The Immune system - thecnm.com 15 - Immune System -201… · Skin & Mucous Membranes = ... •...
99
Biomedicine THE IMMUNE SYSTEM Copyright CNM – College of Naturopathic Medicine 1
Transcript of The Immune system - thecnm.com 15 - Immune System -201… · Skin & Mucous Membranes = ... •...
Biomedicine
THE IMMUNE SYSTEM
Copyright CNM – College of Naturopathic Medicine 1
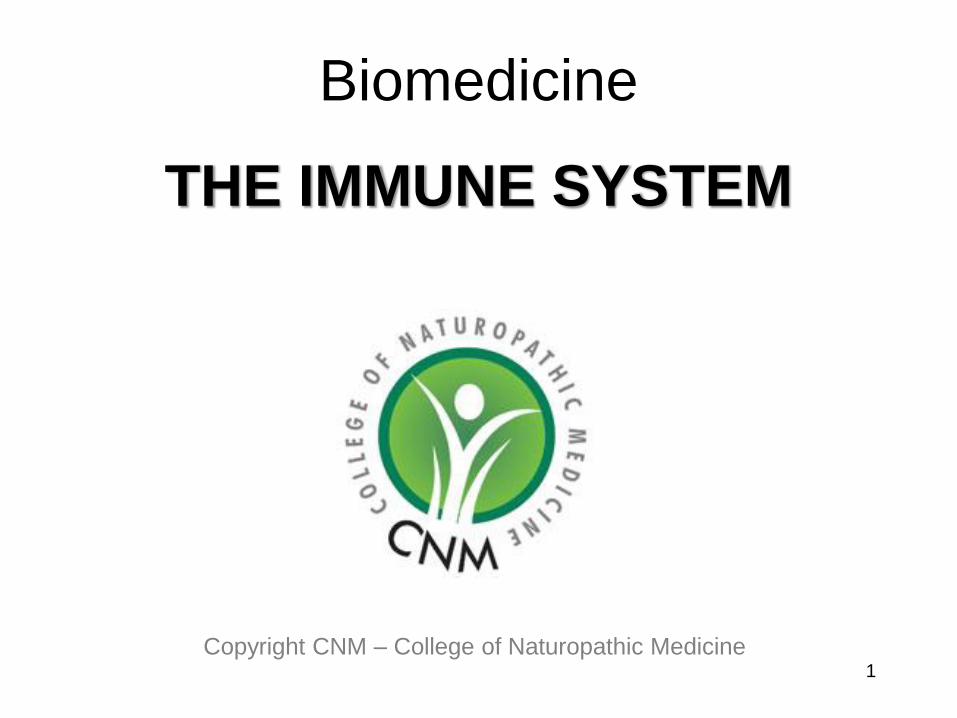
THE IMMUNE SYSTEM The Immune System is a set of protective measures used by the body to defend itself from all kinds of invaders
3 ‘Routes’ of Entry for Pathogens: 1.Respiratory Tract
2.Digestive tract
3.Break in Skin
3 ‘Lines’ Protection providing 2 Main Types of Defence:
1st Line = EXTERNAL = Barriers, Secretions & Excretions
2nd Line = INTERNAL = Antimicrobial Cells, Proteins & Processes (Inflammation & Fever)
3rd Line = INTERNAL & Specialized
Cell & Antibody Mediated
Non-Specific /
Innate Defence
Specific Defence/
Adaptive Immunity
1
2
2
ANTIGENS Def: Any substance that when introduced to the
body, has the POTENTIAL to trigger an Immune Response, especially the production of Antibodies.
Two types:
1. FOREIGN SUBSTANCES (Microbes, Food, Dust, Drugs
etc.)
2. SELF ANTIGEN (present on cell membranes)
http://www.beltina.org/health-dictionary/antigen-antibody-what-are-definition-cancer.html
3
Non-specific Defence Mechanisms
1st Line of Defence
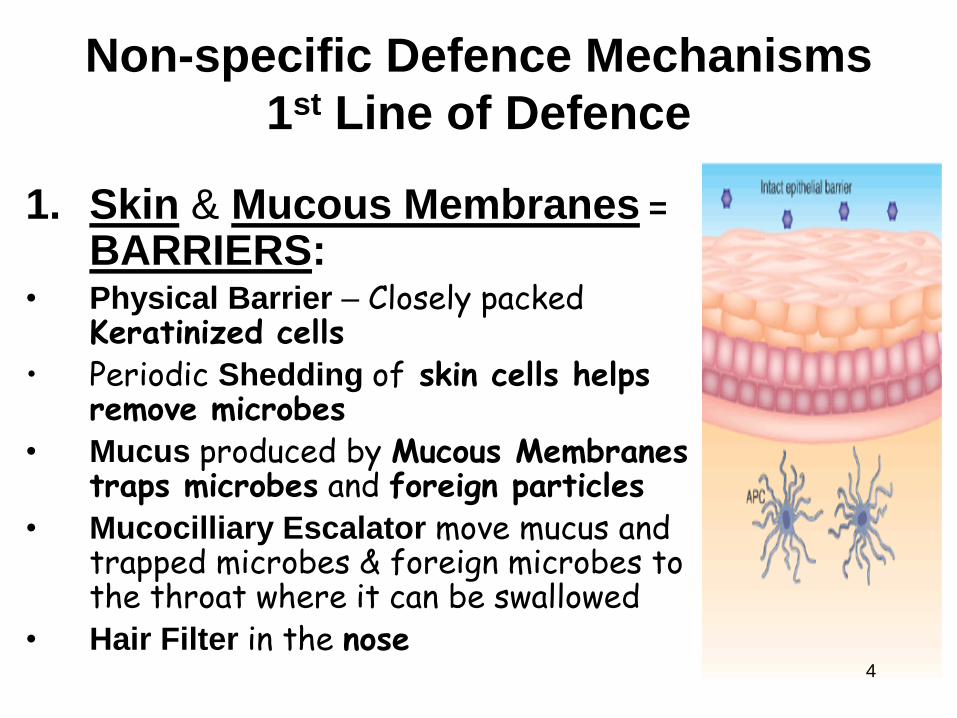
1. Skin & Mucous Membranes =
BARRIERS:
• Physical Barrier – Closely packed Keratinized cells
• Periodic Shedding of skin cells helps remove microbes
• Mucus produced by Mucous Membranes traps microbes and foreign particles
• Mucocilliary Escalator move mucus and trapped microbes & foreign microbes to the throat where it can be swallowed
• Hair Filter in the nose
4
2. ‘FLUIDS/ EXCRETIONS/ SECRETIONS’- Flushing out microbes
• TEARS – Dilute microbes and stops them settling on eye surface
• SALIVA – Cleanses the oral cavity • PERSPIRATION – Helps to flush microbes from skin surface • VAGINAL SECRETIONS – Acidic & Move microbes out of female body • One way flow of URINE & FAECES
• VOMITING and DIARRHOEA – Usually a response to Microbial Toxins
Non-specific Defence Mechanisms
1st Line of Defence
5
Contain
Lysozymes &
Secretory IgA
3. ANTI-MICROBIAL SUBSTANCES
• GASTRIC ACID – Destroys pathogens in swallowed mucus and ingested substances
• SEBUM – Contains Fatty Acids which inhibit microbe growth
• TEARS, SALIVA & PERSPIRATION - Contain Lysozyme, an enzyme that breaks down bacteria
• VAGINAL SECRETIONS – Slightly acidic to discourage bacterial growth
Non-specific Defence Mechanisms
1st Line of Defence
6
These include:
• Internal anti-microbial proteins
• Phagocytes
• Natural killer cells
• Inflammation
• Fever
7
Non-specific Defence Mechanisms INTERNAL Defences:
2nd Line of Defence
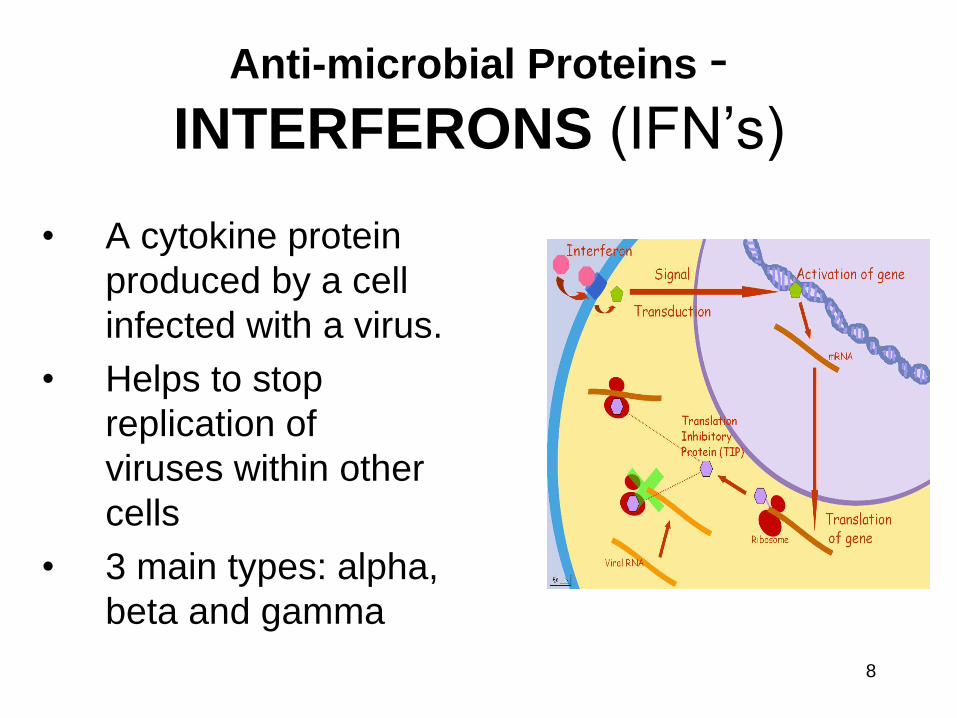
Anti-microbial Proteins -
INTERFERONS (IFN’s)
• A cytokine protein
produced by a cell
infected with a virus.
• Helps to stop
replication of
viruses within other
cells
• 3 main types: alpha,
beta and gamma
8
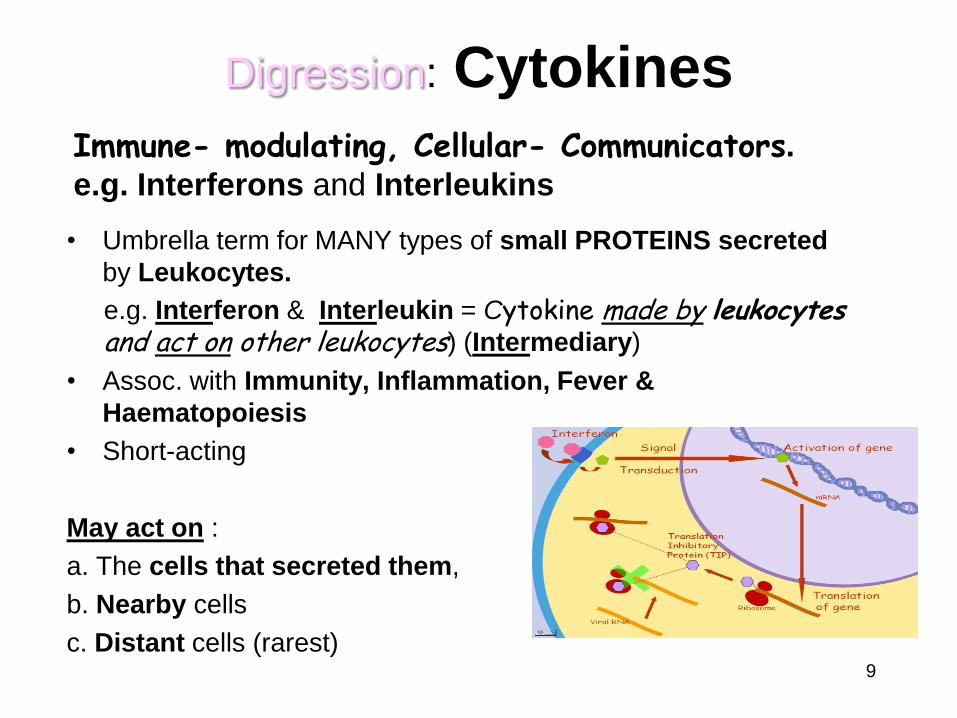
Digression: Cytokines
• Umbrella term for MANY types of small PROTEINS secreted
by Leukocytes.
e.g. Interferon & Interleukin = Cytokine made by leukocytes and act on other leukocytes) (Intermediary)
• Assoc. with Immunity, Inflammation, Fever &
Haematopoiesis
• Short-acting
May act on :
a. The cells that secreted them,
b. Nearby cells
c. Distant cells (rarest)
Immune- modulating, Cellular- Communicators.
e.g. Interferons and Interleukins
9
Anti-microbial Proteins -
COMPLEMENT SYSTEM • A system made of over 30 proteins
produced by the Liver and found circulating around the body.
• Complement proteins are identified by a letter with a number e.g. C3
• Normally inactive but when activated these proteins act in a cascade to ‘complement’ Immune Processes.
• Collectively, complement proteins destroy microbes & promote Immunity by...
– Promoting Phagocytosis
– Contributing to Inflammation
– Causing Cytolysis (bursting) of Microbes
10
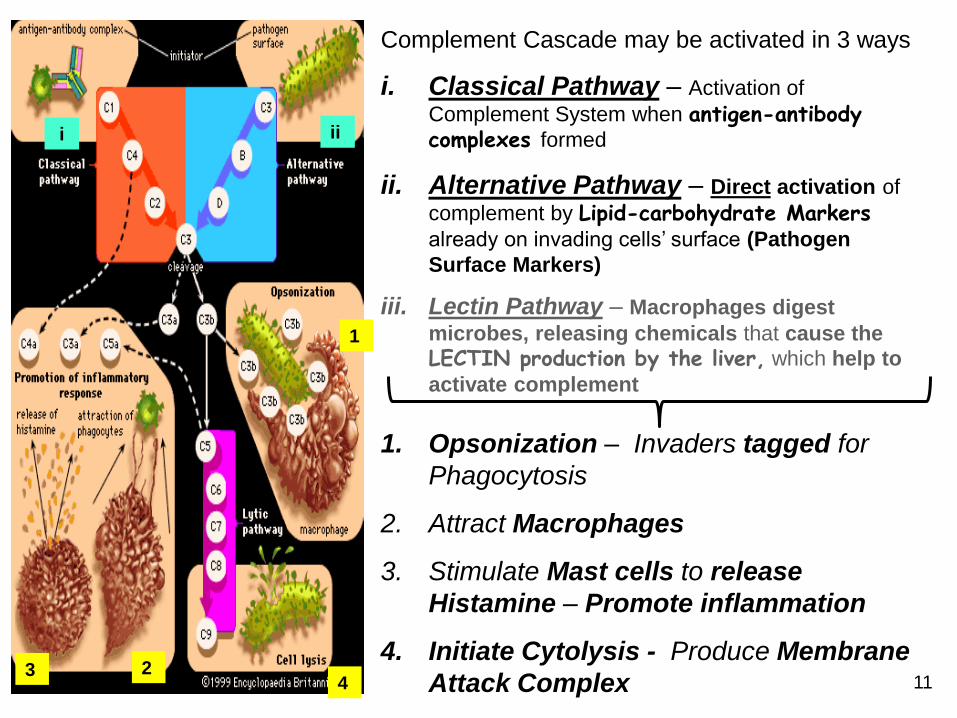
Complement Cascade may be activated in 3 ways
i. Classical Pathway – Activation of
Complement System when antigen-antibody complexes formed
ii. Alternative Pathway – Direct activation of
complement by Lipid-carbohydrate Markers
already on invading cells’ surface (Pathogen
Surface Markers)
iii. Lectin Pathway – Macrophages digest
microbes, releasing chemicals that cause the
LECTIN production by the liver, which help to
activate complement
1. Opsonization – Invaders tagged for
Phagocytosis
2. Attract Macrophages
3. Stimulate Mast cells to release
Histamine – Promote inflammation
4. Initiate Cytolysis - Produce Membrane
Attack Complex
1
2 3 4
i ii
11
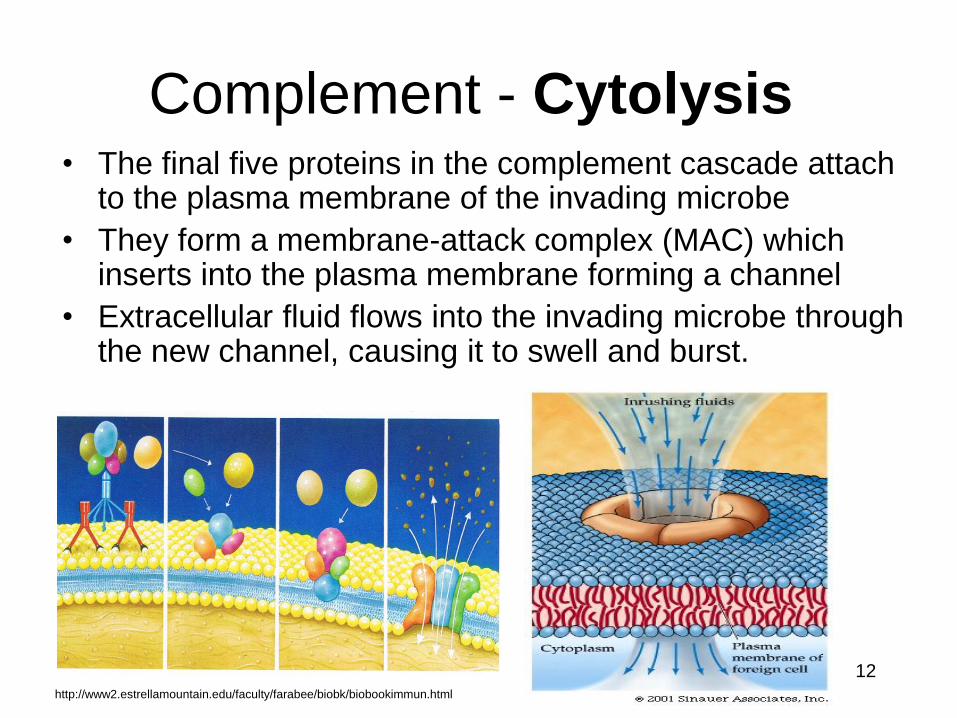
Complement - Cytolysis • The final five proteins in the complement cascade attach
to the plasma membrane of the invading microbe
• They form a membrane-attack complex (MAC) which inserts into the plasma membrane forming a channel
• Extracellular fluid flows into the invading microbe through the new channel, causing it to swell and burst.
