The expected and unexpected: Initial experiences in a de novo fMRI program Tannenbaum AD, Sakai O,...
43
The expected and unexpected: Initial experiences in a de novo fMRI program Tannenbaum AD, Sakai O, Jara H, Barest G, Norbash AM, Mian AZ Department of Radiology Boston University School of Medicine Boston Medical Center Boston, MA
-
Upload
winfred-pearson -
Category
Documents
-
view
217 -
download
0
Transcript of The expected and unexpected: Initial experiences in a de novo fMRI program Tannenbaum AD, Sakai O,...

The expected and unexpected:Initial experiences in a de novo fMRI program
Tannenbaum AD, Sakai O, Jara H, Barest G, Norbash AM, Mian AZ
Department of RadiologyBoston University School of Medicine
Boston Medical CenterBoston, MA

_
Petrella, J. R., Shah, L. M., Harris, K. M., Friedman, A. H., George, T. M., Sampson, J. H., et al. (2006). Preoperative functional MR imaging localization of language and motor areas: effect on therapeutic decision making in patients with potentially resectable brain tumors. Radiology, 240(3), 793–802. doi:10.1148/radiol.2403051153
Medina, L. S., Aguirre, E., Bernal, B., & Altman, N. R. (2004). Functional MR imaging versus Wada test for evaluation of language lateralization: cost analysis. Radiology, 230(1), 49–54. doi:10.1148/radiol.2301021122
Mahvash, M., Maslehaty, H., Jansen, O., Mehdorn, H. M., & Petridis, A. K. (2014). Functional magnetic resonance imaging of motor and language for preoperative planning of neurosurgical procedures adjacent to functional areas. Clinical Neurology and Neurosurgery, 123, 72–77. doi:10.1016/j.clineuro.2014.05.011
Functional magnetic resonance imaging (fMRI) of the brain allows for identification of eloquent areas for preoperative planning and for various psychiatric and neurological disorders.
-Predominantly used for preoperative planning-Localization is achieved using various paradigms designed to stimulate specific areas such as motor, speech, and sensory regions-Precise preoperative localization enables maximal resection and may also help predict postoperative deficits-High concordance rates with Wada testing and intraoperative cortical stimulation-Has been shown to alter surgical management-Data is generated using paradigms and BOLD imaging
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion

Blood Oxygen Level-dependent Imaging (BOLD)
Basic Principles of BOLD-Originally discovered in 1990 by Ogawa et al -Deoxyhemoglobin (deoxyHb) acts as an endogenous paramagnetic contrast agent for BOLD-Images are acquired using echoplanar imaging-Cortical activation leads to a drop in oxyHB and increase in CO2 with a compensatory increase in blood flow, leading to higher oxyHb and dilution of deoxyHb-BOLD relies on the gradient of oxyHb:deoxyHb to generate functional dataKim, S.-G., & Ogawa, S. (2012). Biophysical and physiological origins of blood oxygenation level-dependent fMRI signals. Journal of Cerebral Blood Flow and Metabolism : Official Journal of the International Society of Cerebral Blood Flow and Metabolism, 32(7), 1188–1206. doi:10.1038/jcbfm.2012.23
_BOLD Hardware/Software
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion

_Stimulus
HemodynamicResponse
MRI Pulse Sequence
fMRI Paradigm
Stimulus-dependentMRI signal change
NeurovascularCoupling
BOLD Hardware/Software
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion
Short T2*: deoxygenated
Long T2*: oxygenated

*2T
*2T
Fig.1: Schematic showing the time course of BOLD response to a short stimulus. The fast response has a negative peak at about two seconds poststimulus due to brief decrease in blood oxygenation after neural activity. The main BOLD response peaks at about five seconds with FWHM(full width at half maximum) of about four seconds. The signal takes about a minute to return to baseline.
Main BOLD response

