: distribution in germ-free rat and in human tumor tissue. Proc Natl Acad Sci U S A. 1981 Oct;78(10):6513-6.
5. Ames MM, Moyer TP, Kovach JS, Moertel CG, Rubin J. Pharmacology of amygdalin (laetrile) in cancer patients. Cancer Chemother Pharmacol. 1981;6(1):51-7.
6. Rauws AG, Olling M, Timmerman A. The pharmacokinetics of prunasin, a metabolite of amygdalin. J Toxicol Clin Toxicol. 1982 Oct;19(8):851-6.
7. Kochi M, Takeuchi S, Mizutani T, Mochizuki K, Matsumoto Y, Saito Y. Antitumor activity of benzaldehyde. Cancer Treat Rep. 1980 Jan;64(1):21-3.
8. Milazzo S, Horneber M. Laetrile treatment for cancer. Cochrane Database Syst Rev. 2015 Apr 28;(4):CD005476.
9. Lerner IJ. Laetrile: a lesson in cancer quackery. CA Cancer J Clin. 1981 Mar-Apr;31(2):91-5.
10. Ellison NM, Byar DP, Newell GR. Special report on Laetrile: the NCI Laetrile Review. Results of the National Cancer Institute’s retrospective Laetrile analysis. N Engl J Med. 1978 Sep 7;299(10):549-52.
11. https://www.cancertutor.com/laetrile
12. Sabelli R, Iorio E, De Martino A, et al. Rhodanese-thioredoxin system and allyl sulfur com-pounds. FEBS J. 2008 Aug;275(15):3884-99.
13. Bernacki RJ, Niedbala MJ, Korytnyk W. Glycosidases in cancer and invasion. Cancer Metasta-sis Rev. 1985;4(1):81-101.
14. Chen X, Wu B, Wang PG. Glucuronides in anti-cancer therapy. Curr Med Chem Anticancer Agents. 2003 Mar;3(2):139-50.
15. Liczbiński P, Bukowska B. Molecular mechanism of amygdalin action in vitro: review of the latest research. Immunopharmacol Immunotoxicol. 2018 Feb 28:1-7.
16. Wodinsky I, Swiniarski JK. Antitumor activity of amygdalin MF (NSC-15780) as a single agent and with beta-glucosidase (NSC-128056) on a spectrum of transplantable rodent tumors. Cancer Chemother Rep. 1975 Sep-Oct;59(5):939-50.
17. Laster WR Jr, Schabel FM Jr. Experimental studies of the antitumor activity of amygdalin MF (NSC-15780) alone and in combination with beta-glucosidase (NSC-128056). Cancer Chemother Rep. 1975 Sep-Oct;59(5):951-65.
18. Ovejera AA, Houchens DP, Barker AD, Venditti JM. Inactivity of DL-amygdalin against human breast and colon tumor xenografts in athymic (nude) mice. Cancer Treat Rep. 1978
Apr;62(4):576-8.
19. Stock CC, Tarnowski GS, Schmid FA, Hutchison DJ, Teller MN. Antitumor tests of amygdalin in transplantable animal tumor systems. J Surg Oncol. 1978;10(2):81-8.
20. Manner HW, DiSanti SJ, Maggio MI, et al. Amygdalin, vitamin A and enzyme induced regres-sion of murine mammary adenocarcinomas. J Manipulative Physiol Ther. 1978;1(4):246-8.
21. https://www.secondopinionfilm.com
22. Moertel CG, Ames MM, Kovach JS, Moyer TP, Rubin JR, Tinker JH. A pharmacologic and toxicological study of amygdalin. JAMA. 1981 Feb 13;245(6):591-4.
23. Moertel CG, Fleming TR, Rubin J, et al. A clinical trial of amygdalin (Laetrile) in the treatment of human cancer. N Engl J Med. 1982 Jan 28;306(4):201-6.
24. Krashen S. Does Laetrile Work? Another Look at the Mayo Clinic Study (Moertel et al., 1982). Internet Journal Alt Med. 2008;7(1).
25. Chang HK, Shin MS, Yang HY, et al. Amygdalin induces apoptosis through regulation of Bax and Bcl-2 expressions in human DU145 and LNCaP prostate cancer cells. Biol Pharm Bull. 2006 Aug;29(8):1597-602.
26. Park HJ, Yoon SH, Han LS, et al. Amygdalin inhibits genes related to cell cycle in SNU-C4 human colon cancer cells. World J Gastroenterol. 2005 Sep 7;11(33):5156-61.
27. Zhou C, Qian L, Ma H, et al. Enhancement of amygdalin activated with β-D-glucosidase on HepG2 cells proliferation and apoptosis. Carbohydr Polym. 2012 Sep 1;90(1):516-23.
28. Chen Y, Ma J, Wang F, et al. Amygdalin induces apoptosis in human cervical cancer cell line HeLa cells. Immunopharmacol Immunotoxicol. 2013 Feb;35(1):43-51.
29. Makarević J, Tsaur I, Juengel E, et al. Amygdalin delays cell cycle progression and blocks growth of prostate cancer cells in vitro. Life Sci. 2016 Feb 15;147:137-42.
30. Juengel E, Afschar M, Makarević J, et al. Amygdalin blocks the in vitro adhesion and invasion of renal cell carcinoma cells by an integrin-dependent mechanism. Int J Mol Med. 2016 Mar;37(3):843-50.
31. Juengel E, Thomas A, Rutz J, et al. Amygdalin inhibits the growth of renal cell carcinoma cells in vitro. Int J Mol Med. 2016 Feb;37(2):526-32.
32. Makarević J, Rutz J, Juengel E, et al. Amygdalin influences bladder cancer cell adhesion and invasion in vitro. PLoS One. 2014 Oct 15;9(10):e110244.
33. The trophoblastic nature of cancer and the allied diseases. Navarro MD, Navarro RP. J Philipp Med Assoc. 1966 Jan;42(1):39-56.
34. The mechanism of action and therapeutic effects of laetrile in cancer. NAVARRO MD. J Philipp Med Assoc. 1957 Aug;33(8):620-7.
35. Five years experience with laetrile therapy in advanced cancer. NAVARRO MD. Acta Unio Int Contra Cancrum. 1959;15(Suppl 1):209-21.
36. I’ve got a couple of other good books on laetrile at home (I’m at the office, now)—but can let you know what they are if needed.
Healthy Cells
animal and human studies performed in the 1970’s and early 1980’s that culminated with the one (and only) human efficacy trial, the conclusion of which ended the possibility of further clinical testing. But despite that grim assessment, interest in amygdalin has been reawakened
over the past dozen years and a slew of positive studies using cell cultures has demonstrated its potential to inhibit a range of cancer types. Perhaps ongoing research will finally and definitively establish amygdalin’s role in cancer prevention and treatment.
VITAMIN B17: AN ALTERNATIVE CANCER TREATMENTVITAMIN B17: AN ALTERNATIVE CANCER TREATMENT
22 AGINGMATTERS AGINGMATTERS 23
By Will Block
Memory is, therefore, neither Perception nor Conception, but a state or affection of one of these, conditioned by lapse of time. — Aristotle, On Memory and Reminiscence
THE BIRTH OF CONSCIOUSNESS
Odysseus, the King of Ithaca and the hero of these tales, is a hero of memory. The Greek word for mind or intellect or consciousness, nóos, is essential to his character, and its opposite, antinóos — defined as forgetfulness, stupidity, or arrogance — is the enemy of Odysseus. Forgetting, in the epic tales, is seen by Odysseus as an affront to memory and is
punishable by severe reprisal, in which, as often as not, the perpetrator is killed. In his ten years of wandering throughout the known world, there are many adventures, but in the history of pharmacopoeia, one stands out: his encounter with the beautiful sorceress Circe on Aeaea, on her island home near Italy.
Homer’s great epic of the ancient Mediterranean world, the Odyssey, was an oral history, argues mythologist Robert Graves.1 In his notable opinion, the ancient Greek myths are not merely esthetic and poetic creations, but records of events that took place and were forgotten by most — and would have been forgotten by all, had not Homer and others like him valued their preservation, telling and retelling the stories. In this way, the Odyssey is a tool for learning about mankind’s past triumphs and errors. It is also a tribute to the value and sanctity of memory.
FIGHTING ALZHEIMER’S DISEASE WITH GALANTAMINE
FIGHTING ALZHEIMER’S DISEASE WITH GALANTAMINE
SYNAPSE DECONSTRUCTING
24 AGINGMATTERS AGINGMATTERS 25

MEMORY DILEMMA
When Odysseus and his crew arrive on Aeaea, they are tired of the hardships of travel and fearful for their safety. Deciding to reduce their risk, Odysseus remains with his ship while half of his crew ventures inland, where they meet Circe, who offers her “hospitality.” According to Homer, she serves up a banquet of food into which she mixes malignant drugs so that they might forget their fatherland and their desire to return to it. Then, with a wave of her hand, she turns them into swine.
