
The elderly. Aging Aging- the process by which human behavior alters with time Wisdom and judgment...
68
he elderly
-
Upload
jonas-hart -
Category
Documents
-
view
215 -
download
0
Transcript of The elderly. Aging Aging- the process by which human behavior alters with time Wisdom and judgment...
The elderly
AgingAging- the process by which human behavior
alters with timeWisdom and judgment become more acute
and powerful.Fifty is a crucial age in determining the
brain’s pattern of agingAfter this age, brain functioning and mental
ability are determined by three factors: mental habits, chronic disease, and mind’s flexibility.

AgingElderly population is now the fastest growing
population.It is estimated that by 2030, there will be 50
million people over 65. More focus is being placed on geriatric health
issues: disabilities, chronic health problems, living alone or assisted living, depression, loss, pain, Alzheimer’s and dementia.
Year
0
5
10
15
20
25
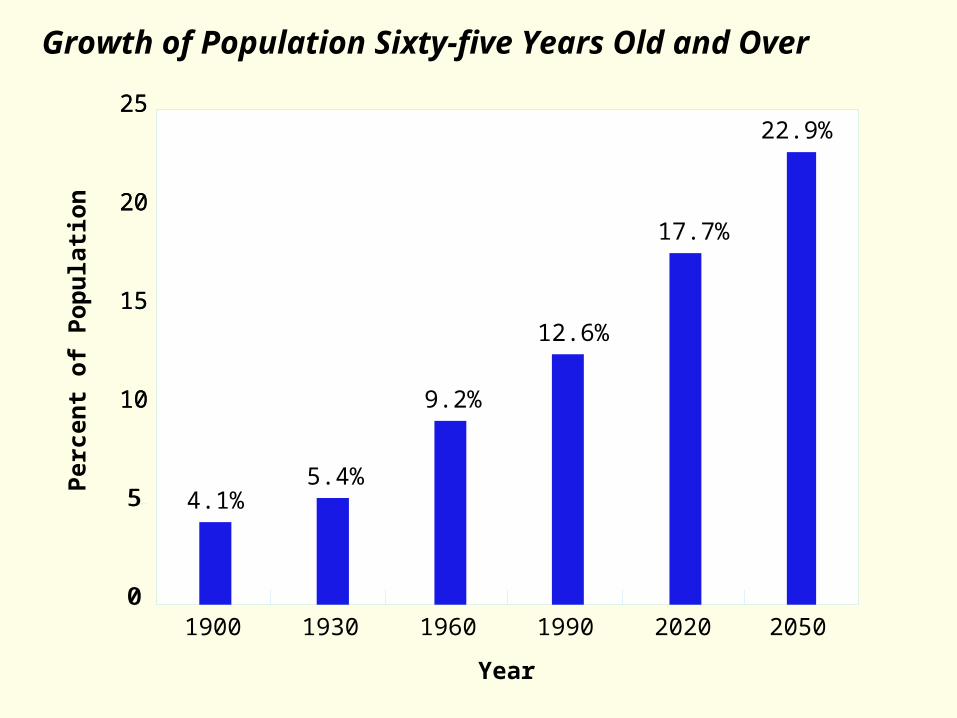
205020201990196019301900
4.1%5.4%
9.2%
12.6%
17.7%
22.9%
Per
cen
t o
f P
op
ula
tio
n
0
5
10
15
20
25
Growth of Population Sixty-five Years Old and Over

• We are living currently in the very oldest world society that
has ever existed.
• Aging population will be one of the dominant trends over the
next decades in the industrialized world.
• Over-65 population in the U.S. is 11 times what it was in
1900. General population is only 3 times as many as in
1900.
• We are living currently in the very oldest world society that
has ever existed.
• Aging population will be one of the dominant trends over the
next decades in the industrialized world.
• Over-65 population in the U.S. is 11 times what it was in
1900. General population is only 3 times as many as in
1900.
Demographic Revolution

Men WomenChina 68 71India 59 60Israel 76 81Japan 76 83Turkey 70 74Canada 76 83Cuba 75 80Mexico 70 77USA 73 79Poland 68 76France 74 82Germany 73 79Greece 76 81Italy 75 81Spain 74 81Switzerland 75 82Egypt 60 63Kenya 56 56Nigeria 53 56South Africa 57 62Zambia 36 36Australia 76 83New Zealand 74 80
Men WomenChina 68 71India 59 60Israel 76 81Japan 76 83Turkey 70 74Canada 76 83Cuba 75 80Mexico 70 77USA 73 79Poland 68 76France 74 82Germany 73 79Greece 76 81Italy 75 81Spain 74 81Switzerland 75 82Egypt 60 63Kenya 56 56Nigeria 53 56South Africa 57 62Zambia 36 36Australia 76 83New Zealand 74 80
Life Expectancy:Selected Data for Men and Women in Industrialized Nations

