The effect of etching on the dentin of the clinical cavity floor
6
operative Dentistry The effect of etching on the dentin of the clinical cavity floor Norimasa Kurosaki* / Minoru Kubota** / Yumiko Yamatnoto*** / Takao Fusayama**** '^^^ "'OJ/ conservative cavity préparation, which takes full advantage of chemically ad- hesive composite resin, involves removal of only the infecied outer carious dentin that is stainable by the caries detector. This preparation exposes in ¡he cavity ßoor either the l"''t>id layer at the top of the inner carious dentin or the underlying transparent layer. Examination by scanning electron microscope revealed thai etching the cavityfloorde- mineralized the interiiihular dentinal surface slightly and produced tapered, cylindrical f>ole^ or ring-shaped holes a! the dentinal tubule apertures of the turbid or transparent layer, respectively. The holes were blind with solid floors of intratubular crystal depos- '« of the transparent layer, suggesting that etching increases permeability little. Place- '"^'" '^f '^^ adhesive resin on the etched cavity floors produced a resin-itnpregnated dentinal layer and tapered, cylindrical or tubular-shaped resin tags, which apparently improved the bond and tubule aperture seal. (Quintessence Int Í99O;2Í.-87-92.) Introduction The ideal restorative technique, gentlest to teeth, is believed to be the most conservative cavity prepara- tion, which requires reduction of no more than the infected carious dentin. This preparation was enabled by development of the caries detector' and Ihe chem- ically adhesive composite resin, Clearfil (Kuraray Co),' by Fusayama et al. The new system^'"^ has already been used for one decade and has excellent technical sim- plicity and pulpal compatibility.' Two other chemically adhesive composite resins subsequently developed by modification, Scotchbond (3M Dental Products Div) and Pyrofil = D21 (Sankin Co) systems, have com- parable adhesive properties and are useful in the same system,* Associate Professor of Oral Diagnosis, Tokyo Medical and Denial University, 1-5-45 Yushima, Bunkyo-feu, Tokyo 113, Japan. Instructor of Oral Diagnosis, Tokyo Medical and Dental Uni- versity, Assistant of Oral Diagnosis, Tokyo Medical and Dental Uni- versiiy. Emeritus Professor, Tokyo Medical and Dental University, This system is simple, because both enamel and den- tinal walls are treated by one etchant, without lining, and the adhesive composite resin is immediately in- serted. It has been shown that etching of dentin con- tribiates to bond strength- as well as to pulpal protec- tion.^ ' Nevertheless, the traditional fear of dentina! etching, analogized from experiences with nonadhe- sive or insufficiently adhesive traditional composite resins, persists in some areas, Oniy enamel is etched, and the whole dentinal wall is covered by lining even if chemically adhesive composite resins are used. Such a lining considerably weakens the retentive stability and therefore requires some mechanical retention form, deviating from the ideally conservative prepa- ration.'" The lining also weakens the gingival marginal seal of a cervical restoration," The main reason for such a fear seems to be past experience with pulpal irritation by traditional ma- terials, which opened the dentinal tubule apertures by etching, increasing the cavity floor permeability of normal dentin,'- The cavity floor ot" the new system, however, is not the normal dentin, but the top of the inner carious dentin. The purpose of this study was to observe the effect of etching on the structure and character of the denttn of the clinical cavity lloor of the ideally conservative cavity preparation. 87
Transcript of The effect of etching on the dentin of the clinical cavity floor

operative Dentistry
The effect of etching on the dentin of the clinical cavity floorNorimasa Kurosaki* / Minoru Kubota** / Yumiko Yamatnoto*** / Takao Fusayama****
'^^^ "'OJ/ conservative cavity préparation, which takes full advantage of chemically ad-hesive composite resin, involves removal of only the infecied outer carious dentin that isstainable by the caries detector. This preparation exposes in ¡he cavity ßoor either thel"''t>id layer at the top of the inner carious dentin or the underlying transparent layer.Examination by scanning electron microscope revealed thai etching the cavity floor de-mineralized the interiiihular dentinal surface slightly and produced tapered, cylindricalf>ole^ or ring-shaped holes a! the dentinal tubule apertures of the turbid or transparentlayer, respectively. The holes were blind with solid floors of intratubular crystal depos-' « of the transparent layer, suggesting that etching increases permeability little. Place-'"^'" '^f '^^ adhesive resin on the etched cavity floors produced a resin-itnpregnateddentinal layer and tapered, cylindrical or tubular-shaped resin tags, which apparentlyimproved the bond and tubule aperture seal. (Quintessence Int Í99O;2Í.-87-92.)