Hearing of their plight, Odysseus sets out to free them. Along the way, in a forest glen, he is counseled by the god Hermes, in the form of a young man, who cautions him about dealing with Circe and gives him an antidote to protect him from the drugs that have taken down his crew. Hermes shows Odysseus the nature of the medicine, which has “a black root, but milk-like flower. The gods call it moly and it is difficult for men to dig up.”
GALANTAMINE’S BREAKTHROUGH: ALZHEIMER’S DISEASE REVERSAL?
The realization of Odysseus, Homer, and Dioscorides is ours too, when the value of two recent, randomized, double-blind, placebo-controlled studies becomes apparent. Their welcome finding is that galantamine may be superior to any other cholinergic supplement. Galantamine may not only slow the decline into the black night of Alzheimer’s disease, but, for the first time, reverse it.
GALANTAMINE: THE FIRST NOOTROPIC
According to a paper published in 1983, the drug given to the crew was likely to be an extract from the plant Datura stramonium (thorn apple, or jimsonweed). This makes sense, because not only were their memories taken from them, they were cast into a delusional-hallucinatory state during which they believed they had been turned into animals.2
D. stramonium, among other drugs known to the ancient Greeks, is an anticholinergic that contains atropine and is known to produce such effects. Based on the description of the antidote moly, together with the immunity it gave Odysseus — thereby allowing him to rescue his crew from Circe and recover their memories — the researchers assert that moly is none other than the acetylcholinesterase inhibitor galanthamine (or galantamine, as it is now more commonly called), derived from the snowdrop (Galanthus nivalis) and related species. Galantamine may be the first nootropic agent — a substance that enhances intelligent, purposive consciousness (nóos = consciousness, trope = a turning).
As further evidence, the researchers offer the site of
the picking: a forest glen, where the snowdrop grows more readily because of the moist, sheltered ground.
The Snowdrop is small, inconspicuous, and difficult to find, flowering only briefly in the early spring. Its flower is milky-white, as indicated by the name Galanthus (gala = milk, anthus = flower), its root is dark, and its bulb, when peeled, is onion-like.
It can be found growing wild on the Balkan peninsula, including the Greek mainland and its islands, where it was thought to have originated. Also, the Greek physician and herbalist Dioscorides, who wrote the authoritative De Materia Medica, described the moly plant, (without ever acknowledging its epic use) in ways that substantiate its identity as Galanthus, from which galantamine is derived.
Snowdrop (Galanthus nivalis)
KEEPING MEMORY INTACT
While other evidence points to the antidotal use of other acetylcholinesterase inhibitors (AChEIs) — e.g., physostigmine (from Physostigma venonosum) for atropine toxicity — long before the underlying mechanisms were understood, the Homerian description reflects perhaps the earliest empirical knowledge of an AChEI in distant antiquity, about 3000 years ago.
As recent studies have shown, galantamine is one of the few long-lasting anticholinergic antidotes known, one that could easily have given Odysseus enough time to overpower Circe. In so doing, Odysseus liberates himself, his men, and their memories, giving them the courage and desire to go on. Thus, within this story and throughout the entire epic tale, the knowledge of the past is maintained and transmitted. Civilization is enriched by good history, artfully told, and we as its beneficiaries are less likely to repeat the errors of the past. So, it is when our memories remain intact.
THE DAWN OF CHOLINERGIC ENHANCEMENT
Before the so-called consciousness revolution kicked into high gear in the 1960s, a little-known discovery occurred in the unlikely country of Bulgaria. In the 1950s, a Bulgarian pharmacologist noticed that local villagers made use of the wild-growing common snowdrop plant by rubbing it on their foreheads to ease nerve pain. Further investigation led to the isolation of an alkaloid extract of the snowdrop, galantamine, that helped inhibit acetylcholinesterase, an enzyme that breaks down acetylcholine (ACh).
An important nerve messenger, ACh is a biochemical that plays a role in muscle contraction and the maintenance of proper muscle tone; this was known throughout the world. Scientific literature indicates extensive use of snowdrop in Eastern Europe, such as Romania3 and
the Ukraine,4 as well as the Balkan peninsula and other Mediterranean countries, where it was used topically and internally.5
At first, based on the surviving folkloric usage, galantamine was used in anesthesiology to increase muscle relaxation.6,7 Thereafter, it was rapidly introduced in other areas of medicine, such as neurology, ophthalmology, gastroenterology, intensive care and resuscitation, cardiology, and physiotherapy. For example, galantamine has been used successfully for the treatment of neuritis and neuralgia.8 Also intriguing is the ability of galantamine to increase color differentiation in monkeys,9 and it has been found to alleviate GI disturbances in rats.10
FIGHTING ALZHEIMER’S DISEASE WITH GALANTAMINE
FIGHTING ALZHEIMER’S DISEASE WITH GALANTAMINE FIGHTING ALZHEIMER’S DISEASE WITH GALANTAMINE
26 AGINGMATTERS AGINGMATTERS 27

CHOLINERGIC PLANTS FOR HEALING
In nature, plants have evolved cholinergic compounds for self-defense, among other self-serving mechanisms. Humans in the ancient world soon learned to use these plants therapeutically for their maladies as well as for the age-related decline in acetylcholine activity.11 While few, if any, of these plants were adequately understood, dosing knowledge was usually refined by folk herbal doctors and wielders of magic, (often the same individuals).
Some plants were used, as Datura was used by Circe, for ritualistic, prophetic, or anesthetic purposes, or to investigate or perpetrate dementia and even madness. Among these other herbal cholinergics were Atropa belladonna (deadly nightshade), Hyoscyamus niger (henbane), and Mandragora officinarum (mandrake). Long before the current biologically based hypothesis of cholinergic derangement in Alzheimer’s disease emerged, plants now known to contain cholinergic antagonists were recorded for their amnesia- and dementia-inducing properties.
Others have been used positively for healing, recuperation, and memory maintenance or memory recovery. These include Melissa officinalis (balm, containing choline)12 and Salvia officinalis (sage, containing choline)13 to enhance mental functions; Galanthus nivalis (snowdrop, containing galantamine) for muscle relaxation and memory restoration; and Panax ginseng (Chinese ginseng) and Panax quinquefolius (American ginseng) for age-related cognitive impairment.14 The active choline-like agents of the ginsengs have not yet been identified. Also, Ginkgo biloba contains active ingredients in the form of ginkgolides that have been found to possess antioxidant, neuroprotective, and cholinergic activities relevant to Alzheimer’s disease mechanisms.15
ALZHEIMER’S: PREVALENT AND GROWING
According to the World Health Organization,16 around 35 million people in industrialized countries suffered from Alzheimer’s disease in 2010. As people live longer, the probability of contracting this disease increases with advancing “memory age.” It may thus be thought of as an age-related memory impairment (ARMI). Currently, the percentage of Alzheimer disease sufferers among those aged 65 to 69 is 1.4%, but between 85 and 89, the incidence reaches 21.6%. As we progress in our ability to stave off other so-called “diseases of aging,” which high levels of well-chosen dietary supplements can help to accomplish, there is still Alzheimer’s looming, not to mention other ARMIs, such as dementia.
CHOLINERGIC SUPPLEMENTATION
As we have been aware for some time now, the use of cholinergic precursors such as choline and CDP-choline, cholinergic agonists such as DMAE, and cholinergic breakdown inhibitors such as huperzine may be able to put a brake on our decline into memory oblivion (see “Alzheimer’s Disease” in the Life Enhancement magazine, August 1999, p. 12), helping Alzheimer’s sufferers.
These common nutrients can help save us from mental perdition by helping to maintain proper cholinergic function. Not only are they derived from natural sources, they are virtually without side effects and with fewer problems than common food. As relatively new kids on the block, some acetylcholinesterase inhibitors (AChEIs) are synthetic drugs having no identical counterparts in the plant kingdom. Others are nutrients extracted from plants, and it is these that look more promising.
The structure of galantamine.
ALZHEIMER’S CHOLINERGIC DISEASE
Although in use for several thousand years —with about 30 years of scientifically documented human studies —galantamine has only recently been looked at for its ability to alleviate one of the cholinergic problems common to us all as we age, and especially for those with Alzheimer’s. That problem is the progressive decline of the neurotransmitter acetylcholine in our brains and bodies caused by the enzyme acetylcholinesterase.
Galantamine helps preserve cholinergic function by effectively increasing the abundance of acetylcholine, which is required for proper memory function.
Unlike other AChEIs, however, galantamine can also have a positive influence on cholinergic function through improvement of nicotinic acetylcholine receptors, the deterioration of which is largely unheralded as a mechanism of age-related memory decline.
EXTENSIVE TRIALS
Starting in 1985, galantamine underwent a series of clinical tests as a treatment for age-related impairment, dementia, and Alzheimer’s. But the quality of available Bulgarian snowdrops was dwindling, the extraction was time-consuming and expensive, and the yield was small. Also, wild snowdrop could not be patented. An Austrian group attempted to breed its own snowdrops, but the project was abandoned when a dramatic loss of the active substance was noted.
