
Tratamiento de placenta previa. Tratamiento de placenta previa oGrado de placenta previa.

Gorodeski et al, Placenta previa localization 169
J. Perinat. Med.15 (1987) 169
The effect of placenta previa localization upon maternal and fetal-neonatal outcome
Israel G. Gorodeski and Charles M. Bahari
Department of Obstetrics and Gynecology "B", Meir Hospital, Sapir MedicalCenter, Kfar Saba, and Tel Aviv University Sackler School of Medicine, Israel
1 Introduction
Patients with placenta previa (PP) provide animportant practical problem in obstetrics withregard both to mother and fetus-neonate [11].The functional efficiency of the placenta inwomen with PP could be reduced because ofan unfavorable implantation site or because ofareas of fibrosis related to repeated bleedingepisodes [13]. These pregnancies may be com-plicated by placental insufficiency and intra-uterine fetal death because of extensive placen-tal damage from separation and infarction [14].
Previous studies [3, 4, 7, 8] have dealt withthe problem whether major types of PP areassociated with worsening of maternal andfetal-neonatal prognosis. It has been difficultto draw definitive conclusions because resultshave been contradictory. Most studies have notincluded the low lying type of PP [3, 4, 7],and use was made of different parameters forpurposes of evaluation. The studies of MORGAN[8], HIBBARD [7], and CRENSHAW et al. [4] pre-sent data of women treated 2 to 3 decades ago,while that of COTTON et al. [3] present dataof women treated during 1975 — 1978, usingmodern diagnostic techniques, as well as dif-ferent management modalities. It is not surpris-ing to find different results including perinatalmortality rate of 39% [4] vs. 12.6% [3].
The present study was undertaken to clarifythe association of maternal and fetal-neonataloutcomes with different types of PP.
2 Material and methods
This study is based on our experience withtreatment of PP in 164 consecutive patients(165 pregnancies) over a period of 11 yearsending in 1983 with an incidence of 0.5% (1 in200 deliveries). PP was diagnosed if the placentawas sited in the lower uterine segment (lowlying), if the placental margin extended to theinternal os of the cervix (marginal), or if itcovered the dilating cervix partially (partial) ortotally (total).The management policy with PP was classifiedas "conservative — active" as follows:1. The premature patient, i.e. 37 menstrualweeks gestation or less, was managed expect-antly whenever possible.2. Early placental localization was obtained byvarious radiological and ultrasonographicmethods.3. There was avoidance of vaginal or rectalexaminations except under very unusual cir-cumstances (see 5).4. Frequent hospitalizations and liberal bloodtransfusions (Hb < 10 gr% or protracted va-ginal bleeding) were used.5. With severe hemorrhage, premature ruptureof membranes, premature labor or other condi-tions necessitating urgent delivery, vaginalexamination was performed under "double setup" conditions.6. Cesarean section was indicated electively incases of marginal posterior, partial and totalPP.
1987 by Walter de Gruyter & Co. Berlin · New York

170 Gorodeski et al, Placenta previa localization
7. Neonates were hospitalized when indicatedin a modern neonatal intensive care unit.The study group consisted of cases of PP identi-fied by a documented history of vaginal bleed-ing and ultrasonographic placental imaging us-ing the full bladder technique. In all thesewomen the site of PP was confirmed at vaginalexamination or during manual removal of theplacenta in cases of vaginal delivery or by in-spection at cesarean section. Ten women wereexcluded from the study because of lack ofinformation.The following parameters were evaluated withrespect to placental localization: maternal age,previous obstetrical performance and presentpregnancy, the latter with respect to maternaland perinatal outcome.The following parameters were used to evaluateblood loss: onset of bleeding, number of bleed-ing episodes and the amount of antepartumblood transfusions. A bleeding episode was de-fined as a period of hospitalization associatedwith antenatal vaginal bleeding and lasting nomore than 7 days. We found the use of theseparameters more accurate than a rough estima-tion of blood loss in ml in defining the clinicalcondition and laboratory status of the patientwhen blood less occurred.The control group was composed of womenwithout PP, who were arbitrarily selected fromamong the parturients in the same years andwho were matched by the day of confinement.There were two controls for each test subject:one who delivered before and one who deli-vered after the index case.
