The esophagus
81
-
Upload
masooma-alsharakhat -
Category
Health & Medicine
-
view
36 -
download
0
Transcript of The esophagus


THE ESOPHAGUS




المريء في أشباح

• * Esophagus is lined by stratified squamous epithelial tissue. (Interspersed in between Langerhans cells “phagocytes”).
• the role of esophagus is mainly mechanical transportation of ingested and partially digested food
• * It’s divided into 3 parts: upper, middle and lower.
• It is about 25 cm in length .
• C6 – T11


• Within the submucosa we can see glands (esophageal glands)>>> which is mostly secreting mucus (lubricating) and other pepsinogen and lysozymes for protection.
• Muscularis externa : inner circular and outer longitudinal
- Upper third: mostly striated ( 90%) - Middle third: mixed (50% striated , 50% smooth )- Lower third : entirely smooth

DISEASES OF THE ESOPHAGUS
• Congenital anatomic disorders– Agenesis, atresia, fistula, stenosis
• Acquired anatomic/motor disorders– Stenosis, webs & rings, HH, achalasia, ...
• Inflammations– Reflux esophagitis
• Barrett’s esophagus • Vascular diseases• Tumors
Most cases occurs at the lower part of the esophagus.
(metaplasia induced by acid exposure) is a specific disorder that is restricted to the esophagus

• ‐ The lower part of the esophagus is in contact with the upper part of stomach (cardiac part) at a junction known as “gastro esophageal ‐junction” which takes a Zigzag form “Z line”

2Lower part
This angle Works as anti
reflex ( protect the esophagus
from gastric juice)
Anatomic
junction
histological junction
Lower part of esophagus

Clinical Features Of Esophygeal diseases: terminology
• Dysphagia: difficulty in swallowingdue to mechanical narrowing or obstruction, tumor• Heartburnحرقة : retrosternal burning pain regurgitation of
gastric contents• Hematemesis: vomiting of blood• Melena:caused by excessive upper GIT bleeding, blood in
stools.>>dark• Hematochezia (fresh blood in the feces) if the
hemorrhage is severe. • severe inflammation, ulceration or lacerationتمزق • Respiratory symptoms: dyspnea, cough,..
>>aspiration: breathing in a foreign object

Congenital disorders of the esophagus:
• Present at birth with vomiting, aspiration (pneumonia, asphyxiaاختناق) and gastric distention.
• 1. Agenesis: Complete Loss of the esophagus. It’s very rare.

• 2. Atresia: Atresia is a condition in which an orifice or passage in the body is abnormally closed or absent
** Most common** Part of the esophagus is lost and replaced by thin
non canalized cord. ‐• Most commonly occurs near the tracheal
bifurcation.• ** Fistula (A connection between the trachea and esophagus due to failure of
separation)might be on the upper or lower part of the esophageal ligaments though commonly, it occurs at the lower part.
• ** Gases from the stomach will pass to trachea then to the LRT leading to pneumonia.