Aging
Primary Aging Secondary AgingPhysical changes due to
aging. Due to maturation
Changes due to illness, health habits and are not inevitable.
AgeismPrejudice Against Older People1- Negative attitudes about older people
regarding competence & attractiveness2- Identical behavior by an older person and a
younger one is interpreted differently.3- People use baby talk to address older people
in nursing homes4- Job discrimination5- Misinformation
• Gradual decline, begun decades ago, continues
• Presbycus (hearing loss)
• Presbyopia (“far-sightedness”)
• Shrinkage of internal organs
• Shrinkage in height
• Muscles less flexible
• Canities (hair becoming gray to white)
• Wrinkling and mottling skin
• Neuronal conduction slows
• Less deep sleep
• Higher rates of chronic diseases
• Gradual decline, begun decades ago, continues
• Presbycus (hearing loss)
• Presbyopia (“far-sightedness”)
• Shrinkage of internal organs
• Shrinkage in height
• Muscles less flexible
• Canities (hair becoming gray to white)
• Wrinkling and mottling skin
• Neuronal conduction slows
• Less deep sleep
• Higher rates of chronic diseases
The Aging Process

•Falls (a major cause of death or disability)
•Misuse of medicines
•Social isolation
•Infections
•Osteoporosis
•Nutritional deficiencies
•Depression
•Cancer
•Cardiac Disorder/stroke/pneumonia/diabetes/arteriosclerosis
•Dementia
The Good News: Many older individuals lead satisfying lives and maintain their health well beyond society’s expectations.
•Falls (a major cause of death or disability)
•Misuse of medicines
•Social isolation
•Infections
•Osteoporosis
•Nutritional deficiencies
•Depression
•Cancer
•Cardiac Disorder/stroke/pneumonia/diabetes/arteriosclerosis
•Dementia
The Good News: Many older individuals lead satisfying lives and maintain their health well beyond society’s expectations.
Risk Factors in Late Adulthood

• The majority of elderly adults take some medications.
• Some take as many as 7 different drugs.
• Most common medications are:• Sleeping pills• Laxatives• Anti-hypertensives• Diuretics• Cardiac medications• Antacids• Antibiotics• Cold remedies• Analgesics• Psychotropics
• Drugs metabolize more slowly as people age and kidney and liver functions decline
• Hazards include• Toxic interactions• Improper dosages• Outdated drugs• Storage problems• Confusion
• The majority of elderly adults take some medications.
• Some take as many as 7 different drugs.
• Most common medications are:• Sleeping pills• Laxatives• Anti-hypertensives• Diuretics• Cardiac medications• Antacids• Antibiotics• Cold remedies• Analgesics• Psychotropics
• Drugs metabolize more slowly as people age and kidney and liver functions decline
• Hazards include• Toxic interactions• Improper dosages• Outdated drugs• Storage problems• Confusion
Prescription Drug Use in Late Adulthood

Major Theories of Aging
1. Wear and Tear Theory (Common Sense)
Body is like a car that wears out after so much mileage. Looks at buildup of
toxins in the body.
2. Cellular Theories
All cells die and are replaced. Toxins and pollutants affect this cell
reproduction with mutations and imperfection. Metabolic wastes accumulate.
Electrons (free radicals) break away and destabilize atoms.
3. Genetic Programming Theories
We inherit a biological blueprint that switches off growth cells. Cells are
unable to continue dividing and deteriorate. Each time the cells die, the
telomeres grow shorter and eventually don’t allow the cell to replicate.
1. Wear and Tear Theory (Common Sense)
Body is like a car that wears out after so much mileage. Looks at buildup of
toxins in the body.
2. Cellular Theories
All cells die and are replaced. Toxins and pollutants affect this cell
reproduction with mutations and imperfection. Metabolic wastes accumulate.
Electrons (free radicals) break away and destabilize atoms.
3. Genetic Programming Theories
We inherit a biological blueprint that switches off growth cells. Cells are
unable to continue dividing and deteriorate. Each time the cells die, the
telomeres grow shorter and eventually don’t allow the cell to replicate.
4.- The Peripheral Slowing HypothesisThe overall processing speed declines in the
peripheral nervous system.It takes longer for information to reach the
brain.It takes longer for commands from the brain
to be transmitted to the body muscles

5.- The Generalized Slowing ProcessProcessing in all parts of the nervous system
is less efficient due to loss of neuronsThey are unable to receive efficiently
information from the environment to indicate a dangerous situation
Their decision process may be slower and their ability to remove themselves from harm is impaired
Living longer1. Telomeres-working on how to keep
them from decreasing in size2. Finding the longevity gene3. Reducing free radicals with antioxidant
drugs4. Restricting calories5. Bionic approach – replacing worn out
genesBUT AT WHAT COST???