Statistical analysis of the data was performedby conducting the chi-square analysis for differ-ences in incidence between groups, and the Stu-dents' t test for differences in means betweengroups.
3 Results
The study group consisted of 155 pregnancieswith PP and 159 newborns. This group included2 sets of twins and one set of triplets. Onewoman delivered twice during this period withrecurrent PP. The distribution of women withrespect to the type of PP is presented in table I.The control group consisted of 300 women whodelivered a total of 305 newborns, including 5sets of twins.Maternal age: Women with PP were older thanwomen in the control group. A clear cut associ-ation was demonstrated between an older ageand major types of PP (figure 1).
CONTROL
LOW LYINGMARGINAL ANTERIOR
MARGINAL POSTERIOR
PARTIAL
TOTAL
MATERNAL AGE
Figure 1. Cumulative destribution curves of varioustypes of placenta previa with respect to maternal age.
Table I. Composition of the study group by the type of placenta previa (PP).
Type of placentaprevia
Number of womenNumber of newborns
Lowlying
4142**
Marginalanterior
3333
Marginalposterior
2930**
Partial
12*12
Total
40*42***
Totalnumber
155159
* — Same woman in 2 episodes** - Set of twins
*** - Set of triplets
J. Perinat. Med. 15 (1987)
Gorodeski et al, Placenta previa localization 171
Previous obstetrical performance: Women withPP had greater gravidity and parity, and theyhad higher rates of previous cesarean sectionsas compared to women in the control group.We could not establish a connection betweenany of these findings and the type of PP (tableΠ).Present pregnancy — maternal aspects: Ninety-nine women (64%) presented with bleeding ep-isodes during the first to third trimesters andwere managed "expectantly" (table III). Fifty-three women (34%) were delivered following asingle, usually severe antepartum hemorrhage,while in 3 (2%) no symptoms of antepartumbleeding were documented and the PP was dia-gnosed incidentally either at cesarean section(1 patient with low-lying and 2 with marginalposterior), or during vaginal delivery (marginalanterior). In women who presented with mul-tiple antenatal bleeding episodes, we found nosignificant association between the number ofbleeding episodes or number of antepartumtransfusions and the major types of PP. In 8women with PP an additional placental patho-logical state, namely focal accretion, was diag-nosed; 7 out of 8 of these women had minortypes of PP (table III). The rate of pathologicalpositions and presentations was higher inwomen with PP compared to the control group
but was not influenced by the type of PP (tableIV). Seventy-three percent of women with PPwere delivered by cesarean section as comparedto 12% of the controls; 96% of the womenwith marginal posterior, partial or total PP weredelivered by cesarean section in comparisonwith 47% of those with low lying or marginalanterior PP (table V). In this latter group of 35women who were operated upon, 29 presentedwith severe antepartum hemorrhage (including10 with abnormal presentations), and 2 under-went repeat caesarean section. In the PP groupas a whole, severe antepartum bleeding was themain indication for cesarean section (table VI).Postnatal maternal complications occurred in4 women, 1 with low lying placenta and 3 withmarginal anterior, and included postpartum he-morrhage in all with disseminated intravascularcoagulopathy (DIG) in 2 women. The only ma-ternal death occurred in a woman with lowlying placenta who developed postpartum he-morrhage, DIG and histologically confirmedamniotic fluid embolism.Present pregnancy — fetal-neonatal aspects: Themale: female ratio was slightly higher in womenwith PP than in the control group, but thisfinding was not associated specifically with anytype of PP (table VII). The median deliverydate in women with PP was 36.3 weeks gesta-
Table Π. Previous obstetrical performance in women with placenta previa (PP) and the control group.