_BOLD Hardware/Software
Cortical Stimulation
Cortical Stimulation
Increased Neuronal Activity
Increased Neuronal Activity
Increased blood flowIncreased blood flow
Increased O2 Extraction
Increased O2 Extraction
Increased oxyHbIncreased oxyHb
Increased deoxyHbIncreased deoxyHb
Decreased deoxyHb
concentration
Decreased deoxyHb
concentration
Schematic of BOLD signal generation
deoxyHb has a paramagnetic effect;
Increased blood flow is sufficient to dilute deoxyHb concentration
fMRIsigna
l
fMRIsigna
l
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion
Adapted from Daniel Marcus PhD., “Brain Imaging for fun and Profit”
HbO2HbO2
HbO2HbO2
HbO2HbO2
HbHb
HbHb
HbHb
HbO2HbO2
HbO2HbO2
HbO2HbO2 HbO2
HbO2
HbO2HbO2
Resting state schematic illustrating the paramagnetic effect of deoxyHb
Activated state with increase in oxyHb. Measurement of the gradient between oxyHb and deoxyHb will yield BOLD signal.
Blood Oxygen Level-dependent Imaging (BOLD)BOLD Hardware/Software
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion
HbHb
Distorted field lines

Blood Oxygen Level-dependent Imaging (BOLD)
Limitations of BOLD-Relies on T2* imaging which is sensitive to magnetic field inhomogeneity
-Very sensitive to patient motion
-An indirect measurement of cortical neuronal activity. Data reflects changes in blood flow rather than direct neuronal activity
Kim, S.-G., & Ogawa, S. (2012). Biophysical and physiological origins of blood oxygenation level-dependent fMRI signals. Journal of Cerebral Blood Flow and Metabolism : Official Journal of the International Society of Cerebral Blood Flow and Metabolism, 32(7), 1188–1206. doi:10.1038/jcbfm.2012.23
_BOLD Hardware/Software
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion

At our institution we employ the following system-GE Discovery 750W 3 Tesla MRI-Sensavue fMRI by Invivo Corp.-Images processed in DynaSuite by Invivo Corp.
Typical fMRI Acquisition Parameters-TR = 2000 ms-Number of volumes 120-Control 10 repetitions-Stimulus 10 repetitions
Each volume takes 2 seconds to acquire and the first 4 volumes are discarded. Total scan time is 4 min 8 sec for each of our paradigms.
BOLD Hardware/Software
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion
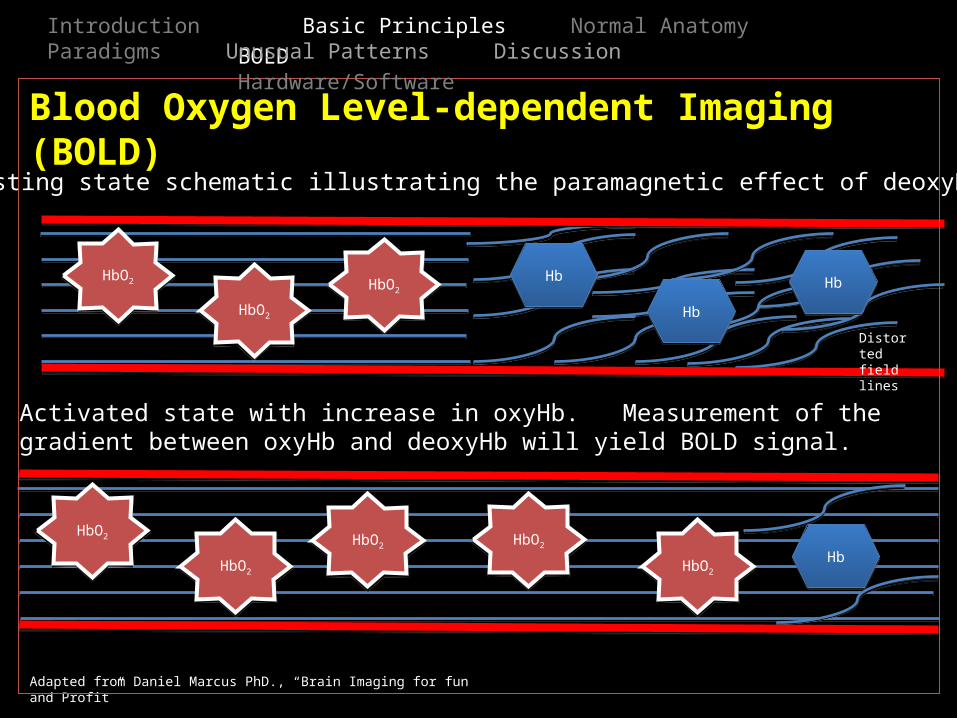
Acquisition Parameters, continued
FSPGR BRAVO (IR-prep fast SPGR) image for anatomic localization
Images are obtained using a 256 x 256 matrix with 1.2 mm slice thickness. 1 slab is obtained with 16 locs per slab. TE = 3.3, TR = 8.5, NEX = 1, Flip Angle = 12
Diffusion Tensor Imaging (DTI) 4mm
Images are obtained using a 129 (freq.) x 128 (phase) matrix with 5 mm slice thickness with 1 mm spacing. 29 slices are obtained. TEmin = 98.6, TR = 8000, NEX = 1, B = 1000
BOLD Hardware/Software
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion

I
Image source: https://en.wikipedia.org/wiki/Broca%27s_area#mediaviewer/File:Broca%27s_area_-_lateral_view.png. Licensed under CC-BY-SA-2.1-jp
_ Broca’s AreaClassically located in the left frontal lobe, refers to the pars triangularis(red) and the pars opercularis(blue) of the inferior frontal gyrus
Wernicke’s AreaClassically located in the posterior portion of the left superior temporal gyrus
Arcuate FasciculusA segment of the superior longitudinal fasciculus that connects Wernicke’s and Broca’s
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion Language Motor

I_ Broca’s AreaClassically located in the left frontal lobe, refers to the pars triangularis and the pars opercularis of the inferior frontal gyrus
Wernicke’s AreaClassically located in the posterior portion of the left superior temporal gyrus
Arcuate FasciculusA segment of the superior longitudinal fasciculus that connects Wernicke’s and Broca’s
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion Language Motor

I
Modified from: https://en.wikipedia.org/wiki/Broca%27s_area#mediaviewer/File:Broca%27s_area_-_lateral_view.png. Licensed under CC-BY-SA-2.1-jp
_ Broca’s AreaClassically located in the left frontal lobe, refers to the pars triangularis(red) and the pars opercularis(blue) of the inferior frontal gyrus
Wernicke’s AreaClassically located in the posterior portion of the left superior temporal gyrus
Arcuate FasciculusA segment of the superior longitudinal fasciculus that connects Wernicke’s and Broca’s
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion Language Motor

I_ Broca’s AreaClassically located in the left frontal lobe, refers to the pars triangularis and the pars opercularis of the inferior frontal gyrus
Wernicke’s AreaClassically located in the posterior portion of the left superior temporal gyrus
Arcuate FasciculusA segment of the superior longitudinal fasciculus that connects Wernicke’s and Broca’s
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion Language Motor
Receptive language center In this healthy volunteerdid not localize to the classic location

I
Modified from: https://en.wikipedia.org/wiki/Broca%27s_area#mediaviewer/File:Broca%27s_area_-_lateral_view.png. Licensed under CC-BY-SA-2.1-jp
_ Broca’s AreaClassically located in the left frontal lobe, refers to the pars triangularis(red) and the pars opercularis(blue) of the inferior frontal gyrus
Wernicke’s AreaClassically located in the posterior portion of the left superior temporal gyrus
Arcuate FasciculusA segment of the superior longitudinal fasciculus that connects Wernicke’s and Broca’s
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion Language Motor

I_ Broca’s AreaClassically located in the left frontal lobe, refers to the pars triangularis(red) and the pars opercularis(blue) of the inferior frontal gyrus
Wernicke’s AreaClassically located in the posterior portion of the left superior temporal gyrus
Arcuate FasciculusA segment of the superior longitudinal fasciculus that connects Wernicke’s and Broca’s
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion Language Motor