food
vomiting
gastric distention
aspiration

To remember
Tricuspid
atresia

• 3. Stenosis: • ** developmental defect resulting in partial
obstruction or narrowing of the esophageal lumen.
• **It may be due to neuronal or motor disorders
Treatment: Urgent medical and surgical intervention
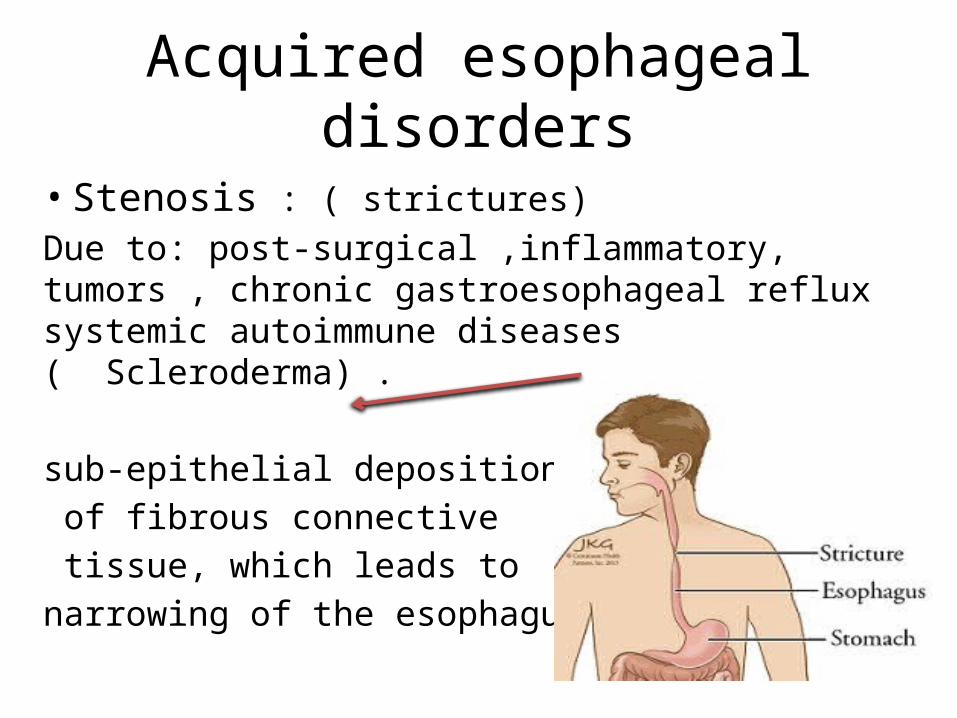
Acquired esophageal disorders
• Stenosis : ( strictures)Due to: post-surgical ,inflammatory, tumors , chronic gastroesophageal reflux systemic autoimmune diseases ( Scleroderma) .
sub epithelial deposition‐ of fibrous connective tissue, which leads to narrowing of the esophagus.

More illustration

• 2.Webs & rings: Mucosal or sub mucosal ‐protrusion in the esophagus in form of concentric rings, which partially occlude the esophagus.
• - most often in the upper esophagus.

• 3. Diverticula: Out pouching of the esophageal wall outside the esophageal lining .might be due to tumer or mechanical traction of the mucosa.
Food will accumulate here>>halitosis

ACQUIRED ANATOMIC/MOTOR DISORDERS OF THE ESOPHAGUS 4. HIATAL HERNIA
• Protrusion of a dilated sac-like segment of stomach above the diaphragm
• Separation of the diaphragmatic crura• Incidence; increase with age• Mostly asymptomatic• Some patient have: heartburn & regurgitation of
gastric juices due to LES incompetence; related to position; symptoms are accentuated by positions favoring reflux
• Patients with severe reflux esophagitis usually have HH;.>>>>>why?due to loss of the angle.

diaphragmatic crura (two fibromuscular bands that arise from the lumbar vertebrae and insert into the central tendon of the diaphragm).

Types of HH:
1. sliding (axial):• most common• Part of the stomach is located
above the diaphragm. bell‐shaped dilation(hourglass stomach).
• due to congenital short esophagus, strictures, spasm or long standing fibrous scarring of ‐esophagus. predisposing to gastroesophageal reflux
disease (GERD).

• 2. paraesophageal (non axial or ‐rolling):
• less common,• fundus protrudes into the thorax. • It’s due to traumatic rupture of
the diaphragm. • May lead to Strangulation and
infarction of that segment of the stomach due to the compression forced by the diaphragm on stomach.


• 5. Achalasia: ** Failure of relaxation

• * Normally, when we swallow there will be a relaxation in the LES. achalasia is a failure of doing that process which leads to functional obstruction and subsequent dilation of the proximal part of esophagus.
• characterized by a triade of (Abnormal manometric studies): (1) Incomplete relaxation of LES. (2) Aperistalsis. (3) Increase basal tone of LES.
https://www.youtube.com/watch?v=KtxuGwIoo5U
procedure for determining how the muscle of the esophagus and the sphincter (valve) works by measuring pressures (manometry) generated by the esophageal muscles and the sphincter.