Introduction
The ideal restorative technique, gentlest to teeth, isbelieved to be the most conservative cavity prepara-tion, which requires reduction of no more than theinfected carious dentin. This preparation was enabledby development of the caries detector' and Ihe chem-ically adhesive composite resin, Clearfil (Kuraray Co),'by Fusayama et al. The new system '̂"̂ has already beenused for one decade and has excellent technical sim-plicity and pulpal compatibility.' Two other chemicallyadhesive composite resins subsequently developed bymodification, Scotchbond (3M Dental Products Div)and Pyrofil = D21 (Sankin Co) systems, have com-parable adhesive properties and are useful in the samesystem,*
Associate Professor of Oral Diagnosis, Tokyo Medical andDenial University, 1-5-45 Yushima, Bunkyo-feu, Tokyo 113,Japan.Instructor of Oral Diagnosis, Tokyo Medical and Dental Uni-versity,Assistant of Oral Diagnosis, Tokyo Medical and Dental Uni-versiiy.Emeritus Professor, Tokyo Medical and Dental University,
This system is simple, because both enamel and den-tinal walls are treated by one etchant, without lining,and the adhesive composite resin is immediately in-serted. It has been shown that etching of dentin con-tribiates to bond strength- as well as to pulpal protec-tion.^ ' Nevertheless, the traditional fear of dentina!etching, analogized from experiences with nonadhe-sive or insufficiently adhesive traditional compositeresins, persists in some areas, Oniy enamel is etched,and the whole dentinal wall is covered by lining evenif chemically adhesive composite resins are used. Sucha lining considerably weakens the retentive stabilityand therefore requires some mechanical retentionform, deviating from the ideally conservative prepa-ration.'" The lining also weakens the gingival marginalseal of a cervical restoration,"
The main reason for such a fear seems to be pastexperience with pulpal irritation by traditional ma-terials, which opened the dentinal tubule apertures byetching, increasing the cavity floor permeability ofnormal dentin,'- The cavity floor ot" the new system,however, is not the normal dentin, but the top of theinner carious dentin. The purpose of this study wasto observe the effect of etching on the structure andcharacter of the denttn of the clinical cavity lloor ofthe ideally conservative cavity preparation.
87

operative Dentistry
Ouler Carious Dantin(carles detec(or-stainable)lo be removed
Inrer Carious DEnlin(caries deteetor-LnslaJnable)lu be fjcesBrved
' ' S.b.Turbid I Transparenl I transparenl
Normal Denlinpulp
layer I layer I layer
O i^
Perilubulidentin
Collapsing end Odontóblaslof OB. process process
Whilfookitecrystals
Interlubulsrdenim
Odontoblastprocess
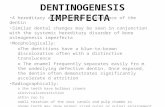
Fig 1 Contents (organic and inorganic) of the dentinal tubules in various layers ot carious dentin.
Methods
Freshly extracted human teeth with dentinal earieswere stored in water and used within 2 hours afterextraction. Following Fusayama's system,̂ experimen-tal cavities were prepared and treated as below.
Under the guide of the caries detector solution(10% Acid Red 52 in propylene glycol), the stainableouter carious dentin was completely removed.' Thisdetector was applied for 10 seconds and rinsed withwater, and then the stained dentin was excavated bya round bur mounted on a slow-speed electric hand-piece. This procedure was repeated until the remainingdentin could no longer be stained by the dye. Theturbid layer at the top of the unstainable inner cariousdentin was thus exposed in the floor of 30 cariousteeth.
Figure 1 illustrates the structure of a dentinal tubuleof carious dentin. Two previous works on the inor-ganic and organic contents of tubules'^''' define thelocation of the cavity floor. The turbid layer refers tothe thin layer of dentin in whieh the dentinal tubulesare filled with the odontoblastic processes without in-tra tu bular crystals.
In another 30 carious teeth, the cavity floors wereshghtly overredueed to reach the transparent layer be-yond the turbid layer, because overreduetion some-times occurs in clinical practice. The transparent layerwas defined as the layer below the tnrbid layer thatlooks homogeneous on ground secfions because thetubules in this region are filled with deposits of intra-tubular crystals (Fig 1).
