
the eosinophil and peripartum heart disease ! myocarditis and
6
ELSEVIER Cardiovascular Research 33 (1997) 527-532 Gwdiovascular Research Review Review and hypothesis: the eosinophil and peripartum heart disease ! myocarditis and coronary artery dissection) -coincidence or pathogenetic significance? Alain C. Borczuk a, * , Karen H. van Hoeven b, Stephen M. Factor a a Department of Pathology, Albert Einstein College of Medicine, Bronx, NY, USA b Department of Pathology, Thomas Jefferson Unirer.~ity, Philadelphia, PA, USA Received 9 May 1996;accepted 2 I October 1996 Abstract Objectives: To examine a possible relationship between peripartum heart disease (myocarditis and spontaneous coronary dissection) and the presence of eosinophils. Background: Eosinophils have been shown to have potential collagenolytic and cytotoxic activity. Eosinophils may play a role in postpartum uterine involution. The presence of eosinophils in spontaneous coronary dissection and myocarditis in the postpartum period raises the possibility of a role for eosinophils in these diseases. Methods: We reviewed the files of one of us (S.M.F.) for cases of peripartum myocarditis and spontaneous coronary dissection and assessed the frequency of eosinophilic inflammation. Seventeen postpartum myocarditis and/or cardiomyopathy cases were found and two spontaneous coronary dissections. Fifteen sex- and age-matched controls on non-postpartum myocarditis and borderline myocarditis were evaluated and eosinophil counts per unit area compared. Also, a Medline search of all previously published cases of spontaneous coronary dissection was performed back to 1966. Results: Of the 16 heart biopsies and one autopsy in the peripartum period, 10 were shown to contain easily identified eosinophils (6 myocarditis, 1 borderline, 3 cardiomyopathy). When presence of eosinophils was compared with the control group, a statistically significant difference was obtained (P = 0.036). The two new spontaneous coronary dissection cases had eosinophils along the dissection plane; the literature search produced 13 of 24 autopsied peripartum spontaneous coronary dissections with eosinophils for a total of 15 of 26 with our cases. Conclusions: An association exists between eosinophils and peripartum cardiac disease (myocarditis and spontaneous coronary dissection). The role of eosinophils in labor, uterine involution and collagenolysis and the possible relation to cardiac disease are discussed. Keywords: Eosinophils; Peripartum heart disease;Spontaneous coronary dissection: Myocarditis 1. Introduction and results The etiology and pathogenesis of peripartum heart dis- ease is unknown. By generally accepted definitions the condition represents the onset of cardiac failure occurring during the last trimester of pregnancy through the first 6 months post partum [l]. Among proposed etiologies, hypersensitivity to fetal antigens has been suggested, al- though there is no evidence to support this hypothesis [2]. It is likely that there are multiple etiologies, with at least some cases representing the ‘unmasking’ of prior subclini- cal cardiac damage. Myocardial injury secondary to hyper- tension, eclampsia, and anemia also may play a role. In a recent series of 13 cases of peripartum heart disease from our institution [3], 7 had evidence of active myocarditis, established by endomyocardial biopsy. Two additional biopsied myocarditis cases were identified re- cently (one of which is shown in Fig. 1 A), and a case of sudden death in a 31 year old woman approximately nine months peripartum also was found to have myocarditis ’ Corresponding author. Jacobi Medical Center, Van Etten Hospital, Department of Pathology, Room 6C-3, Morris Park and Seminole Av- enue, Bronx, NY 10461, USA. Tel. + 1 718 918-4803; Fax + 1 718 9 I g-4809. Time for primary review 16 days. 0008-6363/97/$17X10 Copyright 0 1997 Elsevier Science B.V. All rights reserved PI1 SOOOX-6363(96)00257-X Downloaded from https://academic.oup.com/cardiovascres/article/33/3/527/2462566 by guest on 07 January 2022
Transcript of the eosinophil and peripartum heart disease ! myocarditis and

ELSEVIER Cardiovascular Research 33 (1997) 527-532
Gwdiovascular Research
Review
Review and hypothesis: the eosinophil and peripartum heart disease ! myocarditis and coronary artery dissection) -coincidence or
pathogenetic significance?