Type ofplacentaprevia(number)
Gravidity-0(%)
Parity-0 (%)l-3(%)4 + (%)
Abortions-0 (%)l-2(%)3 + (%)
Previouscesareansection (%)
Lowlying
(41)
6(15%)
12 (29%)28 (68%)1 (3%)
18 (44%)16(39%)7(17%)
7 (17%)
Marginalanterior
(33)
3 (9%)
10 (30%)20 (60%)3 (10%)
18 (55%)10(30%)5(15%)
1 (3%)
Marginalposterior
(29)
3 (10%)
5 (17%)21 (72%)3(11%)
13(45%)10 (34%)6(21%)
3 (10%)
Partial
(12)
0
1 (8%)7 (59%)4 (33%)
2(17%)8 (67%)2(16%)
2(17%)
Total
(40)
3 (7.5%)
8 (20%)25 (62.5%)7 (17.5%)
13 (33%)20 (50%)7 (17%)
5 (12.5%)
TotalnumberPP(155)
15(9.7%)
36 (23%)101 (65%)18(12%)
64(41%)64(41%)27(18%)
18(11.6%)
Controlgroup
(300)
80 (27%)
119(39%)167 (56%)14 (5%)
212 (72%)71 (24%)12(4%)
9(3%)
Signifi-cance
p < 0.01
p < 0.05p < 0.5p < 0.025
p < 0.01p < 0.025p < 0.05
p < 0.05
J. Perinat. Med. 15 (1987)

172 Gorodeski et al, Placenta previa localization
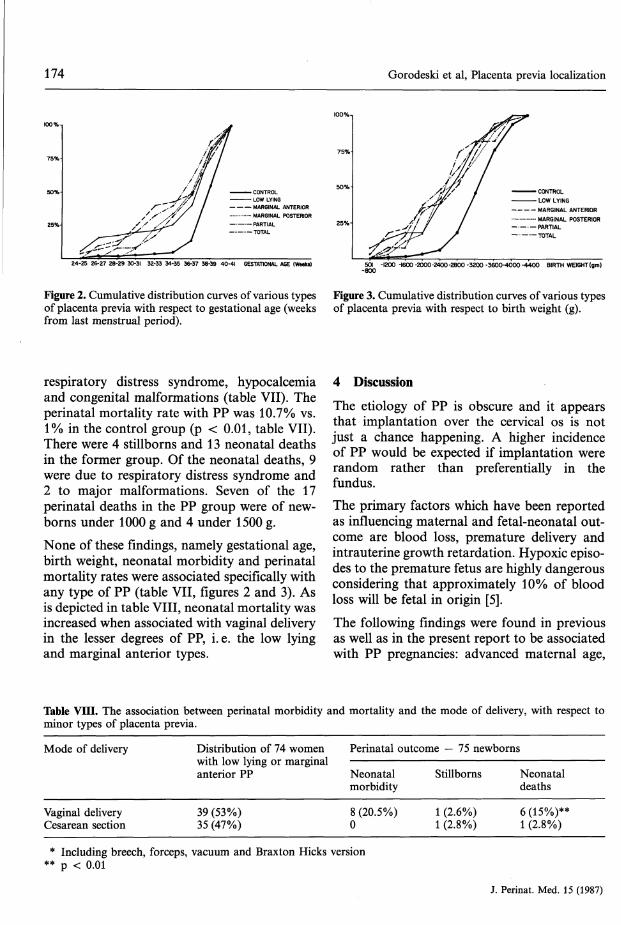
tion (from last menstrual period) in contrast to38.1 in the control group (p < 0.05) (figure 2).The median weight of the newborns in womenwith PP was 2530 g vs 3180 g in the control
group (p < 0.05) (figure 3). Neonatal morbidityoccurred in 51.5% of infants born to PPpatients vs. 44% in the control group. Theincrease was due to higher rates of anemia,
Table III. Antenatal and postnatal maternal course and complications in the women with placenta previa and inthe control group.