12 http://www2.estrellamountain.edu/faculty/farabee/biobk/biobookimmun.html
Anti-microbial Proteins -
TRANSFERRINS • Iron-binding proteins
that inhibit the growth
of certain bacteria by
inhibiting the
available iron that
they need for growth
• Creates an
environment low in
iron by binding iron -
Bacteria cannot
survive 13
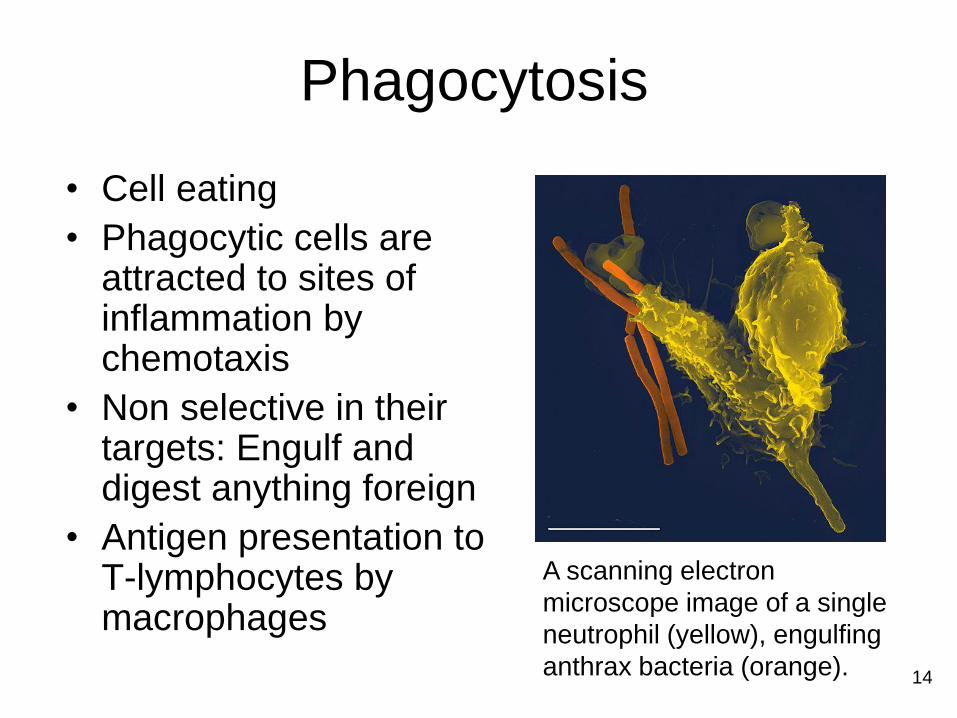
Phagocytosis
• Cell eating
• Phagocytic cells are attracted to sites of inflammation by chemotaxis
• Non selective in their targets: Engulf and digest anything foreign
• Antigen presentation to T-lymphocytes by macrophages
A scanning electron
microscope image of a single
neutrophil (yellow), engulfing
anthrax bacteria (orange).
14
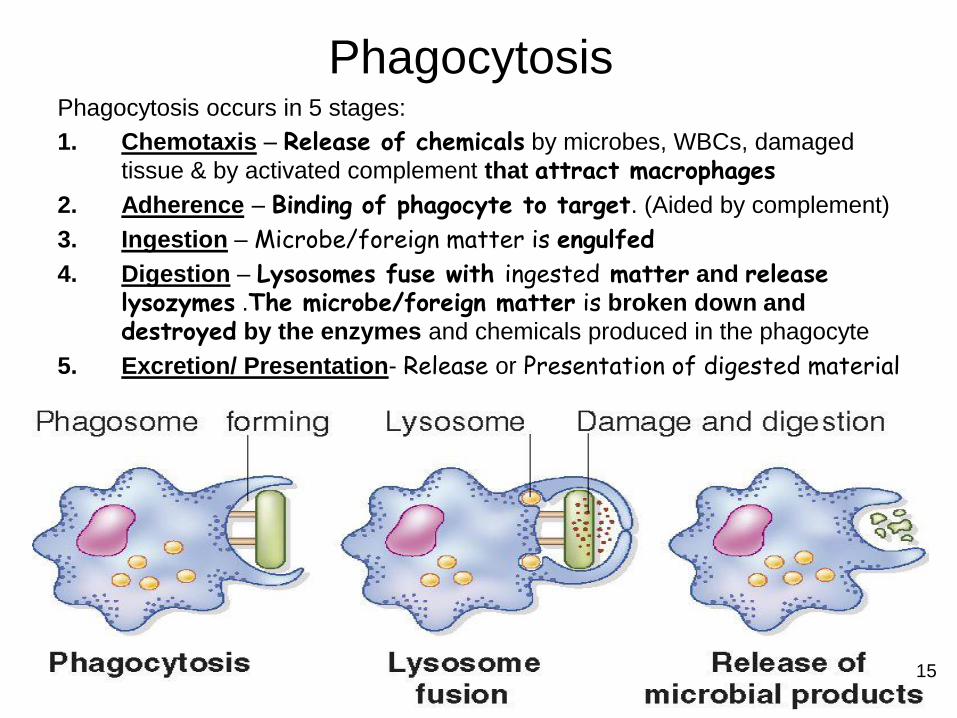
Phagocytosis Phagocytosis occurs in 5 stages:
1. Chemotaxis – Release of chemicals by microbes, WBCs, damaged
tissue & by activated complement that attract macrophages
2. Adherence – Binding of phagocyte to target. (Aided by complement)
3. Ingestion – Microbe/foreign matter is engulfed
4. Digestion – Lysosomes fuse with ingested matter and release lysozymes .The microbe/foreign matter is broken down and
destroyed by the enzymes and chemicals produced in the phagocyte
5. Excretion/ Presentation- Release or Presentation of digested material
15
PHAGOCYTES
• Specialised cells that Engulf and digest anything foreign (cellular and foreign material).
• The two major types are Macrophages (Monocytes in Blood) and Neutrophils, which migrate to an infected area
• Some other kinds of phagocytes are Fixed such as:
Histiocytes (Connective tissue),
Kupffer cells (Liver)
Alveolar Macrophages (Lungs),
Microglia (Nervous tissue)
Tissue Macrophages (Spleen, Bone marrow & Lymph Nodes)
Langerhans Cells (Skin) Antigen-presenting Cells -process & present antigens to T-cells.
16
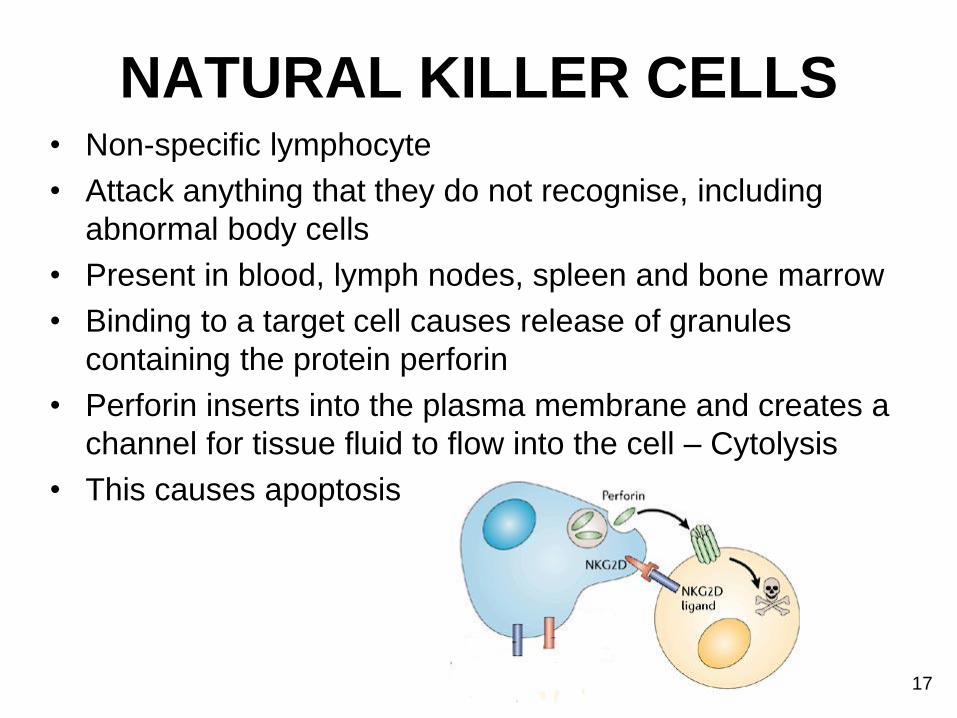
NATURAL KILLER CELLS • Non-specific lymphocyte
• Attack anything that they do not recognise, including
abnormal body cells
• Present in blood, lymph nodes, spleen and bone marrow
• Binding to a target cell causes release of granules
containing the protein perforin
• Perforin inserts into the plasma membrane and creates a
channel for tissue fluid to flow into the cell – Cytolysis
• This causes apoptosis
17
Summary Type of
defence
Interferons Complement Transferrins NK cells Phagocytes
Cell or
Protein?
How does
it work?
What does
it attack?
18
INFLAMMATION
Non- specific immune defence to tissue damage
Causes of inflammation:
• Pathogens
• Abrasions
• Chemicals
• Cells distortion or disturbance
• Extreme temperatures
19
The Inflammatory Response
Clinical signs of inflammation:
- Redness (rubor)
- Heat (calor)
- Pain (dolor)
- Swelling (tumor)
- Loss of function
20
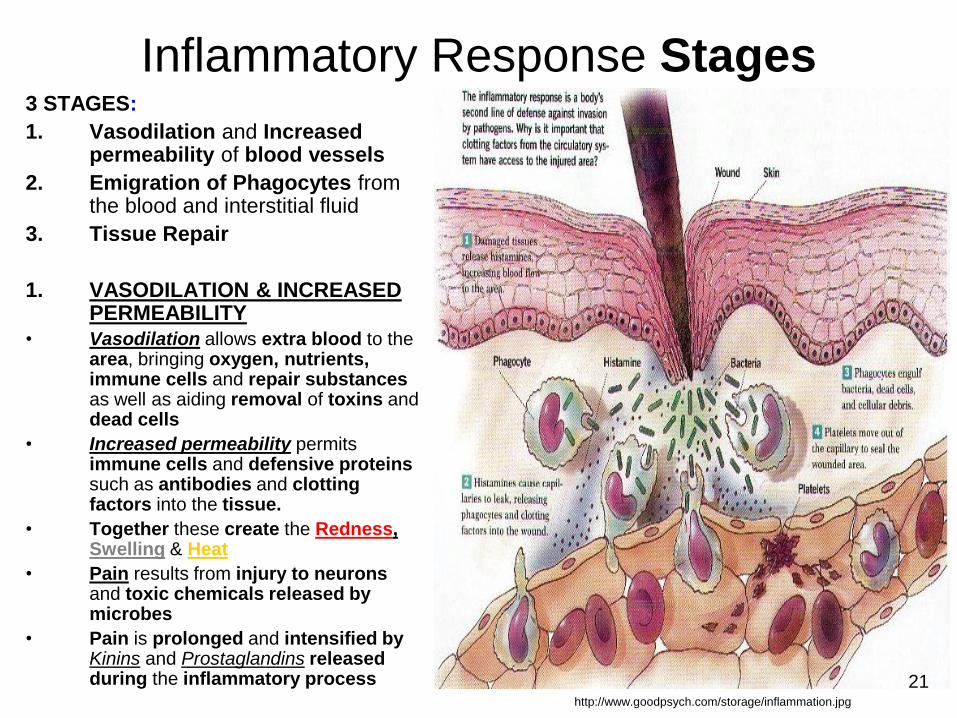
Inflammatory Response Stages 3 STAGES:
1. Vasodilation and Increased permeability of blood vessels
2. Emigration of Phagocytes from the blood and interstitial fluid
3. Tissue Repair
1. VASODILATION & INCREASED PERMEABILITY
• Vasodilation allows extra blood to the area, bringing oxygen, nutrients, immune cells and repair substances as well as aiding removal of toxins and dead cells
• Increased permeability permits immune cells and defensive proteins such as antibodies and clotting factors into the tissue.
• Together these create the Redness, Swelling & Heat
• Pain results from injury to neurons and toxic chemicals released by microbes
• Pain is prolonged and intensified by Kinins and Prostaglandins released during the inflammatory process
http://www.goodpsych.com/storage/inflammation.jpg
21
2. EMIGRATION OF PHAGOCYTES
• Within an hour of initial inflammation
• numbers of WBC migrate to site due to Chemotaxis
• Neutrophils are first on the scene, followed by monocytes (in blood) and
macrophages (in tissues). • Dead phagocytes accumulate as pus PUS = Dead Phagocytes (N), cell debris, fibrin,
inflammatory exudate and living and dead microbes
3.TISSUE REPAIR 22
Substances which contribute to inflammation
1. Histamine - Released in response to injury by mast cells and basophils
2. Leukotrienes - Released by basophils and mast cells. Attract phagocytes and aid adherence of phagocytes to pathogens
3. Kinins – Induce vasodilation and increased permeability. Attract phagocytes. Example: Bradykinin
4. Prostaglandins - Released by damaged cells. Enhance effects of histamine and kinins as well as stimulating emigration of phagocytes
5. Complement system – See before
INFLAMMATORY
MEDIATORS
23
Benefits of Inflammation 1. Promotion of Phagocytosis – Phagocytic cells are attracted by
Chemotaxis and the Temperature (caused by inflammation)
promotes their activity
2. Promotion of Immune Response – Protective proteins such as
Antibodies can leave blood stream and enter the tissues as blood
vessels become more permeable
3. Toxin Dilution – Accumulation of Fluid dilutes damaging toxins
and waste materials
4. Fibrin Formation – Damaged cells promote the formation of a
fibrin network. This can...