Alain C. Borczuk a, * , Karen H. van Hoeven b, Stephen M. Factor a a Department of Pathology, Albert Einstein College of Medicine, Bronx, NY, USA b Department of Pathology, Thomas Jefferson Unirer.~ity, Philadelphia, PA, USA
Received 9 May 1996; accepted 2 I October 1996
Abstract
Objectives: To examine a possible relationship between peripartum heart disease (myocarditis and spontaneous coronary dissection) and the presence of eosinophils. Background: Eosinophils have been shown to have potential collagenolytic and cytotoxic activity. Eosinophils may play a role in postpartum uterine involution. The presence of eosinophils in spontaneous coronary dissection and myocarditis in the postpartum period raises the possibility of a role for eosinophils in these diseases. Methods: We reviewed the files of one of us (S.M.F.) for cases of peripartum myocarditis and spontaneous coronary dissection and assessed the frequency of eosinophilic inflammation. Seventeen postpartum myocarditis and/or cardiomyopathy cases were found and two spontaneous coronary dissections. Fifteen sex- and age-matched controls on non-postpartum myocarditis and borderline myocarditis were evaluated and eosinophil counts per unit area compared. Also, a Medline search of all previously published cases of spontaneous coronary dissection was performed back to 1966. Results: Of the 16 heart biopsies and one autopsy in the peripartum period, 10 were shown to contain easily identified eosinophils (6 myocarditis, 1 borderline, 3 cardiomyopathy). When presence of eosinophils was compared with the control group, a statistically significant difference was obtained (P = 0.036). The two new spontaneous coronary dissection cases had eosinophils along the dissection plane; the literature search produced 13 of 24 autopsied peripartum spontaneous coronary dissections with eosinophils for a total of 15 of 26 with our cases. Conclusions: An association exists between eosinophils and peripartum cardiac disease (myocarditis and spontaneous coronary dissection). The role of eosinophils in labor, uterine involution and collagenolysis and the possible relation to cardiac disease are discussed.
Keywords: Eosinophils; Peripartum heart disease; Spontaneous coronary dissection: Myocarditis
1. Introduction and results
The etiology and pathogenesis of peripartum heart dis- ease is unknown. By generally accepted definitions the condition represents the onset of cardiac failure occurring during the last trimester of pregnancy through the first 6 months post partum [l]. Among proposed etiologies, hypersensitivity to fetal antigens has been suggested, al- though there is no evidence to support this hypothesis [2].
It is likely that there are multiple etiologies, with at least some cases representing the ‘unmasking’ of prior subclini- cal cardiac damage. Myocardial injury secondary to hyper- tension, eclampsia, and anemia also may play a role.
In a recent series of 13 cases of peripartum heart disease from our institution [3], 7 had evidence of active myocarditis, established by endomyocardial biopsy. Two additional biopsied myocarditis cases were identified re- cently (one of which is shown in Fig. 1 A), and a case of sudden death in a 31 year old woman approximately nine months peripartum also was found to have myocarditis