Because up to 10 grams per year of galantamine are needed per person, and the total annual crop of snowdrops was small, another source had to be found, and finally one was identified in the common daffodil (Narcissus pseudonarcissus L.). This source proved to be abundant and somewhat more economical.
OH
O
NCH3
CH O3
NEURON WITH AMYLOID PLAQUES
FIGHTING ALZHEIMER’S DISEASE WITH GALANTAMINEFIGHTING ALZHEIMER’S DISEASE WITH GALANTAMINE
28 AGINGMATTERS AGINGMATTERS 29
ALZHEIMER’S IMPROVEMENT
A paper appeared in 1996 testing the hypothesis that the central feature of chronic fatigue syndrome is a cholinergic defect. The researchers chose galantamine to see if it could inhibit the irritability that this defect caused, believing that this played a large role in the pathogenesis of the illness.19 Of 39 subjects taking galantamine at 16 mg/day over an 8-week period, 43% reported a 50% improvement in their pain, sleep, and fatigue levels. A huge 70% reported 30% improvement, while the placebo group reported only 10% improvement. The improvements did not occur overnight, but gradually over 4 to 8 weeks.
ALZHEIMER’S DISEASE
“Depending on where you set your sights, Alzheimer’s disease is a scientific puzzle, a medical whodunit, a psychological tragedy, a financial disaster, or an ethical, legal, and political dilemma. The disease quietly loots the brain, nerve cell by nerve cell, like a burglar returning to the same house each night.”
— Z. S. Khachaturian, Director of the Ronald and Nancy Reagan Research Institute of the Alzheimer’s Association.
GALANTAMINE TRIUMPHS
The two most dramatic clinical studies have just been published, and the results are better than expected. In the first study, 636 patients with mild to moderate Alzheimer’s disease were given galantamine or placebo over a 6-month period.17 Of the study group, 62% were female, and the mean age was 75.
The trial was double-blinded and was conducted simultaneously at several different locations where the subjects were randomly assigned to galantamine or placebo. Doses were low at the start and were increased to either 24 or 32 mg/day. After the 6-month period, some patients were extended another 6 months, this time with open-label dosing at 24 mg/day.
At the end of the study, galantamine was found to have significantly improved cognitive function relative to placebo. Not only were baseline levels of cognition maintained, (about the same for both 24 and 32 mg/day) whereas the scores of those taking placebo declined at month 6, but the therapeutic response was not affected by those who have the genotype for Alzheimer’s.
After 12 months, the baseline for patients receiving galantamine at 24 mg/day on the open-label extension held: there was no further cognitive decline. In fact, patients taking galantamine improved significantly over their baseline scores. The cognitive performance of patients taking a placebo declined by about the same amount. This means that those taking galantamine not only held their ground, they improved.
Initial data suggest that the first signs of cognitive improvement are experienced in patients as soon as one week after reaching their target dose. Unlike synthetic AChEIs such as Tacrine® (THA), the side effects, primarily gastrointestinal, were minor and diminished over the months of the study. There was no evidence of any liver toxicity. Galantamine was found to improve cognition and global function significantly.
In the second study, galantamine was again tested using a slow dose escalation, this time over a period of 8 weeks, in 978 patients with mild to moderate Alzheimer’s disease.18 Following a 4-week placebo run-in, the 8-week escalation proceeded in several locations, with random selection of those receiving galantamine or placebo in the double-blind trial. Those receiving galantamine were escalated to final maintenance doses of 8, 16, or 24 mg/day.
After 5 months, measurements were made with a variety of standardized assessment scales. At the end-point, those taking galantamine at 24 mg/day scored about 10% better than those at 16 mg/day. Compared to the placebo group, the differences were significantly better in the measure of cognition, daily activities, and behavioral symptoms. Adverse effects were of little significance in the galantamine groups. Because of its short half-life (calculated to be about 5 hours), galantamine was given twice per day, but three or four times per day might have been better.
GALANTAMINE REVERSES ALCOHOL-FREE LEARNING DECLINE
At the Medical University in Sofia, Bulgaria, rats were fed a steady diet of alcohol for 16 weeks.20 After a 2-week pause, they were given galantamine, which was found to reverse the decrease in speed of learning and short-term memory induced by the alcohol. After 4 weeks of galantamine, there was significant improvement in the passive avoidance memory test and a maze test, as compared to the saline-injected alcoholic group. Galantamine improved the speed of learning, short-term memory, and spatial orientation in these alcohol-impaired rats.
HOLY MOLY: BRINGING UP THE PAST
“Odysseus, the great teller of tales, launched out on his story,” begins the ninth book of the epic poem. In addition to having a great episodic memory, he is cast as a hero of memory, a great voyager, a hero of poetry, and a master of rhetoric. Memory is rhetoric (in the classical sense, the art of persuasion), entailing, per Aristotle, a thorough awareness of one’s audience. Thus, rhetoric involves the artistry of memory, and like poetry, is composed of one’s experiences, eidetic images, and the core abilities of the poet-remember-er. Thus, at the end of the journey, the heroic survival of Odysseus clearly
demonstrates not only the importance of memory and of nóos (mind), but of poetry itself—and, by extension, of language and communication.
Moly (galantamine) is instrumental to the triumph of Odysseus, as it may be for you. And if memory is a tool for learning about our own past triumphs and errors, mastery of it is also a tribute to the value and sanctity of memory. And now you know where the expression “Holy Moly” comes from. Holy Moly is galantamine.
References1. Graves R. The Greek Myths. Penguin Books, Harmondworth, England, 1960.
2. Plaitakis A, Duvoisin RC. Homer’s moly identified as Galanthus nivalis L.: physiologic anti-dote to stramonium poisoning. Clin Neuropharmacol 1983 Mar;6(1):1-5.
3. Paskov DS. Nivalin: Pharmacology and Clinical Application. Medicina i Fizkultura, Sofia, 1959.
4. Kalashnikov ID. Isolation of alkaloids from Galanthus nivalis L. Farm Zh 1970;25(3):40-4.
5. Venturi VM, Piccinin GL, Taddei I. Pharmacognostic study of self-sown Galanthus nivalis (var. gracilis) in Italy. Boll Soc Ital Biol Sper 1965 Jun 15;41(11):593-7.
6. Kirchev P, Stoyanov E. Studies in the activity of serum cholinesterase and histaminase in anaesthesia and surgical interventions. Nauchni Tr Vissh Med Inst Sofia 1966;45(4):27-34.
7. Paskov DS, Stoyanov KA, Saev SK, Tenev AK, Mincheva.ML. Clinical experience with Nivalin as anticholinesterase drug in anaesthesiological practice. Proc First Eur Congr Anesthesiol, Vienna, Sept. 3-9, 1962.
8. Strobbia R, Lalloni R, Dalzotto U The association of Nivaline with the vitamins of the B group (B1, B6, B12) and pyridoxal phosphate in the therapy of neuritis and neuralgia. Minerva Med 1968 Oct 27;59(86):4566-77.
9. Dudkin KN, Kruchinin VK, Chueva IV, Noskov OF, Tonkopii VD. Th e effect of cholinergic substances on the mechanisms of visual recognition in monkeys. Zh Vyssh Nerv Deiat Im I P Pavlova 1990 Sep-Oct;40(5):968-73.
10. Sirakov V, Kostadinova I, Velkova K, Kristev A. Roentgenographic study of ethosuximide-in-duced functional changes in rat gastrointestinal tract and their modulation by Nivalin in a chronic experiment. Folia Med (Plovdiv) 1998;40(4):71-7.
11. Perry EK. Cholinergic phytochemicals: from magic to medicine. Aging Ment Health 1997;1(1):23-32.
12. Wake G, Court J, Pickering A, Lewis R, Wilkins R, Perry E. CNS acetylcholine receptor activity in European medicinal plants traditionally used to improve failing memory. J Ethnopharma-col 2000 Feb;69(2):105-14.
13. Perry EK, Pickering AT, Wang WW, Houghton PJ, Perry NS. Medicinal plants and Alzheimer’s disease: from ethnobotany to phytotherapy. J Pharm Pharmacol 1999 May;51(5):527-34.
14. Lewis R, Wake G, Court G, Court JA, Pickering AT, Kim YC, Perry EK. Non-ginsenoside nicotin-ic activity in ginseng species. Phytother Res 1999 Feb;13(1):59-64.
15. Perry EK, Pickering AT, Wang WW, Houghton P, Perry NS. Medicinal plants and Alzheimer’s disease: integrating ethnobotanical and contemporary scientific evidence. J Altern Comple-ment Med 1998 Winter;4(4):419-28.
16. http://www.who.int/
17. Raskind MA, Peskind ER, Wessel T, Yuan W. Galantamine in AD: a 6-month randomized, placebo-controlled trial with a 6-month extension. The Galantamine USA-1 Study Group. Neurology 2000 Jun 27;54(12):2261-8.