I_
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion
Primary Motor CortexClassically located in the dorsal aspect of the precentral gyrus of the frontal lobe. Primary coordinator of movement.
Premotor CortexLocated just anterior to the primary motor cortex. Function uncertain, may play a role in planning.
Supplementary Motor AreaLocated at the medial surface of the hemispheres just anterior to the primary motor cortex. Contributes to control of movement.
Image source: http://www.neuroscientificallychallenged.com/glossary/primary-motor-cortex
Language Motor

I_
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion
Primary Motor CortexClassically located in the dorsal aspect of the precentral gyrus of the frontal lobe. Primary coordinator of movement.
Premotor CortexLocated just anterior to the primary motor cortex. Function uncertain, may play a role in planning.
Supplementary Motor AreaLocated at the medial surface of the hemispheres just anterior to the primary motor cortex. Contributes to control of movement.
Language Motor

I_
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion
Primary Motor CortexClassically located in the dorsal aspect of the precentral gyrus of the frontal lobe. Primary coordinator of movement.
Premotor CortexLocated just anterior to the primary motor cortex. Function uncertain, may play a role in planning.
Supplementary Motor AreaLocated at the medial surface of the hemispheres just anterior to the primary motor cortex. Contributes to control of movement.
Image modified from: http://www.neuroscientificallychallenged.com/glossary/premotor-cortex/
Language Motor

I_
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion
Primary Motor CortexClassically located in the dorsal aspect of the precentral gyrus of the frontal lobe. Primary coordinator of movement.
Premotor CortexLocated just anterior to the primary motor cortex. Function uncertain, may play a role in planning.
Supplementary Motor AreaLocated at the medial surface of the hemispheres just anterior to the primary motor cortex. Contributes to control of movement. Approximate location of premotor
cortex highlighted in red
Language Motor

I_ Primary Motor CortexClassically located in the dorsal aspect of the precentral gyrus of the frontal lobe. Primary coordinator of movement.
Premotor CortexLocated just anterior to the primary motor cortex. Function uncertain, may play a role in planning.
Supplementary Motor AreaLocated at the medial surface of the hemispheres just anterior to the primary motor cortex. Contributes to control of movement.
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion
Image modified from: http://www.arts.uwaterloo.ca/~bfleming/psych261/lec16no9.htm
Language Motor
Supplementary motor area
Primary motor cortex

I_ Primary Motor CortexClassically located in the dorsal aspect of the precentral gyrus of the frontal lobe. Primary coordinator of movement.
Premotor CortexLocated just anterior to the primary motor cortex. Function uncertain, may play a role in planning.
Supplementary Motor AreaLocated at the medial surface of the hemispheres just anterior to the primary motor cortex. Contributes to control of movement.
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion Language Motor

fMRI Paradigms
-A paradigm is an activity or stimulus designed to elicit a specific cortical response-Typically target visual, speech, motor, or memory areas-Successful localization of eloquent areas requires that the patient is able to comply with the paradigm-Block design: the most common type during which a specific stimulus is repeated over a stimulus-rest cycle-Event related design: single events designed to elicit a cortical response
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion Overview Motor Language Other
_
ASFNR Paradigms. Available at http://www.asfnr.org/paradigms.html. Date accessed 03/10/2015.

_time _
Actual recorded data showing a block design paradigm with the smoothed predicted value and the actual recorded values (here labeled R3)
Rest
Stimulus
804020 60 100 120
Time (sec)
Activ
ation
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion Overview Motor Language Other
Block design paradigm schematic showing 20 second rest/stimulus cycles

Motor Paradigms
-Designed to stimulate motor, pre-motor and supplementary motor areas-Typically block design paradigms-Examples include:
o Bilateral complex finger tappingo Unilateral sequential finger tappingo Tongue movement/lip puckeringo Toe motion
-Requires adequate patient dexterity and ability to cooperate (if lacking dexterity hand-grip can be attempted)-Physician or technologist can actively assist patient with finger motion or toe motion if patient unable to follow command in a timely fashion
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion Overview Motor Language Other
_
ASFNR Paradigms. Available at http://www.asfnr.org/paradigms.html. Date accessed 03/10/2015.