Type ofplacentaprevia(Number)
Accidental finding at delivery
Intrapartum bleeding*
Antepartum bleeding— from 1st trimester— from 2nd trimester— from 3rd trimester
Lowlying
(41)
1 (2.5%)
13(325)
27 (66%)1
134
— from last month of pregnancy 9
Number of bleeding episodesper patient (mean)
Antepartum hospitalizationin days (mean)
Antepartum or intrapartumhemotransfusion— blood units/patient (mean)
Placenta previa with focalaccretion
Postpartum hemorrhage
Disseminated intravascularcoagulopathy
Maternal death
1-5(2)
0-24(7.2)
0-4(0.8)
3 (7%)
1 (2.5%)
2 (2.5%)
1 (2.5%)
Marginalanterior
(33)
1 (3%)
16(48%)
16 (48%)3454
1-6(1.9)
4-12(6.4)
0-4(1.25)
2 (6%)
3 (9%)
1 (3%)
0
Marginalposterior
(29)
1 (3.5%)
6(21%)
22 (76%)335
11
1-6(1.7)
4-16(7.6)
0-4(1.75)
2(7%)
0
0
0
Partial
(12)
0
3 (25%)
9 (75%)3114
1-6(2.1)
4-12(7.6)
0-4(1.2)
1 (8%)
0
0
0
Total
(40)
0
15(37.5%)
25 (62.5%)4
1290
1-6(2.4)
4-16(9.6)
0-4(1.4)
0
0
0
0
TotalnumberPP(155)
3 (2%)
53 (34%)
99 (64%)14331537
1-6(2.0)
0-24(7.7)
0-4(1.25)
8 (5%)
4(2.5%)
2(1.5%)
1 (0.6%)
Controlgroup
(300)
-
0
4(1.5%)2110
—
0-11(0.2)
0
2 (0.5%)**
0
0
* — As the first episode of uterine bleeding; ** — p < 0.01
Table IV. Pathological positions and presentations(excluding twins and triplets).
Type of placentaprevia(Number)
Head presentationBreechTransverse lieOblique lieCompound presentationUnstable lie
% pathological positionsand presentations (exclud-ing head presentation)
Lowlying(40)
27 (67.5%)5 (12.5%)8 (20%)000
32.5%NS
Marginalanterior(33)
25 (76%)4 (12%)3 (9%)01 (3%)0
24%NS
in women
Marginalposterior(28)
19 (68%)4 (14%)5(18%)000
32%NS
with placenta previa and in the control group
Partial
(12)
6 (50%)1 (8.5%)4(33%)1 (8.5%)00
50%NS
Total
(39)
25 (64%)2(5%)7 (18%)3 (8%)02(5%)
36%NS
Totalnumber PP(155)
102 (67%)16(10.5%)27(18%)4 (2.6%)1 (2.6%)2(1.3%)
33%
Controlgroup(300)
274(93%)18 (6%)3(1%)000
7%
NS = not significant
J. Perinat. Med. 15 (1987)

Gorodeski et al, Placenta previa localization 173
Table V. Mode of delivery of women with placenta previa and of women in the control group.
Type of placenta Low Marginal Marginalprevia lying anterior posterior(Number) (41) (33) (29)
Vaginal delivery 12 (29.2%) 23 (70%)Assisted breech 1 (2.6%) 1 (3%)Braxton Hicks version 2 (3%)Forceps 1 (2.6%)Vacuum 1 (2.6%)Cesarean section 26 (63 %) 9 (27%) 28 (97%)
* 1 — prolapse of cord
Partial
(12)
2* (17%)
10 (83%)
Total
(40)
40 (100%)
Totalnumber PP(155)
37 (24%)2(1.2%)1 (0.6%)1 (0.6%)1 (0.6%)
113(73%)
Controlgroup(300)
232 (77%)5(2%)
27 (9%)
36(12%)
Signifi-cance
p < 0.01p > 0.05
p < 0.01
p < 0.01
Table VI. Indications for cesarean section in women with placenta previa and in the control group.
Type of placentaprevia(Number)
LaborAntepartum hemorrhageAcute fetal distressRepeated sectionToxemiaDystociaOthers
Total
Lowlying(41)
21 (51%)2(5%)2(5%)1 (2%)
26(63%)
Marginalanterior(33)
8 (24%)
i (3%)*
9 (27%)
Marginalposterior(29)
8 (28%)16(55%)2 (8%)1 (3%)1 (3%)
28 (87%)
Partial Total Total Controlnumber PP group
(12)
3 (25%)7 (58%)
10(83%)
(40)
10 (25%)25 (63%)
5 (12%)
(155)
21 (14%)77 (50%)4 (2.5%)8 (5%)2(1%)
1 (0.5%)
40(100%) 113(73%)
(300)
6(2%)15(5%)4(1.3%)
10(3%)1 (0.7%)
36 (12%)
Signifi-cance
p > 0.05p > 0.05p > 0.05
p > 0.05
p < 0.05
* — failed Braxton Hicks version
Table VII. Fetal/neonatal outcome in the placenta previa
Type of placentaprevia(Number)
Male/female ratio
Neonatal morbidity— Anemia— Hypoglycemia— Hypocalcemia— Jaundice- RDS*— Asphyxia— Infection— Trauma— Meconium aspiration— Cranial hemorrhage— Secondary hydrocephalus— Congenital malformation— Miscellaneous- Subtotal
Perinatal mortality- Stillborns— Neonatal death- Subtotal
Lowlying(42)
1.625
5144341100000
23 (55%)
13
Marginalanterior(33)
1.20
0014300002130
12(36%)
14
4(9.5%) 5(15%)
Marginalposterior(30)
1.00
4134401000020
19 (63%)
112(7%)
and the control group.