18. Tariot PN, Solomon PR, Morris JC, Kershaw P, Lilienfeld S, Ding C. A 5-month, randomized, placebo-controlled trial of galantamine in AD. The Galantamine USA-10 Study Group. Neurology 2000 Jun 27;54(12):2269-76.
19. Snorrasson E, Geirsson A, Stefansson K. Trial of a selective acetylcholinesterase inhibitor, galanthamine hydrobromide, in the treatment of chronic fatigue syndrome. J Chron Fatigue Syndrome 1996;2(2/3):35-52.
20. Iliev A, Traykov V, Prodanov D, Mantchev G, Yakimova K, Krushkov I, Boyadjieva N. Effect of the acetylcholinesterase inhibitor galantamine on learning and memory in prolonged alcohol intake rat model of acetylcholine deficit. Methods Find Exp Clin Pharmacol 1999 May;21(4):297-301.
FIGHTING ALZHEIMER’S DISEASE WITH GALANTAMINE FIGHTING ALZHEIMER’S DISEASE WITH GALANTAMINE
30 AGINGMATTERS AGINGMATTERS 31
CANCER CELLS
WHY BOTHER?
WHY BOTHER?By Richard Swift
This article is written for a special side of you, let’s start with what and why. We have different mental and emotional states, and these combine to create attitudes. The combination that comes to the forefront at any time is influenced by what we are doing. We have one attitude at the office, another at parties, another with our family and another ‘investor’ attitude when making big decisions. This is the special side of you we invite you to bring out today.
Why? Because this article deals with maximising the return on the biggest investment you have ever made. The aim is to help you take a best practice approach to one of the biggest decisions you need to make from today onward. You will see why making no decision is highly likely to lead to the worst outcome.
Best practice in decision making is well known in the approach that Judges use. They listen to evidence and arguments for and against a proposition, they weigh the evidence and then they come to a reasoned decision. This approach is also used in Parliaments and businesses around the world and also in academic debates. The process can be tough to do, but if it is not corrupted it works every time. The first value of knowing how and why you reached a decision is firstly that you have a decision you can believe in, and secondly if circumstances change then you have a process you already understand. You can insert the change and see if it makes a real difference.
32 AGINGMATTERS AGINGMATTERS 33
WHY BOTHER?CROSS SECTION OF
THICK SKIN TISSUE IN MICROSCOPIC VIEW
WHY BOTHER?WHY BOTHER?
THE QUESTION WE LOOK AT TODAY IS: WHY BOTHER ABOUT AGING?
The most publicised view is a comforting ‘don’t bother, let the medical experts take care of you’. Government sanctioned drug company adverts show happy people taking pills and doctors from big hospitals looking wise.
The article below gives the main evidence and arguments for the opposite view.
“Why bother” is an abbreviation of “why should I bother to invest time and effort into something?”
We put the case for what we feel is worth bothering about and why it’s important. We also look at which people will consider it important and who will not be interested. We also look at why.
Finally, we outline how to get the best result from your effort if you decide to make it. The next article will deal with the detail of how to proceed.
Let’s start the main arguments.
WHAT IS WORTH BOTHERING ABOUT?
A little thought reveals that the popular phrase ‘Anti-Aging’ is not quite right. One cannot slow or reverse chronological aging any more than one can slow time, tides, winds or any other natural force.
But what we can do and what some people will consider well worth the investment of time and effort; is slowing and reversing the decline in our physical and mental vitality.
WHY IS THIS IMPORTANT?
Because we need our physical and mental vitality to get out to and to enjoy the special places the real world can show us, and the special times it can give us.
Why is it important to get out to see the world’s special places and have the special times? Because that was our dream when we were young. That is why most of us entered business or professional careers in the first place.
We did not enter careers to wall ourselves away in offices and gaze at spread sheets. We entered careers to eventually be free and able to get out and gaze in wonder at mountains and oceans and to enjoy life. The difference is that we chose to do it on a foundation of financial security- rather than have the precarious life of a wanderer.
The reason that tackling age-related decline is important is that physical and mental decline robs us of the ability to fulfil our young dreams; it robs us of our ability to fulfil our life purpose. Decline robs us of the return we deserve on the biggest investment we have ever made, the 25+ years of our peak vitality we put into our careers and raising our families.
Decline snatches victory away from us and it puts us on an ever-steepening slope into a depressing and often painful prison. Yes, it really is as bad as that. Look at the less fortunate souls around you who are trying to stay positive and cheerful. But you know it is a mask or a delusion, because you see that the light in their eyes is dying and the song inside them is silent.
These are the main arguments for why we should bother. Now on to the Who, When, How and finally the What.
34 AGINGMATTERS AGINGMATTERS 35

WHY BOTHER? WHY BOTHER?
WHO WILL AVOID THE FATE MOST PEOPLE SUFFER?
The take-away from this next section is: “if you do what most people do, you will get what most people get”.
In the context of age-related decline, we argue: “If you are in average health for your age, and you do what most people do, which is going to see a doctor when you feel ill and take his/ her advice, then you can expect to decline at the average rate and die at the average age”.
Some people will invest time and effort to beat the average, while most people will not. Let’s now look at a rational argument for why this happens.
The key is to look at what type of person will consider age-related decline important enough to bother. Then we may see why the majority do not bother.
Basically, people who have a big investment in their lives will see declining vitality as a priority problem and will act. These people will have a good chance of beating the average if their actions are well thought through and sensibly implemented. We cover these in the How and What sections below.
Most people who have no serious investment in their lives will probably nod and pay lip service to this article but are unlikely to do anything. This is no secret; we see it happening around us every day.
Asking ‘why’ most people do nothing gets us to the root of the problem. It seems to be mainly because most people regard themselves as consumers rather than creators and co-creators.
In this context ‘consumer’ means people who expect to have things done for them, either for a payment or as a right. An example is an all-inclusive resort. People pay, turn up and consume unlimited food and drink. It is an overall ‘consumer experience’. Drive-through fast food outlets are another example--people consume without even leaving their cars. Many people live in commercially produced synthetic worlds in which they passively consume stimulation from sport and films on TV. They also consume
thoughts and opinions from TV that they can regurgitate at other times. At the same time synthetic food additives, sugars and alcohols numb their consciousness.
The real problem comes when consumers regard their health the same way, laying off the responsibility to doctors and their medical insurance. Government sanctioned marketing of “a pill for every ill” encourages this attitude.
A passive consumer attitude is appropriate for emergency treatment required after car crashes and other traumas. However, you will see in the How and What sections that a consumer attitude certainly does not work to reverse the chronic conditions brought on by a consumer lifestyle.
Chronic conditions now account for over 80% of premature decline, disability and death in the West and in most other developed countries around the world.
A creator and co-creator attitude means that people feel responsible, or more accurately, “response-able”, for their future success or failure.
We first experience this reality and this response-ability in school and university. We find that our teachers and professors are there to help us learn, but we are responsible for doing the study work with their help.
Later we experience creation and co-creation in our business or professional career. Building a business or a professional practice is certainly not a consumer experience; it is very much hands-on creating and building brick-by-brick. Staff and consultants can help you create, but they cannot and should not be asked to plan and build a business; that rarely works for long.
Even beauty is a mainly a creation and co-creation experience. Makeup and clothes certainly can help, but in the end, beauty depends on a sound foundation of a healthy diet and lifestyle. Most of the most attractive people practice calorie restriction and go to bed early most of the time.
WHEN SHOULD WE START TAKING ACTION?
Let’s look at a simplified graph of the rise and fall over a lifetime of the average person’s ability to get out and enjoy the world. You need freedom, which comes at the end of school. You need physical and mental vitality, which peaks at around 19. You need some money to buy a backpack and get a ticket to somewhere special; most 19-year olds can find that. Finally, you need a dream destination to go for, because; “if you don’t have a dream, how are you going to make a dream come true?”
0 10 20 30 40 50 60 70 80 90 100
20
40
60
80
100
Age
Figure 1: Loss of vitality and ability correlated with age.
Around age 37, if we are in normal health, we notice the first signs of decline in mental and physical vitality. This is the age at which most athletes retire. Decline starts in our late 20s but experience holds athletes up for a while. We non-athletes don’t drive ourselves to the last 1% so we don’t notice until we have dropped a way.
By the time we hit 50, most of us find that peak physical performance is down to about 70% of what it was at age 20. By age 60 it is down to about 50%. To check this, see how far and fast you can run now and compare it with then.
Currently, the average age of death for men is 79, and 83 for women. As mentioned, if we are in average heath and
we do the average things that people do (see a doctor when we feel ill and take his/ her advice) then logic dictates that we can expect the average result.
Figure 1 shows our best estimate of the true decline curve. If you don’t agree with the straight line from 37 to 79, then draw your own curve- it makes little difference to the area under the graph and this is the important measure of your remaining enjoyable lifespan.
Figure 1 brings us face-to-face with reality and that can be tough to deal with. However, business and professional people and investors face tough realities and they have the tools to search for and implement real world solutions.