The HeartThe arteries hardenThe blood vessels shrinkReduction in the capacity of the heart to
pump blood through out the circulatory system
A 75-year-old’s heart pumps less than three-quarters of the blood it pumped during early adulthood

The BrainA reduction of the blood flow to the brainThe space between the skull and the brain
doublesThe number of neurons declines in some
parts of the brain, though not as much as was once thought

Vision Lens becomes less transparent and the
pupils shrinkThe optic nerve becomes less efficientDistant object becomes less acuteMore light is needed to seeIt take longer to adjust to a change from
light to darkness and vice versa.Driving at night becomes difficultReading becomes more of a strain
Hearing50% of adults over 75 have hearing lossHigh frequencies are the hardest to hearHearing aids would be helpful 75% of the
time, but only 20% of people wear themHearing aids amplify all sounds so it is
difficult to discern conversationsSome people withdraw from society because
they feel left out and lonely
Psychological ProblemsA result of cumulative lossesDeclining health may contribute to
psychological problemsAnxiety may be caused by inappropriate drug
dosageChanges in metabolismThe effects of drug interaction

Dementia
Dementia is a disease marked by a gradual loss of cognitive functioning which can also incorporate losses of motor, emotional, and social functioning as well..
It is a permanent and progressive disease that eventually renders people unable to care for themselves.

Reversible causes of dementiaAlcohol use
Depression
Medication side effects /
Drug interaction
Nutritional deficiencies
Thyroid imbalance

Stages of Progressive Dementia
The following may occur over a 5 to 15 year period:
• General Forgetfulness – losing keys, eyeglasses, forgetting names and appointments
• Forgetfulness More Intense and Prevalent – become repetitive, confused, unable to concentrate. Dysphasic.
• Dangerous Stage – getting lost, dressing inappropriately, forgetting to eat, forgetting to turn off the stove.
• Totally Confused and Disoriented – doesn’t recognize spouse or family members. Cannot control body functions. Requires full-time care.
The following may occur over a 5 to 15 year period:
• General Forgetfulness – losing keys, eyeglasses, forgetting names and appointments
• Forgetfulness More Intense and Prevalent – become repetitive, confused, unable to concentrate. Dysphasic.
• Dangerous Stage – getting lost, dressing inappropriately, forgetting to eat, forgetting to turn off the stove.
• Totally Confused and Disoriented – doesn’t recognize spouse or family members. Cannot control body functions. Requires full-time care.

DementiaBegins with
forgetfulness - isolated incidents of memory loss do not constitute dementia.
Forgetfulness progresses to confusion and eventually disorientation.
Problem solving
Judgment
Decision making
Orienting to space and time
Personality changes - irritable, agitated, sadness (depression), manic episodes
Dementia - Causes50 different causes
Neurological disorders such as Alzheimer’s (est. 50-70% of people with dementia have Alzheimer’s)
Drugs and alcohol
Vascular disorders such as multi-infarct disease (multiple strokes)Inherited disorders such as Huntington’sInfections such as HIV

Causes of Dementia
Alzheimer’s(56%)
Brain Injury (4%)
Other Causes (6%)
Parkinson’s Disease (8%)
Multi-InfarctDementia or Vascular Causes(14%)
Multiple Causes (12%)
Source: Trushke, Edward F. (Fall 1998) ADVANCES. Bulletin of Progress in Alzheimer’s Disease Research and Care.

Two types of dementiaCortical - Disorder affecting the cortex,
the outer portion or layers of the brain.
Alzheimer’s and Creutzfeldt-Jakob are two forms of cortical dementia
Memory and language difficulties (Aphasia) most pronounced symptoms.
Aphasia is the inability to recall words and understand common language.
Subcortical - Dysfunction in parts of the brain that are beneath the cortex.
Memory loss & language difficulties not present or less severe than cortical.
Huntington’s disease and AIDS dementia complex.
Changes in their personality and attention span.
Thinking slows down.
Vascular dementia – the second leading type of dementia
Strokes cause between 10% and 20% of dementia cases.