Partial
(12)
0.70
0014200000
0007 (58%)
000
Total
(42)
1.80
505632100
0030
21 (50%)
156 (14%)
Totalnumber PP(159)
1.34
14 (8.8%)2(1.3%)
14 (8.8%)22 (14%)15(9.4%)6 (3.7%)3(1.9%)1 (0.6%)02(1.3%)1 (0.6%)8 (5.0%)0
88 (55.3%)
4 (2.5%)13 (8.3%)17 (10.7%)
Controlgroup(305)
1.13
2 (0.7%)4(1.3%)2 (0.7%)
84 (27.4%)0
13(4.3%)2 (0.7%)2 (0.7%)
15(5.1%)2 (0.7%)09 (2.8%)7(2.3%)
142 (46.7%)
1 (0.35%)2 (0.65%)3(1%)
Signifi-cance
No
p < 0.01p > 0.05p < 0.01p < 0.05p < 0.01p > 0.05p > 0.05p > 0.05p < 0.025p > 0.05—p > 0.05p < 0.05p > 0.05
p < 0.025p < 0.01p < 0.01
* — Respiratory distress syndrome
J. Perinat. Med. 15 (1987)
174 Gorodeski et al, Placenta previa localization
- CONTROL- LOW LYING- MARGINAL ANTERIOR- MARGINAL POSTERIOR- PARTIAL- TOTAL
24-25 26-27 28-29 30-31 32-33 34-35 36-37 38-39 40-41 GESTATIONAL AGE (Weeks)
• CONTROL- LOW LYING
MARGINAL ANTERIOR· MARGINAL POSTERIOR
PARTIALTOTAL
501 -1200 -1600 -2000 -2400 -2800 -3200 -3600-4000 -4400 BIRTH WEIGHT (gm)-800
Figure 2. Cumulative distribution curves of various types Figure 3. Cumulative distribution curves of various typesof placenta previa with respect to gestational age (weeks of placenta previa with respect to birth weight (g).from last menstrual period).
respiratory distress syndrome, hypocalcemiaand congenital malformations (table VII). Theperinatal mortality rate with PP was 10.7% vs.1% in the control group (p < 0.01, table VII).There were 4 stillborns and 13 neonatal deathsin the former group. Of the neonatal deaths, 9were due to respiratory distress syndrome and2 to major malformations. Seven of the 17perinatal deaths in the PP group were of new-borns under 1000 g and 4 under 1500 g.
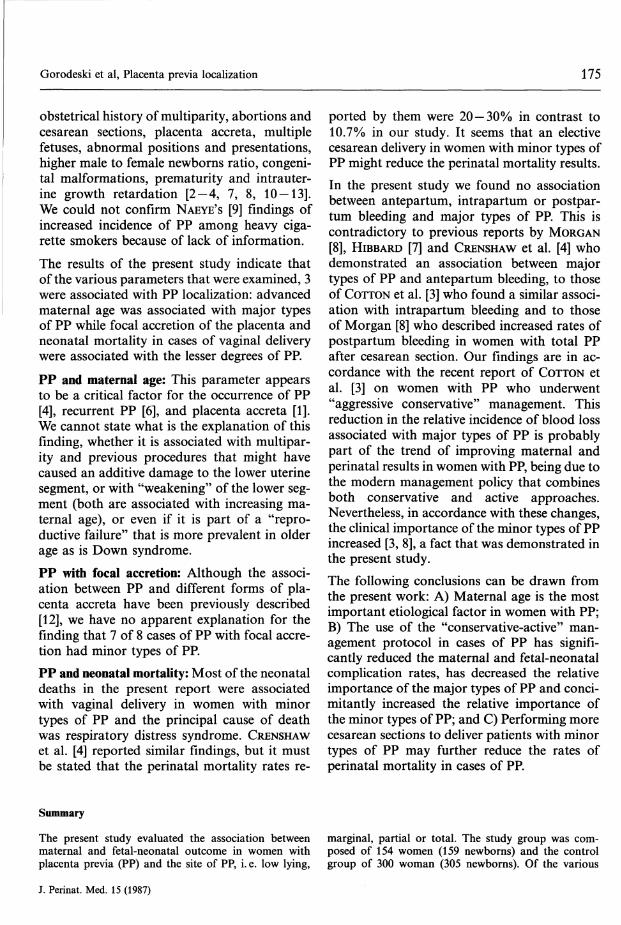
None of these findings, namely gestational age,birth weight, neonatal morbidity and perinatalmortality rates were associated specifically withany type of PP (table VII, figures 2 and 3). Asis depicted in table VIII, neonatal mortality wasincreased when associated with vaginal deliveryin the lesser degrees of PP, i. e. the low lyingand marginal anterior types.