Vita
lity/
Abi
lity
(%)
36 AGINGMATTERS AGINGMATTERS 37
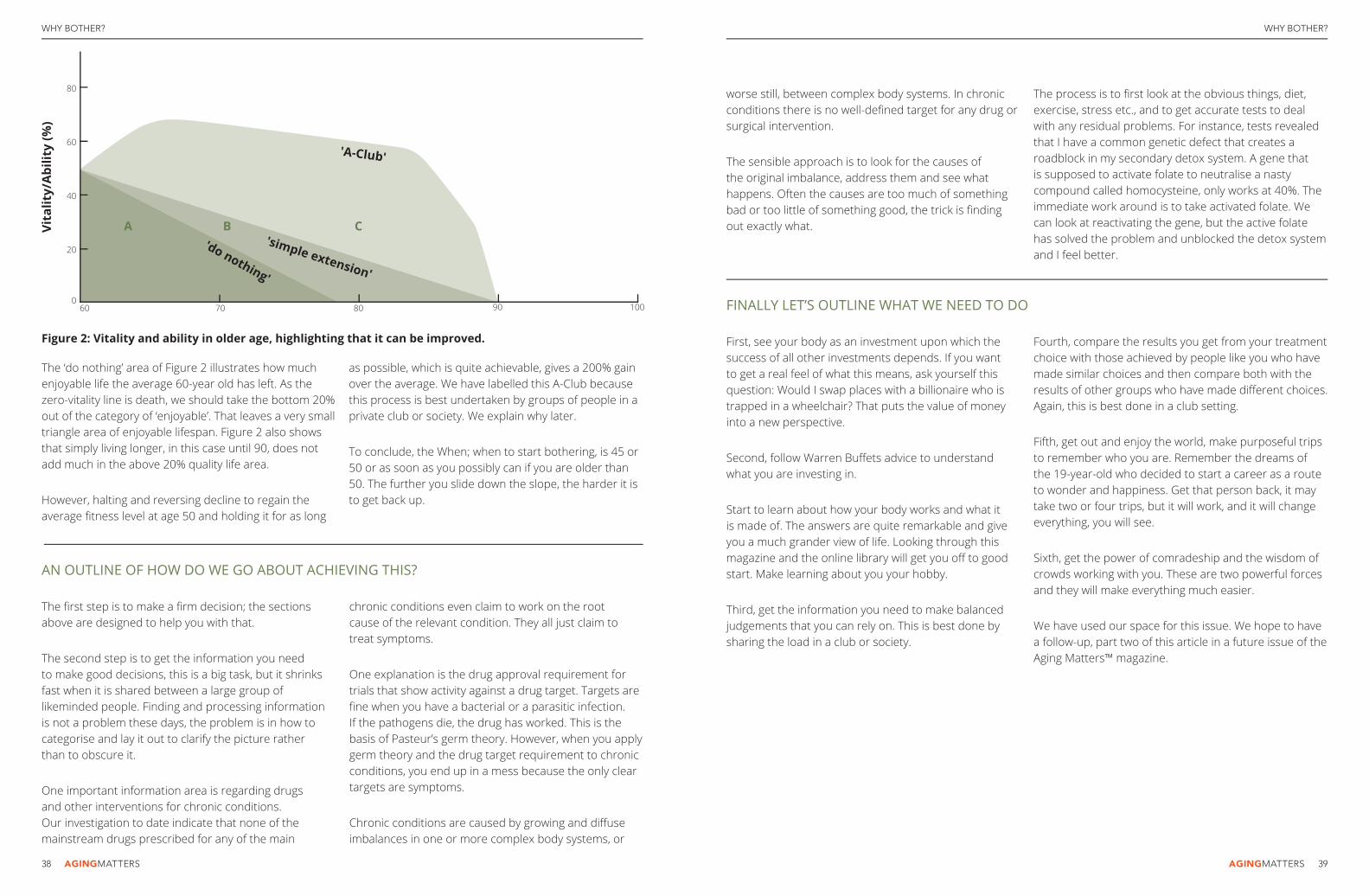
WHY BOTHER? WHY BOTHER?
070 80 90 100
20
60
40
60
80
Vita
lity/
Abi
lity
(%)
'A-Club'
A B C'simple extension'
'do nothing'
Figure 2: Vitality and ability in older age, highlighting that it can be improved.
The ‘do nothing’ area of Figure 2 illustrates how much enjoyable life the average 60-year old has left. As the zero-vitality line is death, we should take the bottom 20% out of the category of ‘enjoyable’. That leaves a very small triangle area of enjoyable lifespan. Figure 2 also shows that simply living longer, in this case until 90, does not add much in the above 20% quality life area.
However, halting and reversing decline to regain the average fi tness level at age 50 and holding it for as long
as possible, which is quite achievable, gives a 200% gain over the average. We have labelled this A-Club because this process is best undertaken by groups of people in a private club or society. We explain why later.
To conclude, the When; when to start bothering, is 45 or 50 or as soon as you possibly can if you are older than 50. The further you slide down the slope, the harder it is to get back up.
FINALLY LET’S OUTLINE WHAT WE NEED TO DO
First, see your body as an investment upon which the success of all other investments depends. If you want to get a real feel of what this means, ask yourself this question: Would I swap places with a billionaire who is trapped in a wheelchair? That puts the value of money into a new perspective.
Second, follow Warren Buff ets advice to understand what you are investing in.
Start to learn about how your body works and what it is made of. The answers are quite remarkable and give you a much grander view of life. Looking through this magazine and the online library will get you off to good start. Make learning about you your hobby.
Third, get the information you need to make balanced judgements that you can rely on. This is best done by sharing the load in a club or society.
Fourth, compare the results you get from your treatment choice with those achieved by people like you who have made similar choices and then compare both with the results of other groups who have made diff erent choices. Again, this is best done in a club setting.
Fifth, get out and enjoy the world, make purposeful trips to remember who you are. Remember the dreams of the 19-year-old who decided to start a career as a route to wonder and happiness. Get that person back, it may take two or four trips, but it will work, and it will change everything, you will see.
Sixth, get the power of comradeship and the wisdom of crowds working with you. These are two powerful forces and they will make everything much easier.
We have used our space for this issue. We hope to have a follow-up, part two of this article in a future issue of the Aging Matters™ magazine.
AN OUTLINE OF HOW DO WE GO ABOUT ACHIEVING THIS?
The fi rst step is to make a fi rm decision; the sections above are designed to help you with that.
The second step is to get the information you needto make good decisions, this is a big task, but it shrinks fast when it is shared between a large group of likeminded people. Finding and processing information is not a problem these days, the problem is in how to categorise and lay it out to clarify the picture ratherthan to obscure it.
One important information area is regarding drugs and other interventions for chronic conditions. Our investigation to date indicate that none of the mainstream drugs prescribed for any of the main
chronic conditions even claim to work on the rootcause of the relevant condition. They all just claim to treat symptoms.
One explanation is the drug approval requirement for trials that show activity against a drug target. Targets are fi ne when you have a bacterial or a parasitic infection. If the pathogens die, the drug has worked. This is the basis of Pasteur’s germ theory. However, when you apply germ theory and the drug target requirement to chronic conditions, you end up in a mess because the only clear targets are symptoms.
Chronic conditions are caused by growing and diff use imbalances in one or more complex body systems, or
worse still, between complex body systems. In chronic conditions there is no well-defi ned target for any drug or surgical intervention.
The sensible approach is to look for the causes ofthe original imbalance, address them and see what happens. Often the causes are too much of something bad or too little of something good, the trick is fi nding out exactly what.
The process is to fi rst look at the obvious things, diet, exercise, stress etc., and to get accurate tests to deal with any residual problems. For instance, tests revealed that I have a common genetic defect that creates a roadblock in my secondary detox system. A gene that is supposed to activate folate to neutralise a nasty compound called homocysteine, only works at 40%. The immediate work around is to take activated folate. We can look at reactivating the gene, but the active folate has solved the problem and unblocked the detox system and I feel better.
38 AGINGMATTERS AGINGMATTERS 39
MZS™SPOTLIGHT
BECAUSE NOT ALL MELATONINS’ ARECREATED EQUAL
Melatonin is produced by the pineal gland at night to regulate our circadian rhythm, (sometimes called the sleep wake cycle). As we age the amount of melatonin we produce reduces resulting in many older people sleeping less and having a lower quality of sleep. Our melatonin has been formulated by the world’s foremost melatonin expert Dr. Walter Pierpaoli, his Melatonin Zn Se, or MZS™, is totally unique since it is designed to mimic the natural night peak of melatonin- to leave you feeling refreshed and alert the following day.
What does Melatonin do?
Melatonin is vital to protect our hormonal system, regulate immunity and repair our body’s cells. It is commonly used by shift workers and also to treat jet lag and age related sleep disorders. Melatonin is an extremely eff ective antioxidant; in fact on a molecule to molecule
basis; melatonin has proved to be signifi cantly more effi cient in neutralizing toxic hydroxyl-radicals than the two well-known freeradical scavengers, glutathioneand mannitol. Its eff ect on longevity is well documented. Experts believe melatonin has a positive eff ecton aging.