’ Corresponding author. Jacobi Medical Center, Van Etten Hospital, Department of Pathology, Room 6C-3, Morris Park and Seminole Av- enue, Bronx, NY 10461, USA. Tel. + 1 718 918-4803; Fax + 1 718 9 I g-4809. Time for primary review 16 days.
0008-6363/97/$17X10 Copyright 0 1997 Elsevier Science B.V. All rights reserved PI1 SOOOX-6363(96)00257-X
Dow
nloaded from https://academ
ic.oup.com/cardiovascres/article/33/3/527/2462566 by guest on 07 January 2022
528 A.C. Borczuk et al. /Cardiovascular Research 33 (1997) 527-532
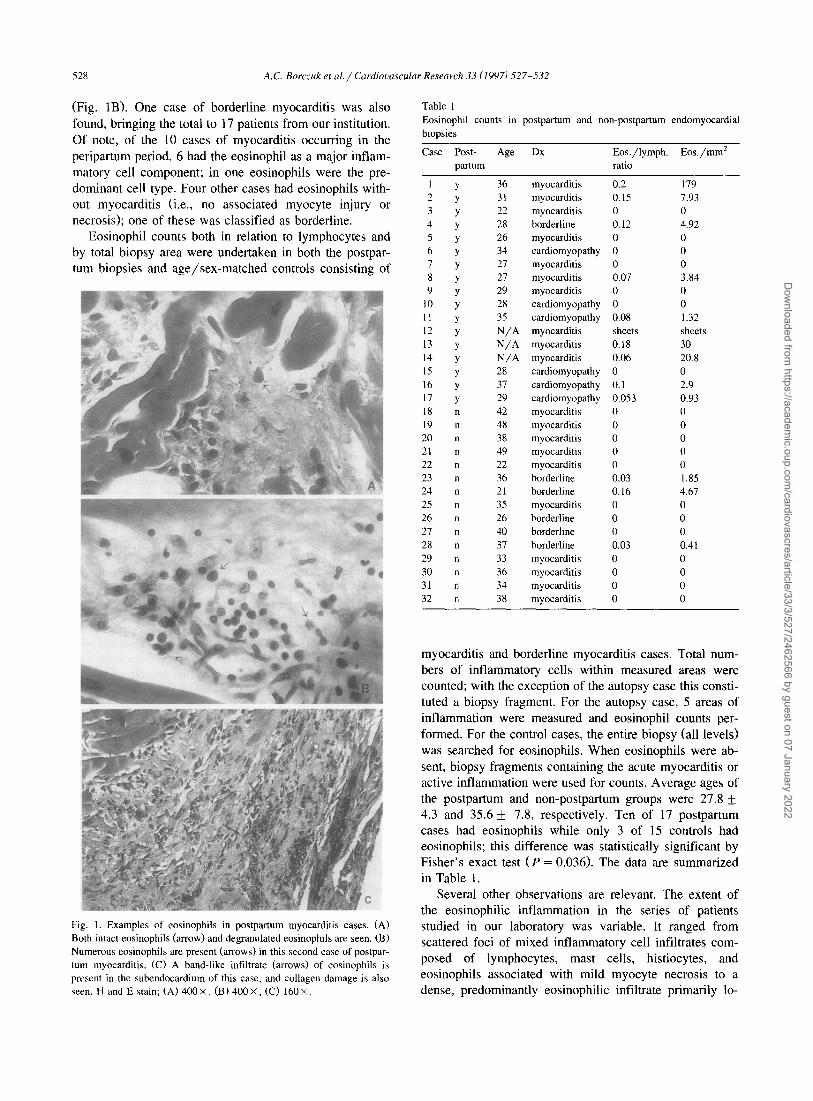
(Fig. 1B). One case of borderline myocarditis was also found, bringing the total to 17 patients from our institution. Of note, of the 10 cases of myocarditis occurring in the peripartum period, 6 had the eosinophil as a major inflam- matory cell component; in one eosinophils were the pre- dominant cell type. Four other cases had eosinophils with- out myocarditis (i.e., no associated myocyte injury or necrosis); one of these was classified as borderline.
Eosinophil counts both in relation to lymphocytes and by total biopsy area were undertaken in both the postpar- tum biopsies and age/sex-matched controls consisting of
Fig. I. Examples of eosinophils in postpartum myocarditis cases. (A) Both intact eosinophils (arrow) and degranulated eosinophils are seen. (B) Numerous eosinophils are present (arrows) in this second case of postpar- tum myocarditis. (C) A band-like infiltrate (arrows) of eosinophils is present in the subendocardium of this case, and collagen damage is also seen. H and E stain; (A) 400 X , (B) 400 X , (C) 160 X
Table 1 Eosinophil counts in postpartum and non-postpartum endomyocardial biopsies
Case Post- Age Dx Eos./lymph. Eos./mm’ partum ratio
1 2 3 4 5 6 I 8 9
10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 21 28 29 30 31 32
Y
n n n n n n n n n n n n
n
36 myocarditis 0.2 179 31 myocarditis 0.15 1.93 22 myocarditis 0 0 28 borderline 0.12 4.92 26 myocarditis 0 0 34 cardiomyopathy 0 0 27 myocarditis 0 0 21 myocarditis 0.07 3.84 29 myocarditis 0 0 28 cardiomyopathy 0 0 35 cardiomyopathy 0.08 1.32
N/A myocarditis sheets sheets
N/A myocarditis 0.18 30
N/A myocarditis 0.06 20.8 28 cardiomyopathy 0 0 31 cardiomyopathy 0.1 2.9 29 cardiomyopathy 0.053 0.93 42 myocarditis 0 0 48 myocarditis 0 0 38 myocarditis 0 0 49 myocarditis 0 0 22 myocarditis 0 0 36 borderline 0.03 1.85 21 borderline 0.16 4.67 35 myocarditis 0 0 26 borderline 0 0 40 borderline 0 0 31 borderline 0.03 0.41 33 myocarditis 0 0 36 myocarditis 0 0 34 myocarditis 0 0 38 myocarditis 0 0
myocarditis and borderline myocarditis cases. Total num- bers of inflammatory cells within measured areas were counted; with the exception of the autopsy case this consti- tuted a biopsy fragment. For the autopsy case, 5 areas of inflammation were measured and eosinophil counts per- formed. For the control cases, the entire biopsy (all levels) was searched for eosinophils. When eosinophils were ab- sent, biopsy fragments containing the acute myocarditis or active inflammation were used for counts. Average ages of the postpartum and non-postpartum groups were 27.8 + 4.3 and 35.6 & 7.8, respectively. Ten of 17 postpartum cases had eosinophils while only 3 of 15 controls had eosinophils; this difference was statistically significant by Fisher’s exact test (P = 0.036). The data are summarized in Table 1.