Delirium Definition
Disturbance of consciousness i.e., reduced clarity of awareness of the
environment with reduced ability to focus, sustain, or shift attention
Change in cognition (memory, orientation, language, perception)
Development over a short period (hours to days), tends to fluctuate
Evidence of medical etiology

DeliriumTends to occur with:
the elderly
those with medical conditions such as Cancer, AIDS or fevers (more prevalent in children)
Can also be diagnosed with those who are taking drugs
PREVALENCERange: 20-30% of all patients acutely
hospitalizedUnrecognized in up to 32-67% of cases
Morbidity:Skin breakdownAspiration pneumoniaCardiovascular stressProlonged hospitalization
Mortality: 20-30% *according to one study

DeliriumDrugs that may contribute to delirium
- Anticonvulsants- Barbiturates-Insulin/hypoglycemic agents- Antipsychotics- Benzodiazepines- Narcotics
Alzheimer’s disease –the most common type of dementia
6 out of 10 cases of dementia are Alzheimer’s disease.

• Affects 4 million Americans. 14 million predicted to have it by 2050
• 1 out of 10 people over 65 have Alzheimer’s. 1 out of 2 over 85 have it.
• Costs over $100 billion annually in health care and related costs.
• Definitive diagnosis only on autopsy, with findings of plaques and tangles in the brain cortex.
• Possible causes include genetic inheritance, slow virus, or environmental toxins.
• No known cure.
• Affects 4 million Americans. 14 million predicted to have it by 2050
• 1 out of 10 people over 65 have Alzheimer’s. 1 out of 2 over 85 have it.
• Costs over $100 billion annually in health care and related costs.
• Definitive diagnosis only on autopsy, with findings of plaques and tangles in the brain cortex.
• Possible causes include genetic inheritance, slow virus, or environmental toxins.
• No known cure.
Alzheimer’s Disease
Alzheimers DiseaseProgressive disorder in which neurons
deteriorate resulting in the loss of cognitive functions (memory), judgment and reasoning, movement coordination, and pattern recognition. Predominantly affects the cerebral cortex and hippocampus which atrophy as the disease progresses.

Alzheimer’s – plaques and tanglesNeuritic PlaquesCommonly found in brains
of elderly people but appear in excessive numbers in the cortex of AD pt.’s
Surrounded by deteriorating neurons that produce acetylcholine (neurotransmitter essential for processing memory and learning.
Neurofibrillary TanglesTwisted remains of a
protein which is essential for maintaining proper cell structure.
It is not known whether the plaques and tangles are the cause of AD or part of the results of the disorder.
Areas of the brain that may be affectedFrontal lobe
thinking, planning, judging, movement
Parietal lobeSensations like
pain, temperature, touch
Temporal lobeUnderstanding
sounds and speech
Occipital lobeProcesses visual
information

Affected area of the brainHippocampus
Plays a crucial role in both the encoding and retrieval of information.Damage to the hippocampus produces global retrograde amnesia, which is the inability to retain newly learned information.
Symptoms of Alzheimer’s Aphasia – difficulty processing or speaking language
Apraxia - (decreased ability to perform physical tasks such as dressing, eating, etc.)
Delusions
Easily lost and confused
Inability to learn new tasks
Loss of judgment and reason
Loss of inhibitions and belligerence
Social Withdrawal
Visual hallucinations

Alzheimer’s – early stageCharacteristics
Begins with forgetfulness
Progresses to disorientation and confusionPersonality changes
Symptoms of depression/manic behaviors
Interventions
Medications - Aricept and Cognex (both are commercial names).
Both increase acetylcholine (Ach) in the brain by inhibiting the enzyme that breaks it down.
Therapy (deal with depression that often accompanies diagnosis
Counseling with family

Early StageMusic Therapy
Used to relieve depression
Coupled with exercise and relaxation techniques
Increase or maintain social relationships (dancing, improvisation)
Maintain positive activities (church choir, Senior social dances, etc.)