Motor Paradigms – Our methods
-At our institution we begin every fMRI with tongue movement to help separate this from the later language paradigms (if necessary)
The patient is asked to move their tongue side to side in 20 second rest-stimulus intervals-Bilateral toe-motion
The patient is asked to move their toes randomly in 20 second rest-stimulus intervals. It is important patients
not move feet excessively to avoid head motion artifact-Bilateral finger tapping
Rapid finger tapping over 20 second rest-stimulus cycles
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion Overview Motor Language Other
_

I
Tongue movement (pink) with motor cortex activity
Toe motion (yellow) with motor activity
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion Overview Motor Language Other

_Language Paradigms
-Designed to lateralize and stimulate Broca’s area, Wernicke’s area and the arcuate fasciculus-Examples include:
o Sentence completiono Verb generation (i.e. Ball “throw”)o Passive listening (Wernicke’s area)o Word naming (i.e. think of words that start with “A”)o Object naming
-Typically a block design paradigm
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion Overview Motor Language Other

Language Paradigms
-Requires the patient to be literate and able to recognize and read the letters on the display
-It is essential that patients do not actually move their tongue/lips during the procedure to avoid confounding activation
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion Overview Motor Language Other
_
Gracco, V. L., Tremblay, P., & Pike, B. (2005). Imaging speech production using fMRI. Neuroimage, 26(1), 294–301. doi:10.1016/j.neuroimage.2005.01.033

Language Paradigms – Our methods
We employ the following standardized paradigms:-Verb generation
The patient is shown a noun and asked to think of a verb such as “car” “drive”-Word generation
The patient is asked to think of as many words as they can that start with a specific letter-Sentence completion
The patient is given a sentence and asked to complete it-Object naming
The patient is shown various objects (e.g. house, chair) and asked to recognize and name them
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion
_Overview Motor Language Other

I
Word generation (orange) showing activity in Broca’s area in a left language dominant subject.
Sentence completion paradigm showing activity in Wernicke’s area (red)
Overview Motor Language Other
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion

fMRI Paradigms – Other uses
-Script-driven fMRI has been used to investigate patterns of activation in PTSD -Alzheimer’s disease characterization via parahippocampal and hippocampal activation in memory tasks-Assessment of addiction with focus on prefrontal cortex-Evaluation of traumatic brain injury (TBI), able to show subtle changes in mild TBI in the absence of structural defects on static images. Dependent on site of injury
_
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion Overview Motor Language Other
Hughes, K. C., & Shin, L. M. (2011). Functional neuroimaging studies of post-traumatic stress disorder. Expert Review of Neurotherapeutics, 11(2), 275–285. doi:10.1586/ern.10.198Sperling, R. (2011). The potential of functional MRI as a biomarker in early Alzheimer's disease. Neurobiology of Aging, 32, S37–S43. doi:10.1016/j.neurobiolaging.2011.09.009Luijten, M., Machielsen, M., Veltman, D., Hester, R., de Haan, L., & Franken, I. (2014). Systematic review of ERP and fMRI studies investigating inhibitory control and error processing in people. Journal of Psychiatry & Neuroscience, 39(3), 149–169. doi:10.1503/jpn.130052McDonald, B. C., Saykin, A. J., & McAllister, T. W. (2012). Functional MRI of mild traumatic brain injury (mTBI): progress and perspectives from the first decade of studies. Brain Imaging and Behavior, 6(2), 193–207. doi:10.1007/s11682-012-9173-4