The eavity walls of 20 of each group were thetietched with 40% phosphoric acid gel to remove thesmear layer and the cutting debris packed in the tubuleapertures. After 60 seconds of etching, the cavitieswere strongly washed with a water-jet spray for 15seconds and dried with an air syringe for 15 seconds.The cavities of 10 of the etched specimens from eachgroup were treated with a chemically adhesive bondingagent, Clearfil New Bond, and filled with Ciearfil FIlcomposite resin according to instructions. One hourafter polymerization, the restored teeth were immersedin IN of hydrochloric acid for 1 week to eliminate thedental tissue for observation of the interfacial resinsurfaces.
As a control to observe the etching effect, non-cadous dentinal cavity fioors were also prepared in 10
Quintessence International Voiume 21. 2/199f

operative Dentistry
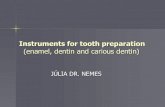
Fig 2 Scanning electron micro-graphic observation of ttie dentin ofthe cavity fioors in the normal, tur-bid, and transparent iayers beforeand after etching.
Normal layer Turbid layer Transparent layer
beforeetching
afteretching
intact, freshly extracted teeth using the same proce-dure. Five were left unetched and tlve were etched.
The side walls of the cavity were cut otT to facilitateobservation. The cavity floors, before and after etch-ing ofthe noncarious, turbid, and transparent layersof dentin, were coated with a thin film of gold andobserved by scanning electron microscope (SEM) atX 10,000 magnification following the routine proc-essing technique.'^ The resin interfacial surfaces werealso coated with gold and observed by SEM at x20,000 magnification for comparison to the corre-sponding etched dentinai surfaces.
Results
The steel bur-reduced surfaces of all three types ofdentin were covered by a smear layer, which had someclefts indicating the location of the dentinai tubules(Fig 2). When etched, the tubule apertures of the non-carious dentin showed open holes with no apparenttloors, whereas those of the turbid layer showed bhndholes. Most tubule apertures of the transparent layershowed ring-shaped depressions of smaller depth, withcylindrical cores remaining in the centers. The cores
were missing in some tubules, probably because ofthevariation in depth of intratubular crystal deposits. Theetched intertubular dentinai surface was roughest inthe turbid layer, followed hy the transparent layer.
Higher magnification (Fig 3) showed that the holeof the turbid layer was remarkably tapered and hadan apparently solid floor. The correspondent resin tagwas a conical prominence and showed a deep, hollowdepression at the top surface. The ring-shaped hole ofthe transparent layer was slightly tapered and the cor-responding resin tag was a tubular-shaped promi-nence. All of these tags stood on the resin bases andappeared rough or porous to some extent.
Discussion
Morphology of tiie etched clinical cavity floor
As previously observed,'- the cutting debris penetratedthe dentinai tubules of the noncarious dentin to dis-place the soft odontoblastic process," Acid etchingdissolved the packed debris and the peritubular den-tinai wall, producing a tapered, cylindrical hole withno solid fioor (Fig 2), The end ofthe water-rich pro-teinous process is thought to become slightly de-
Quintessence ,^ -2Í, Stwiber 2/1990
Operative Dentistry
Turbid layer Transparent layer
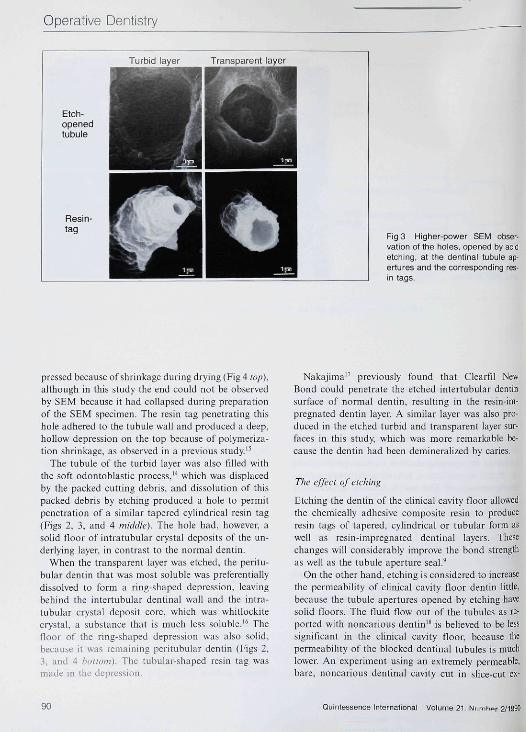
Fig 3 Higher-power SEM obser-vation of the holes, opened by acidetching, at the dentinal tubuie ap-ertures and the corresponding res-in tags.