4 Discussion
The etiology of PP is obscure and it appearsthat implantation over the cervical os is notjust a chance happening. A higher incidenceof PP would be expected if implantation wererandom rather than preferentially in thefundus.The primary factors which have been reportedas influencing maternal and fetal-neonatal out-come are blood loss, premature delivery andintrauterine growth retardation. Hypoxie episo-des to the premature fetus are highly dangerousconsidering that approximately 10% of bloodloss will be fetal in origin [5].
The following findings were found in previousas well as in the present report to be associatedwith PP pregnancies: advanced maternal age,
Table VIII. The association between perinatal morbidity and mortality and the mode of delivery, with respect tominor types of placenta previa.
Mode of delivery Distribution of 74 women Perinatal outcome — 75 newborns
Vaginal deliveryCesarean section
wnn low lying or marguanterior PP
39 (53%)35 (47%)
laiNeonatalmorbidity
8 (20.5%)0
Stillborns
1 (2.6%)1 (2.8%)
Neonataldeaths
6(15%)**1 (2.8%)
* Including breech, forceps, vacuum and Braxton Hicks version** p < 0.01
J. Perinat. Med. 15 (1987)
Gorodeski et al, Placenta previa localization 175
obstetrical history of multiparity, abortions andcesarean sections, placenta accreta, multiplefetuses, abnormal positions and presentations,higher male to female newborns ratio, congeni-tal malformations, prematurity and intrauter-ine growth retardation [2-4, 7, 8, 10-13].We could not confirm NAEYE'S [9] findings ofincreased incidence of PP among heavy ciga-rette smokers because of lack of information.The results of the present study indicate thatof the various parameters that were examined, 3were associated with PP localization: advancedmaternal age was associated with major typesof PP while focal accretion of the placenta andneonatal mortality in cases of vaginal deliverywere associated with the lesser degrees of PP.PP and maternal age: This parameter appearsto be a critical factor for the occurrence of PP[4], recurrent PP [6], and placenta accreta [1].We cannot state what is the explanation of thisfinding, whether it is associated with multipar-ity and previous procedures that might havecaused an additive damage to the lower uterinesegment, or with "weakening" of the lower seg-ment (both are associated with increasing ma-ternal age), or even if it is part of a "repro-ductive failure" that is more prevalent in olderage as is Down syndrome.PP with focal accretion: Although the associ-ation between PP and different forms of pla-centa accreta have been previously described[12], we have no apparent explanation for thefinding that 7 of 8 cases of PP with focal accre-tion had minor types of PP.PP and neonatal mortality: Most of the neonataldeaths in the present report were associatedwith vaginal delivery in women with minortypes of PP and the principal cause of deathwas respiratory distress syndrome. CRENSHAWet al. [4] reported similar findings, but it mustbe stated that the perinatal mortality rates re-
ported by them were 20 — 30% in contrast to10.7% in our study. It seems that an electivecesarean delivery in women with minor types ofPP might reduce the perinatal mortality results.In the present study we found no associationbetween antepartum, intrapartum or postpar-tum bleeding and major types of PP. This iscontradictory to previous reports by MORGAN[8], HIBBARD [7] and CRENSHAW et al. [4] whodemonstrated an association between majortypes of PP and antepartum bleeding, to thoseof COTTON et al. [3] who found a similar associ-ation with intrapartum bleeding and to thoseof Morgan [8] who described increased rates ofpostpartum bleeding in women with total PPafter cesarean section. Our findings are in ac-cordance with the recent report of COTTON etal. [3] on women with PP who underwent"aggressive conservative" management. Thisreduction in the relative incidence of blood lossassociated with major types of PP is probablypart of the trend of improving maternal andperinatal results in women with PP, being due tothe modern management policy that combinesboth conservative and active approaches.Nevertheless, in accordance with these changes,the clinical importance of the minor types of PPincreased [3, 8], a fact that was demonstrated inthe present study.The following conclusions can be drawn fromthe present work: A) Maternal age is the mostimportant etiological factor in women with PP;B) The use of the "conservative-active" man-agement protocol in cases of PP has signifi-cantly reduced the maternal and fetal-neonatalcomplication rates, has decreased the relativeimportance of the major types of PP and conci-mitantly increased the relative importance ofthe minor types of PP; and C) Performing morecesarean sections to deliver patients with minortypes of PP may further reduce the rates ofperinatal mortality in cases of PP.