Several other observations are relevant. The extent of the eosinophilic inflammation in the series of patients studied in our laboratory was variable. It ranged from scattered foci of mixed inflammatory cell infiltrates com- posed of lymphocytes, mast cells, histiocytes, and eosinophils associated with mild myocyte necrosis to a dense, predominantly eosinophilic infiltrate primarily lo-
Dow
nloaded from https://academ
ic.oup.com/cardiovascres/article/33/3/527/2462566 by guest on 07 January 2022

A.C. Borczuk et al. / Cardiooascular Research 33 (1997) 527-532 529
calized to the subendocardium. The latter case was particu- larly noteworthy because of the band-like infiltrate (Fig. 1C) between the endocardial surface and the myocardium with degradation of subendocardial collagen noted. Even when localized, however, the inflammation tended to have an interstitial predominance with focal connective iissue dissolution.
The lack of continued cardiac damage and frequent improvement in cardiac functional class among peripartum cardiomyopathy have been noted [3-61. When compared to idiopathic dilated cardiomyopathy, improvements in ejec- tion fraction and survival have been shown for peripartum cardiomyopathy. Such improvement is also seen in the acute myocarditic state [7]. This improvement in function indicates that some of the initial insult is reversible, and suggests that damage is neither ongoing nor specifically directed against the myocyte.
The association of eosinophilic myocarditis with peri- partum heart disease may be coincidence, or it may repre- sent a previously underrecognized association. Addition- ally, it may be a clue to the pathogenesis of the condition.
I. 1. Spontaneous coronary dissection
Since the original description of this disease in 193 1 [8], spontaneous coronary dissection has been a disease pre- dominantly of women with a predilection for the peripar- turn period. Although initially described in postmortem series, prognosis in those surviving the acute event was good (85%) [9]. Improved angiographic detection and treatment with thrombolytic agents, angioplasty or coro- nary artery bypass grafting has improved antemortem de- tection and survival; the recent literature reflects this im- provement [lO,l 11. In fact, a recent review of postpartum dissection revealed a 66% mortality overall and a high rate of survival after surgical intervention [ 121.
We performed a Medline search for all cases of sponta- neous coronary dissection back to 1966; with the addition of a case from our institution (Fig. 2A) and a case seen in consultation by one of us (S.M.F.), a total of 144 cases (plus approximately 11 from French, German and Japanese journals) have been reported [9-371. Of these, 106 were female (75%), and 37 were peripartum (35% of females). The average age was 39.2 overall; the average age for females was 38.8. Twenty-four of 37 postpartum women expired and were autopsied; of these, eosinophils were mentioned as a prominent part of the inflammatory infil- trate in 13. The involved vessels included 5 right coronary, 21 left anterior descending, 5 left main and 1 left circum- flex coronary arteries. This is consistent with the observa- tion that male disease is right-sided and female disease predominantly left-sided [9].
Eosinophils were also mentioned in autopsied cases that were not in the peripartum period. Sixty cases were autop- sied and of those, 27 reported eosinophils among the inflammatory infiltrate.
Fig. 2. (A) A gross cross-section of a spontaneous coronary dissection with luminal compression by outer media/adventitial blood accumula- tion. (B) A section of artery from (A) showing that the plane of cleavage histologically is at the media/adventitial interface. EVG (B): 25 X
The histology of spontaneous coronary dissection in association with an inflammatory infiltrate generally shows periadventitial inflammation involving vasa vasorum. The dissection occurs in the outer l/3 of the media of the vessel (Fig. 2B); in some cases a relationship with an intimal tear has been reported. The lumen of the vessel becomes compressed by expansion of the media (Fig. 2A). Some cases have shown cystic medial degeneration with dissection [37], but this is not a consistent feature. The autopsied peripartum cases report an eosinophilic infiltrate in over 50% of the dissections (15 of 26).
The location of the dissection raises the possibility that collagen damage may be responsible for weakening the vessel wall and creating the setting for dissection. The associated inflammatory infiltrate, although previously de- scribed as probably reactive [32], usually involves the adventitia including vasa vasorum. Is the eosinophil a potential source of damaging substances, and can the pregnant or postpartum state contribute to eosinophil acti- vation, thereby setting up a higher risk environment for dissection?