• WALL OFF the inflamed area preventing
spread of infection
• Help BIND wound edges during healing
Some bacteria such as Streptococcus pyrogenes (tonsillitis, pharyngitis,
some skin infections) can break down fibrin so that the infection can
spread.
24
Harmful Effects
of inflammation
1. SWELLING- In a confined space, can cause severe Pain due to
Pressure on nerves. Can Also be DANGEROUS (ICP)
2. PAIN - Occurs when swelling compresses the Sensory Nerve
endings and as a Reaction to Chemical Mediators
like Bradykinin, Prostaglandins etc.
3. SUPPURATION / PUS FORMATION
PUS = Dead Phagocytes, Dead cells, Debris, Fibrin, Inflammatory Exudate & living/dead Microbes.
Main Cause = Staphylococcus aureus &
Streptococcus pyrogenes
4. ABSCESS FORMATION = Localized, Painful
accumulation of Pus, surrounded by Inflamed Tissue
5. ATHEROSCLEROSIS
6. ADHESIONS & SCAR TISSUE
Larynx
25
ABSCESSES SUPERFICIAL ABSCESSES tend to Rupture
through the skin and Discharge pus
DEEP SEATED ABSCESSES can...
1. Rupture through the skin
2. Rupture with minimal discharge - developing a Chronic
Abscess with an infected open channel or Sinus
3. Rupture & Discharge pus into an adjacent organ forming a
Fistula = an infected channel open at both ends.
4. Become enclosed by Fibrous Tissue becoming a source of further
infection
5. Form Adhesions
6. Cause Shrinkage of fibrous tissues
7. Heal
A pilonidal sinus
is a small hole or
tunnel in the skin,
usually at the very
top of the cleft
between the
buttocks 26
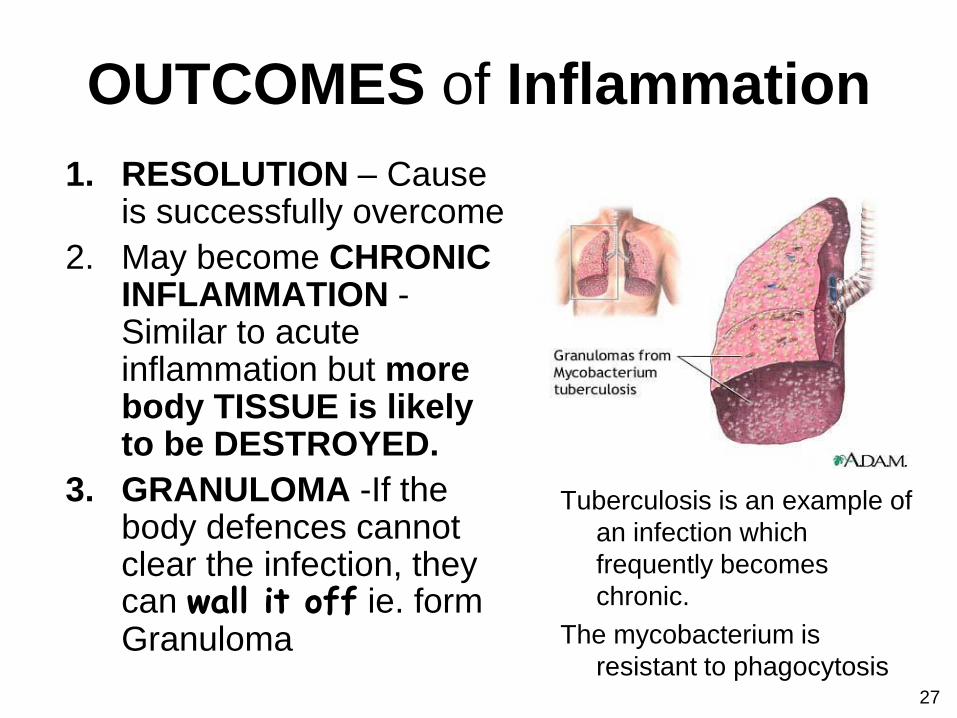
OUTCOMES of Inflammation
1. RESOLUTION – Cause is successfully overcome
2. May become CHRONIC INFLAMMATION - Similar to acute inflammation but more body TISSUE is likely to be DESTROYED.
3. GRANULOMA -If the body defences cannot clear the infection, they can wall it off ie. form Granuloma
Tuberculosis is an example of
an infection which
frequently becomes
chronic.
The mycobacterium is
resistant to phagocytosis 27
4. FIBROSIS- Scar Tissue Formation Occurs in healing when:
- There is loss of tissue
- Cells don‘t regenerate
- Can be a result of chronic inflammation
Scar tissue consists of collagen fibres
secreted by Fibroblasts
It can have Damaging Effects like...
1. Adhesions
2. Fibrosis of Thrombus or embolus blocking a blood vessel
3. Tissue shrinkage Tissue shrinkage after
a burn
OUTCOMES of Inflammation
Adhesions can cause problems such as Infertility & Intestinal obstruction
28
FEVER
• Abnormally high body temperature
• Occurs because the hypothalamus thermostat is reset
• Common in infection/inflammation
• Can be triggered by bacterial toxins which cause macrophages to release fever causing chemical called cytokines. One example is interleukin-1
• High body temperature: – Makes interferons more effective
– Inhibits growth of some microbes
– Speeds up the reactions that aid repair 29
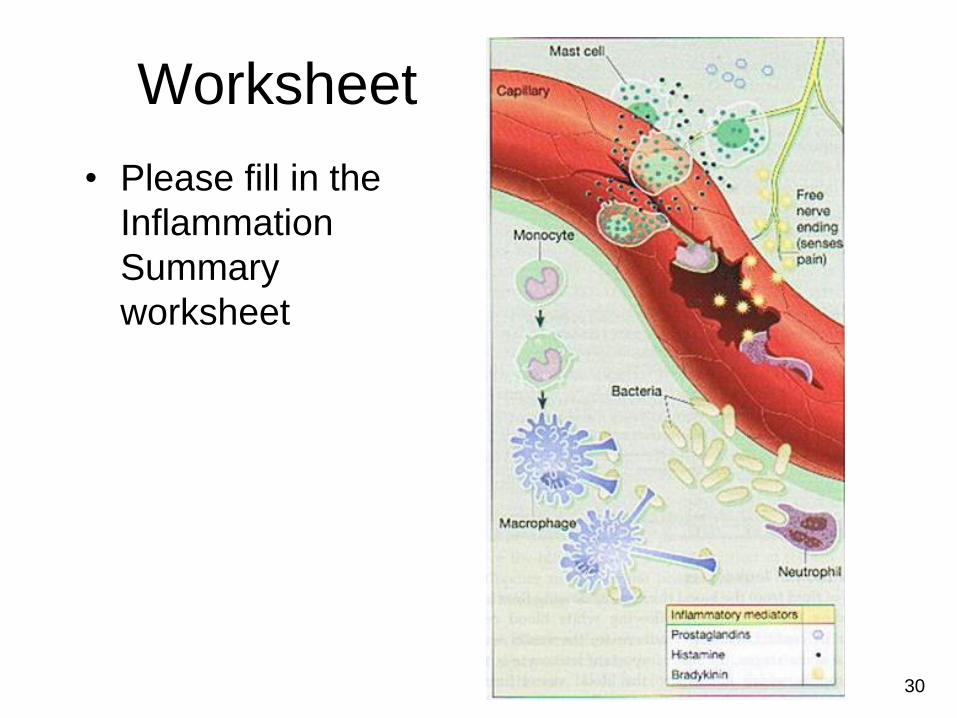
Worksheet
• Please fill in the
Inflammation
Summary
worksheet
30

Cells of the Immune System
31
Cells of the Immune System
• Basophils and Mast cells - Chemotaxic
• Eosinophils – Protect against large microbes
such as parasites and worms
• Neutrophils - Protect against foreign
invaders
• Monocytes and Macrophages - Produce
interleukin which promotes fever, globulin
production and T-cell activation.
• Lymphocytes - T and B cells and NK Cells.
Part of specific immunity
32
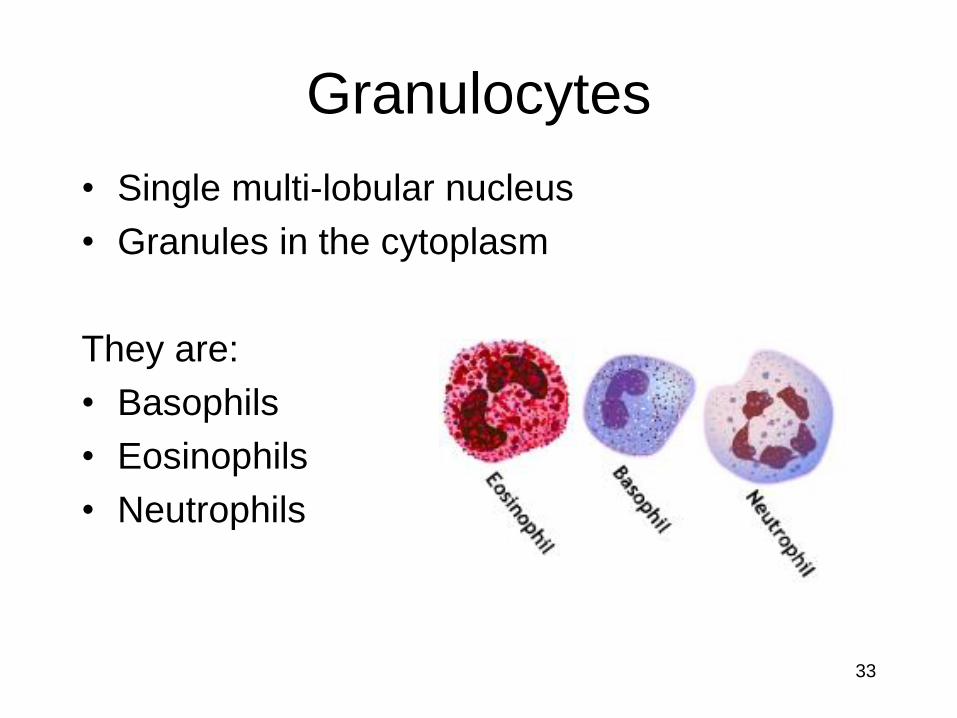
Granulocytes
• Single multi-lobular nucleus
• Granules in the cytoplasm
They are:
• Basophils
• Eosinophils
• Neutrophils
33

Basophils & Mast Cells
• Contain Heparin (anticoagulant) + Histamine (vasodilator) and other things that promote inflammation (Leukotrienes & Cytokines).
• Not phagocytic
• In Blood = Basophil
• In Tissue = Mast cells
• Anaphylaxis- Basophils have IgE protein receptors on their cell surface that bind IgE antibody very tightly.
Increasing Inflammation!
•Yobos of the immune system = Inflame the situation!
34
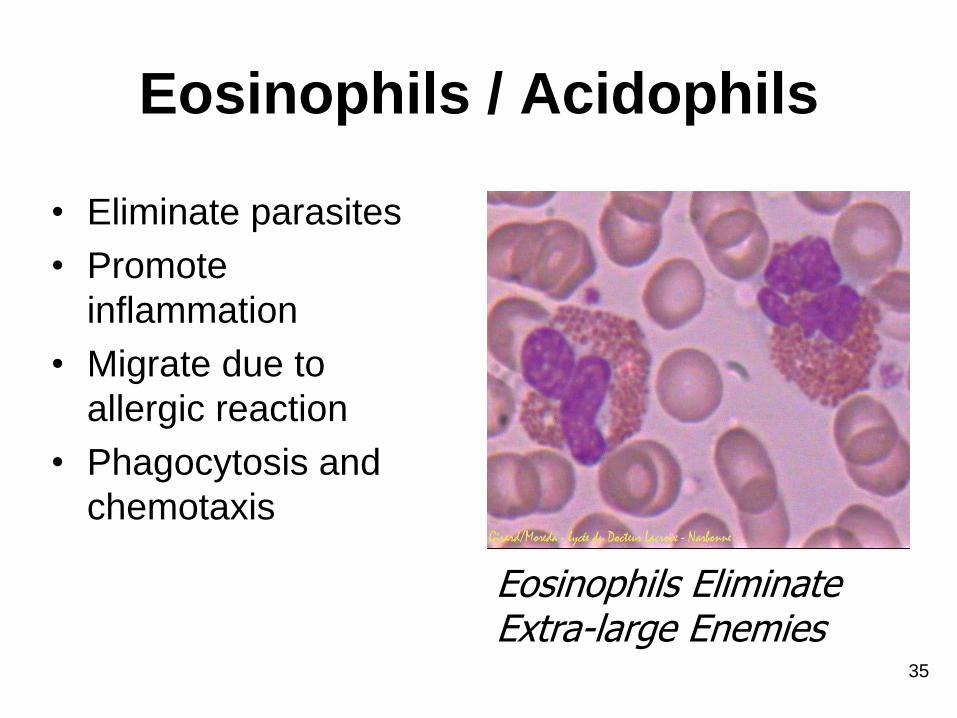
Eosinophils / Acidophils
• Eliminate parasites
• Promote
inflammation
• Migrate due to
allergic reaction
• Phagocytosis and
chemotaxis
Eosinophils Eliminate Extra-large Enemies
35
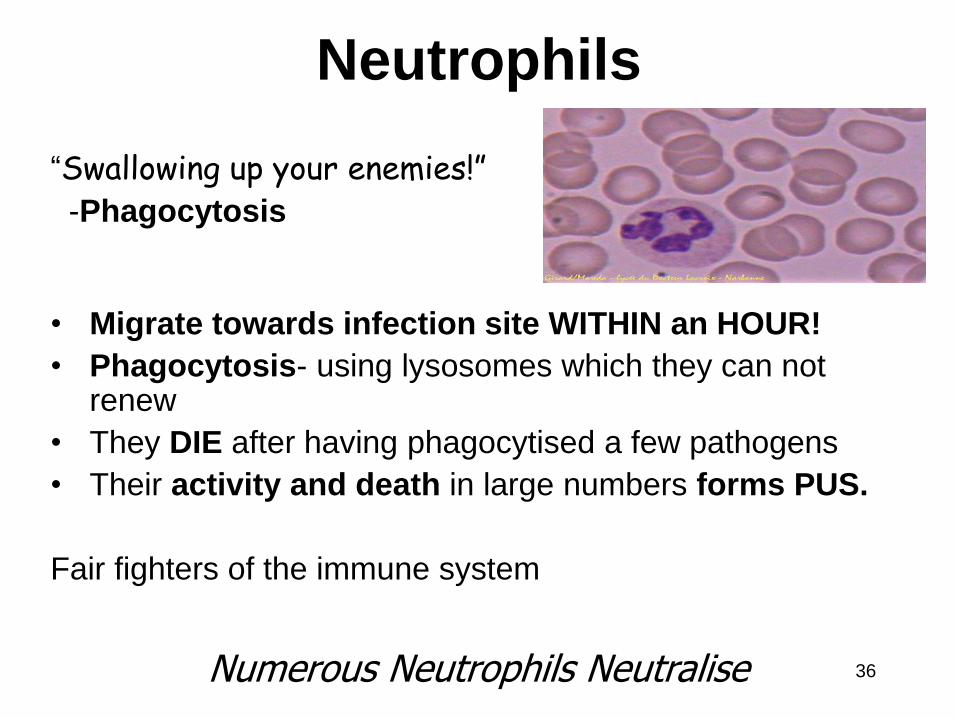
Neutrophils
“Swallowing up your enemies!” -Phagocytosis
• Migrate towards infection site WITHIN an HOUR!
• Phagocytosis- using lysosomes which they can not renew
• They DIE after having phagocytised a few pathogens
• Their activity and death in large numbers forms PUS.