pressed because ofshrinkage during drying (Fig 4 lop)..although in this study the end could nol be observedby SEM because it had collapsed during preparationof the SEM specimen. The rcsin tag penetrating thishole adhered to the tubule wall and produced a deep,hollow depression on the top because of polymeriza-tion shrinkage, as observed in a previous study"
The tubule of the turbid layer was also filled withthe soft odontoblastic process,''' which was displacedby the packed cutting debris, and dissolution of thispacked debris by etching produced a hole to permitpenetration of a similar tapered cylindrical resin tag(Figs 2, 3, and 4 miildle). The hole had, however, asolid floor of intratubular crystal deposits of the un-derlying layer, in contrast to the normal dentin.
When the transparent layer was etched, the peritu-bular dentin that was most soluble was preferentiallydissolved to form a ring-shaped depression, leavingbehind the intertubular dentinal wall and the intra-tubular crystal deposit core, which was whitlockitecrystal, a substance that is much less soluble,'* Thefloor of the ring-shaped depression was also solid,because it was remaining peritubular dentin (Figs 2,3, and 4 bottom). The tubular-shaped resin tag wasmade in the depression.
Nakajima" previously found that Clearfil NewBond could penetrate the etched intertubular dentinsurface of normal dentin, resulting in the resin-im-pregnated dentin layer, A similar layer was also pro-duced in the etched turbid and transparent layer sur-faces in this study, which was more remarkable be-cause the dentin had been demineralized by earies.
The effect ofetdiing
Etching the dentin of the clinical cavity floor allowedthe chemically adhesive composite resin to produceresin tags of tapered, cylindrical or tubular form aswell as resin-impregnated dentinal layers. Thesechanges will considerably improve the bond strengthas well as the tubule aperture seal,̂
On the other hand, etching is considered to increasethe permeability of clinical cavity floor dentin little,because the tubule apertures opened by etching havesolid floors. The fluid flow out of the tubules as re-ported with noncarious dentin'* is believed to be lesssignificant in the clinical cavity floor, because thepermeability of the blocked dentinal tubules is muchlower. An experiment using an extremely permeable,bare, noncarious dentinal cavity cut in slice-cut ex-
90 Quintessence International Volume 21. Numhor 2/1990

Operative Dentistry
cavityfloorofNORMALDENTIN
ClinicalcavityfloorctTURBIDLAVER
TRANSPARENTLAVEH
cutting Qebris
intertubl.• denlin EL
^ odontcblB.process
— perilLbl.denlin
. odontb. pr.
psritubl."*" dentmL
intertubl.derlin
___ crjislal
t;
(••
• • * * ««•*
~__ crystal( y j " deposition
Fig 4 Change, after etching, of the dentinal tubule aperture of normal dentin and dentin of the ciinical cavity floor, and theresin tag formation of the chemicaily adhesive composite resin.
tracted teeth'^ can also provide misleading data be-cause the permeability of hollow tubules unrealisti-cally acute with collapsing odontoblastic processes.
A number of researchers have studied the effect ofetching on dentin, but most used extracted teeth.However, acid etching affects extracted teelh far moreacutely than it does vital teeth, peuetrating the hollowdentinal tubules of extracted teeth as deeply as severalhundred micrometers. Vital dentin, which has tubuiesfilled with odontoblast processes, permits the acid topenetrate only to the depth of cutting debris packing,about 10 |im.-" Particularly in a clinical cavity floor mwhich the inner carious dentin has been left, the acidcan little penetrate through the transparent layer.
Even in noncarious dentm, the acid dissolves thesurface of apatite crystals and affects the collagen fi-bers to some extent, but the dentinal layer that is de-mineralized by etching is soon completely remineral-ized, proving that a short period of etching does notaffect the tissue deleteriously.^'
Conclusion
Etching the ciinical cavity floor in a conservative res-torative system using a chemically adhesive composite
resin does not increase permeability appreciably, andit improves the resin bond and the tubule apertureseal.
References
1. Fusayama T: Two layers of carious dentin; diagnosis and Ireat-ment. Oper Dem 1979;4:63-70.
2. Fusayama T, Nakamura M, Kurosaki N, et al: Non pressureadhesion of a new restorative resin. / Dent Res 1979;58:1364-137Ü.