1.2. Discussion
Eosinophils are present in a significant subset of cases of peripartum cardiomyopathy (both with and without
Dow
nloaded from https://academ
ic.oup.com/cardiovascres/article/33/3/527/2462566 by guest on 07 January 2022

530 A.C. Borczuk et al. / Cardiovascular Research 33 (19971 527-532
myocarditis) as well as in peripartum spontaneous coro- nary dissections. The presence of eosinophils in the latter condition has been interpreted in various, albeit completely opposite, ways. It has been suggested that eosinophils represent a reactive, secondary phenomenon rather than an etiologically significant one, since eosinophils are absent in so many cases [32]. It could be argued, however, that absence of eosinophils in some cases reflects a different mechanism leading to collagen abnormality. Collagen de- fects may play a role in some cases, and the damage to collagen in others may be multifactorial. A case report of a coronary dissection in a patient with Ehlers-Danlos Type IV [38] as well as a report showing an in vitro impairment in collagen synthesis in tissue obtained from a case of postpartum coronary dissection [39] support heterogeneous causes for a collagen abnormality resulting in dissection.
The localization of the eosinophils to the plane of cleavage and the existence of tissue damaging eosinophil granule components [40] has been used as evidence to implicate the eosinophil in the process of coronary dissec- tion. The importance of eosinophils in this process has subsequently been supported by 3 cases of dissection with underlying eosinophilic syndromes (2 males, 1 female): one with drug-induced hypereosinophilia [16], one with Churg-Strauss syndrome [3 11, and one with marked periph- eral eosinophilia [27]. In the third case, dissection was associated with cardiomyopathy.
Eosinophil granules contain a variety of substances including a collagenase that cleaves type I and III collagen, peroxidase [41], major basic protein, acid phosphatase, alkaline phosphatase, aryl sulphatase, ribonuclease and P-glucuronidase. Major basic protein is cytotoxic and is known to be associated with myocyte damage [42]. Eosinophil levels have been shown to be higher in cases of cardiac rupture [43], although it is unclear what specific component is contributed by eosinophils. In a recent study of eosinophilic myocarditis (one Churg-Strauss, one hyper- sensitivity to ranitidine), a close interaction of eosinophils and degraded collagen was noted ultrastructurally; in addi- tion, eosinophil granule components were detected within collagen [44]. These findings support the potentially dam- aging effects of eosinophils; the question that remains is why eosinophils may be associated with the postpartum period.
As noted in our postpartum cardiac diseases, including cardiomyopathy, myocarditis and spontaneous coronary dissection, eosinophils are present. Although circulating and uterine eosinophils are dramatically reduced during pregnancy [45], parturition and the postpartum period are characterized first by cervical eosinophilic infiltration. This is followed by collagen remodeling, then eosinophil uter- ine infiltration (along with other inflammatory cells) with subsequent collagenolysis and involution (as described be- low). Although the source of uterine collagenase appears to be the smooth muscle cell [46], the presence of eosinophils seems to at least ‘herald’ the collagenolysis.
Their involvement may be to prepare the tissue in some way for collagenolysis, or to remove a potential inhibitor of collagenolysis (e.g., eosinophil degranulation causes estrogen breakdown [47]; estrogen is a known inhibitor of collagenolysis [48]).
2. Hypothesis
The onset of labor and the subsequent postpartum pe- riod is a time of intense remodeling of the cervix and uterus. Important events take place in the hormonal milieu as uterine involution occurs with the eventual return of normal menses. The eosinophil is clearly sensitive to, if not actually involved in, steroid-hormone-mediated events [49]. In addition, the degranulation of already migrated eosinophils can be induced by estrogen [50] and under some circumstances progesterone [5 I], releasing granules that contain a variety of hydrolytic substances including collagenase.
The postpartum period in rats is notable for striking changes in hormone levels; these are required for success- ful uterine involution. Progesterone decreases before deliv- ery to reach a nadir 24 h postpartum [52]. Plasma estrogen rises suddenly and transiently at birth [45], and by 1 day postpartum is low again. Low levels of both hormones are needed for successful involution and administration of either hormone impedes the process [53]. This control of involution seems to be related to levels of collagenase activity. Serum levels of collagenase, while quiescent dur- ing pregnancy, rapidly increase during labor (66%) and then again after 24 h postpartum, an elevation that persists for about 4 days [54].