Alzheimer’s – middle stage Characteristics
Need assistance with daily skills
Unable to remember names
Loss of short-term recall
May display anxious, agitated, delusional, or obsessive behavior
May be physically or verbally aggressive
Poor personal hygiene
Disturbed sleep
Inability to carry on a conversation
May use “word salad” (sentence fragments)
Posture may be altered
Disoriented to time and place
May ask questions repeatedly

Middle StageInterventions
Validation Therapy
Structured Areas for MobilityPositive, nurturing, loving environment
Music Therapy

Alzheimer’s – later stageCharacteristics
Loss of verbal articulation
Loss of ambulation
Bowel and bladder incontinenceExtended sleep patterns
Unresponsive to most stimuli
Interventions
Caring for physical needsMaintain integrity of the skinMedical interventions
Most activities are inaccessible

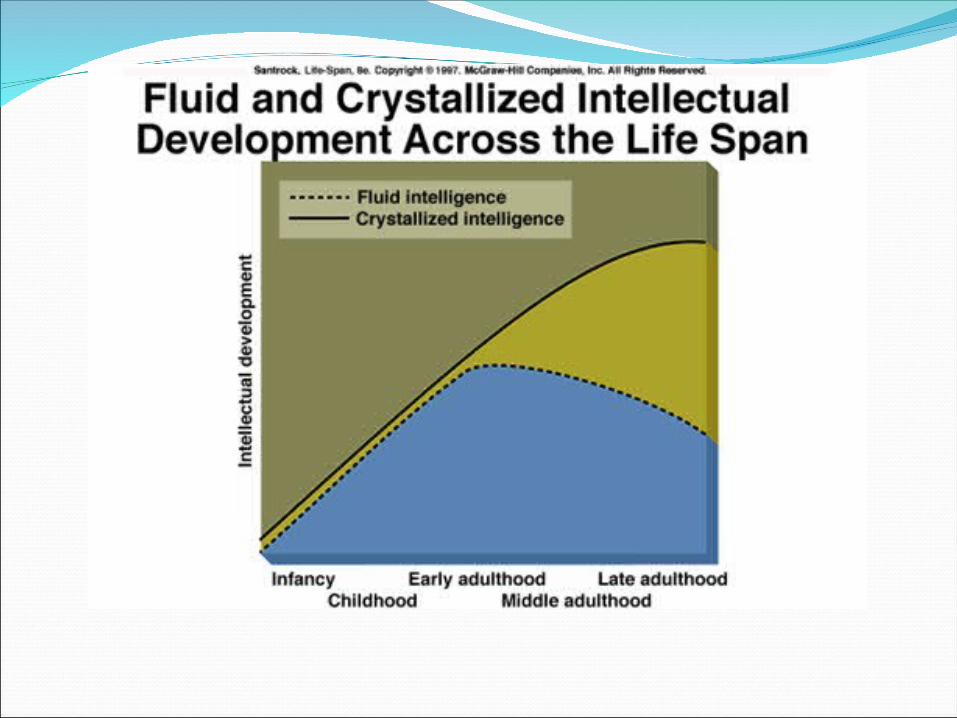
Cognitive DevelopmentSchaie’s StudiesResults show no uniform pattern of adulthood
age-related changes across all intellectual abilities
Fluid intelligence decline starting age 25Crystallized intelligence stay steady or
increaseTraining can improve reasoning and spatial
skills
MemoryPeople are less likely to experience memory
loss in societies where older people are held in high esteem
Memory losses occur primarily to episodic memory
Semantic memories and implicit memories are largely unaffected by age
Short-term memory declines gradually until age 70
Atchley’s Stages of Retirement
Phase 1. Preretirement – disengage from workplace and plan for retirement. May have mixed feelings.

Atchley’s Stages of Retirement Phase 2 - RETIREMENT – people do one of three things:
A. Honeymoon – initially feel on top of the world and do things that they could not when they were employed.
B. Immediate retirement routine – those who already had a full and active schedule in addition to their employment will become individuals who establish comfortable, yet busy schedules soon after retirement.
C. Rest and relaxation - period of very low activity as compared to the "honeymoon" path. Persons who have had very busy careers with limited time to themselves frequently choose to do very little in their early retirement years. Frequently, however, activity levels do increase after a few years of rest and relaxation.