Fair fighters of the immune system
Numerous Neutrophils Neutralise 36
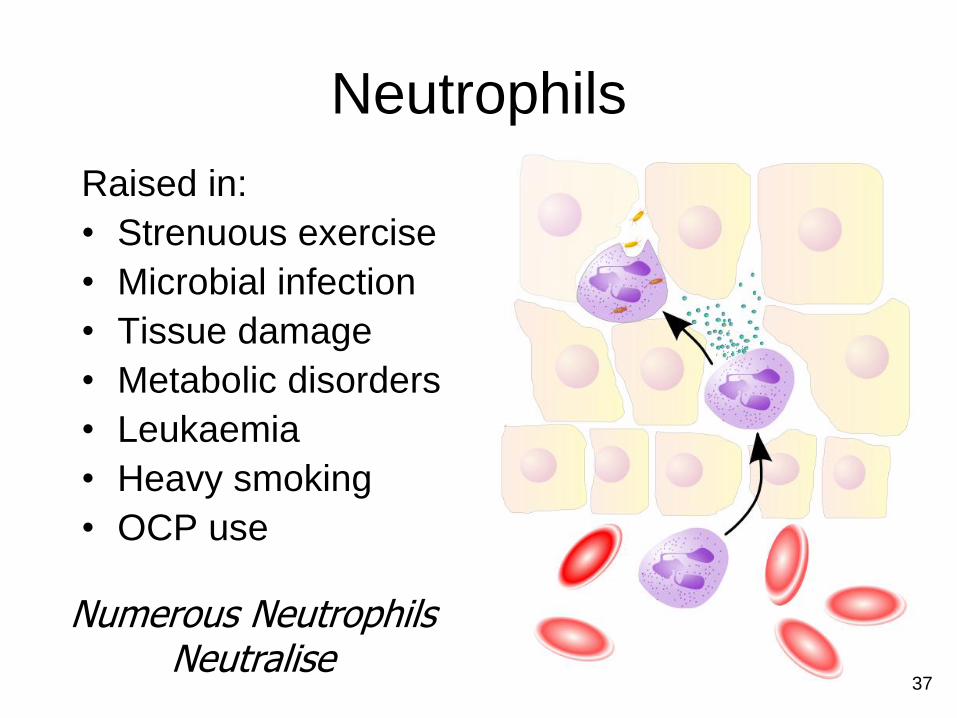
Neutrophils
Raised in:
• Strenuous exercise
• Microbial infection
• Tissue damage
• Metabolic disorders
• Leukaemia
• Heavy smoking
• OCP use
Numerous Neutrophils Neutralise
37

Agranulocytes:
Monocytes & Macrophages
• In Blood: Monocytes
• In Tissue: Macrophages
• Form: – Kupffer cells
– Microglia
– Langerhans Cells
– Peyer's Patches etc.
• Both Monocytes/Macrophages secrete Cytokines e.g. Interleukin 1
1. Induce Fever
2. Produce Globulins
3. Activate T-cell
38

RECALL: Cytokines
• General name for MANY types of small PROTEINS
secreted by Leukocytes.
• e.g. Interleukin = Cytokine made by leukocytes and act on other leukocytes) (Intermediary)
• Assoc. with Immunity, Inflammation, Fever &
Haematopoiesis
• Short-acting
• May act on :
a. The cells that secreted them,
b. Nearby cells
c. Distant cells (rarest)
Immune- modulating, Cellular- Communicators.
e.g. Interferons and Interleukins
39
Monocytes & Macrophages
Monocytes • Large, phagocytic
• Mono-nuclear, no lobes
• Some become macrophages
• Increased with microbial infection
Macrophages • Protection! (Defence) via Phagocytosis &
• Isolating dangers (Walling off)
• Release cytokines (inflammatory signals)
• Immune system- Stimulate lymphocytes &
other immune cells to respond to the pathogen.
(Innate Immunity)
• Inflammation
• Repair & Clean up Police Patrols – Protect, Prevent,
“Pick up the Pieces” 40
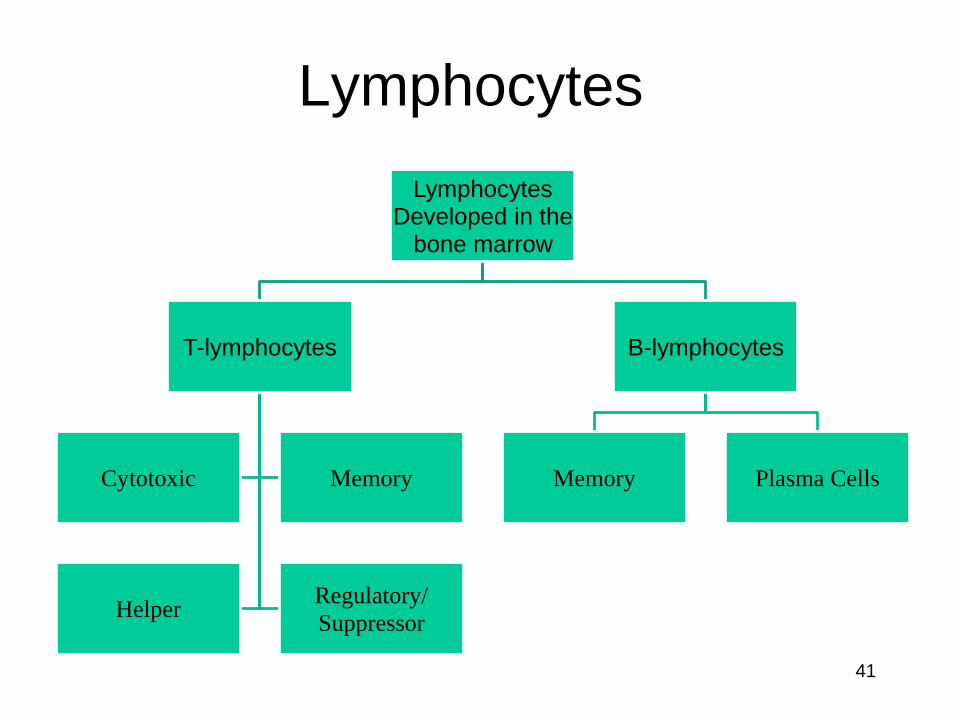
Lymphocytes
Lymphocytes Developed in the
bone marrow
T-lymphocytes
Cytotoxic Memory
Helper Regulatory/
Suppressor
B-lymphocytes
Memory Plasma Cells
41
B & T Cells
• IMMUNOCOMPETENT
– They learn to respond to Antigens
(foreign material)
– They learn to respond to Immune Labels
1. Possess specificity for antigens: Recognise self
from non-self molecules (Each B cell and T cell is
specific for a particular antigen. So each is able to
bind to a particular molecular structure.
2. Possess memory for previously encountered
Antigens: They can mount a greater attack next time.
T-Lymphocyte
42
B & T Cells
• T cells are made in the Bone marrow
and mature in the Thymus
• Most T cells arise before puberty but continue to
mature and leave the Thymus throughout life
• The 2 Major types of T Cells:
T-helper 1 (Th1) - Involved in Cell Mediated Immunity
T-helper 2 (Th2) - Involved in Antibody Mediated Immunity
The balance between the 2 is maintained
by Another type of T Cell = Regulatory T Cells / Suppressor T
Cell.
• B cells are made in the Bone marrow and mature
continually (mostly in Bone Marrow).
B-Lymphocyte
43
B and T cells
T-lymphocytes
• Made in Bone marrow.
• Processed ( & mature) in the Thymus (Lymphoid
Organ)
• Numerous in Lymph nodes
• Attack Antigens: Cell Mediated Immunity
• Antibody mediated too
B-lymphocytes
• Made in Bone marrow.
• Processed in the Bone marrow
• Mature in Lymph organs (Bone marrow, Lymph nodes & Lymph Glands)
• Numerous in Lymph nodes
• Produce Antibodies (Immunoglobulins): Antibody mediated immunity
44
SELF TOLERANCE
& SELF RECOGNITION
• To function properly, T cells must be able to recognise the body’s own Immune Labels (Self-Recognition) and own Proteins (Self-Tolerance)
• They learn how to do this in the Thymus
• T-cells that don’t display proper self recognition (immune labels) and self tolerance (proteins) are deleted or inactivated
• Only about 1-5% of T-cells make it through the screening process!
• B cell also have to be self tolerant so they undergo a similar screening process in the Bone marrow
45
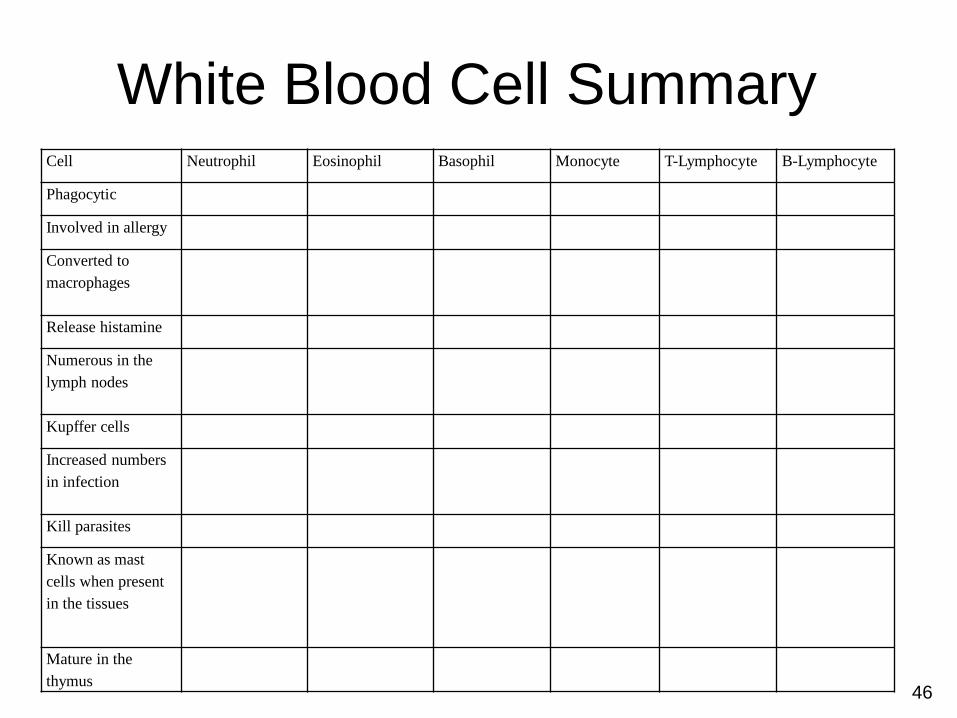
White Blood Cell Summary Cell Neutrophil Eosinophil Basophil Monocyte T-Lymphocyte B-Lymphocyte
Phagocytic
Involved in allergy
Converted to
macrophages
Release histamine
Numerous in the
lymph nodes
Kupffer cells
Increased numbers
in infection
Kill parasites
Known as mast
cells when present
in the tissues
Mature in the
thymus 46

Specific Defence =
Adaptive Immunity Mediated (brought about) by B & T-lymphocytes
1. CELL-MEDIATED IMMUNITY: (T- Lymphocytes)
Immunity provided via (production of) Cytotoxic T cells/
Killer T cells
Defence against Intra-cellular Pathogens, Cancer Cells and
Transplants
2. ANTIBODY-MEDIATED/ HUMORAL IMMUNITY:
(mainly B- Lymphocytes)
Immunity provided via Antibodies (Immunoglobulins)
Defence against extra- cellular Pathogens 47
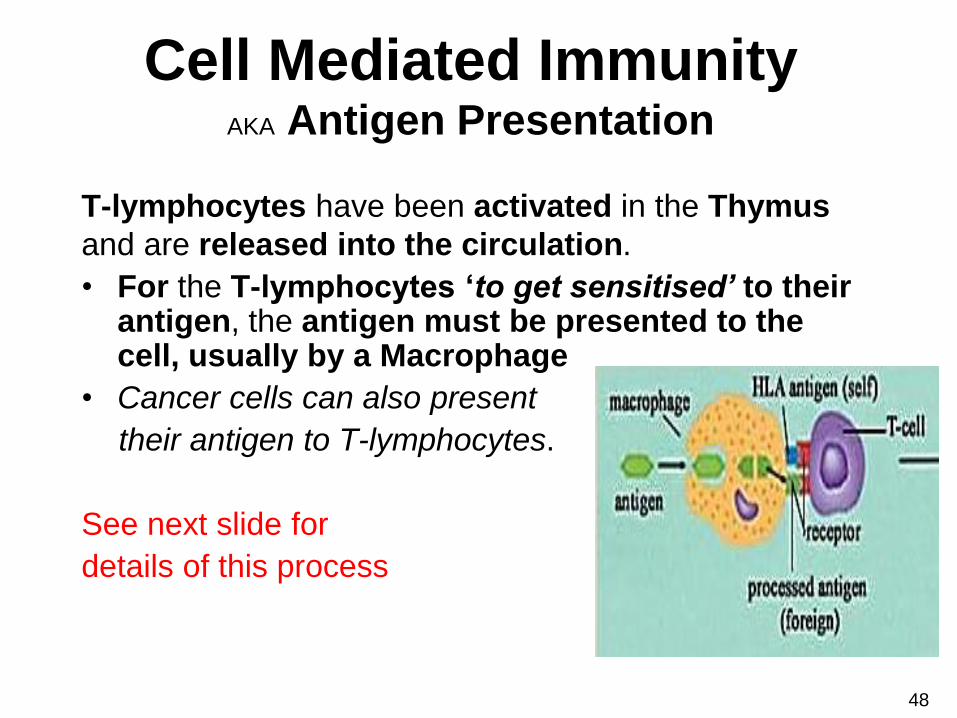
Cell Mediated Immunity AKA Antigen Presentation
T-lymphocytes have been activated in the Thymus
and are released into the circulation.
• For the T-lymphocytes ‘to get sensitised’ to their antigen, the antigen must be presented to the cell, usually by a Macrophage
• Cancer cells can also present
their antigen to T-lymphocytes.
See next slide for
details of this process
48

1. A T-cell (TH-1) doesn’t recognise an antigen in
the body (Because antigen doesn’t fit into T-Cell receptor) until it is
presented to it. Active T-cells have to be ‘sensitized’
to the antigen.
2. & 3. So, Antigen- presenting / Dendritic /
Phagocytic cells engulf the antigen and then use
enzymes to break the antigen into fragments
(process the antigen). Some antigen fragments are combined with
Human Leukocyte Antigen Molecules (HLA)
4. These fragments are then displayed on the
phagocytic cells’ surface and presented to a T-
lymphocyte which can now recognise the
antigen
5. The T-lymphocyte binds onto the antigen and
releases IL-2.