The eosinophil has been shown to be influenced by these events. In the cervix, eosinophils heavily infiltrate during parturition in the rat, and ultrastructural examina- tion of the cervix shows degranulated eosinophils and collagen breakdown [52]. In studies on uterine regression in the rat uterus, Tansey and Padykula showed that early normal uterine regression involved infiltration by polymor- phonuclear cells, macrophages, eosinophils and lympho- cytes with eosinophils present in the deep stroma [53]. As involution progressed and collagen changes were seen, eosinophils and polymorphonuclear cells disappeared and macrophages predominated. When gestation was pro- longed by exogenous progesterone, eosinophil levels did not increase. When progesterone was administered after parturition, deep stromal eosinophilic infiltration was de- creased as was collagen breakdown in that area. It seems that eosinophils migrate into areas that subsequently are remodeled.
The presence of eosinophils in postpartum cardiac dis- ease may be a systemic reflection of events that are taking place in uterine involution. Migration and diapedesis of eosinophils are occurring, and localization in the coronary arteries and myocardium may be a phase of a normal
Dow
nloaded from https://academ
ic.oup.com/cardiovascres/article/33/3/527/2462566 by guest on 07 January 2022

A.C. Borczuk et al. / Cardiooascular Research 33 (1997) 527-532 531
process or may represent an idiosyncratic pathological response. Subsequent tissue damage may be due to inap- propriate eosinophil degranulation, release of eosinophil collagenase or major basic protein following restoration of steroid hormones after uterine involution, or may result from circulating collagenases that are measurable postpar- tum acting on tissue sensitized by the eosinophil. A less likely possibility is that, like the smooth muscle cell of the uterus, vascular smooth muscle can synthesize a collage- nase that, under the conditions that exist post partum (prior eosinophil ‘preparation’), leads to adventitial degradation. The weakening of the adventitia may enhance the suscepti- bility to dissection.
3. Conclusion
Eosinophils may be present and activated because of the systemic hormonal perturbations occurring during the pe- riod of uterine involution. Remodeling occurring in the uterus may cause systemic changes that produce a period of susceptibility to spontaneous coronary dissection; hemo- dynamic changes or other precipitating factors may be needed to produce dissection in that window period. Eosinophil damage to myocytes may cause cardiomyopa- thy; the improvement in peripartum cardiomyopathy over time suggests a temporally limited event related to preg- nancy. The role of the eosinophil is still unknown, but its presence and potential for damaging effects in two postpar- tum disease states raise the possibility that eosinophils are active participants rather than innocent bystanders.
References
[I] Demakis JG, Rahimtoola SH. Peripartum cardiomyopathy. Circula- tion 197 1;44:964-968.
[2] Midei MG, DeMent SH, Feldman AM, Hutchins GM, Baughman KL. Peripartum myocarditis and cardiomyopathy. Circulation I990;8 1:922-928.
[3] van Hoeven KH, Kitsis RN, Katz SD, Factor SM. Peripartum versus idiopathic cardiomyopathy in young women - a comparison of clinical, pathologic and prognostic features. Int J Cardiol 1993;40:57-65.
[4] O’Connell JB, Costanzo-Nordin MR, Subramanian R, et al. Peripar- turn cardiomyopathy: clinical, hemodynamic, histologic, and prog- nostic characteristics. J Am Co11 Cardiol 1986;8:52-56.
[5] Meadows WR. Idiopathic myocardial failure in the last trimester of pregnancy and the puerperium. Circulation 1957;15:903-914.
[6] Demakis JG, Rahimtoola SH, Sutton GC, et al. Natural course of peripartum cardiomyopathy. Circulation 1971;44:1053- 1061.
[7] Remes J, Helin M, Vaino P, Rautio P. Clinical outcome and left ventricular function 23 years after acute Coxsackie virus myoperi- carditis. Eur Heart J 1990;11:182-188.
[8] Pretty HC. Dissecting aneurysm of a coronary artery in a woman aged 42. Br Med J 1931:1:667.
[9] DeMaio SJ, Kinsella SH, Silverman ME. Clinical course and long term prognosis of spontaneous coronary artery dissection. Am J Cardiol 1989;64:47 I-474.
[IO] Wellford LA, Kelly TM. Survival with acute primary coronary
artery dissection: a case report and review of the literature. J Emerg Med 1993;12:193-198.
[ 1 l] Jorgensen MB, Aaronian V, Mansukhani P, Mahrer PR. Sponta- neous coronary dissection: a cluster of cases with this rare finding. Am Heart J 1994;127:1382-1387.