Age related macular degeneration (ARMD) comes in two forms, wet and dry and is a notoriously diffi cult disorder to treat and is linked to blindness. A 24-month study, (published in NY Academy of Science, 2005, 1057:384-392) on 100 patients showed that after 3 months, the majority of patients taking 3 mg of Melatonin Zn Se nightly had halted the progression of their age related macular degeneration and at 6 months many showed reversal of their ARMD. Remarkably this was true for both the wet and dry forms!
Why is Dr. Pierpaoli’s MZS™ more eff ective than other melatonin supplements?
Firstly it is of pharmaceutical quality
at a dose of 3mg. Secondly, it contains the synergistic ingredients of selenium and zinc. Thirdly and most importantly- it is designed to release at a very specifi c time. Dr. Pierpaoli’s research led him to perfect a formula that exactly mimics the pineal gland’s release of melatonin. MZS is the only melatonin supplement to follow nature’s own night peak. Take half to one 3mg tablet at bedtime only; do not take more than two tablets. By taking MZS™ between 9pm and 11pm you will create a night peak between 1am and 3am, this is the most natural and normal time to have the highest melatonin levels.
MZS is much more than a sleep aid and melatonin has many published benefi ts. MZS comes with the endorsement of Dr. Pierpaoli. If you’ve tried other melatonin and didn’t notice a signifi cant eff ect, then we highly recommend you try Dr.Pierpaoli MZS for a superior experience.
OXYTOCINSPOTLIGHT
OXYTOCIN FOR PASSIONAND SEX
Oxytocin is a hormone produced by the hypothalamus, excreted via the pituitary gland. Its orthodox medicine role is to help women give birth, since the large dose that’s injected helps to relax the uterus and alleviates the passage of the child. Dr.Thierry Hertoghe’s book, ‘Passion, sex and longevity, the oxytocin adventure’ highlights that it has many other roles too.
The Love Hormone
Oxytocin has been dubbed ‘the love hormone’. It can induce feelings of bonding and care. Its measurements have been taken between lovers, friends, relatives, parents and their children etc. it has been noted that oxytocin levels are higher when they are in their presence. Mothers naturally bond with their children, but even men, (especially those who experience the live birth), express their emotions as wanting to care and protect their off spring. These eff ects may be attributable to the
release of oxytocin hencetriggering the bond. However, psychopaths are notoriously low in their oxytocin levels, which may be a cause of their uncaring feelings towards other humans.
The pain and orgasm connection- Fibromyalgia can be a very debilitating disorder with a lot of pain, sometimes constant for those who suff er with it. In women, it was noted that when they were experiencing an orgasm they felt no pain at all. Women undergo a burst of oxytocin during orgasm. Trails were undertaken to see if oxytocin supplementation could alleviate the pain of Fibromyalgia, there was some success, but the side-eff ect noted was that those women now enjoyed multiple orgasms!
The eff ects of Oxytocin
Dr. Hertoghe explained that some will not feel the eff ects of oxytocin. For two reasons, (if we consider that the dose is correct for that individual). Firstly, some people are ‘low’ in their principal sex hormone,
so if a man is low testosterone, or if a woman is low estrogen, it is possible that oxytocin will not elicit its full potential in those persons. The other issue could be low vasopressin, vasopressin is a counterpart to oxytocin, produced and released via the same glands. In cases of vasopressin defi ciency, the patient may enhance the oxytocin experience by adding one or two sprays (10IU) each of vasopressin via the Vaso-Pro nasal spray.
Doses are very dependent upon its use. For social or sexual enhancement, 5 IU to 10 IU is a ‘typical’ dose. Dr. Hertoghe reduced the doses that he recommends in his books, (Transmitted via personal conversation to me). Currently IAS is providing Oxy-sub in 20 IU trouches ( a soft sublingual tablet). These can be cut into half or a quarter for a dose of 5 or 10 IU and should be placed under the tongue and allowed to melt. The other option is Oxy-Pro which is applied intranasally delivering 10 IU per spray.
OXYTOCIN
SPOTLIGHTSPOTLIGHT
40 AGINGMATTERS AGINGMATTERS 41
CAN-C™ SPOTLIGHT
A BREAKTHROUGH FOR CATARACT
Can-C™ eye-drops are the original™ brand- developed by Innovative Vision Products (IVP). This group were the fi rst to research, publish and prove how eye-drops can reduce and even eradicate cataract. Accordingly there are active US and EU patents (and others pending) on this unique and special product.
Unique formula:
Can-C™ eye-drops are the formula from the original published human trials. They contain a purifi ed and racemized form of n-acetylcarnosine (made in Japan); this natural di-peptide has potent anti-glycating and anti-oxidant properties that prevents lipid peroxidation. Note that the formula is important- it’s not all about the n-acetylcarnosine; the specifi c carrier agents and their purity are also important. If you look at the Can-C™ formula you will see diff erences to the copycats, (remember it is only Can-C™ that is patented in recognition of the original work). If you want the best possible results in the fastest
possible time, then choose Can-C™ to deliver them according to the clinical trials.
Clinical trial:
Patients placed two-drops of Can-C™ into their eyes twice daily for a 6-month period, the outcome was:
– 90% saw an improvement in their visual acuity.
– 88.9% of patients showed improvement in the clarity oftheir lens.
There have been numerous reports of cataract shrinkage and even disappearance with documented evidence that Can-C™ eye-drops remain eff ective (and safe) more than 24-months later. The most commonly expressed initial reports are that glare is signifi cantly improved, (for example night driving is much safer) and color perception is enhanced.
Improving eye-sight:
More evidence is mounting that Can-C™ is effi cacious for many
conditions including: – Cataracts (particularly the senile version)
– Glaucoma – Presbyopia – Corneal disorders – Eye strain – Ocular infl ammation – Blurred vision – Vitreous opacities and lesions – Diabetes mellitus complications – Contact lens users – Dry eye syndrome
Of special interest may be to persons who wear contact lenses. This is because Can-C™ inhibits the accumulation of lactic acid and therefore contacts can be worn for longer periods without pain.
We have also received reports that Can-C™ not only aids dry-eye syndrome with its lubricants, but that Can-C™ helps to unclog proteins from the lacrimal ducts, thus releasing more natural tears onto the eye.
In a similar way, it is also believed that the unclogging of proteins in the eye’s drain, (the Schlemm valve), helps to reduce intraocular pressure and thus aids glaucoma.
DEPRENYLSPOTLIGHT
FOR FOCUS AND CONCENTRATION
Deprenyl is also known as selegiline, it was created in the 1960s by Professor Joseph Knoll, principally as an aid to Parkinson’s patients- because deprenyl has a signifi cant benefi t to improve dopamine levels in the brain.
Signifi cant longevity studies
Professor Knoll’s experiments with rats produced some of the most incredible longevity benefi ts. When fed deprenyl in their food, they lived longer than those that were not. After the last non-treated rat died, the fi rst of the deprenyl rats hadn’t! These results were in another study conducted from research by, Dean, Fowkes and Morgenthaler-published in the book, ‘Smart drugs & nutrients’. It highlights that the loss of dopamine in humans with age, can be mapped against the development of Parkinson’s and even death.
Deprenyl has been expressed as a MAO-b inhibitor. Preventing the enzyme monoamine-oxidise type-b from destroying dopamine, ergo
leading to its greater availability in the brain.
The inhibition of the more common MAO-a can be problematic, leading to something called ‘the cheese eff ect,’ not a side eff ect of deprenyl, although it should be noted that dopamine can inhibit type-a, usually at very high doses of 20mg. Professor Knoll has noted that there is another signifi cant action of deprenyl and this is the raising of PEA levels. PEA is a catecholamine activity enhancer that raises norepinephrine levels, it’s a signifi cant attention agent that is behind the primary mechanism of the famous Eugeroic drug- modafi nil (Provigil). Read professor Knoll’s books- ‘The brain and itself’, or ‘How selegiline/deprenyl slows brain aging.’
Typical patient responses
A patient who has mild cognitive impairment, or age related minor cognitive dysfunction, the most common report is a signifi cant improvement in their focus and concentration. Persons with higher dopamine levels often appear more ‘driven’ and ‘dedicated’.
Avoid overuse since it can lead to what may appear to be an oppressive behaviour, as others around you are not focused and ‘on the ball’ as you! We recommend breaks from deprenyl use.
Some advocate one week off in the month and other use it during the weekdays but not at the weekends.
Doses are based on need and age. Parkinson’s patients will require large doses. A person wanting to improve their cognitive performance may want to consider 1mg to 3mg per day, with occasional breaks. These doses do not take into account synergy with other dopamine enhancing agents and persons using anti-depressants should consult with their physician. Deprenyl tablets are provided in 5mg form (Jumex), some like to take ½ to 1 of these tablets 3 times a week. The use of the deprenyl liquid (Dep-Pro) is particularly attractive for those using deprenyl to generally support, portect and improve neurological function, since 1 drop = 1mg, the liquid can be dosed very precisely by placing those drops into a cold drink. Avoid use in the late evening to prevent any sleep disruption.