6. This then initiates the T-lymphocyte to
proliferate and differentiate into Cytotoxic/killer,
Memory and Helper T-cells (Clonal Selection)
49
Diversion: Interleukin-2
• = Cytokine
• Produced by a leukocyte, acting on a
leukocyte
• Causes growth, proliferation & activation
of NK cells, T and B cells
• Produced by T-helper cells when they bind
to an antigen
50
CLONAL SELECTION
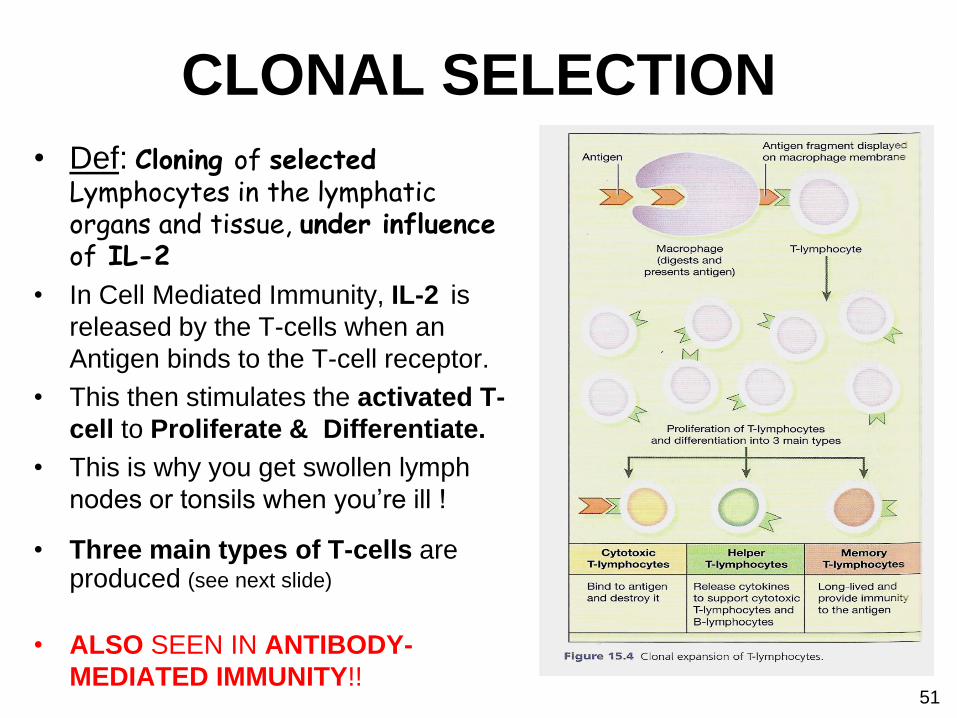
• Def: Cloning of selected Lymphocytes in the lymphatic organs and tissue, under influence of IL-2
• In Cell Mediated Immunity, IL-2 is
released by the T-cells when an
Antigen binds to the T-cell receptor.
• This then stimulates the activated T-
cell to Proliferate & Differentiate.
• This is why you get swollen lymph
nodes or tonsils when you’re ill !
• Three main types of T-cells are produced (see next slide)
• ALSO SEEN IN ANTIBODY-
MEDIATED IMMUNITY!!
51
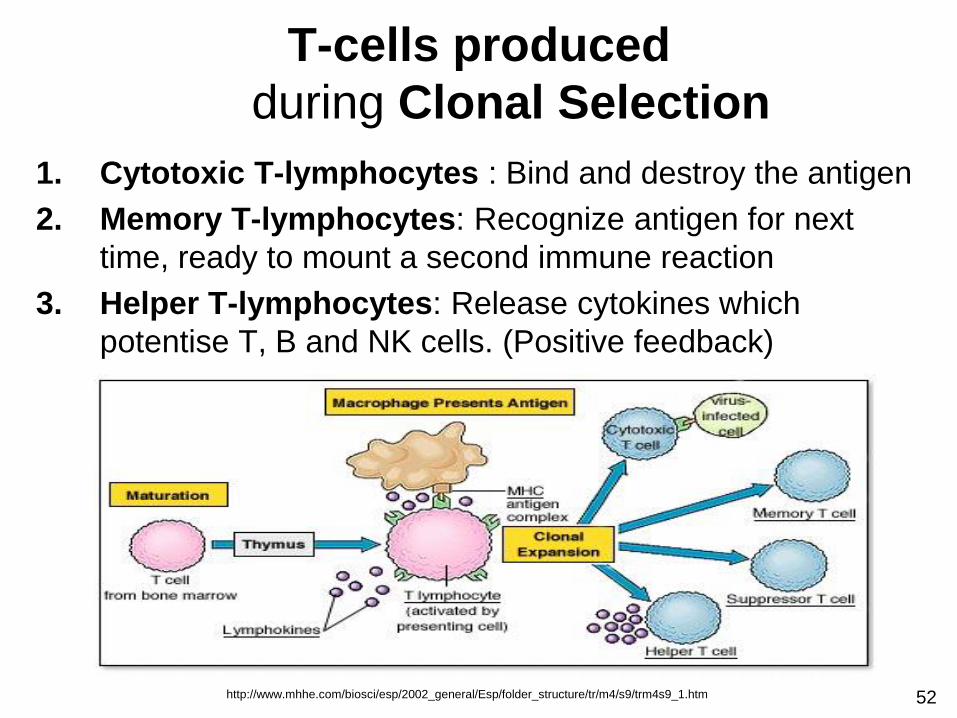
1. Cytotoxic T-lymphocytes : Bind and destroy the antigen
2. Memory T-lymphocytes: Recognize antigen for next
time, ready to mount a second immune reaction
3. Helper T-lymphocytes: Release cytokines which
potentise T, B and NK cells. (Positive feedback)
52
T-cells produced
during Clonal Selection
http://www.mhhe.com/biosci/esp/2002_general/Esp/folder_structure/tr/m4/s9/trm4s9_1.htm
53
Specialized, subpopulation of T cells which send messages to and so "de-activate" the other immune cells (T-Helper, B Cells & Macrophages) when an immune response is no longer required.
Thereby maintain immune system homeostasis and tolerance to self-antigens.
Without the Regulatory T cells, the body would continue trying to fight off a disease that no longer exists (and eventually would end up fighting its own cells).
This is an important regulatory, "self-check“ mechanism built into the immune system to prevent excessive reactions
Regulatory T Cells (Tregs ) (Formerly Suppressor T Cells)
Worksheet
• Please fill in your Cell Mediated Immunity
worksheet
54

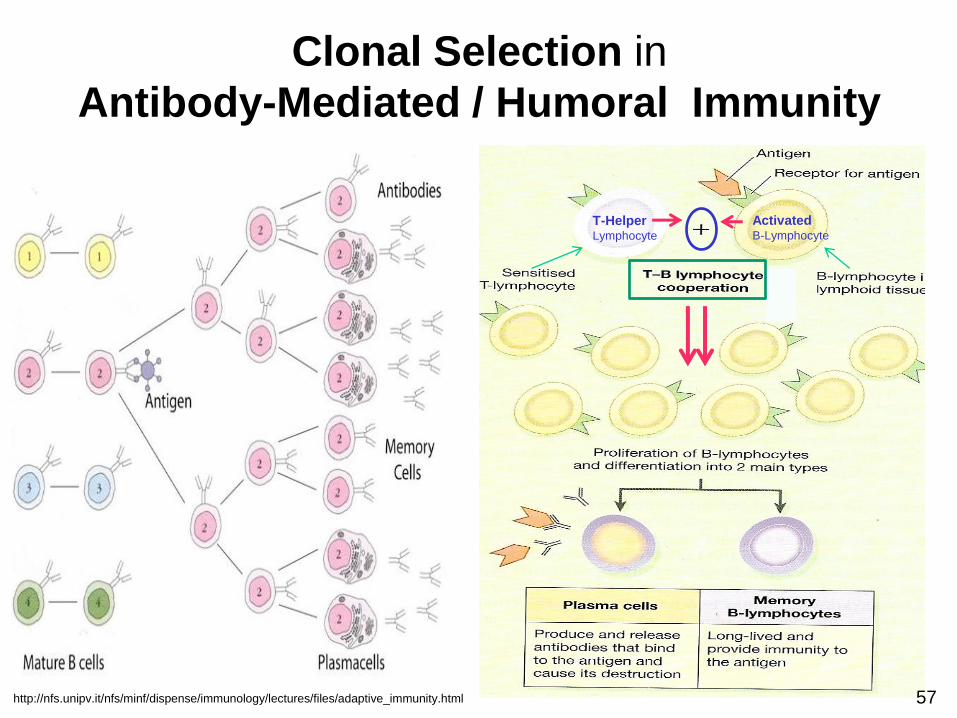
Mediated by B cells • B-lymphocytes are fixed in
lymphoid tissue (Spleen and Lymph Nodes).
• They can recognise and bind antigens without prior presentation.
• Once the B-lymphocyte has bonded to an antigen, a Helper T-lymphocyte stimulates it (Activates it by releasing IL-2) to enlarge then Divide, Proliferate & Differentiate
• CLONAL SELECTION!!
http://dev.nsta.org/evwebs/1887/immune%20system.JPG 55
Antibody-Mediated Immunity (Humoral Immunity)
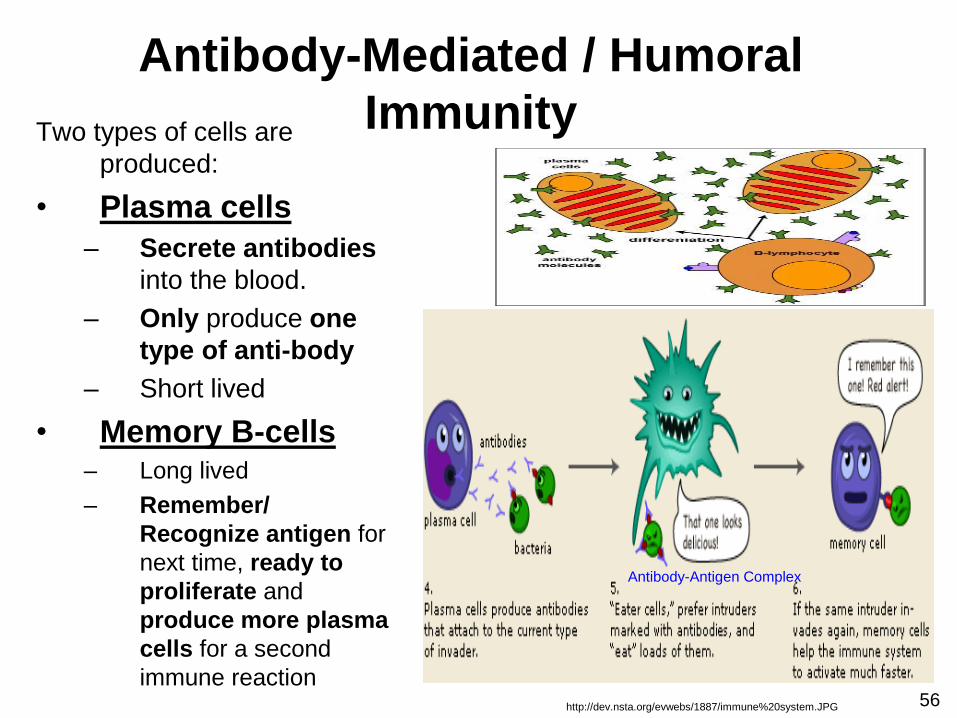
Two types of cells are
produced:
• Plasma cells
– Secrete antibodies
into the blood.
– Only produce one
type of anti-body
– Short lived
• Memory B-cells – Long lived
– Remember/
Recognize antigen for
next time, ready to
proliferate and
produce more plasma
cells for a second
immune reaction
Antibody-Mediated / Humoral
Immunity
Antibody-Antigen Complex
http://dev.nsta.org/evwebs/1887/immune%20system.JPG 56
T-Helper Lymphocyte
Activated B-Lymphocyte
57
Clonal Selection in
Antibody-Mediated / Humoral Immunity
http://nfs.unipv.it/nfs/minf/dispense/immunology/lectures/files/adaptive_immunity.html
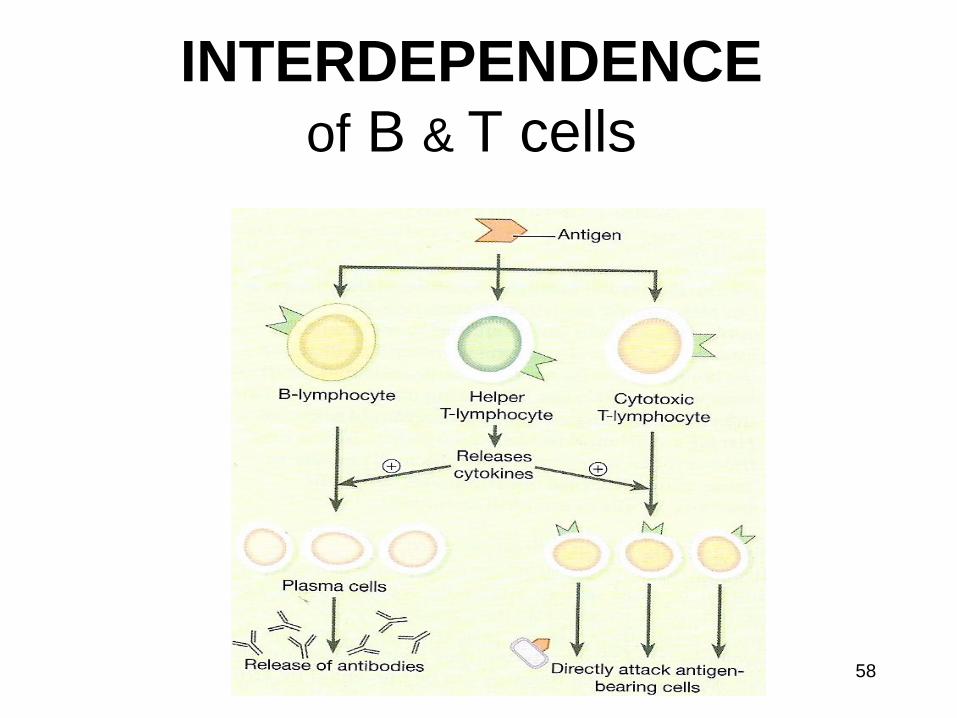
INTERDEPENDENCE
of B & T cells
58
Worksheet
• Please fill in your Antibody Mediated/
Humoral Immunity Worksheet
59
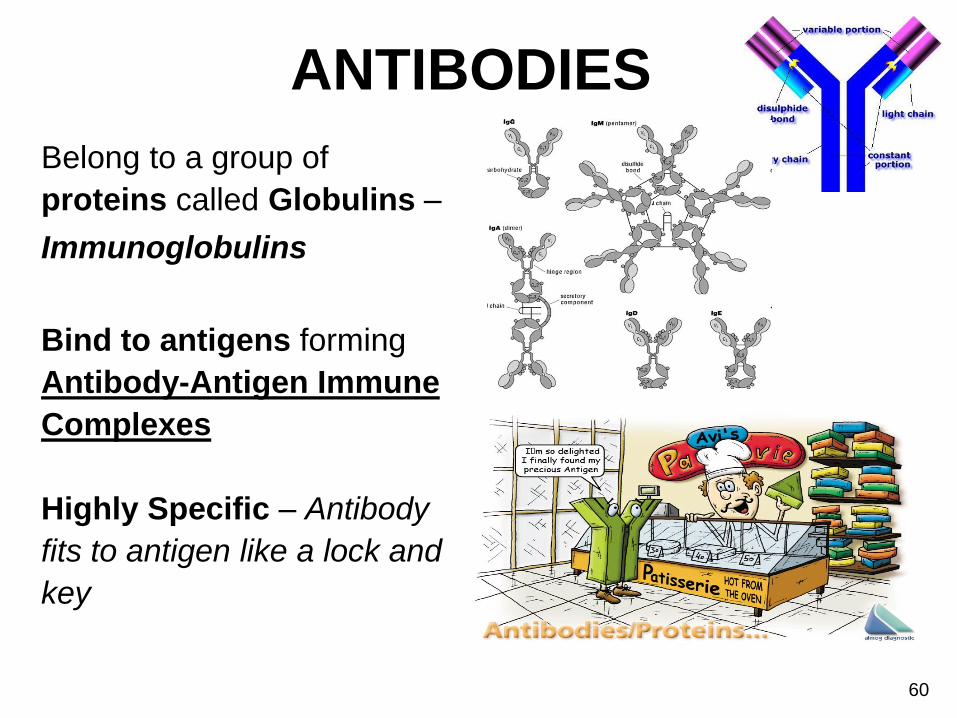
ANTIBODIES
Belong to a group of
proteins called Globulins –
Immunoglobulins
Bind to antigens forming
Antibody-Antigen Immune
Complexes
Highly Specific – Antibody
fits to antigen like a lock and
key
60

1. Neutralising – Neutralise Bacterial TOXINS or prevent viral attachment to cells
2. Immobilising – Bind to antigens on bacterial cilia or flagella
3. Agglutinating & Precipitating – Cause antigen carrying matter to clump together /become insoluble making it easier to for phagocytic cells to engulf
ANTIBODY CLASSES
61
Binding of Antibodies to Antigens inactivates Antigens by:
1 3 3
http://www.austincc.edu/apreview/EmphasisItems/Inflammatoryresponse.html
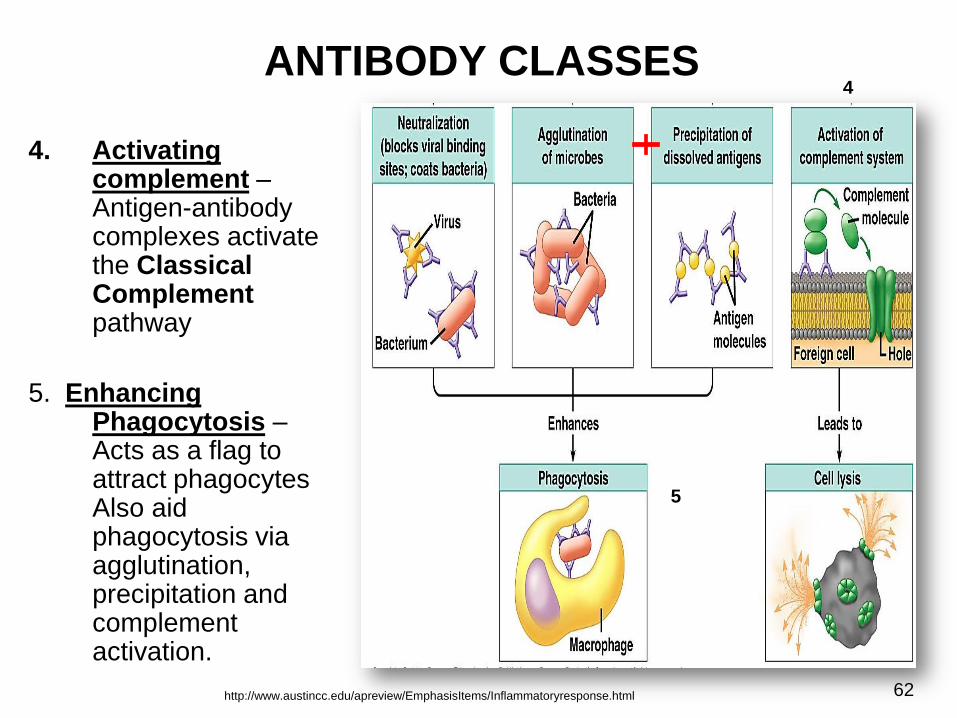
ANTIBODY CLASSES
4. Activating complement – Antigen-antibody complexes activate the Classical Complement pathway
5. Enhancing Phagocytosis – Acts as a flag to attract phagocytes Also aid phagocytosis via agglutination, precipitation and complement activation.