• ** complications: • ‐ progressive dysphagia to liquids and solid
foods.• ‐ nocturnal regurgitation & aspiration of
undigested food, aspiration pneumonia. “respiratory symptoms”
Achalasia

Achalasia• Pathology: في innervation المشكلة• ‐ Defect in the inhibitory neurons of LES which
results in absence in myenteric ganglia in esophagus.
• ‐ Muscular tissue: may still normal, or try to compensate by Hypertrophy , or thin muscle.
• associated mucosal inflammation,ulcers and fibrosis , or bleeding are common due to the effect of stucke food.

Sphincter• Sphincter: a cylindrical muscle that normally
maintains constriction of a natural body passage or orifice which relaxes as required by normal physiological functioning.
• Anatomical sphincter: has a localized and often circular muscular thickening to facilitate its action as a sphincter. So there is a function with an anatomical structure, so the sphincter is built in. (a ring of muscle that contracts to close an opening) .

• Physiological sphincter: A sphincter that is not recognizable at an autopsy because its resting arrangement cannot be distinguished from adjacent tissue. Functional sphincters do not have this localized muscular thickening, however, they can achieve their action through muscle contractions around (extrinsic) the structure. So there is no built in sphincter (no structure). So in this case (Cardiac orifice) its function is coming from the right crus of diaphragm.
If we say anatomical sphincter we mean a structure and function, while if we say a sphincter is a physiologic sphincter we mean that it has a function without an intrinsic structure. So it’s redundant to say a sphincter is anatomic and physiologic sphincter.


** Types of Achalasia • 1. Primary: Unknown etiology, commoner. Can be related to autoimmune disease or previous viral
infection.
• 2. Secondary: degeneration in neural plexus ‐Chaga’s disease (mainly): Tryponosoma cruzi infection
causing destruction of myenteric plexus ganglion cells in the GIT (esophagus, dudenom and colon)& ureters leads to having: megaduodenum, megacolon, megaureter.
‐ Diabetes (Autonomic neuropathy); vagus nerve injury

** Patients with a history of having achalasia are at a higher risk of developing esophageal Squamous cell carcinoma.


6. LACERATIONS Mallory‐Weiss syndrome whiskey ;)
• ‐Longitudinal tears at the esophago gastric ‐junction.
• ‐Encountered in alcoholics due to repetitive vomiting and bulimics [ who force themselves to vomit after eating in order to lose weight !. But may occur in patients without history of repetitive vomiting.
• Pathogenesis: inadequate relaxation of LES muscle during vomiting.

LACERATIONS
• HH is found in 75% of patients with MWS• Linear irregular lacerations, few mm-cm in
length• Involve mucosa or deeply penetrate &
perforate wall
• 5-10% of all cases of massive hemetemesis; however, the majority do not cause profuse bleeding

LACERATIONS

• the postmortemالتشريح examination is of 2 types:
• 1- forensic postmortem : by forensic pathologists ,, for medico legal purposes.
• 2- hospital postmortem : to know the exact cause of death in hospitalized patients ,,
- EX: if our patient was alcoholic we are concerned with specific findings
- [ look for bleeding due to MWS , CNS damage , esophageal varices (EV) and liver cirrhosis (LC) as
they are the main complications in alcoholics

DISEASES OF THE ESOPHAGUS
• Congenital anatomic disorders– Agenesis, atresia, fistula, stenosis
• Acquired anatomic/motor disorders– Stenosis, webs & rings, HH, achalasia, ...
• Inflammations– Reflux esophagitis
• Barrett’s esophagus • Vascular diseases• Tumors

• Due to portal hypertension, which leads to formation of portal-systemic collateral bypass channels.
VASCULAR LESIONS OF THE ESOPHAGUSVARICES
as the veins in the systemic part of this anastomosis are not designed to handle this increased amount of blood , increased pressure will induce their diltation

https://www.youtube.com/watch?v=Cox6Z5pqMBo1;30
the sinusoids are compressed


1) Splenic vein.drains blood from spleen, pancreas and two stomach veins "Left gastroepiploic vein & Short gastric vein“(fundic v)..
2) Inferior mesentric vein. Drains blood from the hindgut (distal 1/3 of the transverse colon “left colic vein “until the upper 2/3 of the anal canal).” superior rectal vein”.