[ 121 Engelman DT, Thayer J, Derossi J, Schineman J, Brown L. Preg- nancy related coronary artery dissection: a case report and collective review. Conn Med 1993;57 I : 135- 139.
[13] Virmani R, Forman MB, Robinowitz M, McAllister HA. Coronary artery dissections. Cardiol Clin 1984;2:633-646.
[I41 Emori T, Goto Y, Maeda T, Chiba Y, Haze K. Multiple coronary artery dissections diagnosed in vivo in a pregnant woman. Chest 1993; 104:289-290.
[15] Himbert D, Makowski S, Laperche T, Steg PG, Juliard JM, Gourgon R. Left main coronary spontaneous dissection: progressive angio- graphic healing without coronary surgery. Am Heart J 1991;122:1757-1759.
[ 161 Saunders SL, Ford SE. Primary coronary dissection possibly related to drug hypersensitivity in a male. Can J Cardiol 1991;7:138-140.
[ 171 Behnam R, Tillinghast S. Thrombolytic therapy in spontaneous coronary dissection. Clin Cardiol 1991; 14:61 l-614.
[ 181 Madu EC, Kosinski DJ, Wilson WR, Burket MW, Fraker TD, Ansel GM. Two vessel coronary artery dissection in the peripartum period. Case report and literature review. Angiology 1994;45:809-8 16.
[19] Siegel RJ, Koponen M. Spontaneous coronary artery dissection causing sudden death. Mechanical arterial failure or primary vasculi- tis? Arch Path01 Lab Med 1994;118:863-864.
[20] Verkaaik AP, Visser W, Deckers JW, Lotgering FK. Multiple coronary artery dissections in a woman at term. Br J Anaesth 1993;71:301-302.
[21] Burkey D, Love J, Fanning J, Lambrew C. Multiple spontaneous coronary artery dissections in a middle aged woman: support for an underlying eosinophilic arteritis predisposing to intimal disruption. Catheter Cardiol Diagn 1993;30:303-305.
[22] Ellis CJ, Haywood GA, Monro JL. Spontaneous coronary dissection in a young woman resulting from an intense gymnasium ‘workout’. Int J Cardiol 1994;47: 1!)3-194.
[23] Keamey P, Singh H, Hutter J. Khan S, Lee G, Lucey J. Spontaneous coronary artery dissection: a report of three cases and review of the literature. Postgrad Med J 1993;69(818):940-945.
[24] Gonzalez JI, Hill JA, Conti CR. Spontaneous coronary artery dissec- tion treated with percutaneous transluminal angioplasty. Am J Car- diol 1989;63:885-886.
[25] Sage MD, Koelmeyer TD, Smeeton WM. Fatal postpartum coronary artery dissection. A light and electron microscope study. Am J Foren Med Pathol 1986:7:107--I I 1.
[26] Wisecarver J, Jones J, Goaley T, McManus B. Spontaneous coro- nary artery dissection. The challenge of detection, the enigma of cause. Am J Foren Med Pathol 1989;10:60-62.
[27] Huikuri HV. Mallon SM, Myerburg RJ. Cardiac arrest due to spontaneous coronary artery dissection in a patient with coronary ectasia - a case report. Angiology 1991:42:148-151.
[28] Corrado D, Thiene G, Cocco P, Frescura C. Non-atherosclerotic coronary disease and sudden death in the young. Br Heart J 1992;68:601-607.
[29] Pasalodos PJ, Vasquez. Gonzalez N, Perez Alvarez L, Vazquez Rodriquez JM, Castro Beiras A. Spontaneous coronary artery dissec- tion. Catheter Cardiol Diagn 1994;32:27-32.
[30] Parry R, MacConnell T, Wilde P. Case report: spontaneous coronary artery dissection, Clin Radio1 1994;49: 142- 143.
[31] Hunsaker JC, O’Connor WN, Lie JT. Spontaneous coronary dissec- tion and isolated eosinophilic coronary arteritis: sudden cardiac death in a patient with limited variant of Churg-Strauss syndrome. Mayo Clin Proc 1992;67:761-766.
[32] Dowling GP, Buja LM. Spontaneous coronary artery dissection occurs with and without periadventitial inflammation. Arch Pathol Lab Med 1987: 1 I 1:470-472.
Dow
nloaded from https://academ
ic.oup.com/cardiovascres/article/33/3/527/2462566 by guest on 07 January 2022

532 A.C. Borczuk et al. /Cardiovascular Research 33 (1997) 527-532
[33] Lie JT, Berg KK. Isolated fibromuscular dysplasia of the coronary arteries with spontaneous dissection and myocardial infarction. Hum Path01 1987;18:654-656.