62
4
5
http://www.austincc.edu/apreview/EmphasisItems/Inflammatoryresponse.html
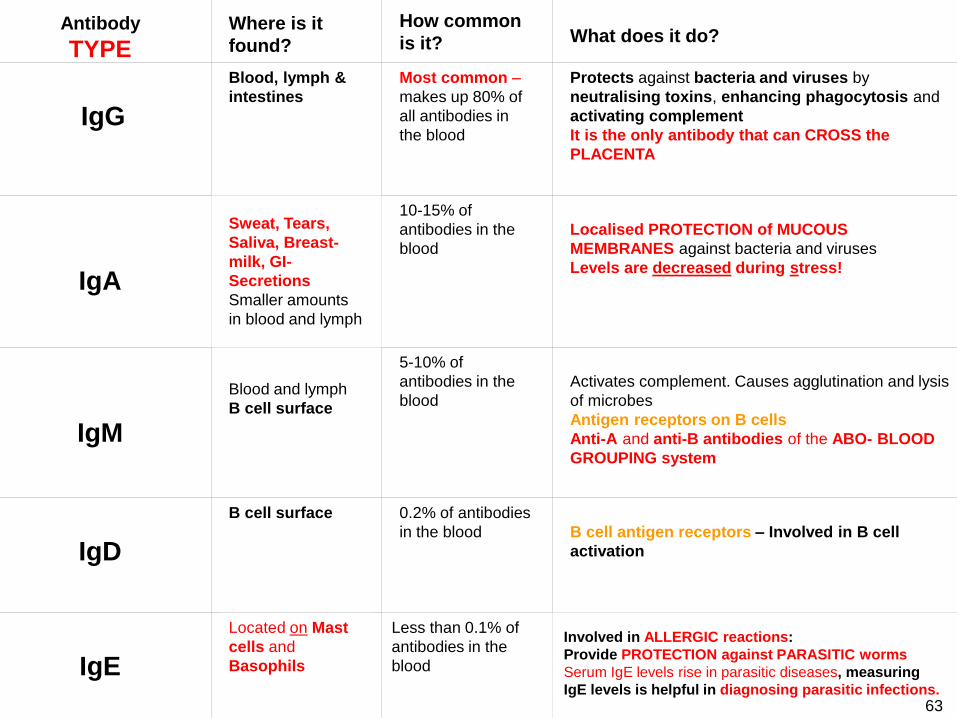
Antibody
TYPE
Where is it
found?
How common
is it?
What does it do?
IgG
Blood, lymph &
intestines
Most common –
makes up 80% of
all antibodies in
the blood
Protects against bacteria and viruses by
neutralising toxins, enhancing phagocytosis and
activating complement
It is the only antibody that can CROSS the
PLACENTA
IgA
Sweat, Tears,
Saliva, Breast-
milk, GI-
Secretions
Smaller amounts
in blood and lymph
10-15% of
antibodies in the
blood
Localised PROTECTION of MUCOUS
MEMBRANES against bacteria and viruses
Levels are decreased during stress!
IgM
Blood and lymph
B cell surface
5-10% of
antibodies in the
blood
Activates complement. Causes agglutination and lysis
of microbes
Antigen receptors on B cells
Anti-A and anti-B antibodies of the ABO- BLOOD
GROUPING system
IgD
B cell surface 0.2% of antibodies
in the blood
B cell antigen receptors – Involved in B cell
activation
IgE
Located on Mast
cells and
Basophils
Less than 0.1% of
antibodies in the
blood
Involved in ALLERGIC reactions:
Provide PROTECTION against PARASITIC worms
Serum IgE levels rise in parasitic diseases, measuring
IgE levels is helpful in diagnosing parasitic infections.
63
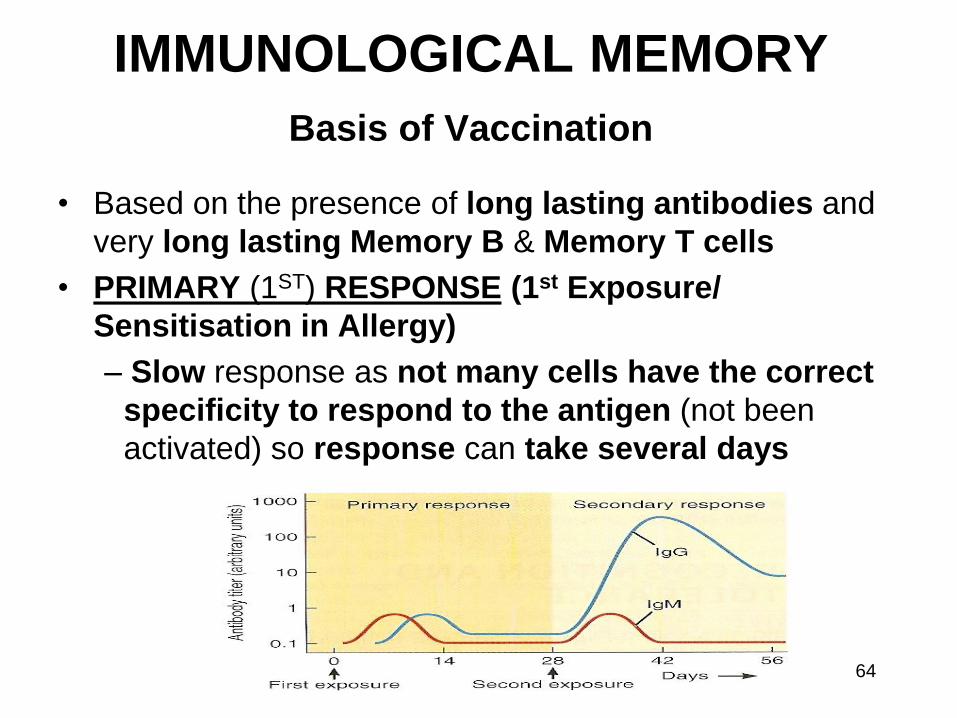
IMMUNOLOGICAL MEMORY
Basis of Vaccination
• Based on the presence of long lasting antibodies and
very long lasting Memory B & Memory T cells
• PRIMARY (1ST) RESPONSE (1st Exposure/
Sensitisation in Allergy)
– Slow response as not many cells have the correct
specificity to respond to the antigen (not been
activated) so response can take several days
64
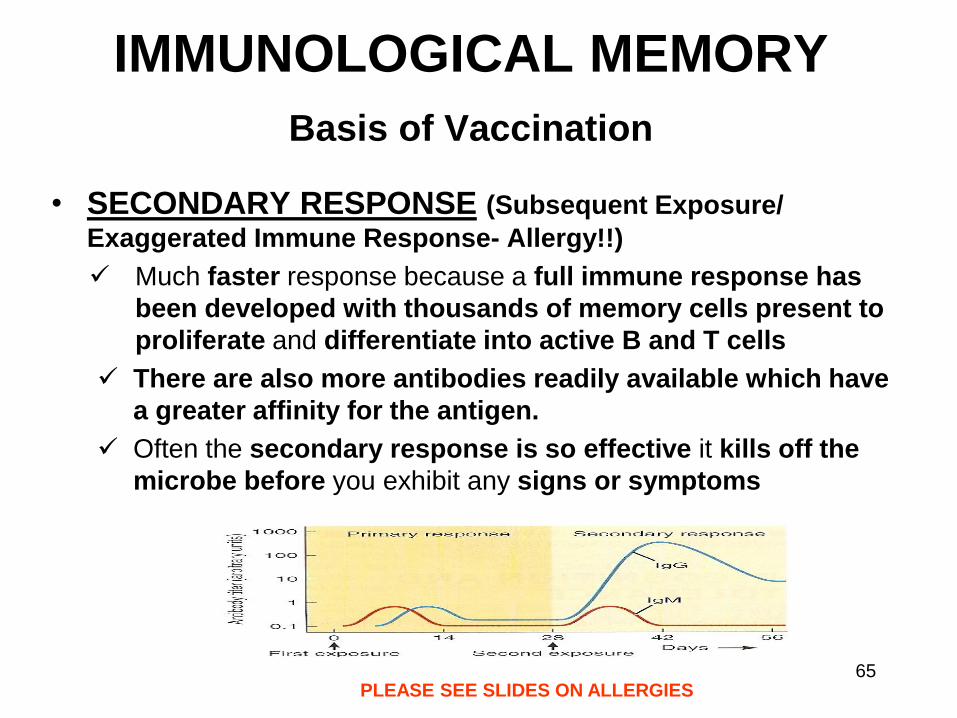
IMMUNOLOGICAL MEMORY
Basis of Vaccination
• SECONDARY RESPONSE (Subsequent Exposure/
Exaggerated Immune Response- Allergy!!)
Much faster response because a full immune response has
been developed with thousands of memory cells present to
proliferate and differentiate into active B and T cells
There are also more antibodies readily available which have
a greater affinity for the antigen.
Often the secondary response is so effective it kills off the
microbe before you exhibit any signs or symptoms
PLEASE SEE SLIDES ON ALLERGIES 65
• Immunological Memory is the basis for vaccination against certain
diseases
1. Vaccines contain Attenuated (weakened) /Killed, Whole/Portions
of Microbes
This ensures the Microbes are Immunogenic but NOT Pathogenic
i.e. They cause an immune response but not the illness
2. This activates the B and T cells = Primary Response. Not many
cells have the correct specificity to respond to the antigen, so a
response can take several days.
3. Subsequent exposure to the Living Pathogen initiates a far more
Effective Secondary Response- This response is much quicker as
thousands of Memory cells are now present to Proliferate and
Differentiate into Active B & T cells, often without any symptoms
being experienced.
66
IMMUNISATION / VACCINATION
VACCINATION
• Diseases preventable
by vaccination....
– Anthrax
– Cholera
– Diphtheria
– Hepatitis B
– Measles
– Mumps
– Poliomyelitis
– Rubella
– Smallpox
– Tetanus
– Tuberculosis
– Typhoid
– Whooping cough
67
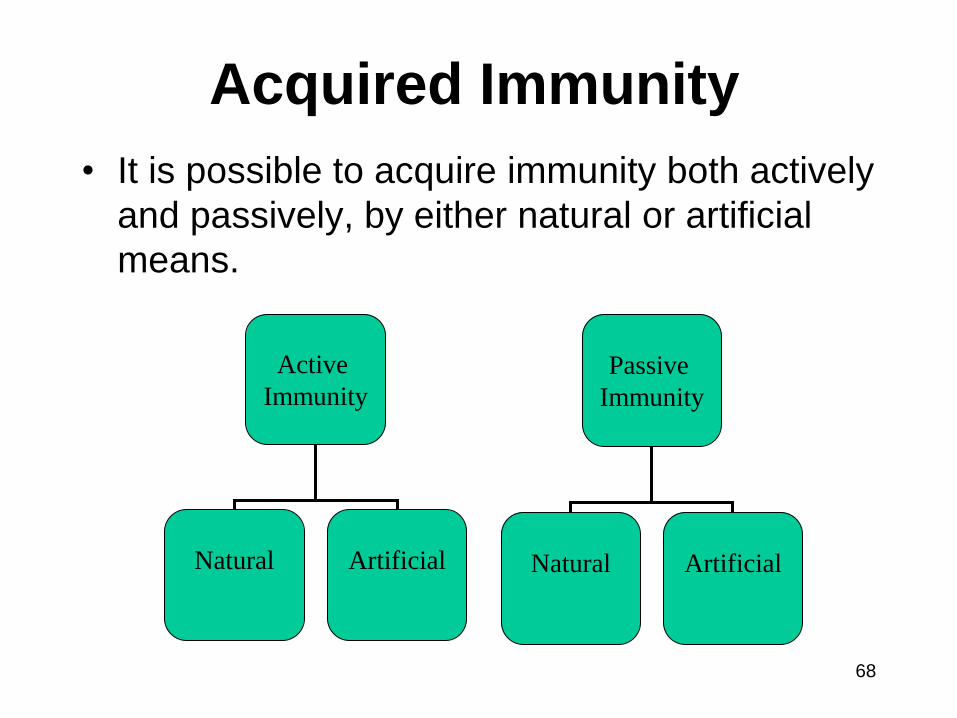
Acquired Immunity
• It is possible to acquire immunity both actively
and passively, by either natural or artificial
means.
Active
Immunity
Natural
Artificial
Passive
Immunity
Natural
Artificial
68
Acquired Immunity
• Naturally acquired active immunity • Natural exposure to a disease either clinical presentation or sub-
clinically
• Naturally acquired passive immunity • Transfer of IgG antibodies across the placenta from mother to
child.