_
Presumed Wernicke’s area (blue arrow), slightly more anterior than expected, potentially distorted by tumor
Hx: 55F Spanish-speaking with glioblastoma multiforme(red arrow) presents for preoperative evaluation prior to resection. Before starting the test it was discovered she was illiterate and thus unable to follow written directions.
Challenge: Illiterate Spanish-speaking patient, unable to perform language tasks without assistance.Solution: Spanish-speaking interpreter read letters on screen and patient was able to complete word generation paradigm, resulting in faint activation of Wernicke’s area.
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion

_
Broca’s area localizes to inferior frontal lobule(blue arrow)
Hx: 51M Cantonese-speaking with complex partial seizures due to a left frontal lobe mass(red arrow). Pre-operative evaluation given proximity to eloquent areas.
Challenge: Cantonese-speaking patient with limited English fluency.
Solution: To complete object naming paradigm, the patient was shown images and asked to silently name them in his native language, resulting in activation of the language centers.
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion
Expected Wernicke’s area(yellow arrow)
Object naming paradigm

_
Two distinct Broca’s areas(blue arrows)
Hx: 37F right-handed with intractable epilepsy s/p trauma found to have multiple prominent areas of left-sided activation during language tasks
Challenge: Multiple areas of activation on language related paradigm.
Solution: Correlate with the patient’s medical record or patient query. We discovered the patient was trilingual, likely explaining the multiple Broca’s areas.
Single Wernicke’s area(yellow arrow)
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion
Sentence completion paradigm
Arcuate fasciculus

_
Bilateral Broca’s areas (blue arrows)
Hx: 71M right-handed with intractable epilepsy for preoperative evaluation prior to right-sided amygdalohippocampectomy.
Challenge: Bilateral language centers with no clear dominant side by fMRI. Evaluation for Wernickes was inconclusive.Solution: Confirmatory testing. Post-fMRI preoperative Wada test confirmed bilateral co-dominant language centers, noting dysphasia with right-sided injection and non-fluency with left-sided injection. This patient suffered a postoperative right MCA territory infarct with hemorrhage resulting in severe aphasia consistent with Wada testing.
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion
Word generation paradigm
_(
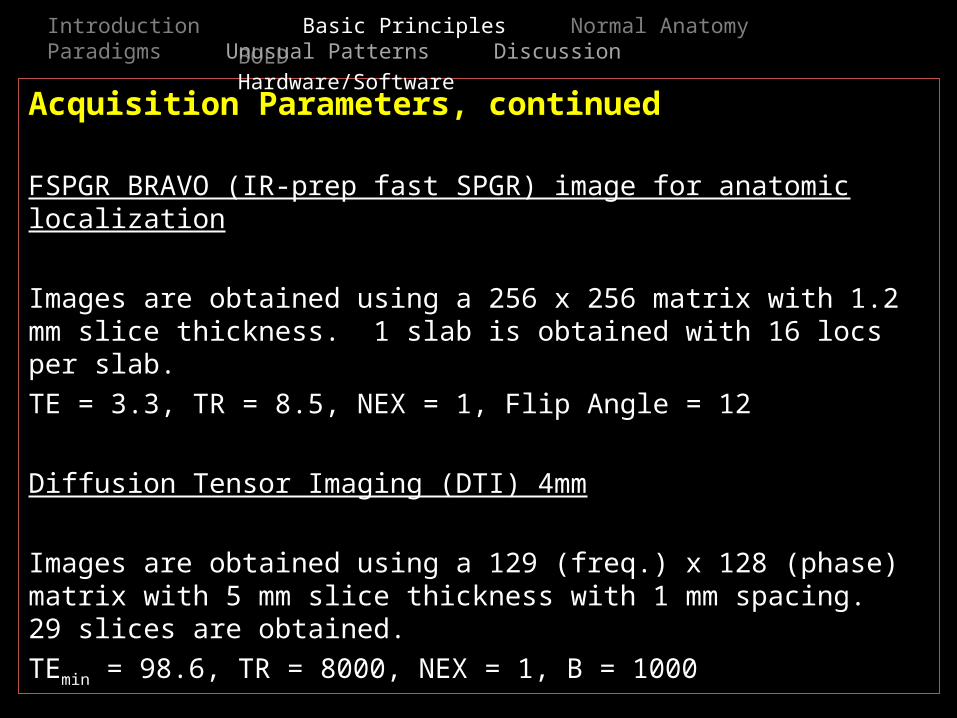
Faint Broca’s activation (blue arrow)
Hx: 60M left-handed semi-literate with right frontal glioblastoma multiforme(red arrow), preoperative evaluation.
Challenge: Semi-literate patient, able to recognize letters.
Solution: The patient was asked to think of any words that came to mind when he saw a letter on the screen, which resulted in faint Broca’s area activation. This was confirmed by language deficits after postoperative infarct in this region.
Word generation paradigm
DWI showing infarct
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion

_
Intense motor activity(blue arrow)
Hx: 70F right-handed with glioblastoma multiforme(red arrow) being evaluated prior to brain biopsy. fMRI demonstrated robust tongue activation.
Challenge: Separate tongue activity from language activity in Wernicke’s area.
Solution: Perform tongue movement paradigm first in order to localize tongue activity. This will help to differentiate activation of Wernicke’s area in case of inadvertent tongue movement during language generation paradigm.
Wernicke’s with arcuate fasciculus(yellow arrow)
Tongue movement paradigm Word generation paradigm
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion

_
Intense motor activity(blue arrow)adjacent to mass
Hx: 48M with limited reading capacity, with large left-sided mass(red arrow) for evaluation prior to resection. fMRI results influenced a change to conservative management.
Challenge 1: Left corticospinal tract not well visualized adjacent to mass.
Solutions: Review literature and consult experienced colleagues. The mass caused medialization of the left corticospinal tract and adjacent edema likely altered diffusivity rendering the fibers unapparent at the level of the motor strip.
Right and left corticospinal tracts(yellow arrows)
Partially visualized left corticospinal tract(yellow arrow)
Finger tapping paradigm
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion

_
Broca’s area(blue arrow) visualized using modified word generation paradigm
Hx: 48M with limited reading capacity, with large left-sided mass for evaluation prior to resection. fMRI results influenced a change to conservative management.
Challenge 2: Patient had limited ability to recognize letters.
Solution: Patient instructed to think of any word that came to mind regardless of letter presented in word generation paradigm.
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion

_Hx: 29M, right handed, with intractable epilepsy and left mesial temporal sclerosis, evaluation prior to amygdalohippocampectomy. This patient was able to undergo left-sided resection without postoperative language deficits.
Challenge: Language center not in the expected location.
Solution: Recognize normal anatomic variation. Approximately 5% of right handed patients can have right hemisphere language dominance. This was confirmed with a WADA test.
Broca’s area(blue arrow) on the right
Word generation paradigm
Wernicke’s area(yellow arrow) & arcuate fasciculus on right
Verb generation paradigm
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion

Discussion
-fMRI is becoming a standard tool in the preoperative evaluation of neurosurgical patients and can affect operative planning
-fMRI must be performed and interpreted in the context of the patient with attention to pre-existing deficits (i.e. level of literacy, prior insult, ability to follow directions)
-Unexpected patterns of activation can be challenging in a de novo fMRI program.
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion

Discussion
-Challenging cases we have encountered include bilateral, multiple or unexpected locations of language centers, and distortion of the usual anatomy. Additional history from the patient may be helpful.
-Varying levels of literacy or English language proficiency that render implementation of paradigms challenging. The operator must improvise to complete the paradigm. Performing object naming tasks or involvement of interpreters can assist in paradigm completion.
-Different paradigms are used to activate specific language centers(Brocas, Wernickes) however intensity and center of activation can be variable. Operator must utilize any available paradigms to obtain results useful for patient care.
-When in doubt, refer to the literature and consult with experienced colleagues.
Introduction Basic Principles Normal Anatomy Paradigms Unusual Patterns Discussion