Summary
The present study evaluated the association betweenmaternal and fetal-neonatal outcome in women withplacenta previa (PP) and the site of PP, i. e. low lying,
marginal, partial or total. The study group was com-posed of 154 women (159 newborns) and the controlgroup of 300 woman (305 newborns). Of the various
J. Perinat. Med. 15 (1987)

176 Gorodeski et al, Placenta previa localization
parameters examined, tljle following 3 were associatedwith PP localization: advanced maternal age was associ-ated with major types <|>f PP, while focal accretion ofthe placenta and neonatal mortality in cases of vaginaldelivery were associateji with minor types of PP. Noconnection was found between antepartum, intrapartumor postparturn blood'loss and any specific type of PP.
Keywords: Placenta previa localization.
A review of the literature and the results of the presentstudy revealed that the use of the modern aggressive(conservative — active) management protocol in womenwith PP has resulted in a significant reduction in thematernal and perinatal complication rates, as well as arelative decrease in the importance of major types of PPand a relative increase of that of the minor types.
Zusammenfassung
Einfluß der Plazentalokalisation auf das maternale undfetale/neonatale OutcomeIn der vorliegenden Studie wurden die Beziehungen zwi-schen maternalem und fetalem/neonatalem Outcome beiFrauen mit Plazenta praevia untersucht, was sowohltiefliegende Plazenten wie auch eine Plazenta praeviamarginalis, partialis und totalis einschloß. Das Kollektivbestand aus 154 Frauen (159 Neugeborene), die Kon-trollgruppe aus 300 Frauen (305 Neugeborene). Von denverschiedenen Untersuchungsparametern ergab sich beiden folgenden 3 eine deutliche Beziehung: bei fortge-schrittenem mütterlichem Alter gab es häufiger schwer-wiegende Fälle von atypischen Plazentalokalisationen,während bei leichteren Fällen von atypischen Lokalisa-
Schlüsselwörter: Plazenta-praevia-Lokalisation.
tionen häufiger eine fokale Plazenta accreta auftrat undauch die neonatale Mortalität bei vaginaler Entbindungerhöht war. Bezüglich des antepartalen, intrapartalenund postpartalen Blutverlustes gab es zwischen den ein-zelnen abweichenden Plazentalokalisationen keine Un-terschiede. Nach Durchsicht der Literatur und Berück-sichtigung der vorliegenden Ergebnisse kommen wir zuder Feststellung, daß das moderne geburtshilfliche Ma-nagement bei Frauen mit Plazenta praevia zu einer deut-lichen Reduktion der maternalen und perinatalen Kom-plikationsrate geführt hat. Die Bedeutung der echtenPlazenta praevia scheint abzunehmen, während leichte-ren Fällen von atypischen Plazentalokalisationen einezunehmende Bedeutung zukommt.