SPOTLIGHTSPOTLIGHT
42 AGINGMATTERS AGINGMATTERS 43
PEPTIDE BIOREGULATORS
SPOTLIGHT
PIRACETAMSPOTLIGHT
SPOTLIGHT
THE DISCOVERY OF GENE SWITCHES IN FOOD
Today Professor Vladimir Khavinson is the President of the European Academy of Gerontology and Geriatrics, but in the 1980’s he was a Colonel in the Soviet Union military medical corps. At the time, he and his team were approached by Kremlin offi cials, they wanted them to fi nd a way to protect their troops from a myriad of problems; issues such as radiation for submariners in nuclear submarines to troops that may be blinded from known, (but thankfully unused) new weapons such as battlefi eld lasers.
A former Sovietmilitary secret!
What their research uncovered - that was used for two decades on many thousands of men and women - was a remarkable link between short chain peptides and DNA. This former military secret is now available to the public as peptide bioregulators. Their published research has identifi ed that each organ / gland / tissue uses a highly specifi c short chain peptide, obtained from food,
to act as a ‘short-cut’ to initiate protein synthesis. These peptides, unlike proteins, can enter the blood through the stomach. Through a comprehensive list of patents and even copyrighted PowerPoint slides, the Russian research group have shown that each of the concentrated peptide bioregulators so far examined, interact with particular strands of DNA - eff ectively and very specifi cally activating repair and regenerative processes.
This is a remarkable story since what we are describing here are peptides that act as individualised gene switches. To date, they have been tested for many years on thousands of individuals, without report of any serious side eff ects or contraindications. We believe that they could be set to ‘out do’ stem cells. Why? Because this peptide therapy is relatively cheap, highly specifi c, can be taken orally and doesn’t require any suppression of the immune system to operate fully (as stem cells do).
Oral material from the trials
The peptide bioregulators available via IAS are the bovine originals;
sourced from carefully chosen Danish calves and processed through pharmaceutical processes and fi lters. They are not the synthetic versions which have not been studied/ proven. Peptide bioregulators act as they sound-to regulate; for example, Thryreogen® the thyroid peptide would increase thyroid activity if it were too low, but decrease if it were too high.
Dosing
Doses are very dependent upon the need and unlike hormones these peptides do not have to be taken every day, hence making them a cost eff ective regime. A typical/ average use could be considered as follows:
– Start with an intensive course: 2 capsules once a day for 30-days.
– Thereafter use 2 capsules once a day for 10-days, repeat every 2, 3, 4 or even as little as 6-months.
The story of the peptide bioregulators is a remarkable one and we recommend that you to read the articles and interviews and see the video on the IAS website.
SPOTLIGHT
PIRACETAM, THEORIGINAL NOOTROPIC
Smart drugs and nutrients, or to give them their correct medical terminology- nootropics, are agents that can not only improve conditions of senile dementias, but in recent times have become popular for older individuals to improve their mental and cognitive processes.
It was Ward Dean, M.D. who highlighted these facts throughhis very popular ‘Smart Drug’series of books in the 1980s, since then the term ‘smart drugs’ hasbecome mainstream.
Piracetam, theoriginal nootropic
The smart-drug we focus on here was in fact the fi rst, developed as it was by Dr. Giurgea for UCB laboratories in Belgium in the 1960s. Originally it was designed to assist with travel and altitude sickness, but shortly afterward individuals realised that piracetam had positive cognitive enhancement eff ects.
Piracetam is a cognition agent that has been used successfully to treat a wide range of conditions, for example it has been shown to increase a person’s attention levels and improve memory and intelligence. Piracetam can help to slow down ‘senile involution’, dementia and Alzheimer’s disease. In tests and trials, piracetam induces signifi cant improvement to memory consolidation and recall in those suff ering from ‘age-associated memory impairment’.
Piracetam has also been used to improve patient’s recovery from strokes, particularly improving post stroke speech impairment (aphasia). Another use has been in cases of acute and chronic cerebral ischaemia, (decreased blood fl ow to the brain). Using piracetam has restored speech and the use of limbs in these patients; it has also increased neuronal activity in the brain when measured with EEG.
For regular individuals, piracetam has been shown to enhance idea creation and the ability to ‘see things through,’ in other words to have
ideas and being them to fruition. The level of clarity piracetam creates is often described/ perceived as; “the fog has lifted.”
How does piracetam work?
Piracetam’s key and uniquemethod of action is upon theCorpus Callosum, the region of the brain that links the two hemispheres. Most experts believe it is the keythat gives piracetam users the ability to channel greater brain potentialby connecting the logical side ofthe brain with the creative sidemore eff ectively.
What are the doses of piracetam? A common dose is 800mg tablets three times a day, then lowering to 800mg twice a day after the fi rst month. The eff ects of piracetam can be enhanced if taken concurrently with centrophenoxine or hydergine. Side eff ects are minimal and seldom experienced, but should you experience nausea or a headache then it is usually caused by an overdose. In which case reduce the dose and build up more slowly.
SPOTLIGHT
44 AGINGMATTERS AGINGMATTERS 45

THYROID SUPPORTSPOTLIGHT
NATURAL HRTSPOTLIGHT
SPOTLIGHT
FOR THE HYPOTHYROID EPIDEMIC
Dr. Broda Barnes in the 1970s estimated that 40% of the adult population was defi cient in thyroid hormones; he published this statement in his excellent book- ‘hypothyroidism, the unsuspected epidemic.’ Since then, pupils of Dr. Barnes, such as Dr. Richard Wilkinson, have suggested that this fi gure could be even greater now!
This is important because the thyroid gland is of pivotal importance to our overall health, but like the majority of hormones, as we age the production of thyroid hormones decline. This lack of thyroid function is the root cause of a wide variety of age-related health disorders. Ergo, supplementation with a synthetic, or a natural thyroid can have a signifi cant positive eff ect on a wide range of age-related problems.
The importance of the thyroid gland
The hormones produced by the thyroid control the body's metabolism- the rate at which it burns calories for energy. It also controls the body's utilization of fat, so a decline in the secretion of hormones from the thyroid gland, (known as hypothyroidism) can result in wide range of symptoms such as poor concentration, confusion, memory problems, cold hands and feet and weight gain.
Another serious condition which can be caused by and result from an underactive thyroid are painful musculoskeletal issues that aff ect tendons, muscles and ligaments.
Choosing between synthetic and natural thyroid supplements
IAS stocks a comprehensive range of both synthetic and natural thyroids, although we advocate the use of a natural supplement over a synthetic,
this is because products such as Armour® are of a porcine origin, so they naturally contain the full spectrum of T1, T2, T3 and T4 thyroid hormones, (note the bottles only list the amounts of T3 and T4 because very few physicians are familiar with T1 and T2).
Natural desiccated thyroids are measured in grains; with one grain being equivalent to approximately 60 mg. IAS carries doses from ¼ grain to 2 grains, with brands including Armour®, ERFA® and Nature®. IAS also provides synthetic T3 in 20 mcg and T4 in 100 mcg tablets.
Thyroid supplements provide potent antiaging protection. Many aging individuals can benefi t from taking a thyroid supplement because this remarkable hormone has such a profound aff ect across so many diff erent conditions. Many antiaging physicians consider thyroid support an essential part of any serious attempt to improve a person’s health-span and longevity.
THYROID SUPPORT
SPOTLIGHT
NATURAL ESTROGENS AND PROGESTERONE FOR WOMEN
In this featured section we are focusing on the use of natural estrogens and progesterone for women, normally utilised to aidthe menopause. IAS carries a wide range of bioidentical hormones - a term that means ‘natural to and in the body.’
When hormone replacement therapy (HRT) was developed in the 1920s, estrogens had to be derived from horse urine because a laboratory solution was too diffi cult or expensive to synthesize. Facts pointed out by Dr.Wright in his best-selling book ‘Stay Young & Sexy’. Estrogens can be easily produced now. Some people believe that the known side-eff ects from ‘traditional HRT’ are due to the fact that the hormones given are not correct.
Introducing Esnatri
Esnatri™ is our bioidentical triple estrogen cream. One of the best
biodentical estrogen creams available. It comes directly from the work of Dr.Wright who has shown that the majority of women produce estrogens in the ratios of 90% estriol, 7% estradiol and 3% estrone.
Most tri-estrogen preparations attempt to replicate the human hormones estriol, estradiol and estrone, apply them in the ratioof 80:10:10, while some evenentirely over-look estriol, claiming it is a weak estrogen. But, women naturally produce high levels of estriol and it is considered to have anticarcinogenic eff ects.
The Esnatri cream can be applied by daily rotation to your neck, upper chest, breasts and behind your knees, or inner thighs. A typical starting dose is 2mg. Start from day one (of what would have been the start of your menstrual cycle) and continue until day 25. You should stop for fi ve days, before repeating the application at the start of the next menstrual cycle. During these last few days, the estrogen receptors are being allowed to ‘rest’ as they have been accustomed.
