the dual arch technique demystified Jeremy Cooperonly satisfactory and durable solution to the...
3
Volume 9 No 1 • February 2015 AESTHETIC DENTISTRY TODAY EARN THREE HOURS OF VERIFIABLE WITH THIS ISSUE Volume 9 No 1 • February 2015 BEAUTY, BRAINS, AND BUSINESS ACUMEN Apprentice winner Leah Totton opens up on her range of skin clinics THE DUAL ARCH TECHNIQUE DEMYSTIFIED Jeremy Cooper AESTHETIC DENTISTRY AWARDS 2015 See the shortlist inside!
Transcript of the dual arch technique demystified Jeremy Cooperonly satisfactory and durable solution to the...

Volume 9 No 1 • February 2015
Aesth
etic Den
tistry toD
Ay
earn THree Hours of verifiable wiTH THis issue
Volume 9 N
o 1 • February 2015
Beauty, Brains, and Business acumenapprentice winner leah Totton opens up on her range of skin clinics the dual arch technique demystifiedJeremy Cooper
aesthetic dentistry awards 2015see the shortlist inside!

adt February 2015 9
‘No-prep’ adhesive restorations: dealing with aesthetic deficiencies
clinical
Dr Didier Dietschi DMD PhD Privat-Docent is a lecturer at the University of Geneva, Switzerland, and assistant professor at the University Case Western in Cleveland, Ohio, USA.
Didier Dietschi presents the indications and advantages of the concept of natural stratification in a young smile
The use of ceramics in the form of veneers or crowns was for a long time considered the only satisfactory and durable solution to the aesthetic deficiencies of the smile, in young as well as adult patients. This hegemony of ceramics, which tends to linger, is favoured by the dental industry that invests significant amounts of money to promote its materials and new technologies, without always showing a lot of consideration for the biomechanics of the healthy tooth.
The sheer aesthetic criteria must therefore be weighed against the biological and mechanical fundamental principles of the natural tooth in order to ensure the longevity of the restorations on the one hand, and preserve the vitality and the integrity of the dental organ on the other. Thus, these considerations have been encouraging dentists for a long time to consider direct bonding techniques as a first choice alternative for the treatment of aesthetics deficiencies in a young smile, especially (and generally) every time the extent of the defects allows it (Macedo, Raj and Ritter, 2006; Peumans et al, 1997; Dietschi, Ardu and Krejci, 2006; Magne and So, 2008; Dietschi, 2008).
According to studies, the improvement of the aesthetic properties of restorative composite materials based on the model of the natural tooth (Magne and So, 2008; Dietschi, 2008; Cook and McAree, 1985; Dietschi, Ardu and Krejci, 2000; Ubassy, 1993) also make
direct restorations available to everyone, since they are no longer the prerogative of gifted clinicians trained to complex stratification techniques, inaccessible to the general practitioner.
Indeed, several systems have been developed during the past 10 years that have been building on the concept of natural stratification, consisting of only two basic layers (dentine and enamel) and an appropriate shade guide.
The clinical protocols logically followed a simplification and an increase in reliability, which bodes well for our profession (always under economic pressure).
Moreover, clinical results in the medium and long term about the use of direct composite
as an aesthetic correction material proved to be reliable (Dietschi, 1995; 1997; 2001).
The goal of this article is to present two clinical cases that illustrate the direct therapeutic approach and the aesthetic potential of composite systems based on the concept of natural stratification.
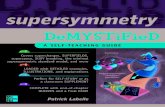
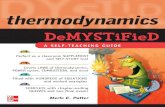
Clinical casesCase one – diastema closureThis first case presents a simple application of direct bonding for diastema closure in a young patient also showing a dark dentine shade, as well as a mild fluorosis especially visible on incisal edges and canine tips (Figure 1).
Given the age of the patient (15 years old), it was decided not to treat the fluorosis,
Education aims and objectives This article aims to demonstrate two clinical cases that illustrate the direct therapeutic approach and the aesthetic potential of composite systems based on the concept of natural stratification.
Expected outcomes Correctly answering the questions on page 54, worth one hour of verifiable CPD, will demonstrate that the reader understands the indications and advantages of the concept of natural stratification in providing reliable and highly aesthetic results.
Figures 1-4: Preoperative extra- and intraoral views of a young patient showing bilateral diastemas, complicated by a mild fluorosis

adt February 2015 33
Sharp needles versus blunt cannulas
facialaesthetics
Dr Ian Hallam MBE BDS qualified in dentistry at Birmingham University in 1971. He owns two private practices in Petersfield, Hampshire, dividing his time between cosmetic and implant dentistry at Meon Dental, and
facial aesthetics at Meon Face, which he launched in 2012. He is a former professional racing cyclist and was a double Olympic and World Championship medallist and triple Commonwealth Champion.
Ian Hallam discusses the relative merits of needles and cannulas when it comes to facial aesthetic treatments
I am often asked whether I use needles or cannulas. Traditionally, the way to inject products into the face was by using fine needles. These varied from short 30-gauge needles for injecting botulinum toxin to long 21-gauge for injecting viscous fillers for chin or cheek augmentation.
The only alternative was comparatively thickly walled, blunt-ended cannulas, which required an incision using a scalpel to make the entry point. This placed the technique more into the hands of a plastic surgeon.
However, more recently, very thinly walled flexible cannulas have been made available by companies such as Q-Med and Thiebaud (Pix’l), Merz amd Cosmofrance (Dermasculpt) and Tochigi-Ken in Japan (TSK Steriglide), and this has made it possible for most aesthetic practitioners to have the choice of using either needles or cannulas (Figure 1).
There are advantages and disadvantages of each, so which technique is best? Table 1 shows the comparative merits of needles and cannulas.
Familiarity and ease of useAs dental surgeons, we are familiar with the use of needles. We give many injections every day and are very skilled with how to use them. Although it is different injecting into the face, we are better placed than other aesthetic practitioners who may not be as comfortable using needles and may have to learn to hold
a syringe in a steady and controlled way, so as to inject safely.
However, the use of cannulas is a technique that we all have to learn. It involves making an initial entry point using a needle of the same or slightly larger diameter, followed by inserting the cannula into the hole created at the same path of entry. This can sometimes be more challenging because the hole created is very small and the blunt tip tends to slide across the surface of the skin (Figures 2-4).
ControllabilityA sharp needle will penetrate the tissues with ease whereas a cannula will meet the resistance of the different facias and retaining ligaments. In the more superficial levels such as the dermis or subdermal layer, there is little resistance using a cannula, but in the
deeper levels such as cheek augmentations or tear troughs, resistance is encountered and it may be necessary to withdraw slightly and advance again in order to penetrate a retaining ligament.
Furthermore, in order to assess the depth and position of the tip before injecting, it is easy to feel the tip of a needle when lifting the syringe. However, due to the flexibility of the narrower diameter cannulas and their length,
Needles Cannulas
Familiarity Familiar Unfamiliar
Ease of use Easy Difficult
Controllability Easily controlled More difficult
Lengths available Shorter lengths Long
Diameters Multiple choice Choice but not ultra-fine
Entry points Often multiple Minimum
Patient comfort Some discomfort Little discomfort
Post-operative inflammation Can be high Can be low
Risk of bruising High Low
Results Good Good
Table 1: Comparison between needles and cannulas
‘A sharp needle will penetrate the tissues with ease whereas a cannula will meet the resistance of the different facias and retaining ligaments’
Figure 1: Needles or cannulas? Figure 2: Cannula for treating tear trough and lid/cheek junction