Atchley’s Stages of RetirementPhase 3 – Disenchantment:
Following the honeymoon period or a time of continued rest and relaxation, there may be a period of disappointment or uncertainty. A person may miss the feelings of productivity they experienced when working. Disenchantment with retirement can also occur if there is a significant disruption in the retirement experience, such as the death of a spouse or an undesired move.
Atchley’s Stages of RetirementPhase 4: Reorientation:
"take inventory" of their retirement experience and find ways that will improve their retirement role. Becoming more involved in community activities, taking up a new hobby or relocating to a more affordable setting may contribute to this "second chance" at retirement. A common goal of reorientation is to design a retirement lifestyle that is satisfying and enjoyable

Atchley’s Stages of RetirementPhase 5 – Retirement
Routine:Mastering a comfortable
and rewarding retirement routine is the ultimate goal of retirement. Once a fulfilling and comfortable retirement routine has been found, this phase of retirement can last for many years.
Atchley’s Stages of RetirementPhase 6 - Termination
of Retirement:Eventually the
retirement role becomes less relevant in the lives of older adults. When a person can no longer live independently due to disability or illness, the role of disabled elder becomes the primary focus of his or her life.

Top Five Causes of Death1900Influenza,
pneumonia 11.8%
Tuberculosis11.3%
Gastritis, enteritis 8.3%
Heart Disease 8.0%
Stroke 6.2%
2000Heart Disease
25.7%Cancer
20.0%Stroke
6.0%COPD
4.5%Accidents
3.4%

Where We Die6%
57%
17%
20%
ResidenceNursing Home
HospitalOther
1992 Data

AgingThe most common psychological disorder
associated with aging is depression.Suicide rates among the elderly are
increasing at startling rates.The highest suicide rates are for white men
over age 85.The elderly comprise about 13% of the
population and account for about 20% of all suicides.

African American females
White females
African American males
White males
26.0
10.1
7.2
2.0
32.0
53.0
67.6
11.8
18.5
18.9
6.6
6.3
6.3
2.6
1.4
0.1
Per
cen
t
Age Groupings
0
10
20
30
40
50
60
70
80
85+75-8465-7455-64
Older Suicide by Race and Gender, 1992

Risk Factors for Suicide in Late Adulthood
• Living alone and being socially isolated
• Experiencing financial difficulty
• Feeling depressed or useless
• Being alcohol or drug dependent
• Having a mental illness that reduces communication
• Suffering from chronic pain, illness, or incapacity
• Being unable to express grief or suffering
• Losing significant relationships due to the death of loved ones
Ways in Which Culture Influences Death Concerns
• Affects the assessment of comfort needs of the dying and the
kind of care provided
• Influences selection, perception, and evaluation of health care
givers and their methods
• Shapes beliefs about causes of death.
• Determines the disposition of the body and funeral and burial
rituals
• Patterns grief responses and bereavement roles.
Dying is Largely Publicly Funded in U.S.A.
70% of people dying are covered by Medicare
13% of Medicare recipients also receive Medicaid
Impact on family? 30% of families are impoverished by the process of dying

MemoryMemory deteriorates with age, specifically short-
term memory as well as the ability to perform certain tasks under time constraints.
In psychometric psychology, fluid and crystallized intelligence are both factors of general intelligence.
Fluid Intelligence- ability to find meaning in confusion and solve new problems.
Crystallized Intelligence- ability to utilize previously acquired knowledge and experience
Brain regions important to memory begin to atrophy as we age.

Kubler-Ross Theory Stages of Dying
1. Denial and Isolation: Used by almost all patients in some form. It is a usually temporary shock response to bad news. Isolation arises from people avoiding the dying person. People can slip back into this stage when new developments emerge or they can no longer cope.

2. Anger: Different ways of expression -Anger at God: "Why me?" They feel
others are more deserving. -Envy of others: Other people are
enjoying life while the dying person experiences pain.
-Projected on environment: Anger towards doctors, nurses, and families.
3. Bargaining: A brief stage, hard to study because it is often between patient and God.
-If God didn't respond to anger, maybe being "good" will work.
-Attempts to postpone: "If only I could live to see . . ."
4. Depression: Mourning for losses -Reactive depression (past losses): loss of job,
hobbies, mobility. -Preparatory depression (losses yet to come):
dependence on family, etc.

5. Acceptance: This is not a "happy" stage, it is usually void of feelings. It takes a while to reach this stage; it consists of basically giving up and realizing that death is inevitable. Hope is an important aspect of all stages. A
person's hope can help them through difficult times.

Elizabeth Kubler-Ross’s Stages of Coping with Death
Denial “Not me.”
Anger “Why me?”
Bargaining “Yes me, but . . .”
Depression “Yes me.”Begin to mourn.
Acceptance “My time is very close now, and it’s all right.”
Stage Associated Feelings

EriksonEight Stages of Psychosocial Development
Integrity vs. Despair
Elderly deal with questions of integrity and despair
Often reminisce aboutpast, evoking feelings ofworthlessness orsatisfaction


