Combining Estrogen with Progesterone
Progesterone is the counterbalance to estrogens. Women can signifi cantly decline in estrogen levels during menopause – they rarely reach zero production levels, whereas progesterone can sometimes not be measured at all in elderly women. It is also the low progesterone that most signifi cantly impacts bone strength, leading onto osteoporosis. There are numerous reasons to ensure that progesterone is also taken alongside an estrogen therapy. IAS provides a 5% strength natural progesterone cream. Typical doses are 25mg to 30mg of progesterone applied on day 10 and continuing to 25. The start date varies according to the usual timing of your ovulation. As with the Esnatri cream, sop for the last 5 days of your cycle so that the estrogen receptors have their accustomed ‘rest’ period. Remember, your hormone replacement therapy should be overseen by a physician and should not be undertaken if you have undergone cancer treatment.
46 AGINGMATTERS AGINGMATTERS 47
SAVE ON MANY ANTIAGING PRODUCTS.
Simply use the voucher codes below within the stated timeframe and on the websites mentioned, (products may be restricted in some countries and prices may be subject to taxes and S&H where appropriate).
THE ANTIAGING STORE
For the above go to: www.theantiaging.store (payments by e-Check and Wire).
4MU-PRO™ 100x1000mg tablets $119.99 Buy 3x and save $20.00 per pack.
OFFERS PAGELONGEVITY SUPPLEMENTS STORE
For the above go to: www.longevitysupplements.store (accepts payments by all major credit cards).
ACF-228®30-capsules $39.99 Buy 3x and save $6.66 per pack.
ATP-PRO™(ADENOSINE TRIPHOSPHATE)Save $5.00 normally $24.99 just $19.99for 60 capsules.
B17-PRO™ (AMADAYLIN)Save $5.00 normally $29.99 just $24.99 for 90x100mg tablets,VALID UNTIL 31/12/2018 WITH CODE: ANTIAGING-3
DMSA (DMSA-PRO™)Save $5.00 normally $39.99 just $34.99 for 60x 100mg capsules.
GALANTAMINE (REMINYL®)28x 8 mg tablets $29.99 (save $5.00 with voucher at $24.99)SHORT EXPIRY: 31/12/2018
MSH2 (MSH2-PRO™)Save $10.00 normally $49.99 just $39.99 for 20ml 20mg nasal spray.
SILDENAFIL-PRO™ (GENERIC VIAGRA®)Save $6.00 normally $19.99 just $13.99 for 10x100mg double-scored tablets.
BETA-GLUCANS CREAM (BG-PRO™)Save $12.00 normally $39.99 just $27.99 for 50ml tube.
CAN-C™ EYE-DROPS1x pack (2x 5ml bottles) $39.99Buy 3x and save 10% Buy 6x and save 20%
GCB70-PRO™ (GREEN COFFEE BEAN EXTRACT)Save $6.99 normally $24.99just $17.99 for 30x 500mg capsules.
PEPTIDE BIOREGULATORSFrom $59.99 for 20x 200 mg capsules.Save $30.00 when you buy them in 60-capsule packs.
PEPTIDES IN THE EPIGENETIC CONTROL OF AGEINGA 263-page book by Professor Vladimir Khavinson.Save $20.00 normally $94.99 just $74.99VALID UNTIL 31/01/2019 WITH CODE: LONGEVITY-2
THE ANTIAGING STORE
100x1000mg tablets $119.99 Buy 3x and save
(ADENOSINE TRIPHOSPHATE) normally $24.99 just $19.99
OFFERS OFFERS
48 AGINGMATTERS AGINGMATTERS 49

www.antiaging-systems.com is your comprehensive resource for information about all the leading commercially available antiaging, preventative and regenerative products and therapies available today. Visit www.antiaging-systems.com and find articles, videos, audio-files, all referenced with a guide of where to obtain your needs.
Currently the site covers topics related to all the following products.
BOOKS
– Atlas of Endocrinology – Great Teeth for Life – Passion, Sex & Oxytocin – Physician Hormone Handbook V2
– Cataract Cure – Melatonin, the Key of Life – Peptides in the Control of Ageing – Reversing Physical Aging V1
– Eyesight Saviors – Natural Skin Cancer Treatments – Peptide Biomarker Revolution
HORMONES
– Aldosterone (Aldo-Pro™) – HCG (HCG-Pro™) – MSH2 (MSH2-Pro™) – Progesterone (Progest-Pro™) – TRH (Abaris™)
– DHEA (DHEA-Pro™) – Hydrocortisone (Hydrocort-Pro™) – Oxytocin (Oxy-Pro™) – Thymus – Vasopressin (Vaso-Pro™)
– Estrogens (Esnatri™) – Melatonin (MZS™) – Pregnenolone (Preg-Pro™) – Thyroid (Armour™ etc.)
NUTRITION
– 1st Line™ (OSCN) – Benfotiamine (Milgamma™) – Boluoke® (Lumbrokinase)
– 5HTP (5-HTP-Pro™) – Beta-Glucans (BG-Pro™) – Boost-Pro™
– ACF-228®
– Boluoke® (Lumbrokinase) – Can-C™ + capsules
DIAGNOSTICS
– Bio-Clip™ CUFF – Foodsafe® – Vielight®
GHRPS
– GHRP2 (GHRP2-Pro™) – GHRP6 (Release-Pro™) – Sermorelin (Serm-Pro™)
ANTIAGING-SYSTEMS.COM
PEPTIDE BIOREGULATORS
– Adrenal (Glandokort®) – Bone Marrow (Bonomarlot®) – Heart (Chelohart®) – Lungs (Taxorest®) – Pancreas (Suprefort®) – Prostate (Libidon®) – Testes (Testoluten®)
– Bladder (Chitomur®) – Cartilage (Sigumir®) – Kidney (Pielotax®) – Muscle (Gotratix®) – Parathyroid (Bonothyrk®) – Retina (Visoluten®) – Thymus (Vladonix®)
– Blood Cell (Ventfort®) – CNS/ Brain (Cerluten®) – Liver (Svetinorm®) – Ovaries (Zhenoluten®) – Pineal (Endoluten®) – Stomach (Stamakort®) – Thyroid (Thyreogen®)
SMARTS
– Adrafinil (Adra-Pro™) – Deprenyl (Dep-Pro™) – Modafinil (Moda-Pro™) – Pramiracetam (Pram-Pro™)
– Aniracetam (Ani-Pro™) – Hydergine® (Hy-Pro3™) – Picamilone (Picamilon-Pro™) – Reminyl® (Galantamine)
– Centrophenoxine (Centro-Pro™) – Idebenone (Ideb-Pro™) – Piracetam (Pira-Pro™) – Vinpocetine (Vin-Pro™)
TOPICALS
– BEC5® Curaderm cream – Minmax-Pro™ – Retin-Pro™
– Can-C™ eye-drops – NeyDent® toothpaste – TA65® cream
– Joint-Pro™ cream – Oraltide™ mouthwash – Youth Gems®
SPECIALIST (INCLUDING MEDICINES)
– 4MU (4MU-Pro™) – Anastrozole (Arimidex®) – BHT (BHT-Pro™) – Doxycycline – Finasteride (Proscar®) – Naltrexone (Nal-Pro™) – SAMe (SAMe-Pro™)
– Acarbose (Glucobay®) – ATP-Pro™ – Bromocriptine (Parlodel®) – Dutasteride (Avodart®) – Gerovital-H3® (GH3-Pro™) – Relax-Pro™ (GABOB) – Sildenafil (Sildenafil-Pro™)
– Aminoguanidine (Amino-Pro™) – B17-Pro™ (amadaylin) – DMSA (DMSA-Pro™) – EDTA (EDTA-Pro™) – Metformin (Met-Pro™) – Reminyl® (galantamine)
– Carnosine (Carno-Pro™) – DIM (DIM-Pro3™) – L-tryptophan (Ltryp-Pro™) – NADH – Novisyn® (Hyaluronan) – PQQ (PQQ-Pro™) – Symprove®
– Vitamin D3 (D3-5000™)
– CoQ10 (CoQ10-Pro™) – Fenfuro-Pro™ – MultiV45-Pro™ – NEO40®
– PEA (Pain-Pro™) – Resveratrol (Resveratrol-Pro™) – TA65® capsules (250)
– Curcumin (Curcumin-Pro™) – GCB70-Pro™ – NAD+ (NAD+Pro™) – Nitric-Pro™ – PEO (PEO-Pro™) – Sleep-Pro™ – Vitamin B12 (B12-Pro™)
ANTIAGING SYSTEMS ANTIAGING SYSTEMS
50 AGINGMATTERS AGINGMATTERS 51

www.antiaging-systems.com
Growing older never felt better
• World’s largest antiaging resource
• Global perspective
• More than 25 years’ experience
Tomorrow's treatments today™


