Resume
Effet de l'emplacement du placenta praevia sur le devenirmaternei et foetal-neonatalCette etude evalue l'association entre le devenir materneiet fetal-neonatal chez les femmes presentant un placentapraevia (PP) et le type du PP, c'est-a-dire: bas, marginal,partiel ou total. Le groupe etudie est compose de 154femmes (avec 159 nouveaux-nes) et le groupe contrölede 300 femmes (305 nouveaux-nes). Parmis les nombreuxparametres etudies, les 3 suivants sont correles avec lalocalisation du PP: Tage maternei eleve est correle avecles PP les plus importants, tandis que le caractere accretalocalise du placenta et la mortalite neonatale lors d'ac-
Mots-cles: Localisation du placenta praevia.
couchements par voie basse sont correles avec les PP lesmoins importants. On n'a pas trouve de relation entrela perte sanguine avant, pendant ou apres l'accouche-ment et un type particulier de PP. La revue de la littera-ture et les resultats de cette etude mettent en evidenceque la mise en service des protocoles de prise en chargemoderne et aggressifs (conservateurs-actifs) chez les fem-mes presentant un PP a entraine une diminution signifi-cative du taux de complications maternelles et perinata-les, de meme qu'une diminution relative de l'importancedes PP les plus graves et une augmentation relative decelle des PP les moins graves.
References
[1] BREEN JL, R NEUBECKER, CA GREGORI, JE FRANK-LIN JR: Placenta accreta, increta and percreta.Obstet Gynecol 49 (1977) 43
[2] BRENNER WE, DA EDELMAN, CH HENDRICKS:Characteristics of patients with placenta previa andresults of "expectant management". Am J ObstetGynecol 132 (1978) 180
[3] COTTON DB, JA READ, RH PAUL, EJ QUILLIGAN:The conservative aggressive management of pla-centa previa. Am J Obstet Gynecol 137 (1980) 687
[4] CRENSHAW C, DED JONES, RT PARKER: Placentaprevia: A survey of twenty years experience withimproved perinatal survival by expectant therapyand cesarean delivery. Obstet Gynecol Surv 28(1973) 461
J. Perinat. Med. 15 (1987)

Gorodeski et al, Placenta previa localization 177
[5] DECENZO JA: In discussion of: BRENNER WE, DA [11] PRITCHARD JA, PC MACDONALD: Williams Obstet-EDELMAN, CH HENDRICKS: Characteristics of rics, ed. 15, p 415. Appleton-Century-Crofts, Newpatients with placenta previa and results of "expect- York 1976.ant management". Am J Obstet Gynecol 132 (1978) [12] READ JA, DB COTTON, FC MILLER: Placenta ac-180 creta: changing clinical aspects and outcome.
(6] GORODESKI IG, CM BAHARI, A SCHACHTER, A Obstet Gynecol 56 (1980) 31NERI: Recurrent placenta previa. Eur J Obstet Gy- [13] VARMA TR: Fetal growth and placental function innecol Reprod Biol 12 (1981) 7 patients with placenta previa. J Obstet Gynaecol
[7] HIBBARD LT: Placenta previa. Am J Obstet Gynecol Br Commwlth 80 (1973) 311104 (1969) 172 [14] ZIEL HA: Circumvallate placenta, a cause of ante-
[8] MORGAN J: Placenta previa: report on a series of partum bleeding, premature delivery, and perinatal538 cases (1938 -1962). J Obstet Gynaecol Br Com- mortality. Obstet Gynecol 2 (1963) 798mwlth 72 (1965) 700 Received February 25, 1986. Revised August 24, 1986.
[9] NAEYE RL: Abruptio placentae and placenta previa: Accepted September 16, 1986.Frequency, perinatal mortality and cigarette smok- T , ̂ ~ A ^- \Λ π \Λ c /nr> r-vxning. Obstet Gynecol 55 (1980) 701 ^rael ?^?Γθα*δ1α> M\?" M
A Sc; (°B-GYN>
[10] NERI A, I GORODESKI, C BAHARY, Υ OVADIA: Im- £lmicf ™Τηκ?Γ· Repr°d"ctlon .pact of placenta previa on intrauterine fetal growth. ™Ρ*Λ™ c°f 9*te*?cs
1'£d ̂IST J Med Sei 16 (1980) 429 ™e Mount Smai Medical Centerv ' One Mt. Sinai Dnve
Cleveland, OH 44106-4198, U.S.A.
J. Perinat. Med. 15 (1987)