3. Fuîayama T: New Concepls in Operaiivc Denlistry. Chicago,Quintessence Publ Co, 1981, pp 1-I5fi.
4 Hosoda H, Fusayama T: A tooth substance saving restorativetechnique. Int Dent J I9B3;34:1-12.
5. Iwaku M, liiokoslii S, Hosoda H. et al: Conservative dentistrywith a caries delector and a chemically adhesive composite, alongitudinal sludy of a new system. Br Den! J 1983; 155:19-22.
6. Nakajima A: Bond slrenglh of the adhesive composite resins.Part 1. J Jpn S(K Dent i^ut Dev 1983;2:623-633.
7. Inokoshi S, Iwaku M, Fusayama T' Pulpal response to a newadhesive restorative resin. J Dem Res I982;6I1(1I4~1O19.
8. Fujilani M, Inokoshi S, Hosoda H: Effect of acid etching ondental pulp in adhesive composite restoralion. J Denf ResI984;65:764 (abslr No. 34S).
9. Fusayama T: Factors and prevention of pulp irritation by ad-hesive composite resin restorations. Quintessence In!1987;18:633-641.
Quintessence I 91
Operative Dentistry
10. Phillips RW; Era of new biomalerials in esthetic dentistry. / .-itnDem Assoc 19í4?:ll5(special issue)7IE-l2E,
11. Fusayama A. K,ono A: Marginal closure of composite restora-tions with the gingival wall in cementum/demin. / Prosihei Dent1988;61:293-296.
12. Stanley HR, Going RE. Chauncay HH: Human pulp responseto acid pretrcatment of dentiti atid to composite restoration.J Am Dent Assoc 1975:91:817-825.
O. Ogawa K.. Yamashita Y. Ichijo T, el al: The ull rast rue tu re andhardness of ihe transparent layer of human carious dentiti.J Dent Ri-s 1983;62:7-10,
14, Yamada T, Nakamura M, Iwiiku M. et al: The extent of theodontoblast process in normal and carious human dentin.J Dent Res ]983;62:789-í402.
15. Iwaku M, Nakamichi I, Horie K, el al: Tags penetrating dentinof a new adhesive resin. Bull Tokyo Meci Dent Univ 1981;28:45-51.
16, Frank RM, VoegelJC: Ultrastructure of ihehutnan odonloblastprocess and its mineralization during denial caries. Caries Res1980:14:367 380,
17, Nakajima A: Bond strength of the adhesive composite resins.Part 2. Jpn J Conserv Dent 1985:28:850 863.
18, Brännslrötn M: Communication between the oral cavity andthe dental pulp associated wtth restorative treatment. Oper Dent1984:9:57-68.
19, Asmussen E: Composite restorative resins, composition verstisvvall-to-wall polymerization contraction, AeUi Odotuol Scand1975:23:337-344.
20, Iwaku M, Nakamichi [. Horie K. et al: Tags penctniting dentinof a new adhesive resin. Bull Tokyo Meil Dent Univ 1981:28:45-51,
21, Tatsumi K: Physiological remineralizaiion of artificially decal-cified monkey dentin under adhesive composite resin restora-tion, J Slonwiol Soc Jpn 1989:56:47-74, 1 I
"Innovations Prize" — Call for Papers
The Dental Society of Hessen (West Germany) has established an "Innovations Prize" tostimulate new scientific knowledge that can be used in genera! dental practice.
Papers in the following areas are welcome: Operative Dentistry. Endodontics. Prostho-dontics, Periodontics, Implant Therapy, Dental Radiology, and Oral and Ma.xillofacialSurgery. (No preference will be given to any one specialty; all papers will be treated equally.)
Regulations
• All papers must be unpublishedoriginal work.
• Prints of any illustrations should besubmitted with the paper.
Deadline for submission
September 1, 1990
Award
• The winning paper will be chosen inJanuary of 1991 by the DentalSociety of Hessen.
• An award of DM 10,000 (approxi-mately $6,000) will be given to theauthor(s) of the winning paper.
For more information
Address your inquiries to: Secretary, Zahnärztliche Gesellschaft in Hessen (DentalSociety of Hessen), Ludwigstrasse 34, D-6050 Offenbach, West Germany
92 Quintessence International Volume 21, Number 2/1990













![1.3GHz Cavity Development at TRIUMFreceived >120 P m of surface etch while most of the Phase II cavities were limited to 60P m etching [5]. This motivates the etching studies on the](https://static.fdocuments.net/doc/165x107/60a68dae024cca21206cdc39/13ghz-cavity-development-at-triumf-received-120-p-m-of-surface-etch-while-most.jpg)