• Transfer of IgA antibodies from mother to child via the breast milk
• Artificially acquired active immunity • Vaccination
• Artificially acquired passive immunity • Injection with immunoglobulin (antibodies) e.g. Snake anti-venom
69

Worksheet
• Please fill in the acquired immunity worksheet
70
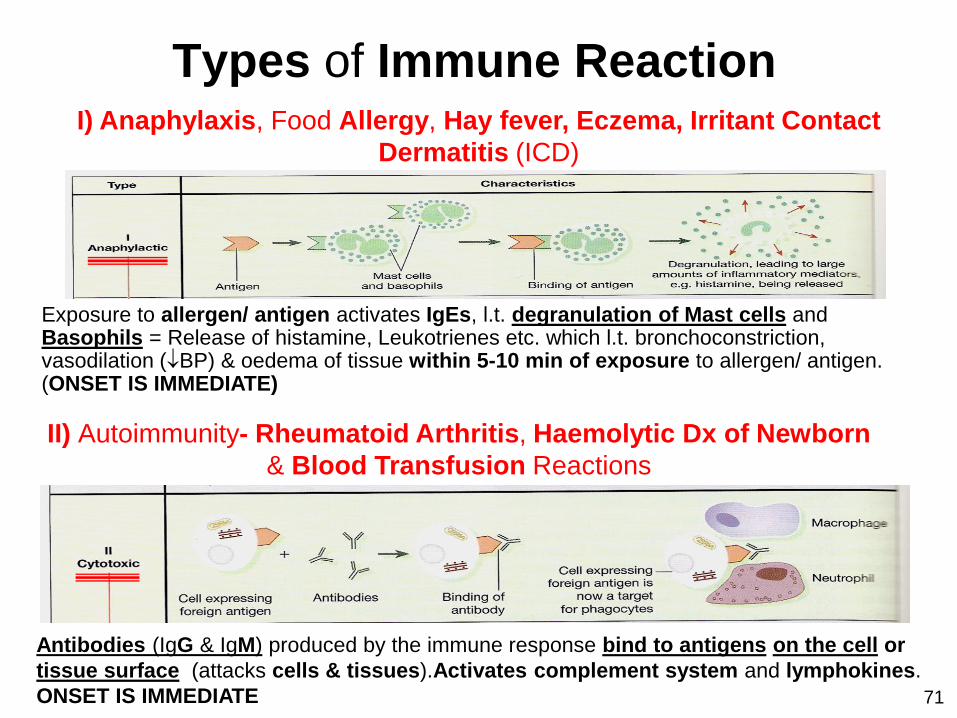
Types of Immune Reaction I) Anaphylaxis, Food Allergy, Hay fever, Eczema, Irritant Contact
Dermatitis (ICD)
II) Autoimmunity- Rheumatoid Arthritis, Haemolytic Dx of Newborn
& Blood Transfusion Reactions
Exposure to allergen/ antigen activates IgEs, l.t. degranulation of Mast cells and Basophils = Release of histamine, Leukotrienes etc. which l.t. bronchoconstriction, vasodilation (BP) & oedema of tissue within 5-10 min of exposure to allergen/ antigen. (ONSET IS IMMEDIATE)
Antibodies (IgG & IgM) produced by the immune response bind to antigens on the cell or
tissue surface (attacks cells & tissues).Activates complement system and lymphokines.
ONSET IS IMMEDIATE 71
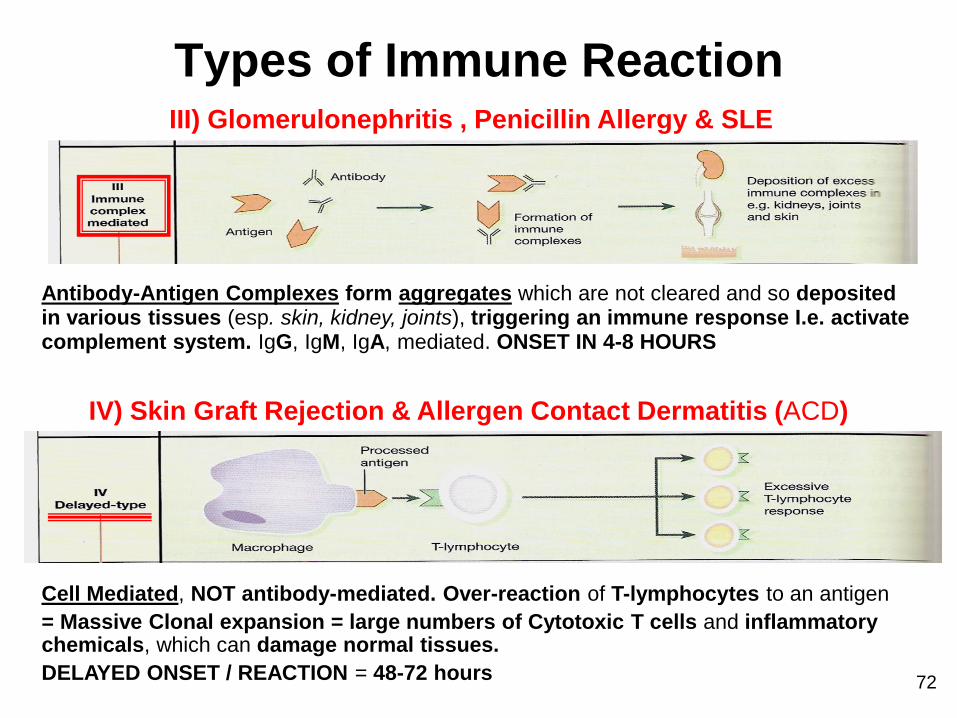
Types of Immune Reaction III) Glomerulonephritis , Penicillin Allergy & SLE
Antibody-Antigen Complexes form aggregates which are not cleared and so deposited in various tissues (esp. skin, kidney, joints), triggering an immune response I.e. activate complement system. IgG, IgM, IgA, mediated. ONSET IN 4-8 HOURS
Cell Mediated, NOT antibody-mediated. Over-reaction of T-lymphocytes to an antigen
= Massive Clonal expansion = large numbers of Cytotoxic T cells and inflammatory chemicals, which can damage normal tissues.
DELAYED ONSET / REACTION = 48-72 hours 72
IV) Skin Graft Rejection & Allergen Contact Dermatitis (ACD)
PROBIOTICS, DIGESTIONS
& IMMUNITY
ACQUIRED IMMUNITY
Gut Associated Lymphoid Tissue
• About 70% of the body's Immune System is found in the Digestive Tract.
• The GALT includes several types of Lymphoid Tissues that store Immune
cells, such as T and B lymphocytes.
• Example of GALT:
Tonsils, Adenoids (Pharyngeal Tonsils), Peyer's Patches & Appendix
Probiotics Pathogens
INNATE IMMUNITY of the GIT Wall (BASIC DEFENCE)
73
IMMUNE SYSTEM
PATHOLOGIES
74

ALLERGY
Examples of Allergens:
• Certain Foods
• Animal Dander
• Mites
• Dust
• Chemicals/ detergents/ perfumes/soaps/
• Latex
• Pollen
Def: Powerful Immune Response to an Allergen Allergen = Antigen that generates allergy.
The allergen itself is usually harmless, it is the immune response that causes damage to the body
75
ALLERGY • Initial Exposure = Sensitisation (Slow
response as not many cells have the correct specificity to respond to the antigen /allergen (not been activated). So this response can take several days
• Subsequent Exposure = Exaggerated Immune Response
• The full immune response has been developed and antibodies are readily available!
• Symptoms can range from mild presentation such as running nose and streaming eyes to anaphylaxis which can be fatal
76
Food Allergy vs. Intolerance
• True food allergy only affect 2% of adults and 6% of
children
• It is an IgE -Mediated Immune Response that can be
triggered by even the smallest amount of food
• Far more people have a Food Intolerance –
unpleasant symptoms triggered by eating a
significant quantity of a particular food and lacking
Probiotics, Enzymes, Bile, HCL or other Digestive
Factors needed to deal with the food.
• Food intolerance does not have a defined immune
response
• Example of a food intolerance: Lactose intolerance
77
Anaphylactic Shock
• Severe, Systemic, Allergic Response within 5-10 mins of exposure to an antigen.
• Inherited high levels of IgE
• Exposure to allergen causes IgEs to activate mast cells and basophils – Release of histamine
• Causes bronchoconstriction, vasodilation, oedema of tissue
• Rx: Epi-pen
78
AUTO IMMUNE CONDITIONS
Autoimmunity = The immune system failing to display Self Tolerance and Self Recognition
Auto antibodies = Antibodies/ Immunoglobulins & Cytotoxic T-Cells formed against self Antigens.
• The Antibody-Antigen reaction leads to Complement Activation, Inflammation and Tissue damage
• Autoimmunity often has a Genetic link – Tend to run in families.
• Some disorders affect specific tissue others are generalised
79
Systemic Lupus Erythematosus
A chronic autoimmune, Connective Tissue disease that can affect ANY part of the body
Cause:
1. AUTOIMMUNE
• B-cell activation increased IgG levels against DNA, platelets,
erythrocytes, nucleic acid and other nuclear materials
• Inability to remove immune complexes from tissue - Complement is
activated causing inflammation
• Impaired T-cell regulation
• Abnormal cytokine production
2. Can be caused by DRUGS: Flare-ups can be induced by OCP & HRT
3. GENETIC
4. ENVIRONMENTAL ( UV light, mercury, pesticides exacerbate it)
80
Systemic Lupus Erythematosus
Varies in manifestation:
• Fever
• Depression
• Photosensitivity
• Butterfly Rash
• Vasculitis, purpura,
urticaria
• Pleurisy
• Raynaud’s
• Polyarthralgia
• NS damage
• Heart damage
• Abdominal pain
• Renal disease
• Anaemia
Signs & Symptoms: The course of the disease is unpredictable, with periods of illness
(called flares) alternating with remissions.
81
Systemic Lupus Erythematosus
Investigations-
• Full blood count,
• Antinuclear antibody test
• Rheumatoid factor
• Complement levels
• Anti-phospholipids antibodies: IgG, IgE
• ESR
Management
• Immunosuppressive
• NSAIDS 82
Rheumatoid Arthritis
Chronic, Systemic Inflammation of many tissues, primarily the Synovium (potentially all organs except brain)
• Affects 1% people worldwide
• C: Considered to be Autoimmune
• Rheumatoid Factor (RF) - an Auto-antibody which can bind to other antibodies- is directed against a portion of IgG
• The resultant Immune Complex activates Complement proteins leading to inflammation and damage.
• RF is Present in the majority of suffers (~80%)but not all. RF may also be present in other conditions
83
Rheumatoid Arthritis
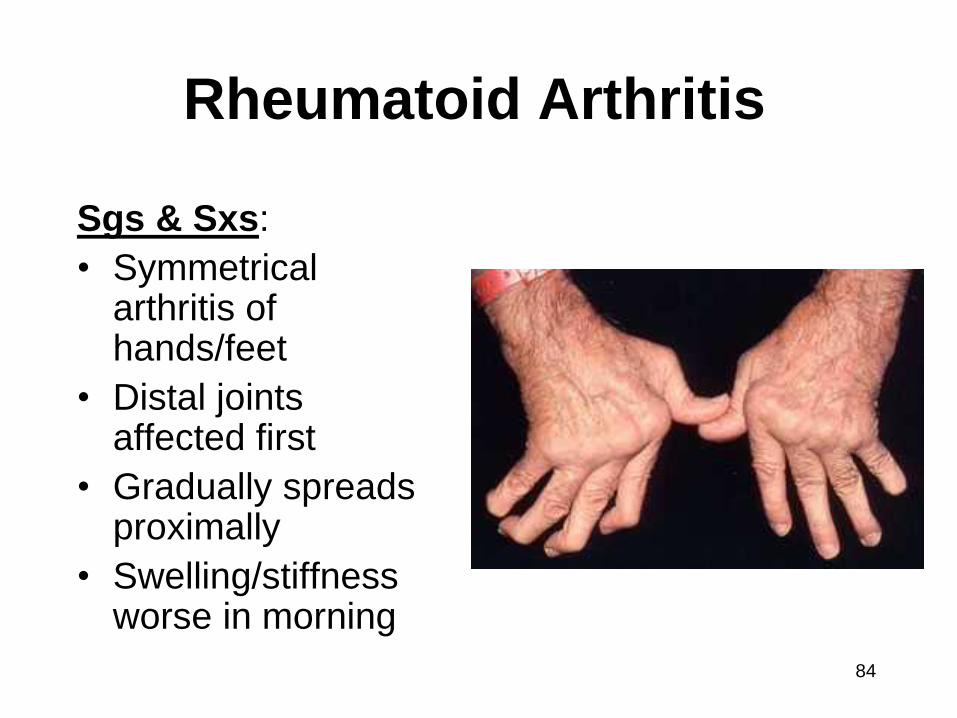
Sgs & Sxs:
• Symmetrical arthritis of hands/feet
• Distal joints affected first
• Gradually spreads proximally
• Swelling/stiffness worse in morning
84
Rheumatoid Arthritis
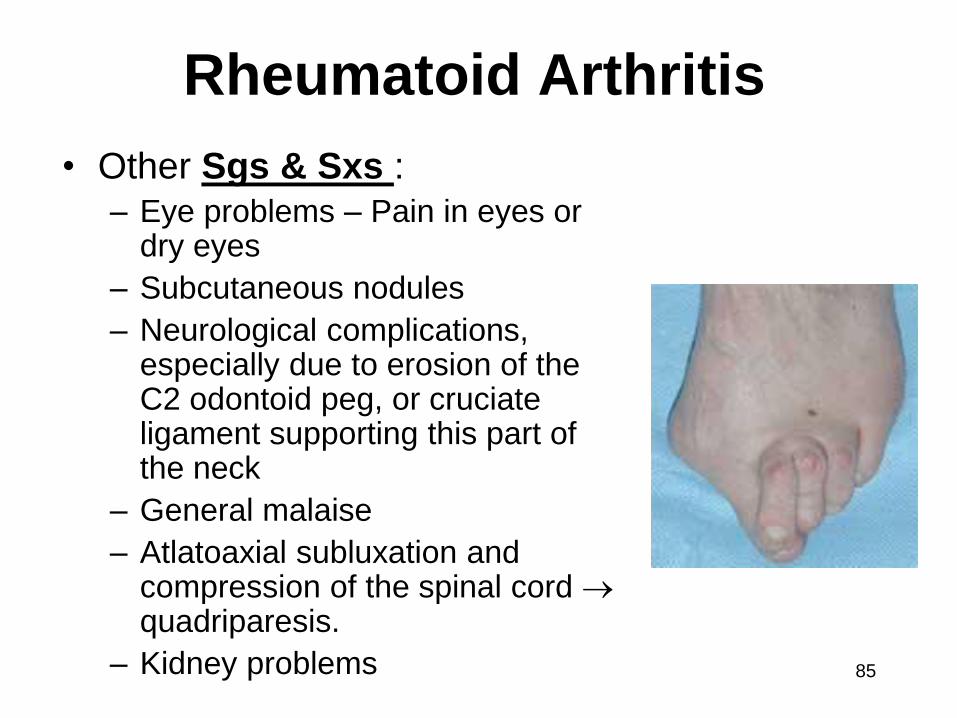
• Other Sgs & Sxs : – Eye problems – Pain in eyes or
dry eyes
– Subcutaneous nodules
– Neurological complications, especially due to erosion of the C2 odontoid peg, or cruciate ligament supporting this part of the neck
– General malaise
– Atlatoaxial subluxation and compression of the spinal cord quadriparesis.