• 1) Venous blood from GIT goes to liver through the portal vein before going to the IVC. when there is a defect in the portal vein>>>>>>>>>>the blood can’t go to the liver
• Collateral veins will develop in the region of lower esophagus when portal flow is diverted through the coronary veins of stomach into the plexus of esophageal submucosal veins into azygous veins

• Most common cause of portal hypertension is liver cirrhosis
• Rare causes: portal vein thrombosis, hepatic vein thrombosis (Budd-Chiari syndrome), pylephlebitis, tumor compression or invasion into major portal radicals
*Develops in 2/3 of cirrhotic patients; accounts for 50% of deaths in liver cirrhosis
Irreversible End stage of chronic liver disease.
hepatitis C is the most common cause of cirrhosis.

chronic hepatitis
• is graded according to degree of fibrosis into :1. Portal (mild ) 2. Periportal 3. Bridging
(cirrhosis ).• Initially, the liver is yellow tan,fatty & enlarged• Eventually, it becomes brown, shrunken & non
fatty

• With excessive intake of alcohol, the liver switches over from the use of fats and carbohydrates as its primary "fuel" to the use of alcohol as its primary fuel.
• As alcohol-induced hepatitis progresses, the unused fat accumulates in the liver, causing the organ to change in color from a dark, reddish brown to a yellowish color that resembles nutmeg (hence the terms "nutmeg liver" or "fatty liver").
chronic hepatitis


Consequences of liver cirrhosis :• Portal hypertension which leads to :
hemorrhoids, esophageal varices, capot medusa ( all are at the portosystemic anastomosis)
• Splenomegaly• Charachtarised histologically by :1. Bridging fibrous septa ( delicate fibers between two portal tracts and between portal tracts and central veins)2. Paranchymal nodules ( which are regeneretive hepatocytes encircled by fibrous tissue )





Due to scratchy food :nuts ,…
• Asymptomatic until they rupture when massive hematemesis results; rupture may be spontaneous or secondary to vomiting; hemorrhage rarely subsides spontaneously; 40% die after 1st episode
• 70% of survivors will re-bleed within 1 year; mortality rate 40%
• *It’s very emergent case and should be treated even though the prognosis is very .
• bad balloon temponade is the way by which we can stop the bleeding in order to be able to perform the endoscopy
VASCULAR LESIONS OF THE ESOPHAGUSVARICES





INFLAMMATIONS OF THE ESOPHAGUS ESOPHAGITIS
• Caused by multiple factors:
– 1. Reflux of gastric contents (reflux esophagitis)– 2. Ingestion of irritants (alcohol, corrosive acids, alkali, excessive hot fluids like tea, heavy smoking).- Infective eosphagitis:measles, scarlet fever, diphtheria, typhoid– 3. Bacteremia & viremia with direct infection of esophageal wall or contiguous structures (HSV, CMV)– 4. Fungal infections in immunocompromised patients (Candidiasis, mucormycosis, aspergillosis)– 5. because the esophagus lining is squamous epithelium .>> Systemic
desquamative skin diseases (pemphigoid)– 6. Graft-versus-host disease– 7. Radiation; cytotoxic therapy; uremia


Oesophageal candidiasis Herpes simplex oesophagitis
characterized by multiple ulcers


Oesophagitis: Morson & Dawson, 5th ed, 2012• Reflux• Infective oesophagitis
herpes simplex CMV candidiasis immunocompetent: measles, scarlet fever, diphtheria &
typhoid immunoparetic: HIV, HZV, HPV, HHV6, varied bacteria
& fungi• Pill oesophagitis: ferrus sulfate, (tetracyclines), NSAIDs, drugs used for
osteoporosis]-- risk factors includes [elderly, diabetes, women (M:F = 1:2) ]• Sloughing oesophagitis• Eosinophilic oesophagitis• Radiation oesophagitis• Chagas disease


1. Reflux of gastric contents (reflux esophagitis)
• including some refluxed contents from the intestines (bile, bile salts, bile acids).
• Predisposing factors:– Fat, chocolate, alcohol, smoking– Hiatal hernia– Pregnancy (increases the abdominal pressure)– Drugs

• the main pathological/histological finding for Reflux Esophagitis is: basal zone hyperplasia and the presence of intra-epithelial eosinophils&/or PMNs.