[34] Keon WJ, Koshal A, Boyd WD, Laramee L, Farrell E, Walley VM. Survival after spontaneous primary left main coronary artery dissec- tion. Acute surgical intervention with the Jarvik 7-70 artificial heart. J Cardiovasc Surg 1989;30:786-789.
[35] Shioi K, Nagata Y, Tsuchioka H. Spontaneous coronary artery dissection with left ventricular aneurysm - a case report of success- ful surgical repair. Thor Card Surg 1989;37:324-326.
[36] Bateman AC, Gallagher PJ, Vincenti AC. Sudden death for coronary artery dissection. J Clin Path01 1995;48:781-784.
[37] Smith JC. Dissecting aneurysms of coronary arteries. Arch Path01 1975:99:117-121.
[44] Kendell KR, Day JD, Hruban RH, et al. Intimate association of eosinophils to collagen bundles in eosinophilic myocarditis and ranitidine induced hypersensitivity myocarditis. Arch Path01 Lab Med 1995;119:1154-1160.
[45] Rebar RW, Nakane PK, Midgley AR. Postpartum release of luteiniz- ing hormone in the rat as determined by radioimmunoassay. En- docrinol 1969;84:1352-1358.
[46] Blair HC, Teitelbaum SL Ehlich LS, et al. Collagenase production by smooth muscle: correlation of immunoreactivity with functional enzyme in the myometrium. J Cell Physiol 1986:129: 1 1 l- 123.
[47] Klebanoff SJ. Inactivation of estrogen by rat uterine preparations. Endocrinology 1965;76:301-3 10.
[38] Ades LC, Waltham RD, Chiodo AA, Bateman JF. Myocardial infarction resulting from coronary artery dissection in an adolescent with Ehlers-Danlos type IV due to a type III collagen mutation. Br Heart J 1995;74:112-116.
[48] Woessner JF, Ryan JN. Effect of estradiol on the postpartum rat uterus: peroxidase activity and collagen breakdown. J Endocrinol 1980;85:387-391,
[39] Bonnet J, Aumailley M, Thomas D, Grosgogeat Y, Broustet JP, Bricaud H. Spontaneous coronary artery dissection - case report and evidence for a defect in collagen metabolism. Eur Heart J 1986:7:904-909.
[40] Robinowitz M, Virmani R, McAllister HA. Spontaneous coronary dissection and eosinophilic inflammation: a cause and effect rela- tionship? Am J Med 1982;72:923-928.
[41] Keeping HS, Lyttle CR. Monoclonal antibody to rat uterine peroxi- dase and its use in identification of the peroxidase as being of eosinophil origin. Biochim Biophys Acta 1984;802:399-406.
[42] Spry CJ, Tai PC, Davies J. The cardiotoxicity of eosinophils. Postgrad Med J 1983;59:147-153.
[49] Leiva MC, Xu Q, Galman M, Lyttle CR. Ontogeny of the produc- tion of an estrogen regulated eosinophil chemotactic factor in the rat uterus. Biol Reprod 1991;45:818-823.
[50] Tchemitchin AN, Barrera J, Arroyo P, Mena MA, Vilches K, Grunert G. Degranulatory action of estradiol on blood eosinophil leukocytes in vivo and in vitro. Agents Actions 1985;17:60-66.
[5 11 Grunert G, Tchemitchin AN. Effect of progesterone on the non-ge- nomic response to estrogen in the rat. J Endrocrinol 1982;94:307- 315.
1521 Wiest WG. Progesterone and 20o-hydroxypregnenone in plasma, ovaries and uteri during pregnancy in the rat. Endocrinology 1970;87:43-48.
[53] Tansey TR, Padykula HA. Cellular responses to experimental inhibi- tion of collagen degradation in the postpartum rat uterus. Anat Ret 1978;191:287-310.
1431 Atkinson JB, Robinowitz M, McAllister HA, Virmani R. Associa- 1541 Rajabi M, Dean DD, Woessner JF. High levels of serum collagenase tion of eosinophils with cardiac rupture. Hum Path01 1985;16:562- in premature labor - a potential biochemical marker. Obstet Gynecol 568. 1987;69(21: 179- 186.
Dow
nloaded from https://academ
ic.oup.com/cardiovascres/article/33/3/527/2462566 by guest on 07 January 2022


