– Kidney problems 85
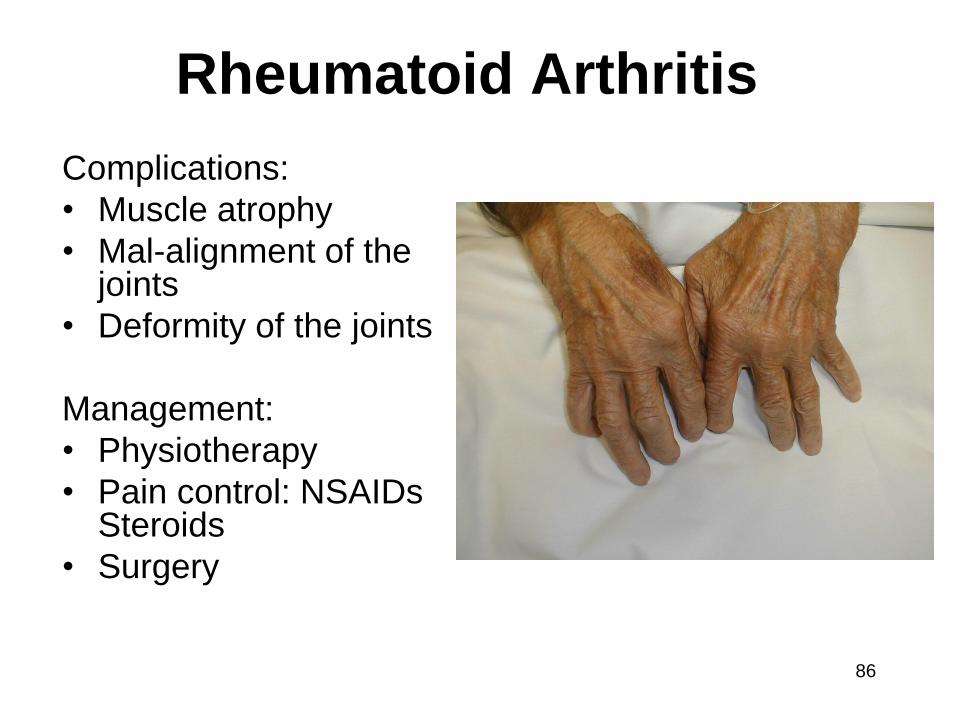
Rheumatoid Arthritis
Complications:
• Muscle atrophy
• Mal-alignment of the joints
• Deformity of the joints
Management:
• Physiotherapy
• Pain control: NSAIDs Steroids
• Surgery
86
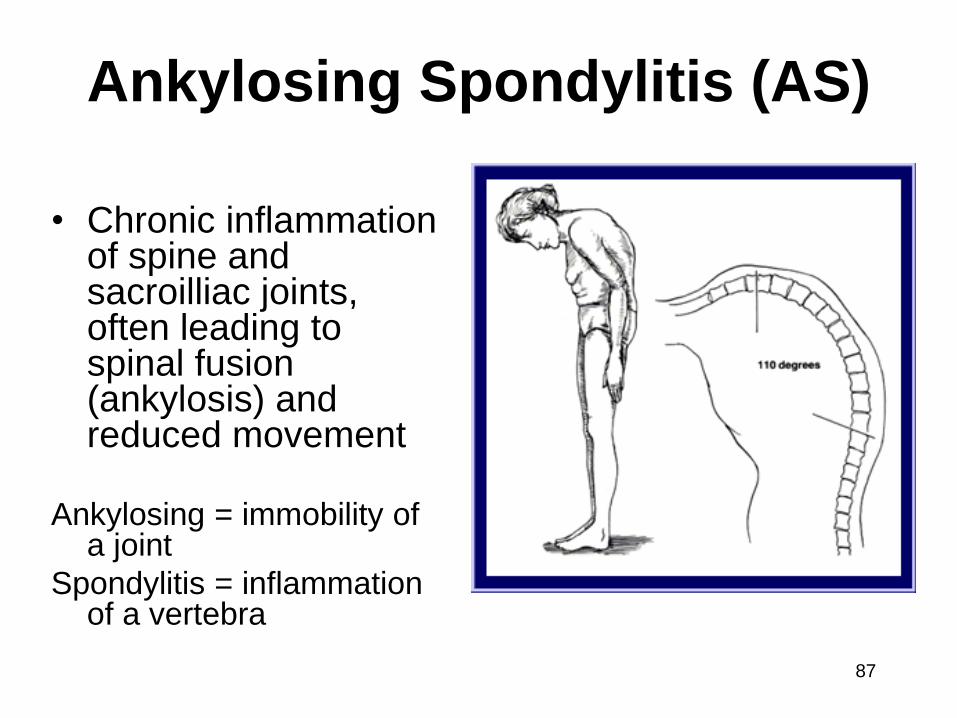
Ankylosing Spondylitis (AS)
• Chronic inflammation of spine and sacroilliac joints, often leading to spinal fusion (ankylosis) and reduced movement
Ankylosing = immobility of a joint
Spondylitis = inflammation of a vertebra
87
Cause:
• Autoimmune with a genetic basis
• 95% of patients test positive for the HLA–B27 Gene
• Age of onset 20–45.
• 1/3 have a family history
• M:W – 8:1
• No direct diagnostic tool
88
Ankylosing Spondylitis (AS)
Ankylosing Spondylitis (AS)
Sgs & Sxs :
• A sufferer presents with low back pain, possibly radiating into posterior thighs.
• Stiffness and pain is marked in the mornings,
and improves with activity.
• Sometimes systemic signs like fatigue, fever,
weight loss, eye inflammation
89
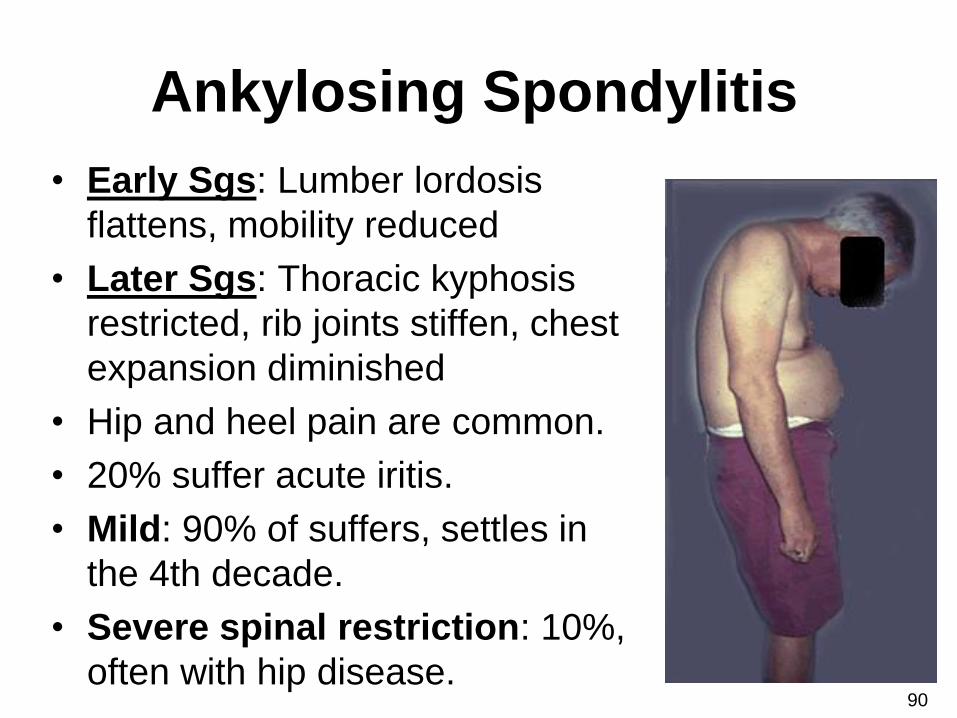
Ankylosing Spondylitis
• Early Sgs: Lumber lordosis
flattens, mobility reduced
• Later Sgs: Thoracic kyphosis
restricted, rib joints stiffen, chest
expansion diminished
• Hip and heel pain are common.
• 20% suffer acute iritis.
• Mild: 90% of suffers, settles in
the 4th decade.
• Severe spinal restriction: 10%,
often with hip disease. 90
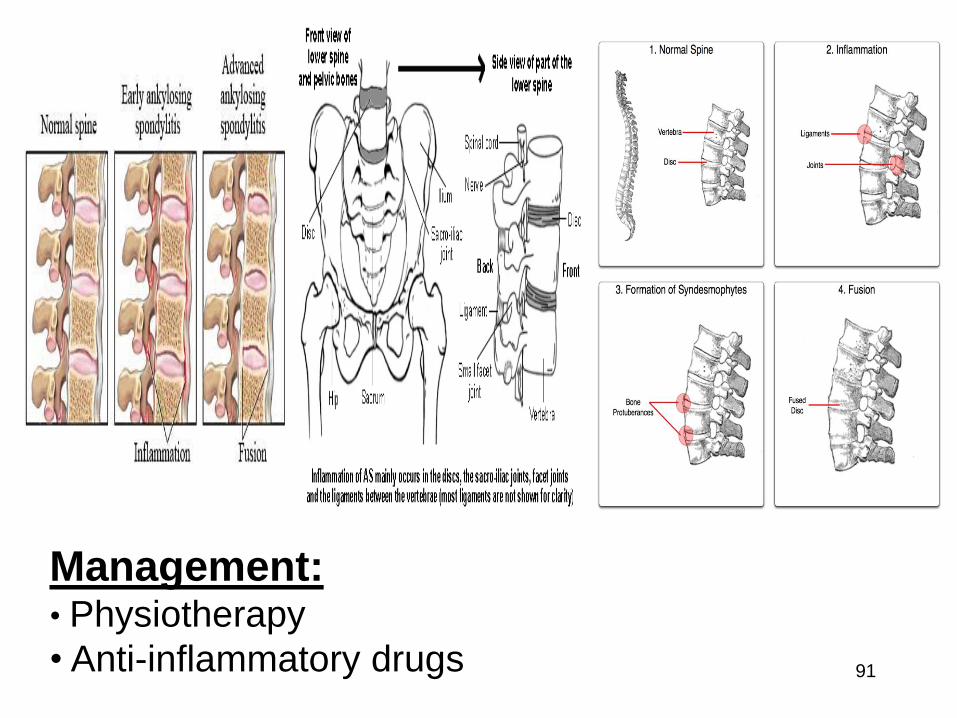
Management: • Physiotherapy
• Anti-inflammatory drugs 91
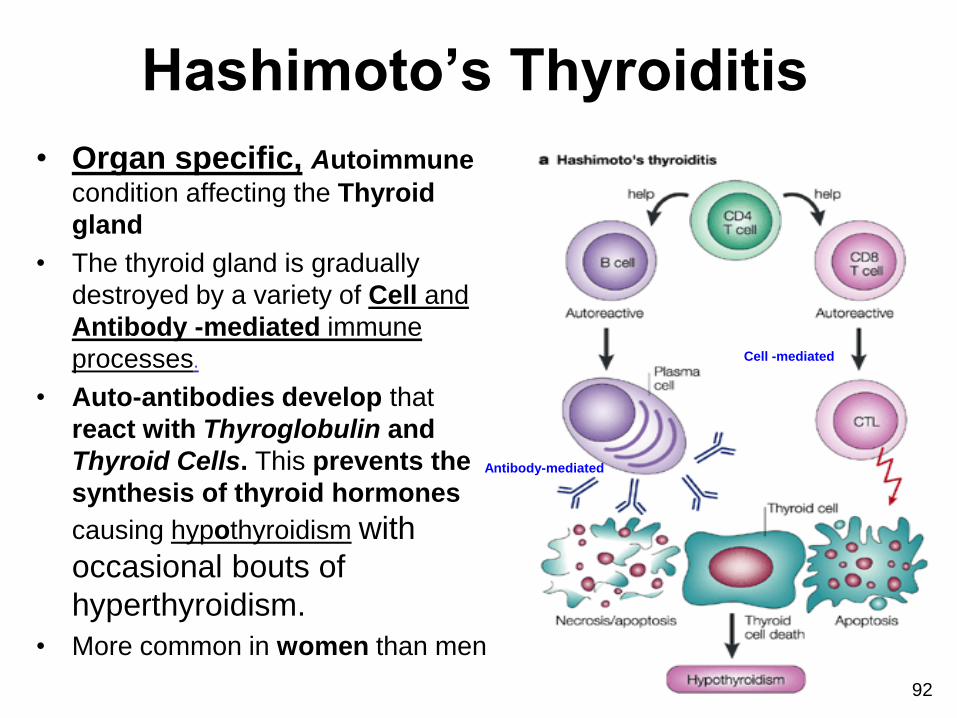
Hashimoto’s Thyroiditis
• Organ specific, Autoimmune
condition affecting the Thyroid
gland
• The thyroid gland is gradually
destroyed by a variety of Cell and
Antibody -mediated immune
processes.
• Auto-antibodies develop that
react with Thyroglobulin and
Thyroid Cells. This prevents the
synthesis of thyroid hormones
causing hypothyroidism with
occasional bouts of
hyperthyroidism.
• More common in women than men
Antibody-mediated
Cell -mediated
92
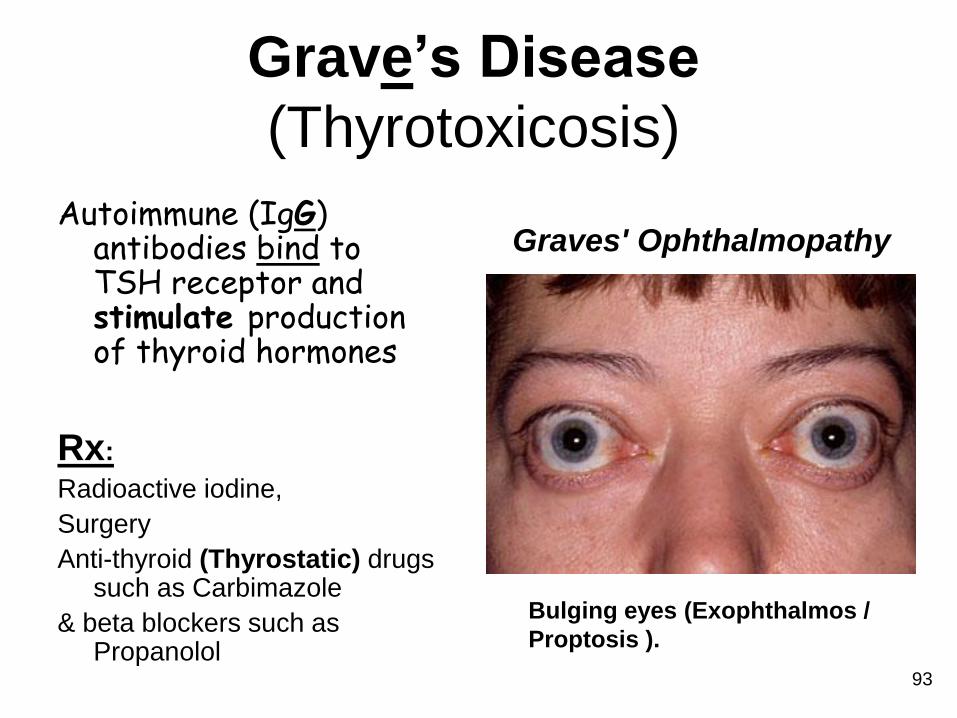
Grave’s Disease
(Thyrotoxicosis)
Autoimmune (IgG) antibodies bind to TSH receptor and stimulate production of thyroid hormones
Rx:
Radioactive iodine,
Surgery
Anti-thyroid (Thyrostatic) drugs such as Carbimazole
& beta blockers such as Propanolol
Bulging eyes (Exophthalmos /
Proptosis ).
Graves' Ophthalmopathy
93
Role of Lymphatic and Immune
Systems in Homeostasis Whole body:
• Immune cells and antibodies protect the body from foreign invaders, foreign cells and cancer cells
• Lymphatic system drains excess tissue fluid
Integumentary system:
• Langerhans cells help protect the skin
• Lymphatic tissue provides IgAs in sweat
94
Skeletal and muscular systems:
• Lymphatic vessels drain excess tissue fluid and leaked plasma proteins from the muscle tissue and connective tissue surrounding bones
Endocrine system:
• Lymph flow helps distribute some hormones and cytokines
Role of Lymphatic and Immune
Systems in Homeostasis
95
Cardiovascular system:
• Lymph returns excess fluid and leaked plasma proteins to the blood stream
• Macrophages in the spleen destroy old red blood cells
Respiratory system:
• Tonsils, alveolar macrophages and MALT help protect the lungs from pathogens
Urinary system:
• MALT defends against pathogens that penetrate the body via the urethra
Role of Lymphatic and Immune
Systems in Homeostasis
96
Digestive system:
• Tonsils and MALT defend against pathogens entering the GI tract
• IgA antibodies in saliva
• Lymphatic vessel pick up absorbed dietary lipids and fat soluble vitamins from the small intestine and transport them to the blood
Role of Lymphatic and Immune
Systems in Homeostasis
97
Reproductive system:
• MALT helps defend against pathogens entering via the vagina/penis
• IgG antibodies can cross the placenta to provide protection for the developing fetus
• IgA antibodies are passed to the neonate via the breast milk
Role of Lymphatic and Immune
Systems in Homeostasis
98
Quiz!
• Teams of 4
• Decide on a team name
• 33 Questions
• Possible 77 marks
• Write neatly so the
marking team can read
you answers!
99