ESOPHAGEAL TUMORS
• Benign tumors are rare: leiomyoma is the most common, and is usually ,asymptomatic and discovered incidentally.
• Malignant tumors- More common in males (M:F=3:1).

SQUAMOUS CELL CARCINOMA
• The most common malignant tumor of esophagus.
• has a higher contribution to mortality, why? (asymptomatic with late diagnosis).
• Patients: most patients are adults >50 years.• Higher incidence in blacks than whites.


Esophageal cancers often spreadto surrounding structures, making surgical removal difficult.
infiltrating nests of neoplastic cellshave abundant pink cytoplasm and distinct cell borders typical for squamous cell carcinoma.

• Associated factors/Risk factors:- 1) Dietary:- Fungal contamination of food by Aspergillus, High content of nitrites/ nitrosamines, Deficiency of vitamins (A, C, riboflavin, thiamin), Deficiency of trace metals (zinc, molybdenum).- 2) Esophageal disease: achalasia, reflux
esophagitis , strictures, Plummer-Vinson syndrome.
- 4) genetic predisposition: celiac disease,Tylosis.

• Pathology:- 50% of the cases happen in middle third of the
esophagus, 30% in lower third and 20% in upper third.
• Prognosis: 70% die within 1 year, 5 years survival 5-10% (poor prognosis).
full thickness dysplasia and invasion of the sub mucosa

SQUAMOUS CELL CARCINOMA

ADENOCARCINOMA
• Middle or lower third; may extend to stomach
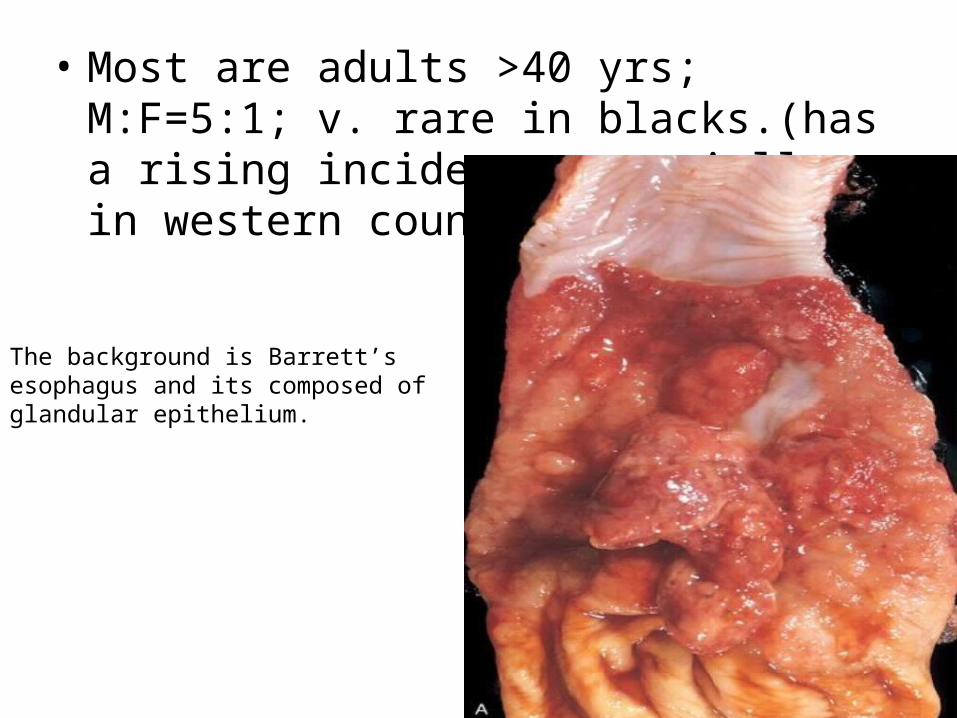
• Most are adults >40 yrs; M:F=5:1; v. rare in blacks.(has a rising incidence especially in western countries).
The background is Barrett’s esophagus and its composed of glandular epithelium.